
Abstract
This mixed-methods study explored the recovery process and outcomes for 37 women formerly in an abusive intimate partner relationship. Standardized measures of current psychosocial functioning indicated participants were largely asymptomatic for posttraumatic stress disorder and had relatively strong resilience. Qualitative analysis revealed how social and spiritual support was instrumental to participants’ recovery, growth, and resilience. Implications for helping professionals include gaining a more comprehensive understanding of recovery from domestic violence. This type of knowledge may contribute to interventions that build on women’s strengths and resourcefulness.
Practically every aspect of a domestic abuser survivor’s life is altered in the aftermath of domestic violence. Leaving an abusive relationship involves transitioning from being controlled to being in control while coping with the costs of a domestic life filled with fear, terror, and devastation. This change takes tremendous strength as one’s energy shifts from survival mode to starting a new life (Senter & Caldwell, 2002). Because domestic violence often leads to severe physical, emotional, and sexual assault and lasts for several years, the following consequences may linger on well after the violence has ended: posttraumatic stress disorder (PTSD), depression (Fergusson, Horwood, & Ridder, 2005; Mechanic, Weaver, & Resick, 2008), substance abuse (Waldrop & Resick, 1993), and other negative mental health and physical health outcomes (Coker et al., 2002; Straight, Harper, & Arias, 2003).
In regard to women’s adaptation after leaving an abusive relationship, we know far more about posttraumatic symptoms than we do about resiliency (Humphreys, 2003). Traumatic responses vary for each individual, yet a substantial percentage of domestic violence survivors (31% to 84%) exhibit PTSD symptoms (see review by Jones, Hughes, & Unterstaller, 2001). “People subjected to prolonged, repeated trauma develop an insidious progressive form of posttraumatic stress disorder that invades and erodes the personality” (Herman, 1997, p. 78). Herman’s ‘dose-response’ curve implies that the more one is exposed to traumatic effects, the more severe the symptoms will be and, consequently, the more difficulty one has with recovery. Factors associated with the intensity of PTSD for battered women include one’s age at the onset of the abusive relationship (i.e., adolescence) along with severity, extent, and types of abuse (Dutton, 2009). In addition, individuals exposed to multiple victimization experiences (e.g., child abuse and domestic violence) have increased odds of developing symptoms of PTSD (Jones et al., 2001).
Research on domestic violence has thoroughly addressed its negative consequences; however, this line of inquiry obscures how women transform their struggles with such adversity and, consequently, a more complete picture of recovery is missed (Cobb, Tedeschi, Calhoun, & Cann, 2006). In other words, a list of symptoms tells us little about the tremendous strengths and resources battered women draw on to recover from domestic violence. The pain individuals experience from domestic violence should not be minimized. Yet, it does not have to be the centerpiece of one’s identity. Standing alongside the entire range of debilitating effects of trauma, most survivors display a stunning capacity for survival and perseverance. Growth and pain, therefore, are not necessarily mutually exclusive, but instead are inextricably linked in recovery from trauma (Saakvitne, Tenne, & Affleck, 1998).
Trauma Recovery and Resilience in Domestic Violence Survivors
Women are able to recover from domestic violence, but information is lacking on how these women do so and whether or not they continue to be successful over the long run (Goodman, Dutton, Weinfurt, & Cook, 2003). Landenburger (1998) identified recovery as gaining a new balance and meaning in one’s life after the violence has ended; however, what helps individuals to achieve this state is not fully illuminated. Other authors relate adaptation to managing posttraumatic symptoms and other life demands (e.g., housing, food, clothing, and medical needs ) without indicating what helps individuals to do this effectively (Benight, Harding-Taylor, Midboe, & Durhan, 2004; Woods & Isenberg, 2001). In other words, we do not know how battered women fully achieve psychological and physical well-being as they encounter the demands of creating a new life. Research on recovery outcomes is encouraging and important, but fails to fully take into account the process and outcome of resilience for women in the aftermath of domestic violence.
Resilience studies reveal that some individuals can develop healthy and stable personalities despite enduring highly stressful environments (Linley & Joseph, 2004), including those impacted by domestic violence. Humphreys (2003) studied resilience and its relationship to psychological distress in 50 battered women residing in domestic violence shelters. Resilience was considered “a positive personality characteristic that enhances individual adaptation” (p. 142). In this study, psychological distress was measured through the Symptom Checklist-90-Revised (SCL-90; Derogatis, 1994), which includes nine primary symptom dimensions (e.g., somatization, depression, anxiety). For measuring growth, the Resilience Scale (RS; Wagnild & Young, 1993) assessed two factors: personal competence and acceptance of self. Participants reported frequent and distressful symptoms on each of the nine dimensions of the SCL-90. Yet, their RS mean score indicated relatively strong resilience and was significantly (inversely) correlated with SCL-90. Humphreys’s findings indicate that battered women can exhibit resilience despite enduring intense stressors (e.g., leaving an abusive relationship, living in a shelter, enduring psychological symptoms).
Interestingly, Humphreys identified resilience as a personality characteristic, yet other research on resiliency recognizes a complex interaction among individual attributes (e.g., intelligence, insight), family milieu (e.g., safe and secure connections), and social interactions (e.g., positive peer relations) in promoting well-being (Fraser, 1997; Masten, 2001). With the exception of Humphreys’s study, the RS has not been used with trauma populations. Therefore, a multidimensional measure (i.e., captures both personal qualities and social conditions) of resilience that is applicable to trauma populations is perhaps more in line with capturing the resilience of domestic violence survivors.
Recovery from domestic violence is possible, but more information is needed regarding how recovery is achieved and sustained over the long run (Goodman et al., 2003). The authors of this study consequently set out to learn more about women’s current psychosocial functioning and what experiences were selected and given meaning in regard to their recovery from domestic violence. Understanding how individuals interpret the personal and environmental strengths that led to their recovery is essential because it assists survivors and helping professionals gain a comprehensive view of the many dimensions of healing from domestic violence. In addition, focusing on battered women’s recovery provides a good fit with feminist empowerment practice and the strengths perspective in social work practice as they both recognize and appreciate one’s potential for growth in the face of adversity (Busch & Valentine, 2000; Saleebey, 2006).
Present Study
This exploratory study used a mixed-methods approach to further identify women’s perceptions of their recovery process and adaptation in the aftermath of domestic violence. Standardized measures of psychosocial functioning were used to identify levels of PTSD and resilience for women formerly in an abusive intimate partner relationship.
Method
Data Collection
The primary sources were women (N = 37) formerly in a battering relationship defined, for the purposes of this study, as the repeated use of physical, sexual, or verbal force by a male against his intimate female partner. Upon approval of the University’s Institutional Review Board, letters about the study, along with requests to post recruitment flyers, were mailed to County Health Departments and electronically sent through the member Listserv of a Midwestern State’s Coalition Against Domestic and Sexual Violence. Recruitment flyers directed potential participants to contact the first researcher (via a toll-free telephone number or email), who then discussed the purpose of the study, explained the consent form, and explored each person’s interest in the project. Purposive sampling criteria included formerly battered women who were 21 years or older and had not been in an abusive relationship in the past year. Of the 61 women who expressed interest in the study, 52 met the purposive sampling criteria and were mailed the survey instruments with a self-addressed return envelope. In addition, respondents were asked to participate in an in-depth interview. Thirty-seven of the 52 qualified respondents completed and returned the study questionnaire, along with the consent form, and volunteered to be interviewed. Interviews took place approximately two weeks after the respondents returned the questionnaires and were held at their homes (n = 20), churches (n = 4), parks (n = 2), a domestic violence shelter or agency (n = 2), county health departments (n = 2), or at the first researcher’s office (n = 7). Each in-depth interview lasted approximately ninety minutes and was audio-taped for later transcription. The in-person interviews consisted of open-ended questions eliciting participants’ descriptions of their recovery experiences. Each participant later received a copy of her interview transcript for her review and input. A 30-min follow-up telephone interview with the first researcher occurred to gain participants’ insights regarding the final analysis. At the conclusion of the study, each participant was provided a US$20 gift certificate to a national department store.
Measures
Demographics
Participant demographic factors included age, ethnicity, sexual orientation, education level, employment status, current relationship status, and number of children.
Childhood exposure to violence
Participants were asked whether or not they had directly experienced childhood abuse or witnessed the abuse of their mother by an intimate partner.
Intimate partner victimization
Participants were asked how old they were when the relationship started, the duration of the relationship, the duration of the violence, and the length of time since the relationship ended.
The short (14-item) version of the Psychological Maltreatment of Women Inventory (PMWI) was used to measure psychological abuse (Tolman, 1989). This inventory asks whether participants have experienced different forms of psychological abuse, such as “My partner called me names.” Individuals used a 5-point Likert-type scale, ranging from 1 (never) to 5 (very frequently) to indicate the frequency of abusive behaviors. The total frequency score was calculated by summing the ratings for each question. The range of possible scores is 14 (i.e., no psychological abuse) to 70 (i.e., very frequent abuse) with higher scores indicating greater exposure to psychological abuse. The PMWI is shown to successfully discriminate between battered and nonbattered women (Tolman, 1989). Previous researchers have validated the reliability and validity of the measure (Arias & Pape, 1999). Cronbach’s α with the present sample was 0.77. In addition to capturing the frequency of psychological abuse, we recoded each of the 14 items on the PMWI-F to create a dichotomous variable for the occurrence of each individual item (scores of 1 were recoded as 0 = never happened and scores of 2 to 5 were recoded as 1 = happened). This recoded variable resulted in a measure of the number of types of psychological abuse reported by women, with a possible range of 0 to 14.
To measure physical and sexual violence, items from the Violence Against Women Survey (Tjaden & Thoennes, 2000) were modified to include 14 items of physical violence and 2 items of sexual violence. Participants used the same response set as the PMWI-Short Form. The types of physical violence included, “My partner kicked me” and “My partner beat me up.” The two sexual violence items included, “My partner forced me to have sex” and “I had sex with my partner because I was afraid of what he would do if I didn’t.” For physical violence, the possible range of frequency scores was 14 (i.e., no physical abuse) to 70 (i.e., very frequent abuse), and for sexual violence the possible range of frequency scores was 2 (i.e., no sexual abuse) to 10 (i.e., very frequent sexual abuse). Cronbach’s α for the physical and sexual violence scales in the present study were 0.93 and 0.79, respectively. We also recoded items in the physical (range: 0 to 14) and sexual (range: 0 to 2) abuse scales to capture the occurrence of these types of abuse. Combining measures of psychological, physical, and sexual abuse produced a total of 30 types of violence.
Posttraumatic stress disorder (PTSD)
PTSD was measured by the PTSD Checklist Version for Civilians (PCL-C). The PCL-C is a 17-item, self-report rating scale used to assess symptom clusters (i.e., intrusion, avoidance, and arousal) experienced within the past 30 days (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). Responses range from 1 (not at all) to 5 (extremely). Symptomatic responses range between 3 and 5 (total scores ranging from 51 to 85) and nonsymptomatic responses include a “1” or “2” (total scores ranging from 17 to 34). The PCL-C corresponds to diagnostic criteria B to D as specified in the Diagnostic and statistical manual of mental disorders (4th ed., Text Revision) (DSM-IV-TR; American Psychiatric Association, 2000) and has demonstrated strong internal consistency in female samples of sexual assault and domestic violence survivors (Street, Gibson, & Holohan, 2005) with Cronbach’s αs of 0.96 (Kocot & Goodman, 2003) and 0.97 (Avdibegovic & Sinanovic, 2006). Cronbach’s α coefficients (0.94, 0.89, 0.78, and 0.89 for the PCL-C total, intrusion, avoidance, and arousal clusters, respectively) were indicative of high internal consistency in the current sample.
Resilience
The Connor-Davidson Resilience Scale (CD-RISC; Conner & Davidson, 2003) is a 25-item scale designed to address psycho-social-spiritual aspects of resilience displayed in the last month. A factor analysis of the CD-RISC indicates a multistructural nature of resilience. Factor 1 corresponds to personal competence, high standards, and tenacity (eight items, e.g., “Even when things look hopeless I don’t give up.”). Factor 2 relates to trust in one’s instincts, tolerance of negative affect, and the strengthening effects of stress (seven items, e.g., “Under pressure, I stay focused and think clearly.”). Factor 3 reflects a positive acceptance of change and having secure relationships (five items, e.g., “I have at least one close and secure relationship which helps me when I am stressed.”). Factor 4 corresponds to personal control (three items, e.g., “I feel in control of my life.”), whereas factor 5 relates to spiritual influences (two items, e.g., “Good or bad, I think most things happen for a reason.”). Response options are based on a 4-point Likert-type scale (0 = not true at all, 1 = rarely true, 2 = sometimes true, 3 = often true, and 4 = true nearly all the time). Participant responses for the 25 items are summed to create a total resilience score that ranges from 0 to 100 with higher scores representing greater levels of resilience. For instance, scores of “3” or “4” for each of the 25 items would yield a range of 75 to 100 and demonstrate a relatively high level of resilience. The CD-RISC has been tested in the general population, as well as clinical samples, and has demonstrated sound psychometric properties (Conner & Davidson, 2003). The mean score for the general population is 80.4 (± 12.8); for primary care outpatients, 71.4 (± 18.4); for psychiatric outpatients, 68 (± 15.3); for generalized anxiety disorder patients, 62.4 (± 10.7); and for PTSD patients, 47.8 (± 19.5). Thus, this measure has been tested with populations similar in levels of psychological distress as domestic violence survivors. Cronbach’s α for the study sample was 0.92.
Interview guide
An interview guide was prepared by drawing from the domestic violence and resilience literature; however, once the interview began participants narrated their own recovery stories as they felt appropriate. The semistructured interviews began with asking participants to share their perspectives regarding the impact of domestic violence on their lives and included questions such as, “How did you feel about yourself after the relationship ended?” and “How do you feel about yourself now?” Participants were also asked, “Please describe what has helped you in healing from domestic violence, with any lessons about recovery learned along the way.” Participants were encouraged to disclose as much of the background and context surrounding their life experiences as possible. As their stories unfolded, participants were also asked, “Please discuss any personal qualities and social conditions that impacted your recovery.” Prompts to this question included informal and formal support systems along with skills, ideas, turning points and a sense of self-regard, control, and purpose in life.
Results
Demographic Statistics
Table 1 presents descriptive information on study participants (N= 37) who ranged in age from 22 to 64 years old (M = 42.62) and resided in a rural Midwestern state. The majority of participants were Caucasian (n = 28), and 36 of the participants identified themselves as heterosexual. Twenty-two participants were employed either full-time or part-time, and 33 participants had children. Nineteen participants were divorced at the time of the study, whereas 13 were married. Participants were diverse in their highest level of education with 14 participants reporting a GED/high school diploma and 13 reporting they had earned undergraduate or graduate degrees.
Demographic Information for Women in Study (N = 37).

Participants reported abuse by either their husbands (n = 33) or boyfriends (n = 4). The participant’s age when the relationship started ranged from 15 to 49 years old (M = 22.16). Fifteen (40.54%) of the women reported that their abuse began during adolescence (i.e., 19 years old or younger). Characteristics of the battering experience revealed that 29 (78.38%) women had experienced violence in the relationship for 5 or more years (M = 11.05). The range of years from the time the violence had ended was 1 to 28 years (M = 8.0), with 17 (45.95%) women reporting the violence had ended during the past 1 to 5 years. Participants experienced an average of 24 (M = 23.84, sample range 14 to 30) of the 30 different types of psychological, physical, and sexual abuse. Thirty-two of the 37 women in the study reported combined experiences of psychological, physical, and sexual abuse, whereas the remaining five women reported experiencing two types of abuse—either psychological and physical or psychological and sexual. The most commonly reported type of abuse was psychological, with all 37 respondents indicating they experienced this type of abuse. During childhood, 20 participants reported experiencing child abuse and 14 reported witnessing their mothers being battered.
Recovery Outcomes: PTSD and Resilience
Information on recovery outcomes was ascertained by examining women’s levels of psychosocial functioning on measures of PTSD and resilience. At the time of the study, participants were largely asymptomatic for PTSD. PLC-C scores in the current sample ranged from 17 to 75 (M = 39.89; SD = 15.45). Item means ranged from 1.92 to 2.78 (M = 11.86; SD = 5.03) for the intrusion cluster, from 1.92 to 2.32 (M = 15.24; SD = 5.96) for the avoidance cluster, and from 2.32 to 2.86 (M = 12.78; SD = 5.92) for the arousal cluster. Participants primarily scored in the nonclinical levels of PTSD with mean item scores ranging from 1.92 to 2.89, indicating symptoms were experienced “a little bit.” Symptoms participants experienced most often were trouble falling or staying asleep (M = 2.89), feeling very upset at reminders of a stressful experience (M = 2.78), and being “super alert” or “on guard” (M = 2.73). Figure 1 graphically presents the total PLC-C scores for each individual study participant.
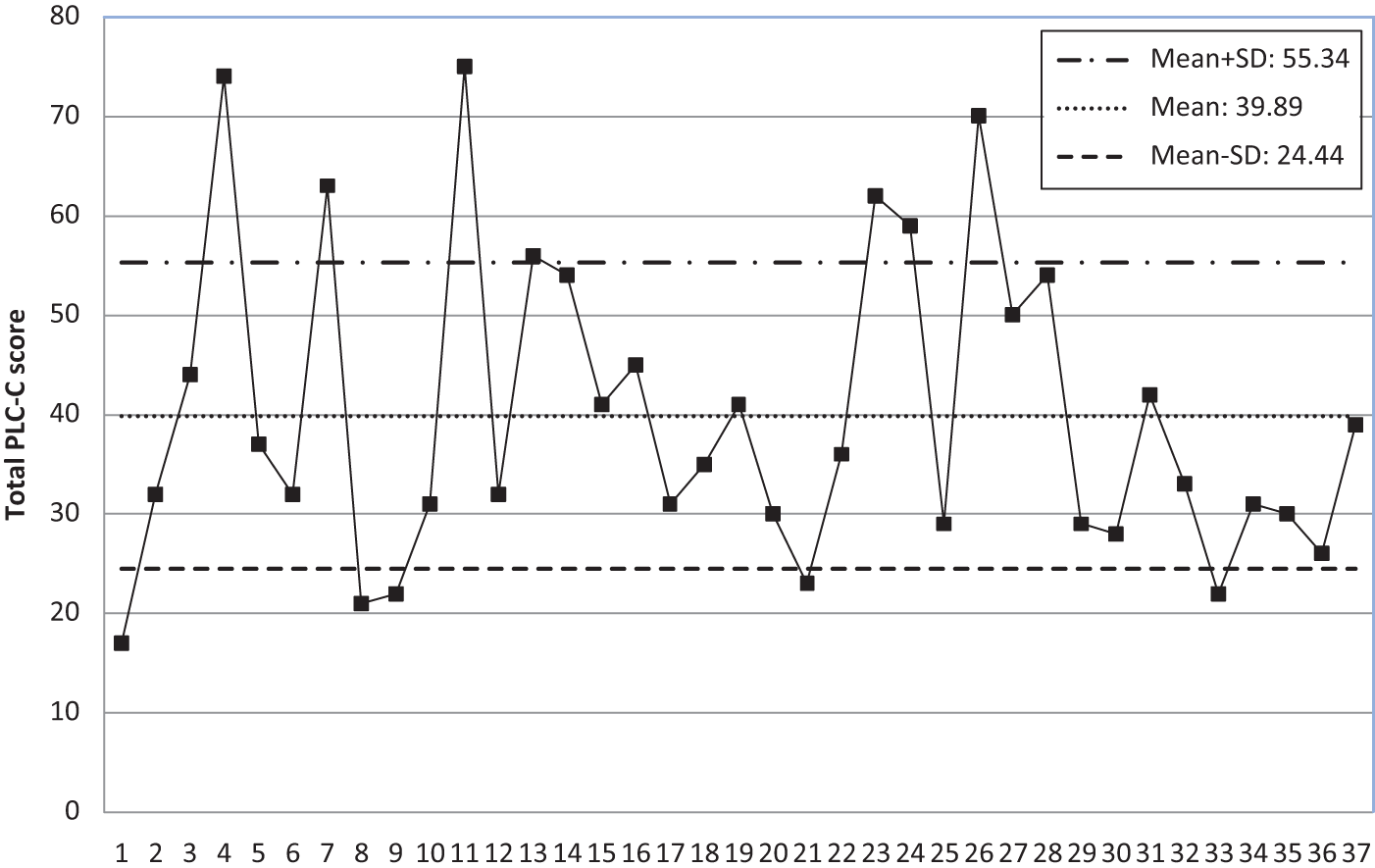
Total score on PTSD (possible range: 17 to 85).
To examine the relationships among study variables, we ran Pearson correlations and independent samples t-tests. After conducting bivariate analyses between PTSD and aspects of victimization, we found a few significant relationships. Higher education levels were negatively correlated with the total PTSD score (r = −0.37, p < .05). There were significant differences in PTSD levels between women with and without a history of childhood maltreatment (M = 46.20 and 32.47, respectively; t = −3.10, p = .005) and between women who reported the battering began while they were teenagers (≤19) compared to women who reported the abuse began after age 20 (M = 46.27 and 35.55, respectively; t = −2.0; p < .10). Women who reported more frequent physical abuse had more PTSD symptoms (r = 0.43, p < .01). Also, women who reported more frequent sexual abuse had significantly more PTSD symptoms (r = 0.45, p < .01).
Nine of the 37 women reported total PTSD scores above 51, thus indicating symptomatic levels of PTSD based on the PLC-C criteria. Follow-up analyses and interviews revealed these nine women had significantly lower levels of education (average highest level = high school diploma compared to Associate’s degree), lower total resilience scores (M = 63.11 and 78.79) and experienced greater physical and sexual battering compared to the 28 women who were asymptomatic for PTSD. Table 2 presents bivariate results for symptomatic and asymptomatic women in the study.
PTSD symptom clusters.

According to participants’ scores on the CD-RISC, participants demonstrated high levels of overall resilience (M = 74.97, range = 0 to 100). Mean scores on the five scale factors were 24.32 on personal competence (range = 0 to 32), 19.22 on trust in one’s instincts (range = 0 to 28), 15.76 on positive acceptance of change and secure relationships (range = 0 to 20), 8.92 on control (range = 0 to 12), and 6.76 on spirituality (range = 0 to 8). For women in this study, higher resilience scores were significantly correlated with lower PTSD (r = −0.55, p < .001). Four of the five resilience factors were significantly correlated with women’s overall PTSD scores. Scores on personal competence (r = −0.42, p < .01), instincts (r = −0.42, p < .01), acceptance of change (r = −0.59, p < .001), and control (r = −0.61, p < .001) were all negatively correlated with the total PTSD score. These results indicate higher resilience scores on these four factors were significantly associated with lower total levels of PTSD.
Respondents showed high mean scores on four individual items. The highest scoring single item was “I have at least one close and secure relationship which helps me when I am stressed” (M = 3.49), and another item with an elevated mean for the total sample—“I take pride in my achievements”—had a similar mean score (3.35). The second highest scoring item (one of the two items in the spirituality factor) on the CD-RISC was their belief in God or fate as reported, “When there are no clear solutions to my problems, sometimes fate or God can help” (M = 3.43). The fourth highest rated item (the second item of the spirituality factor) on the CD-RISC included, “Good or bad, I believe that most things happen for a reason” (M = 3.32). Items on the CD-RISC with the lowest scores, and thus participants rated as less true about themselves, were “Under pressure, I stay focused and think clearly” (M = 2.54), “I can make unpopular or difficult decisions that affect other people, if it is necessary” (M = 2.57), and “I am able to handle unpleasant or painful feelings like sadness, fear, and anger” (M = 2.57).
Qualitative Inquiry
Qualitative inquiry addressed the contextual specificity of the solutions these women found to recover and grow in the aftermath of domestic violence. This process included repeatedly sorting, coding, and making comparisons that yielded increasingly complex and inclusive categories and continued until all of the data (i.e., interview transcripts) were accounted for in the core categories of the grounded theory paradigm (Glaser, 2001). Final categories represented theoretical saturation of key psychosocial patterns related to recovery and resilience that were consistent across variation in the sample, including differences in demographics, childhood exposure to violence, characteristics of the battering experience, and psychosocial functioning. As theoretical categories and themes emerged, they were coded and organized using the qualitative data analysis program, ATLAS/ti (Drisko, 2004). Examples drawn from interview transcripts (using pseudonyms) are highlighted in the results.
Recovery and Resilience in the Aftermath of Domestic Violence
Participants had inevitably experienced the trials and tribulations of recovery. These women faced stressors in the aftermath of domestic violence, including reoccurring trauma symptoms (e.g., depression, anxiety) and their batterers’ persistent attempts at controlling them (i.e., stalking; breaking into their homes; and harassing the women’s employers, friends, and family). As a result, participants reported lingering effects in their ability to make decisions, concentrate, and tolerate negative emotions. For these participants, leaving an abusive relationship and working toward recovery, took a tremendous amount of personal strength that was bolstered through spiritual and social support. Spirituality and corresponding religious beliefs played an important role in participants’ recovery by giving them the strength to prevail, uncovering the benefits of their suffering, and giving their lives purpose. In addition, until they were strong enough to support themselves, participants found it necessary to seek and accept informal and formal support from others. These women identified how in rebuilding their lives they experienced growth in their self-awareness, faith, and interpersonal relationships.
Spiritual Support: Relationship to a Higher Power
Thirty-one participants reported how depending upon a transcendent force, something beyond themselves, helped them to rise above their suffering. Seven participants discussed how their spirituality was not related to faith-based settings, while the remaining 24 discussed how their spirituality was a blend of organized religion and informal experiences. Such spiritual support contributed to personal and social transformation for these women during their recovery. Participants described the importance of a spiritual relationship to help them view their trauma and life purpose in a different light. Instead of thinking one’s lot in life was to be abused, they were able to appreciate what they had learned from their struggles, such as increased strength, wisdom, and compassion:
I tell you it was the worst experience in my life, but it was also the best experience in my life . . . It made me a stronger person, and I feel like what I have gone through, I can pass along to others, and I feel like I have this intuition when I’m around people that are in those situations, and I try to make it evident but not obvious, that I’m there for them if they need anything. (Denise, age 42)
A connection to a Higher Power fostered a sense of meaning, purpose, and value in life; all heighten areas for these women in the aftermath of their trauma. The following quote exemplifies the growth in their beliefs about self (from vulnerability to strength), victimization (from questioning their suffering to finding meaning), and life purpose (from doubting their existence to valuing their lives):
There were many nights I prayed. I prayed either to get me out of the situation or to give me the knowledge to get me out of the situation. Maybe the good Lord knew that I needed to go through this to get to where I’m at now. I really believe that everything happens in your life for a purpose. I think I had to go through what I went through . . . and I know mine wasn’t as bad . . . because a lot of women have it a lot worse than I did. But I feel like I had to go through that. (Karen, age 52)
For 23 (of 31) participants, spirituality was a constant throughout their lives as God (or a Higher Power or Spirit) was viewed as a source of strength, protection, love, and hope. They viewed God as a guiding force that saved their lives, helped them to prevail, and gave them strength to end their abusive relationships:
I’ve always believed that things happen for a reason. I mean, what doesn’t kill you always makes you stronger, that’s just what I think. I’ve been through a lot. I’ve been through things that a lot of people can’t make it through, and I ask myself how can I be so forgiving to people for what they’ve done to me, and how did I manage to make it this far? And the only answer that I come up with is by the grace of God; I don’t know how else to explain it. (Jill, age 32)
Eight (of 31) women discussed how their spiritual development evolved once they were free of the abusive relationship. While the violence was occurring, these eight women discussed having an uneasy relationship with a Higher Power as they viewed Him/Her as failing to protect them during the abuse. Yet, as they worked through these spiritual conflicts and crises of faith during their recovery it allowed them to alter previously held assumptions about a Higher Power as being neglectful and uncaring:
I’ve always believed in God, but during this turmoil, it was like God had abandoned me. And I come to find out, I come to realize God didn’t abandon me, I walked away from him. So it took from my pastor, the support from my family, to help me get where I am. I still have a ways to go, and I’m not going to stop ‘til I get there. (Angel, age 42)
For six women, spirituality was not a significant factor in their recovery. Two did not mention it in their interviews, one continued to express doubts in trusting a Higher Power, and the remaining three did not perceive spirituality (as opposed to other support systems) as key to their healing. These six women also struggled with life crises related to finances, health, and/or mental health. Thus, their life focus was on securing needed resources, rather than working through spiritual and existential matters.
Spiritual Support: Religious Community and Leaders
Nineteen participants reported that church support and involvement were instrumental in their recovery. Their religious communities offered emotional comfort, a sense of belonging, security, and practical assistance (e.g., financial, shelter). A particular benefit was women-to-women ministry, which provided guidance, mentoring, and companionship:
Never say that faith isn’t the answer. I had counselors telling me that my faith wouldn’t get me through. I had counselors telling me that my religion wasn’t going to save me, and I can look back, and that’s what did save me. It was my church community; it was these people at “Women to Women.” They are all Christian-based women who have been through this [domestic violence] and have come to know the Lord through these situations. People say that He’s not around. I always thought God had abandoned me. When I look back, He was right there by my side every step of the way. He put people in my path that He knew I would need to strengthen me, to guide me, before I even did. I mean, it was like divine intervention that me and my daughter got out of our situation. (Daisey, age 31)
Three women discussed how their church communities were not helpful while the violence was occurring as they were pressured to forgive their abusive spouses and evoked guilt for ending their marriages. Upon leaving the abuser, two women not only changed churches but denominations as well.
I also feel like this fundamental sort of Baptist thinking that the church had at that time on domestic violence was save the marriage at all costs. I feel like I would have left him sooner than I did had the church not been saying, “Oh, just pray to God that it will be okay.” And that’s part of the reason I’ve done the [psychology] degree, because “just pray to God that it will be okay” is not an answer. (Lou, age 50)
Nine participants discussed turning to religious leaders for counsel, solace, and clarity of scriptures and core doctrines. These women experienced spiritual anguish between upholding their Christian values (i.e., marriage is sacred, uniting, and forever) with their desire to leave their abusive relationship. Two women discussed how seeking spiritual advice was not helpful as they felt pressured to preserve the sanctity of the marriage. Although religious leaders did not blame them for the abuse, they did encourage them to remain in the relationship and receive religious counsel with their spouses. In contrast, seven participants talked about how clergy put their safety first, provided needed resources (e.g., financial, shelter) for them to leave, and were a catalyst for them to end the marriage:
I had to go see a priest before I would even complete the process of getting a divorce. I needed to know that I was not sinning. I’m Catholic, and so divorce is huge. And so I went to talk to a priest, and I’m like, “My mom stayed, and dad [former batterer] got better,” and fortunately I had a great priest, who was very reassuring and said, “Your husband broke your marriage vows the first time he laid his hand on you. You have nothing to worry about. Get out.” (Trista, age 33)
Social Support: Informal Networks
Participants gave regular testimony on the importance of having family (n = 26), friends (n = 18), and supportive employers (n = 5) in their lives as their recovery and growth could not have occurred in isolation. These women stressed how support systems were essential, particularly during the first two years after leaving the batterer, because of the affirmation, encouragement, stability, and resources (e.g., financial, housing) they provided. They discussed how they were more able to take action in their lives as their informal network was available to ease their burdens:
It was hard to bounce back and get the strength to believe in myself again, but I was able to have a good support background. I feel sorry for anybody out there who doesn’t have a loving family, because that’s going to be your main strength. I went from wanting to kill myself every day to, right now, just being able to stand up and say, “Hey, I’m me, and I love myself.” It was really hard to go from one point to the other without support. (Angel, age 42) I thought I would lose my job. But I asked everybody [staff] to sit down and I just told them. I said, “Here is what is going on in my home life.” You could have heard a pin drop. None of them suspected anything. But from that moment on they became my strongest allies. And they were the ones that actually helped me do all the planning. They were the ones that would ensure that if the vehicle came anywhere on the grounds of the hospital, that I was alerted. They were splendid. (Susie, age 56)
For 26 women, their families-of-origin were a significant support for them during their recovery. Yet, during the time of the violence, their families often did not actively intervene for such reasons as being unaware, not wanting to interfere, or not knowing how to help. Occasionally, some family members sanctioned the violence by encouraging the participant to remain in the relationship. Betsy (married 12 years to the batterer), reported, “My mother said, ‘You probably deserved it, you made your bed, now lie on it.’” Interestingly, family members for these 26 women did get “on board” in providing support once the woman decided to leave the batterer for good. Even in Betsy’s case, her parents provided financial support for legal fees. Families risked their own safety and often went to great lengths to protect their loved ones; for example, the participant whose parents built their retirement home as a safe haven for her and her daughter:
My mom and dad were building their retirement home, and my dad sat his granddaughter on his lap and he looked at her and said, “You’re going to have a home, and nobody’s ever going to hurt you again.” And that was the moment that he started asking my daughter and I, “What’s it going to take for you guys to feel safe?” My parents spent a lot of extra expense in doing it. The locks are special locks for safety reasons and we’re in the ground with concrete all around us. We’re safe. (Daisey, age 31)
Social Support: Formal Networks
An essential strength of the participants was their ability during times of stress and crisis to seek help, including accessing formal networks (e.g., domestic violence services, mental health counseling). Although community resources were used less often than spiritual and informal supports, those who sought such services often found them helpful for their recovery. Of the 12 women who stayed at domestic violence shelters, 10 found it to be a positive experience in providing safety, support, education (e.g., safety strategies), and connection to other helping systems (e.g., legal, financial, health). Two women found residential services not helpful due to restrictive shelter rules, negative staff demeanor, and communal living chaos (e.g., mothers not supervising their children). Six women wanted to access domestic violence shelters, but no such services existed in their rural areas. In addition, four women sought out nonresidential domestic violence resources (e.g., support groups, information on community resources, crisis hotline), which they viewed as beneficial to their recovery.
Probably asking for help is one of the hardest things a person can do, but it’s one of the best things a person can do. Cause you can find out that there’s something else out there and that you don’t have to hurt all the time. You don’t have to be demeaned in various ways. You don’t have to be in the hospital with a broken arm and say you fell down the stairs. There is another way to live and they can help you find that way to live and show you how to live. (Ruby, age 24)
Supportive and therapeutic community resources included Alanon (n = 1), AA (n = 1), and individual counseling (n = 11). Of those who sought mental health counseling, nine found it helpful in talking about the abuse, processing their trauma, and managing their PTSD symptoms:
Today, I can honestly say my feelings, my emotions, I don’t let the past control me anymore. When you get those flashbacks from the past, you’ve just got to tell yourself, “No, you’re not going to steal my joy. No, you’re not gonna take away this moment.” (Daisey, age 31)
Two women found therapeutic services not helpful due to the provider’s lack of expertise in the area of domestic violence resulting in blaming them for the abuse:
I’ve had some therapists that I went to once and never went back. Because the minute I feel that blame is being placed on me, they’re not doing their jobs, and they’re not being effective to me, and I’m not wasting my time. But I know for other women who maybe it’s the first time they’ve gone to a therapist, they don’t know; and so, those kind of therapists can be more harm than good, and so I think if women are seeking counseling and they go to a therapist and they leave there feeling worse than they did when they walked in the door, don’t go back. Don’t go back, ‘cause it’s not your fault. There is nothing that you did wrong to make this abuse occur. They think, “They’re a therapist, they’re gonna help me. They got a degree. I’ll keep going back.” Well, it does more harm than good. (Katie, age 30)
Discussion
This study’s findings are encouraging as we discovered that women can recover and be successful upon leaving an abusive relationship, even when the abuse lasts for many years. The 37 women interviewed were at risk for anxiety, depression, low self-esteem, and other interpersonal difficulties due to experiencing domestic violence. Surprisingly, at the time of the study these women did not significantly suffer from these adverse effects and had relatively strong resilience. Participants, however, were not free of trauma symptoms, including limitations in their decision-making and ability to tolerate negative emotions. Nine women were symptomatic for PTSD, yet they also showed hardiness as their average resilience score was higher compared to other PTSD populations (M = 63.11 vs. M = 47.8, Conner & Davidson, 2003). Humphreys’s study with battered women (residing in domestic violence shelters) found participants showed both psychological distress and resilience as well. Our results and Humphreys’s suggest resilience and impairment are not necessarily opposites, but instead appear to be different aspects of the overall experience of coping and adjustment for survivors of domestic violence. In other words, demonstrating resilience may not necessarily infer absence of psychopathology. Our qualitative findings also support such speculation as key psychosocial patterns related to recovery were consistent across differences in psychosocial functioning. Consequently, further research is needed in regard to the relationship between resilience and psychological distress as they may not always be predictably related (Tedeschi & Calhoun, 1995).
Developing support systems and mobilizing resources were central to participants’ resilience and ultimately to their recovery from domestic violence. Accessing spiritual and informal support was particularly helpful for their healing and growth. The rural context, where individuals often turn to faith-based communities and informal support first before seeking public resources, may have influenced this study’s findings. In addition, formal service accessibility is limited in rural areas and those that do exist often are not adequately funded or staffed (Logan, Walker, Cole, Ratliff, & Leukefeld, 2003). Yet, regardless of physical location, spiritual and social support are pervasive and beneficial aspects in many individuals’ lives, including domestic violence survivors, with direct relevance to mental health and quality of life issues (Bent-Goodley & Fowler, 2006; Farley, 2007; Kocot & Goodman, 2003). For instance, Gillum, Sullivan, and Bybee’s (2006) study of domestic violence survivors found that 97% of their study sample (151 urban and culturally diverse women) reported that spirituality or God was a source of comfort for them and that religious involvement tended to increase their psychological well-being. In addition, several researchers have identified the importance of support from religious leaders and communities along with a personal relationship with God as important aspects of recovery for domestic violence survivors (Giesbrecht & Sevcik, 2000; Postmus, Severson, Berry, & Yoo, 2009; Senter & Caldwell, 2002; Shannon-Lewy & Dull, 2005; Wendt, 2008). Discussions of religiosity and spirituality, therefore, should not be solely left up to faith-based communities to address with women survivors. Providers of domestic violence services also need to openly approach these matters as they are vital for some individuals in their healing process (Bent-Goodley & Fowler, 2006).
Implications for Practice
Looking at long-term recovery outcomes gives hope to others on what can happen upon leaving an abusive relationship. For the women in this study, their lives did improve as a result of the many internal and external resources they were able to access and develop. In addition to tangible resources, positive social support can provide opportunities for survivors to speak the unspeakable, receive affirmation and validation, along with reviewing and even rewriting their life stories (Herman, 1997). Thus, professionals may assist each survivor in figuring out who is supportive in one’s environment and strengthen those connections while allowing for disengagement from negative support.
Although several women in this study spoke of personal strength they discovered through their experiences of abuse, professionals must be careful not to minimize victimization and its often devastating consequences as a person is not better off, for instance, because she experienced domestic violence. Rather, individuals may redefine themselves by their struggles to prevail despite their victimization (Norman, 2000). If applicable, practitioners may aid survivors to recreate a narrative that includes positive outcomes from one’s struggle to overcome the trauma, but not from any loss or changes that may have occurred as a result of it (Tedeschi & Calhoun, 1995). The goal of the helping process should not be for professionals to impose a resiliency framework onto survivors’ life experiences. The intent is not to deny the real trauma of domestic violence and its consequences. However, helping women reformulate life stories that feature their strengths and resourcefulness does refute that people who endure such hardships are lacking in resilience or are unable to achieve their aspirations.
Changes in a survivor’s behavior are propelled or constrained by the meaning she attaches to her experiences (Goodman et al., 2003). As survivors try to understand the purpose and meaning of their lives, they may seek answers for the “why” of their suffering. Thus, helping professionals cannot discount the spiritual dimension so long as clients question injustice and seek spiritual responses to it (Asher, 2001; Coholic, 2003). Practitioners often discuss the dynamics of abusive intimate relationships (e.g., power and control) with survivors, providing them with important knowledge on the causes of violence, yet it does not necessarily address or resolve the “why” of suffering for such individuals. For those survivors who are interested in addressing the purpose of their suffering, they may be guided to draw upon their intuition, wisdom, and, if applicable, a spiritual connection. Answering “why” differs for each individual; however, commonalities among participants in this study included an improved evaluation of self (e.g., stronger, more compassionate), a more profound understanding of the world (e.g., life is not easy, thus to be human is to suffer), and a greater life purpose (e.g., breaking the cycle of violence, helping other survivors). We propose that helping professionals may use the following questions to assist survivors who seek answers to “why me?”
What are the lessons learned, if any, from enduring suffering in regard to positive changes in yourself, relationships with others, and the beyond (e.g., a Higher Self, a Higher Power or God, nature, humanity, or the universe)? How, if in any way, have you found meaning in your suffering? How, if in any way, does your suffering provide you with a greater life purpose (e.g., breaking the cycle of violence, wanting to make a difference for others)? Have you ever felt connected to something beyond yourself (e.g., a Higher Self, a Higher Power or God, nature, humanity, or the universe)? How does this connection, if in any way, give you a sense of meaning and/or purpose in life?
Strengths and Limitations of the Study
This exploratory study is one of few to examine the process of resilience among women formerly in an abusive relationship. In doing so, it provides fruitful insights for practitioners and researchers on how women can begin and sustain recovery in the aftermath of traumatic experiences. While the study’s sample was diverse in some demographic (particularly education and employment levels) and abuse-related variables, the sample was drawn from rural areas in one Midwestern state where ethnic and racial diversity is lacking. Findings from this study show promise for future researchers interested in understanding more about how women recover from domestic violence, but generalizing to other samples of women is limited.
Conclusion
Exploring domestic abuse survivors’ perceptions of what happened to them in the aftermath of traumatic events, as in this study, assists in understanding how resilience can emerge from such chaos and devastation. Such information underscores the inordinate amount of strengths present among many women who have experienced domestic violence and adds to literature focused on understanding the process of resilience that may greatly benefit practitioners, advocates, and researchers alike.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded through a Women’s and Gender Studies Grant at the University of Missouri-Columbia.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.