
Abstract
Objective:
Problematic maternal alcohol use confers risk for child maltreatment, though the effect on specific aspects of parenting is unclear. This study examined concurrent and prospective links among maternal alcohol use history, care neglect, supervisory neglect, and harsh or inconsistent discipline.
Method:
Multimethod multisource data were utilized to assess deficient parenting in 311 economically disadvantaged mothers at high risk of child maltreatment. Structural equation modeling was used to test hypothesized relations.
Results:
Maternal history of alcohol use was associated with more inconsistent discipline and higher levels of subsequent supervisory neglect. Secondary analyses among two-parent families found that paternal substance misuse was associated with maternal care neglect and poor supervision.
Conclusions:
Among low socioeconomic status families, maternal alcohol use increases the risk of inconsistent discipline and inadequate supervision. Inconsistent discipline may also lead to punitive parenting practices. Given the potential effect of paternal substance use on maternal parenting, findings highlight the importance of screening all caregivers for substance use in child welfare and research contexts to clarify when and how to intervene most effectively.
Excessive use of alcohol and illicit substances has long been implicated as a contributor to deficient parenting and poor child outcomes. Recent estimates suggest that 8.7 million children in the United States reside with a parent who misuses substances, with alcohol use in particular having the broadest reach (Lipari & Van Horn, 2017). Alcohol misuse may place parents at an increased risk of maltreating their children (Seay, 2015; Sedlack et al., 2010) and has been linked to higher rates of substantiated re-reporting to child welfare (Fluke et al., 2008). Research to date has primarily examined this association within the context of the child welfare system or under circumstances of more severe alcohol use (e.g., Chaffin et al., 1996; Murphy et al., 1991), which may result in the selection of restricted samples and limit the generalizability of findings (Widom, 1988). Furthermore, evidence of substance misuse in the home is often assumed to be an unequivocal indication of neglectful parenting. As such, it is difficult to delineate the specific role of problematic parental alcohol use in parenting practices when it is taken as prima facie evidence of poor parenting.
Child maltreatment has been conceptualized as falling on the extreme end of a continuum of deficient parenting, and findings support the utility of this approach in predicting adverse child outcomes (e.g., Knutson et al., 2004, 2005). Such an approach accounts for the theoretical and empirical associations between types of deficient parenting (e.g., neglect, supervision, harsh or inconsistent discipline) and allows for a more fine-grained examination of how parental alcohol use relates to specific aspects of deficient parenting. While it has been postulated that parental alcohol or substance use generally impairs parenting skills (Dunn et al., 2002), it is less clear whether specific aspects of parenting are compromised, particularly when accounting for the overlap between neglectful and abusive parenting practices, which tend to be highly comorbid (Herrenkohl & Herrenkohl, 2009). The current study builds on the deficient parenting framework to explore how problematic alcohol use might increase the risk of neglectful parenting, poor supervision, and inconsistent or punitive discipline.
Parental alcohol misuse has been linked to neglectful parenting (Connell-Carrick, 2003), though neglect is a broad construct that is often poorly differentiated within the literature. Care neglect has been defined as the failure to provide for a child’s essential health, nutritional, and environmental needs (e.g., Trocmé, 1996). It has been suggested that parental alcohol or substance use could increase the risk of care neglect by reducing one’s capacity to respond to a child’s needs (Child Welfare Information Gateway, 2014). To date, there has not been a direct examination of this association. Supervisory neglect refers to inadequate awareness of a child’s behavior, locus of activity, and peer relationships to minimize deviant behavior or involvement in a hazardous activity, with the implication that such awareness is a prerequisite for effective monitoring. The link between parental alcohol misuse and supervisory neglect has garnered more attention, though evidence for this association is somewhat mixed (e.g., Coohey, 2008; Freisthler et al., 2014). Notably, prior research has demonstrated that poor supervision increases the risk of care neglect (e.g., Knutson et al., 2005), though studies examining the effects of alcohol use on parenting have not taken these relations into account.
Research has also demonstrated that parental alcohol misuse increases the risk of harsh discipline and physical abuse, particularly among parents with more severe use (Fluke et al., 2008; Freisthler & Gruenewald, 2013). Interestingly, Miller et al. (1999) found that substance use problems significantly predicted mothers’ punitiveness, even when these problems were in remission, suggesting that a history of problematic alcohol or substance use may continue to influence mothers’ use of punitive discipline. While previous models of punitive discipline have combined inconsistent and harsh parenting (e.g., Knutson et al., 2005), inconsistent discipline is also conceptualized as the foundation of developing harsher parenting practices over time (Reid, 1986). Moreover, there is some evidence that parents with histories of substance misuse are less consistent relative to parents without problematic substance use (Arria et al., 2012). As such, parents with a history of alcohol or substance misuse may be more likely to respond to child misbehaviors in an inconsistent or erratic matter and over time escalate to punitive and injurious strategies (cf. Patterson, 1982).
Overview of the Current Study
The present study examined whether problematic maternal alcohol use was associated with deficient practices in an economically disadvantaged sample at high risk of child maltreatment. Based on prior research, it was hypothesized that problematic maternal alcohol use would be associated with greater levels of care neglect, supervisory neglect, and harsh and inconsistent discipline. Prospective studies examining these associations over time are lacking. As such, we assessed parenting at two time points and based on the work of Miller et al. (1999) hypothesized that maternal alcohol use would be associated with higher levels of deficient parenting 1 year later. Associations among parenting constructs were specified in the model based on previous studies examining relations among care neglect, supervision, and punitive discipline (e.g., Knutson et al., 2004, 2005). Given the work regarding coercive family processes (Patterson, 1982), it was also hypothesized that inconsistent discipline would be associated with higher levels of harsh discipline.
Finally, evidence of child maltreatment, and in particular, child neglect, is often based on presumed maternal responsibility (i.e., inadequate care), regardless of whether mothers are the actual perpetrators. Nonetheless, research suggests that paternal substance use is a risk of different types of child maltreatment (e.g., Coohey & Zhang, 2006) and may account for some of the association between maternal alcohol use and maltreatment (Smith et al., 2007). Thus, paternal substance misuse may operate through both direct and indirect pathways to confer risk of child maltreatment (Guterman & Lee, 2005). As such, a secondary aim of this study was to examine the association between problematic paternal substance use and maternal parenting practices. It was hypothesized that paternal substance misuse would be associated with higher levels of maternal deficient parenting.
Method
Participants, Recruitment, and Eligibility
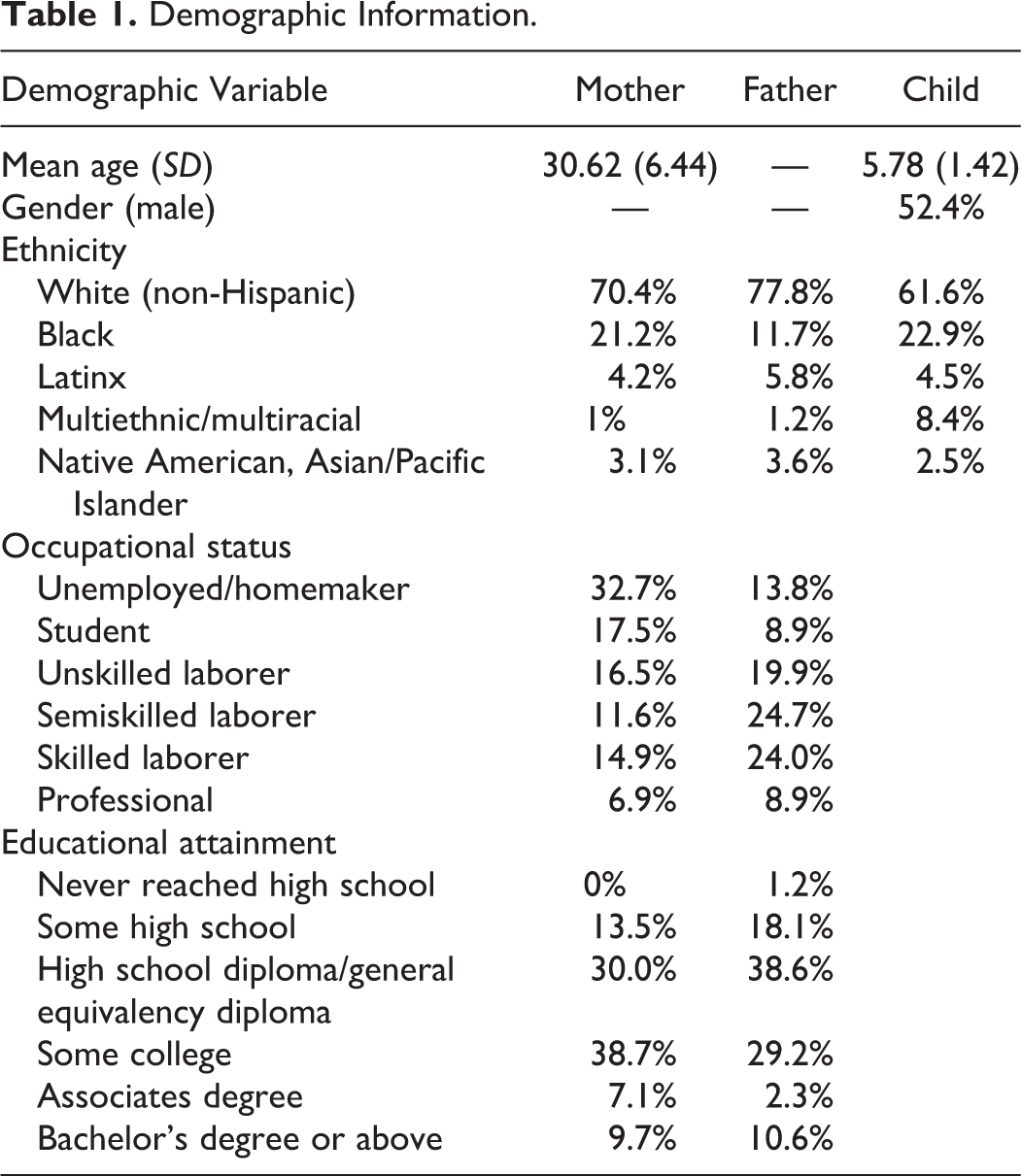
The current sample was drawn from 335 economically disadvantaged families who were enrolled in a 3-year longitudinal study examining neglectful parenting and children’s aggression. Of these 335 families, 7 withdrew after the initial in-home session (2% attrition) and 17 single-father families were excluded from the present study given the focus on maternal alcohol use. Within the remaining 311 families, 98% of maternal caregivers were the child’s biological mother. The present study reports on data from the first 2 years of the parent project. Approximately 21% of families were lost to follow-up between Years 1 and 2, primarily due to moving out of the area. The sample was diverse with respect to occupational status and educational attainment (see Table 1). In addition, the sample was significantly more ethnically diverse than the geographical catchment areas from which they were recruited. At the time of enrollment, 45% of children were residing in single-parent homes; 58% of children in two-parent homes were residing with both biological parents. The number of siblings residing in the home ranged from 0 to 7 (M = 1.4, SD = 1.2, median = 1).
Demographic Information.
Participants were recruited from two counties in Southeast Iowa and North Central Wisconsin, selected to assure the sample was diverse with respect to degree of urbanization. English-speaking families with a child between the ages of 4 and 8 years who were recipients of social services were eligible to participate whether they had been newly referred for neglectful or physically abusive parenting in the preceding 90 days, the child had not been in an out-of-home placement, and the family had not been recipients of intensive in-home interventions. Families receiving economic assistance (e.g., Temporary Assistance for Needy Families, Medicaid, Food Stamps) or health care support (e.g., Title XIX) were also eligible. Children residing in out-of-home placements were not enrolled because the study focused on naturally occurring parent–child relations, and such services could directly impact parenting of that child or preclude the direct observational methods used. Because the focus of the larger study was on neglect and harsh discipline, families of children known (at the time of enrollment) to have been sexually abused were not eligible.
Procedures
Agency administrators from the social services agencies in each county (e.g., Department of Human Services [DHS]) provided eligible families with an initial letter informing them of their eligibility to participate in a research study. The letter included information on how to contact the research team to learn about the project and schedule an initial in-home meeting, for which they would be compensated US$50. They were informed that participation or failure to participate would not influence their eligibility for any services. Informing sentinel agencies whether families enrolled in the project was prohibited due to the study being issued a Certificate of Confidentiality from NIH to protect participants’ privacy. Thus, there were no social service or clinical inducements to participate.
Given the complexity of recruitment procedures, it is impossible to determine the exact number of eligible families who were actually contacted (i.e., read the recruitment letter). Based on indirect evidence from telephone contacts (institutional review board [IRB] precluded leaving messages), returned letters, and focus groups in the target population, it is estimated that initial recruitment efforts actually reached approximately half of eligible parents, with approximately 55% of the contacted families scheduling an in-home visit. Less than 1% of those scheduling a visit declined to participate. Based on contemporaneous county records, the sample in WI closely matched the ethnic and racial composition of the populations from which they were drawn; the sample in IA included a somewhat greater percentage of minority group members than would be expected from the population of DHS recipients in the recruitment area. This study was conducted under approval of the University of Iowa IRB.
Informed consent was obtained during the initial in-home appointment, followed by a semistructured interview (described below), conducted by two trained research assistants. After the home visit, all data were collected continuously during laboratory sessions, typically scheduled within 30 days of enrollment. In subsequent years of the study, families were contacted approximately 12 months after their initial consent to schedule laboratory visits. Items or measures relying on direct home observation were modified or omitted in follow-up years. Parents were compensated $50 and children were compensated $10 or the selection of a toy (valued at $10), for each session in which they participated.
Measures
Home interview
A semistructured interview was completed in participants’ homes during the initial appointment in order to obtain information regarding demographics, family background, home safety, and parenting practices (e.g., parental routines, supervision, discipline). This interview was based, in part, on a version of the Home Observation for Measurement of the Environment (Caldwell & Bradley, 1978) modified for the Project on Human Development in Chicago Neighborhoods (Leventhal et al., 2004) and, in part, on the information framework emerging from recommendations of the Research Sub-Committee of the Interagency Task Force on Child Abuse and Neglect (Sternberg et al., 2004). During Year 2 of the study, this interview was administered during laboratory sessions.
Care neglect index
The care neglect index (cf. Knutson et al., 2004, 2005) is a 49-item summative risk index derived from parent report and objective observer ratings (e.g., a child does not have a toothbrush) during the home interview, and household environmental conditions that could occasion social (e.g., inadequate living space) and physical (e.g., access to hazardous substances, inadequate plumbing) risks for the child. Immediately following the interview, proximal circumstances observed outside the home that could occasion direct risk to the child (e.g., broken glass, unsecured containers of toxins) were also rated jointly by two research assistants conducting the home interview. All items were scored dichotomously in a direction to indicate neglect and summed. Because families completed all assessments in the laboratory during follow-up years, direct observational items of the home were not obtained, and the Year 2 care neglect index included only the 34 items based on parental self-report.
Supervisory neglect
Supervisory neglect was assessed using two measures. During the first year of the study, children and parents independently completed the Children’s Experiences and Excitement Scale (CEES; Selner, 1992) in the laboratory. The CEES consists of 44 slide images each depicting a child engaging in a range of deviant (e.g., stealing, setting fires, taking drugs) and nondeviant (e.g., eating, sleeping, cooking) activities. Respondents are asked to indicate “yes,” “no,” or “don’t know,” whether the child ever engaged in each depicted activity. To minimize sex role responding, separate forms are used for girls and boys, depicting either all female or all male actors. The final CEES score was the summation of a disagreement score and inadequate knowledge score. Disagreement was calculated by adding discordant mother–child pairs (i.e., yes–no and no–yes) across all slides. Inadequate knowledge was calculated by counting the number of “don’t know” parent responses. The CEES has demonstrated suitable reliability and validity in previous studies predicting the occurrence of accidental injury (Selner & Knutson, 1990) and distinguishing between children with conduct problems (Selner, 1992). The second measure was a summative index of supervisory neglect, derived from the home interview, which included 9 items related to parental supervision (e.g., lack of a curfew, lack of awareness of child’s activities, child eating meals alone). Responses were scored dichotomously in a direction to indicate poor supervision (higher scores reflect less supervision) and summed. Total scores from the CEES and supervisory neglect index were standardized and summed to generate a single indicator of poor supervision. In Year 2, total scores on the supervisory neglect index were used as the sole indicator of poor supervision.
Harsh punitive discipline
Harsh discipline was assessed using three measures. Seven dichotomous questions included in the home interview were used to assess maternal abusive disciplinary practices. In Year 1, these items included recent events (i.e., spanked in the past week) and lifetime occurrence for lower base rate items (e.g., whether child ever experienced bruising, fractures, sutures, from being disciplined). In Year 2, items referenced both recent events and events within the past year. Mothers’ responses were scored as 0 (did not occur) or 1 (occurred) and summed. Second, an analog parenting task (APT) was administered in each year of the study to assess acceptability of physical discipline in response to child transgressions. Analog tasks were chosen because they allow for a standardized set of stimuli and are able to effectively evoke discipline responses (DeGarmo et al., 2006; Shay & Knutson, 2008). In Year 1, the APT (Zaidi et al., 1989) was administered, which consists of 28 slides depicting a child engaging in a destructive, dangerous, rule violating, or age-appropriate activity. Parents are asked to respond as the depicted child’s caretaker and indicate their emotional reaction, classify the behavior, and select a disciplinary response to each image from a closed set of choices (e.g., takeaway privileges, spank, strike other than spanking). They are also asked to indicate how many times they would allow the child to engage in the behavior before changing their disciplinary strategy and to select an alternative response. Two measures were obtained from the APT: total physical discipline (the number of initial choices that involved the use of physical discipline) and escalated discipline, which is either a shift from nonphysical to physical discipline or from physical discipline that is minor (e.g., spanking) to more severe (e.g., striking with an object), in response to persistent child behavior.
In Year 2, a video APT was used that consists of nine video episodes depicting a child engaging in destructive, dangerous, rule violating, or age-appropriate activity. Each episode is broken into one to six sequentially ordered scenes and depicts a child engaging in a potentially irritating manner. At the end of each scene, the video is interrupted and parents are asked to respond to a series of questions as the depicted child’s caretaker, including evaluating the behavior and selecting 1 of the 10 disciplinary response options (e.g., no response, explain why the behavior is wrong, yell at the child, spank the child). As the episode continues, the child persists, ceases, or increases the intensity of the behavior. This task has previously been used to assess escalated physical discipline (Shay & Knutson, 2008). The number of harsh disciplinary responses endorsed across scenes was used as the final score.
The third measure of harsh discipline was derived from microsocial indices of parent–child interactions coded from videotaped interactions that occurred during a structured laboratory task. The Year 1 task is a 45-min interaction involving a communication task, a social problem-solving task, discussion of an important issue regarding the child’s behavior (chosen by the parent), and free play followed by “cleanup” (see Knutson et al., 2005, for a more detailed description of the task). In subsequent years, the interaction task includes only the discussion of an important issue, child-led play, parent-led play, and cleanup. A professional team of coders at the Oregon Social Learning Center coded the videotapes using the Family and Peer Process Code (Stubbs et al., 1998). Rate per minute frequencies of mothers engaging in negative physical behavior toward their child (e.g., hit, pinch, slap) during the interaction were calculated. Due to a very low base rate of these physical behaviors, scores were coded dichotomously to represent the presence (1) or the absence (0) of observed physical discipline. In order to establish inter- and intracoder reliability, 15% of the video records were sampled, with sampling conducted continuously to guard against coder drift. Throughout coding, coders had to meet minimum standards of 75% effective agreement (κ = .65) for content and affect codes or recalibration training was required. Reliability indices were all above the minimum standards with all effective agreement scores at least 89% and all κ scores at least .75.
Inconsistent discipline
Inconsistent discipline was assessed with two measures, combined using principal component factor analysis. First, during the home interview (and follow-up interview), mothers reported how frequently they responded to their child’s misbehavior in an inconsistent or erratic manner (e.g., do not follow through when punishing child), ranging from never/almost never to all of the time. Response were scored as 0 (consistent) or 1 (inconsistent) and summed; the index contains 11 items. Second, rate per minute frequencies of observed maternal aversive behaviors (e.g., anger, hostility, contempt) directed toward the child during the laboratory interaction tasks (described above) were calculated.
Parental alcohol and substance use
Maternal history of alcohol use was assessed using the Michigan Alcohol Screening Test (MAST; Selzer, 1971), which is a 25-item screener widely used to obtain information regarding alcohol-related problems and problem severity. Potential scores range from 0 to 53. According to Skinner’s (1982) problem severity criteria, scores ranging from 7 to 24 reflect clear evidence of drinking-related problems, and scores ≥25 reflect substantial problems. If mothers reported having an intimate partner who resided in the home and provided care for the child, they were also asked whether that individual had a history of problematic alcohol or substance use scored dichotomously as 0 (no) or 1 (yes).
Covariates
Three control variables were included in the analyses. First, even within a disadvantaged sample, there is variance on a number of socioeconomic status (SES) factors, and such factors have been identified as conferring risk of both child maltreatment (Sedlak et al., 2010) and alcohol misuse (Huckle et al., 2010; Widom & Hiller-Sturmhofel, 2001). Three markers of SES were combined using principal components analysis: maternal education, maternal occupation, and self-reported social status. Mothers reported their highest level of educational attainment and current occupation (see Table 1). The SES Scale of the Home Environment Questionnaire (HEQ; Sines et al., 1984) was used to assess social status. Second, the number of siblings residing in the home was controlled, as larger family size has been linked to risk of abusive and neglectful parenting (Sedlak et al., 2010). Finally, because a chaotic or unstable home environment could impact parental alcohol use and/or parenting practices, household instability was assessed. In Year 2, parents reported changes in the home that had occurred during the previous year, including whether the enrolled child had moved out of the home for any period of time, the number of residential moves, parental separations, and changes in household composition (i.e., persons moving into or out of the home). Responses were scored dichotomously and summed with the final score reflecting the total number of changes in the child’s home during a 12-month period.
Analytic Strategy
The hypothesized associations among maternal alcohol use and deficient parenting were tested using structural equation modeling (SEM) techniques in IBM SPSS Amos Version 21 (Arbuckle, 2012), which uses full information maximum likelihood (FIML) for the estimation of missing data. FIML estimates a likelihood function for each individual based on the variables that are present, so all available data are used. SEM is particularly suited for multimethod multisource covariance matrices used in the present studies because it can control for method and source biases, allowing for examination of the unique variance of each construct. The structural model was tested first in the full sample to examine the hypothesized relations among the variables of interest. To address the secondary aim, a second structural model was estimated to examine relations among maternal alcohol use, paternal substance use, and maternal parenting practices (two-parent households only). The following fit indices and recommended cutoffs were used to determine goodness of fit, based on recommendations by Kline (2016) and Hu and Bentler (1999): χ2 test statistic (nonsignificant at p < .05), the comparative fit index (CFI; ≥ .95 for excellent fit), and root mean square error of approximation (RMSEA) with its 90% confidence interval (RMSEA; <.06 for good fit). Reported model parameters are statistically significant at the .05 level.
Results
Preliminary Analyses and Descriptive Statistics
Descriptive statistics and bivariate correlations for all measures are reported in Tables 2 and 3. Even within this at-risk sample, indices of care neglect, supervision, and inconsistent discipline were normally distributed, suggesting an adequate range of parenting behavior. Although total scores of physical discipline were low overall, 82% of mothers reported using at least some form of physical discipline, 18% endorsed initial physical discipline responses on the analog task, and 29% were directly observed engaging in physical discipline during the parent–child interaction. Mothers’ rates of problematic alcohol use were low overall, though comparable to the rate of problematic alcohol use in the general population at the time of the study (Substance Abuse and Mental Health Services Administration, 2007). On the MAST, approximately 10% (n = 32) of mothers reported clear evidence of drinking-related problems (Score 7–24) and less than 3% (n = 8) reported substantial problems (score ≥ 25; Skinner, 1982). In 25% of two-caregiver households, mothers reported that the paternal caregiver had a history of problematic alcohol or substance use (n = 43).
Descriptive Statistics.

Note. APT = analog parenting task; CEES = Children’s Experiences and Excitement Scale; FPP = Family and Peer Process Code; HEQ = Home Environment Questionnaire; MAST = Michigan Alcohol Screening Test.
Bivariate Correlations Among Parenting Measures and Maternal Alcohol Use.
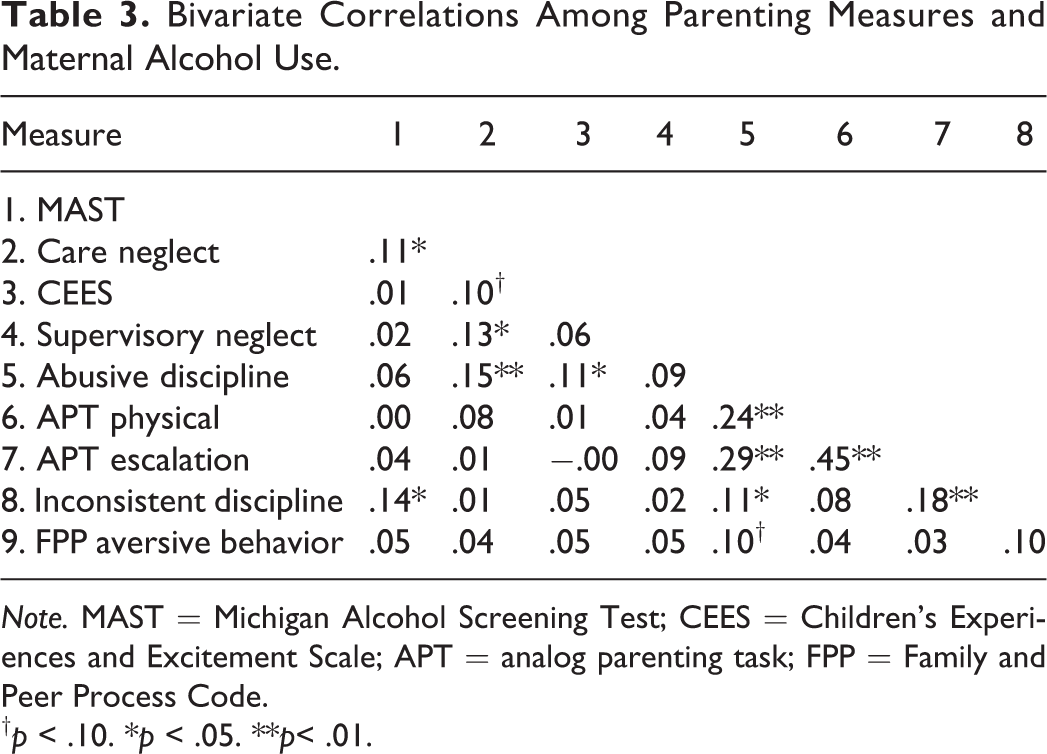
Note. MAST = Michigan Alcohol Screening Test; CEES = Children’s Experiences and Excitement Scale; APT = analog parenting task; FPP = Family and Peer Process Code.
Prior to conducting the SEM analyses, variable distributions were examined to ensure normality (i.e., skewness < 2 and kurtosis < 5), and when needed, transformations were applied to the raw scores. A logarithmic transformation (ln[X + .5]) was applied to the APT scores, the analog video score, and observed maternal aversiveness scores; the square root transformation was applied to MAST scores. Subsequently, all variables fell within the limits of skewness and kurtosis noted above. Of note, although harsh discipline was originally modeled as a latent variable at each time point, the CFA did not achieve an admissible solution. As such, the individual indicators of harsh discipline were combined using principal component analysis in SPSS Version 21, and the factor scores were used in the structural model.
SEM Results
As shown in Figure 1, examination of the structural model yielded an excellent global fit: χ2 = 24.93 (311), p = .63, CFI = 1.00, RMSEA = .00, 90% CI [.00, .04]. Examination of the component fit suggests that in Year 1 of the study, there was no significant direct effect of maternal alcohol misuse on care neglect, supervisory neglect, or harsh discipline; however, the direct path from maternal alcohol history to inconsistent discipline was significant and positive (β = .11). Interestingly, the pattern of these associations changed over time. In Year 2, the direct path from maternal alcohol history to poor supervision was significant and positive (β = .13), while the path to inconsistent discipline was no longer significant. Maternal history of alcohol misuse was also associated with greater household instability in Year 2 (β = .15), though household instability was not associated with any of the Year 2 parenting measures. The direct paths from SES to concurrent care neglect (β = −.22) and inconsistent discipline (β = −.19) were also significant and negative. Having more siblings in the home was associated with higher levels of supervisory neglect (β = .15), but lower levels of inconsistent discipline (β = −.12). Finally, larger family size was also negatively correlated with SES (r = −.16).
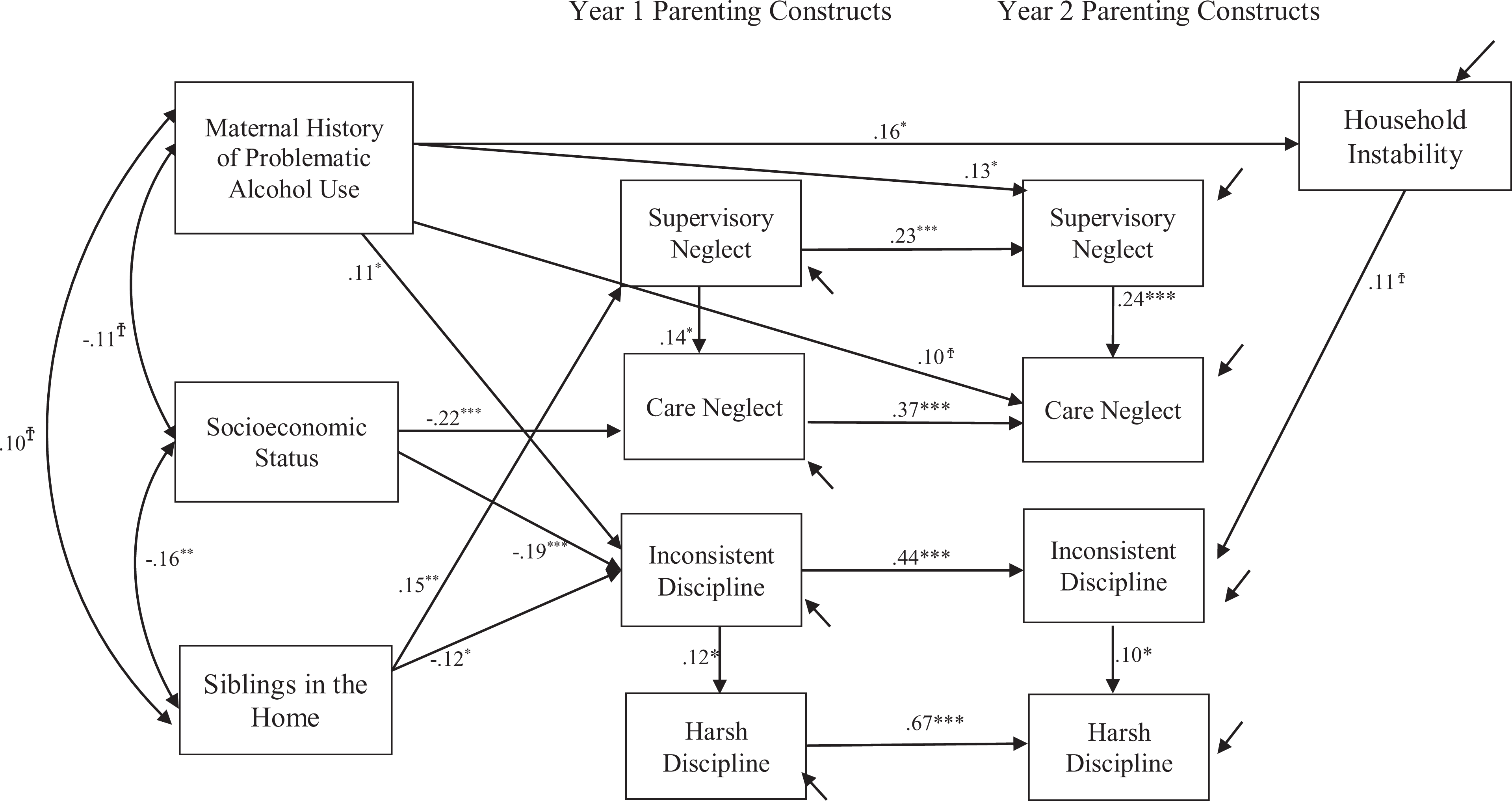
Associations between maternal alcohol use history and deficient parenting. Note. χ2 = 24.93 (311), p = .631, comparative fit index = 1.0, root mean square error of approximation = .00 (.00, >038; †p < .10. *p < .05. **p < .01. ***p < .001). Sample size in Year 1 was n = 311; Sample size in Year 2 was n = 251.
Consistent with previous research, poor supervision was associated with higher levels of neglect, and this was consistent across Years 1 and 2 (β = .14 and β =.24). Unlike previous findings, there was no association between care neglect and harsh discipline. In contrast, the direct path from inconsistent discipline to harsh discipline was significant and positive in both years (β = .12 and β = .10). Parenting practices were generally stable from Year 1 to Year 2 (βs ranged from .22 to .66).
Paternal substance use
In order to examine the potential influence of paternal substance use on maternal parenting practices, a second structural model was tested using two-parent households only, which included mothers’ reports of problematic paternal substance use history (see Figure 2). Results yielded an excellent global fit: χ2 = 30.87 (172), p = .52, CFI = 1.00, RMSEA = .00, 90% CI [.00, .05]. The direct paths from history of paternal substance use to maternal supervisory neglect (β = .18) and care neglect (β = .18) were significant and positive; however, paternal substance use history was not significantly associated with maternal disciplinary practices. Paternal substance use was associated with higher levels of household instability in Year 2 (β = .23). Within these families, lower SES was also associated with greater household instability in Year 2 (β = −.21). Finally, maternal alcohol histories were only marginally related to paternal substance use history (r = .14, p =.08).

Associations between paternal alcohol use history and maternal deficient parenting in two-parent households. Note. χ2 = 30.87 (172), p = .52, comparative fit index = 1.00, root mean square error of approximation = .00 (.00, .05; †p < .10. *p < .05. **p < .01. ***p < .001). Only significant covariances and regression paths are shown. Because paternal substance use was the primary variable of interest, those associations are in bold.
Discussion
The current study examined associations among mothers’ problematic history of alcohol use, neglectful parenting, and discipline, within an economically disadvantaged sample. Of note, these findings reflect the use of transformed scores for some variables (maternal alcohol use and harsh discipline), in order to minimize the influence of outliers and distributional aspects of the data. Overall, findings suggest that a mother’s history of problematic alcohol use may be associated with difficulties responding to her child’s misbehavior in a consistent manner. In addition, over time, alcohol use history may be a risk factor for inadequate supervision.
Interestingly, there was somewhat of a delayed effect on maternal alcohol misuse on supervisory practices, in that the association was only significant in Year 2 of the study. This is consistent with previous work that has found supervision to become more influential as children develop and become increasingly independent (Loeber et al., 2000). Although the lifetime assessment of alcohol use adds complexity to understanding the timing of this association, it may be that supervisory practices are most likely to be negatively affected later in development, when children begin engaging in more activities outside the home, regardless of whether mothers are currently or had previously been misusing alcohol. This account is bolstered somewhat by the fact that the measure of supervision emphasized maternal awareness of child reported activities outside the direct involvement of the mother. In contrast, mothers’ history of problematic alcohol use was not associated with her ability to provide adequate care. Although theoretical arguments for this association have been made, the current data suggest that when associations between types of deficient parenting are taken into account (e.g., Knutson et al., 2005), maternal alcohol use history is not uniquely associated with care neglect. These findings highlight the importance of differentiating among types of neglect, consistent with what others have argued (e.g., Freisthler et al., 2014). Moreover, it is possible that a mother’s ability to provide adequate care is influenced in states of acute intoxication rather than in an ongoing or cumulative manner.
With regard to harsh discipline, in contrast to previous research (e.g., Chaffin et al., 1996; Miller et al., 1999), there was no direct association between maternal alcohol misuse and harsh discipline. There are important differences between the current sample and those reported in earlier studies, however. First, the current sample was characterized by less severe levels of alcohol use and child maltreatment than is typical of administratively defined samples (e.g., Famularo et al., 1992; Murphy et al., 1991). Second, mothers were reporting on their lifetime history of alcohol use problems rather than current problems. As such, while some of the mothers with elevated MAST scores may have been currently abusing alcohol, it is likely that a portion of the sample was no longer evidencing problematic drinking. While Miller et al. (1999) found higher levels of maternal punitiveness even when problems were in remission, they examined alcohol and substance use problems, occurring during the previous 12 months, rather than in their lifetime. Thus, maternal alcohol use may increase the risk of abusive discipline under more severe circumstances of use or in a more proximal fashion. Moreover, previous studies have not accounted for the role of inconsistent discipline in the development of punitive discipline practices (Patterson, 1982). Our findings demonstrate that within the context of economic disadvantage, inconsistent discipline is associated with both harsh discipline and maternal alcohol use history, and links between these constructs warrant further attention.
Maternal alcohol use was also associated with greater household instability in Year 2. Although there was no direct effect of household instability on parenting, within the context of economic disadvantage, children residing with a mother with a history of alcohol problems may be at greater risk of disruptions in the home. In turn, such instability could confer risk of other important adverse child outcomes. In addition, consistent with previous research (e.g., Knutson et al., 2004), lower SES was associated with higher levels of neglect and inconsistent discipline. This suggests that even within an economically disadvantaged sample, markers of SES such as maternal education, occupation, and social status remain an important risk factor for neglect.
Finally, within two-parent households, the maternal report of a paternal history of problematic substance use was associated with increased levels of both care and supervisory maternal neglect, after accounting for the potential effect of maternal alcohol use history. This suggests that residing with a partner with a problematic substance use history may negatively affect mothers’ ability to provide adequate care and supervision. These findings are consistent with previous research that has pointed to the important role of paternal caregivers in risk of maltreatment (e.g., Coohey & Zhang, 2006; Smith et al., 2007). Some research suggests that mothers’ physical and mental health are negatively impacted by a partner’s substance use (Dawson et al., 2007), and this could result in mothers having fewer resources to devote to parenting. Because the current sample assessed lifetime misuse, however, it is unclear whether mothers might be affected differently by residing with a partner with current substance misuse versus a partner who has a prior history of substance misuse. Nonetheless, these findings highlight the value of incorporating data on paternal caregivers in child maltreatment research.
Strengths and Limitations
The multimethod multisource approach to data collection and use of SEM techniques allowed for a more sensitive and comprehensive assessment of parenting constructs. By accounting for the overlap and comorbidity among types of deficient parenting, the current findings speak to unique associations between maternal alcohol misuse and parenting. In short, this study reflects a robust test of the relations among alcohol use, neglectful parenting, and harsh and inconsistent discipline. Given the prospective design of this study, it was also possible to add to the limited research examining how maternal alcohol use influences parenting over time. Last, paternal caregivers have historically been underrepresented in child maltreatment research (Guterman & Lee, 2005), which limits our understanding of how paternal substance misuse might increase risk of subsequent maltreatment. The current study aimed to incorporate an assessment of paternal substance use in order to begin to address this gap in the literature.
Nonetheless, there are also several limitations that warrant attention. First, the assessment of paternal substance use history was based solely on mothers’ reports. While it is possible that mothers reporting a positive substance history for their partner may have differed from other mothers in the sample, post hoc comparisons revealed that there were no significant differences in mothers’ age, t(157) = −1.89, p = .06; SES, t(157) = .83, p = .41; minority status, t(158) = .60, p = .55; or number of children in the home, t(158) = −.26, p = .80. In short, on at least some key variables, mothers in the current sample were comparable whether or not they reported having a partner with a history of problematic substance use. Despite this, the reliance on maternal report for paternal substance use is a notable limitation, and as such, the findings regarding paternal substance use should be interpreted with some caution.
Although fathers were eligible to participate and actively recruited, the ability to fully assess paternal substance use was limited by low paternal caregiver participation; difficulty in recruiting fathers in parenting research is widely recognized as problematic. Only one third of two-parent families had a father agree to participate, which precluded the inclusion of paternal caregivers in the SEM analyses. Furthermore, due to frequent changes in paternal caregiver status, there was not adequate power to assess the influence of paternal substance use during the second year of the study. Importantly, over the course of 1 year, approximately 43% of the enrolled families reported at least some change in household composition (i.e., adult male moving in or out of home). Thus, while even potentially “temporary” substance-using father figures pose risk of child maltreatment, it is possible that mothers’ deficient parenting practices could be further exacerbated by the sustained presence of a substance-using partner, and in turn, this may confer greater risk of poor child outcomes.
Finally, other adverse factors that could also confer risk of deficient parenting, such as maternal psychopathology (e.g., Shay & Knutson, 2008) or marital conflict (Keller et al., 2005), were not included in the current study. Future research would benefit from a broader inclusion of such factors in examinations of the link between parenting and alcohol or substance misuse.
Implications
These findings highlight the importance of accounting for associations between types of child maltreatment when examining the link between parental alcohol or substance use and parenting. Given the complex ways in which parents may continue to be at risk over time, the current study demonstrates the importance of assessing parenting behaviors over time rather than focusing only on acute risk. Moreover, this study supports the potential role of paternal substance use in maternal neglect and points to the importance of assessing all caregivers in the home including caregivers that may be “temporary” or have limited contact with the child (e.g., mothers’ new boyfriends), which could ultimately enhance prevention efforts. Further consideration of interventions focused on couples or families (e.g., Parent Skills with Behavioral Couples Therapy; Lam et al., 2009) should continue to be explored as a potential strategy to mitigate risk of maltreatment.
Footnotes
Acknowledgment
The facilitation of the research by Trisha Barto, Marc Batey, Barry Bennett, Wayne McCracken, Mark Schmidt, and Cheryl Whitney (Iowa Department of Human Services), Paul Spencer (Oneida County Department of Social Services), and the assistance of Ashley Anderson, Robin Barry, Allyson Bone, Beth Boyer, Kristy DePalma, Aubra Hoffman, Esther Hoffman, Kathryn Holman, Kathy Jordan, Robert Latzman, Theresa Mayne, Mary McCarren, Katie Meyer, Amanda Murray, Donna Palmer, Laureen Ann Rapier, Nicole Shay, and Nizete-Ly Valles is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by Grant RO1 MH 61731 funded by the National Institute of Mental Health; and the Administration on Children, Youth, and Families (John F. Knutson, PI) and, in part, by Grant R01-HD046789 funded by the National Institute of Child Health and Human Development.