
Abstract
Using a nationally representative sample of 10,171 women, this study examines the association between current and previous intimate partner violence and current health status. Current physical or sexual violence was associated with the highest likelihood of reporting health outcomes, followed by current emotional or economic abuse. Current controlling behavior increased the odds of reporting poor health whereas previous controlling behavior has less effect on current health. Controlling behavior alone often is the first expression of mistreatment. If health professionals could identify violence at this early stage, long-term effects on women’s health could be minimized. The implications for health of the cumulative effects of violence and of its timing are discussed.
Keywords
Introduction
Intimate partner violence (IPV) against women is a major public health and human rights issue (World Health Organization [WHO], 2013). Research has demonstrated the high prevalence of violence against women globally and its adverse physical and mental health outcomes, including depression, anxiety, posttraumatic stress disorder, and suicidal thoughts (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; J. C. Campbell, 2002; Coker et al., 2002; Plichta, 2004) in both the short and long term (Bonomi, Anderson, Rivara, & Thompson, 2009; Bott, Guedes, Goodwin, & Mendoza, 2012; J. C. Campbell, García-Moreno, & Sharps, 2004; Ellsberg et al., 2008; García-Moreno, Jansen, Ellsberg, Heise, & Watts, 2005; Martínez, García-Linares, & Pico-Alfonso, 2004; Vives-Cases, Ruiz-Cantero, Escribà-Agüir, & Miralles, 2011). This type of violence includes a variety of strategies an abuser uses over time to coercively control a current or former intimate partner; such strategies include physical, sexual, or psychological abuse.
Over the last two decades, the number of studies that describe the effects of IPV on women’s health has increased significantly. Studies have primarily focused on physical and sexual violence although some studies have addressed psychological violence (Arias & Pape, 1999; Blasco-Ros, Sánchez-Lorente, & Martínez, 2010; Coker et al., 2002; Follingstad, 2009; Jordan, Campbell, & Follingstad, 2010; Katz & Arias, 1999; Lawrence, Yoon, Langer, & Ro, 2009; O’leary, 1999; Pico-Alfonso, 2005; Pico-Alfonso et al., 2006; Ruiz-Pérez & Plazaola-Castaño, 2005; Taft et al., 2006; Tiwari et al., 2008; Tjaden & Thoennes, 1998). These studies have identified evidence of the potentially devastating effects of psychological victimization on women’s health. However, differences in psychological victimization have received less attention, and research in this area is necessary. The relative scarcity of research in this area may be in part because of problems in conceptualizing, defining, and measuring psychological abuse because this type of abuse is the most difficult to validly and reliably define (Follingstad, 2007). Thus, the research on psychological abuse has largely focused on the complexities of psychometric measurement rather than on understanding the effects of psychological abuse on mental health outcomes (Jordan et al., 2010; Maiuro, 2001; Mechanic, Weaver, & Resick, 2008). Many forms of psychological victimization have been described in the literature (Aguilar & Nightingale, 1994; Follingstad, Rutledge, Berg, Hause, & Polek, 1990; Maiuro, 2001); however, because of an absence of consensus on defining and labeling different types of psychological mistreatment, findings have not been integrated (Katz & Arias, 1999). Tolman (1989) proposed two types of psychological abuse: dominance/isolation abuse that included items related to a partner’s demands for compliance/subservience, isolation from personal and social sources, and observance of traditional gender roles; emotional/verbal abuse that included items related to a partner’s devaluing, humiliation, and withholding of emotional support/affection. More recently, Stark (2007) developed the concept of coercive control, a pattern of behavior that seeks to remove the victim’s freedom. Coercive control may be defined as an ongoing pattern of domination in which abusive male partners primarily intertwine repeated physical and sexual violence with intimidation, sexual degradation, isolation, and control (Stark, 2012). This model is not intended to minimize the level or scope of physical or sexual violence that can occur in IPV, but to highlight what is significant: control. Coercive control is the most widespread and devastating strategy men use to dominate women in personal life (Stark, 2007). Coercive control is perceived to be a holistic approach to understanding the roots of violence. Conversely, in an attempt to standardize the measuring of IPV, the United Nations Statistics Division (2014) developed the Guidelines for Producing Statistics on Violence Against Women, which propose the following classifications of IPV: physical violence, sexual violence, economic violence, emotional abuse, and controlling behavior. For the purposes of the present research, the classifications proposed by the Guidelines for Producing Statistics on Violence Against Women (United Nations Statistics Division, 2014) have been followed.
In addition to the type of violence, the timing of violence should also be considered when assessing the effects of IPV on health. In general, previous studies reported an improvement in mental health status over time (R. Campbell, Sullivan, & Davidson, 1995; Johnson & Zlotnick, 2009; Mertin & Mohr, 2001), suggesting that women experiencing recent IPV have poorer health than women with a more remote IPV history (Brokaw et al., 2002; McNutt, Carlson, Persaud, & Postmus, 2002). Other studies have observed that symptoms continue despite the absence of recent re-victimization (Anderson, Saunders, Yoshihama, Bybee, & Sullivan, 2003; J. C. Campbell, Kub, Belknap, & Templin, 1997; J. C. Campbell & Soeken, 1999).
IPV is a complex phenomenon, and all types of IPV, as well as their timing, should be considered when assessing the relation between IPV and women’s health status. Moreover, research has shown that women who have experienced IPV are more likely than non-abused women to seek health care even if the victims do not disclose the violence (Ansara & Hindin, 2010; Black, 2011; J. C. Campbell, 2002; Sprague et al., 2014; WHO, 2013). Thus, although health care providers can play a vital role in detecting IPV (Davidson et al., 2001), identification is not always easy. As Stark (2012) noted, most tactics used in coercive control are rarely identified with abuse or targeted for intervention. Health care providers who encounter women facing any type of violence must be able to recognize signs of IPV.
The primary objective of this study was to clarify the effects of various IPV categories and their timing (past or current) on women’s health, utilizing a large population-based sample. As a secondary objective, we proposed to identify the most relevant symptoms of poor health among the different types of battered women. A symptom is defined as subjective evidence of disease or disturbance observed by a patient. Symptoms are often the catalyst for patients to seek medical care (Gerber, Wittenberg, Ganz, Williams, & McCloskey, 2008).
We hypothesized that women who are currently suffering any type of IPV would be significantly more likely to report the various symptoms of poor health than women who had experienced IPV in the past but not in the 12 months prior to the interviews. We assumed that all categories of violence would follow the same pattern, although to varying degrees. If the effect on health of the various types of victimization differed, and the sequelae once the violence had ceased varied according to the type of victimization, an early identification and intervention could lead to a reduction in the long-term effects on the health of the affected women.
More specifically, we hypothesized that controlling behavior without associated violence, frequently one of the first signals of mistreatment in a relationship, would affect women’s health while the violence was occurring; however, the behavior would not leave lasting effects once the violence ceased. Thus, an early identification of violence and a prompt and adequate intervention would be crucial in preventing long-term consequences to women’s health.
Methods
Participants and Data Collection
Data from the Spanish Survey on Violence Against Women 2015 were used. This survey is a nationally representative, cross-sectional, and dedicated survey of 10,171 women residing in Spain and aged 16 years or above (Ministry of Health, Social Services and Equality, 2015a). Fieldwork was conducted between September and December 2014. Dedicated surveys generally yield higher prevalence rates than a module of questions incorporated into large-scale surveys on broader topics (Ellsberg & Heise, 2005; Walby & Myhill, 2001). The estimates produced by dedicated surveys are considered to be a more accurate reflection of the prevalence of violence.
Data were collected in face-to-face interviews in women’s households by female interviewers who ensured confidentiality and anonymity. Utilizing female interviewers increases the disclosure of sensitive information, particularly information relating to experiences involving sexual victimization and violence perpetrated by male partners (United Nations Office on Drugs and Crime & United Nations Economic Commission for Europe, 2010). Face-to-face interviewing leads to increased disclosures of sensitive experiences (Coker & Stasny, 1995). Cards were used for the most sensitive questions to increase the privacy of the responses. For each sensitive question, the interviewer, instead of reading the question to the interviewed woman, handed her a card containing the text of the question and the various possible answers, numbered. Thus, the women could read the question and tell the interviewer the number of the selected answer, minimizing the woman’s possible discomfort. In those cases in which the woman was unable to read (e.g., illiterate, vision problems) cards were not used, and the interviewer read the questions normally.
Estimates regarding IPV are extremely sensitive to the specific definitions used and to the manner in which the questions are asked. Thus, questions asked about specific behaviors rather than asking about abuse generally (Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002). Previous research has shown that this technique yields more positive answers than questions that inquire about violence in general (Fisher, Cullen, & Turner, 2000; Percy & Mayhew, 1997; Russell, 1982). Moreover, the phrasing of the questions was based on the Guidelines for Producing Statistics on Violence Against Women developed by the United Nations (United Nations Statistics Division, 2014).
Variables
Predictor variables
We characterized IPV by (a) the type of violence (physical, sexual, emotional, economic, and controlling behavior) and (b) the time frame of violence (past: violence suffered but not in the past 12 months, and current: violence within the past 12 months). Past IPV exposure was exclusive of recent IPV exposure. Women were asked whether any intimate partner (spouses, non-marital partners, former marital, or non-marital partners) had abused them:
physically (slapped, pushed, shoved, hit with a fist, kicked, dragged, or beaten them; tried to choke or burn the woman on purpose; used a gun, knife, or other weapon against the woman);
sexually (forced the woman to have sexual intercourse against her will, a woman had sexual intercourse that the woman did not want because of fear of what the partner would do if the woman refused, forced the woman to do something sexual that the woman did not want to do or that the woman deemed degrading or humiliating, attempted to force the woman into sexual intercourse by holding the woman down or hurting the woman in some manner);
emotionally (insulted, belittled, humiliated in front of other people, did things to scare or intimidate the woman on purpose, verbally threatened to hurt the woman or someone the woman cared about);
economically (refused to give the woman sufficient money for household expenses, prevented the woman from making decisions regarding family finances and from shopping independently, forbade the woman from working or studying outside the household),
by controlling behavior (tried to keep the woman from seeing friends, tried to restrict contact with her family of birth, insisted on knowing where the woman was at all times, ignored the woman and treated her indifferently, became angry if the woman spoke with another man or woman, unjustifiably suspected that the woman was unfaithful, and expected the woman to ask for permission before going certain places by herself).
The exact phrasing of the items can be observed in the study of the Ministry of Health, Social Services and Equality (2015a). Data were collected regarding whether a woman had ever experienced these acts and whether the woman had experienced the acts within the past 12 months. A woman was identified as experiencing IPV if she reported yes to any of the acts of violence included in the questions.
Because there is generally considerable collinearity among IPV types, we created three mutually exclusive categories. The first group included respondents ever experiencing physical or sexual violence with or without emotional abuse, economic abuse, or controlling behavior. The second group included women ever experiencing emotional or economic abuse but not physical or sexual violence. The third group included women ever experiencing controlling behavior alone without physical, sexual, emotional, or economic violence. Economic abuse was grouped with emotional abuse because both types performed similarly, and current economic abuse did not generate sufficient cases to be accurately studied on its own (39 cases for current economic abuse without physical, sexual, or emotional abuse).
Control variables
The following variables were included: age (16-34, 35-59, 60+) and educational level (no formal education, primary, lower secondary education, upper secondary education, university).
Based on previous research, other possible confounders were initially considered (social support, country of birth, employment status, income) but not included in the final models to avoid problems with over-adjustment (Jewell, 2004; Schisterman, Cole, & Platt, 2009; Selvin, 2008; Stoltzfus, 2011; Walter & Tiemeier, 2009) because such confounders either were not statistically significant or did not change the estimates by more than 5%.
Outcome variables
Eight symptoms of poor health were measured in addition to a subjective question regarding the woman’s self-perceived state of health. Symptoms were expressed in a manner that allowed respondents to clearly identify symptoms rather than using medical terminology. Respondents were asked whether they had suffered the following symptoms with a certain frequency in the 12 months prior to the interview: (a) anxiety or anguish; (b) sadness because of feelings of worthlessness; (c) wanting to cry for no reason; (d) mood swings; (e) irritability; (f) insomnia, sleep disorders; (g) permanent fatigue; and (h) lack of sexual desire.
The woman’s self-perceived state of health was elicited by asking the respondent to describe her general health in the past 12 months as very good, good, fair, bad, or very bad. The variable was dichotomized by combining the categories good and very good on the one side, and bad and very bad on the other. Those describing a fair health condition were excluded from the logistic analyses.
Statistical Analyses
We calculated the prevalence of different types and categories of IPV by time frame, as shown in Table 1. After descriptive analysis, logistic regression models were fitted for each outcome variable. Odds ratio (OR) was adjusted for potential confounding factors. The reference group for analysis was, in all cases, the group of women that had never experienced any form of IPV. All analyses were conducted using SPSS Version 21.
Prevalence of IPV Among Women Residing in Spain Aged 16 or Above.
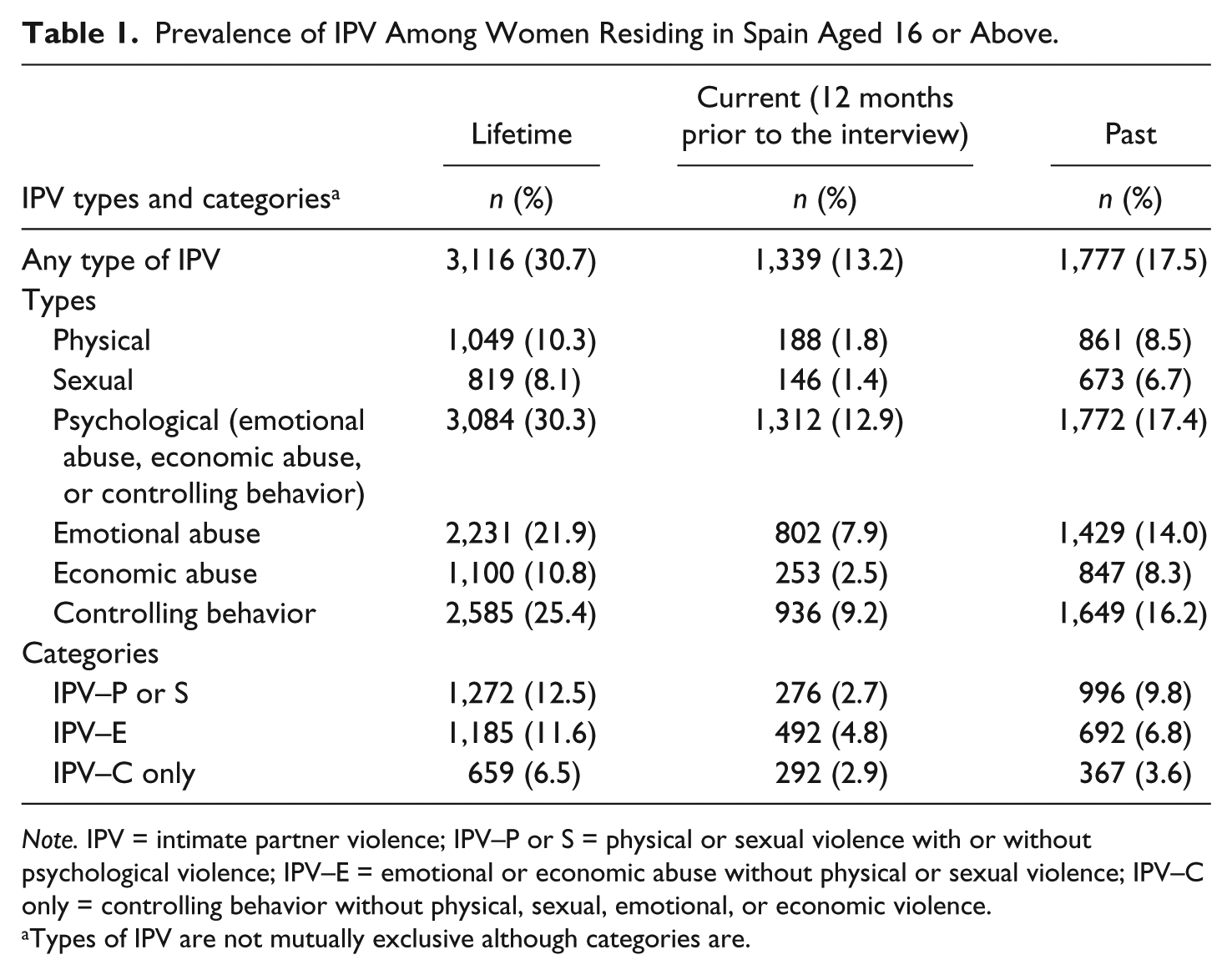
Note. IPV = intimate partner violence; IPV–P or S = physical or sexual violence with or without psychological violence; IPV–E = emotional or economic abuse without physical or sexual violence; IPV–C only = controlling behavior without physical, sexual, emotional, or economic violence.
Types of IPV are not mutually exclusive although categories are.
Results
Table 1 presents the prevalence of IPV by type, category, and time frame. The percentage of women who reported IPV of any type (physical, sexual, emotional, economic, or controlling behavior) during their lives was 30.7%. Of the women, 13.2% reported current IPV of any type, 2.7% reported current physical or sexual IPV, and 4.8% reported current emotional or economic abuse without physical or sexual violence. Of the women, 9.8% had experienced physical or sexual IPV in the past but not in the 12 months prior to the interviews, and 6.8% reported past emotional or economic abuse without physical or sexual violence. Controlling behavior is often strongly correlated with other types of IPV although 2.9% of women experienced controlling behavior without physical, sexual, emotional, or economic violence in the 12 months prior to the interviews.
Table 2 shows the association between different IPV categories and health symptoms; women who were never abused serve as the comparison group for each of the bivariate analyses. Having suffered any of the categories of abuse was significantly associated with all the symptoms. However, no association was observed between past controlling behavior alone and the various symptoms.
Prevalence of Health Symptoms by Category of IPV Violence Among Spanish Women Aged 16 or Above.
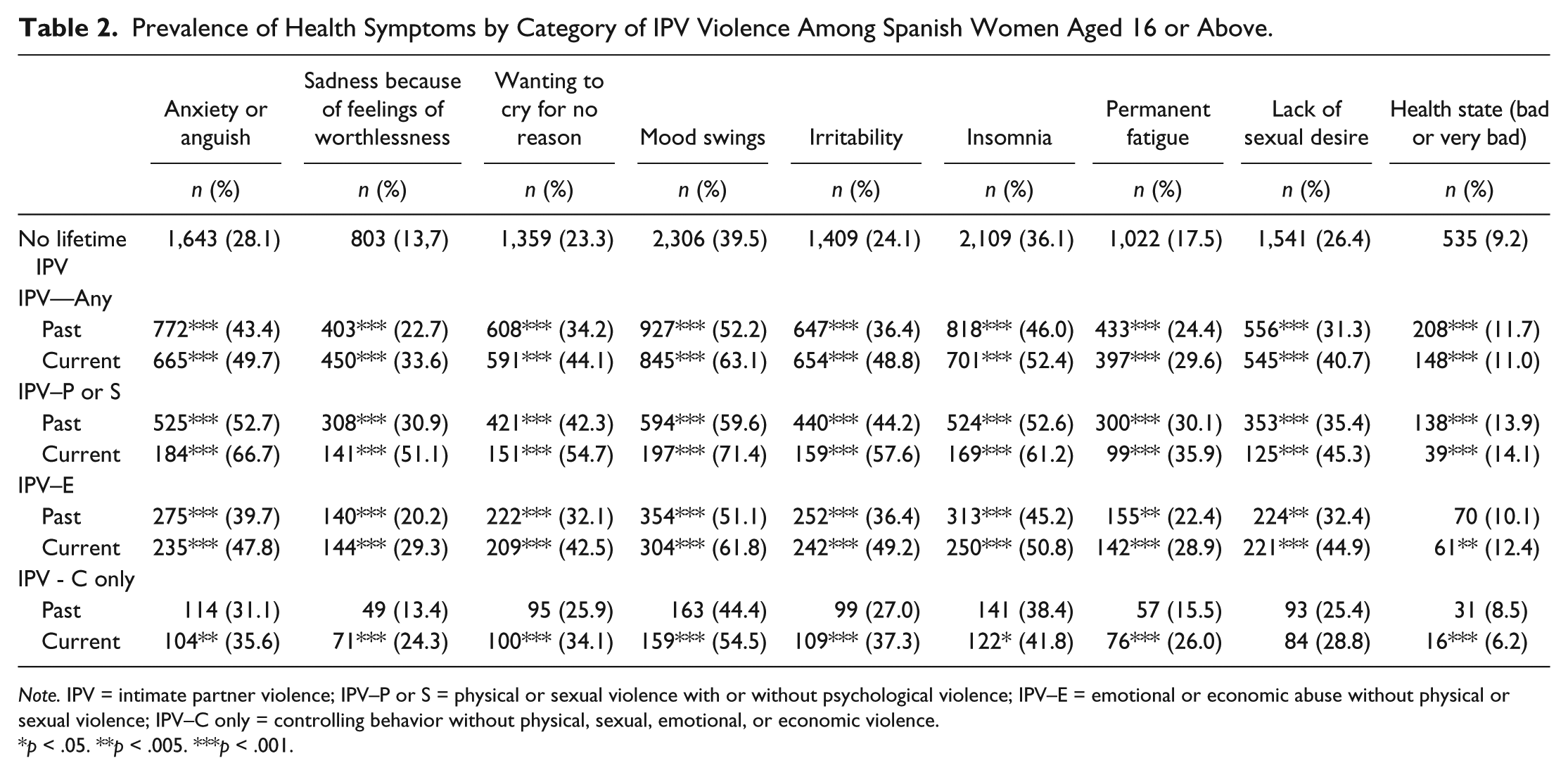
Note. IPV = intimate partner violence; IPV–P or S = physical or sexual violence with or without psychological violence; IPV–E = emotional or economic abuse without physical or sexual violence; IPV–C only = controlling behavior without physical, sexual, emotional, or economic violence.
p < .05. **p < .005. ***p < .001.
The results of the logistic regressions are presented in Table 3. IPV increased the risk of suffering all the health symptoms; however, as hypothesized, we observed that women who currently suffered any type of IPV were significantly more likely to report all the symptoms of poor health than those women who had experienced IPV in the past but not in the 12 months prior to the interviews. All categories of violence followed the same pattern, although to varying degrees.
Logistic Regression Analyses for Poor Health Symptoms in Women Who Reported IPV. a
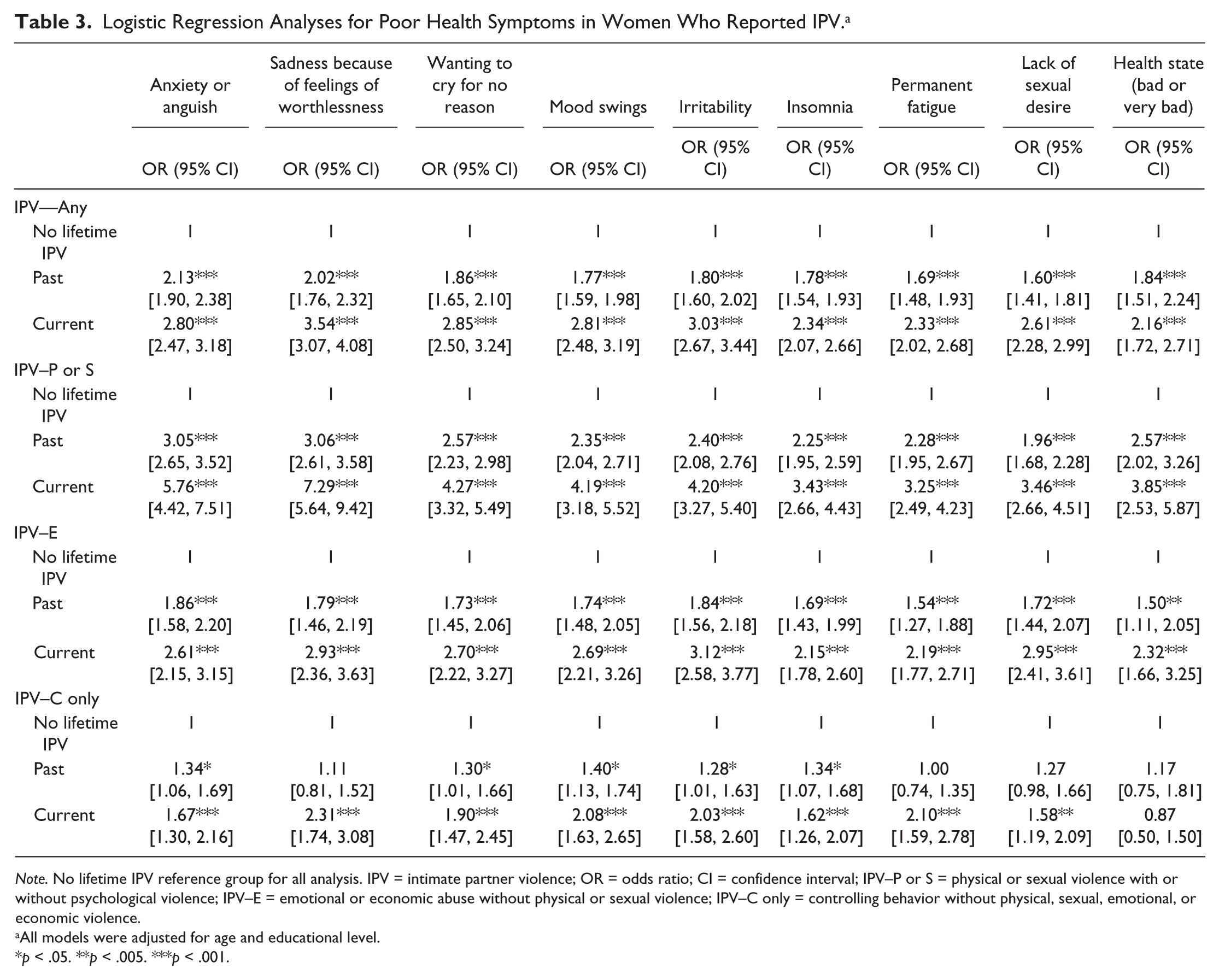
Note. No lifetime IPV reference group for all analysis. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval; IPV–P or S = physical or sexual violence with or without psychological violence; IPV–E = emotional or economic abuse without physical or sexual violence; IPV–C only = controlling behavior without physical, sexual, emotional, or economic violence.
All models were adjusted for age and educational level.
p < .05. **p < .005. ***p < .001.
Past physical or sexual violence increased threefold the likelihood of reporting anxiety (OR = 3.05, [2.65, 3.52]) and sadness because of feelings of worthlessness (OR = 3.06, [2.61, 3.58]), whereas current physical or sexual violence increased nearly sixfold the odds of reporting anxiety (OR = 5.76, [4.42, 7.51]) and by sevenfold the likelihood of sadness because of feelings of worthlessness (OR = 7.29, [5.64, 9.42]).
Physical violence without a sexual component and sexual violence without a physical component were also examined (results not presented); however, there were no significant differences between the two categories with regard to the various health outcomes. We also analyzed data from those women who experienced both physical and sexual violence (results not presented). The odds ratio was higher for all symptoms among those women who experienced physical or sexual violence alone; however, the reduction in the number of cases did not result in statistically significant differences between the odds ratios except in the case of anxiety, whose likelihood was significantly higher among those women reporting both physical and sexual violence than among those women experiencing physical or sexual violence alone.
Women who experienced emotional or economic violence without physical and sexual violence in the past were approximately 1.5 times more likely to report all the symptoms than women reporting no lifetime IPV. For women who were currently experiencing this type of violence, the effect was higher and statistically significant for all the symptoms.
Reporting only controlling behavior in the past slightly increased the likelihood of reporting anxiety, wanting to cry for no reason, mood swings, irritability, and insomnia, whereas women who were currently experiencing controlling behavior not associated with other types of violence were significantly more likely to report all the symptoms than women reporting no lifetime IPV. However, current controlling behavior alone was not associated with a higher risk of reporting poor health. Compared with women who reported controlling behavior in the past, women who were currently experiencing controlling behavior were significantly more likely to report sadness, wanting to cry for no reason, mood swings, irritability, and permanent fatigue.
When comparing the likelihood of the various symptoms in women who reported emotional or economic violence without physical or sexual violence with women who experienced physical or sexual violence, statistically significant differences were observed, both for past and current violence, for all the symptoms except lack of sexual desire. The likelihood of these symptoms was higher among women who reported current or past physical/sexual violence than among women who experienced current or past emotional/economic violence without physical or sexual violence.
The effects on health of current emotional or economic violence without physical or sexual violence were similar to the effects on health of past physical or sexual violence, with no statistically significant differences in the likelihood of reporting any of the symptoms except irritability and the lack of sexual desire. The likelihood of these two symptoms was higher among women who reported current emotional or economic violence (irritability: OR = 3.12, [2.58, 3.77]; lack of sexual desire: OR = 2.95, [2.41, 3.61]) than among women who reported past physical or sexual violence (irritability: OR = 2.40, [2.08, 2.76]; lack of sexual desire: OR = 1.96, [1.68, 2.28]).
Discussion
The results of this study indicate that 30.7% of women residing in Spain aged 16 and above have experienced at least one type of IPV, and 13.2% reported IPV in the 12 months prior to the interview. Of the women, 12.5% aged 16 years or older reported physical or sexual violence by a partner in their lives, 25.4% experienced controlling behavior, 21.9% experienced emotional abuse, and 10.8% experienced economic abuse. Concerning current IPV, 2.7% experienced physical or sexual violence in the 12 months prior to the interviews, 9.2% experienced controlling behavior, 7.9% experienced emotional abuse, and 2.5% experienced economic abuse. Psychological violence is far more prevalent than physical or sexual violence, consistent with the reported prevalence in other studies that analyzed samples of Spanish women (Montero et al., 2011; Ruiz-Pérez et al., 2006). Although research has begun to measure the effects of psychological abuse on a range of outcomes, most studies have studied psychological abuse as a discrete entity without considering its various dimensions. Our study analyzed different categories of psychological violence to measure their effects on women’s health.
Our analysis indicates that women experiencing any type of past or current IPV are more likely to report a greater prevalence of physical and mental symptoms related to poor health than women without an IPV history. These results are consistent with the results of other studies (Coker, Smith, McKeown, & King, 2000; Golding, 1999; Jaffe, Wolfe, Wilson, & Zak, 1986; Mullen, Romans-Clarkson, Walton, & Herbison, 1988; Plichta, 1992; Vives-Cases et al., 2011) and corroborate the theory that IPV victimization is associated with a higher risk of negative mental and physical health outcomes. This study also shows, consistent with previous studies (Anderson, Saunders, Yoshihama, Bybee, & Sullivan, 2003; R. Campbell et al., 1995; Gerber et al., 2008; Johnson & Zlotnick, 2009; Kernic, Holt, Stoner, Wolf, & Rivara, 2003; Mertin & Mohr, 2001), that the timing of violence is crucial; women who reported past but not current IPV exhibited a lower incidence of the various symptoms associated with poor health. Using a large, population-based sample, we were able to provide more disaggregated and accurate results.
Current physical or sexual violence was associated with the greatest likelihood of reporting various symptoms, followed by current emotional or economic abuse and past physical or sexual violence. The only differences that were statistically significant were symptoms of irritability and lack of sexual desire, which were more likely to occur among women currently experiencing emotional or economic abuse than among women who reported past physical or sexual violence.
Anxiety and sadness because of feelings of worthlessness have the greatest odds of being reported among those women who have experienced physical or sexual violence with the likelihood increasing sixfold in women reporting current physical or sexual abuse and threefold in women who experienced this violence in the past. Depression has been shown in previous literature to be one of the most prevalent mental health sequelae of IPV, and anxiety has also been widely detected (Beydoun et al., 2012; J. C. Campbell, 2002; Coker et al., 2002; Jordan et al., 2010; Mechanic et al., 2008; Plichta, 1996).
Some previous literature has suggested that psychological violence may be at least as detrimental to women’s health as physical or sexual violence (Arias & Pape, 1999; Blasco-Ros et al., 2010; Coker et al., 2002; Lawrence et al., 2009). Other authors have noted the importance of considering the cumulative effects of violence, suggesting that a woman who experiences a greater number of abuse categories experiences a greater effect on her health (Anderson et al., 2003; J. C. Campbell & Soeken, 1999; Maiuro, 2001; Ruiz-Pérez, Plazaola-Castaño, & Del Río-Lozano, 2007). Psychological aggression appears to be both an antecedent and a correlate of physical or sexual aggression (Lawrence et al., 2009). Our analysis indicates that although emotional and economic violence without physical or sexual violence strongly affects women’s health even after the violence has ended, this effect is not as strong as the effect of physical or sexual violence. Physical and sexual violence, however, are virtually always accompanied by psychological violence, implying that the effects on health of physical or sexual violence without psychological violence cannot be determined. Thus, our results concerning the stronger health effects of physical or sexual violence are likely because of the cumulative effects of violence on health.
Current controlling behavior by itself significantly increased the odds of reporting various health outcomes, except for the self-perceived health state, whereas previous controlling behavior appeared, from all the studied categories, to have less effect on present health. Controlling behavior without associated violence categories often is the first expression of mistreatment in a relationship. Control sets the stage for violence and injury, and research has shown that women’s vulnerability to physical and sexual abuse is typically a by-product of a previously established pattern of domination that has disabled their capacity to mobilize personal, material, and social resources to resist or escape (Stark, 2012). If health professionals can identify this type of victimization early and conduct a proper intervention, long-term effects on women’s health can be minimized.
The WHO does not recommend universal screening and favors instead enhancing providers’ ability to respond adequately to women who do disclose violence or show signs and symptoms associated with violence (WHO, 2013). The WHO considers that women with mental health symptoms or disorders such as depression, anxiety, posttraumatic stress disorder, or self-harm/suicide attempts should be asked about IPV.
Our results reveal that anxiety and depression are strongly correlated with physical or sexual violence. However, to detect emotional or economic violence that does not co-occur with physical or sexual violence or controlling behavior that does not co-occur with other types of violence, professionals should focus on women who manifest other symptoms of discomfort such as mood swings, crying without reason, irritability, insomnia, or permanent fatigue. Physicians frequently fail to diagnose IPV (Davis, 2008; Sprague et al., 2014), contributing to recidivism and long-term health problems (Glass, Dearwater, & Campbell, 2001). Thus, IPV training for health care professionals should be widespread. A survey among primary care practitioners revealed that training in IPV enhances the detection of victimization situations (Ministry of Health, Social Services and Equality, 2015b). To enhance the detection of all types of abuse, it would help to reframe partner abuse as a pattern or course of conduct and to broaden the scope of identification and intervention (Stark, 2012).
Strengths and Limitations
Our study has noteworthy strengths, including the use of a large, nationally representative sample of women aged 16 years or above; a rigorous methodological design that included the pre-testing of survey instruments, extensive interviewer training and specific training in violence against women; fieldwork conducted exclusively by female interviewers; and the development of a questionnaire based on the Guidelines for Producing Statistics on Violence Against Women developed by the United Nations Statistics Division that included reliable and valid measures of a range of violence. This sound methodology is likely to increase the disclosure of sensitive information and minimize the reporting bias of partner violence. To our knowledge, this study is the first utilizing nationally representative data for Spain fulfilling these quality standards and therefore the first time that IPV and its consequences to women can be accurately measured in Spain.
The use of a large, representative population survey allowed having statistically significant differences between the odds ratio of the various violence categories and accurate results. Likewise, the use of a large sample allowed making a clear distinction between past and current violence to measure health effects. If there is not a clear division between past and current violence, the effects of the IPV typologies could be confused with typologies related to the timing of violence.
Questions regarding health symptoms were asked prior to asking respondents about their experiences with violence. The order of the questions helped ensure that answers to questions regarding health would not be influenced by disclosure of experiences with violence.
However, there are limitations to consider. The cross-sectional design implies that causality cannot be determined. To better measure the IPV effects on health, questions that have been effective in previous research should be included in the next edition of the survey. Such questions would consider the use of tranquilizers, antidepressants or analgesics, suicidal thoughts and attempts, or the search for health care. Furthermore, as previously stated, physical and sexual violence are nearly always accompanied by psychological violence. Therefore, the effects of physical or sexual violence without psychological violence on health could not be determined.
Conclusion
Our findings support and extend the body of research highlighting the effects on women’s health of various forms of current and past IPV. Although a clear improvement in health status was observed among those women who reported IPV in the past compared with women who had experienced IPV within the 12 months prior to the interviews, strong, lasting effects on health were identified in all women who reported past physical, sexual, emotional, or economic abuse. Our primary contribution is that controlling behavior appeared to be the only category of violence that, although having negative effects on women’s health while being experienced, did not leave significant lasting effects once that type of violence was over. This finding has important implications for intervention because controlling behavior without other categories of associated violence often is the first expression of a violent relationship. If violence could be identified at this early stage, long-term effects on women’s health could be minimized. Thus, health care professionals should be adequately trained to recognize not only the symptomatology associated with physical or sexual violence (primarily high levels of anxiety and depression) but also signals of discomfort that could be caused by this type of abuse. The scope of identification and intervention must be broadened.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.