
Abstract
In this research, we used a multi-level contextual-effects analysis to disentangle the household- and community-level associations between income and intimate partner violence (IPV) against women in Bangladesh. Our analyses of data from 2,668 women interviewed as part of the World Health Organization (WHO) multi-country study on women’s health and domestic violence against women showed that household income was negatively associated with women’s risk of experiencing IPV. Controlling for residence in a low-income household, living in a low-income community was not associated with women’s risk of experiencing IPV. These results support a household-level, not community-level, relationship between income and IPV in Bangladesh.
Intimate partner violence (IPV), defined as “behavior within an intimate relationship that causes physical, sexual, or psychological harm, including acts of physical aggression, sexual abuse, and controlling behaviors” (World Health Organization [WHO], 2010, p. 11), is a major public health problem affecting women around the world. The consequences of IPV are severe. Women experiencing IPV are at increased risk for multiple physical, psychological, and reproductive health problems, including poor pregnancy outcomes (Devries et al., 2011; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Yount, DiGirolamo, & Ramakrishnan, 2011). Women in all countries and across all social, economic, cultural, and religious groups are at some level of risk for experiencing IPV (WHO, 2002). In a multi-country study of IPV against women, physical and sexual IPV often co-occurred, and 15% to 71% of ever-partnered women reported experiencing physical or sexual IPV, or both, at some point in their lives (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). Another multi-country, population-based study documented lifetime rates of IPV against ever-married women ranging from 18% to 48% (Kishor & Johnson, 2004). In Bangladesh, population-based studies have documented high rates of lifetime physical (42%-51%) and sexual (37%-50%) IPV against women (Garcia-Moreno et al., 2006; Koenig, Ahmed, Hossain, & Khorshed Alam Mozumder, 2003).
An ecological framework has characterized IPV as an outcome of direct and interacting personal, situational, community, and sociocultural influences (Heise, 1998). Globally, most research on the correlates of IPV has focused on individual, couple, and family factors, but increasingly, researchers have begun to focus on community-level factors, particularly on the relationship between community economic status or disadvantage and IPV against women (VanderEnde, Yount, Dynes, & Sibley, 2012). The relationship between economic status and IPV has been theorized to operate at multiple levels. At the community level, researchers have drawn from social disorganization theory, a theory rooted in U.S. criminology. At the household level, researchers have drawn from resource theory (Goode, 1971), which posits that there is an inverse relationship between individual resources and IPV. Pertinent to the discussion of economic status and IPV is the differentiation of contextual and compositional effects. Specifically, a contextual effect refers to the characteristics of a group or area, whereas a compositional effect refers to the characteristics of individuals (Diez-Roux, 2000, 2002). A contextual effect is present if the aggregate of a person-level characteristic is related to an outcome after controlling for the effect of the person-level characteristic (Raudenbush & Bryk, 2002).
Researchers have demonstrated a negative association between household economic status, measured in terms of household assets and income, and physical IPV in Bangladesh (Ahmed, 2005; Bates, Schuler, Islam, & Islam, 2004; Hadi, 2005; Koenig et al., 2003; Sambisa, Angeles, Lance, Naved, & Curtis, 2010; Sambisa, Angeles, Lance, Naved, & Thornton, 2011); however, to our knowledge, none has explored the association between community-level economic status and physical and/or sexual IPV in Bangladesh, controlling for household economic status (VanderEnde et al., 2012). To address this gap in the literature, we used a multi-level contextual-effects analysis to disentangle the household- and community-level associations between income and prior-year physical and/or sexual IPV against women.
Theoretical Perspectives and Empirical Research
Community-Level Factors and IPV
In the 1990s, researchers began to explore the relationship between community economic status and physical IPV, particularly in urban, U.S. settings (O’Campo et al., 1995). Research, especially in the United States, adapted social disorganization theory (Shaw & McKay, 1942/1969) to explain community-level variations in IPV against women. Criminologists originally used this theory to explain crime and delinquency in urban, North American cities. The main premise of the theory is that economically deprived, ethnically heterogeneous neighborhoods with high levels of residential mobility are unable to organize to reduce crime and deviant behavior in their neighborhoods. Social disorganization has been examined in relation to IPV through multi-level regression analyses of community characteristics, including concentrated disadvantage (Benson, Fox, DeMaris, & Van Wyk, 2003; Benson, Wooldredge, Thistlethwaite, & Fox, 2004; DeMaris, Benson, Fox, Hill, & Van Wyk, 2003; Jain, Buka, Subramanian, & Molnar, 2010; Van Wyk, Benson, Fox, & DeMaris, 2003; Wright & Benson, 2010, 2011), neighborhood deprivation (Kiss et al., 2012), the percentage of the population living in poverty (Caetano, Mikler, & Harris, 2010; Cunradi, Caetano, Clark, & Schafer, 2000; Lauritsen & Schaum, 2004), asset-based measures for standard of living (Ackerson & Subramanian, 2008; Boyle, Georgiades, Cullen, & Racine, 2009; Gage, 2005), neighborhood rates of overall unemployment or male unemployment (Caetano et al., 2010; Cunradi, Caetano, & Schafer, 2002; Gage, 2005), residential stability or instability (Benson et al., 2003; Browning, 2002; Wright & Benson, 2010), and immigrant concentration (Browning, 2002; Wright & Benson, 2010). Researchers examining community-level correlates of IPV against women have focused on measures of community economic status, such as concentrated disadvantage (operationalized by summary measures including percentage below the poverty line, percentage on public assistance, percentage of female-headed households, percentage non-White, and percentage unemployed living in a neighborhood), neighborhood poverty, and standard of living (VanderEnde et al., 2012). These analyses, which controlled for variables at the individual-, couple-, and/or household levels, showed a positive relationship between neighborhood concentrated disadvantage and physical IPV against women in the United States (Benson et al., 2003; Benson et al., 2004; DeMaris et al., 2003; Van Wyk et al., 2003; Wright & Benson, 2010, 2011). However, findings from Brazil (Kiss et al., 2012), Columbia (Hynes, 2012), Haiti (Gage, 2005), India (Ackerson & Subramanian, 2008; Boyle et al., 2009), and the United States (Caetano et al., 2010; Cunradi et al., 2000; Lauritsen & Schaum, 2004) have shown inconsistent associations between neighborhood deprivation, neighborhood standard of living, or neighborhood poverty and physical IPV (Ackerson & Subramanian, 2008; Boyle et al., 2009; Gage, 2005) and physical and/or sexual IPV against women (Caetano et al., 2010; Cunradi et al., 2000; Hynes, 2012; Kiss et al., 2012; Lauritsen & Schaum, 2004). Empirical findings from Chicago-based research also have failed to support other aspects of the theory, specifically the association of residential instability and immigrant concentration with physical IPV against women (Browning, 2002; Wright & Benson, 2010).
Given these contradictory findings, we argue that the relationship between community economic status and IPV against women, as posited by social disorganization theory, may not be applicable to non-urban, non-U.S. settings for several reasons. First, measures often used to operationalize the construct—such as the percentages of residents on public assistance, residents who are non-White, and female-headed households—may not capture relevant features of communities cross-culturally. Second, other measures often included in indices of concentrated disadvantage—such as the percentage in poverty and percentage unemployed—have not been consistently independently associated with IPV against women. Third, an underlying assumption of social disorganization theory is that “organized” communities act to prevent deviant behavior. We question whether this assumption is applicable in the case of IPV against women, as there is wide variation in justification of wife beating across countries (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2005; Kishor & Johnson, 2004; Yount, Halim, Hynes, & Hillman, 2011). Moreover, communities may differ in their recognition of IPV as a deviant behavior (Yount, 2011; Yount & Li, 2009), which distinguishes IPV from other forms of violence.
Household-Level Factors and IPV
Goode’s (1971) theory of resources and force asserts that in households with fewer economic resources, individuals have less power and prestige, and thus have fewer resources available to achieve their goals. As a consequence, they are more likely to rely on force to achieve these outcomes. Others have viewed stress as a mediator of the relationship between household poverty and IPV, as low-income increases stress, which in turn leads to violence (Gelles, 1974; Jewkes, 2002). Empirical support for the relationship between household economic status and physical IPV against women has accrued across a range of settings, including Cambodia (Yount & Carrera, 2006), Egypt (Yount, 2005; Yount & Li, 2010), India (Jejeebhoy & Cook, 1997), North America (Smith, 1990), the Philippines (Hindin & Adair, 2002), and Thailand (Hoffman, Demo, & Edwards, 1994). A systematic review of studies from 34 sites in low- and middle-income countries found that higher household wealth (as measured by assets) was, in general, negatively related to physical and sexual IPV against women (Vyas & Watts, 2009). Similarly, results from a multi-country study of the correlates of IPV against women in 15 sites in 10 countries demonstrated a statistically significant association between higher household socioeconomic status (SES) and a lower risk of IPV (physical and/or sexual) against women in 8 of 15 sites (Abramsky et al., 2011). In contrast, Kishor and Johnson’s (2004) analysis of Demographic and Health Survey (DHS) data from nine countries found an inconsistent relationship between household SES and physical and/or sexual IPV. Specifically, analyses of data from India, Egypt, and Peru showed lower odds of women experiencing violence in wealthier households, whereas analyses from other countries demonstrated non-significant or inconsistent relationships (Kishor & Johnson, 2004).
In Bangladesh, the relationship between economic status and IPV against women has focused mainly on household-, not community-level factors. Studies have shown that women living in poorer households have higher risks of experiencing physical and psychological IPV than do women living in wealthier households (Ahmed, 2005; Hadi, 2005). In rural Bangladesh, Bates and colleagues (2004) found women’s odds of experiencing physical IPV were lower with higher economic status, as measured with an aggregate scale of household building materials and ownership of assets. In slum and non-slum areas of urban Bangladesh, higher household wealth has been negatively associated with physical and sexual IPV, but researchers did not find a significant association between IPV and residing in slum versus non-slum urban areas (Sambisa et al., 2010; Sambisa et al., 2011). The ownership of land also has been negatively associated with IPV. In two rural areas of Bangladesh, for example, Koenig and colleagues (2003) reported an inverse relationship between household landholdings and women’s experiences of physical violence perpetrated by their husband or husband’s family, with women living in households with more land at a lower risk of violence. In another study, ownership of land was shown to have a negative association with sexual IPV, but only for women with children in the neonatal period (Hadi, 2000).
Other Factors
Community-level factors
Analyses of the relationship between economic status and IPV need to account for potential confounders at both the community and household levels. In population-based studies of nine countries, urban residence was positively associated with women’s reports of experiencing physical and/or sexual IPV in six countries, whereas in two countries (India and Egypt), urban residence was negatively associated with women’s reports of IPV (Kishor & Johnson, 2004; Yount & Li, 2010). In DHS surveys, urban residence has been associated with higher levels of wealth (Rutstein & Johnson, 2004). In the 2011 Bangladesh DHS, more than half of the population in urban areas (55.1%) was classified in the highest wealth quintile, compared with only 8.8% of those in rural areas (National Institute of Population Research and Training [NIPORT], Mitra and Associates, & ICF International, 2013).
Individual- and couple-level factors
Individual demographic factors, specifically age and educational level, may also confound the relationship between economic status and IPV. In Bangladesh, persons living in lower wealth quintiles have been less likely to attend school (NIPORT et al., 2013), and both women’s young age and lower educational level have been associated with higher risks of physical and sexual IPV (Ahmed, 2005; Bates et al., 2004; Hadi, 2000, 2005; Koenig et al., 2003; Naved & Persson, 2005; Schuler, Hashemi, Riley, & Akhter, 1996). In Bangladesh specifically, marriages involving a dowry, poor spousal communication, women’s contributions to household earnings in poor households, and a history of abuse of a woman’s husband’s mother by his father, all have been associated with higher risks of physical and sexual IPV in urban and rural areas (Bates et al., 2004; Naved & Persson, 2005, 2010).
Summary
Based on the above theory and corresponding evidence, we hypothesized that the relationship between economic status and physical and/or sexual IPV against women in Bangladesh is a household-level, rather than a community-level, association. After accounting for potential confounders and other risk factors for IPV, we expected that women living in poorer households would be more likely to experience physical and/or sexual IPV than women living in less poor households. Controlling for household economic status, we anticipated no higher risk of experiencing physical and/or sexual IPV for women living in poorer communities compared with less poor communities.
Method
The analysis was based on data drawn from the Bangladesh subset of the WHO’s Multi-Country Study on Women’s Health and Domestic Violence Against Women (Garcia-Moreno et al., 2005). The International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) an international research organization based in Dhaka, in collaboration with Naripokkho, a women’s activist organization (Naved & Persson, 2005), conducted the study in one urban and one rural area of Bangladesh. The urban setting for the study, a city with a population of more than 10 million people, included areas of extreme poverty and low literacy. The population of the city was 90% Muslim. The rural setting for the study was a densely populated rural district of Bangladesh located southeast of the capital, Dhaka. Also a predominantly Muslim area, the rural area was characterized by subsistence farming and pervasive landlessness (Naved, Azim, Bhuiya, & Persson, 2006).
Using a multi-stage sampling strategy, clusters comprised of 42 villages in the rural area, and 39 moholla (the smallest administrative unit, in the urban area) were randomly selected (Naved et al., 2006). In the rural area, a household list, updated each month by icddr,b, was used to randomly select 20% of households within each cluster, for a total of 1,946 selected households. In the urban area, every sixth household in a cluster was selected, starting from a randomly selected point using the probability-proportionate-to-size method, for a total of 2,105 selected households (Naved et al., 2006). Of the households selected, approximately 10% in each cluster were empty or destroyed. The response rate for the remaining households was 95.8% in the rural area and 95.9% in the urban area (Naved et al., 2006). A total of 3,505 household questionnaires, which included questions on economic indicators, such as household income, were administered. This form also included a list of the age and initials of girls and women in the household. If more than one eligible woman lived in the household, one woman was selected randomly from the list to participate. Women 15 to 49 years old and living in the study households were eligible to participate in the study. The women’s questionnaire was administered in a private setting after the woman provided her informed consent (Naved et al., 2006). In total, 3,130 never- and ever-married women were interviewed between June 25 and November 25, 2001. Of these, 2,702 were ever-married women between the ages 15 and 49 years (Naved et al., 2006). After excluding 34 women with missing data on the outcome or covariates, the final analysis included 2,668 ever-married women aged 15 to 49 years. We found no significant differences in demographic characteristics or experience of prior-year physical and/or sexual IPV between those with missing data and the 2,668 women included in the final sample.
Because of the sensitivity of violence-related events, the validity and reliability of reports of IPV may suffer from some rate of non-disclosure. Despite this concern, the Bangladesh study team followed international guidelines (WHO, 2001) regarding the design and wording of the questions, the training of the interviewers, and the implementation of the study to enhance disclosure of personal experiences of IPV (Ellsberg & Heise, 2005; Ellsberg, Heise, Pena, Agurto, & Winkvist, 2001). First, questions were focused on specific acts, such as being hit or slapped, and avoided using loaded terms such as violence or abuse (Jansen, Watts, Ellsberg, Heise, & Garcia-Moreno, 2004). Second, only female interviewers and supervisors were employed, and an emphasis was placed on cultural sensitivity (Jansen et al., 2004). Interviewers received a standardized 3-week training program in which interviewers were sensitized to gender issues and gender-based violence, trained on skills to minimize any distress experienced by respondents during the interview, and familiarized with the study questionnaire through role-plays and field practice. During the final week of interviewer training, the questionnaire was piloted in the research area. Third, for the protection of the respondents and study-team members, the study was introduced to the community and households as a survey on women’s health and life experiences. Each interview was conducted in a non-judgmental manner when the woman was alone, or with a child no older than 2 years of age. Questions relating to violence were introduced near the end of the survey, following the development of rapport between the respondents and the interviewers (Jansen et al., 2004). Ethical approval for the Bangladesh study was granted by the Ethical Review Committee of icddr,b.
Variables
Prior-year physical and/or sexual IPV
Nine items adapted from the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) captured physical and/or sexual IPV in the prior 12 months. The outcome variable was dichotomous, with a positive response to any physical and/or sexual IPV item in the prior 12 months coded as 1, and no experience of IPV in the prior 12 months coded as 0. Physical violence items captured whether or not a woman reported that her husband or partner (a) slapped her or threw something at her that could hurt her; (b) pushed or shoved her; (c) hit her with his fist or with something else that could hurt her; (d) kicked her, dragged her, or beat her up; (e) choked or burnt her on purpose; or (f) threatened to use or actually used a gun, knife, or other weapon against her. Sexual violence items captured whether or not a woman reported that her husband or partner (g) physically forced her to have sexual intercourse when she did not want to; (h) forced her to do something sexual she found degrading or humiliating; or (i) she had sexual intercourse when she did not want to because she was afraid of what he might do.
The CTS2 has been used widely in the United States and internationally (Langhinrichsen-Rohling, 2010) and provides a standard approach to measure IPV (Johnson, 2006). The scale has adequate internal consistency, with a Cronbach’s alpha of .80 for the measure of prior-year physical and/or sexual IPV for the Bangladesh subset of the WHO multi-country study. The measurement of prior-year physical and/or sexual IPV in this analysis is consistent with quantitative measures of IPV in Bangladesh (Naved & Persson, 2005) and other settings (Garcia-Moreno et al., 2005).
Household income, a measure of household economic status, was represented by annual household income in Bangladeshi taka divided by the number of individuals in the household, creating a per capita measure. In the household questionnaire administered to an adult household member before the interview with the selected woman, respondents were asked, “How much is your household’s total annual income, in cash and kind?” Per capita annual income permitted comparisons across urban and rural areas more so than a composite measure for household assets and amenities because the latter often differ substantially across urban and rural areas in Bangladesh.
Community income
A measure of community economic status was represented by the mean per capita household income for each village or moholla. To construct this measure, we used information on household income from all completed household questionnaires (n = 3,424). In Bangladesh, relatively few women earn an income (Naved & Persson, 2005; NIPORT et al., 2013); thus, this measure of income disproportionately captures husbands’ earnings.
Univariate analyses of the income variables revealed positively skewed distributions, necessitating log transformations of the income variables at both the household and community levels. We refer to these transformed variables as household income (log) and community income (log).
Control variables
As our sample was drawn from urban and rural areas of Bangladesh, we controlled for residence, a potential community-level confounder. We also controlled for women’s age (in years) and education (in completed grades). To assess the significance of the relationship between household- and community-level income and prior-year physical and/or sexual IPV, net of other known risk factors, we included the following variables as controls: marriage involving a dowry (yes, no), woman earns an income (yes, no), husband’s family history of IPV (yes, no), and the respondent’s reports of spousal communication. To measure spousal communication, we created an index based on four items (yes, no) assessing whether a couple often talked about what the respondent’s day was like, what her husband’s day was like, or discussed any worries of the respondent or her husband. Four yes responses were rated as high spousal communication, two or three yes responses as moderate spousal communication, and one or fewer yes responses as low spousal communication.
Analysis
First, descriptive statistics were generated in SPSS Version 20.0® for Mac (IBM, 2011) for all variables to identify missing and improbable values and to verify that assumptions for statistical tests were met. Second, we examined the associations between each covariate and prior-year physical and/or sexual IPV. Third, we used hierarchical generalized linear models (Gelman & Hill, 2007; Raudenbush & Bryk, 2002) to predict women’s likelihood of experiencing prior-year physical and/or sexual IPV. These models accommodate the multi-level or nested structure inherent in the data set due to the clustering of women within communities. Using HLM7 (Raudenbush, Bryk, Cheong, Congdon, & du Toit, 2011), we fit two-level models with participants as Level 1 units and communities as Level 2 units. To assess the variability of IPV across communities, we first ran an unconditional model with no person- or community-level predictors. Then we estimated a contextual-effects model to examine whether community income (log) predicts prior-year physical and/or sexual IPV after controlling for household income (log) and other covariates.
Let Yij take on a value of unity if participant i in community j reported that she experienced physical and/or sexual IPV in the prior year, with Yij = 0 if not; and µ ij denote the probability Yij = 1. This probability varies randomly over communities. However, conditioning on this probability, we have


We define η ij as the log odds of the probability of the occurrence of self-reported prior-year physical and/or sexual IPV for participant i in community j. Thus, we have

For the unconditional model, the Level 1 model is

where β0j is the community-average log odds of self-reported prior-year physical and/or sexual IPV. The Level 2 model is

where β00k is the average log odds of self-reported prior-year physical and/or sexual IPV across communities and τ is the variance between communities in community-average log odds of self-reported prior-year physical and/or sexual IPV.
To assess for the presence of a contextual effect of income, we added to the Level 1 model a Level-1 household income measure (log transformation) along with other Level-1 control variables, including the age and educational level of the participant, whether the marriage involved a dowry or not, whether a woman earns an income, the husband’s family history of IPV, and the level of spousal communication. The Level 1 model can be expressed as

At Level 2, we added an aggregate measure of income (log transformation) with a control for location:

For simplicity, we constrained all the β pj s to be invariant across communities. To address potentially high collinearity between household income (log) and community-level income (log), we centered household income around the group mean (group-mean centered). The household income variable (γ10) is orthogonal to its aggregate-level counterpart, community income (γ01), overcoming any possible collinearity problem (Suzuki, Yamamoto, Takao, Kawachi, & Subramanian, 2012). In this model, γ10 measures the association of household income (log) with the probability of the occurrence of self-reported IPV within communities, whereas γ01 measures the aggregate association of community income (log) with self-reported IPV between communities. The contextual effect, or the extent to which the relationship between community income and IPV differs from the relationship between household income and IPV, is equal to γ01 − γ10. If γ01 and γ10 are equal, no contextual effect is present (Raudenbush & Bryk, 2002; Suzuki et al., 2012).
We also tested an interaction between community income (log) and location at Level 2 (not shown), and found it non-significant, indicating that the relationship between community income (log) and IPV did not differ by urban or rural residence. We did not include the interaction term in subsequent models.
Results
Characteristics of the Sample
The sample was predominantly Muslim in both urban and rural areas (Table 1). The women were, on average, 30.9 years of age and had 5.9 completed grades of formal schooling, with urban women reporting more grades of schooling than their rural counterparts. Over half of the women in the rural area reported a marriage involving a dowry (51.4%), compared with 13.8% of women in the urban area. Across all sites, 8.8% of women reported a history of IPV in their husband’s family, and 18.4% of women reported earning an income. Annual household income, weighted by the number of individuals in the household, varied widely within and between urban and rural areas. On average, however, household income was higher in the urban than the rural area (M = 33,200 vs. 9,700 taka per year). Across all sites, 29.6% of women reported experiencing physical and/or sexual IPV in the prior year.
Sample Characteristics, Overall and by Location, Ever-Married Women 15 to 49 Years, Urban and Rural Bangladesh.
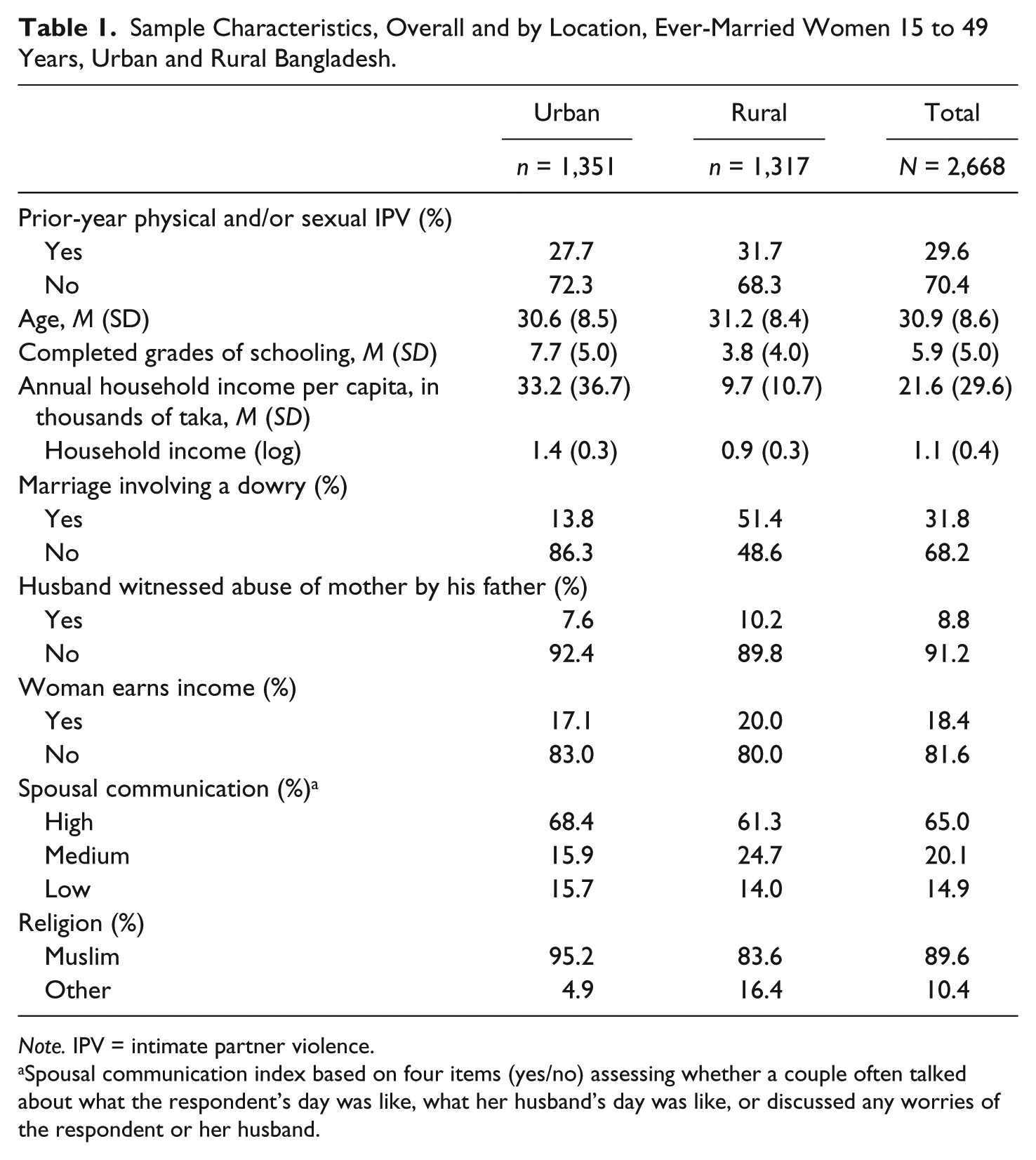
Note. IPV = intimate partner violence.
Spousal communication index based on four items (yes/no) assessing whether a couple often talked about what the respondent’s day was like, what her husband’s day was like, or discussed any worries of the respondent or her husband.
The sample available for the construction of the community income variable (n = 3,424) was larger than that available for the individual-level outcomes, which was limited to information from ever-married women between the ages of 15 and 49 years (n = 2,702). Across all sites, the mean number of ever-married women per community was 33.4, but this varied widely between communities (SD = 37.1). The percentages of women reporting prior-year physical and/or sexual IPV in each community ranged widely, from 0% to 71% in the urban area and from 6% to 80% in the rural area (Table 2). The mean annual per capita household income per community followed a similar pattern to household-level income, with higher mean per capita household incomes reported in the urban area.
Characteristics of Sampled Urban and Rural Communities in Bangladesh.
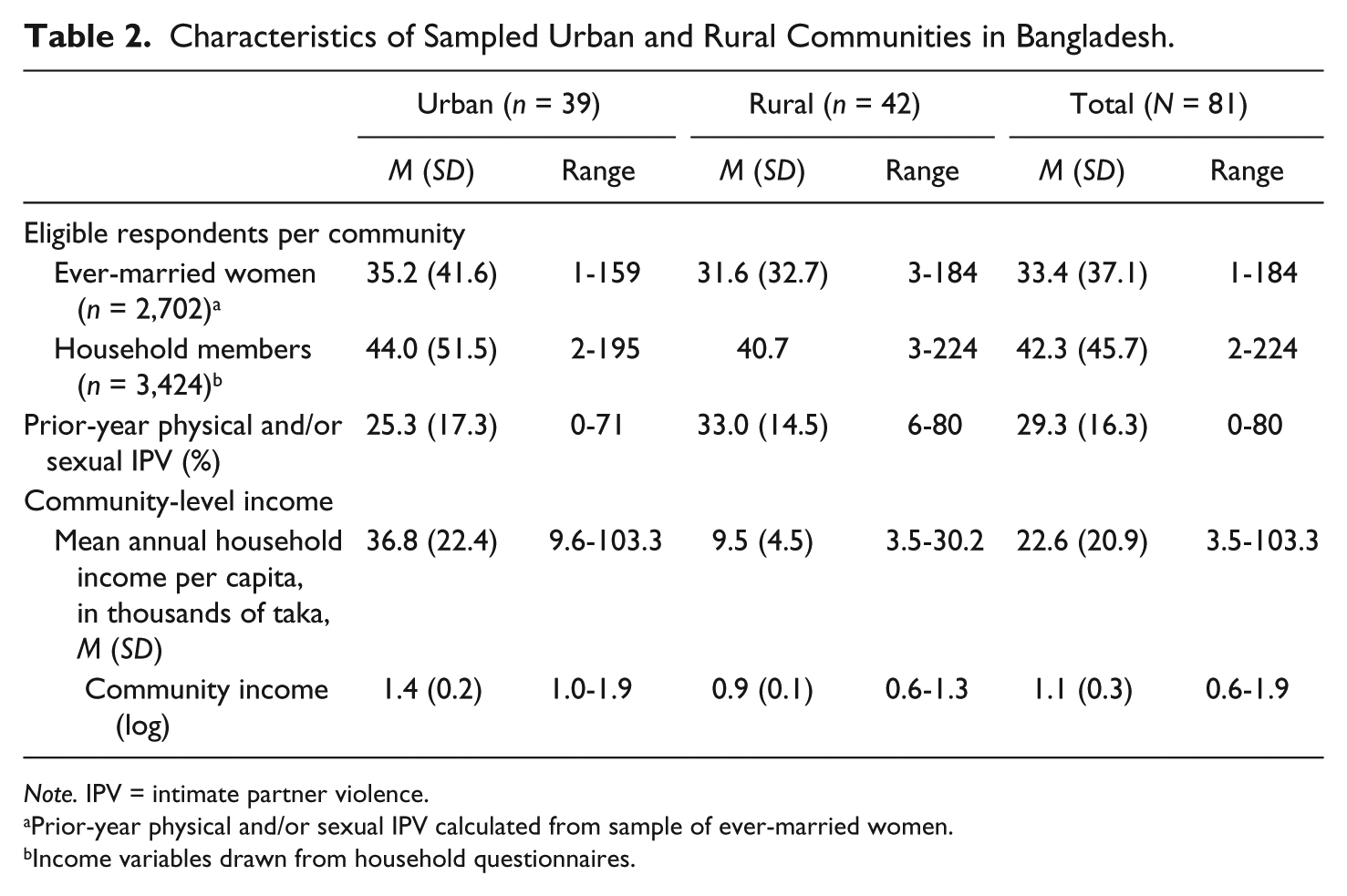
Note. IPV = intimate partner violence.
Prior-year physical and/or sexual IPV calculated from sample of ever-married women.
Income variables drawn from household questionnaires.
Multivariate Results
Model 1, an unconditional model with random effects, shows variation in prior-year physical and/or sexual IPV between communities (
Multivariate Models for Prior-Year Physical and/or Sexual IPV, Ever-Married Women (N = 2,668) 15 to 49 Years, Urban and Rural Bangladesh.
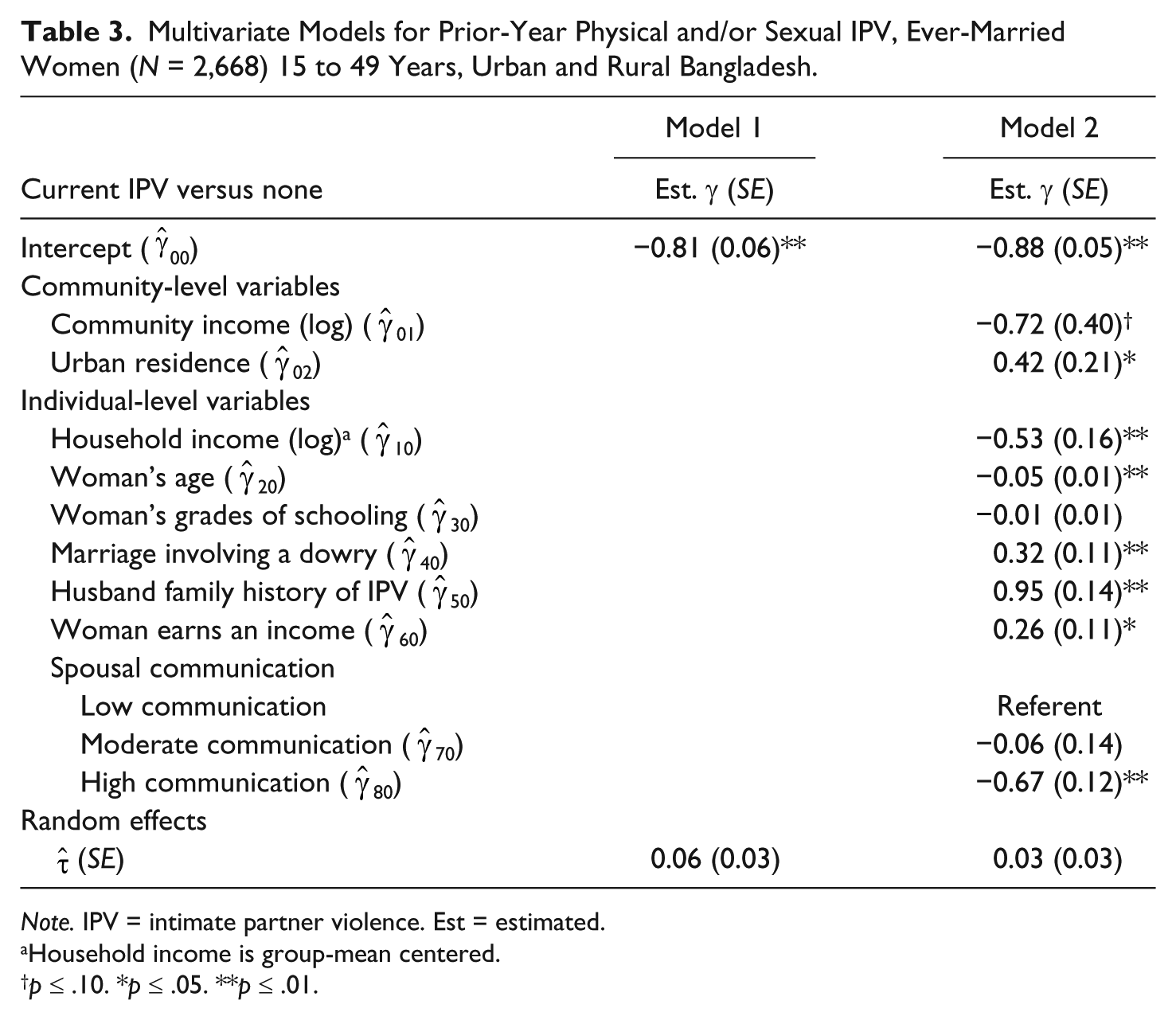
Note. IPV = intimate partner violence. Est = estimated.
Household income is group-mean centered.
p ≤ .10. *p ≤ .05. **p ≤ .01.
Discussion
In this analysis, we examined the relationship between economic status and IPV, a relationship that has been theorized to operate at both the household and community levels. To differentiate between compositional (household) and contextual (community) effects, we used a multi-level contextual-effects analysis to disentangle the associations of income at the household and community levels with physical and/or sexual IPV in the prior year. We expected that the relationship between economic status and prior-year physical and/or sexual IPV against women in Bangladesh would be a household-level, not a community-level, association. The study findings support our hypothesis. Specifically, the relationship between household income and prior-year physical and/or sexual IPV was negative. For higher household incomes, women’s risk of experiencing prior-year physical and/or sexual IPV was lower. These findings are consistent with other research from Bangladesh demonstrating a negative relationship between physical and sexual IPV and both various measures of household wealth (Ahmed, 2005; Bates et al., 2004; Hadi, 2005; Sambisa et al., 2010; Sambisa et al., 2011) and greater land ownership (Hadi, 2000; Koenig et al., 2003). These findings also are consistent with the results from a multi-country study of correlates of physical and/or sexual IPV against women (Abramsky et al., 2011) and a systematic review examining the relationship between household wealth and physical and sexual IPV against women in low- and middle-income countries (Vyas & Watts, 2009).
As hypothesized, the contextual effect between community income and prior-year physical and/or sexual IPV was non-significant after controlling for urban residence. From these results, we conclude that in these urban and rural areas of Bangladesh, the relationship between income and IPV operates at the household level. Controlling for IPV’s association with living in a poorer household, we found no additional association of reported exposure to prior-year physical and/or sexual IPV with women’s residence in a poorer community. These results corroborate others from India (Ackerson & Subramanian, 2008; Boyle et al., 2009) demonstrating no significant relationship between community standard of living and physical IPV, and findings from Brazil (Kiss et al., 2012) and Columbia (Hynes, 2012) demonstrating no significant relationship between living in socioeconomically deprived neighborhoods and women’s risk of experiencing physical and/or sexual IPV. These results also corroborate those from research in urban Bangladesh showing a negative relationship between household wealth and physical and sexual IPV, but no significant relationship between residence in slum versus non-slum urban communities and physical and sexual IPV (Sambisa et al., 2010; Sambisa et al., 2011).
These results, specifically the non-significance of the contextual effect of community income in relation to physical and/or sexual IPV, lend support to our argument that common explanations for the relationship between community economic status and IPV, such as those drawn from social disorganization theory, are inadequate to explain the relationship between income and IPV in non-U.S. settings, such as Bangladesh. Instead, we maintain, and our findings support, that the relationship mainly operates at the household level, as men with limited financial resources may use force to exert power in relationships (Goode, 1971). These results also lend support to stress theory, which posits that lower income increases stress, which may lead men to perpetrate violence (Gelles, 1974; Hoffman et al., 1994; Jewkes, 2002; Smith, 1990; Yount, 2005). The consistency of these results with research across diverse low- and middle-income settings (Abramsky et al., 2011; Ackerson & Subramanian, 2008; Boyle et al., 2009; Hynes, 2012; Kiss et al., 2012; Vyas & Watts, 2009) supports the generalizability of our findings.
The relevance of these findings for policy in Bangladesh is notable. A focus on poverty reduction has been identified as an important, but not singular, strategy to reduce IPV globally (Jewkes, 2002). In Bangladesh, poverty alleviation, specifically through microfinance programs targeting women, has been a focus of governmental and non-governmental organizations. Although our findings indicate a relationship between income and prior-year physical and/or sexual IPV at the household, and not community, level, we encourage caution in the application of this finding to policy. The relationship between women’s earnings and IPV differs from the relationship between household income and IPV (Vyas & Watts, 2009). Indeed, one of the control variables in our analysis, the respondent earning an income, was positively associated with women’s prior-year experience of physical and/or sexual IPV (
The limitations of our study suggest important avenues for future research. First, the cross-sectional design does not allow for causal inferences, and longitudinal studies of the income–IPV relationship are needed. Second, the sample is drawn from two distinct areas of Bangladesh (urban and rural), and so national longitudinal studies of the relationships examined here are needed. Despite these limitations, the use of a multi-stage sampling design has advantages for a study focused on community-level associations. The sample clusters, consisting of villages in the rural area and mohollas in the urban area, may correspond better to individuals’ perceptions of community than other constructs of community that have been used in other studies, such as census tracts in the United States. Finally, our measures of economic status relied on reports of annual income, weighted by the number of household members. The use of household income has been critiqued as a measure of economic status in poorer countries, and the use of a household wealth index, which represents a more permanent economic status than income, has been recommended (Rutstein & Johnson, 2004). In addition, the measure of per capita household income may mask the proportionate contributions of women and men to household earnings. Furthermore, women’s contributions to household earnings in poor households may elevate their risk of IPV (Bates et al., 2004; Naved & Persson, 2005). While recognizing these limitations, the use of annual income in taka as a measure of economic status allows for comparability across urban and rural residence, which may differ in household construction materials and types of household assets. Because household income in taka reflects men’s earnings disproportionately, it corresponds to a theoretical argument that men with less control over resources (i.e., less income) would resort to using violence to exert patriarchal control (Goode, 1971). Last, the consistency of our findings with other research on poverty and IPV in Bangladesh lends support to our use of the income measure (Ahmed, 2005; Bates et al., 2004; Hadi, 2005; Sambisa et al., 2010; Sambisa et al., 2011).
Despite the above-mentioned limitations, this study has a number of strengths. To our knowledge, it is the first to address specifically the compositional versus contextual effects of economic status and women’s risk of prior-year physical and/or sexual IPV in Bangladesh. The findings support an income/IPV relationship operating at the household level, suggesting that future research on community-level correlates of IPV should focus less on economic status and more on other promising correlates, such as gender inequality and collective efficacy (VanderEnde et al., 2012).
Footnotes
Acknowledgements
The International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) provided the data for this analysis and acknowledged with gratitude the commitment of Urban Primary Health Care Project (UPHCP), Asian Development Bank (ADB), and the Government of Bangladesh to the Centre’s research efforts. We express our gratitude to the women who provided us with a wealth of information, a fraction of which was used in this study. Comments from Kenneth Hepburn and anonymous reviewers on previous versions of this article are greatly appreciated.
Authors’ Note
This research was presented at the Population Association of America Annual Meeting, 2013, and the 19th Nursing Network on Violence Against Women International Conference, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection for this analysis was funded by the Urban Primary Health Care Project (UPHCP) of Bangladesh, under the auspices of the Government of Bangladesh and the Asian Development Bank (ADB), Grant Number GR-00046. This analysis was conducted while the first author was a doctoral candidate at the Nell Hodgson Woodruff School of Nursing at Emory University and was supported by a Global Health Institute doctoral research dissertation grant through Emory University. The final analysis and writing were supported by a postdoctoral fellowship through the Hubert Department of Global Health, Emory University.