
Abstract
Intimate partner violence (IPV) exposure has been associated with poor mental health outcomes for victims, but fewer studies have examined the unique contributions of emotional abuse to mental health. This study explored the contextual relationships between the type and frequency of IPV, community factors, and emotional health. Data were collected from a community-based IPV intervention program. Logistic regression found an increased likelihood of depression for respondents who experienced emotional abuse more than once per week (odds ratio [OR] = 4.864) and were worried about contact by the abuser (OR = 5.898). Results indicate the need for specific policy and practice attention to this issue.
Introduction
Exposure to intimate partner violence (IPV), particularly physical and sexual abuse, has been linked to negative mental health outcomes for victims, especially in the short term after the violence has occurred. However, relatively few studies have examined the mental health consequences of emotional abuse, though it is often suggested that emotional and psychological abuse can cause higher levels of emotional distress and be more damaging to mental health than other forms of abuse (Hill, Schroeder, Bradley, Kaplan, & Angel, 2009; Mechanic, Weaver, & Resick, 2008; Sullivan, McPartland, Armeli, Jaquier, & Tennen, 2012; Vitanza, Vogel, & Marshall, 1995). Furthermore, little is known about the pathways by which abuse, particularly emotional abuse, influences long-term depression and whether social and economic resources are associated with this outcome. This study sought to examine these contextual issues as they relate to the long-term emotional health of women who had been involved in an abusive relationship. While the conceptual boundaries of emotional and psychological abuse have not always been well-defined (Carbone-Lopez, Kruttschnitt, & MacMillan, 2006; Kelly, Warner, Trahan, & Miscavage, 2009), in this study, we have used the terms emotional and psychological abuse interchangeably, according the Centers for Disease Control and Prevention (CDC) National Center for Injury Prevention and Control’s definition of psychological/emotional abuse (Saltzman, Fanslow, McMahon, & Shelley, 2002).
An increased risk of depression for victims of IPV has been well-established in the literature (Alhabib, Nur, & Jones, 2012; Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Bonomi et al., 2006; Campbell, 2002; Carbone-Lopez et al., 2006; Dutton et al., 2006; Mechanic et al., 2008; VandeWeerd, Coulter, & Mercado-Crespo, 2011; Zlotnick, Johnson, & Kohn, 2006). A review by Dutton and colleagues (2006) suggests that the rate of depression in victims of IPV is twice that of the general population. While many studies focus primarily on physical and/or sexual abuse, a burgeoning area of research has found that emotional abuse predicts depression (Dutton, Goodman, & Bennett, 1999; Mechanic et al., 2008) and limited social functioning (McCaw, Golding, Farley, & Minkoff, 2007) when physical and sexual abuse are controlled. In a community sample, women who had experienced only nonphysical IPV in the past 5 years were 2.06 times as likely to experience minor depression and 1.75 times as likely to experience severe depression as women who had not experienced any abuse. The study also found that the effects of emotional abuse may persist over longer durations of time: Women who experienced nonphysical IPV more than 5 years prior to the study also had increased rates of depression compared with never-abused women, but these rates were lower than women who experienced more recent abuse (Bonomi et al., 2006). Other studies have found that victims report persistent psychological distress two years after experiencing psychological violence (Hill et al., 2009) and that women who experienced only psychological abuse were more than twice as likely to experience psychological distress than women who had not been abused (Romito, Turan, & De Marchi, 2005), particularly depression (Porcerelli, West, Binienda, & Cogan, 2006).
Using an ecological systems approach, factors that affect the relationship between IPV and depression have been found to be related to the abuse itself as well as within other levels of the ecological framework (Beeble, Sullivan, & Bybee, 2011). At the interpersonal level, the duration and severity of abuse have been associated with depression, although most studies focus on overall IPV rather than emotional abuse alone. Bonomi and colleagues (2006) found that longer durations of any type of IPV worsened mental health outcomes, including depression. The severity of IPV was found to have a direct relationship to mental health outcomes in studies of women who have left abusive partners (Black, 2011; Dutton et al., 2006; Ford-Gilboe et al., 2009). Less is known about the relationship between the frequency of emotional abuse and depression.
Perhaps the most extensively researched interpersonal-level mediator between exposure to violence and health outcomes is social support and resources. Studies have indicated that women experiencing IPV tend to have less social support than those not experiencing violence (Katerndahl, Burge, Ferrer, Becho, & Wood, 2013), but that support decreased the likelihood of health problems, especially mental health outcomes (Coker et al., 2002; Goodman, Dutton, Vankos, & Weinfort, 2005; Levendosky et al., 2004). Within the ecological framework, community-level factors that have been found to potentially mediate the relationship between exposure to abuse and depression include social support, economic resources, and housing resources. Ford-Gilboe and colleagues (2009) conducted one of the few studies specifically exploring social and economic resources as a mediator of the relationship between exposure to violence and longer term health outcomes. Although they did not find a specific pathway, their results indicated that social and economic resources had positive effects on both mental and physical health, and also mediated the relationship between IPV and health. They reiterated the need to consider the structural and ecological context in which past abuse may be related to current resources (Ford-Gilboe et al., 2009).
Economic and housing resources have also been examined in the context of IPV, although few studies have specifically linked these factors to mental health consequences. For example, according to a study using a community sample, low-income women who had left a violent situation within 6 months of the study experienced more problems with their credit rating (78%) and had less money than usual (74%), compared with the women who had not been in a violent relationship (58% and 47%, respectively; Eby, 2004). Recent IPV has also been associated with employment instability (Adams, Tolman, Bybee, Sullivan, & Kennedy, 2012; Staggs & Riger, 2005), and women who experienced violence had one third the odds of maintaining employment of at least 30 hr per week for 6 months during the year after the violence as did women who did not experience violence (Browne, Salomon, & Bassuk, 1999). Studies related to IPV and housing have indicated that approximately 25-50% of women who left a violent situation experienced significant difficulties related to housing (Baker, Cooks, & Norris, 2003; Eby, 2004; Gorde, Helfrich, & Finlayson, 2004; Ham-Rowbottom, Gordon, Jarvis, & Novaco, 2005; Ponic et al., 2011).
Although the relationship between exposure to IPV and mental health outcomes has been established, relatively few long-term longitudinal studies of mental health outcomes exist for victims who have left the abusive relationship. Furthermore, little information is available regarding how the context of women’s lives affects the relationship between abuse and long-term mental health after leaving the abuse. The impact of depression on overall functioning may be worsened by other ecological stressors, such as poverty and lack of social and material resources (Mechanic et al., 2008), but relatively little is known about the pathways that lead from IPV to adverse health outcomes (Dutton et al., 2006). In particular, more research is needed to understand “how varied abuse experiences cause health problems, who recovers from these problems, who is most at-risk for sustained poor health, and how the conditions of women’s lives impact outcomes over time” (Ford-Gilboe et al., 2009, p. 1).
The purpose of this pilot study was to explore the contextual relationships between the type and frequency of IPV, community resources and conditions (including transportation, housing, employment, and social support), and the long-term emotional health of women who have left violent situations.
Method
Procedures
Data were collected as part of an ongoing evaluation for a community-based collaborative program that provided concurrent legal and case management services to survivors of IPV and their children. The goal of the program, which began in 1995, was to stabilize their life situations and ultimately reduce further injury to survivors by preventing returns to the violent situation through increasing clients’ knowledge and access to resources. Through the program, families received free legal services and assistance from case managers in managing their unique situational issues. Case managers assisted families in areas such as employment, health, and child care. Attorneys and case managers communicated regularly about each program client to provide the most appropriate and comprehensive services for each situation. Women and men were eligible for this program if they were low income (up to 125% of the federal poverty level); had left an IPV situation and were seeking legal services; resided in Hillsborough County, Florida; and had at least one dependent child or were pregnant. The program followed clients for an average of 2 years after leaving the violent situation.
Sample
This pilot study uses data collected from the community-based collaborative IPV intervention program described above. The individuals in this analysis participated in the program between 2002 and 2009. The sample consists of 156 female clients who completed both a pre-test survey and post-test survey. While the program was available to both men and women, only one male participant completed a pre-test and post-test survey in the time frame utilized for the study and, therefore, was excluded.
Measures
Data collection measures for the independent and dependent variables are summarized in Table 1. Data were collected through a written pre- and post-test survey using the Global History Questionnaire (GHQ). The GHQ is an evaluation instrument that was specifically designed for use in the collaborative program (see Table 1). Clients complete the GHQ at three time points: upon entrance to the program, after approximately 6 months of services, and when they exit the program. The GHQ measures client outcomes in multiple areas of life stability, including employment/finances, education, transportation, housing, child care, children’s school, child health, client health, and safety.
Topic Areas, Questions, and Question Type for All Variables.

Note. GHQ = Global History Questionnaire.
The outcome of interest in this study was self-reported current depression measured at final post-test. Independent variables were assessed in the areas of violence exposure, employment/finances, transportation, housing, health care, social support, and safety. All of the variables examined in this study were derived from the post-test survey, unless they were measured only at pre-test. Items measured only at pre-test include all of the violence variables, the length of time in the relationship with the abuser, and the length of time spent away from the abuser.
Variables that were collected initially on a 5-point Likert-type scale were recoded into dichotomous variables for analysis. In all cases, the responses of not at all and very little were recoded into no, and the responses of somewhat, quite a bit, and very much were recoded into yes.
Variables related to frequency of violence were analyzed by individual type (emotional, physical, verbal) at each of three time frames: once in the past year, once per month, and once per week. Violence variables were also combined into aggregate variables to examine the influence of type of abuse, regardless of frequency, on depression. An overall violence variable was also created, consisting of all frequencies (year, month, week) of all of the types of violence (emotional, physical, sexual). Bivariate analyses revealed that most women had been experiencing regular, ongoing violence and, as a result, only the most frequent form of each violence type (i.e., once per week over the past year) is reported here.
Continuous variables were recoded into categories for analysis. Scatter plots were used to determine the overall distribution of each variable, and categories were created to preserve shape based on these findings. Variables recoded in this way include the length of time the client lived with the abuser (divided into 3-year intervals), the length of time the client was away from the abuser (divided into 6-month intervals), and the number of children in the family (1-2, 3-4, 5 or more).
Analysis
Frequency analysis was performed to describe the sample. Bivariate correlations were used to examine the relationship between each of the independent variables and depression.
Variables that produced significant correlations in the bivariate analyses were entered as predictors into the logistic regression model designed to explore predictors of self-reports of current depression. Variables were tested for multicollinearity prior to the fitting of the regression model. Variables were block-loaded into the regression model. Due to the exploratory nature of the regression analysis, model outcomes were reviewed for significance and goodness of fit. All analyses were conducted using SPSS Version 17.0.
This study was approved by the institutional review board at the University of South Florida.
Results
Sample Characteristics
A total of 156 respondents who completed both a pre-test and post-test survey were included in the analysis. All respondents were female. Table 2 presents the other demographic characteristics of the sample at pre-test.
Sample Characteristics.

Distribution of Influential Factors and Bivariate Correlations: Factors Affecting Depression Outcomes
Table 3 examines the distribution of the factors hypothesized to have an influence on depression in three subgroups: all respondents (n = 156), respondents who reported experiencing depression at post-test (n = 34), and respondents who reported not experiencing depression at post-test (n = 122). Pearson correlations for each factor with self-reported depression at post-test are also reported for the entire sample. These correlations indicate that depression was significantly associated with having experienced frequent emotional abuse, worry that the abuser would contact the victim, and variables in all other domains except demographics.
Distribution of Influential Factors and Bivariate Correlations: Factors Affecting Depression Outcomes.
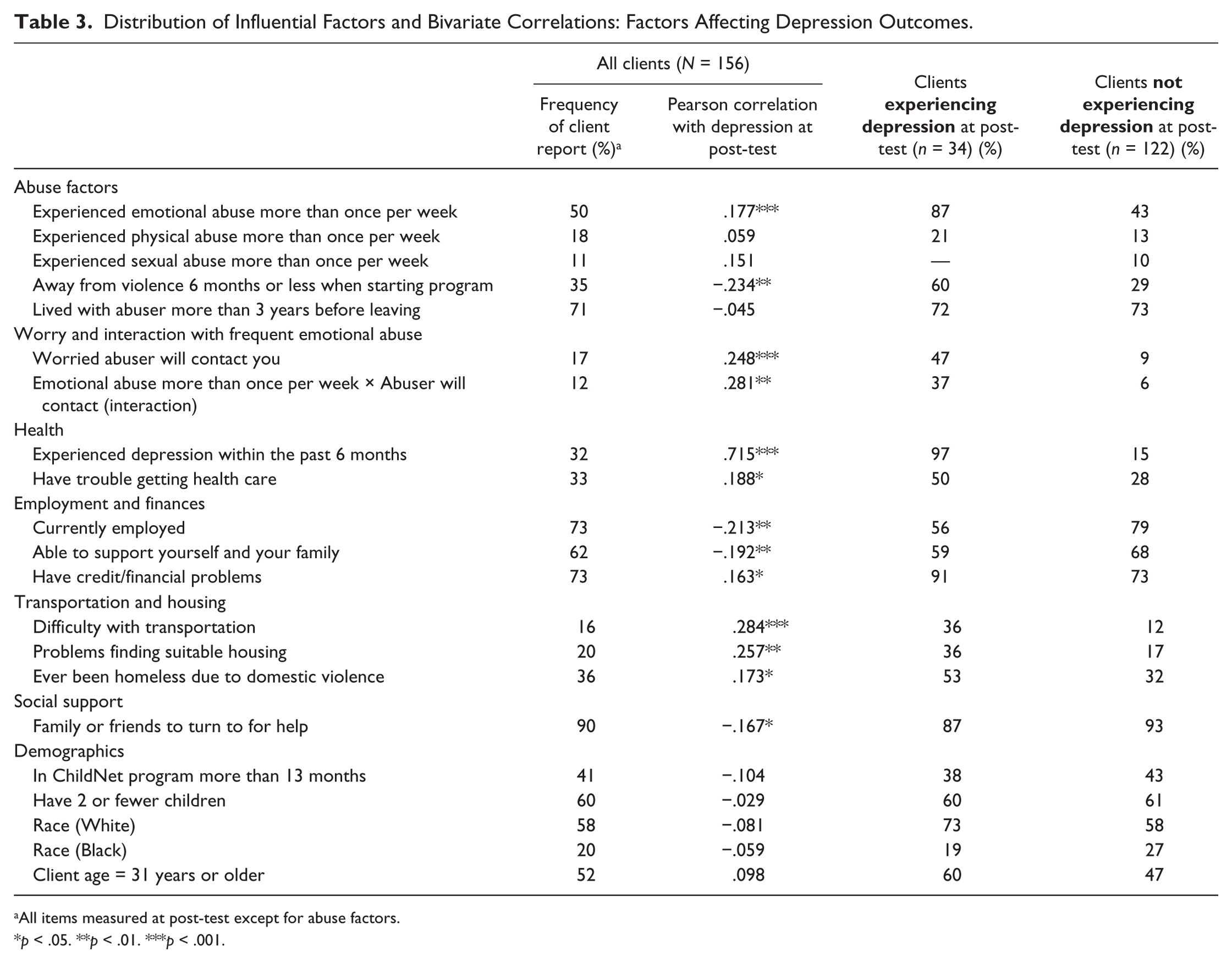
All items measured at post-test except for abuse factors.
p < .05. **p < .01. ***p < .001.
Logistic Regression
The logistic regression model indicated that frequent emotional abuse, worry that the abuser would contact victim, and current employment were significant predictive factors for self-reported depression (see Table 4). Respondents who had experienced emotional abuse more than once per week prior to entrance in the program were almost 5 times more likely to self-report current depression; those who were worried about contact by the abuser were approximately 6 times more likely to self-report current depression; and those who were currently employed were 75% less likely to report current depression. The Nagelkerke R2 = .468. The Hosmer and Lemeshow Test was not significant, indicating good model fit.
Logistic Regression Results (n = 107).
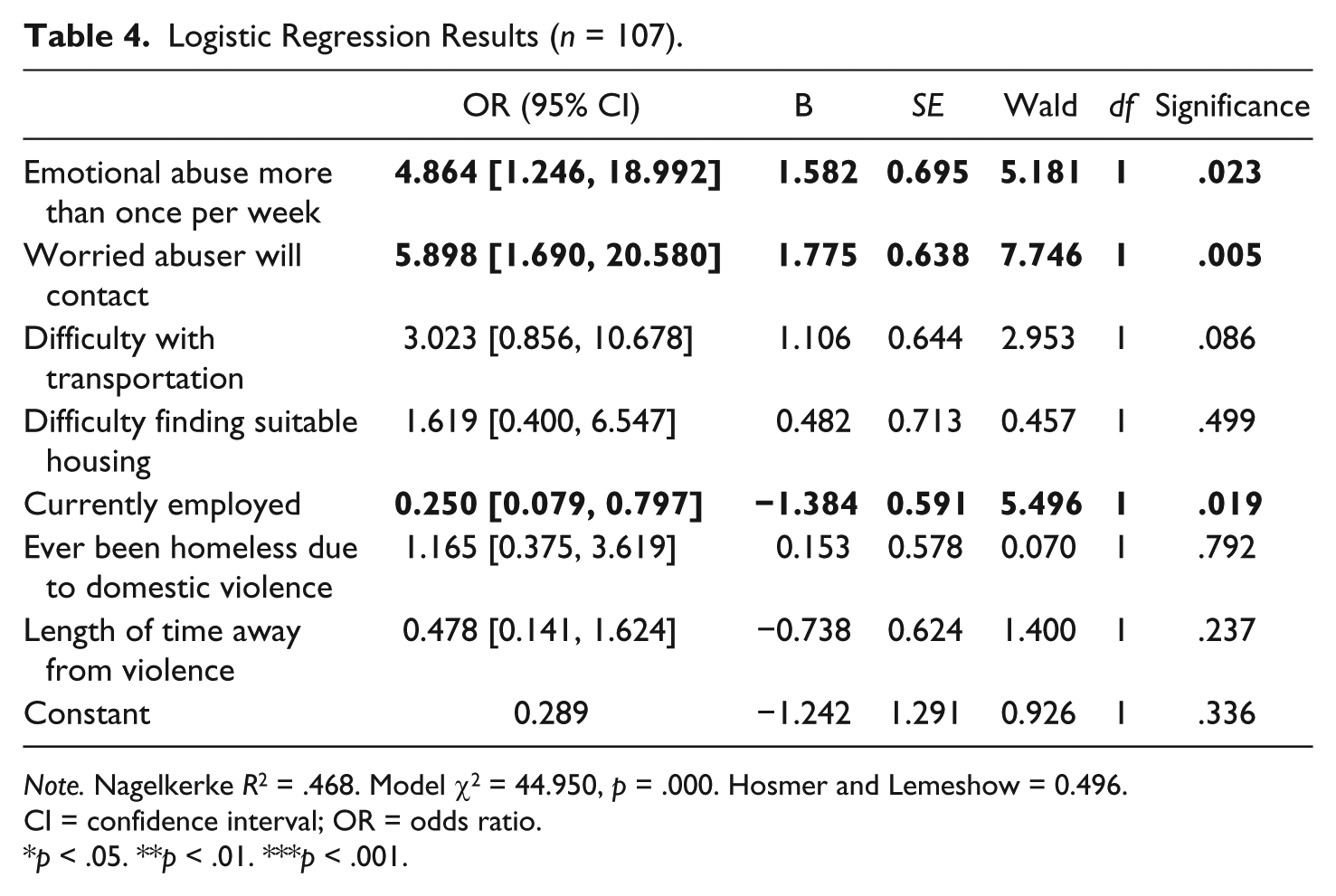
Note. Nagelkerke R2 = .468. Model χ2 = 44.950, p = .000. Hosmer and Lemeshow = 0.496. CI = confidence interval; OR = odds ratio.
p < .05. **p < .01. ***p < .001.
Although the interaction between frequent emotional abuse and worry that the abuser would contact the victim had additive effects in the bivariate analysis over either variable alone, the regression model presented here (without the interaction) explained slightly more of the variance (46.8%) than the interaction model (45.6%), which was run but not presented.
Discussion
The purpose of this pilot study was to examine long-term depression in victims of IPV in relationship to a contextual, ecological set of factors. Frequency analyses revealed that self-reported depression decreased over time for this sample, but an important portion of respondents (22%) continued to self-report problems with depression at the end of the program, and that population is the focus of this analysis. Factors in almost all domains that were examined—including type and frequency of abuse, health, finances, housing, transportation, and social support—were significantly associated with depression in the bivariate analysis. However, the results of the regression model indicate a strikingly persistent relationship between frequent emotional abuse in the past and self-report of long-term depression in victims of IPV. Furthermore, emotional abuse is the only form of abuse that shows these effects, indicating that it may be the most critical form of violence to consider when studying and intervening in the long-term mental health of victims. Additive effects are also present when worry that the abuser would contact the respondent is considered.
These results are interesting in light of the ecological nature of this study. Studies have indicated that women who have left abusive relationships struggle with a variety of stressors, including employment, child care, housing, and social support (Bell, Goodman, & Dutton, 2009; Ford-Gilboe et al., 2009). However, the most predictive factors for self-reported depression in this study were those related to the abuse itself (i.e., frequent emotional abuse and worry about contact by the abuser). This important long-term impact of frequent emotional abuse on mental health is consistent with other recent studies that suggest that psychological violence may be the most detrimental form of violence to the mental health of victims (Hill et al., 2009).
Given the results, the relationships among emotional abuse, fear, and depression in this study are critical to examine. Victims of IPV may be more likely to be able to assess their likelihood of re-abuse, which may then contribute to poorer mental health outcomes. For example, Bennett Cattaneo, Bell, Goodman, and Dutton (2007) found that IPV victims were able to accurately assess their risk of re-abuse in approximately 66% of cases. The authors found that post-traumatic stress disorder scores were highest for women who correctly predicted that they would be re-abused, and those who experienced higher levels of stalking by the batterer were also more likely to correctly assess that they would be re-abused. It may be that increased emotional abuse and fear of contact by the abuser may be more common in victims who believe that they will be re-abused, leading to increased rates of depression.
Authors have also suggested the importance of intuition in the relationship between violence, fear, and re-abuse. DeBecker (1997) compiled a list of pre-incident indicators that were associated with IPV and murder, and the most important indicator was whether a victim had intuitive feelings that she was at risk for repeated violence. Furthermore, verbal abuse and using threats and intimidation as a means of control or abuse were also listed as indicators. While our study did not directly measure stalking behaviors, it may be that the worry and fear about contact by the abuser reported in this study is related to stalking. The National Violence Against Women Survey (NVAWS) has indicated that there are significant mental health consequences that result from stalking, including depression, anxiety, insomnia, and social dysfunction (Tjaden & Thoennes, 1998). Partners who stalked their intimate partners are more likely to have engaged in controlling or emotionally abusive behaviors in the relationship (Mechanic, Weaver, & Resick, 2000; Melton, 2007; Tjaden & Thoennes, 1998). More than half (57%) of the sample in the current study reported emotional abuse more than once per week, and these women were also the most likely to self-report experiencing depression. Taken together, the results of this study and previous work suggest that women who experienced the most frequent emotional abuse may be more likely to be stalked by their abusers, to intuitively feel that this will happen and worry about contact by the abuser, and to subsequently experience more depression. Additional research specifically related to stalking is necessary to confirm this interpretation.
The context of the relationship between the victim and the abuser, as well as the victim’s life circumstances, should also be taken into consideration. The impact of this context on the victim’s mental health may be particularly problematic for women who have custody arrangements with the abusive ex-partner and who must continue to stay in contact even after the relationship has ended. In this study, all respondents had at least one child. Although the number of children was not significantly associated with self-reported depression outcomes, it is likely that the custody and visitation arrangements were necessary for the majority of respondents. Thus, the women must remain in contact with the abusive partners, whether or not they choose to do so. Some victims have no choice about continued contact with the abuser; for example, they may be required by the court to share decision making about the children, or they may be required to see the abuser at times of visitation with the children (Davies, 2009). Many women with supervised child contact in cases of IPV continue to experience violence after leaving the abusive situation, and the knowledge of what the abuser is capable of, including psychological abuse, has resulted in some women fearing for their lives (Harrison, 2008). If the respondent was worried about continuing abuse or stalking, required contact without control over that contact may heighten the fear, and thus lead to increased levels of self-reported depression. More research is needed to understand this specific relationship.
In addition to any continuing relationship with the abuser, the context of the victim’s life must also be taken into consideration. Wuest, Ford-Gilboe, Merritr-Gray, and Berman (2003) cited other undesirable changes in living situations and patters after leaving the abusive situation, including financial losses, employment patterns, the need for relocation, loss of material goods, and social isolation that may be related to lack of control in the time after leaving abuse. The result of this study confirms their hypothesis that lack of community resources, especially access to employment, significantly contributes a unique factor to understanding depression in victims of IPV, as respondents who were employed were 75% less likely to self-report depression than those who were not employed. This is particularly important for victims with low incomes, such as those in this study, as they often already have extremely limited access to resources due to their financial situations.
Limitations
There are several limitations to this study. First, the study utilized data from a community program serving low-income victims of violence, and no control group was available. While the total number of cases entered into the logistic regression model was small, it meets the generally accepted rule of 10 cases per predictor variable (Peduzzi, Concato, Fenstein, & Holford, 1995). It may be that the findings in this study are only relevant to other groups of low-income women who have left violent situations and are receiving similar case management services. However, low-income women are at heightened risk of experiencing multiple challenges after leaving a violent relationship, making this subpopulation important for study. For example, access to transportation and affordable housing can be particularly difficult for this population, which further aggravates the effects of past violence on long-term health, especially mental health. Thus, it is necessary to understand the critical impacts on their mental health, to assure that women can function successfully after leaving and to provide appropriate supports. Additional research is needed to continue to explore the impact of ecological factors on the relationship between emotional abuse and depression.
Another limitation is that the questions were all derived from the program evaluation instrument answered by the clients. There was no diagnostic psychological instrument available, as this pilot study was limited to the data that were being collected from the program evaluation instrument, and psychometric properties of the instrument were not available. Items were measured using one question (e.g., “are you currently experiencing depression?”), which provides an overall estimate of the client’s perception of their own health. The same is true for measures of violence (e.g., “have you experienced emotional abuse more than once per week in the past year?”). Although a diagnostic instrument was not used, subjective self-report of well-being has been shown to be linked to clinical outcomes (Ried, Tueth, Handberg, & Nyanth, 2006), and self-report of psychological abuse has been found to be underreported compared with a clinical instrument (Kelly et al., 2009). Thus, the estimates in the present study may be conservative. In addition, participants’ perceptions of being depressed affects their quality of life, regardless of diagnostic outcome. Future research using diagnostic instruments is necessary.
Future Implications
The results from this study indicate the need to employ a holistic approach to studying and designing interventions to promote the long-term mental health of women who have left violent relationships. It is clear that frequent emotional abuse and worry about contact by the abuser are important predictors of long-term mental health. Much of the work on the health-related consequences of IPV considers physical or sexual abuse rather than emotional abuse, perhaps because the conceptual and operational boundaries of emotional and psychological abuse are less clear (Carbone-Lopez et al., 2006). However, prior emotional abuse has persistent effects on the long-term mental health of IPV victims even after leaving the abusive situation, and it may be more detrimental to mental health than other forms of violence. It is necessary for future research and intervention to continue in this area. As employment was identified as a predictor of depression, further policy attention is also needed to address the area of employment, especially for low-income women who may have limited opportunities. Intensive social support efforts at the community level may also be needed for this population to mitigate the effects of depression (VandeWeerd et al., 2011).
Historically, there has been relatively little program and policy attention to the mental health needs of IPV survivors. IPV advocates and programs have been reluctant to address mental health needs for several reasons, including concerns about placing victims in increased jeopardy due to mental health diagnosis and treatment as well as the lack of training of providers and volunteers around mental health issues. In addition, resources are scarce and thus are most often targeted toward the critical concerns of safety and the practical needs of victims (Moracco et al., 2004; Warshaw, Gugenheim, Moroney, & Barnes, 2003). Similarly, mental health providers have also faced barriers to providing services to victims of IPV, including lack of training regarding the dynamics of family violence, lack of knowledge about community resources, and limited funding, both through public mental health services as well as private health insurance limitations on trauma-related services (Warshaw et al., 2003). Given these barriers, collaboration between IPV and mental health providers has been relatively slow to develop; however, in recent years, collaborative community programs have become increasingly prevalent. To best serve this population in increasingly difficult funding circumstances, community agencies and practitioners should continue to focus on increasing collaborative efforts.
Despite increased attention to the mental health needs of IPV victims in general and increased collaboration between IPV and mental health providers, specific policy attention to the mental health consequences of emotional abuse is needed. Emotional abuse may be associated with a different set of experiences, including specific issues related to control, that translate to worry about contact by the abuser and potential stalking of the victim even after the relationship has ended. These experiences are related to the ongoing mental health of IPV survivors and must be addressed at the program and policy level. However, because little research addresses the unique contribution of emotional abuse to the long-term mental health of victims, correspondingly little program and policy attention has been given to its unique effects. Research and policy both need to devote additional attention to the unique effects of emotional abuse, as well as to how those effects can influence mental health outcomes and the ability for victims to re-establish stability in their lives.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.