
Abstract
This study investigates the relationship between the characteristics of different types of childhood violence and adult victimization using two waves of data from a community telephone survey (T1) and a follow-up survey, including 505 cases and 506 controls, aged 17-35 years (T2). The logistic regression analyses showed that exposure to childhood abuse, regardless of type, was associated with adult victimization. Exposure to multiple types of abuse, victimization both in childhood and in young adulthood, and recency of abuse increased these odds. Our findings emphasize the importance of assessing multiple forms of violence when studying revictimization. Practitioners working with children and young adults should be attentive to the number of victimization types experienced and recent victimization to prevent further abuse.
Introduction
In recent decades, research has repeatedly found that individuals exposed to childhood sexual abuse have a heightened likelihood of experiencing victimization in adolescence or adulthood (Messman-Moore & Long, 2003; Pittenger, Huit, & Hansen, 2016). Findings from community samples have shown that exposure to childhood sexual abuse may double or triple the risk of revictimization (Classen, Palesh, & Aggarwal, 2005), which in turn has been associated with worse mental health outcomes compared with exposure to childhood or adult victimization alone (Thoresen, Myhre, Wentzel-Larsen, Aakvaag, & Hjemdal, 2015). Both individual and contextual factors, such as poor mental health, low self-esteem, feelings of powerlessness, risky behavior, poverty, and low social support, may affect the risk of sexual revictimization (Banyard, Williams, Siegel, & West, 2002; Campbell, Dworkin, & Cabral, 2009; Classen et al., 2005; Fargo, 2009; Gidycz, 2011; Grauerholz, 2000; Strøm, Hjemdal, Myhre, Wentzel-Larsen, & Thoresen, 2017). The characteristics of the initial sexual abuse experience may also influence the risk of subsequent victimization. Research in this area, for the most part, has focused on the severity of the initial abuse, hypothesizing that this experience may predict revictimization as a result of increased mental health problems, early onset of sexual intercourse, and increased sexual risk taking (Arata, 2000; Fergusson, Horwood, & Lynskey, 1997; Finkelhor & Browne, 1985; Koss & Dinero, 1989; Lalor & McElvaney, 2010).
In reviewing the field of sexual revictimization, Macy (2008) called for the use of prospective data to investigate how the timing of the sexual victimization affects the revictimization risk and other factors that connect the initial abuse with re-experiencing violence. Previous research has mainly been cross-sectional, and the few longitudinal studies that have been conducted, with a few notable exceptions (Casey & Nurius, 2005; Collins, 1998; Fergusson et al., 1997; Hamilton & Browne, 1999; Kilpatrick et al., 1997), have mostly involved clinical or college samples (Banyard et al., 2002; Gidycz, 2011; Humphrey & White, 2000; Maker, Kemmelmeier, & Peterson, 2001; Roodman & Clum, 2001). A major research gap in the field is that the majority of studies have focused only on sexual violence in childhood (Pittenger et al., 2016). There is a lack of knowledge of the relationship between the different types of childhood violence and revictimization in young adulthood. Thus, new knowledge of the association between initial abuse and revictimization may be necessary both for preventive purposes and for theory development (Arata, 2002; Macy, 2008). The current article investigates the characteristics of childhood abuse and their association with revictimization (physical and sexual victimization and controlling behavior from a partner). Expanding on the current literature, this prospective study includes different types of violence (sexual, physical, psychological, and neglect) and their combinations, not solely focusing on sexual abuse, and uses a community sample.
Childhood abuse characteristics that have been studied in relation to revictimization include severity of the abuse, age of onset, recency of abuse, and adolescent victimization (Pittenger et al., 2016). Other characteristics that may influence the risk of revictimization include having experienced multiple incidents or multiple types of violence. Experiencing multiple types of abuse is not uncommon among childhood victims and has been found to be associated with re-exposure to violence (Aakvaag, Thoresen, Wentzel-Larsen, & Dyb, 2017; Abajobir, Kisely, Williams, Clavarino, & Najman, 2017; Barnes, Noll, Putnam, & Trickett, 2009; Casey & Nurius, 2005; Coid et al., 2001; Jankowski, Leitenberg, Henning, & Coffey, 2002). Coid et al. (2001) found that unwanted sexual intercourse highly overlapped with other unwanted sexual activities and physical violence in childhood and that exposure to these types of abuse led to an increased risk of violence in adulthood. However, some researchers have also found that sexual abuse alone (Maker et al., 2001) or physical abuse alone (Arata & Lindman, 2002) was associated with a higher likelihood of re-exposure to abuse.
The findings on childhood violence characteristics and their association with revictimization have been mixed, and the definitions have varied. Severity has been the most common measure, although it has been defined in different ways: as sexual contact/penetration, close relationship to the perpetrator, physical injury following the abuse, frequency of the abuse, and duration and use of force (Casey & Nurius, 2005; Classen et al., 2005; Messman-Moore & Long, 2003). Some researchers have found that frequent and more severe incidents of abuse are associated with subsequent violence in youth and adults (Arata, 2000; Barnes et al., 2009; Casey & Nurius, 2005; Fergusson et al., 1997; Fortier et al., 2009; Roodman & Clum, 2001; Swanston et al., 2002; Waldron, Wilson, Patriquin, & Scarpa, 2015), whereas others have not found this association (Maker et al., 2001; Matta Oshima, Jonson-Reid, & Seay, 2014). These contrasting findings may point to different explanations. Severe childhood sexual abuse may imply more self-blame, posttraumatic stress disorder (PTSD), and consensual sexual behavior, which may increase vulnerability to subsequent victimization (Arata, 2000). Alternatively, being exposed to abuse in childhood in itself may be sufficient to put one at risk for further victimization, independent of severity (Maker et al., 2001). These contrasting findings warrant further exploration of the relationship between childhood violence characteristics and revictimization.
With regard to age of onset and recency of abuse, the findings have differed. Several researchers have found that the earlier in age the victimization occurs, the higher the risk of revictimization (Casey & Nurius, 2005; Simmel, Postmus, & Lee, 2012), whereas others have found that recency of the initial abuse contributes to a higher risk of revictimization in adulthood (Classen et al., 2005; Collins, 1998; Himelein, 1995; Humphrey & White, 2000). Thus, it is unclear whether experiencing violence in childhood or in late adolescence will lead to a greater risk of revictimization in adulthood. Explanations for both are reasonable. Experiencing abuse early in life may shape personality and social relations, for example, poor mental and physical health, ineffective coping strategies, and risky behavior (Anda et al., 2006; Grauerholz, 2000), which in turn may increase the risk of revictimization. Alternatively, the effect of childhood abuse may be restricted in time, meaning that the more time that passes without experiencing new victimization, the less the abuse may contribute to a person’s overall vulnerability (Himelein, 1995). In her longitudinal study of a female college sample, Himelein (1995) found an association between precollege dating violence and revictimization, while there was no significant association between childhood sexual abuse and college victimization when controlled for precollege dating. Thus, it is unclear whether exposure to childhood abuse leads to both adolescent abuse (Fergusson et al., 1997) and adulthood abuse (Roodman & Clum, 2001), or whether it is the combination of childhood and adolescent abuse that leads to a heightened risk of revictimization in adulthood (Arata, 2002; Banyard et al., 2002; Gidycz, Coble, Latham, & Layman, 1993; Humphrey & White, 2000).
A limitation of the current literature is the various definitions used for the different developmental stages. Childhood sexual abuse has been defined as sexual victimization that occurs before 14 years of age and extending to 18 years of age (Arata, 2000; Classen et al., 2005; Coid et al., 2001; Fortier et al., 2009; Maker et al., 2001). Adolescence has been defined as ranging from 14-18 years or 15-18 years of age (Classen et al., 2005; Fergusson et al., 1997), while others include adulthood as ranging from above 14 to above 18 years of age (Arata, 2000; Classen et al., 2005; Coid et al., 2001; Fortier et al., 2009; Maker et al., 2001). Consequently, the results are hard to compare because they vary according to the defined age.
In summary, it is clear that there are discrepancies in the findings of the relationship between childhood violence characteristics and revictimization. Thus, we aimed to explore these hypotheses:
These hypotheses were investigated by using two waves of data (N = 1,011, 16-33 years) from a community telephone survey (T1) with a follow-up time of 12-18 months (T2).
Method
Participants and Procedure
This is a follow-up study (T2) of a subsample of participants from a population study (T1). The baseline survey included an adult sample (18-75 years of age, n = 4,527 responders) and an adolescent sample (16-17 years of age, n = 2,062 responders) that were drawn from the General Population Registry of Norway. The participants of the population survey received an information letter at least a week before being contacted by phone. The interviews were conducted by phone in the second and third quarters of 2013. The response rate was 42.9% for the adult sample and 61.7% for the youth sample (see Thoresen et al., 2015, for more details about the procedure at T1).
For the follow-up (T2), we contacted both respondents exposed to childhood violence (cases) and respondents not exposed to childhood violence (controls). Of the participants at T1 who had consented to be recontacted (92%, N = 5,996), the youngest individuals (aged 17-33 years at T1) were contacted (n = 2,549) and were interviewed by phone 12-18 months after the baseline survey. Of these, 1,325 individuals were not reachable because of technical errors, no answer, incorrect registration information, incorrect numbers, or because the informant had moved abroad or was traveling during the interview period. Of the individuals who answered the phone (n = 1,224), 1,011 (82.6%) participated, which is 39.7% of the individuals we attempted to reach. This final sample included 505 cases and 506 controls. Both T1 and T2 were conducted by the data collection agency Ipsos and were approved by the Regional Committee for Medical and Health Research Ethics in Southeast Norway.
A previously conducted attrition analysis showed that the respondents had a significantly higher prevalence of violence exposure than the individuals who could not be reached, but there were no significant differences in age and violence exposure between the respondents and the individuals who refused to participate. The responders were more often female, although there were small differences between genders with respect to refusing to participate (men, 51.2%; women, 48.8%; see Strøm et al., 2017, for more details about the attrition analysis).
Sample description
The total sample (N = 1,011) included 59.7% (n = 604) women, and the mean age was 22 years at T2. There were no significant gender or age differences between the cases and the controls. The individuals exposed to childhood violence had a significantly, χ2(1, N = 1,011) = 48.47, p < .001, higher occurrence of T2 victimization (N = 159, 31.5%) compared with controls (N = 67, 13.2%) (Strøm et al., 2017). A majority of the respondents had Norwegian-born parents (95.1%) and a perceived family financial situation (measured as better, similar, or worse than others) similar to others (64.1%). Their highest level of education was college or university (72.2%). There were no significant sociodemographic differences between the cases and the controls, except for perceived family financial situation; the cases reported a higher prevalence of having a worse family financial situation than most people (12.2%) compared with the controls (5.0%), χ² = 16.73, df = 2, p < .001.
Measures
T1 measures
Childhood violence was measured as exposure to violence occurring before the age of 18 years. The childhood violence categories were combined into three main categories: childhood sexual abuse, physical violence, neglect and psychological violence.
Childhood sexual abuse included sexual abuse occurring before 13 years of age, forcible rape, and other forms of unwanted sexual contact. Sexual abuse occurring before 13 years of age was defined as any form of sexual contact (vaginal, oral, or anal penetration) occurring before 13 years of age by someone who was at least 5 years older (Kilpatrick, Resnick, Baber, Guille, & Gros, 2011). Forcible rape included forceful intercourse, oral sex, anal sex, or having had fingers or objects put in the vagina or anus using physical force or threats. Other forms of unwanted sexual contact included questions about unwanted sexual contact while intoxicated, subject to fondling or touching of genitals using physical force or threats, having been pressured into sexual acts or other forms of sexual assault, or abuse other than the ones listed above. The items were adapted from two American surveys (Kilpatrick et al., 2003). Being exposed to childhood sexual abuse was defined as an affirmative response to at least one item within one of the categories.
Physical violence included exposure to violence from parents and witnessing parental interpersonal violence (intimate partner violence [IPV]). Measures of exposure to violence included seven forms of violence: having been (a) pinched hard, (b) shaken or pushed violently, (c) hit with a flat hand, (d) hit with a fist or a hard object, (e) kicked, (f) beaten up, and/or (g) physically attacked in other ways. Parental IPV included seeing, hearing, or knowing about violence between parents in which one of the parents had been slapping, hitting with fist or object, kicking, strangulating, or otherwise physically attacking the other parent (Kilpatrick et al., 2003). The overlap between physical violence and IPV was considerable (63.3% of the ones reporting parental IPV had also experienced physical violence, and 23.5% of the ones reporting physical violence had also experienced parental IPV). Being exposed to physical violence was defined as an affirmative response to at least one of these items.
Neglect and psychological violence included parental psychological violence and parental emotional neglect. Parental psychological violence was measured by asking whether “your parent(s) repeatedly ridiculed you, put you down, ignored you, or told you that you were no good” (Goodman, Corcoran, Turner, Yuan, & Green, 1998). Parental emotional neglect was measured by the following question: “In your childhood, how often did you feel loved?” Parental physical neglect was measured by the following question: “In your childhood, how often did you feel that someone could take care of you and protect you?” Both neglect questions were measured using a 5-point scale ranging from “never” to “very often” or “always.” Responding “never,” “seldom,” or “sometimes” defined neglect (Thoresen et al., 2015). Being exposed to neglect and/or psychological violence was defined as an affirmative response to at least one item within one of the mentioned categories.
Combination of violence types
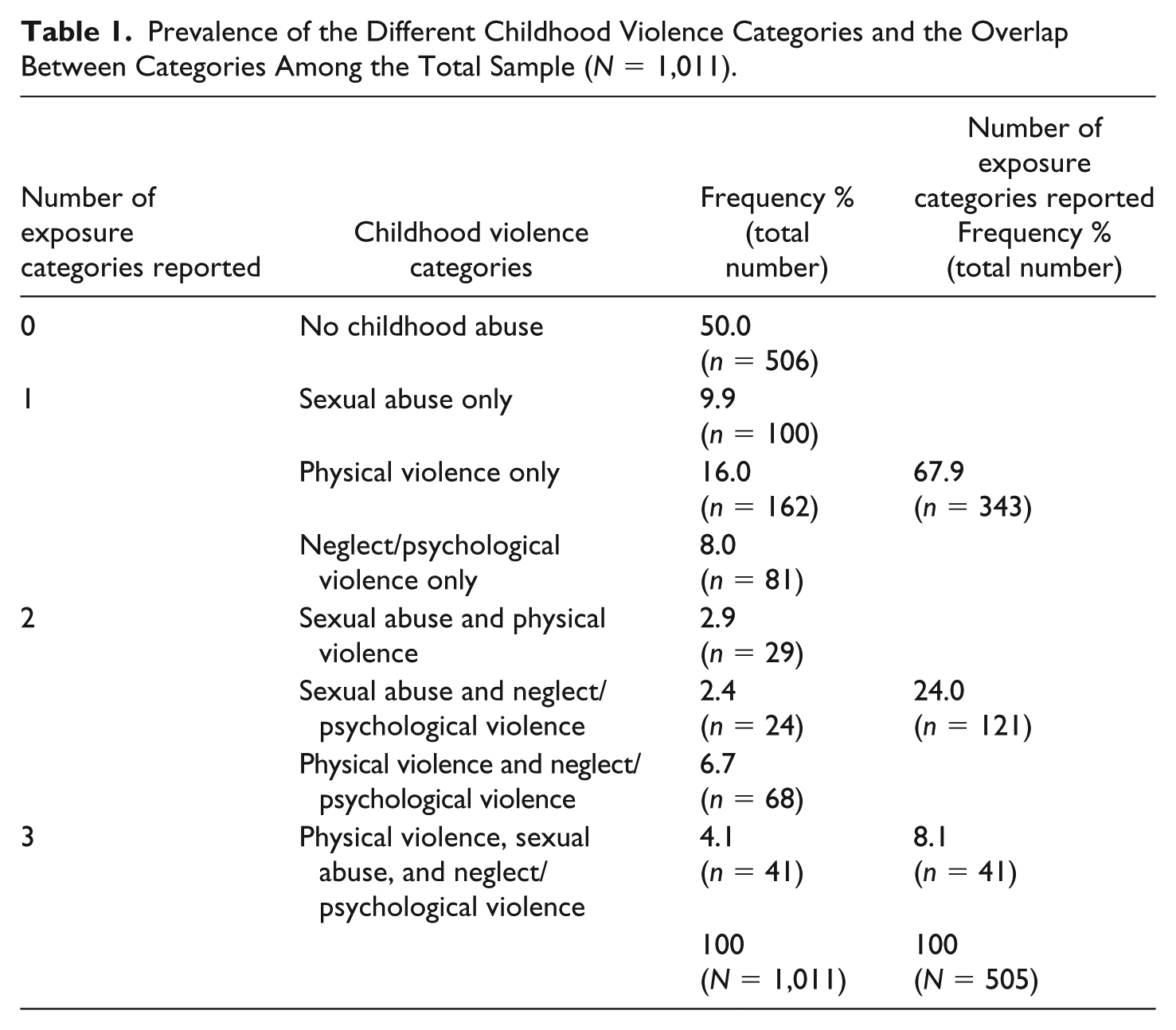
To investigate the associations of T2 victimization with each of the childhood abuse categories separately as well as in combination, a variable that accounted for all possible combinations of childhood abuse was created (Table 1). To investigate the association with revictimization, a variable that accounted for one, two, and three types of abuse was made.
Prevalence of the Different Childhood Violence Categories and the Overlap Between Categories Among the Total Sample (N = 1,011).
Characteristics of violent episodes
For those who reported certain types of violent events, follow-up questions regarding the characteristics of the event were asked, which included physical violence and sexual violence, while there were no follow-up questions regarding parental IPV. Neglect and psychological violence are phenomena characterized by a pattern of behaviors, instead of single, discrete episodes, and in our study are measured as such. Therefore, the follow-up questions would not make sense for these types of violence and were consequently not posed after these events.
Physical injury was measured for childhood physical abuse, sexual abuse occurring before 13 years of age, and forcible rape in childhood. The individuals who answered affirmatively to these types of abuse were further questioned about whether they were physically injured because of the abuse.
Exposure to violence multiple times was measured by asking the respondents whether the incident occurred once or multiple times.
Age of onset and last violence experience were reported by the respondents for childhood exposure to physical and sexual abuse.
Victimization reported after age 18 years at T1 was recorded for respondents who were adults (older than 18 years of age) when interviewed at T1 and included experiences of sexual and physical violence. Only the respondents who were at least 18 years of age at T1 were included in the analyses (Table 4).
T2 measures
T2 victimization was defined as occurring when the respondents were exposed to sexual victimization, physical victimization, and/or controlling behavior from a partner during the period between T1 and T2 (Strøm et al., 2017). The term revictimization was used when this incident occurred to individuals who had been exposed to childhood violence. Sexual victimization included rape and other unwanted sexual experiences, as defined above, occurring in the last 12-18 months. Physical victimization included less severe violence and severe violence. Measures of less severe violence included having been hit with a flat hand, having hair yanked/pulled, having been scratched, and/or having been pinched hard (the respondents were asked to ignore unintentional acts, for example, play or sports). Severe violence included being hit with a fist or a hard object, being kicked, strangled, beaten up, threatened with a weapon, and/or being physically attacked in other ways. Being exposed to physical violence was defined as an affirmative response to at least one of these items (Thoresen et al., 2015). Controlling behavior was measured by answering affirmatively to having had a partner or spouse who was controlling, for example, controlling their time, demanding them to account for where they had been at all times, and being jealous or suspicious of friends (Strøm et al., 2017).
Statistical Analyses
Chi-square tests were used to compare the demographics for cases and controls (1,011). Logistic regression analyses were conducted to investigate relationships in three different ways: (a) between different types of childhood violence categories and different types of T2 victimization in the total sample (N = 1,011), (b) between different combinations of childhood violence types and T2 victimization (in one combined category; N = 1,011), and (c) between the number of childhood violence categories reported and T2 victimization (N = 1,011). As there was some overlap between the violence types and perpetrator reported after the age of 18 years at T1 and within the 12-18 months at T2 (n = 29), we conducted sensitivity analyses to assess whether the associations were due to the overlap.
As we wanted to look at the differences between those childhood-exposed individuals who had experienced revictimization and those who did not, only those cases were chosen for the next analyses (N = 505). As commented in section “Measures,” we did not have measures of frequency (multiple times vs. once) and physical injury for neglect and psychological violence. Thus, the “neglect/psychological violence only” category (n = 81) was excluded from our analyses investigating such characteristics, meaning that the following analyses included only physical (without parental IPV) and sexual abuse. Logistic regressions were employed to test associations with revictimization. Logistic regressions were also used in examining violence experienced after the age of 18 years in childhood-exposed individuals and nonchildhood-exposed individuals and their association with T2 victimization. Because the respondents who had not turned 18 years old at T1 were excluded, the total number for these analyses was 525, controlling for sociodemographics except age. These analyses were also run without the overlap. All of the analyses were conducted using IBM SPSS statistics versions 22 and 24.
Results
T2 Victimization in Childhood Violence–Exposed Cases and Nonexposed Controls
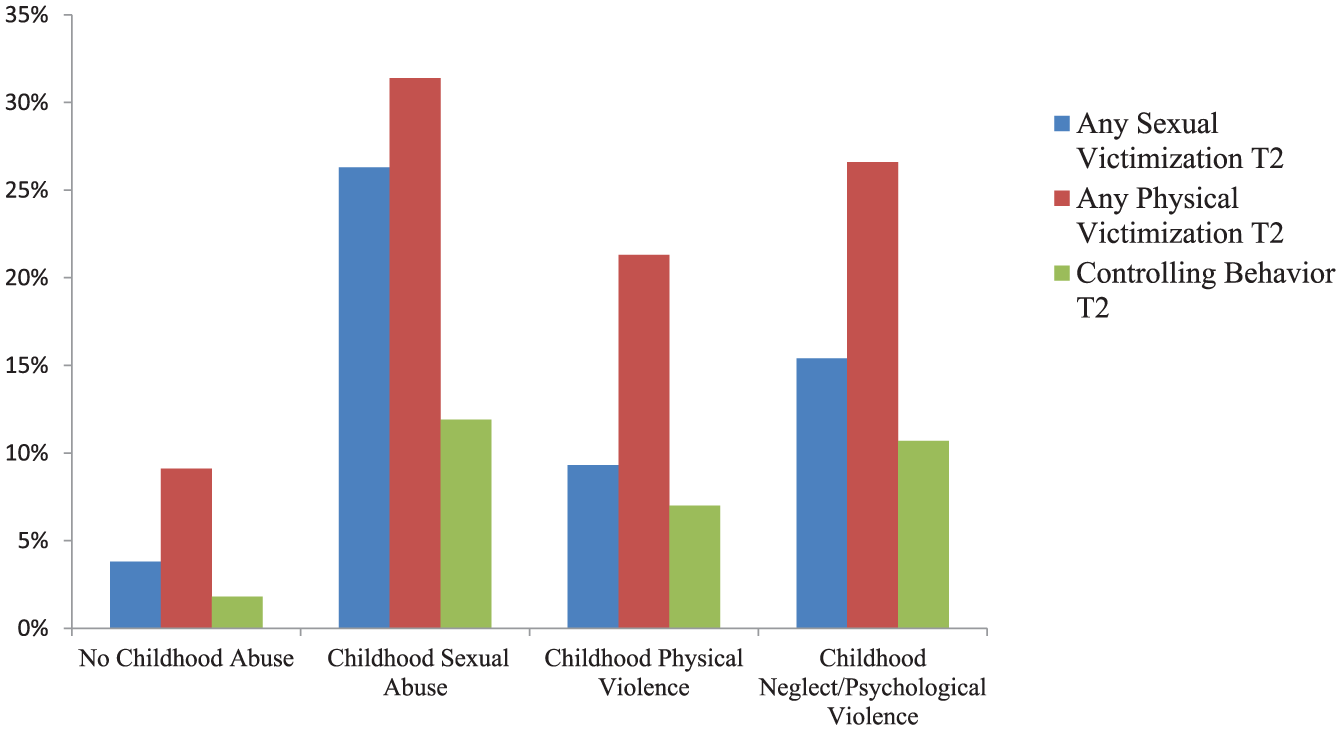
Victimization at T2 occurred more frequently in all childhood violence groups, compared with those who had not experienced any childhood abuse (Figure 1). The risk of T2 victimization was not restricted to the same violence type as the violence experienced in childhood; rather, it appeared that exposure to childhood violence meant an increased risk of all types of T2 victimization. For example, 30.4% of child sexual abuse victims reported physical violence, and 10.3% reported partner-controlling behavior at T2.
T2 victimization types within the various childhood exposure groups.
T2 victimization types within the various childhood exposure groups
Of the childhood-exposed cases, the majority of the respondents (n = 343) had experienced one type of abuse (Table 1), although a substantial minority had experienced two types of abuse (n = 121) and some respondents had experienced three types of abuse (n = 41). Among the single types of abuse, exposure to parental physical violence was the most prevalent, followed by sexual abuse and neglect/psychological violence. For the individuals experiencing two types of abuse, the combination of physical violence and neglect/psychological violence had the highest frequency.
Different Types of Childhood Violence, Number and Combinations of Childhood Violence Categories, and Their Associations With T2 Victimization
All the childhood violence categories had significantly higher odds of T2 victimization compared with the controls, adjusting for sociodemographics (Table 2). Among the single categories, individuals who had experienced childhood sexual abuse had the highest odds for T2 victimization compared with the controls. An increase in the number of childhood violence types led to higher odds of T2 victimization. For example, sexual abuse alone led to a fourfold risk of T2 victimization, but when combined with neglect/psychological violence, the odds ratio (OR) for T2 victimization increased to 22. A significant relationship could also be observed for the association between the number of exposure categories and T2 victimization. The individuals exposed to three types of violence had the highest risk of T2 victimization (unadjusted: OR = 9.25; 95% confidence interval [CI]: [4.72, 18.12]; p < .001; adjusted: OR = 9.83; 95% CI: [4.85, 19.91]; p < .001), followed by two types of victimization (unadjusted: OR = 3.88; 95% CI: [2.47, 6.08]; p < .001; adjusted: OR = 4.04; 95% CI: [2.52, 6.48]; p < .001) and, finally, one type of victimization (unadjusted: OR = 2.33; 95% CI: [1.64, 3.31]; p < .001; adjusted: OR = 2.41; 95% CI: [1.68, 3.44]; p < .001) compared with the individuals not exposed to these types of violence.
Logistic Regression Analysis Displaying Associations Between Categories of Childhood Violence, Compared With Those Who Had Not Experienced Childhood Violence and T2 Victimization (N = 1,011).

Note. Unadjusted model. p value for unadjusted model, χ2 (7, N = 1,011) = 100.09, p < .001. p value for adjusted model, χ2(13, N = 1,003) = 119.29, p< .001. Adjusted for gender, age, perceived family financial situation, education, and ethnicity. CI = confidence Interval.
Reference group.
Associations Between T1 Violence Characteristics (Age of Onset, Age of Last Abuse Experience, Frequency, and Physical Injury) and Revictimization
Of the individuals who had experienced physical violence or rape in childhood (n = 235), 40 (11.1%) reported physical injuries as a result of the violence. The mean age of onset for physical and sexual violence (n = 424) in childhood was 10.3 years (n = 362, SD = 4.3), ranging from 1 to 17 years. The mean age at the last violent incident was 13.0 years, ranging from 4 to 17 years (n = 315, SD = 3.5). Of the 404 persons who experienced physical violence and/or sexual violence, 64.0% (n =323) reported that it occurred multiple times.
Age of onset, age of last abuse experience, and physical injury were all significantly associated with revictimization in the unadjusted analyses, but only age was significantly associated with revictimization when adjusting for sociodemographics (Table 3). Being exposed to violence multiple times was insignificant in the unadjusted as well as in the adjusted analyses.
Logistic Regression Analyses of the Association Between Physical Injury, Frequency, Age of Onset, Age of Last Abuse Experience, and Revictimization.
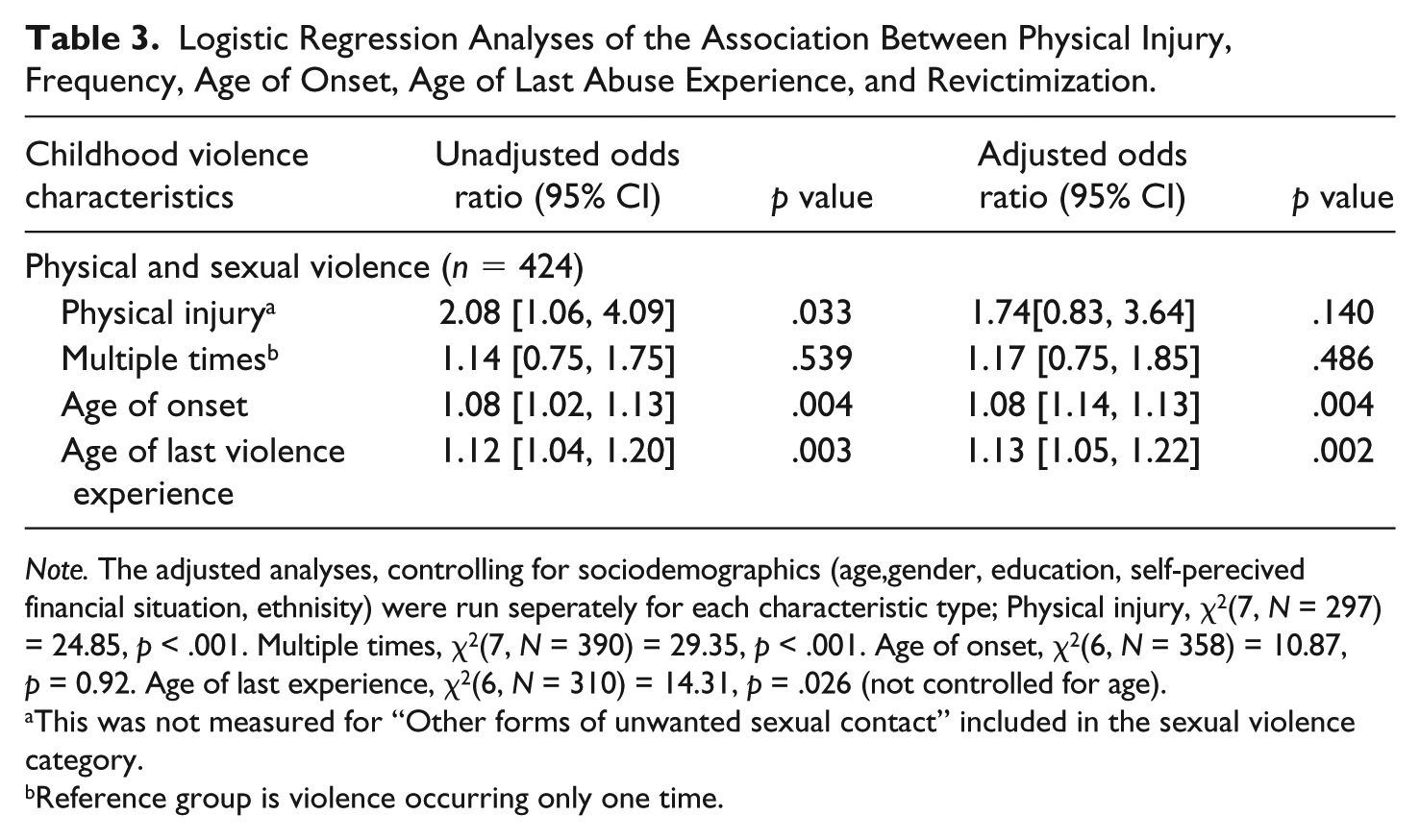
Note. The adjusted analyses, controlling for sociodemographics (age,gender, education, self-perecived financial situation, ethnisity) were run seperately for each characteristic type; Physical injury, χ2(7, N = 297) = 24.85, p < .001. Multiple times, χ2(7, N = 390) = 29.35, p < .001. Age of onset, χ2(6, N = 358) = 10.87, p = 0.92. Age of last experience, χ2(6, N = 310) = 14.31, p = .026 (not controlled for age).
This was not measured for “Other forms of unwanted sexual contact” included in the sexual violence category.
Reference group is violence occurring only one time.
Violence in Childhood After Age 18 Years and Associations With T2 Victimization
For those older than 18 years at T1 (n = 525), we investigated whether violence occurring after 18 years of age reported at T1 was associated with T2 revictimization, adjusting for sociodemographics. The individuals who had experienced both childhood abuse and violence after 18 years of age at T1 (N = 109) had the highest odds for T2 victimization compared with the individuals who had not experienced violence (Table 4). Exposure to violence after 18 years of age at T1 but no childhood abuse followed as having the second highest odds, while being exposed to only childhood abuse, and not to abuse after 18 years of age, was not significantly associated with T2 victimization. To explore this relationship further, we ran the analyses with each of the different categories as reference; T2 victimization was not significantly different between these groups (only compared with the nonexposed). There were two exceptions in which exposure to childhood abuse only (OR = 0.29; 95% CI: [0.16, 0.53]; p <.001) and experiencing only violence after 18 years of age at T1 (OR = 0.52; 95% CI: [0.27, 0.98]; p = .042) had lower odds of T2 victimization compared with experiencing both childhood abuse and violence after 18 years of age at T1.
Logistic Regression Between Experiencing Violence Before and/or After 18 Years at T1 and T2 Victimization (n = 525).
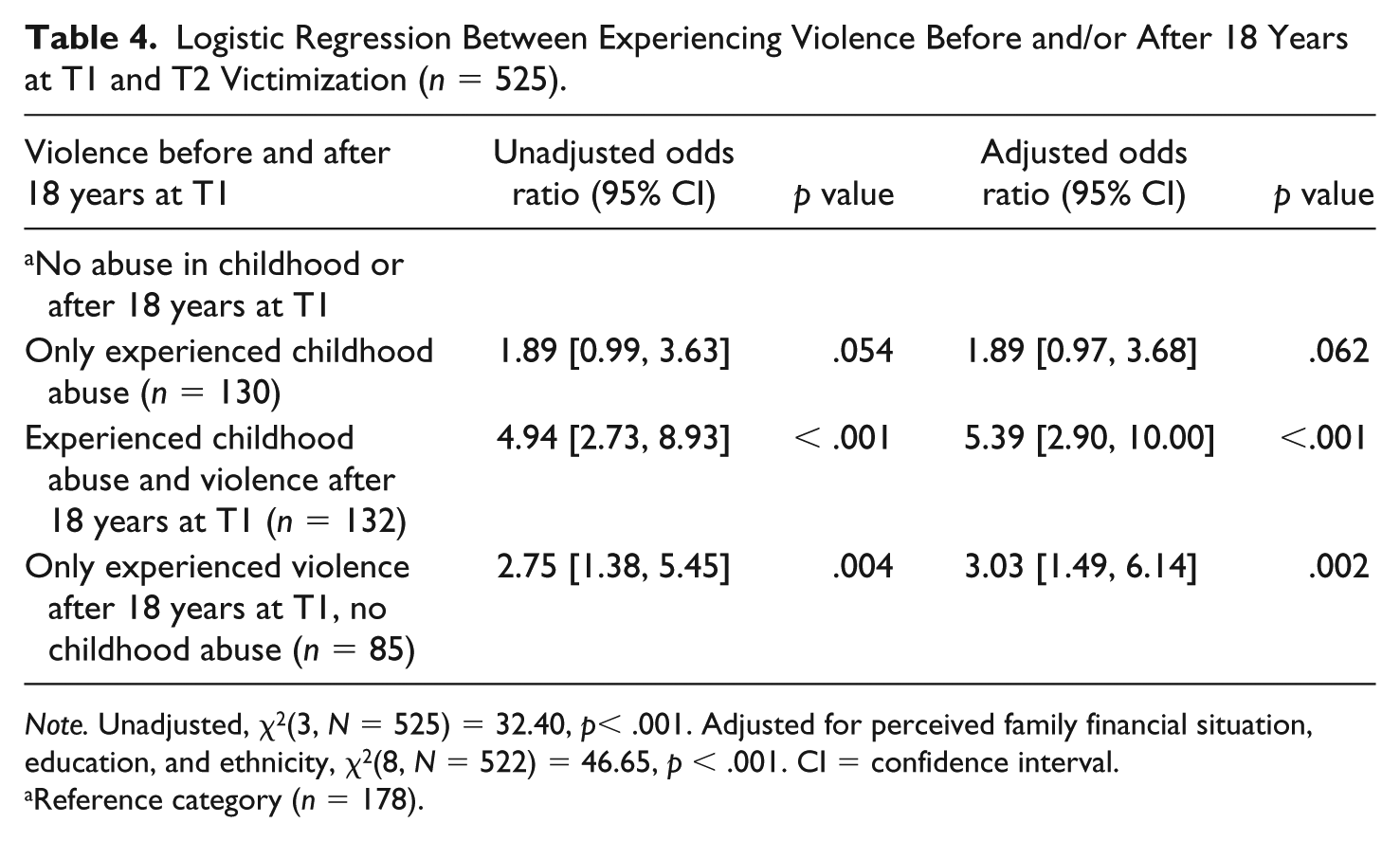
Note. Unadjusted, χ2(3, N = 525) = 32.40, p< .001. Adjusted for perceived family financial situation, education, and ethnicity, χ2(8, N = 522) = 46.65, p < .001. CI = confidence interval.
Reference category (n = 178).
Telescoping Effect
To explore the likelihood that our findings were due to a “telescoping effect” (distant events being recalled as more recent), we investigated whether there was an overlap between perpetrator and violence type in reports of T1 violence after 18 years of age and T2 victimization. Of the total sample (N = 1,011), 21.5% (n = 217) reported experiencing violence after 18 years of age at baseline (T1). Of these individuals, 13.4% (n = 32, of whom 29 are used in the analyses as three individuals overlapped, as they had reported both severe and less severe violence) reported the same type of violence (mild and severe violence, rape, and sexual contact) and perpetrator at T1 and T2.
Additional analyses of these 32 showed that for the less severe violence category (n = 14), the violence had occurred 2-3 years before T1 for three of the four individuals who had reported age of onset and last incident. Hence, it could be considered distant enough from T2 that continuous abuse/telescoping effect was not a likely explanation. For the last person, the violence had occurred over a 5-year period by a partner, including the year of T1, and consequently, continuous abuse/telescoping could not be excluded. For all violence types, violent incidents reported were rarely completely identical at T1 and T2. For example, the respondents could report multiple kinds of one violence type (e.g., sexual abuse) at T1, and then only one kind (e.g., rape) at T2, and the perpetrators could be partly, but not completely, overlapping. Consequently, it was difficult to determine whether the cases were potentially overreporting recent violence due to the “telescoping effect.” However, because of the uncertainty, a telescoping effect cannot be excluded for certain cases.
To avoid that the results in Table 2 could be due to a telescoping effect, the adjusted analysis was also run without those individuals who reported an overlap of type of violence and perpetrator after 18 years of age at T1 and T2. As a result, physical violence only and its combination with neglect/psychological violence became insignificant. The other results remained nearly the same with marginal reductions in OR (see the appendix). The sensitivity analyses (without those who reported such overlap) for the association between the number of exposure categories and T2 victimization did not change the results substantially; only small reductions in the ORs could be observed. In Table 4, for the analyses without the overlap of violence type and perpetrator at T1 and T2, the trend of the main findings remained approximately the same (see the appendix).
Discussion
Revictimization is one of the most potentially distressing consequences of childhood abuse. Investigating the factors that may lead to an increased risk of re-exposure to violence is thus crucial for preventing its occurrence. Our study, using a prospective design and a community sample, confirmed previous findings that childhood abuse victims have a higher likelihood of experiencing victimization in young adulthood compared with nonabused individuals. Adding to the existing literature, the results showed that revictimization does not only occur within sexual victimization. Rather, the different types of childhood victimization and T2 victimization overlapped, indicating that a broader perspective of revictimization is needed. Our data also showed that being exposed to multiple types of violence is common and that this exposure is associated with higher odds of experiencing violence in young adulthood compared with those in individuals not exposed to childhood abuse. These results reinforce previous findings that multivictimized individuals are at a particular risk of re-exposure to violence (Abajobir et al., 2017; Casey & Nurius, 2005; Coid et al., 2001; Jankowski et al., 2002; Thoresen et al., 2015).
Studying the specific forms of childhood abuse, we found that among the single exposure types, childhood sexual abuse had the strongest association with T2 victimization, which is consistent with the majority of the revictimization literature. Several studies have found a strong association between childhood sexual abuse and revictimization (Classen et al., 2005; Messman-Moore & Long, 2003). However, it is important to emphasize that the combination with neglect and psychological violence led to a 22-fold higher odds of T2 victimization (compared with a fourfold higher odds with exposure to sexual abuse alone), highlighting the need to study the different combinations of abuse experienced (Finkelhor, Ormrod, & Turner, 2007). Thus, sexually abused children may face increased risk if they are also neglected or psychologically abused by their parents. Childhood neglect and psychological violence have been understudied in the field of revictimization and, indeed, in the general literature on child maltreatment (Gilbert et al., 2009). Our findings underscore the need to further investigate these types of violence.
When the characteristics were adjusted for sociodemographics, we did not find significant associations between revictimization and physical injury and experiencing multiple incidents of abuse. The reasons for this are unclear. It may be that other characteristics not investigated in the present study are more important in regard to revictimization risk. Alternatively, it may be as Maker et al. (2001) argue: That simply being exposed to violence in childhood, regardless of severity, puts one at risk for further victimization. Similarly, Casey and Nurius (2005) did not find that the severity (physical injury, threats, use of weapon, feeling endangered) of the initial abuse predicts revictimization and concluded that women who are exposed to multiple types of abuse are most vulnerable to re-exposure to sexual assaults. This finding is consistent with our findings, which suggest that it might be more important to look at the number of violence types a person has been exposed to rather than the specific characteristics.
However, the adjusted analyses did show that an increase in age of onset and the last abuse experienced led to higher odds of revictimization. To further explore this finding, we looked at three groups of individuals who were older than 18 years at T1: (a) individuals who had only experienced childhood abuse, (b) individuals who had experienced both childhood abuse and adulthood abuse at T1, and (c) individuals who only had experienced adulthood abuse at T1. We compared these three groups with individuals who had not experienced these types of abuse. Unsurprisingly, the individuals who had experienced both childhood abuse and adulthood abuse at T1 had the highest odds for T2 victimization compared with the nonabused individuals. Moreover, the individuals who had experienced violence after the age of 18 years (but no childhood abuse) at T1 had significantly higher odds of revictimization than the nonexposed, while having experienced childhood abuse only (and no violence after the age of 18 years) was not significantly associated with T2 victimization. This is an important finding as it may imply that for those childhood victims who are not victimized in young adulthood, the risk of revictimization might be reduced. There have been mixed findings regarding the recency of abuse; some researchers have found that abuse earlier in life is more detrimental to experiencing further victimization, while others have argued that more recent abuse is a better predictor of re-experiencing abuse (Casey & Nurius, 2005; Collins, 1998; Himelein, 1995; Simmel et al., 2012). Our findings support the latter. Similar to our findings, Humphrey and White (2000) found in their prospective study that individuals who were exposed to sexual abuse in both childhood and adolescence had the highest risk of revictimization, followed by individuals who were victimized as adolescents but not as children. Maker et al. (2001) also found that having been exposed to both childhood abuse and adulthood victimization led to more detrimental outcomes. Although based on different age groups than those in the current study, these results emphasize the importance of studying re-exposure and recency of abuse when examining the risk of revictimization. The finding that the combination of childhood abuse and victimization in young adulthood (after 18 years of age) is particularly detrimental might imply, as previously suggested, that childhood abuse predicts adolescent abuse, which in turn predicts further victimization at T2. A person who continues to be re-exposed to violence may deal with unresolved trauma and thus remains vulnerable to additional abuse (Gidycz et al., 1993; Humphrey & White, 2000). However, this hypothesis does not explain why first experiencing victimization in young adulthood is significantly associated with further victimization, while exposure to only childhood abuse is not. The recency of abuse may be an indication of an individual’s negative trajectory and dysfunctional environment. A recent study found that being socially disadvantaged and having dysfunctional friends were associated with revictimization, while having social support decreased this risk (Strøm et al., 2017). These findings and others indicate that a person belonging to a negative social environment may be more vulnerable to revictimization (Banyard et al., 2002; Fargo, 2009; Gidycz, 2011), which may also be the case for those who experienced initial victimization in adulthood. In contrast, it may be that some childhood abuse victims have managed to develop a more positive trajectory and healthy environment as the abuse has become more distal, as previously argued (Himelein, 1995; Macy, 2008; Maker et al., 2001). Further research is warranted to investigate potential resilience factors among childhood abuse victims who do not experience revictimization to develop preventive efforts for childhood survivors of victimization (Macy, 2008).
Limitations
The strengths of this study include detailed measures of childhood violence and revictimization and the use of a prospective design and a community sample. The study has some limitations. Although using a community sample, the majority of the respondents were Norwegians, which resulted in a less ethnically diverse sample. We must be careful, therefore, with cross-cultural generalizations, even though the relationship between childhood abuse and revictimization may be less subject to cultural differences. The results on physical violence in Table 2 must be interpreted with caution as the sensitivity analyses (excluding individuals who reported the same perpetrator and violence type of victimization occurring in adulthood at T1 and T2, n = 29) demonstrated an insignificant relationship between physical violence and T2 victimization (see the appendix). We do not know whether these results are due to the telescoping effect, but we cannot exclude it. However, exposure to childhood sexual abuse remained a strong predictor for T2 victimization, despite controlling for the overlap. Confounding factors that were not considered in this study may have influenced our results, for example, relationship to the perpetrator (for sexual abuse), disclosure, mental health problems, risky behaviors, or social factors such as social support. We did not have the characteristics measures for witnessing violence, which led to missing information about this group. Although prospective data were employed, causality is hard to determine as a common causal factor cannot be excluded.
Implications
Individuals who had been exposed to multiple types of abuse in childhood and violence in both childhood and young adulthood were at a particularly high risk of re-experiencing violence. Practitioners need to pay special attention to these individuals and develop strategies that may reduce the risk of revictimization. Individuals who first experienced violence in young adulthood were also at risk of revictimization, which may imply that they have entered a negative trajectory. It is thus important for practitioners to be aware of the high revictimization risk that this group faces, despite not having experienced childhood abuse.
More research is needed to develop strategies aimed at preventing new victimization among those already victimized. Furthermore, our findings emphasize the need to focus on multiple types of violence in both men and women and especially the need to include childhood neglect and psychological violence. This group has been understudied in the field of revictimization; thus, more knowledge is needed. To learn more about the underlying mechanisms leading to further victimization, we need longitudinal studies where we can follow a set of individuals over time. This type of study will inform us about possible negative trajectories and allow us to build upon this knowledge for developing useful preventive strategies for revictimization.
Conclusion
Our findings show that individuals exposed to childhood abuse, regardless of type, are at risk of revictimization. Exposure to multiple types of abuse, repeated victimization, and recency of abuse increased this risk. Practitioners working with children and young adults may want to be attentive to those who have experienced multiple types of victimization in childhood and repeated victimization and also to the young adults who have experienced recent victimization considering their high revictimization risk. Future longitudinal research is warranted to examine the underlying mechanisms leading to revictimization among these groups. Finally, a broad definition of revictimization is needed, involving multiple types of victimization, both in childhood and in adulthood.
Footnotes
Appendix
Logistic Regression (Without Overlap of Violence Type and Perpetrator at T1 and T2) Between Experiencing Violence Before and/or After 18 Years at T1 and Revictimization (n = 496).

| Violence before and after 18 years at T1 | Unadjusted odds ratio (95% CI) | p value | Adjusted odds ratio (95% CI) | p value |
|---|---|---|---|---|
| a No abuse in childhood or after 18 years at T1 | ||||
| Only experienced childhood abuse (n = 130) | 1.89 [0.99, 3.63] | .054 | 1.93 [0.98, 3.81] | .056 |
| Experienced childhood abuse and violence after 18 years at T1 (n = 109) | 2.62 [1.37, 5.01] | .004 | 3.55 [1.76, 7.15] | <.001 |
| Only experienced violence after 18 years at T1, no childhood abuse (n = 79) | 1.96 [0.94, 4.10] | .073 | 2.59 [1.19, 5.63] | .016 |
Note. Unadjusted, χ2(3, N = 496) = 9.38, p = .025. Adjusted, χ2(9, N = 493) = 33.02, p < .001. Adjusted for gender, economic situation, education, and ethnicity. CI = confidence interval.
Reference category (n = 178).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Norwegian Ministry of Justice and Public Security, and the Norwegian Directorate of Health.