
Abstract
Child maltreatment (CM) can have profound intergenerational impacts, with maternal CM experiences increasing the risk of adverse outcomes in the next generation. Using data from the Intergenerational Childhood Adversity and Lifetime Morbidity (I-CALM) study, we examined associations between self-reported CM and statutory child protection data, and adverse neonatal outcomes, including preterm delivery, resuscitation at birth, admission to special care nursery (SCN) or neonatal intensive care units (NICU), and morbidity within 28 days of birth. We also investigated whether risk factors identified at women’s first antenatal care visit mediated these associations. The odds of preterm delivery, SCN or NICU admission units, and neonatal morbidity were significantly higher in births to women with both self-reported CM and statutory notifications. Smoking after 20 weeks’ gestation partially mediated the relationship between statutory notifications and most adverse neonatal outcomes, but all other pathways were non-significant. These findings highlight several avenues for future research.
Introduction
Child maltreatment (CM) – including physical abuse, emotional abuse, sexual abuse, and neglect – is a significant public health and social challenge the world over. While estimates of CM prevalence vary globally, its individual, societal and economic consequences are unambiguous. CM costs global economies billions of dollars each year both directly (e.g., child protection services, out-of-home care placements, and family support services) and indirectly (e.g., housing and homelessness, drug and alcohol problems, poor mental and physical health, policing and crime) (Centre for Excellence in Child and Family Welfare, 2024; Hughes et al., 2021; Pereznieto et al., 2014). Individuals who experience CM are more likely to suffer lifelong impacts including low educational and employment attainment, poorer physical and mental health outcomes, greater likelihood of alcohol and other substance use disorders, and increased risk of involvement with the justice system (Bull, Trott, Najman, Arnautovska, et al., 2024; Currie & Tekin, 2012; Norman et al., 2012; Strathearn et al., 2020).
CM also possess significant intergenerational risks. There is growing evidence to show that maternal experiences of early life adversity, including CM, can increase the risk of adverse pregnancy and birth outcomes with significant short- and long-term consequences for women and their children (Frederickson et al., 2024; Kern et al., 2022; Mamun et al., 2023). Outcomes such as preterm birth, low birthweight, neonatal complications, miscarriage, gestational hypertension, and gestational diabetes can arise through multiple, interacting pathways (Christiaens et al., 2015; Ciciolla et al., 2021; Hardcastle et al., 2022; Keenan-Devlin et al., 2023; Kerkar et al., 2021). Several theories exist to explain how early life adversity influences later risk for poor health (Hertzman, 1999), though it remains unclear whether CM itself leads to adverse outcomes, or maladaptive behaviours and lifestyles that promote adverse outcomes.
At the biological level, early adversity can lead to lasting dysregulation of the hypothalamo-pituitary-adrenal (HPA) axis and autonomic nervous system, resulting in abnormal cortisol secretion, altered immune functioning, and heightened inflammatory activity (Champagne et al., 2024; Frodl & O'Keane, 2013). During pregnancy, when the HPA axis and placenta work in tandem to regulate fetal maturation and the timing of delivery, such dysregulation has been linked with preterm birth, fetal growth restriction, preeclampsia, and postpartum depression (Champagne et al., 2024). Epigenetic mechanisms provide another explanatory pathway. Early life adversity among women is associated with DNA methylation changes, accelerated biological ageing, and altered placental gene expression, all of which may influence fetal development (McKenna et al., 2023; Sun et al., 2022).
Yet behavioural and psychosocial pathways also play a critical role in the intergenerational transmission of adversity. Women who have experienced CM are more likely to experience depression and anxiety during pregnancy (Choi & Sikkema, 2016; Racine et al., 2021), report higher levels of stress (Brunton, 2024; Souch et al., 2022), and are more likely to be exposed to intimate partner violence (Li et al., 2019). They are also more likely to engage in substance use, which further increases risks of adverse pregnancy and neonatal outcomes (Brunton, 2024). Early life adversity is also strongly associated with socioeconomic disadvantage, reduced educational attainment and subsequent employment opportunities, and barriers to healthcare access, which can compound intergenerational risk (Hertzman, 1999; Poulton et al., 2002; Shonkoff & Garner, 2012).
Given these pathways, the antenatal period represents a critical window for early intervention and one of the few universal touchpoints where women and families can be supported to interrupt intergenerational patterns of adversity. For women with experiences of CM, modifiable antenatal factors may play an important role in shaping pregnancy and neonatal outcomes. Women with histories of CM are more likely to engage in tobacco smoking during pregnancy, often as a stress-coping behaviour, which is strongly linked with preterm birth and neonatal complications (Bull, Kisely, et al., 2025; Chamberlain et al., 2017; Da Rosa et al., 2025). CM is also associated with nutritional and metabolic difficulties (Kisely, Siskind, et al., 2023; Molendijk et al., 2017) which may increase the likelihood of entering pregnancy underweight; a recognised risk factor for fetal growth restriction and preterm delivery (Kern et al., 2022; Mamun et al., 2023). Psychosocial sequelae such as reduced trust in healthcare providers, avoidance of institutional settings, and socioeconomic instability can also contribute to delayed initiation of antenatal care, limiting opportunities for early identification and management of pregnancy risk (Frederickson et al., 2024; Isobel, 2023). Finally, CM is strongly associated with socioeconomic disadvantage, which both reflects and reinforces cumulative adversity over the life course and is independently associated with poorer pregnancy and neonatal outcomes (Bywaters et al., 2022; Poulton et al., 2002). Together, these factors represent plausible and potentially modifiable antenatal mediators through which early life adversity may influence neonatal health. Importantly, interventions focused on smoking cessation, nutrition support, and early antenatal engagement have all been shown to improve neonatal outcomes (de Masi et al., 2017; Ota et al., 2015; Sun et al., 2023).
Previous studies have largely relied on self-reported CM data to understand the impact on pregnancy and birth outcomes, and a limited set of outcomes have been examined. Assessing both self-reported CM and statutory notifications is essential, as these measures often identify overlapping but not identical groups (Bull et al., 2025). Self-reports capture the lived experience of CM, whereas statutory data tend to represent only a subgroup of all children exposed to CM, reflecting more severe or chronic cases that come to the attention of services (Bull, Trott, & Kisely, 2025). Considering both enables us to explore whether different forms or severities of CM exposure confer similar risks, or whether distinct mechanisms underlie their associations with neonatal outcomes. Furthermore, few studies have examined potential antenatal mediators that may alter risk, despite the opportunity that the antenatal period presents for intervention. To address these gaps, the present exploratory study sought to use both self-reported CM and statutory child protection data to identify associations with multiple adverse neonatal outcomes, including preterm delivery, resuscitation at birth, admission to special care nursery (SCN) or neonatal intensive care units (NICU), and neonatal morbidity within the first 28 days of life. We further examined whether potentially modifiable risk factors identified at women’s first antenatal care visit mediated these associations, thereby providing new insights into the potential mechanisms underlying intergenerational adversity transmission.
Methods
Overview
This study was approved by the Metro South Human Research Ethics Committee (HREC) (HREC/2024/QMS/107240) and The University of Queensland HREC (2024/HE002338). It was prospectively registered as an observational study with the Australian New Zealand Clinical Trials Registry (ANZCTR12624001423505). Reporting was in accordance with Strengthening The Reporting of Observational Studies in Epidemiology (STROBE) guidelines (von Elm et al., 2007), and the REporting of studies Conducted using Observational Routinely-collect health Data (RECORD) statement (Benchimol et al., 2015).
Study Design and Participants
This study used data from the Intergenerational Childhood Adversity and Lifetime Morbidity (I-CALM) study (Bull et al., 2025). I-CALM is an extension of two previous studies: the Mater-University of Queensland Study of Pregnancy (MUSP) (Najman et al., 2005, 2015), and MUSP Childhood Adversity and Lifetime Morbidity (MUSP-CALM) (Kisely, Leske, et al., 2023). MUSP collected data on 6,753 women giving birth at the Mater Hospital in Brisbane, Australia between 1981-1983 and followed-up their 7,223 offspring from birth to 40 years of age. In 2000, statutory child protection records from the Queensland Department of Families, Seniors, Disability Services and Child Safety were confidentially linked to offspring records, indicating whether a child had or had not experienced CM in the form of statutory notifications and substantiations (Strathearn et al., 2001). A notification occurs when an allegation of abuse, neglect or harm of a child has been made to an authorised department (Australian Institute of Health and Welfare, 2022). A substantiation occurs when, after investigation, there was reasonable cause to believe the child had been, was being, or was likely to be abused, neglected or harmed (Australian Institute of Health and Welfare, 2022). At the 30-year follow-up of the MUSP offspring, participants were asked to complete the Childhood Trauma Questionnaire-Short Form (CTQ-SF), thereby providing self-reported CM experience data (Trott et al., 2025).
In 2023, investigators confidentially linked Queensland-wide administrative health data (including emergency department [ED] presentations, public and private hospital admissions, and community mental health contacts data) to the records of MUSP offspring, allowing an examination of associations between CM (based on statutory child protection notifications, substantiations and self-reported experiences) with lifetime mental and physical health outcomes as well as health service use from ages 25–40. This was the MUSP-CALM study (Kisely, Leske, et al., 2023).
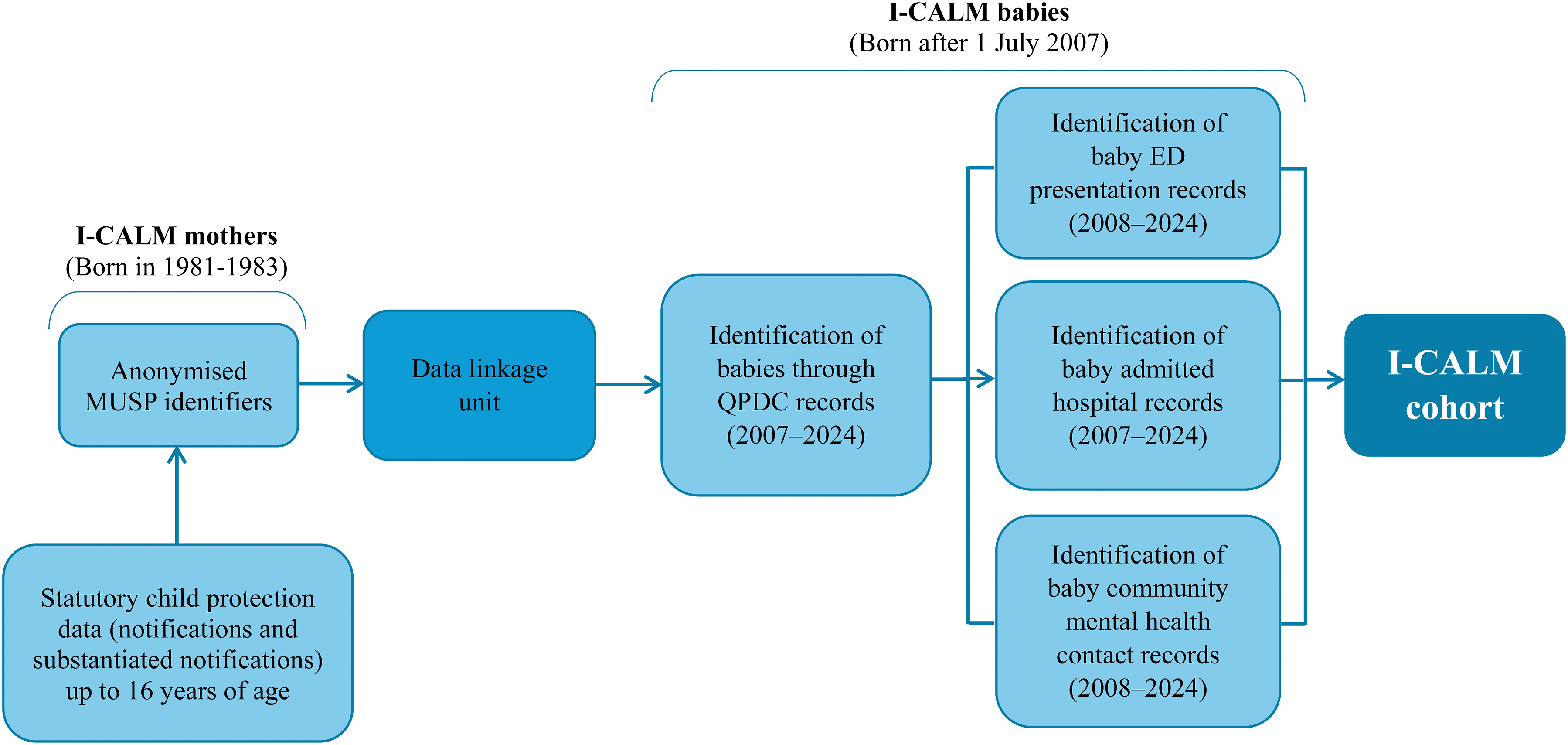
I-CALM is the next iteration of this body of research (Bull et al., 2025). This study confidentially links Queensland Perinatal Data Collection (QPDC) data from 1 July 2007 to 30 June 2024, to the women in the MUSP-CALM sample, subsequently identifying their children (babies in the current study). The QPDC comprises all public and private hospital births across the state, as well as births occurring outside of hospitals with private midwifery or medical practitioners (State of Queensland (Queensland Health), 2024). Queensland-wide administrative health data for these children (including ED presentations, public and private hospital admissions, and community mental health contacts data) were also linked. Figure 1 illustrates the evolution of the cohorts from MUSP to MUSP-CALM to I-CALM. Figure 2 illustrates the I-CALM data linkage. MUSP, MUSP-CALM, and I-CALM cohort composition at each phase of data collection. Reproduced from Bull et al. (2025) I-CALM data linkage. Reproduced from Bull et al. (2025) 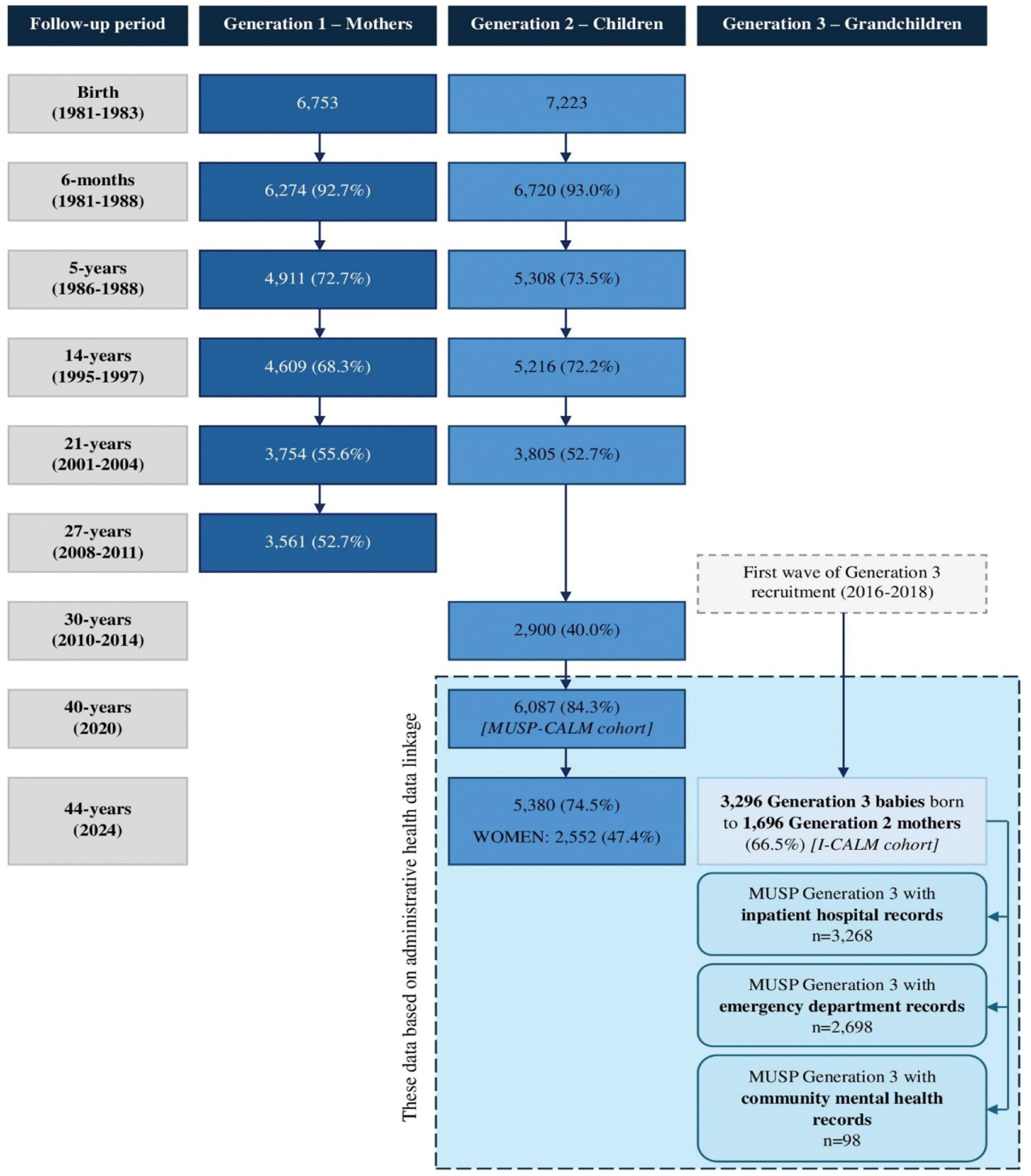
Variables of Interest
For the purposes of this exploratory study, we sought to investigate associations between maternal experiences of CM and adverse neonatal outcomes for their offspring, as well as potentially modifiable risk factors in the antenatal period that may mediate these relationships.
Maternal experiences of CM were based on self-reported CM and statutory child protection data (specifically notifications). Self-reported CM was derived from CTQ-SF responses captured in the MUSP 30-year follow-up study (Najman et al., 2015). The CTQ-SF captures experiences of physical abuse, emotional abuse, emotional neglect, physical neglect and sexual abuse up to 16 years of age on a 5-point Likert scale of ‘never true’ to ‘very often true’ (Bernstein et al., 2003). Responses are then coded into ‘none/minimal’, ‘low’, ‘moderate’, and ‘severe’ experiences of CM (Bernstein et al., 1997). For the purposes of this study, we categorised ‘moderate’ and ‘severe’ as evidence of any self-reported CM. Statutory child protection notifications were dichotomised according to whether any type of notification had been made or not.
Neonatal outcomes were derived from QPDC records. These included: preterm delivery (defined as delivery occurring before 37 weeks’ gestation); resuscitation at birth (defined as active measures taken immediately after birth to establish independent respiration and heartbeat, or to treat depressed respiratory effort and to correct metabolic disturbances); baby admitted to SCN or NICU; and any neonatal morbidity (ICD-10-AM coded conditions arising up to 28 days) (State of Queensland (Queensland Health), 2024).
Mediators were also derived from QPDC and represented potentially modifiable antenatal risk factors. These included: smoking after 20 weeks’ gestation; late antenatal care initiation (after 10-weeks’ gestation); underweight BMI (<18.5 kg/m2); and socioeconomic disadvantage (lowest quintile of the Socio-Economic Indexes for Areas (Australian Bureau of Statistics, 2021)). These mediators were selected as they represent potentially modifiable risk factors (either at the individual-, service- or system/policy-level) where intervention in the antenatal period may disrupt the intergenerational transmission of adversity. Additionally, these variables were the only candidate mediators with adequate data completeness and cell sizes to support reliable causal mediation analysis.
In line with previous studies examining the relationships between maternal experiences of CM and adverse neonatal outcomes (Frederickson et al., 2024), we used the following covariates in our analysis: maternal age (<25 years old vs ≥ 25 years old); marital status (not partnered vs partnered); where women lived (regional/remote vs metropolitan) based on the Accessibility/Remoteness Index of Australia (ARIA+) (Australian Bureau of Statistics, 2023); and previous pregnancies (0 vs ≥ 1).
Statistical Analysis
Patterns of missingness in the dataset were first examined. Few variables had missing data, though missingness ranged from 0.03% (APGAR score at 7 minutes) to 65.2% (total number of antenatal visits). We conducted Little’s Test for data missing completely at random (MCAR) which was rejected (p < 0.05). After a visual examination, we determined the data was missing at random (MAR). Multiple imputation using the R Multivariate Imputation by Chained Equations (MICE) package was subsequently undertaken (Van Buuren & Groothuis-Oudshoorn, 2011). As MICE does not completely impute for variables where there is too much missing data in the predictive set of variables, a small but negligible amount of missingness remained (e.g., 2.4% missing data for BMI at first antenatal care visit).
After assessing normality, data were described using frequencies, proportions, means and standard deviations. Bivariate and multivariate logistic regressions were conducted to determine the unadjusted and adjusted odds, and associated 95% confidence intervals (CI), of adverse neonatal outcomes relative to maternal experiences of CM (both self-report and statutory child protection notifications).
Causal mediation analysis was performed using the mediation package in R (Tingley et al., 2014). A Directed Acyclic Graph (DAG) was created to represent the potential causal pathways examined in our analysis (Figure 3). The primary assumption for the causal mediation analyses was temporal precedence between the exposure, mediator and outcome variables (i.e., the exposure occurred before the mediator, which occurred before the outcome). We estimated the Average Causal Effect (ACE)/Total Effect (TE), Natural Direct Effect (NDE), Natural Indirect Effect (NIE), and proportion mediated for all pathways (Byeon & Lee, 2023). Directed Acyclic Graph (DAG) illustrating tested pathways for causal mediation analysis
To account for maternal clustering (i.e., most women gave birth to more than one baby), we also attempted mixed-effects modelling (Silveira et al., 2023). However, given the relatively small number of outcomes in our sample, the inclusion of random effects for maternal clustering resulted in large variance estimates (e.g., random effect variance >100) and some models failed to converge. Therefore, we used standard logistic regression models to produce stable estimates. All analyses were undertaken on a per birth basis and conducted using RStudio version 2024.02.9 (Posit Software, PBC, 2009-2024).
Results
Maternal Experiences of CM, Including Subtypes (on a per Birth Basis, Total Births n = 3,296)
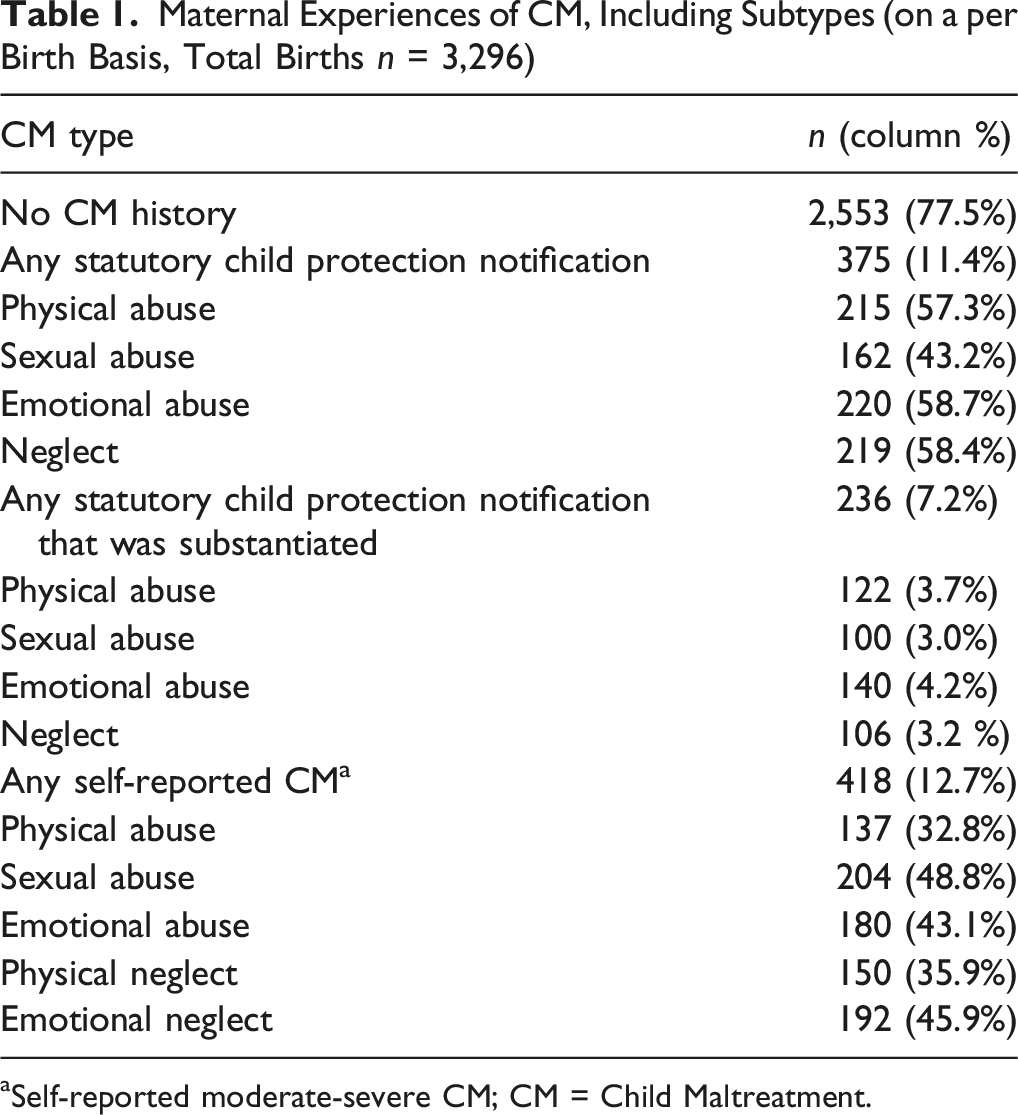
aSelf-reported moderate-severe CM; CM = Child Maltreatment.
Sociodemographic Characteristics of Birthing Women (on a per Birth Basis)
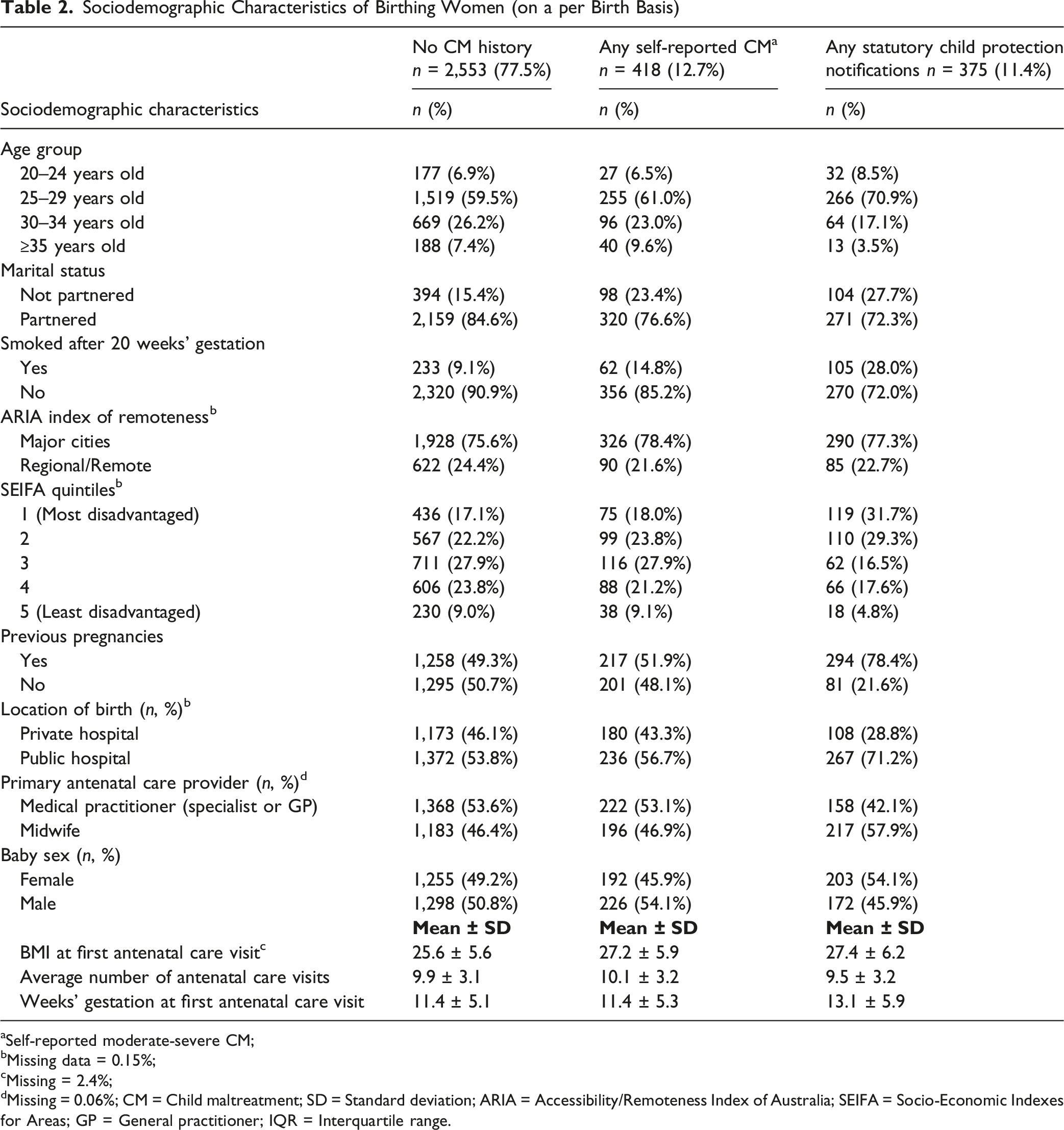
aSelf-reported moderate-severe CM;
bMissing data = 0.15%;
cMissing = 2.4%;
dMissing = 0.06%; CM = Child maltreatment; SD = Standard deviation; ARIA = Accessibility/Remoteness Index of Australia; SEIFA = Socio-Economic Indexes for Areas; GP = General practitioner; IQR = Interquartile range.
Unadjusted and Adjusted Odds of Adverse Neonatal Outcomes Relative to Maternal Experiences of CM (on a per Birth Basis)
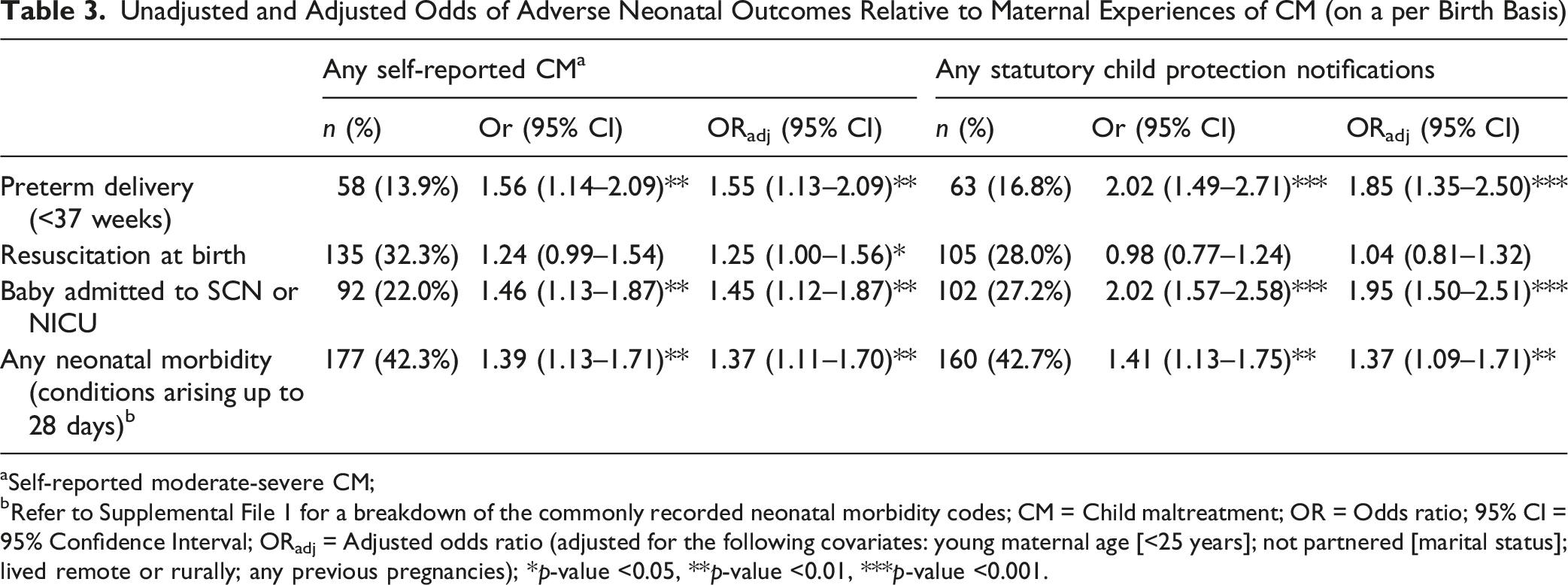
aSelf-reported moderate-severe CM;
bRefer to Supplemental File 1 for a breakdown of the commonly recorded neonatal morbidity codes; CM = Child maltreatment; OR = Odds ratio; 95% CI = 95% Confidence Interval; ORadj = Adjusted odds ratio (adjusted for the following covariates: young maternal age [<25 years]; not partnered [marital status]; lived remote or rurally; any previous pregnancies); *p-value <0.05, **p-value <0.01, ***p-value <0.001.
Mediation Analysis of Antenatal Risk Factors Linking Maternal
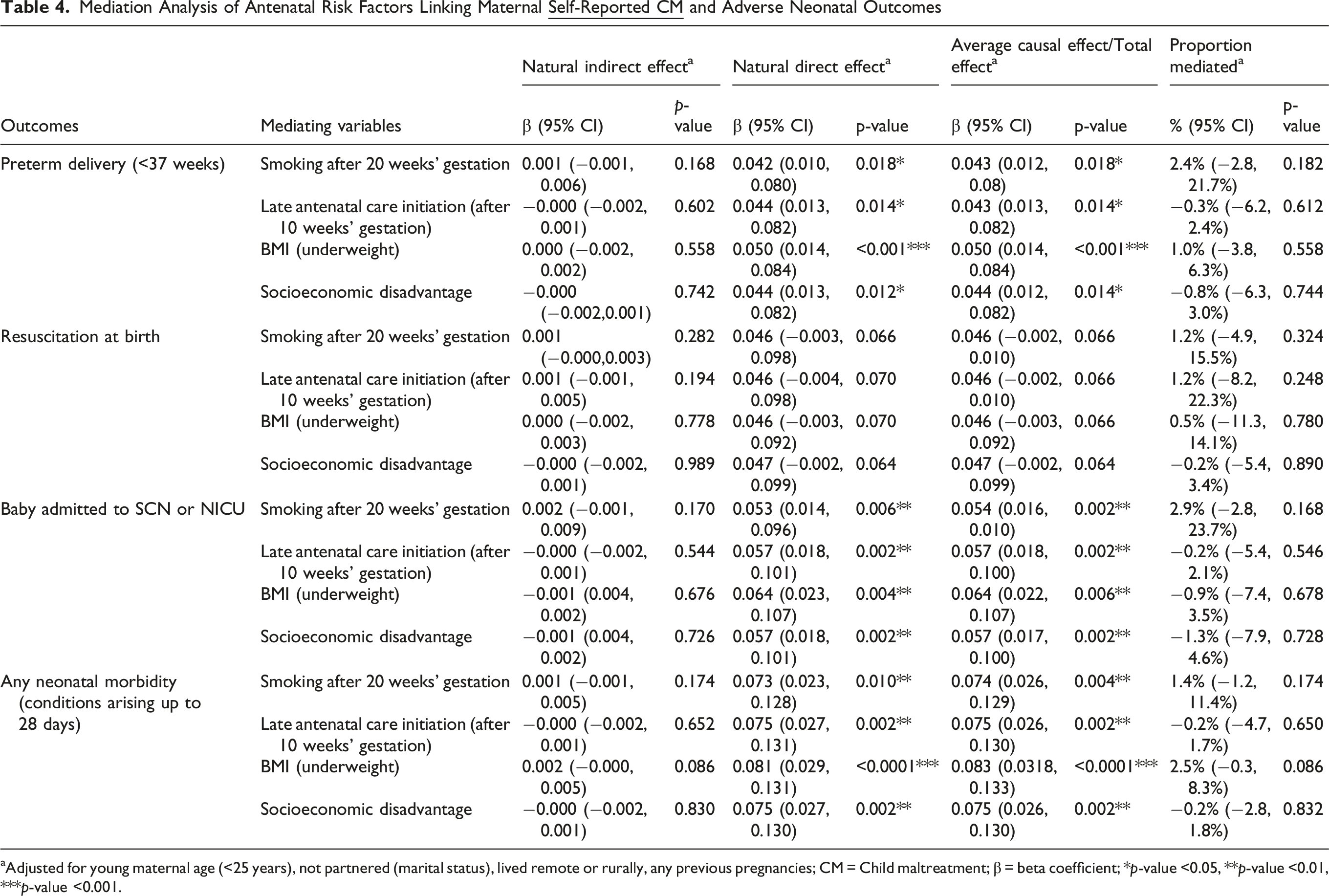
aAdjusted for young maternal age (<25 years), not partnered (marital status), lived remote or rurally, any previous pregnancies; CM = Child maltreatment; β = beta coefficient; *p-value <0.05, **p-value <0.01, ***p-value <0.001.
Causal Mediation of Antenatal Risk Factors in the Association Between Maternal
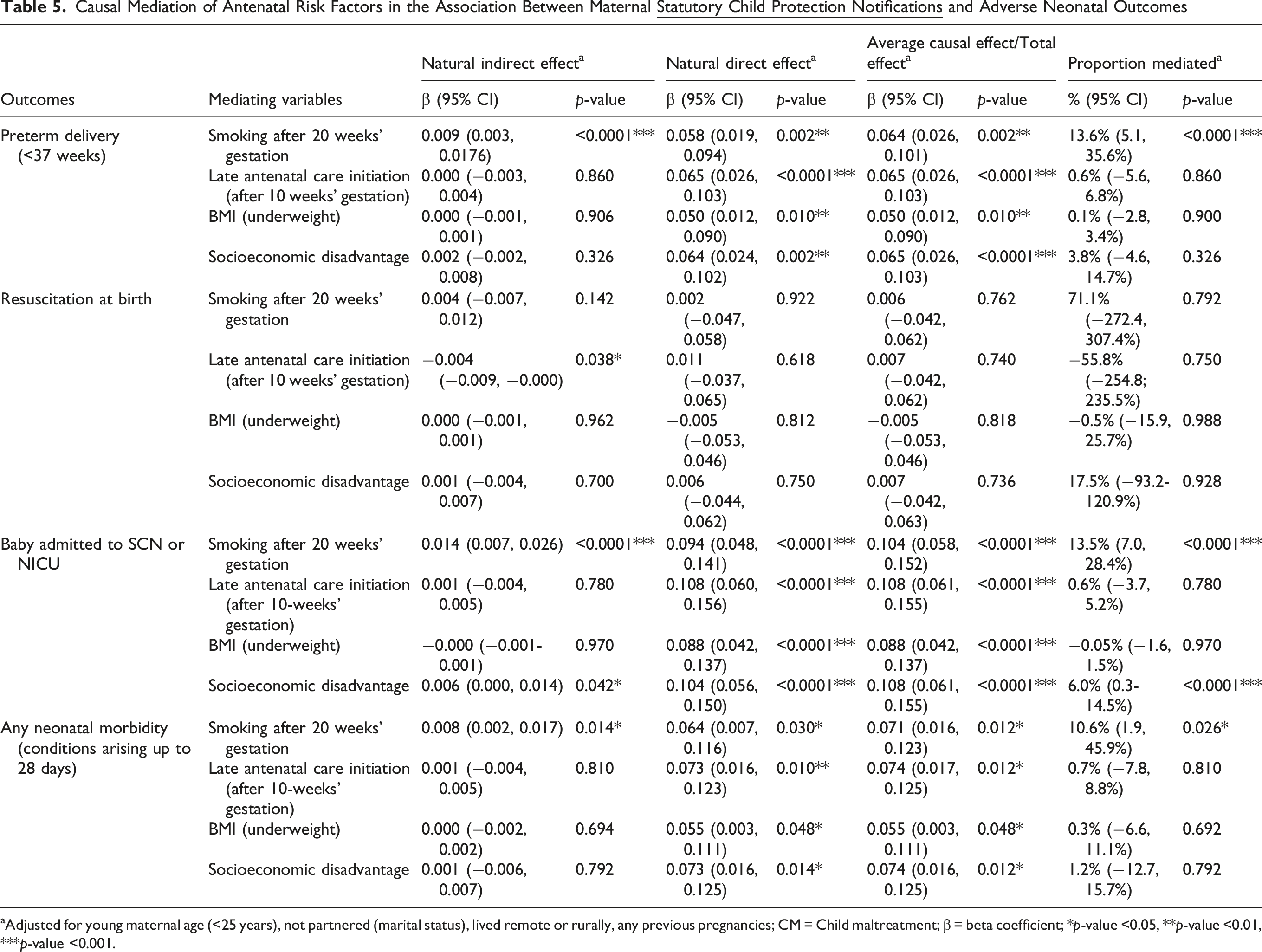
aAdjusted for young maternal age (<25 years), not partnered (marital status), lived remote or rurally, any previous pregnancies; CM = Child maltreatment; β = beta coefficient; *p-value <0.05, **p-value <0.01, ***p-value <0.001.
Discussion
This study sought to investigate associations between maternal experiences of CM (both self-reported and statutory) and adverse neonatal outcomes, as well as potentially modifiable antenatal risk factors that may mediate these outcomes. Both self-reported CM and statutory child protection notifications were significantly associated with increased odds of preterm birth, admissions to SCN or NICU, and the development of neonatal morbidity up to 28 days in their offspring. Women who self-reported CM experiences also had higher odds of giving birth to a baby that required resuscitation. While smoking after 20 weeks’ gestation partially (10.6–13.6%) mediated the relationship between maternal statutory child protection notifications and preterm birth, admissions to SCN or NICU, and neonatal morbidity, no other potentially modifiable risk factors mediated these outcomes (other than socioeconomic disadvantage and admissions to SCN or NICU). Indeed, no causal mediation pathways existed in the context of self-reported CM experiences. To the best of our knowledge, this is the first study to use both self-reported CM and statutory child protection data to investigate intergenerational consequences. The pattern of findings is also compatible with biological theories of intergenerational transmission, which posit that early adversity exerts lasting effects on stress-responsive and inflammatory pathways that can shape perinatal and neonatal outcomes (Champagne et al., 2024; Frodl & O'Keane, 2013; McKenna et al., 2023; Sun et al., 2022).
We identified that smoking after 20 weeks’ gestation was a significant partial mediator in the relationship between statutory child protection notifications and three of the four adverse neonatal outcomes, but not in the context of self-reported CM. There are several possible explanations for this. First, statutory child protection notifications generally capture more severe, chronic and externally validated forms of CM compared to experiences that are self-reported. In their meta-analysis, Baldwin et al. (2019) showed that the level of agreement between prospective (i.e., statutory child protection notifications) and retrospective (i.e., self-reported) measures of CM was poor, indicating that statutory child protection notifications capture only the most severe cases of CM. Consequently, these may have a greater impact on cumulative adversity over the life course that more strongly influences neonatal outcomes. Indeed, families involved with child protection are much more likely to experience socioeconomic disadvantage and psychosocial challenges (e.g., social isolation and mental illness) which compounds the level of cumulative adversity (Bull, Trott, Najman, Reid, & Kisely, 2024; Bywaters et al., 2022).
Second, smoking often serves as a maladaptive coping mechanism for stress and trauma (Australian Institute of Health and Welfare, 2024; Jackson et al., 2019). Despite known harms, some women continue smoking during pregnancy, or even increase their consumption, due to stress, guilt, and limited access to appropriate support (Bull, Kisely, et al., 2025; Chamberlain et al., 2017). However, it is unlikely that smoking alone mediates this relationship. Rather, it is more likely that it is one of a multifaceted set of interrelated coping behaviours and psychosocial vulnerabilities that often co-occur in individuals with histories of CM. Indeed, using the MUSP cohort (of which the mothers in this study are part of), we have previously identified strong associations between both self-reported and statutory CM, and poor mental health and other forms of substance use in adulthood (Bull, Trott, Najman, Arnautovska, et al., 2024; Kisely, Arnautovska, et al., 2024; Kisely, Bull, et al., 2024; Trott et al., 2024, 2025). Many of these variables were unmeasured in the current study, limiting the extent to which we can fully capture the complexity of the pathways linking maternal experiences of CM to adverse neonatal outcomes, and reinforcing the challenges associated with investigating potential pathways of intergenerational trauma transmission. Nonetheless, our findings highlight the need to strengthen smoking cessation initiatives in the perinatal period, particularly for women with a history of statutory child protection notifications. Trauma-informed, woman-centred approaches that integrate therapeutic supports such as cognitive behavioural therapy or other psychosocial interventions may improve cessation outcomes for women whose smoking is closely tied to experiences of CM (Da Rosa et al., 2025; Greaves et al., 2019). Such approaches could have positive flow-on benefits for both maternal and neonatal health.
The broadly similar associations observed across both self-reported CM and statutory notifications suggest convergence in the ways that different forms of documented adversity relate to neonatal risk. At the same time, the somewhat stronger associations linked with statutory notifications are consistent with literature indicating that child protection notifications tend to capture more severe, chronic or externally validated maltreatment, which may carry a higher cumulative burden across the life course. There is also evidence illustrating systemic harm associated with statutory involvement (Gypen et al., 2017; Walsh et al., 2018), which further compounds the relationships and mediating pathways between maternal experiences in child protection systems and neonatal outcomes. Considering both CM indicators therefore helps illuminate the shared and distinct pathways through which different forms and severities of adversity may influence perinatal and neonatal outcomes.
Our findings also highlight the importance of considering where across the life course interventions may be most effective. While the limited mediation observed in the current study suggests that modifiable risk factors in the antenatal period alone may not fully account for intergenerational transmission of adversity, these results should not be interpreted as evidence that the antenatal period is “too late” to intervene. Instead, they indicate the need for antenatal interventions to be complemented by: (i) population-level CM prevention efforts (Higgins et al., 2022); (ii) early life interventions for girls and young women that minimise the enduring consequences of adversity associated with CM and statutory involvement; and (iii) early life interventions for their children that minimise the possibility of intergenerational transmission of adversity. This is particularly important given the unmeasured behavioural, psychosocial and social determinants that likely shape these pathways. Combining population-level prevention, early intervention and targeted antenatal and postnatal supports is therefore a critical avenue for future research.
In common with the general population, increased access to contraceptive and reproductive healthcare is also critical. Globally, around half of all pregnancies are unplanned (The United Nations Population Fund, 2022), and in Australia, the proportion is 40% (Organon Pty Limited & HTANALYSTS, 2022). Woman-centred, equitable contraceptive care, grounded in trauma-informed principles, autonomy and respect, can help ensure that reproductive health services move beyond simply providing contraception to enabling informed, supported, and self-directed reproductive choices (Holt et al., 2020). Such approaches are particularly important for women who have experienced CM, for whom trust, safety, and respectful engagement are essential foundations for breaking intergenerational cycles of adversity (Hillcoat et al., 2023).
Limitations
The results of this exploratory study should be interpreted in light of underlying limitations. First, our sample size was relatively small, which did not allow for mixed-effects modelling, nor analyses of different subtypes of CM captured through self-report and statutory child protection notifications. Moreover, multiple imputation was used and a few variables had high levels of missingness (e.g., number of antenatal care visits). Thus, both the small sample size and need for multiple imputation may impact the precision of some results which should be interpreted with caution.
Second, due to the nature of the data linkage underpinning the I-CALM cohort, we were unable to include paternal data. This is noteworthy because partners can influence the behaviours of pregnant women, as well as their health and wellbeing, which has downstream effects on the fetus (Antoniou et al., 2021; Cheng et al., 2016). This is an area of research that warrants greater attention.
Third, the study’s statutory child protection notification data dates back to the 1980–90’s where reporting processes and criteria may have been different to current practice. It is also likely that these data underestimate the true prevalence of CM in this cohort. Moreover, while statutory child protection notification data were prospectively collected between 1983–1999 and linked to the records of the women included in our I-CALM sample in 2000 (Strathearn et al., 2001), the self-reported data was collected during the 30-year follow-up study (Najman et al., 2015). These data may therefore be subject to recall bias, and represent a proportionally smaller group of women due to loss-to-follow-up of the cohort after 30 years.
Fourth, the limited mediation observed for the selected antenatal factors underscores the complexity of investigating intergenerational pathways of adversity transmission. Even smoking after 20 weeks gestations, despite its significance, only partially mediated the relationship between maternal statutory child protection notifications and preterm birth, admissions to SCN or NICU, and neonatal morbidity. Unmeasured yet complex and intertwined behavioural, socioeconomic, and psychosocial variables likely play a more substantial role in shaping risk than individual antenatal factors alone. Moreover, existing literature suggests that maternal mental illness, substance use, and intimate relationships in the antenatal period play a significant role in the intergenerational transmission of adversity (Frederickson et al., 2024; Madigan et al., 2017; Meinck et al., 2025), and remain a critical area where antenatal support can be provided. However, due to the nature of the administrative health data used in this study, it was not possible to include maternal mental illness or other relevant variables in mediation analyses due to high levels of data missingness and small cell counts. Future research should explore these interlinked mechanisms to better target interventions that can mitigate cumulative adversity.
Conclusion
This exploratory study is the first to draw on both maternal self-reported CM and statutory child protection data to examine associations with adverse neonatal outcomes. Babies born to women with a history of both self-reported and statutory CM had higher odds of preterm birth, SCN/NICU admission, and neonatal morbidity. These findings are consistent with theoretical frameworks of biological embedding and intergenerational transmission, which suggest that early adversity may shape physiological, behavioural and social pathways relevant to perinatal health. Although only smoking after 20 weeks’ gestation emerged as a partial mediator for women with statutory notifications, the limited mediation observed likely reflects the many behavioural, psychosocial and social determinants not captured in our dataset. Together, these findings underscore the importance of strengthening antenatal supports, particularly trauma-informed smoking cessation, while also recognising the need to complement antenatal strategies with population-level prevention efforts and early life interventions for both women and their children. An integrated approach will be essential for reducing intergenerational risk and should be prioritised in future research.
Supplemental Material
Supplemental Material - The Intergenerational Impacts of Maternal Child Maltreatment on Adverse Neonatal Outcomes: Evidence From the I-CALM Study
Supplemental Material for The Intergenerational Impacts of Maternal Child Maltreatment on Adverse Neonatal Outcomes: Evidence From the I-CALM Study by Claudia Bull, Mike Trott, Lakshmi Neelakantan, Natasha Reid, Rebecca Moran, Jake Najman, Anne Edwards, Steve Kisely
Footnotes
Acknowledgements
The authors acknowledge the Statistical Analysis and Linkage Unit of the SSB, Queensland Health for linking the datasets used in this project. No AI tools were used in collecting and/or analysing data, producing images or graphical elements, or in writing the paper.
Ethical Consideration
This study was approved by the Metro South Human Research Ethics Committee (HREC) (HREC/2024/QMS/107240) and The University of Queensland HREC (2024/HE002338).
Consent to Participate
The requirement for informed consent to participate was waived by the abovementioned HRECs.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through the Metro South Research Support Scheme (RSS_2025_34). CB, LN and RM were supported by the National Health and Medical Research Council (NHMRC) Special Initiative in Mental Health (GNT2002047).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to privacy, ethical, and legal considerations, the administrative health data cannot be shared without direct approval from relevant data custodians and the Office of Research and Innovation of Queensland Health. Contact details for Queensland Health custodians can be found at: https://www.health.qld.gov.au/__data/assets/pdf_file/0034/843199/data_custodian_list.pdf. MUSP data are available from a third party on reasonable request. Contact details can be found at: ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.