
Abstract
Using survey data, we investigate perspectives of 80 program directors of domestic violence and/or sexual assault agencies regarding whether gathering specific information at intake is helpful in determining survivors’ needs for five service areas: legal advocacy, medical advocacy, support group, counseling, and shelter. We explore whether directors’ opinions of information-type usefulness differ by type of service agency (single- or dual-focus). Findings show directors perceive the information most helpful to early service provision includes survivors’ goals, experiences of violence and trauma, and health status. MANOVA results show no significant differences among directors from single- or dual-focus agencies.
Violence against women is a growing public health concern in the United States. Approximately 5 million incidents of intimate partner abuse against women occur annually (Tjaden & Thoennes, 2000) and about one in every six women will experience the trauma of rape at some point in her life (Tjaden & Thoennes, 2006). Research has established that the lives of most survivors of domestic violence and sexual assault are profoundly affected by the negative physical and mental aftermath of violence (Campbell, 2002; Golding, 1999; Koss et al., 1994; Plichta, 2004; Polusny & Arbisi, 2006; Robertiello, 2006). Survivors disproportionately report physical and mental health problems such as sleep disturbances, chronic pain, suicidal ideation, anxiety, posttraumatic stress disorder, depression, and low self-esteem (Kass-Bartelmes, 2004; Koss et al., 1994; Polusny & Arbisi, 2006; Robertiello, 2006). However, survivors’ experiences of violence are not limited to physical and mental health problems. They also experience financial, social, and family impairments both directly and indirectly related to their experience of violence (Briere & Jordan, 2004; Sarkar & Sarkar, 2005). To address these various needs, including efforts to secure safety, many survivors of partner abuse and sexual violence seek help from the domestic violence and sexual assault agencies in their communities (Hutchison & Hirschel, 1998; Ingram, 2007; Macy, Nurius, Kernic, & Holt, 2005). In turn, these agencies are faced with the difficult task of assessing a survivor’s most urgent needs, tailoring a plan of short- and long-term services to meet those needs, and determining needs and service plans when the survivor is suffering the aftermath of crisis.
Survivors’ Diverse Needs and Goals
Although research has established the wide array of negative sequelae to violence, most survivors of domestic violence and sexual assault do not experience all possible consequences of their victimization. Rather, the harm experienced by survivors varies as a function of survivor-specific factors (e.g., coping skills, appraisal of the abusive event, previous psychological functioning), trauma-related factors (e.g., frequency and severity of the abuse, life threat, injury), and sociocultural factors (e.g., social support, cultural norms around violence; Briere & Jordan, 2004). Survivors who have been exposed to comparable levels of violence might experience substantially different problems given the influences of other biopsychosocial factors (e.g., physical health, mental health, social support; Nurius & Macy, 2010). Therefore, in terms of their recovery needs, survivors should be considered as a heterogeneous group.
Given the likelihood of variable post-victimization experiences, survivors warrant individualized, tailored interventions. A growing body of research has suggested that interventions adapted to meet the experiences and presenting concerns of survivors are more effective than universal interventions (Briere & Jordan, 2004; Dutton, 2004; Nurius & Macy, 2010). Consistent with tailoring interventions, the domestic violence and sexual assault services literature also emphasizes developing tailored, individualized service plans for survivors (Macy, Giattina, Sangster, Crosby, & Montijo, 2009). To develop and deliver these tailored interventions, service providers must adequately assess survivors’ needs and goals. Unfortunately, research has suggested that typical assessment practices are inadequate to thoroughly appraise survivors’ complex situation (Gondolf, 1998; Lindhorst, Nurius, & Macy, 2005). Without a comprehensive assessment of survivors’ situations, service providers will face increased difficulty in trying to develop and implement helpful advocacy, safety, and service plans.
Domestic Violence and Sexual Assault Service Assessment Recommendations
Although limited, the literature has provided some general recommendations for assessment of those who have survived a violent event. Consistent with these recommendations, intake assessments should explore the survivor’s history of violence, the consequences of those events, and the survivor’s future orientation and needs (Briere & Jordan, 2004; Fitzgerald, McCart, & Kilpatrick, 2009; Gondolf, 1998; Jackson, Petretic-Jackson, & Witte, 2002; Lee, 2007; Polusny & Arbisi, 2006; Roberts, 2007; Rolling & Brosi, 2010). The literature has also recommended that assessments should address survivors’ histories with interventions and survivors’ substance use and mental health status (Briere & Jordan, 2004; Fitzgerald et al., 2009; Jackson et al., 2002; McCart, Fitzgerald, Acierno, Resnick, & Kilpatrick, 2009; McCloskey & Grigsby, 2005; Polusny & Arbisi, 2006). Assessments should include questions that explore the nature of the violent or traumatic event (e.g., severity, frequency, degree of life threat), personal variables (e.g., relationship to the offender, meaning assigned to the event), and environmental variables (e.g., culture, community attitudes or values, setting of the abuse) related to the violence (Petrak, 1996).
Moreover, the literature has recommended assessments to encompass the full range of possible consequences of the violence or traumatic event (Briere & Jordan, 2004; Lindhorst et al., 2005; Roberts, 2007). Of the potential consequences, assessments should give priority to potential lethality (i.e., homicidality and suicidality) and safety (Boes & McDermott, 2002; Fitzgerald et al., 2009; Gondolf, 1998; Lee, 2007; McCart et al., 2009; McCloskey & Grigsby, 2005; Rolling & Brosi, 2010). A thorough assessment should also examine each survivor’s levels of strengths and resources (Boes & McDermott, 2002; Gondolf & Browne, 1998; Lindhorst et al., 2005; McCart et al., 2009; Roberts, 2007; Rolling & Brosi, 2010), specifically coping skills, shelter, transportation, social support, spirituality or religion, and self-esteem (Gondolf & Browne, 1998; Rolling & Brosi, 2010). Last, the literature has recommended that as part of the assessment process, service providers should ask survivors to describe their own goals and plans (Boes & McDermott, 2002; Jackson et al., 2002; Lee, 2007).
Providers’ Perspectives: The Missing Piece
Despite the important benefits of providing comprehensive assessment for violence survivors, the literature is notable for its dearth of empirical research on domestic violence and sexual assault assessment practices in community-based services (Petrak, 1996). In addition, little research has been conducted to determine what types of information service providers in community-based domestic violence and sexual assault agencies consider critical to providing appropriate services. Given that domestic violence and sexual assault agencies are largely grassroots organizations, determining providers’ perspectives on what types of information are helpful for needs assessments is important because current best practices literature has largely been developed by educators and researchers rather than advocates. Moreover, most literature on assessments for violence survivors has focused on conducting assessments in health care and clinical settings. Far less research has examined conducting survivor assessments in community-based service settings such as domestic violence and sexual assault service agencies.
Even less is known about whether different types of information should be gathered from survivors entering particular service areas. Specifically, there is limited empirical research regarding whether assessment practices should differ by the type of services delivered such as legal advocacy, medical advocacy, support group, individual counseling, or shelter services. Moreover, little attention has been paid to the potential for harm to the survivor that might be posed from collecting particular types of information during assessments.
This research aimed to fill the knowledge gaps related to survivor assessment by examining agency directors’ opinions about what information should be collected from survivors at intake to ensure survivors’ varied needs were adequately addressed and services provided.
To help build the knowledge base in these areas, we examined the perspectives of domestic violence and sexual assault agency directors regarding the helpfulness of specific types of information in determining survivors’ needs so appropriate services could be delivered. Given the directors’ leadership positions, agency directors represent a rich resource about service assessment strategies that work well for the survivors in their communities.
We also investigated whether and to what extent directors’ perceptions of information types and utility for service provision differed by agency service focus (i.e., domestic violence, sexual assault, or dual-focus that deliver both services). Domestic violence and sexual assault services are often conceived of and described as distinct sets of services, which are tailored to meet specific needs of survivors who experienced either domestic violence or sexual assault. Moreover, the literature has questioned how well dual-focus agencies deliver services to survivors compared with single-focus agencies (Byington, Martin, DiNitto, & Maxwell, 1991; O’Sullivan & Carlton, 2001). This prior research posits that dual-focus agencies do not deliver services to survivors as well as single-focus agencies. Nevertheless, many sexual assault and domestic violence agencies across the United States, as well as in North Carolina (the site of the present study) provide both types of services and, therefore, are considered dual-focus or combined agencies. We hypothesized that agency service focus is related to variations in directors’ perceptions about the importance of collecting types of information from survivors.
Method
Participants and Procedures
We surveyed all domestic violence and sexual assault agencies in North Carolina by developing a sampling frame from the websites of the following organizations: the North Carolina Council for Women (NCCW); the North Carolina Coalition Against Sexual Assault (NCCASA); and the North Carolina Coalition Against Domestic Violence (NCCADV). Using these sources, we created a database of all North Carolina domestic violence and sexual assault agencies and their executive directors. We then confirmed the accuracy of the information by contacting each agency. The final list of 104 agency directors served as our sampling frame.
The survey was administered over a 20-week period. To encourage maximum participation and reduce response burden, participants could complete the survey either electronically or by a mailed paper copy. The participants received information about the web-based survey in a personalized email, as well as a paper version of the survey delivered via U.S. mail with a personalized cover letter. Typically, the executive director of the agency was the best person to respond to the survey. However, we also knew that some agencies had an associate director or other staff member who directed agency services. Therefore, both formats of the invitation to participate asked the directors to either complete the survey themselves or designate the staff member whom they felt was most knowledgeable about services to complete the survey. Potential respondents were contacted several times during the survey period by email, U.S. mail, and telephone, with the first contact providing recipients several ways of opting out of the study. Out of 104 agency directors in the sampling frame, we received completed surveys from 80 respondents (40 web-based surveys and 40 paper surveys) for a response rate of 77%.
Survey Instrument
We developed the survey instrument to assess sexual assault and domestic violence service providers’ opinions about the types of information they thought would be helpful to determine appropriate individualized services and referrals for survivors entering services. The survey instrument was based on an extensive review of the literature on domestic violence and sexual assault services, including our prior research on domestic violence and sexual assault services (Macy, Giattina, Montijo, & Ermentrout, 2010; Macy et al., 2009). The draft survey instrument was pilot tested by staff members at NCCADV, NCCASA, and individuals with experience working in domestic violence or sexual assault agencies. The pilot participants were not included in the survey-sampling frame. Feedback from the pilot test was used to revise, refine, and finalize the instrument.
The survey asked participants whether and to what extent specific types of information were helpful in determining a survivor’s needs and goals. The survey inquired whether the following types of information were helpful to service providers in service planning for new clients: survivor’s goals he or she wants to accomplish in services; knowledge of particular topics (i.e., safety planning, legal and medical services, legal and medical options, and the emotional consequences of violence); extent of violence and trauma the survivor experienced; survivor’s health and physical functioning such as physical health, mental health, substance use/abuse, and ability to carry out everyday tasks; coping strategies; social support; parenting; school or employment status; housing status; demographic characteristics; intellectual and developmental disabilities; physical disabilities; religion/religious practices; legal or criminal status; sexual orientation; and immigration status.
The survey asked directors’ perceptions about whether these types of information were helpful when collected from survivors entering five types of services, including legal advocacy, medical advocacy, support group, individual counseling, and shelter. We investigated directors’ opinions regarding information they deemed pertinent for these five service areas because these services are recommended practices in the domestic violence and sexual assault literature (Macy et al., 2009), and these are service areas in which survivor information may be feasibly collected. That is, crisis services are also a recommended best practice for domestic violence and sexual assault service providers, but it is often impossible for service providers to collect detailed survivor information in the context of crisis service delivery because they are often brief, one-time service contacts (Riger, Raja, & Camacho, 2002). However, the other service areas (especially counseling, support group, and shelter) are frequently delivered over an extended period, making collecting such information feasible (Riger et al., 2002).
For example, the question focused on legal advocacy services asked, “In order to provide the best legal advocacy services to new or relatively new clients, how helpful would it be to know the following kinds of information?” The survey then provided respondents with a list of information types (e.g., knowledge about safety planning, legal and medical services, legal and medical options) that respondents were asked to rate using a 7-point Likert-type scale (absolutely necessary = 1, extremely helpful = 2, very helpful = 3, somewhat helpful = 4, a little helpful = 5, not helpful = 6, and harmful = 7). Similar questions were asked for each of the other service areas.
Because agencies provide an array of services, the survey instructions asked participants to answer questions for those services provided by their agency. For example, single-focus sexual assault service agencies typically do not provide shelter services. In addition, the survey included questions about characteristics of the agency and the respondent.
Analysis
First, we conducted descriptive statistical analyses to find the means and standard deviations of directors’ perspectives of information types most helpful to service providers in understanding their clients’ needs. Using the results of those analyses, we rank ordered the information types across the service area by the means to understand the participants’ perspective of information importance by service area. To investigate the extent to which that perspective differed based on agency focus (i.e., single-focus agency or combined agency), we used MANOVA to test for statistical differences. We used MANOVA as a conservative test of multiple outcomes to avoid the risk of an inflated overall Type I error rate. In conducting the MANOVA, we grouped items related to (a) legal advocacy, (b) medical advocacy, (c) support group, (d) individual counseling, and (e) shelter.
Findings
Table 1 presents the means and standard deviations for the various information types across the five service areas of legal advocacy, medical advocacy, support group, individual counseling, and shelter. Using the means shown in Table 1, we developed the mean rank order (see Table 2) for the information kinds across the service types to understand the participants’ opinions about the importance of the various kinds of information across service areas. When interpreting the findings, readers should keep in mind the item response values ranged from absolutely necessary (coded as 1) to not helpful (coded 6) to harmful (coded as 7); a response of harmful indicated a respondent thought collecting that type of information posed potential risk or harm to the client. Our analyses showed few significant differences in the MANOVA and ANOVA findings. Specifically, only three survey items showed significance at the ANOVA level. After a careful review of the analysis and findings, we determined that those three findings were likely spurious given the overall pattern of nonsignificant findings; therefore, we did not include those three findings in this article’s discussion.
Agency Directors’ Opinions of the Utility of Information Type at the Start of Five Services (Rating of 1 = Absolutely Necessary to 6 = Not Helpful and 7 = Harmful; n = 76-51).
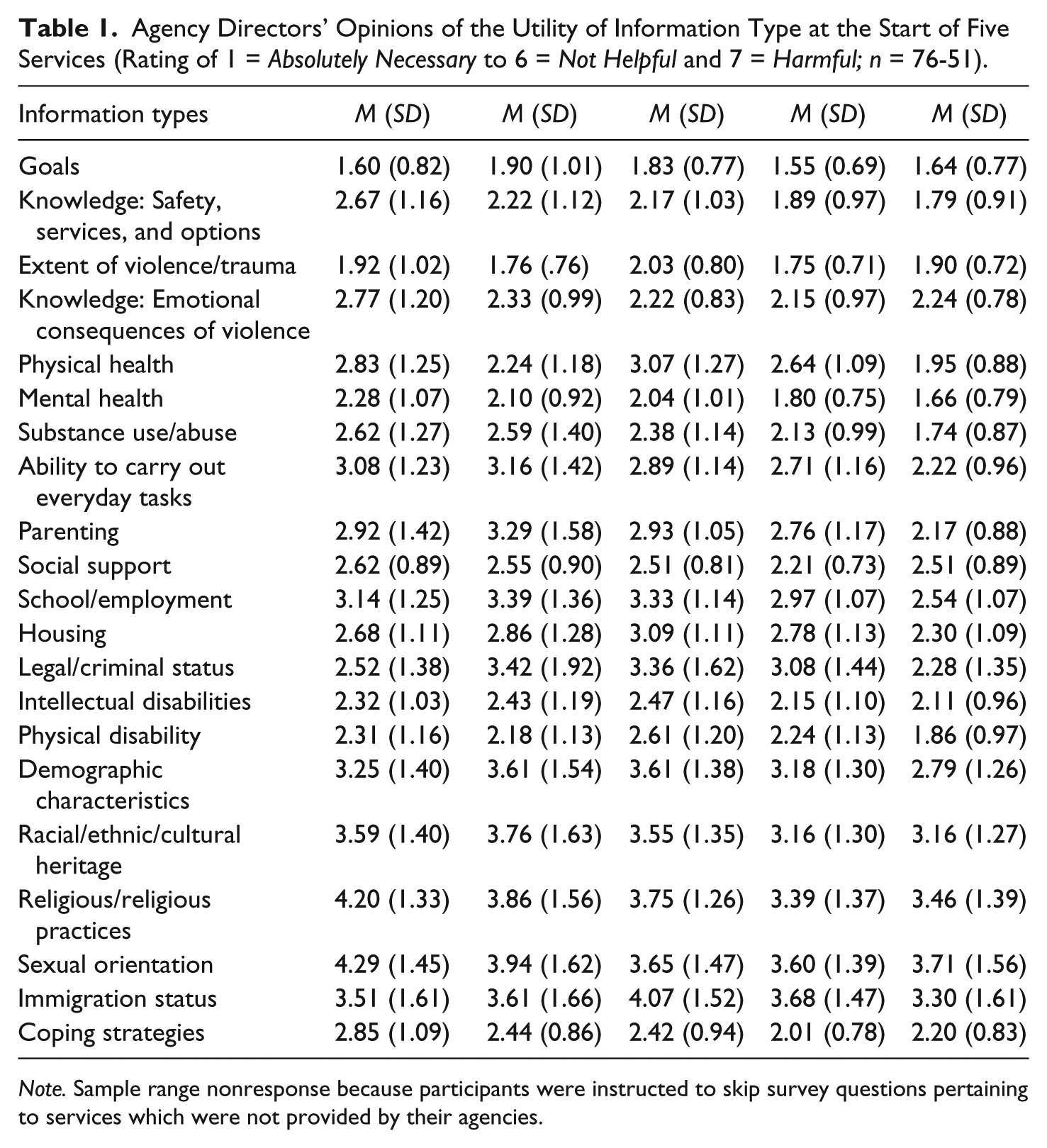
Note. Sample range nonresponse because participants were instructed to skip survey questions pertaining to services which were not provided by their agencies.
Agency Directors’ Perspectives of the Utility of Information Type at the Start of Five Services (Rankings Based on Ratings); n = 76-51.
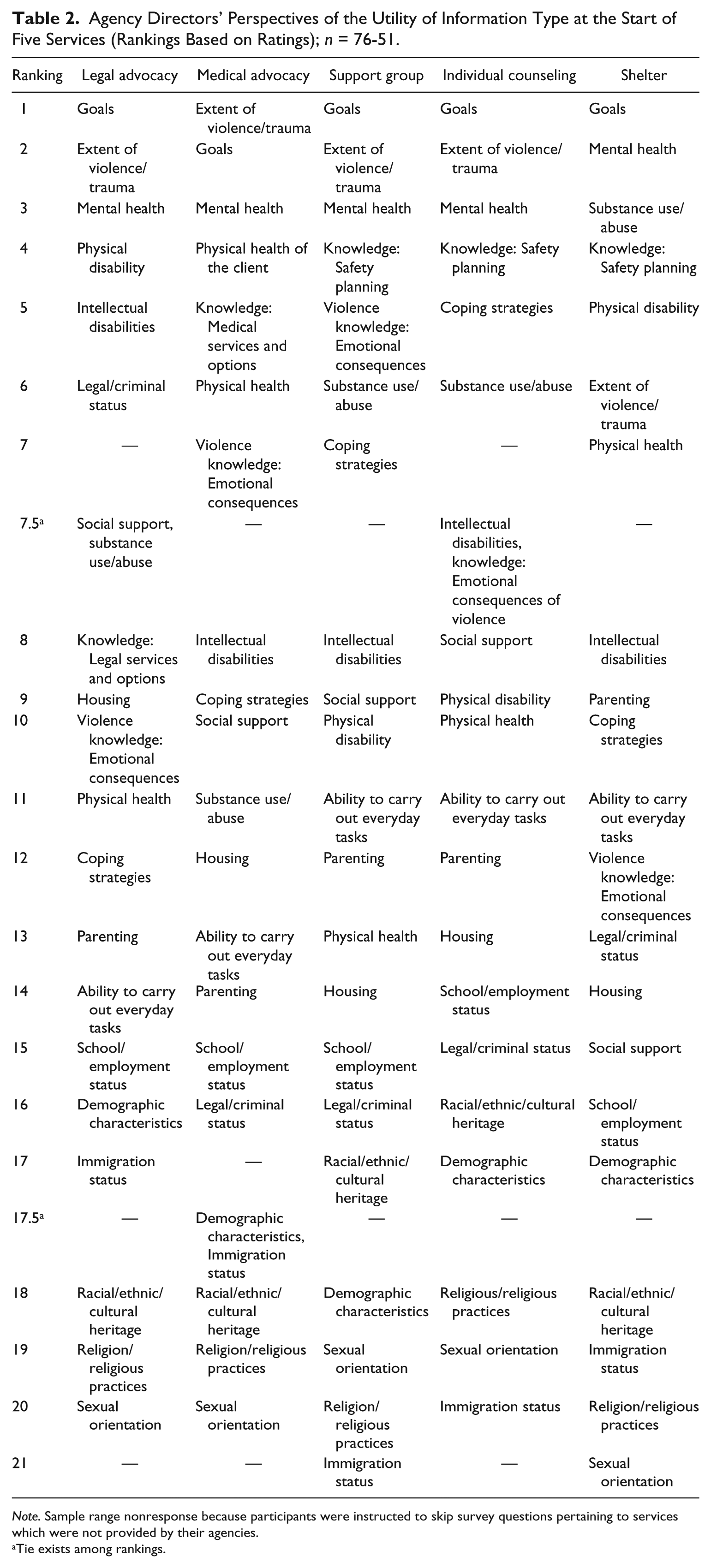
Note. Sample range nonresponse because participants were instructed to skip survey questions pertaining to services which were not provided by their agencies.
Tie exists among rankings.
Participant and Agency Characteristics
Most participants worked in combined agencies (i.e., providing domestic violence and sexual assault services; n = 54; 69.20%). However, some participants represented single-focus agencies that provided domestic violence services only (n = 14; 17.50%) or sexual assault services only (n = 10; 12.50%).
Slightly more than half of the participants reported being employed in their current position for 5 years or less (n = 50; 63.3%); however, most participants had longer histories of providing domestic violence or sexual assault services than was reflected by the years in their current position. Among those who had ever provided domestic violence services, more than half (n = 46; 58.2%) had provided such services for 6 years or more. Among those who had ever provided sexual assault services, nearly half (n = 37; 48.1%) had provided those services for 6 years or more. Furthermore, nearly 95% (n = 75) of the participants continued to provide direct services as some portion of their current work responsibilities, with nearly half (n = 36; 45.6%) of these participants reporting that at least 50% of their work time was spent providing direct services to survivors.
Participants reported a range of educational attainment. Most participants had completed either a 4-year college degree (n = 21; 27.3%) or a graduate degree (n = 34; 44.2%). The remaining 24 participants (28.3%) reported various levels of education, including having completed an associate’s degree (i.e., 2-year college), having completed some college but did not graduate, or having completed high school.
Helpfulness of Various Kinds of Information for Service Provision
Goals
Table 1 shows that for each of the five service areas (i.e., legal advocacy, medical advocacy, support group, individual counseling, and shelter), survey respondents reported it was important to ask incoming clients about their goals. The mean ratings for this question ranged from 1.55-1.90, which indicated the importance of asking about goals was rated between absolutely necessary and extremely helpful. Table 2 shows that the program directors rated client goals as the most important type of information to assess for the service areas, with the exception of medical advocacy services. For medical advocacy, program directors indicated assessing clients’ goals was the second in importance to information about the extent of the violence experienced.
Violence and trauma
The findings in Table 1 also show that, on average, participants perceived collecting information on the extent of violence and trauma experienced by the survivor was extremely helpful to absolutely necessary to arranging for adequate services and referrals. As shown in Table 2, this information type was also ranked high among all types of information and across the five service areas. Survivor’s history of violence and trauma received a ranking of first or second, with the exception of the area of shelter services for which it was ranked sixth.
Health
As seen in Table 1, participants perceived collecting information on a survivor’s health and physical functioning as important to providing adequate services. Furthermore, participants provided the following ratings of importance for information on various aspects of survivors’ health: physical health, very helpful to extremely helpful; mental health, extremely helpful to absolutely necessary; substance use and abuse, very helpful to absolutely necessary; and daily physical functioning, very helpful to extremely helpful. In addition, these types of health information received high overall rankings across all service areas (see Table 2). Mental health information was ranked especially high (i.e., second or third) across all service areas.
Survivors’ knowledge
Assessing survivors’ knowledge about topics such as safety planning, emotional consequences of violence, and a survivor’s legal and medical options was perceived by participants as very helpful to extremely helpful in helping to ensure usefulness of services, depending on the type of service being provided (see Table 1 for these findings). Notably, the rankings in Table 2 show variations among service area regarding the helpfulness of this type of information. For example, assessing survivors’ knowledge about safety planning was ranked fourth among all information types for survivors entering counseling, support group, and shelter services. However, assessing survivors’ knowledge about medical and legal options was ranked fifth and eighth overall, respectively. Furthermore, participants ranked assessing survivors’ knowledge about the emotional consequences of violence at fifth for support group services to 12th for shelter services.
Other information
Overall, although the program directors did not deem the other kinds of information as unimportant, this information was perceived as being less important for service provision. The mean findings across service areas shown in Table 1 indicate information about coping, disabilities, demographics, housing, legal and criminal status, parenting, school and employment, and social support was considered very helpful to extremely helpful to have at the beginning of service provision to ensure that survivors receive the help that they need. In addition, findings across service areas showed that directors considered data about survivors’ immigration status, racial/ethnic/cultural heritage, and sexual orientation somewhat helpful to very helpful to service provision.
Equally important, the mean ranking in Table 2 showed these kinds of information had nuanced helpfulness to service provision. For example, information about survivors’ physical disabilities received high rankings relative to other types of information for the service areas of legal advocacy (fourth) and shelter services (fifth). Information about survivors’ intellectual disabilities was ranked high relative to other types of information for legal advocacy and counseling services, with rankings of fifth and seventh, respectively. Similarly, collecting data on survivors’ legal and criminal status had a mean-based ranking of sixth relative to all information types. Last, the rankings showed that program directors consistently gave low rankings to the importance of collecting information about survivors’ immigration status, racial/ethnic/cultural heritage, religion and religious practice, and sexual orientation in relation to the other types of information across service areas.
Harmful information
As presented in Table 1, the study findings show that, overall, survey participant did not perceive any information types as being harmful to collect from survivors at the beginning of service provision. Nonetheless, we examined the frequencies for each of the item responses to determine how often any participant indicated that a certain kind of information might be harmful to collect from survivors. This review indicated that at least one survey participant deemed some information types harmful to collect for at least one of the service areas, including ability to carry out tasks, demographics, immigration status, legal and criminal status, parenting, physical health, racial/ethnic/cultural heritage, school and employment status, sexual orientation, and substance use and abuse. A few participants perceived several information types as harmful to collect across more than one service area, including demographics, immigration status, legal and criminal status, racial/ethnic/cultural heritage, sexual orientation, and substance use and abuse. However, these ratings of harmful were made by no more than 5% of the survey participants in the context of any specific service area. Moreover, only three information types were deemed harmful by exactly 5% of the survey participants: immigration status in the context of legal advocacy services, legal and criminal status in the context of medical advocacy, and immigration status in the context of support group services. The frequency of response distribution indicated that relatively few participants considered any of the specific types of information investigated in this study as being harmful to collect. Instead, 95% or more of the participants did not consider any of these information types as posing a potential harm to survivors when collected by service providers in the context of legal advocacy, medical advocacy, counseling, support group, or shelter services.
Discussion
We investigated domestic violence and sexual assault agency directors’ perceptions regarding the helpfulness of specific types of information toward determining survivors’ needs and ensuring adequate services and referrals are in place to meet those needs. This study helps to address a knowledge gap about survivors’ assessments in the provision of community-based domestic violence and sexual assault services. Furthermore, the findings suggest differences in assessment practices that are based on the type of services delivered, including legal advocacy, medical advocacy, support group, individual counseling, and shelter.
Consistent with recommendations in the literature that assessments should garner information about survivors’ individual goals and plans (Boes & McDermott, 2002; Jackson et al., 2002; Lee, 2007; Lindhorst et al., 2005), the findings from this study point to the necessity of assessing survivors’ individual goals regardless of service area. In addition, and consistent with the assessment literature cited earlier, the findings from this study show the importance providers place on their understanding of the extent and nature of the violence a survivor has experienced to best help that survivor. The findings also show that the participants in this sample considered information about aspects of the survivors’ health, including physical health and functioning, mental health, and substance use and abuse, critical to gather regardless of type of services the survivor enters. This finding is not surprising given the growing body of research that has demonstrated connections between violent victimization and negative health sequelae (Campbell, 2002; Golding, 1999; Koss et al., 1994; Plichta, 2004). The study findings overall indicate that domestic violence and sexual assault service providers should assess survivors’ goals, the extent of violence and trauma experienced, and the survivors’ health in a comprehensive way regardless of what type of services the survivor first enters.
However, the findings also point to the need to assess specific types of information depending on the services offered to the survivor. For example, knowledge about survivors’ disabilities was considered especially helpful in the context of legal advocacy and shelter services. To best serve survivors receiving medical advocacy services, program directors reported that conducting an assessment of survivors’ knowledge about medical services and options was important. Knowledge about survivors’ coping abilities was considered helpful provider knowledge upon entry into counseling services. The findings suggest that although certain types of information (goals, violence and trauma, and health) should be assessed across all service areas, providers may need additional types of information from survivors to deliver specific services.
This study also helped to address a limitation in the existing literature on domestic violence and sexual assault service assessment. To date, little research attention has been given to the question of what types of information might be harmful to survivors if collected at the beginning of services. Most sample participants did not consider the information types researched here as potentially harmful. We also note program directors consistently perceived some information types as less helpful to collect than others. The information types that were consistently determined as less helpful included survivors’ immigration status, racial/ethnic/cultural heritages, religion and religious practices, and sexual orientations. We speculate these findings reflect that violence services have been largely developed and tend to be delivered in “culturally neutral” ways (Bent-Goodley, 2005, p. 196). However, we encourage future research on these issues to explore the import of assessing these characteristics among survivors, including the need to tailor services to survivors from diverse and vulnerable groups.
We also underscore that our investigation of whether and to what extent directors’ perceptions of the helpfulness of collecting specific types of information differed based on the focus of the service agency (i.e., single-focus agency or combined domestic violence and sexual assault services) provided no findings of meaningful, significant differences. As previously noted, the literature is marked by concern about how well combined agencies deliver services to survivors as compared with single-focus agencies. Domestic violence and sexual assault services are often conceived and described as distinct sets of services that are tailored to meet the needs of survivors who experienced either domestic violence or sexual assault. However, the findings from this research suggest that these services may not differ greatly in terms of program directors’ perceptions of the helpfulness of types of information to collect from survivors during assessments. Alternatively, given a relatively small sample (n = 80), our nonsignificant findings may reflect only a lack of statistical power to determine significant differences among the three types of agencies, especially given the small number of agencies providing sexual assault services in a dedicated fashion in this sample (n = 10). Thus, we encourage future research to investigate these issues using a larger sample of agencies and directors; ideally, such a study would be national in scope.
In addition to these limitations, we encourage readers to be mindful of other study limitations. The comprehensiveness of the sampling frame and high response rate (77%) provide assurance that the findings are representative of the state. However, the sample included only directors from North Carolina agencies, thereby limiting the study’s generalizability. Another limitation is that these findings are based on directors’ perceptions and opinions about assessment practice. Thus, we recommend investigations of other agency staff members’ perspectives about assessment strategies because the perspectives of frontline staff members might vary from those of directors. Furthermore, a next step should include an investigation of survivors’ preferences about domestic violence and/or sexual assault providers’ assessment practices. Even given these limitations, the findings provide empirical information about recommended domestic violence and sexual assault assessment strategies. Sound assessment practices are critically important for domestic violence and sexual assault service providers. Conducting thorough assessments with survivors is an important way that agencies can ensure the helpfulness of their services and survivors’ well-being.
Footnotes
Acknowledgements
The authors acknowledge Carmen Crosby, Natalie Johns, Emily Pelino, Katherine Spinney, and Siobhan Young for their contributions to this research, as well as Diane Wyant for her comments on earlier drafts of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Award 180-1-07-4VD-AW-192 awarded by the U.S. Department of Justice, through the North Carolina Department of Crime Control & Public Safety/Governor’s Crime Commission.