
Abstract
Despite high rates of domestic violence and increased rates of honor killing (HK) over the past decade, there is a paucity of empirical data about how HK affects family members. This study used grounded theory to explore the emotional and social effects of HK on 23 family members of murdered women and found that HK failed to achieve the restoration of honor. Following HK, families subsequently entered a protracted process of grief compounded by negative social interactions, which led to a form of “social death.” The road to social death was a painful and continuous social process, which, for many, never abated.
Introduction
In Palestine, women and girls continue to experience violence at home and within their society (Women Empowerment Centre, 2015). The prevalence rate of violence against women (VAW) in Palestine suggests that there is a high level of VAW committed by family members. Reports from the Human Rights Council (HRC, 2017) and nongovernmental organizations (NGOs) such as Human Rights Watch (HRW, 2006) and Amnesty International (2005) indicate that about 37% of married women had been exposed to violence by their husbands, and that there was a dramatic increase in honor killing (HK) cases during periods of political violence in Palestine (HRW, 2006; Palestinian Central Bureau of Statistics [PCBS], 2011). A correlation has been reported between political violence and increased levels of abuse against women in most of the national and international reports on VAW (Amnesty International, 2005; Hansson, 2008; HRC, 2017; HRW, 2006; PCBS, 2006). In common with other countries where HK is prevalent, in Palestine, female honor is enshrined in concepts such as virginity, modesty, or selfless love. Therefore, male honor is framed by the capacity to defend the honor of the female (Council of Europe Committee on Equal Opportunities for Women and Men, 2003). The Council of Europe Committee on Equal Opportunities for Women and Men (2003) defined HK as The murder of a woman by a close family member or partner as a result of (suspected or alleged) shame being brought on a family by the action (a suspicion or allegation will be enough) of the woman. (Paragraph 10)
Studies have discussed the nature and historical roots of HK in the Middle East, the United Kingdom, and Canada; identified factors contributing to its occurrence (Abu-Rabia, 2011; Ali, 2008; Andersson, 2003; Cinthio & Ericsson, 2006; Kardam, 2008; Kevorkian, 2000; Nimry, 2009; Terman, 2010); offered a brief description of the characteristics of both the victims and the perpetrators (Faqir, 2001; Hasan, 2002; Kardam, 2008; Kevorkian, 2000; Kulwicki, 2002); and have suggested possible strategies for combating it (Ali, 2008; Andersson, 2003; Belge, 2008; Edvardsson, 2008; HRW, 2006; Ishaq, 2010; Kardam, 2008; Kogacioglu, 2004; Kulczycki & Windle, 2011; Kulwicki, 2002; Miller, 2009; Patel & Gadet, 2008; Sev’er, 2005). The reviewed literature provided some theoretical perspectives on HK as created by different social attributes of honor versus dishonor, control, shame, gender, patriarchy, and religious interpretation that could be based on aspects of tradition and heritage (Faqir, 2001; Hasan, 2002; Kardam, 2008; Kevorkian, 2000; Kulwicki, 2002). Some authors have suggested that women in patriarchal society are sacrificed on the altar of “honor” because they have a cheaper social price for the family (Ali, 2008; Andersson, 2003; Cinthio & Ericsson, 2006; Kardam, 2008; Kevorkian, 2000). Because the concept of honor is so embedded in Middle Eastern countries and is connected with female virginity, “honor” was the most often reported cause for the killing of women in the studies we reviewed (Faqir, 2001; Glazer & Abu-Ras, 1994; Kevorkian, 2000). Terman (2010) found that economic conditions and financial causes were closely related to HK in Jordan. However, little is written about the effects of HK on families.
Palestinians are governed by a traditional patriarchal ideology (Abdo, 1999; Kevorkian, 2009). Many Palestinian scholars believe that the patriarchal structure of the Palestinian family and society is considered a primary contributing factor in regulating social behaviors, relations, roles, and responsibilities of members of the society (Abdo, 1999; Barakat, 1985). The family is the key social unit in Palestine and is revered within Palestine culture. The structure of the family has been noted to be patriarchal, patrilineal, and extended (Warnock, 1990), and Palestinians conceptualize their lives as parts of a family group, not as individuals (Warnock, 1990). The Hamouleh (often translated as “clan” or “tribe”) is a group of extended families claiming decent from a common ancestry (Warnock, 1990), which traditionally fulfilled many functions such as protection and support of individuals, as well as maintenance of law and order. The protection of the family, clan, or tribe names is paramount within Palestinian culture, and male domination of this structure is the norm. Patriarchy is a system in which men use various means or strategies such as force, direct pressure or ritual, law and language, custom, etiquette, education, and the division of labor (Warnock, 1990) to determine what part women play or do not play in society. Within Palestinian society and culture, behaviors by members of the family, particularly the behaviors of women that bring attention or shame to the family name, are dealt with severely. In terms of honor and the family name, those behaviors that suggest that a woman has deviated from the norm result in the severest of consequences. Actual or perceived are viewed similarly, as both bring dishonor to the family. In extremis, the male inside the family is responsible for deciding whether the girl or woman is to be killed if he believes she has damaged the family’s honor in any way (Garemani, 2003).
Two studies that have tried to interview victims’ families have reported that recruiting family members was difficult or even impossible (Edvardsson, 2008; Kardam, 2008). A family’s desire not to talk about the incident after the murder inhibited recruitment, and, as suggested by Kardam (2008), reaching families or threatened victims was risky and required having personal connections with people who were trusted by the families and who might be able to help researchers recruit potential participants. Similarly, Edvardsson (2008), in her study, faced the same difficulties as she could not interview either the threatened victims or their families, and instead, she interviewed mental health professionals (MHPs) who worked closely with the threatened victims. The experience of previous research regarding recruitment showed that it is difficult to obtain confirmed firsthand data on HK.
The attention given to HK and its conceptualization in the literature in the past several years could make it seem that this topic is well studied. However, reviewing the literature has shown that there is a lack of national and international research on the aftereffects of HKs on families and the consequences of this extreme form of VAW. The aim of this study is to examine the effects of HK on families. This research should go some way to improve MHPs’ understanding of HK and add to the body of knowledge about the effects of, and potential responses to, HK.
Method
Study Design
The study adopted a grounded theory methodology as developed by Strauss and Corbin (1990). Grounded theory investigates and explains social behaviors and clarifies the cultural and social contexts within which people interact and express meaning (Kaplan & Maxwell, 1994). A feminist paradigm focused on “giving voice” to marginalized individuals (Oakley, 1981) guided the data collection and analysis. The study aim was to understand the effect of HK on family members to uncover the social processes that exist in the aftermath of HK and extreme VAW.
Participants
The initial principal inclusion criteria were all adult family members (female or male) who experienced the murder of a female relative in an HK. Perpetrators were not excluded. The total number of participants who were recruited by purposive and theoretical sampling was 23 family members from 11 families; 15 neighbors were also interviewed making a total of 38 interviews. One interview was a group interview with five sisters who insisted on being interviewed together. They reported that this would help them to talk openly about their experiences and help them feel more relaxed. This created a “comfortable” environment for them, as we observed during the discussion. We noticed that individuals inside the group encouraged each other to talk, reflected on each other’s words, and sometimes added more details about some points. Professionals, including MHPs, police, and lawyers were also consulted during the study and excerpts from these conversations are also included with the study findings.
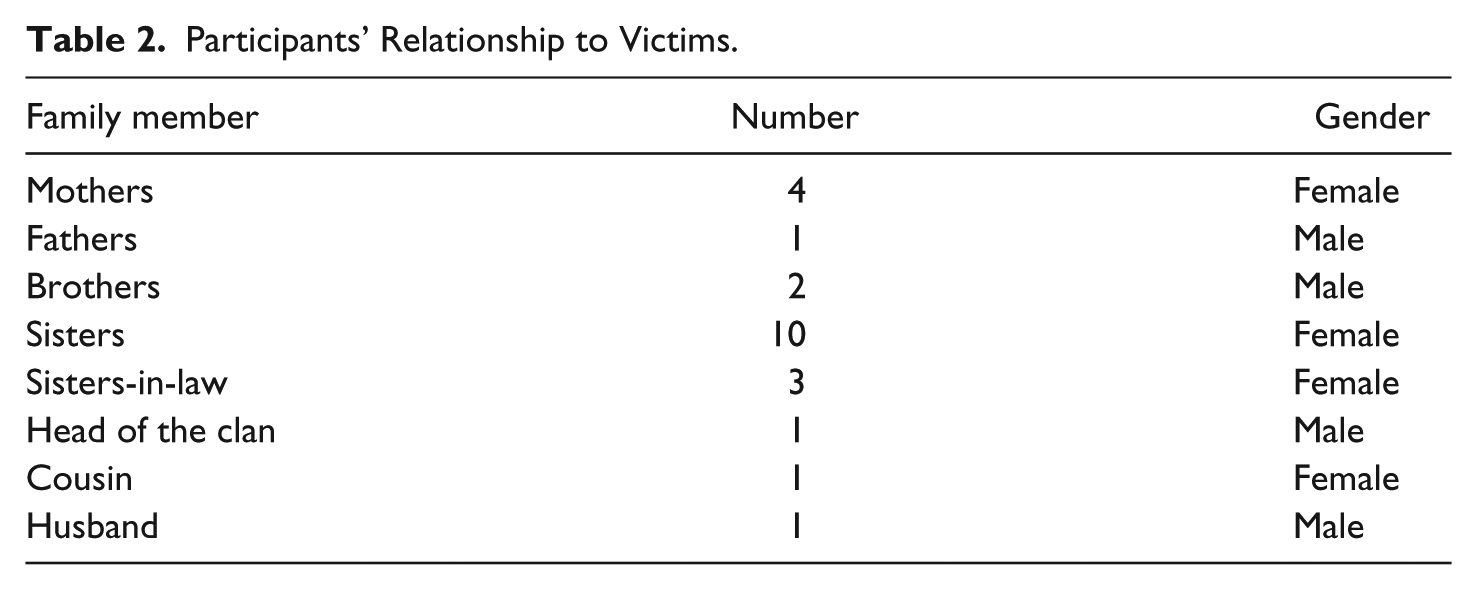
Table 1 provides an overview of the demographic characteristics of the family members. To achieve maximum sample variation, participants were recruited from across the country. They had different forms of residency (villages, refugee camps, towns, and cities) and were aged between 17 and 71 years. Participants were predominantly female. Table 2 presents the participants’ relationship to victims.
Demographics of Family Members.

Note. Size of family: small (one to five)/medium (six to 10)/large ≥10. Socioeconomic status: low if income is less than US$1.25 per day (Oxford Poverty and Human Development Initiative, 2010).
Participants’ Relationship to Victims.
Data Collection
Family members and health care providers were approached by staff from women-related organizations who provided them with information about the study. The potential participants were given 1 week to consider their participation and preference of the time and place of interviews. Prior to commencing data collection, two interview guides (available on request) were developed to facilitate interviews with professionals and family members. Based on topics from the available literature review, the topic guide was refined by piloting it with a small number of key stakeholders and modified in response to interim analysis (Glaser, 2001). Most of the questions were open-ended and related to participants’ perceptions of the emotional and social effects of HK on victims’ relatives, and how MHPs might best help. Individual and small-group semi-structured interviews were used as the main data collection methods in this study, which provided the opportunity for the participants to tell their stories.
Interviews were conducted following standard grounded theory procedures (Glaser & Strauss, 1968) and were influenced by the recommendations of feminist researchers about interviewing women (Oakley, 1981) to provide sensitive exploration of the key social processes. More specifically, the interviewer used active listening and reacted positively to comments to enhance the communication process, using phrases such as “tell me more” and “help me understand this some more,” as well as culturally appropriate nonverbal communication. The interview was started with a warm-up by asking friendly questions and general chat, and when the conversation flowed, moved into the interview proper with the question, “I would like to start by having you tell me your story?” This was followed by questions such as the following: Can you tell me about your experiences after the murder? How did the people around you behave with each other and your family after this incident? and Would you like to tell me more about how this event affected the life of your family in comparison with life before the event?
In general, interviews lasted between 30 min and 2 hr and indicated that participants were comfortable and willing to share their experiences. Interviews were audio-recorded with participants’ permission and subsequently transcribed verbatim.
Ethical Considerations
Ethical approval for the study was granted by the Committee on the Ethics for Research on Human Beings at the University of Manchester (ref. number is 09/1026/NMSW). Anonymity and confidentiality were safeguarded by undertaking several procedures, such as the removal of identifying information and the use of pseudocodes for participants and their settings. Data were kept in accordance with the University of Manchester’s policies compliant with the Data Protection Act (Information Commissioners’ Office, 2014), and all audio-recorded discs and transcriptions were kept in two locked cabinets. Furthermore, a distress policy was considered prior to starting the data collection, and arrangements were made with the women’s institutions for expert help to be made available if emotional distress occurred during the interview process.
Data Analysis
Data analysis was conducted iteratively, starting simultaneously with data collection. The initial stage of the analysis used open coding; open coding facilitated the creation of preliminary categories, which are part of the conceptual data. In the second stage, axial coding involved developing and regrouping the codes and the links between codes, resulting in the subcategories. Selective coding was the third stage of data analysis and involved further iterative processes, whereby categories were linked to form the generation of a tentative theory. Constant comparative analysis (Strauss & Corbin, 1998) was undertaken to enhance sensitivity by questioning the data, looking for relationships and interactions between the data and other sources to ensure that we maintained openness and a willingness to give voice to the participants following the processes advised by Strauss and Corbin (1990, 1998). Analysis was assisted by use of NVivo-8 software (QSR International, 2008).
The rigor of the study was maintained through various strategies. For example, the three researchers were involved in the data analysis as three of the interviews were coded by the research team separately. Then, coding was compared to enhance credibility. Transferability was obtained through thick description that helped in providing the context, intention, and meaning that was gained from the experience, and exposed the experience as a process. Process and theoretical memos were made contemporaneously with data collection and were reviewed periodically.
Results
A grounded theory of “social death” emerged from the study together with two related themes: facing the reality of death and the effect of social ostracism and exclusion. Figure 1 presents the basic social process involved in the theory of social death. It was found that most family members experienced difficulties and disruption to almost every aspect of their individual and collective lives. To summarize the theory, the basic social process of social death explains the experience of bereaved family members and what happened to them following the murder of their female relative. It explains how family members live with the effects of HK. Because of social death, they face a new reality and experience social ostracism as subprocesses of underpinning and contributing to social death. In the “Results” section, quotes will be referred to as FM for family member followed by relationship to victims, number of the interview, F as female, M as male. Figure 1 presents the basic social process of social death.

Effect of HK on family members: Social death.
A summary, Table 3, is presented including the themes and subthemes.
A Summary of Themes and Subthemes.

Facing the Reality of Social Death
The theme, Facing the Reality of Social Death, describes the experience of family members as they encounter the emotional effects of HK. It indicates that following HK, family members must simultaneously face the emotional consequences of losing their female relative and their failure to achieve the anticipated respect from their close-knit society. This theme is built upon four subthemes, which emerged from the data: keeping of bonds, ongoing suffering (lasting pain), anger and vengeance, and loss of security.
Keeping of bonds
In light of the violent nature of HK and the fact that some of the family members were present at the time of the murder, it is not surprising that some participants became preoccupied with thoughts of the victim. Some of the participants reported recalling upsetting memories, yearning, longing, and searching for the victims, as the following excerpt indicates: We miss her always. I could not forget her. She is always around. In the last feast, I and my sisters were here dancing and laughing and suddenly we remembered her and the three of us started crying. (FM2, Sister, F)
Bereaved family members felt guilty as they continued with their lives under the watchful eyes of the community. One of the mothers gave the victim’s name to her new child and named the room where the victim used to sleep with her name, maintaining a continuing bond with her daughter. Many looked at surviving relatives for characteristics of the deceased: Look at my youngest sister, she looks like her. My mother named the room where my sister was sleeping with her name. (FM4, Mother, F)
For bereaved families, keeping connections and maintaining bonds constituted a means of acting against social rejection and continued stigmatization by the community and was evident among many of the participants. Thus, keeping a connection gave the family members emotional energy emanating from the pain of losing both the victim and their social status.
Mementos of the deceased were commonly used to maintain a sense of connection with the person who was taken suddenly and violently: I kept her pictures and put one of her pictures in the front of the main entrance to tell everyone that I was against the killing of my daughter. I lost my relatives after the murder and they talked about us, I want her uncle to suffer when he saw her picture and to know that I adored my daughter. (FM5, Mother, F)
The findings also showed that continuing bonds to the victims were maintained by keeping a physical attachment, through visiting the grave when this was allowed or sanctioned by the community. The mother also dressed in black for more than 2 years; this is meaningful because the cultural norm is to do this for only a year. This practice reflects a feeling of sadness and respect for the memory of the deceased. The ostentatious observance of grieving and funeral rites, when it was possible, functioned as a way of signaling love for the victim and disapproval of the killing—indeed, a form of resistance to the prevailing mores of society: The mother and the sister wore black dresses for two years—could you believe that she slept in the cemetery for a year? (FM18, Cousin, F) One of my sisters always wears black clothes. She cares about people’s talk when all of us are going to visit her grave; we wear black because we walk through the camp. At the time of the killing, many people came to console us because they liked her. (FM, Sisters’ focus group)
The prevailing expectation was that the bereaved families of HK victims should not grieve openly. Continuing bonds with the deceased were reported by some of the participants as a significant element in their grief process, whereby family members continued to relate to the victims as active and living memories at times of success, happiness, or even personal distress or crisis: Her brother visited after he was released from the prison. You know once my son fought with his father and disappeared. We looked for him for a whole day then discovered that he was there, he was in the cemetery. He always goes there when he is stressed. (FM5, Mother, F)
Many of the family members had to develop ways of maintaining often hidden or unique connections with the deceased, in contrast to those who were allowed and or able to visit the grave in the usual way to show respect and continued contact. For example, some reported that they usually cried alone or even woke at night to hold the victim’s pictures because they were afraid that anyone in the family would see them: Every night I went to my room and hold her picture and cried alone, it is five years now and I still miss her but I am afraid to do this in front of my brother. (FM11, Sister, F)
Ongoing suffering (lasting pain)
Feelings of despair or deep sorrow were commonly expressed by participants. Despair occurred when family members realized the impact of the murder on the family. Some of the participants described severe emotional effects of murder on their own mental health. However, the severity of the reactions changed little over time and linked with the gender of the relative and their family members’ previous relationships with the victim. One participant reflected: You know, I am one of the relatives and I noticed that even if the murder was before five years ago, and ‘til now you will see the sadness on her mother’s face, she tried to laugh in front of us but you will feel that. She was the youngest and her mother was closely attached to her and overly protective over her. (FM18, Cousin, F)
Feelings of sadness and distress persisted; these were related to the social consequences that constrain the lives of the family members. This happened because of their inability to express their sorrow and remorse at the loss of their loved one for fear of reaction from others. All family members and even the mother were accused by the close-knit society for the brutal killing. The mother felt unable to share her sadness of losing her daughter out of fear of her sons’ reactions: Do you think that I did not feel sorry at her loss? Sometimes I cried alone because I did not want my sons to see me crying about her because they will be angry at me. (FM7, Mother, F)
It seems not only that the violent loss of the victim increased their pain but also there was an inability among family members to explain the cause of the killing, especially younger members such as siblings of the deceased, showing that the issues and effects remain strong a long time after the event: She just went to bring food to her children and they killed her, no one could accept to kill a mother like this. They shot her from her back. Why she was killed? No one faced such experience. What I have to tell my youngest brother and sister about it when it is extremely difficult for me to understand it? (FM, Sisters’ focus group)
The process of grief had to be conducted/experienced in private and away from the judgments that would be invariably leveled against the family by the community: After what happened, I isolated myself for three months. I was in pain for losing her. I could not talk to anyone about my suffering. After all of that I could not walk in front of people. I felt of low self esteem and self worth. I felt sad always. I still feel embittered by her loss. I am a helpless father who could not believe that his angel was killed like this. I wish that she is still alive. (FM14, Brother, M)
Facing the reality that killing their female relatives did not change their social status, but rather led to their alienation from the close-knit community, was not easy for family members and intensified their feelings of guilt and ongoing pain for supporting and not preventing or warning the victim.
Anger and vengeance
Anger was frequently experienced because of the loss. Anger was mentioned by almost all family members in this study, and was often described as problematic and troublesome for participants. Anger, suppression, and resentment were cited as the most extreme and severe reactions to loss and the murder: I was angry about her murder. I am still angry at him [the killer] but I suppressed my emotion when he came to our house. (FM19, Sister, F)
Family members perceived themselves not only as mourners but also as victims. They had lost their loved one in a violent death and the society was stigmatizing and treating them as “deviants or outcasts” (MHP, F5). Facing the reality of those intense feelings may be the reason why some family members secretly wanted to take revenge; they connected their emotional resolution and healing with revenge, as the following highly charged excerpt demonstrates: I am a mother who wants the justice. I want him to be punished but I know that there is no justice in this life. My only hope to see him hanged in the middle of the city. (FM6, Mother, F)
The intense feeling of anger implied that family members turned their anger inward when they were prevented from directing it outward. To be angry in public would be to take sides against the perpetrator, and this was not acceptable. Respondents reported that they had to be seen publicly as agreeing with the crime to appear united. This led to further judgment by the community and further ostracism.
A loss of security
When the perpetrators were not punished (as in most cases), this had a significant effect on the family members. For some, the relationship with the perpetrator and his continued presence among family members led them to feel insecure. Living under the threat from within their own social network exacerbated the suffering they experienced. In two situations, where the perpetrator was either a blood relative (such as a father or brother) or husband, or a politically affiliated person, their presence within the family amplified feelings of fear: After the killing of my sister, I lost the sense of security, even with all the family around I could not feel safe. My relationship with my father was affected too much. I don’t love him. My brother always fights with him and leaves house when he is around. (FM2, Sister, F)
Feelings of insecurity happened because female family relatives were subjected to monitoring and control by perpetrators and other family members as they were afraid for the family reputation and from further social rejection: Her sister was extremely followed by her brothers. They always checked her mobile and calls. They took her to her school and returned her back. (FM17, Head of clan, M)
Guilt and facing the reality of social death
Guilt represents a sense of responsibility for having harmed others, in this instance, the loved ones murdered in HKs. Facing the reality that killing their female relatives led to social death in regard to the community was not easy for family members, which intensified their feelings of guilt for supporting and not preventing or warning the victim. Because of guilt, individuals face ongoing suffering and distress. Some of the families mentioned their shock relating to the murder. The suddenness of the murder can sometimes feel like a physical assault. Sensing the danger before murder among family members and their inability to anticipate and prevent the killing might contribute to guilt afterward: Maybe if I told her about that dream she will be alive now because she will be careful. I feel guilty because of that I am the only one who did not see her in my dreams. I cry always because I could not. My conscience torments me. (FM, Sisters’ focus group)
In the example above, the origin of the guilt was linked with the participant blaming herself for not telling the victim about an inauspicious dream she had. In turn, participants talked excessively about their sensing of danger and that there was evidence signaling the murder. Some of the participants, mostly female, mentioned that they felt that the victims were in danger before their murders. Family members were often sensitized to the threats that occurred before the murder and were frightened for the safety of the victims. However, sensing danger (which means sensing or feeling that the victims were in danger) does not mean that family members were well prepared for the violent death, despite the severity of the anticipated danger. Most family members did not expect the extent of the family reaction or that they would kill the victims, as exemplified by the following quotation: He came and told my mother that he will cut her body and bring her in a bag but my mother thought that he was not serious but he did it. (FM19, F)
Except for other family members who supported or participated in the murder, family members reported that their feelings of guilt were expressed indirectly by reporting that these HKs could be prevented. This was compounded by the fact that their close-knit society abandoned them and left them alone in their struggle: I believe that they became killers by chance, they were shocked and found themselves in social circumstances that forced them to kill. After that they had conflicting emotions, I met a perpetrator who was psychologically affected because he killed his sister who was raped by one of her husband’s uncles. Another one said that at first he was not sorry for killing her but after that he started to think of her always, felt sorry to kill her and always cried at her. (Police officer 1) Their eldest brother came many times and cried heavily at this sofa. He said that people pushed them to kill but rejected them after. This family was executed from the society and destroyed completely. (Lawyer)
The Effects of Social Ostracism and Exclusion
Social ostracism describes the varying degree of difficulties in interactions with interpersonal relationships within the close-knit society, such as humiliation and social stigma. In response to this, family members employed self-protective behaviors to live with their own social death. Two subthemes emerged from the data: altering communication, and social stigma and community rejection.
Altering communication
The violent deaths associated with HK affected interfamilial relations and led to changing roles inside the family, which disturbed normal relationships. Family members found themselves facing new challenges that affected their relationships with people around them, leading to changes in their way of life. A loss of communication among family members was stated clearly by participants: My husband did not say anything and I did not ask him about anything. In reality we lost communication among us after what happened and no one discussed anything with anyone. (FM7, Mother, F)
Some family members could not live with the ongoing stigma, which was echoed daily within the household. Some got divorced after the murder and others were not able to communicate with each other openly: I and my husband were divorced after the killing of my daughter. I could not look at his face at all. But I was forced to return back to him again for the sake of my children. (FM7, Mother, F)
MHPs also mentioned that murder led to altered interactions and noted that one of the fathers divorced his wife after the murder of his daughter and prevented her from seeing her children: Family function and its interactions patterns are affected badly because of pain inside family, divorce of the mother or sisters, mental disorders or illness, isolation of the family and boycott of them and preventing mothers from having contact with her children after divorce. (MHP, F6)
Family relationships and communication broke down through guilt and anger when they discovered the victim’s innocence. This was compounded by the fact that their close-knit society abandoned them and left them alone in their struggle following the murder: They started to blame each other for the killing after discovering that she was a virgin. I told them that I trusted my girl but they did not believe me and insisted to kill her. Her eldest brother many times came to the office blaming himself and cried. He said they were unaware what the meaning of killing a human soul is. (Lawyer, M)
The data also showed that bereaved family members had little ability to provide emotional help to each other, and despite understanding the importance of open communication, all of them preferred avoiding the subject: My sister does not talk too much and I don’t like to talk about the past to not hurt them. We were distant from each other emotionally. Look to tell the truth I was not close to my mother before that because she sometimes talked nonsense things. (FM16, Sister, M)
The data here demonstrate how HK affects the family unit in terms of communication within the home. The effects are far reaching and range from lack of communication to estrangement and divorce where families are torn apart.
Social stigma and community rejection
Families felt stigmatized because the community judged them negatively, although some family members felt that they had done nothing wrong. Feeling socially stigmatized induced shame: We were ashamed because of her behavior. We started to be as “the sheep that were infected with scabies.” All the people around us did not talk with us because of her. (FM7, Mother, F)
Although HKs were sanctioned and encouraged by the community at large, following the crimes, the community stigmatized family members because crime is always treated as deviant behavior by the community, and consequently, individuals label people involved in these crimes (either family members or perpetrators) as deviants: I am from a village; any rumors could affect us as a whole. Even if I am their cousin but my husband advised me to not be in contact with them to avoid my in-laws’ talking. (FM3, Cousin, F)
The latter quote illustrates that the extended family was fearful that association with the family might tarnish their own reputation and social standing; thus, they considered it safer to avoid them. For the families who were the target of these efforts to maintain a distance, they felt stigmatized and acknowledged that they were very different from the rest of the society. Feeling like a pariah was expressed by the participant: People treated us as criminals—they look at us differently. (FM1, Sister, F)
In general, friends and relatives are the major source of support for bereaved families. Because of the murder, not only were family members rejected by close-knit community but also their close friends showed a lack of sympathy, support, and toleration of the families’ grief: No one cares or shows kindness toward us. No one asked about us, I do not care about any one of them, because no one pitied or showed compassion to us. We were shocked because of our neighbors’ reaction; they did not support us they just gossiped about us. (FM, Sisters’ focus group)
Some friends and neighbors also actively blamed the family members and avoided them: They blamed me for what happened, no one came to visit me not even my closest friends. (FM12, Husband, M)
One participant mentioned that the social rejection, ostracism, and rumormongering of the local community extended into the employment arena, emphasizing that the stigma goes beyond individuals’ experiences, the whole family, or local community and affected their interaction with the larger society as a whole. Citing that the stigma of her sister’s death led to people refusing to employ her: I could not find a job since that time. When people knew the story, they refused to hire me. (FM1, Sister, F)
Sometimes when people knew that one of the family members died by HK, they fired them from their jobs because of their fear about their own reputation; this further contributed to the progression toward social death. The bullying and criticism of children were observed, and these intensified their grief and suffering, and led to many difficulties. Some children started to become aggressive, whereas others isolated themselves from the surrounding community or had regressive behaviors such as enuresis: My children were kind, but other children abused them. Once, my daughter fought with her cousin who used to irritate her by accusing her mum’s behavior to be socially unacceptable. She started to have problems since that time she was always afraid she did not go outside. She is 14 years old and urinated in her bed at night. (FM12, Husband, M)
It is easy to see why families responded to this intense stigmatizing process by withdrawing and avoiding contact, which further compounded their social death within the community. The extent of social ostracism by the community even affected the youngest family members. Not only did the victims’ children face difficulties with their siblings and close community but they were also prevented from having any kind of relationship with victims’ families. Preventing the victims’ children from seeing the victims’ maternal family members left a lot of psychological pain: When I saw her eldest daughter, I remembered her she looks like her. I felt happy when I have the chance to see her children. Their uncle and aunts sent them to one of the shelters and refused to let me see them even there. (FM11, Sister, F)
Although those children lost their mother, their father’s family prevented them from having contact with their mother’s family and preferred to send them to one of the shelters rather than keeping them with their grandmother. This showed the extent to which some families would go to distance themselves from their in-laws, meaning that not only the victims but also their children and their family were treated harshly. This represents another source of isolation and social judgment.
Their feelings of a loss of respect, along with longing for the victims, played a major role in family members’ desire to die, and this reflected how murder affected their social standing. Wishing to die was also associated with feelings of helplessness as a result of extreme social stigma and community rejection of family members and particularly male members: I wish to die when this happened with me. No one respects us since that time. (FM8, Brother, M)
Discussion
This study addressed the effect of HK on family members in Palestine. The key finding in this study is that, contrary to the expectations of perpetrators, killing female relatives generally did not achieve the goal of restoring family “honor.” Close examination of the family members’ lives and views revealed that their social standing and their family honor did not improve after the murder. On the contrary, HK weakened the families’ reputation, isolating them from their close-knit communities, compounding their social marginalization, rejection, and stigmatization.
The consequences of social death extended beyond emotional and social effects on individuals to include the family and their relationships with friends, neighbors, and the whole community, which resulted in them being labeled and stereotyped in their community. Family members described many sources of stigma. Major sources included family, friends and neighbors, school, and the job market. Social death constitutes a shift in social roles, social status, and the breakup of relationships, whereby the individual is treated as if they were dead. Therefore, family members felt powerless, unable to resist social death, which emphasizes that social death and its related elements, such as exclusion and stigma, are part of a complex social process.
Social death is linked with the competition of power. Palestinian society condemns immoral behaviors such as behaving against the honor code of modesty and, at the same time, condemns HK. Both acts are treated as shameful, thus creating difficulties for bereaved family members who, as survivors, face two undesirable alternatives: being labeled as a family in which an HK and immodest behavior have occurred, thus being ostracized, or avoiding mentioning the loss, therefore contributing to the social death of their loved one and themselves, and ultimately shame and stigmatization of the family and the wider clan. This can be explained by understanding the effect of stigma on an individual, as theorized by Bulhan (1985), who asserted that people who faced multiple layers of social disadvantage may find it difficult to challenge their stigmatized status. Therefore, we suggest that the “social death” theory be considered not so much as a homogeneous category, but rather as a more complicated set of relationships, which should also be seen in terms of the social and cultural contexts in which they operate. This study captured the complexity, diversity, and idiosyncratic quality of the grieving experience among family members. It addressed the multiplicity of physical, emotional, and social needs experienced by the bereaved family members and intimate networks.
The concept of social death has some empirical support in the sociological literature. Studies on the plight of slaves in the past and people who have been trafficked for sex work have noted that in the process of importation they experienced a form of social death (Androff, 2011; Brown, 2009; Marshal, 2012; Patterson, 1982). Others have found that a process of social death occurs in people in the later stages of dementia, where social ostracism and avoidance by their others occur as the disease progresses (George, 2010). There is also literature about long-term caregivers who experience a form of social death (see, for example, Holley & Mast, 2009). Social death in these circumstances reflects elements of the ostracism and stigma that have resonance with this study. However, studies specific to HK and the aftermath have not addressed the process of social death to any great extent and, therefore, this study contributes to a new understanding of this process within this context. Three studies about HK (Ali, 2008; Kardam, 2008; Kevorkian, 2009) and a further three studies of bereavement (Asaro, 2001; Burke, Neimeyer, & McDevitt-Murphy, 2010; Wilsey & Shear, 2007) mentioned briefly the experience of losing family members as a result of murder. These studies indicated that bereaved family members felt isolated, sometimes stigmatized, and that they might be viewed more negatively by others in their social network where stigma is often accompanied by shame.
The Palestinian community is like other Arab and Muslim countries, with distinctive social support characteristics including large community network size and mourning ritual systems, whereby large groups of visitors pay their respects to the deceased (Hedayat, 2006). Displays of sadness indicate to the community the loss of a valued family member. Others habitually look after and relieve the bereaved from basic duties during a mourning period, by offering help to the family (for example, by cooking meals for them) (Hedayat, 2006). Therefore, social interaction and social support are deemed necessary for grief resolution. However, like the findings from previous studies of homicide (Burke et al., 2010; Dyregrov, 2004; Wilsey & Shear, 2007), bereaved families of HK in this study were abandoned, humiliated, and socially ostracized from their communities. In this study, community judgment and interactions with family members raised many issues concerning family members’ reactions to the loss of their loved one, which together created new complications for the bereaved and the process of grieving.
The data presented in this study have offered an in-depth examination of these processes, which form the core category of this grounded theory. Many studies have shown that the circumstances of death are liable to negatively affect the grief process among the bereaved family and lead them to experience social death that includes social sanctions (McIntosh, 1999; Mulkay, 1993; Niehaus, 2007; Wertheimer, 1991). In addition, some of the bereavement literature notes that those deaths involving suddenness, interpersonal violence, trauma, suicide and, most importantly, acts of “human design” are more likely to create exaggerated and potentially complicated grief responses (Asaro, 1992, 2001; Burke et al., 2010; DeRanieri, Clements, & Henry, 2002; Rando, 1993; Redmond, 1989). Similarly, participants in this study reported ongoing pain and feelings of the senselessness of death accompanied by their feelings of self-blame and guilt. This was framed against a cultural background of stigma and ostracism by their close-knit community, who also blamed them for the murder.
Family members construct two kinds of bonds. First, it is a private bond that involved emotional involvement with the victims characterized by talking with the deceased victims, holding their photographs, crying silently, and thinking of them constantly. Family members’ compliance with social stigma is explained by Crawford (1997) and Joffe (1999), who highlight the processes through which the individual and the social are inextricably intertwined in the construction of stigma. They argue for a universal human fear of uncertainty and danger, which is associated with the overlaying of stigma. Individuals project this onto identifiable out-groups, responding negatively toward them to distance themselves from the threat (Crawford, 1997; Joffe, 1999), which further adds to the ostracism and social death.
Second, it is a social bonding, which is related to social expectations of bereaved families such as displaying mourning rituals, when permitted, visiting graves, wearing black clothes, and hanging victims’ pictures, or even leaving the possessions of the deceased untouched. However, both kinds of bonding are not culturally permitted or acknowledged by the society or family members, bringing more intense emotional discomfort among family members where HK has occurred. The externalized and internalized keeping of bonds suggests the complex interaction process and the multiplicity of forces at the community level in establishing and maintaining stigma and the road to a social death. Social death plays an important role in maintaining connections and bonding with the deceased and with family members’ need to externalize a continuing bond because they wanted to show the community and perpetrators that their deceased was honored and loved. At the same time, it is their way to punish the perpetrators for bringing more shame to the family and to remind them of the tragedy that they have brought on the whole family.
Most of the participants reported ongoing and lasting pain, guilt feelings, and anger that pose a barrier to the healing process. This is similar to the literature that has been associated with suicide and other types of traumatic death, which supports the evidence that the pain of dealing with the loss of a loved one by suicide and traumatic death is associated with shame, rejection, anger, perceived responsibility, and other risk factors and can be too much to bear (Hibberd, Elwood, & Galovski, 2010; Young et al., 2012; Zisook et al., 2010). As concluded by Asaro (2001), while the victims’ pain and suffering end with death, it is only the beginning for those left behind in the chaotic aftermath. The study reported here is one of only a few that explores the emotional effects in depth and, therefore, adds to the debate.
Implications for Practice
Family members’ and close-knit community members’ descriptions of the experience of the bereaved family members provided useful information that MHPs can utilize to better meet the needs of the bereaved families. The interpretation of the findings leads to the conclusion that bereaved family members can benefit from sharing their experiences through counseling and by making themselves available to help when needed. In addition, they need to find ways to incorporate memories and bonding activities that enable them to keep the memories of the victims alive to honor them. Therefore, MHPs can explore family members’ perceptions and meaning of bonding activities, cultural practice, and memories, and find ways to accomplish these tasks. Gaining an awareness and understanding of the lived experiences of the bereaved families from HK will enable MHPs to provide the proper and additional professional help to assess their needs and to facilitate their handling of grief.
MHPs can better develop programs and interventions for bereaved family members, regardless of how the interaction between them and family members occurs, reducing the social stigma surrounding the issue and working to finally break the silence regarding their experiences.
In addition, VAW and particularly HK can be prevented, and therefore, political commitment to tackling HK is vital to the mental health effort. Sustained efforts must be made by various policy makers in the society to tackle HK, such as NGOs, governmental organizations, and individuals, in addition to truthful efforts by the Palestinian authority itself in adopting policy and legislative measures to prevent the occurrence of HK. Although the study showed that bereaved family members were stigmatized after HK and marginalized by their close-knit society, protective services should provide resources that focus on the most vulnerable and marginalized groups to prevent violence, social rejection, and mental health impacts.
Strengths and Limitations
Although this qualitative study has provided a detailed account of the experiences of family members’ aftermath following HK, as with any study, it is subject to limitations. Qualitative studies are relatively small in scale and focus on a limited number of individuals in a particular setting, context, and time. Thus, the transferability of findings to other settings may not be guaranteed. The developed theory is specific to the study sample from which it was developed. To enhance the theory, we included a wide demographic of participants to ensure variation in the developed theory. The theory presented here can be developed in other contexts, which may allow for transferability and further refinement and enhancement. Lack of control for socioeconomic status is problematic when determining the broader applicability of the findings from this research. However, a concerted attempt was made to solicit participation from various age groups, genders, settings, and families, ensuring that the resulting sample was diverse. The sample may be enhanced by inclusion of male and female MHPs and other key informants from the society. In addition, family members who refused to participate in this study may have recovered better than those who agreed to participate and, therefore, future research may examine the validity of this assumption. We were relatively successful in interviewing male members, but the number of male participants was still half that of the females interviewed. This could be due to several reasons, including their need to bury the story, as men typically supported or motivated the HK in the first instance. It is also possible that sometimes they did not want to show their pain, as men differ from women in the expression of their emotions (particularly in traditional societies; Qasem, 2010), and they also have greater fear for their family reputation and concerns about confidentiality (Al-Krenawi & Graham, 2000). They might also be reluctant to talk freely about their emotions to a female researcher. Although interviewing more male participants was a challenge in the study, it was deemed to be an important aspect. Family members in this study reported that they did not have the opportunity to talk about their experiences to others or to MHPs. MHPs mentioned that their previous experiences with some families were problematic and, thus, they could not provide psychological support to them. Thus, such research gives the participants a genuine experience to reflect upon their life. Participants in this study reported that interviews enabled them to find new directions and increased their self-awareness.
Conclusion
The study focused on family members’ experience after HK and highlighted that, in addition to dealing with the loss and change, family members have to cope with other emotional effects, fear, humiliation, and stigma surrounding HK. A unique finding in this study was that death from HK complicated grief by adding shame to other painful emotions associated with bereavement. Over time, family members learned from the tragedy of the loss and how to deal with its consequences (such as social death) rather than recovering from their loss. They learned how to mediate their suffering, but they could not attach a meaning to the loss or find any positive outcomes. Over time, their pain may have lessened but it never ended, which means that in bereaved families’ experiences of HK, time does not heal, and wounds remain. For the families of victims of HK, the road to social death was a painful and continuous experience which, for many, never abated. This suggests that there is still a long way to go in identifying and meeting the needs of families bereaved through HK.
The findings of this study suggested that the cultural factors that led to social ostracism and rejection following an HK was stronger than the perceived rejection within the community caused for not “punishing” the female for reputedly tarnishing the family honor. Although there may be some families who are able to hide their perceived shame and dishonor from the wider community, there are those who cannot. We do not have data on those who can and do avoid the cultural encounters associated with dishonor and shame, and this would be an important, if methodologically difficult, study for the future. Yes, it is clear from the data presented here that many families, within Palestinian culture still believe that HK can be the right choice to regain cultural acceptance and respect within their culture and society. However, the data presented here suggest that the experience for families (whether they supported or were against the killing) suggests a difficult and painful journey following HK. Perpetrators, male members, and female members, all faced challenges in their relationships inside the family and within their society. Perpetrators were alienated within their culture for perpetrating extreme VAW, and they and their families faced ostracism, stigmatization and, ultimately, a social death within their society.
Footnotes
Acknowledgements
The authors are grateful to all brave family members for sharing their painful stories. They dedicate this study to all women in the world.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.