
Abstract
Adverse childhood experiences (ACEs) and adult mental health were explored in a sample of urban Aboriginal (n = 83) and non-Aboriginal (n = 89) women. Childhood sexual abuse (CSA) was associated with negative home environments, teenage pregnancy, lifetime suicide attempts, and treatment seeking. Aboriginal women with CSA witnessed higher levels of physical/sexual abuse of family members. The severity of current psychological distress was associated with a history of childhood neglect. The results indicate that CSA rarely occurs in isolation, and that multiple ACEs are strongly associated with suicide attempts and treatment seeking in adulthood. Future studies should focus on the role of CSA in suicidality, as well as familial, community, and cultural protective factors.
Keywords
Introduction
Childhood sexual abuse (CSA) is a major public health issue that severely affects well-being during adulthood. Data from the 2012 Canadian Community Health Survey (N = 23,395) estimated that the overall prevalence of CSA was 10.1%, with women more likely to report sexual abuse in childhood compared with men. In 2008, Statistics Canada reported over 13,600 cases of sexual offenses against children and youth, the majority being female (82%; Ogrodnik, 2010). Meta-analysis on the rates of CSA in 22 countries showed that, on average, 20% of women experienced sexual abuse before the age of 18. Most first world countries including Canada, Switzerland, Australia, the United States, Spain, and Great Britain had CSA prevalence rates between 15 and 38% (Pereda, Guilera, Forns, & Gomez-Benito, 2009).
Evidence has suggested that there is a strong relationship between CSA and increased rates of physical and psychiatric illnesses. For example, the Irish Longitudinal Study on Ageing (n = 8,178) showed an association between CSA and numerous measures of poor health, including lung disease, arthritis, peptic ulcer, and chronic pain (Kamiya, Timonen, & Kenny, 2016). Similarly, psychiatric disorders including psychosis, mood disorders, posttraumatic stress disorder, generalized anxiety disorder, and elevated rates of suicidality are all linked with CSA (Afifi et al., 2014; Coles, Lee, Taft, Mazza, & Loxton, 2015; Csoboth, Birkas, & Purebl, 2005; Cutajar et al., 2010).
Women with a history of CSA are also more likely than others to have drug and alcohol problems later in life (Dinwiddie et al., 2000; Ekinci & Kandemir, 2015; Wenzel, Hambarsoomian, D’Amico, Ellison, & Tucker, 2006). In addition, there appears to be a link between histories of sexual abuse and the severity of drug/alcohol problems and psychiatric comorbidities (Brems & Namyniuk, 2002; Robin, Chester, Rasmussen, Jaranson, & Goldman, 1997). One study found a sevenfold increase in the risk for alcohol dependence among women who experienced four or more types of child maltreatment such as physical, sexual, or emotional abuse, and physical or emotional neglect (Koss et al., 2003). Collectively, this research demonstrates that CSA has serious long-lasting impacts on psychological and physical health in adulthood.
CSA has been identified as a major problem by Aboriginal communities (Brzozowski, Taylor-Butts, & Johnson, 2006; Collin-Vézina, Jacinthe, Dion, & Trocmé, 2009; Libby, Orton, Novins, Beals, & Manson, 2005). The term Aboriginal refers to status and nonstatus Native, Inuit, and Metis peoples in Canada, groups with varied linguistic, cultural, social, and historic backgrounds. In an investigation of childhood abuse among female sex workers in Vancouver, British Columbia, Farley, Lynne, and Cotton (2005) found that half of their sample (52%) were Aboriginal women, and that the majority had been sexually (82%) and physically abused (72%) during childhood. Compared with non-Aboriginal women in the sample, Aboriginal women reported significantly higher rates of childhood physical (81 vs. 58%) and sexual abuse (96 vs. 82%). While this sample cannot be generalized to other Native groups, it does indicate that there are pockets of Aboriginal women in urban areas who have experienced multiple disadvantages over the course of their lifetimes. A review of sexual abuse among diverse Aboriginal samples found that the prevalence of CSA ranged between 25 and 50%, far exceeding rates among the general population (Collin-Vézina et al., 2009).
At present, most research among Aboriginals has been conducted in groups living on reserves, or among those seeking Aboriginal targeted medical or drug/alcohol treatment. Relatively little is known about how urban Aboriginal and non-Aboriginal help-seeking women differ in terms of CSA history and its related harms (Collin-Vézina et al., 2009). This study examined physical health, mental health, and substance abuse among a sample of urban, help-seeking women with and without a history of CSA. A secondary aim of this study was to determine whether CSA had diverging effects on the health of Aboriginal and non-Aboriginal women.
Methods
Study Participants
Study participants included 172 women aged 16 years and older who were seeking help at social service agencies at the time of contact. All participants gave informed consent to participate in a study exploring the social, medical, and psychological status of urban women. Two ethnocultural groups were interviewed for this study: Aboriginal women (n = 83) and a comparison group of non-Aboriginal women (n = 89). Participants were recruited through visits to one of nine participating organizations offering social services, assistance in basic needs (i.e., food, shelter), and referrals to other centers for medical/mental health care. None of the social service agencies provided medical care, and none of the participants was being treated at the time of assessment. The design of the study allowed for an examination of differences in adverse childhood events among Aboriginal and non-Aboriginal women with similar life histories, at a similar point in life (e.g., when seeking help for basic needs such as food and shelter). Bilingual (English and French) print advertisements were also used to recruit study participants. All women accessing services at these organizations were eligible for participation, and interviews were conducted in participants’ preferred language (English or French). Respondents were offered a remuneration of CA$20.00 in gift certificates following each interview.
Primary Instruments
Semistructured interviews were conducted using the Addiction Severity Index (ASI; McLellan et al., 1992). The ASI is a structured clinical interview that collects a wide range of information, including sociodemographics, and evaluates problem severity in seven areas: alcohol use, drug use, family/social functioning, medical status, employment/support, legal status, and psychological status. Within each of these problem areas, severity is measured in terms of number, duration, frequency, and intensity of symptoms experienced during the past 30 days, and a composite score is obtained with a range from 0-1. The psychometric properties of the ASI have been found to be excellent, with high interrater reliabilities for all composite scores (Alterman, Brown, Zaballero, & McKay, 1994). Additional questions on symptom-specific health problems (e.g., chest pain, insomnia), help seeking, pregnancies before the age of 18, and number of pregnancies in lifetime were included in the interview.
The Beck Depression Inventory (BDI) is a 21-item self-report questionnaire that assesses the severity and depth of respondents’ depressive symptoms. It uses a 4-point scale, with the total score reflecting overall levels of depressive symptoms experienced in the week prior to the test (Beck & Steer, 1987).
The Child Abuse and Trauma Scale (CATS; Sanders & Becker-Lausen, 1995) was used to gather information on experiences of sexual abuse, neglect, and punishment during childhood. This 38-item self-report questionnaire measures various forms of physical, sexual, and emotional maltreatment. Each item is rated on a 5-point scale (0-4), yielding an overall index of frequency and extent of negative experiences, and three subscales of Negative Home Environment/Neglect, Sexual Abuse, and Punishment.
The Childhood Experience of Care and Abuse (CECA; Bifulco, Brown, & Harris, 1994) was used in a second interview to explore the nature of childhood experiences up until the age of 17. It is a semistructured instrument that uses lead questions and additional probes to collect concrete information on timing, duration, and descriptions of experiences of care and abuse. The CECA collects information on the characteristics of abuse, including the number of perpetrators, the relation of the perpetrator(s) to the abused, and the duration and severity of abuse. Severity ratings of physical abuse, sexual abuse, neglect, and parental antipathy in the CECA are based on objective information about these experiences during childhood. Originally created in English, the CECA was translated into French by researchers at the Université du Québec à Montréal (Tousignant et al., 1999).
Statistical Analysis
All information collected from the interviews was coded and entered into a database using the software program Microsoft Excel. All statistical analyses were conducted using the microcomputer version of SPSS (IBM Corporation, 2013). Analysis of data from the entire sample was conducted using ANOVA and MANOVA techniques for continuous variables and chi-square tests for categorical variables. Post-hoc tests were performed using t tests with a Bonferroni correction.
Information collected by the CATS concerning the experience of sexual abuse was used to create a grouping variable for analysis. This variable was used to explore relationships between CSA and problems in a number of domains, including psychological problems, substance use, and family/social problems. It comprised two categories: those never sexually abused during childhood (NA) and those who experienced CSA. This variable was created by combining four items on the CATS: (1) Before you were 14, did you engage in any sexual activity with an adult? (2) Were there traumatic or upsetting sexual experiences when you were a child or teenager that you couldn’t speak to adults about? (3) Did you have a traumatic sexual experience as a child or teenager? (4) Did your relationship with your parents ever involve a sexual experience? A positive response to any of these items indicated a history of childhood sexual abuse.
This study also employed linear regression analysis to explore factors associated with current psychological distress. Selected variables related to severity of current substance abuse, social problems, and history of adverse childhood events were used in hierarchical linear regression analysis of association with severity of psychological distress. History of adverse childhood events (ACEs) was a continuous variable created by combining seven items from the CATS. Items included parental drug/alcohol use, sexual abuse by a parent, physical mistreatment, witness of physical abuse of another family member, witness of sexual abuse of another family member, feelings of being unwanted/emotionally neglected, and having to take care of one’s self at too early an age. The stepwise model of entry was used for linear regression, allowing a test of each independent variable for their individual contribution to the variance in the dependent variable.
Results
Demographics and Socioeconomic Status (SES)
Analyses revealed that women with and without histories of CSA were comparable on primary sociodemographic characteristics (Table 1). The percentage of Aboriginal women in the NA and CSA groups did not differ. The two groups were also similar in age, marital history, and usual living arrangements in the past 3 years. Neither abuse group had significantly higher levels of education and were equally likely to be unemployed and receiving welfare as their primary source of income.
Selected Demographics Stratified by History of CSA (n = 160).
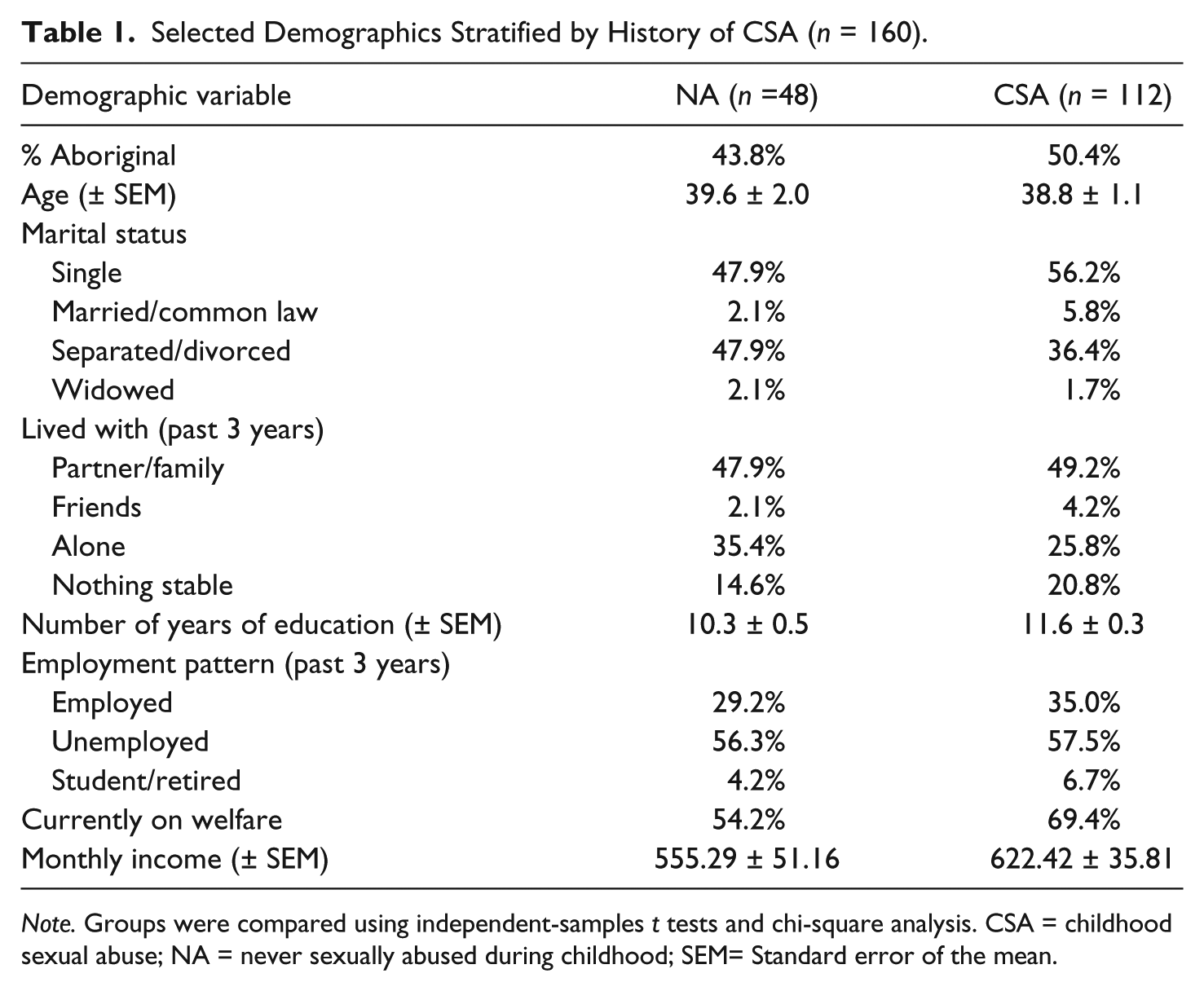
Note. Groups were compared using independent-samples t tests and chi-square analysis. CSA = childhood sexual abuse; NA = never sexually abused during childhood; SEM= Standard error of the mean.
Family/Social Relationships
Rates of close relationships with parents (NA: 76.6%, CSA: 60.9%) and siblings (NA: 69.8%, CSA: 64.8%) were similar between groups, although women in the CSA group reported significantly more relationship problems with their parents over their lifetimes—NA: 42.6%, CSA: 77.3%; χ2(1) = 17.92, p = .0001. A two-way chi-square analysis by abuse history and Aboriginal status revealed that both Aboriginal and non-Aboriginal women with CSA were significantly more likely to have had serious relationship problems with their parents in their lifetimes—Aboriginal, NA: 40.9%, CSA 71.2%, χ2(1) = 6.01, p = .014; non-Aboriginal, NA: 44.0%, CSA 82.8%, χ2(1) = 12.77, p = .001. There were no differences between abuse groups in terms of recent family/social problems or ASI social composite severity scores (NA: 0.15 ± 0.03, CSA: 2.2 ± 0.08).
Adverse Childhood Experiences (ACEs)
Women with CSA reported significantly greater rates of parental psychological problems, NA: 40.0%, CSA: 63.2%; χ2(1) = 5.37, p = .02, and parental drug/alcohol abuse, NA: 57.4%, CSA: 70.1%; χ2(1) = 6.92, p = .009. They were also significantly more likely to have feared being sexually abused when a parent was intoxicated, χ2(1) = 16.38, p < .001. Overall, one third (33.9%) of women with a history of CSA reported a sexual experience with a parent.
Women in the CSA group had significantly higher mean scores on the CATS Neglect/Negative Home Environment, NA: 1.2 ± 0.1, CSA: 2.2 ± 0.08; t(158) = −6.86, p = .0001, and Punishment, NA: 1.7 ± 0.1, CSA: 2.2 ± 0.08; t(158) = −3.56, p = .0001, subscales. The CSA group also reported greater rates of verbally abusive parents, χ2(1) = 23.28, p = .0001, and were more likely to have witnessed physical, χ2(1) = 16.33, p = .0001, and sexual, χ2(1) = 11.43, p = .001, abuse against other family members.
Ethnocultural differences in the rates of various ACEs are presented in Table 2. Both Aboriginal and non-Aboriginal women with CSA experienced significantly greater rates of witnessing parents verbally abusing each other, Aboriginal: χ2(1) = 11.24, p = .002; non-Aboriginal: χ2(1) = 12.70, p = .001, and fear of being sexually mistreated when a parent was intoxicated, Aboriginal: χ2(1) = 9.87, p = .004; non-Aboriginal: χ2(1) = 6.71, p = .02, compared with women in the NA group. Significance remained among Aboriginal women only for experiencing moderate/severe physical punishment, χ2(1) = 19.81, p < .001, witnessing the physical abuse of another family member, χ2(1) = 20.67, p < .001, and witnessing the sexual mistreatment of another family member, χ2(1) = 9.06, p = .006.
Adverse Childhood Experiences Stratified by Ethnocultural Group and History of CSA (n = 160).

Note. Groups were compared using chi-square analysis. A Yates correction was applied on tests with cell counts less than 10. Twelve study participants failed to complete the CATS sexual abuse questions. CSA = childhood sexual abuse; NA = never sexually abused during childhood; CATS = Child Abuse and Trauma Scale.
Significant differences between groups p < .05, corrected for multiple comparisons.
Physical Health
There were no significant differences between those with and without histories of CSA in terms of physical health, total number of pregnancies, abortions, or miscarriages; however, women with a history of CSA were significantly more likely to have had a teenage pregnancy, with rates nearly double that of the NA group, NA: 25.5%; CSA: 47.2%; χ2(1) = 6.39, p = .01. More than 50% of the sample reported chronic medical problems, and, on average, the women reported health problems 16.7 days out of the past 30. Most reported experiencing significant fatigue (76.1%), insomnia (66.7%), and pain-related issues (66.7%). Help seeking for medical issues was also prevalent; however, there were no group differences in ASI medical composite severity scores.
Mental Health
Rates of lifetime psychological distress stratified by childhood abuse are presented in Table 3. ASI measures of current and lifetime depression, anxiety, and substance use disorders did not significantly differ between groups. Both groups also had similar outcomes on the BDI, scoring in the mild–moderate depression range. Over a third of the women surveyed reported prior treatments for drug/alcohol and problems with no significant variation between groups. The majority of the sample also reported previous treatment for psychological problems, with significantly higher rates among women in the CSA group, χ2(1) = 10.48, p = .001. Two-way chi-square analysis examining past treatment for psychological problems showed significant differences that remained among Aboriginal women only, NA: 34.8%, CSA: 75.0%, χ2(1) = 11.02, p = .001.
Recent Psychological Distress Stratified by History of CSA (n = 160).
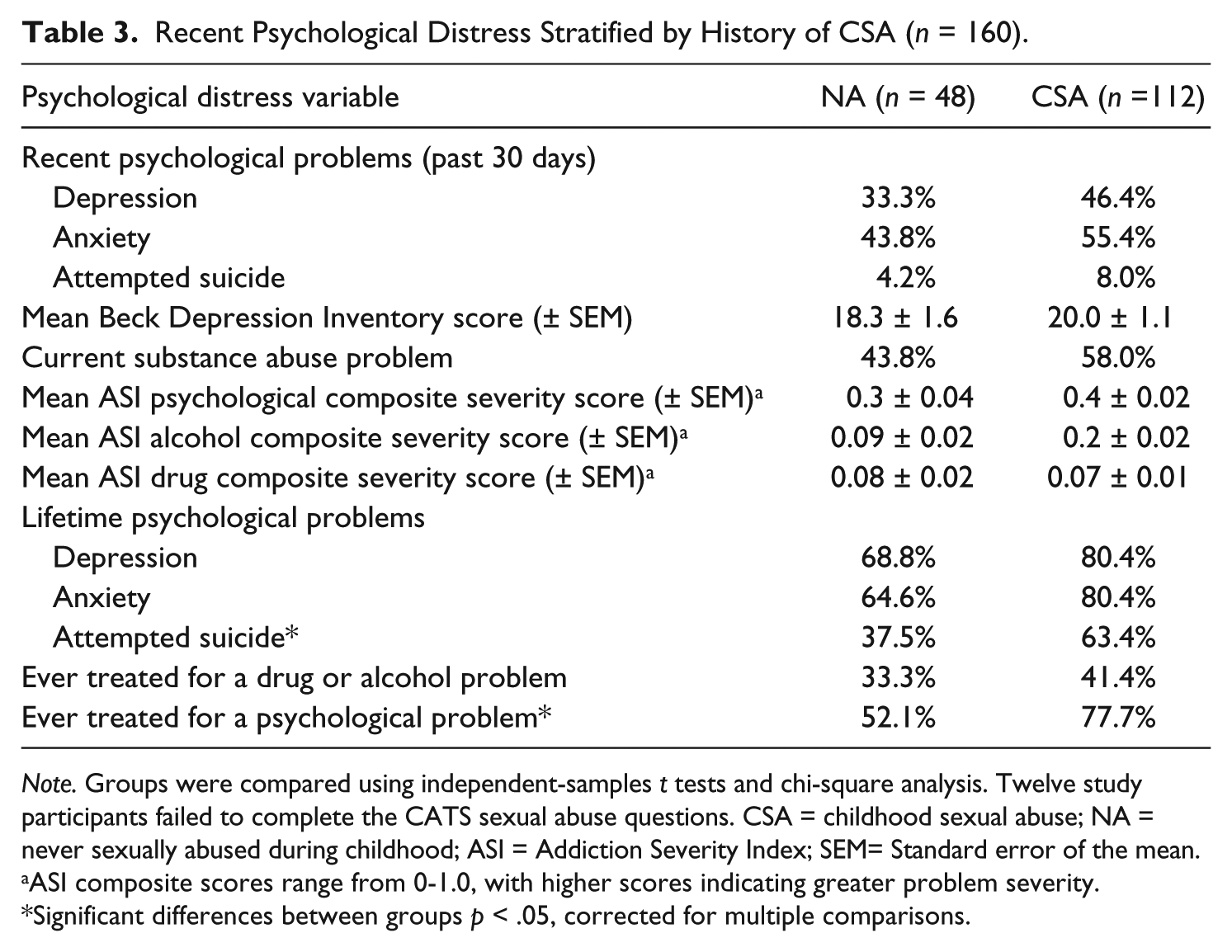
Note. Groups were compared using independent-samples t tests and chi-square analysis. Twelve study participants failed to complete the CATS sexual abuse questions. CSA = childhood sexual abuse; NA = never sexually abused during childhood; ASI = Addiction Severity Index; SEM= Standard error of the mean.
ASI composite scores range from 0-1.0, with higher scores indicating greater problem severity.
Significant differences between groups p < .05, corrected for multiple comparisons.
Table 4 presents a summary of the hierarchical linear regression. Ethnocultural background was significant in the first and final steps of the regression, accounting for 3% of the variance in the severity of current psychological problems as measured by ASI composite severity scores. ASI drug and social composite severity scores were significantly associated with the severity of current psychological problems, accounting for 22% of the variance. Higher mean scores on the CATS Neglect subscale, but not on the CATS Sexual Abuse subscale, were significantly associated with greater severity of current psychological distress.
Summary of Linear Regression for Variables Associated With ASI Psychological Composite Severity Score (n = 150).

Note. ASI = Addiction Severity Index; CATS = Child Abuse and Trauma Scale; ACEs = adverse childhood events.
As shown in Figure 1, several significant group differences emerged when examining suicidal behaviors. The CSA group reported higher rates of both lifetime suicidal ideation, χ2(1) = 9.65, p = .002, and attempted suicide, χ2(1) = 19.12, p = .003. Further analysis within ethnocultural groups revealed that only non-Aboriginal women with CSA were significantly more likely to report a history of suicidal ideation compared with women with no abuse history, NA: 48.0%, CSA: 75.0%, χ2(1) = 5.82, p = .016. However, when examining ethnocultural differences in the relationship between past suicide attempts and CSA, only the differences among Aboriginal women were significant, χ2(1) = 6.89, p = .009.

Lifetime suicide variables by CSA history.
Discussion
CSA is a multifaceted problem for socioeconomically disadvantaged help-seeking Aboriginal and non-Aboriginal women. CSA was associated with more serious relationship problems with parents, and women reporting CSA were more likely to have been raised in households characterized by parental drug/alcohol abuse and/or parental psychological problems. These results support previous studies that suggest a link between CSA and troubled family environments (Classen, Palesh, & Aggarwal, 2005; Dinwiddie et al., 2000; Fergusson, Horwood, & Lynskey, 1997; Kunitz, Levy, McCloskey, & Gabriel, 1998; Schuetze & Eiden, 2005). In a longitudinal study of 520 women, Fergusson and colleagues (1997) reported that women with a history of CSA were more than twice as likely to have had a parent with an alcohol problem (25.0 vs. 10.9%) or problematic drug use (42.9 vs. 24.3%) compared with those with no sexual abuse history.
In addition to being sexually abused, these women were more likely than others to have experience of other ACEs, including physical abuse, neglect, and witnessing the verbal, physical, and/or sexual mistreatment of other family members. There is evidence that different types of childhood maltreatment rarely occur in isolation, and multiple exposure to different types of childhood maltreatment are strongly associated with increased likelihood of psychological problems and treatment seeking (Duran et al., 2004; Tang et al., 2006; Teicher, Samson, Polcari, & McGreenery, 2006; Turner, Finkelhor, & Ormrod, 2006). Furthermore, the experience of multiple ACEs have demonstrated cumulative, long-lasting negative impacts on physical health (Dube et al., 2009) and mental health (Edwards, Holden, Felitti, & Anda, 2003) in adulthood. Among women with a history of CSA, witnessing the sexual mistreatment of another family member was more than twice as prevalent among Aboriginal women. This is particularly striking given the similar SES and abuse histories of Aboriginal and non-Aboriginal women sampled. Data from the 2006 Census reported Aboriginal Canadians were 4 times as likely as non-Aboriginals to live in an overcrowded home (Statistics Canada, 2009), and it is possible that the high rates of witnessing the abuse of other family members among Aboriginal women stem from overcrowded home environments.
Teenage pregnancy has shown a strong relationship with the experience of different types of lifetime abuse (Gessner & Perham-Hester, 1998; Harrykissoon, Rickert, & Wiemann, 2002; Rosen, 2004; Trickett, Aber, Carlson, & Cicchetti, 1991). While women in this sample who had been sexually abused in childhood did not report more lifetime pregnancies, they had nearly doubled rates of teenage pregnancy. Teen pregnancy has been linked to lower educational outcomes, low SES, and worse health outcomes for both mother and child (Drake & Pandey, 1996; Paranjothy, Broughton, Adappa, & Fone, 2009; Penman-Aguilar, Carter, Snead, & Kourtis, 2013; Woodward & Fergusson, 1999).
Despite high rates of health-related problems, including fatigue, insomnia, and chronic medical issues, there were no physical health differences between the two abuse groups. These data contrast with the literature indicating greater rates of health problems among individuals sexually abused as children (Brown, Thacker, & Cohen, 2013; Lind, Aggen, Kendler, York, & Amstadter, 2016; Monnat & Chandler, 2015). It is possible that these effects were masked due to other contributory factors including the overall low SES of the sample and the extremely high rates of violent victimization reported.
In terms of mental health, women in this sample experienced high rates of psychological distress. It was interesting to note that the linear regression analysis showed that psychological distress was most strongly associated with the severity of current social and drug problems, accounting for the largest proportion of the variance. These factors were thus more proximate mediators in the severity of distress experienced by the women in this study. The only adverse childhood event associated with the severity of current psychological problems was a history of childhood neglect.
Although no differences in depression, anxiety, or substance use disorders were found between abuse groups, women in the CSA group were significantly more likely to have seriously contemplated suicide or attempted suicide in their lifetimes. These findings corroborate previous research indicating a higher level of suicide attempts among women with a history of CSA compared with those without (Dube et al., 2005). This trend was particularly evident among Aboriginal women with CSA, who reported greater rates of past suicide attempts compared with their non-Aboriginal counterparts (71.2 vs. 56.7%). This may be partially explained by the higher rates of ACEs among Aboriginal women with CSA compared with non-Aboriginal women. It has been suggested that psychological responses to the trauma of CSA are socially and culturally determined (Barker-Collo, 1999; Wasco, 2003). Individual responses to trauma are framed within and influenced by life experiences such as witnessing violence in the home or community, racism, and sexism. These factors can influence women’s expectations of personal safety and options for recourse following an assault (Wasco, 2003).
Due to the need for individual and community healing, studies on resilience and the effects of individual resources (e.g., social support, family relations) and cultural beliefs on women’s ability to cope with memories of past and current sexual abuse are needed. Future studies in this area should ascertain not only specific protective factors against the development of adverse physical and mental health outcomes but what specific components of family, community, or culture are protective (Bellis et al., 2014; Hébert, Lavoie, & Blais, 2014; Pejovic-Milovancević et al., 2014; Dettmeijer-Vermeulen, van Krimpen, & van der Staal, 2016; Wright et al., 2016). Last, given the consistent finding that women who experience CSA also reported multiple other ACEs, it is essential that future research focus on the early detection and treatment of girls experiencing trauma. This could potentially reduce the experience of traumatic events later in childhood and adulthood, while effecting rates of teenage pregnancy, and long-term health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.