
Abstract
One well-established outcome of child maltreatment is an increased likelihood of substance use in emerging adulthood. However, research identifying the indirect pathways that explain this relation is lacking, thereby limiting substance use prevention efforts for the child maltreatment population. The present study helped address this gap by accessing data from The Longitudinal Studies on Child Abuse and Neglect (LONGSCAN; n = 1,136), a prospective cohort study of child maltreatment from birth through age eighteen. Internalizing and externalizing problems at age twelve were examined as indirect effects of the relation between child maltreatment prior to age four and substance use at age eighteen. A multiple mediator model tested the total and specific indirect effects of internalizing and externalizing concerns while controlling for demographic risk factors. Results demonstrated that the total indirect effect for internalizing and externalizing behaviors was statistically significant, Standardized Point Estimate = 0.01, 95% CI: 0.00-0.02. Examination of the specific indirect effects revealed that only externalizing behaviors constituted an indirect pathway, Standardized Point Estimate = 0.01, 95% CI: 0.00-0.03. These results suggest that externalizing behaviors at the transition to adolescence are important intervention targets for reducing the risk for substance use in emerging adulthood in the child maltreatment population.
More than 164 million people over the age of twelve in the U.S. engage in some form of substance use, defined as the consumption of nicotine, alcohol, marijuana, or other illicit drugs (Substance Abuse and Mental Health Services Administration, 2019). Substance use most often begins in adolescence with those adolescents transitioning to adulthood having the highest annual rate of substance use (Johnston et al., 2020). Annual rates of substance use continue to increase during the first several years of adulthood (Schulenberg et al., 2018), when prevalence rates for substance abuse, that is, repeated consumption of substances for pleasure or alleviation of distress are the highest of any age group (National Institute on Drug Abuse, 2018). The use of illicit substances and misuse of legal substances represents a serious public health concern with conservative estimates placing the total economic burden at $740 billion dollars annually (National Institute on Drug Abuse, 2020). Thus, there is a need to identify risk groups and pathways leading to increased substance use so that prevention efforts can be strategically organized toward those people and targets of highest public health relevance.
There is a well-established relation between child maltreatment and substance use in emerging adulthood (Gilbert et al., 2009; Halpern et al., 2018; Herrenkohl et al., 2013; Yoon et al., 2020). However, identifying the pathways leading children who have been maltreated to substance use in emerging adulthood is an underdeveloped area of research with significant potential, one that can elucidate important targets for substance use prevention. Child behavior problems, specifically broad categories of internalizing and externalizing behaviors, are candidate pathways by which exposure to child maltreatment may increase the risk for later substance use (Cicchetti & Handley, 2019). Internalizing problems are characterized as overcontrolled behaviors that most often occur privately, such as anxiety, depression, fear, and somatic complaints, whereas externalizing behaviors are those considered undercontrolled and most often occur publicly, such as aggression, non-compliance, delinquency, and hyperactivity (Willner et al., 2016). Conceptually, internalizing and externalizing behaviors have unique functional properties that may explain how child maltreatment increases the risk for later substance use (Cicchetti & Handley, 2019). For example, increased subjective distress resulting from greater levels of internalizing behaviors may motivate individuals to use substances that alleviate this distress (Cooper et al., 2016). Similarly, greater levels of externalizing behaviors may set the stage for substance use as a result of selecting into activities or peer groups where substance use is available or encouraged (Samek et al., 2016). While each type of child behavior problem may confer a unique pathway to substance use, internalizing and externalizing behaviors also co-occur (Caspi et al., 2014) and have the potential to exert a cumulative risk greater than any one type of child behavior problem alone. Thus, testing the indirect effects of each type of child behavior problem, uniquely and cumulatively, could inform etiological models of substance use for the child maltreatment population and identify prevention targets.
Prior studies have examined internalizing and externalizing behaviors as indirect effects of child maltreatment and later substance use, producing mixed results. For example, Lewis et al. (2011) examined internalizing behaviors as an indirect pathway and reported that this specific behavior problem partially mediated the association between child maltreatment prior to age twelve and cigarette use at age sixteen. Hudson and colleagues (2017) also demonstrated that internalizing behaviors were an indirect effect of the relation between child maltreatment and alcohol use but only for adolescent females. There is also evidence for externalizing behaviors serving as an indirect effect of the relation between prior child maltreatment and later substance use. For example, Wardell et al. (2016) demonstrated that externalizing behaviors mediated the relations between child maltreatment and subsequent alcohol and marijuana use. However, conflicting results most often occur when both forms of childhood problems are estimated simultaneously in the same statistical model. Blake et al. (2018) found that only the internalizing pathway was a specific indirect effect of later substance use when both internalizing and externalizing behaviors were included in the same model. In contrast, Oshri et al. (2011) and Handley et al. (2015) reported that externalizing behaviors, and not internalizing behaviors, were an indirect pathway to marijuana use following child maltreatment when both types of childhood problems were tested simultaneously. Jones et al. (2013) also reported that externalizing behaviors, and not internalizing behaviors, at age twelve were an indirect pathway between child sexual abuse prior to age twelve and alcohol use at age fourteen but only for females. These mixed results for whether internalizing and externalizing behaviors are more influential than the other when tested simultaneously are considered in the context of other research failing to find any evidence for internalizing or externalizing behaviors as indirect effects (Yoon et al., 2017). The failure to reliably identify internalizing or externalizing behaviors as indirect effects hampers recommendations for whether to target these behaviors at all, and if so, which one specifically, when attempting to prevent substance use in the child maltreatment population.
There are several reasons that might explain the mixed results on child behavior problems as indirect effects of child maltreatment and subsequent substance use. First, child maltreatment, child internalizing and externalizing problems, and substance use are often measured at different points in child development. For example, child maltreatment and comparison conditions across studies are often created using different ages for the time of exposure to child maltreatment. Differences in the timing of when child maltreatment occurs in a child’s life may itself create variation in risk estimates (Thornberry et al., 2001), as can reoccurrences of child maltreatment after child maltreatment conditions are established (Shenk et al., 2016). Rates of substance use also vary across adolescence (Johnston et al., 2020) and measuring it earlier in adolescence or in a shortened assessment window, such as the past thirty days, may make it more difficult to detect or replicate results. Second, examining only one type of child maltreatment or substance use can introduce study-specific variability and limit generalization, as different types of maltreatment (Trickett et al., 2011) and substances (Substance Abuse and Mental Health Services Administration, 2019) often co-occur. Third, differences in sampling, such as child welfare (Blake et al., 2018) or clinical populations (Handley et al., 2015), and measurement strategies, such as using mono-method (Wardell et al., 2016) or self-report of child maltreatment (Yoon et al., 2017) as opposed to confirmed cases (Oshri et al., 2011), can also produce variation in whether internalizing, externalizing, both, or neither function as indirect effects of child maltreatment and substance use. Finally, gender is not always examined as a moderator of indirect effects despite playing an important role in explaining variability in findings on substance use (Kobulsky et al., 2018) and specifically for studies examining internalizing (Hudson et al., 2017) and externalizing behaviors (Jones et al., 2013).
The current study sought to address these challenges and advance research on the indirect effects of child behavior problems when explaining the relation between child maltreatment and later substance use in four ways. One, child maltreatment from birth to age four, while accounting for all subsequent instances of child maltreatment, was selected as the exposure variable of interest. The birth to age four range is important because it not only reflects a potential sensitive period of child development that can have lasting effects on child behavior problems and substance use (Godinet et al., 2014; Lupien et al., 2009) but also the time in child development when maltreatment most often occurs (U.S. Department of Health and Human Services, 2020). This approach can address mixed findings due to maltreatment occurring at different ages, providing a unique assessment of the timing of early child maltreatment and substance use at emerging adulthood. Two, confirmed designations made by independent raters were chosen to characterize child maltreatment in this study, as this method reflects investigative practices throughout the U.S. (U.S. Department of Health and Human Services, 2020) while avoiding potential retrospective recall bias evident in self-report methods (Baldwin et al., 2019). Three, internalizing and externalizing behaviors at the transition to adolescence, while accounting for these same behaviors earlier in development, were selected as indirect pathways between early child maltreatment and substance use at emerging adulthood. The transition to adolescence is an important period to measure the contributions of child behavior problems, as this is a time when these behaviors emerge or increase in frequency and severity (Godinet et al., 2014) and when substance use has yet to occur (Johnston et al., 2020). Finally, the use of several different substances over the past year was chosen as the method in which to measure substance use at emerging adulthood, as this time frame enhances sensitivity to detecting substance use at the developmental period when substance use is at peak frequency (Schulenberg et al., 2018).
To meet these measurement needs, existing data were accessed from the Longitudinal Studies of Child Abuse and Neglect (LONGSCAN; Runyan et al., 1998), a multi-wave prospective cohort study of child maltreatment in the U.S from birth to age eighteen. LONGSCAN provides an opportunity to use multiple methods of measurement, including confirmed designations of child maltreatment, caregiver reports of both internalizing and externalizing concerns, and self-reports of substance use. Thus, access to LONGSCAN data allows for an explicit test of whether internalizing and externalizing behaviors constitute indirect effects of early child maltreatment and emerging adulthood substance use and whether these indirect effects vary by gender. Access to LONGSCAN data also allows for a robustness test of whether subsequent exposure to child maltreatment after age four confounds or moderates the specified indirect effects. There were two primary hypotheses to this study. First, the total indirect effect, that is, the cumulative effect of both internalizing and externalizing behaviors will be statistically significant. Second, based on prior research, the specific indirect effects, that is, the unique effects for internalizing and externalizing problems, will each be statistically significant. Finally, as previous research has shown that pathways to substance use can vary by gender in the child maltreatment population, an exploratory analysis will test whether gender moderates the indirect pathways for internalizing and externalizing behaviors.
Methods
Sample
LONGSCAN participants were recruited from five geographic sites around the United States: East (EA), Midwest (MW), South (SO), Southwest (SW), and Northwest (NW). Each site differed in sampling methodology, varying from recruitment at pediatric clinics serving low-income, inner city children (EA), families who had been reported to Child Protective Services (CPS) and neighborhood controls (MW), families deemed to be at moderate risk due to a referral to CPS (NW), children identified as at-risk through state public health tracking efforts (SO), and children involved in a county dependency system due to maltreatment and placement in foster or kinship care (SW). Each site received approval from their respective Institutional Review Boards and the LONGSCAN Data Coordinating Center prior to data collection with caregivers and children providing consent and assent, respectively. Of the total available LONGSCAN sample (N = 1,354), two hundred eighteen children were omitted from the current sample because they did not provide data on study variables at both the age twelve and age eighteen LONGSCAN assessments, leaving n = 1,136 participants available for analysis. See Table 1 for demographics at the initial LONGSCAN assessment and Table 2 for frequencies of maltreatment subtypes.
Sample Demographics at LONGSCAN Study Enrollment.
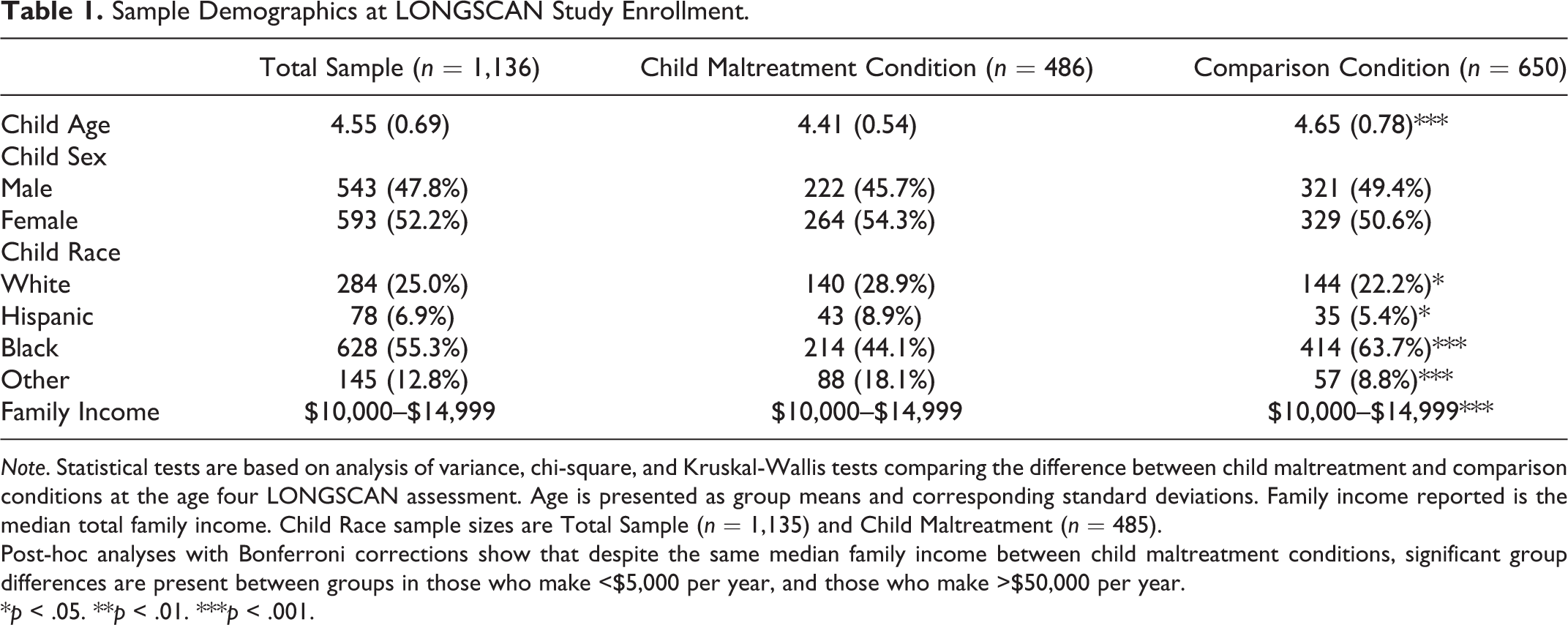
Note. Statistical tests are based on analysis of variance, chi-square, and Kruskal-Wallis tests comparing the difference between child maltreatment and comparison conditions at the age four LONGSCAN assessment. Age is presented as group means and corresponding standard deviations. Family income reported is the median total family income. Child Race sample sizes are Total Sample (n = 1,135) and Child Maltreatment (n = 485).
Post-hoc analyses with Bonferroni corrections show that despite the same median family income between child maltreatment conditions, significant group differences are present between groups in those who make <$5,000 per year, and those who make >$50,000 per year.
*p < .05. **p < .01. ***p < .001.
Descriptive Statistics of Sample (n = 1,136) Child Maltreatment Exposure.

Note. Percentages for subtypes are reported as percentage of those with confirmed cases, not out of total sample. Percentages of subtypes will add to greater to 100% as a result of multiple exposures.
Measures
Confirmed child maltreatment
Confirmed child maltreatment was determined through official case record reviews using the Modified Maltreatment Classification System (MMCS; English et al., 2005). Independent raters using the MMCS reviewed the case record generated by an official investigation into an allegation of child maltreatment and determined whether the information contained in the record met a pre-specified definition of child maltreatment. The MMCS improves detection and classification of child maltreatment over official case records alone (Runyan et al., 2005) and allows for a standardized definition of child maltreatment across data collection sites given that legal definitions vary by State. MMCS coders met a training criterion threshold of 90% inter-rater reliability for reviewing child maltreatment case records. Coders then entered scores on the MMCS based on information contained in the official case record to indicate whether a participant was exposed to child maltreatment from birth through age eighteen. For the present investigation, a dummy-coded variable was created where ‘1’ represented exposure to one or more confirmed cases of child maltreatment across all subtypes assessed from birth to age four, while ‘0’ represented no exposure to confirmed child maltreatment during this same time. Because of the longitudinal nature of the current hypotheses, a second dummy-coded variable was created where ‘1’ indicated exposure to confirmed child maltreatment between ages four and eighteen and ‘0’ indicated no exposure to confirmed child maltreatment during this time. This variable was created to adjust model estimates for any relation between subsequent exposure to child maltreatment and later substance use. Complete data (n = 1,136) are available for confirmed child maltreatment from birth through age eighteen.
Child internalizing and externalizing behaviors
Internalizing and externalizing behaviors were assessed via the Child Behavior Checklist (CBCL/4-18; Achenbach, 1991), a caregiver report measure with strong cross-informant reliability when compared to self and teacher reports (Achenbach et al., 2002; Janssens & Deboutte, 2009) and good predictive validity with adulthood psychiatric disorders (Reef et al., 2010). The CBCL is comprised of 113 items where respondents report the frequency of a specific problem over the last six months using a 3-point Likert scale (0 = Not true, 1 = Somewhat or sometimes true, and 2 = Very true or often true). CBCL raw scores are converted to age-adjusted T-scores. Internalizing and externalizing T-scores at the age four and age twelve LONGSCAN assessments were used in the present study. The reliability of the internalizing problems scale at age four was α = .80 and at age twelve, α = .88. The reliability of externalizing problems scale at age four was α = .89 and at age twelve, α = .92. Of the n = 976 families who participated in the age twelve LONGSCAN assessment, there was available CBCL data for n = 951 participants.
Past year substance use
Substance use was assessed via self-report at the age eighteen LONGSCAN assessment where participants reported on the past year use of tobacco, alcohol, marijuana, and any other illegal drugs (LONGSCAN Investigators, 2000). Respondents answered whether they used each of the substances noted above in the past year (0 = No; 1 = Yes). A summary score was then computed for each participant that indicates the total number of substances used in the past year, such that a total score of 0 indicates no substances used during the past year while a score of 4 represents use of each class of substances assessed. A higher score on this measure indicates the use of more types of substances in the past year. Of the n = 932 participants attending the age eighteen LONGSCAN assessment, n = 904 completed the substance use assessment.
Data Analysis
The primary hypotheses were that internalizing and externalizing problems, both cumulatively and uniquely, would constitute indirect effects of the relation between confirmed child maltreatment prior to age four and greater use of different types of substances at age eighteen. To test these hypotheses, a multiple mediator model (Preacher & Hayes, 2008) using Mplus 7.4 estimated the total indirect effect to obtain a cumulative estimate of both internalizing and externalizing problems as well as the specific indirect effects for each unique child behavior problem. Standardized estimates for these effects are reported. Missing data were addressed using maximum likelihood estimation under the missing at random (MAR) assumption. Several tests were completed to assess if the MAR assumption was plausible for the current data. One, results from Little’s missing completely at random test for internalizing and externalizing behavior problems at age twelve as well as substance use at age eighteen were nonsignificant, χ2(3) = 4.371, p = .224, suggesting these data were missing completely at random. An additional step created indicator variables to represent missingness (missing = 1, not missing = 0) for internalizing and externalizing behaviors at age twelve and substance use at age eighteen. These missingness indicators were then correlated with variables measured at the age four and age twelve LONGSCAN assessments. Variables that were significantly related to missingness were then included in our mediation model, assuming that once these relations were accounted for that any remaining missingness was at random, thereby meeting the MAR assumption (Graham, 2009). Standard errors and corresponding 95% confidence intervals (CI) are based on k = 5,000 bias-corrected (BC) bootstrapped samples. Once model results for the indirect effects were obtained, invariance tests were conducted using the GROUPING command to determine if the results of the multiple mediator model and specific model pathways varied by gender.
Child gender, age, race, annual family income, and foster care status at the age four LONGSCAN assessment were included as covariates in the multiple mediator model. Child gender was coded as ‘0=Male’ and ‘1=Female.’ Child race was dummy coded into three variables (Black, Hispanic, Other) with Whites representing the reference category for each code. Annual family income was coded as 1 = <$5,000; 2 = $5,000–$9,999; 3 = $10,000–$14,999; 4 = $15,000–$19,999; 5 = $20,000–$24,999; 6 = $25,000–$29,999; 7 = $30,000–$34,999; 8 = $35,000–$39,999; 9 = $40,000–$44,999; 10 = $45,000–$49,999; 11 ≥ $50,000. Foster care status was coded a ‘0 = No and 1 = Yes.’ Internalizing and externalizing T-scores at the age four assessment were entered as covariates to adjust the respective estimates for child problems measured at age twelve. Finally, confirmed child maltreatment occurring between ages four and eighteen was entered as a covariate to control for any relation between confirmed maltreatment during this time and substance use at age eighteen. All covariates were retained in the multiple mediator model regardless of whether the respective pathway was statistically significant or not. Because recruitment strategies varied across each LONGSCAN site, site effects were first examined to determine whether data from all sites can be combined and used in the present analysis. Specifically, interactions among each LONGSCAN site and all predictors and covariates were examined with results indicating that there were no statistically significant interactions, all p’s > .08, allowing for the combination of all LONGSCAN data.
Results
Descriptive Statistics
Table 3 presents descriptive information on child behavior problems and specific types of substances used, categorized according to the total sample as well as child maltreatment and comparison groups. Of those who reported on substance use at age eighteen, 37.8% (n = 342) reported using zero substances in the past year, 26.5% (n = 240) reported using one substance in the past year, 18.1% (n = 164) reported using two substances, 13.5% (n = 122) reported using three substances in the past year, and 4% (n = 36) reported using all four substances in the past year. This represents a total, past-year substance use prevalence of 62.2% (n = 562).
Descriptive Statistics for Child Behavior Problems and Substance Use.
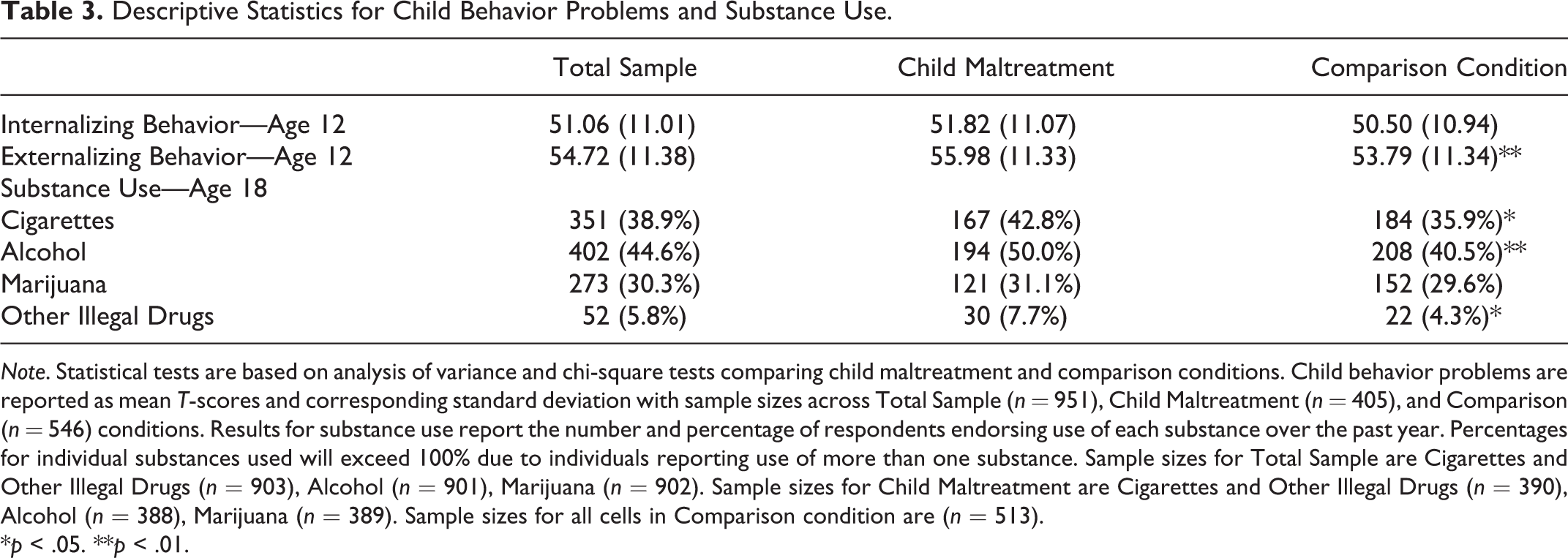
Note. Statistical tests are based on analysis of variance and chi-square tests comparing child maltreatment and comparison conditions. Child behavior problems are reported as mean T-scores and corresponding standard deviation with sample sizes across Total Sample (n = 951), Child Maltreatment (n = 405), and Comparison (n = 546) conditions. Results for substance use report the number and percentage of respondents endorsing use of each substance over the past year. Percentages for individual substances used will exceed 100% due to individuals reporting use of more than one substance. Sample sizes for Total Sample are Cigarettes and Other Illegal Drugs (n = 903), Alcohol (n = 901), Marijuana (n = 902). Sample sizes for Child Maltreatment are Cigarettes and Other Illegal Drugs (n = 390), Alcohol (n = 388), Marijuana (n = 389). Sample sizes for all cells in Comparison condition are (n = 513).
*p < .05. **p < .01.
Multiple Mediator Model
The multiple mediator model (see Figure 1), including covariates, provided an acceptable fit to the observed data: Comparative Fit Index (CFI) = 0.94; Root Mean Square Error of Approximation = 0.06; Standardized Root Mean Square Residual = 0.03; χ2 (15) = 81.90, p < .001. After adjusting for all specified covariates, model results indicated that the total indirect effect was significantly different from zero, Standardized Point Estimate = 0.01 (BC 95% CI: 0.00-0.02), providing evidence that internalizing and externalizing problems, as a cumulative set, is an indirect pathway to the use of different substances in emerging adulthood following early child maltreatment. The total indirect effect was driven by a significant specific indirect effect for externalizing problems when simultaneously estimating the effects of internalizing behavior problems, Standardized Point Estimate = 0.01 (BC 95% CI: 0.00-0.03). This provided evidence for the second hypothesis that externalizing problems would function uniquely as an indirect pathway. Inspection of the individual regression coefficients for this indirect pathway indicated that exposure to confirmed child maltreatment prior to age four significantly predicted greater levels of externalizing problems at age twelve, β = 0.06, SE = 0.03 p = .045, even after controlling for levels of externalizing problems at age four. In turn, greater levels of externalizing problems at age twelve significantly predicted greater use of different substances at age eighteen, β = 0.15, SE = 0.05, p = .003. However, there was no significant indirect effect for internalizing behavior problems when simultaneously estimating the indirect effects of externalizing behavior problems, Standardized Point Estimate = 0.00 (BC 95% CI: -0.01-0.01), failing to provide full support for the second hypothesis.
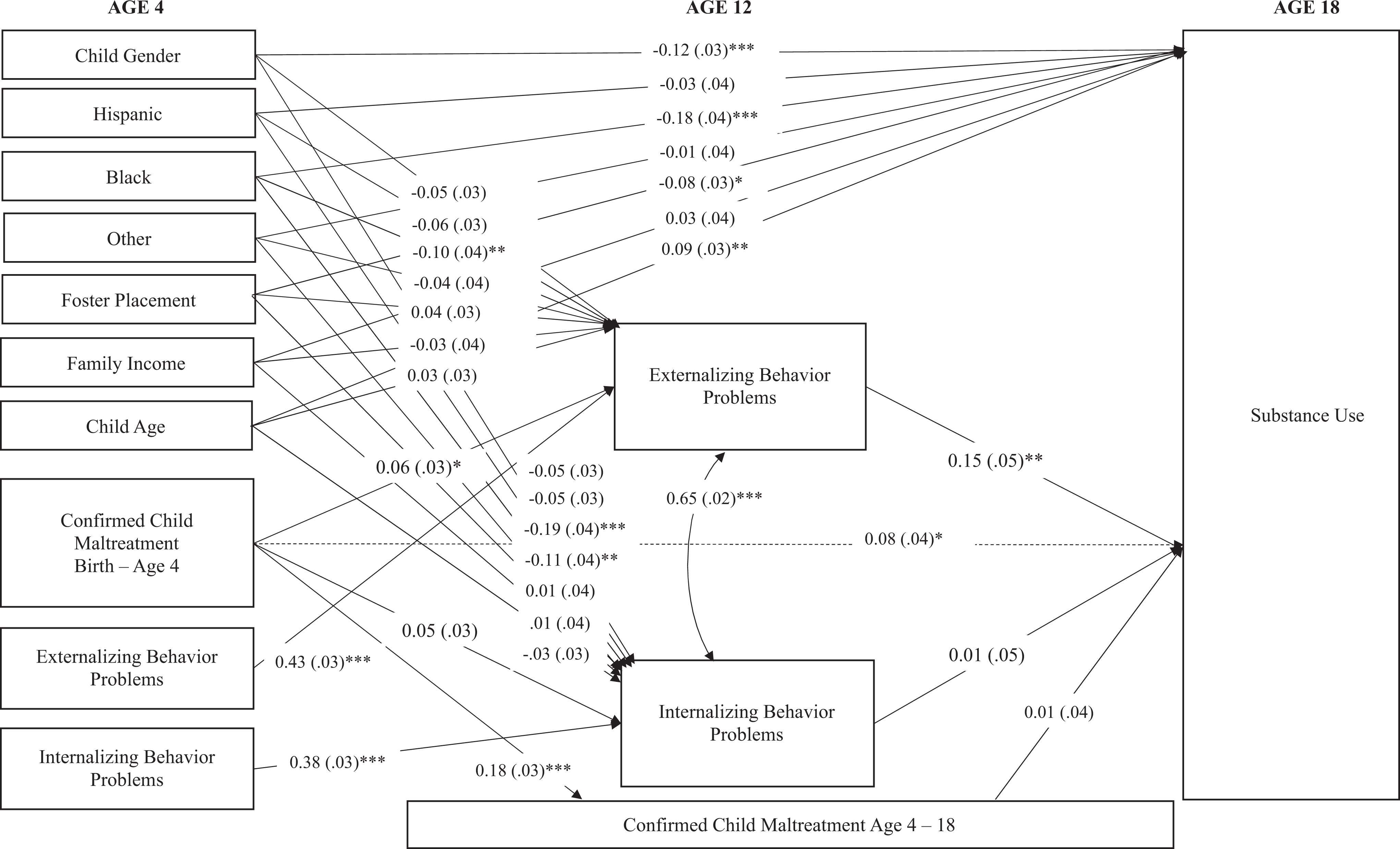
Results of multiple mediator model for internalizing and externalizing behavior problems. Note. Standardized parameter estimates and standard errors are reported. Covariances among all covariates at age four were estimated but are not shown to maintain clarity. The indirect effect of externalizing behavior problems is statistically significant. *p < .05. **p < .01. ***p < .001.
The total effect, which is the sum of the indirect and direct effects, was statistically significant, β = 0.09 (BC 95% CI: 0.02-0.16). The direct effect of child maltreatment on substance use, which is the difference between the total effect and all specified indirect effects, was also significant, β = 0.08, SE = 0.04, p = .024. The difference between the total and direct effects is equal to the total indirect effect (see above), indicating that the difference between these effects is significantly different from zero. A proportion of the total effect accounted for by each indirect effect can be calculated as a measure of effect size (Miočević et al., 2018). The proportion of the total effect accounted for by the externalizing behavior problems is 0.01/0.09, indicating that the externalizing behavior problems accounted for 11.11% of the total effect of child maltreatment on substance use. In contrast, the proportion of the total effect accounted for by internalizing behavior problems is 0.00/0.09, indicating that internalizing behavior problems accounted for 1.11% of the total effect of child maltreatment on substance use.
Whether gender status moderated any of the individual pathways making up the mediation model was then tested using invariance tests according established benchmarks for model fit indicators. First, a baseline model, where all pathways were estimated freely, was conducted, resulting in a model fit of χ2(28) = 94.68, CFI = 0.94. Five separate nested models, one for each of the individual a1, b1, a2, b2, and c′ pathways making up the multiple mediator model, were then conducted that constrained the respective pathway to be equal across gender status. This approach allows for an assessment of degradation in chi-square and CFI model fit across the respective baseline and nested models, as only one pathway was different between the nested and baseline models. The critical χ2 value at p < .05 for a one degree of freedom test is 3.84, which indicates whether constraining the respective pathway to be equal across gender status results in a statistically significant degradation in model fit. A criterion of 0.01 change has been established as the benchmark for evaluating degradation in model fit for the CFI (Cheung & Rensvold, 2002). Statistically significant degradation in model fit indicates that the respective risk pathway is different for males and females and therefore gender status moderates that pathway. Results from these five nested models indicated that there was no significant degradation in model fit with χ2 difference values ranging from 0.02 to 1.18, all below the 3.84 critical value, and CFI difference values ranging from 0 to 0.001, all below the 0.01 criteria. Thus, gender status did not moderate any of the individual pathways making up the mediation model.
An additional series of invariance tests were completed to determine whether confirmed maltreatment between four and twelve moderated the a1 or a2 pathways and whether confirmed maltreatment twelve to eighteen moderated the b1 or b2 pathways. Chi-square difference values ranged from 0.00 to 1.23 for each of these tests, below the 3.84 critical value, and change in CFI values ranged from 0 to 0.001, below the 0.01 criteria. Thus, these robustness tests revealed that there was no evidence that confirmed maltreatment between four and twelve confounded or moderated the pathways from confirmed maltreatment before age four and internalizing and externalizing problems at age twelve, or that confirmed maltreatment between twelve and eighteen confounded or moderated the pathways from internalizing and externalizing problems at age twelve to substance use at age eighteen.
Discussion
Substance use is a well-established outcome of child maltreatment (Gilbert et al., 2009; Halpern et al., 2018). This study tested whether child internalizing and externalizing behaviors at the transition to adolescence explained this relation and served as indirect effects of early child maltreatment and substance use in emerging adulthood. There are several notable strengths of the current study that serve to advance the larger research literature in this area. First, this study tested a model spanning the entire period of child development and measured key events, processes, and outcomes at important ages, providing an explicit test of whether child maltreatment early in life increases the risk for substance use in emerging adulthood through adolescent internalizing and externalizing problems. Second, this study used data from a large, geographically and ethnically diverse prospective cohort study to test specific study hypotheses. Access to this cohort allowed for the use of a multi-method data collection approach that included independent ratings of child maltreatment based on official case records, caregiver reported childhood problems, and self-reported substance use in early adulthood. Third, a multiple mediator model simultaneously estimated the indirect effects of internalizing and externalizing problems while controlling for demographic and study related variables. These strengths provide greater confidence in risk estimates, improved generalization to individuals who have experienced child maltreatment, and enhanced translation to substance use prevention.
Results from this study indicated that the timing of exposure to child maltreatment, specifically from birth to age four, has lasting implications for an increased risk for using different types of substances at the transition to adulthood, an age where substance use is common in the general population (Johnston et al., 2020; Schulenberg et al., 2018) and where rates of substance abuse and dependence are highest (Substance Abuse and Mental Health Services Administration, 2019). The current study adds unique results on this relation that are distinct from other LONGSCAN studies that used a much wider age range of exposure to child maltreatment (birth to age twelve, birth to age eighteen) as a predictor of later substance use (Dubowitz et al., 2019, 2020; Kobulsky et al., 2018; Yoon et al., 2017) or that assessed substance use earlier in adolescence (Duprey et al., 2017; Yoon et al., 2018, 2020). Moreover, this study not only generated risk estimates for substance use after controlling all subsequent instances of child maltreatment from age four to age eighteen but conducted a robustness assessment that showed child maltreatment at distinct age ranges (4–12, 12–18) was not a confound or moderator of the indirect pathways in the specified multiple mediator model. Thus, the timing of child maltreatment early in life, when it is most common (U.S. Department of Health and Human Services, 2020), appears to be a unique risk factor for subsequent substance use. Universal and selective prevention of child maltreatment should therefore remain a top public health priority.
The relation between early child maltreatment and use of different types of substances in emerging adulthood was explained by greater levels of child internalizing and externalizing problems at the transition to adolescence, providing support for the stated cumulative hypothesis. However, only externalizing problems functioned as an indirect pathway that uniquely explained the relation between early child maltreatment and substance use at young adulthood for both males and females. This finding was obtained even after accounting for a host of demographic risk factors, prior levels of externalizing problems, and exposure to child maltreatment after age four. The externalizing pathway to substance use is characterized by greater displays of non-compliance, delinquency, and affiliation with deviant peers that can promote the subsequent engagement of substance use (Samek et al., 2016). Results from this study highlight not only that these behaviors increase the risk for greater substance use in emerging adulthood but also that externalizing behaviors at the transition to adolescence are a key target for substance use prevention. Capitalizing on the wealth of evidence for parent-training programs in reducing externalizing problems among youth experiencing child maltreatment (Cohen et al., 2010), substance use prevention programming and child welfare policies could adopt similar strategies when attempting to reduce the risk for substance use following early maltreatment.
There was no support for internalizing problems exerting a unique indirect effect for those exposed to child maltreatment. However, this result is consistent with prior research testing internalizing and externalizing problems simultaneously when explaining the risk for various forms of substance use following child maltreatment. For instance, Oshri et al. (2011) and Handley et al. (2015) found that externalizing concerns, and not internalizing concerns, were an indirect effect for marijuana use following exposure to child maltreatment generally. Jones et al. (2013) reported similar results in a study of child sexual abuse and later alcohol use, but only for females. The results from the current study add to a growing consensus that externalizing problems are more influential in determining later substance use than internalizing behaviors for those who have experienced maltreatment (Cicchetti & Handley, 2019). However, this consensus is at odds with findings reported by Blake et al. (2018), which found that internalizing behaviors, and not externalizing behaviors, were an indirect pathway to later substance use. This could be due to differences in sampling across these studies, where results from the current study focused exclusively on child maltreatment while Blake et al. (2018) focused on children who were placed in foster care and subsequently adopted. For instance, child maltreatment is not the only cause for placement in the child welfare system (Blake et al., 2018), something that can explain inconsistent results across studies using these different sampling strategies. Moreover, different reasons for entering the child welfare system may engage different pathways to substance use (McLaughlin & Sheridan, 2016). Future research examining the effects of child maltreatment specifically may continue to clarify such mixed results and strengthen the available evidence on the pathways to substance use in this particular population.
The current results also stand in contrast to some prior studies in that the indirect pathways to substance use did not differ across males and females. Although gender does not always moderate the indirect pathways to substance use (Wardell et al., 2016), several prior studies have shown that the pathways to substance use can vary by gender, where women are at greater risk for alcohol use specifically (Hudson et al., 2017; Jones et al., 2013). One reason for the discrepancy with prior research could be that the current study examined greater use of multiple substances, including but not limited to alcohol, and variation by gender may be most readily observed when examining this single substance versus the use of multiple substances.
Limitations
Several limitations of the present study are worth noting. First, substance use was assessed via a self-report questionnaire and it is possible that there was bias in the self-report of substances used, although efforts were made in LONGSCAN to anonymize the reporting of such information to promote accuracy. Second, the measure of substance use in the current study captured information on the total number of different substances used in the past year and generalizations to recent substance use, such as in the past thirty days, or the chronic use of one substance, are not possible. Third, prior child maltreatment research (Wall & Kohl, 2007) weighted the use of certain substances differently, where the use of illicit drugs was weighted more heavily than other substances. The current study weighted all substances equally. Four, it is important to note that the age eighteen LONGSCAN assessment, where substance use at the transition to adulthood was measured, occurred through 2012. It is therefore critical to consider the extent of changing cultural trends in substance use since the conclusion of this assessment, such as changing legalization laws regarding marijuana use, large increases in vaping, as well as the ongoing opioid epidemic. Fifth, individual subtypes of child maltreatment were not examined in this study, as different subtypes often co-occur in cross-section and over a child’s life, which can make it difficult to parse the unique effects of any one subtype. While examining child maltreatment as a general category is not a limitation of this study, we cannot rule out the possibility that the results are driven by the higher prevalence of neglect from birth to age four, a trend that is also observed nationally (Sedlak et al., 2010). Sixth, one area of future research could be an examination of the frequency and severity of child maltreatment as explicit third variable moderators, as this was not done in the current study. Finally, as with any prospective cohort study with multiple repeated assessments spanning early childhood to adulthood, there were varying rates of participation at each study assessment. However, the current study retained as much of the original LONGSCAN cohort as was available (n = 1,136) and addressed attrition and missing data using established statistical approaches designed to address these concerns.
Conclusion
Efforts are needed to understand the pathways to substance use, especially for children who have been maltreated. The present study adds to the existing literature by modeling child maltreatment, child internalizing and externalizing behaviors, and substance use at critical developmental periods using multiple methods and a rigorous multiple mediator modeling approach. Results provide evidence of an externalizing pathway to substance use following early child maltreatment and suggest that reducing externalizing behaviors at the transition to adolescence may serve as a valuable target for substance use prevention in this population.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Acknowledgments
The data used in this publication were made available by the National Data Archive on Child Abuse and Neglect (NDACAN), Cornell University, Ithaca, NY, and have been used with permission. Data from Longitudinal Studies of Child Abuse and Neglect (LONGSCAN) Assessments 0–12 were originally collected by Desmond K. Runyan, Howard Dubowitz, Diana J. English, Jonathan Kotch, Alan Litrownik, Richard Thompson and Terri Lewis & The LONGSCAN Investigator Group. The collector of the original data, the funder, NDACAN, Cornell University and their agents or employees bear no responsibility for the analyses or interpretations presented here.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anneke E. Olson received support from the National Institutes of Child Health and Human Development (NICHD), T32 grant number T32HD101390. This research was also supported by the NICHD under award number P50HD089922. Funding for the project was provided by the Office on Child Abuse and Neglect (OCAN), Children’s Bureau, Administration for Children and Families, Dept. of Health and Human Services (The National Center on Child Abuse and Neglect (NCCAN), under the Office of Human Services funded this consortium of studies during the early years of data collection from 04/01/1991 until NCCAN became part of OCAN in 1998).