
Abstract
This article uses survey data from 131 women living in urban slums in Kenya to explore associations between stigma, stigma challenges, empowerment, and disclosure of intimate partner violence (IPV). A total of 81.7% of women reported informal or formal disclosure of IPV. A bystander offering help and experiencing stigma were associated with significant increases in the odds of informal and formal disclosure. There were also significant positive associations between participating in financial decision-making, membership in survivor support groups, and formal disclosure. Results suggest that interpersonal, community, and structural challenges to stigma interfere with stigma as a barrier to disclosure.
One in three women worldwide experiences gender-based violence (GBV; World Health Organization [WHO], 2013). Intimate partner violence (IPV), a form of GBV, is common in Kenya, with 40.7% of women reporting IPV (Kenya Demographic and Health Survey, 2014). Programming to address IPV often focuses on changing the social context in which violence occurs, for example, Bringing in the Bystander, SASA! (Abramsky et al., 2016; Moynihan et al., 2015). It seeks to address social norms that promote IPV and to improve outcomes for survivors through, in part, encouraging disclosure and nonstigmatizing responses to disclosure by community members (referenced as bystanders in most programming in the global north). Despite the social emphasis in programming, research on stigma, stigma challenges (e.g., bystander action), and disclosure or help seeking has largely focused on individual-level variables. While stigma has been established as a barrier to help seeking (Overstreet & Quinn, 2013), associations between stigma challenges, disclosure, and stigma are less well understood. This article combines theories of IPV stigma and help seeking to explore these associations in a sample of Kenyan women living in informal settlements (commonly known as urban slums) who have recent experiences of IPV.
Slums were chosen as the setting for the current study because of the large and growing proportion of Kenya’s urban population living in urban slums (estimated at 56% in 2015; Mutisya & Yarime, 2011; http://mdgs.un.org/unsd/mdg/SeriesDetail.aspx?srid=710) and the elevated rates of crime and violence, including IPV (Jewkes, 2002; Mutisya & Yarime, 2011; Oduro, Swartz, & Arnot, 2012; UN-HABITAT, 2003), in these communities. Slums are sites of severe poverty where basic necessities such as potable water, sanitation, energy, and food are absent or severely inadequate, and housing is overcrowded, insecure, and structurally unsound (Mutisya & Yarime, 2011; UN-HABITAT, 2003). As informal settlements, they are commonly excluded from government-funded services (UN-HABITAT, 2003). An average household in Nairobi’s slums comprises seven people living in a 12-ft × 12-ft structure (Mutisya & Yarime, 2011), with water available from shared “water spouts” or payment to private vendors (Karanja & Makau, 2009) and modern toilets built by nongovernmental organizations (NGO) requiring payment of a fee (Swart, 2012). Services and programming related to IPV are extremely limited. For example, police response to active scenes of IPV, safe houses, and other “safety nets” commonly available in resource-rich countries are largely absent. In this context, informal networks of support within the neighborhood take on greater importance for women experiencing IPV. These are precisely the networks targeted for change in community-level interventions.
Stigma and Help Seeking
IPV Stigma
Barnett, Maticka-Tyndale, and Trócaire Kenya (2016) proposed a model of GBV stigma as a community process of social control with moral, cognitive, interpersonal, and structural components. The moral component includes community norms. The cognitive component includes labeling and separating people based on a discreditable characteristic. The interpersonal component includes individual discrimination, and the structural component includes structural discrimination.
In this model, stigma operates to maintain the status quo by silencing or punishing women who complain about their experiences of GBV. This model of GBV stigma shifts focus onto the social context of both the stigma and the violence. One important aspect of social context, at the interpersonal level, is the role of active bystanders. Active bystanders are those who intervene in violent situations and/or provide help or support for the survivor. As such, they challenge stigmatization. Barnett and colleagues (2016), relying on qualitative data from Kenyan slums, reported that those who “‘meddled’ in violent relationships or supported women who left them [i.e. active bystanders] were also stigmatized” (p. 460) as part of the process of social control. The following review of IPV disclosure and help seeking frames the empirical evidence through this model of GBV stigma and attends to the role of active bystanders in this process.
IPV Disclosure and Help Seeking
Analyzing Demographic and Health Survey data, Palermo, Bleck, and Peterman (2013) reported the average rate of IPV disclosure globally as 40%, ranging from a low of 32% to a high of 48% across regions. Distinctions between “disclosure” and “help seeking” are not uniform across studies. Drawing from both, we here use informal disclosure/help seeking to refer to family and friends and formal disclosure/help seeking to refer to institutional actors (e.g., police, health care provider, and paralegal). Liang, Goodman, Tummala-Narra, and Weintraub’s (2005) model of help seeking in the context of IPV proposes three distinct steps that a woman takes to seek help: (a) recognizing and defining the problem, (b) deciding to seek help for the problem, and (c) selecting a source of support (e.g., friend, police, counselor). Stigma plays a role in each step.
Recognizing and Defining
At the first step, the normalization of violence as an acceptable correction for role failures or violations affects women’s ability to recognize and define the violence in their lives as a “problem.” Instead, it is their failure that is framed as problematic (Barnett et al., 2016). In this situation, women are more likely to blame themselves for the violence, resulting in shame or self-stigma (Abrahams & Jewkes, 2010). Thus, they are less likely to label an unwanted sexual experience as “rape” (Abrahams & Jewkes, 2010; Boonzaier, 1998) or IPV as “abuse” (Eisikovits & Enosh, 1997). Research on the association between endorsement of IPV norms (violence as expected or acceptable) and help seeking shows mixed results in low-resourced countries such as Kenya; studies in Bangladesh and Pakistan demonstrate a negative association (Andersson et al., 2010; Naved, Azim, Bhuiya, & Persson, 2006; Parvin, Sultana, & Naved, 2016), whereas those in Nigeria do not (Linos, Slopen, Berkman, Subramanian, & Kawachi, 2014; Okenwa, Lawoko, & Jansson, 2009).
Deciding to Seek Help
At the second step, deciding to seek help, the self-blame or stigmatization that can result from the internalization of IPV norms, together with fear of negative or stigmatizing reactions from others, has been linked to reduced likelihood of seeking help (Abrahams & Jewkes, 2010; Buchbinder & Eisikovits, 2003; Overstreet & Quinn, 2013). Thus, the normalization of IPV, self-blame, and anticipation of stigmatizing reactions of others are theoretically linked as the moral and cognitive aspects of IPV stigma (Barnett et al., 2016), empirically associated with disclosure or help seeking.
In the face of stigma-related disincentives for disclosure, it is perhaps unsurprising that qualitative work indicates that women are unlikely to seek help unless they believe they cannot resolve the situation on their own (Mannell, Jackson, & Umutoni, 2015). This is consistent with findings that women are more willing to seek help for physical and sexual violence than for emotional violence (Kim & Hogge, 2015; Odero et al., 2014), that they are significantly more likely to seek help if they have experienced more severe forms of violence (Naved et al., 2006; Parvin et al., 2016; Tenkorang, Sedziafa, & Owusu, 2017), and that fear for their life is the strongest predictor of using either formal or informal supports (Barrett & St. Pierre, 2011).
Several individual characteristics are also associated with disclosure, including being older, unmarried, or separated (Palermo et al., 2013); more educated (Kim & Hogge, 2015; Naved et al., 2006; Parvin et al., 2016; Tenkorang et al., 2017); and employed or participating in economic decision-making (Mannell et al., 2015; Okenwa et al., 2009). However, associations between disclosure and each of these individual characteristics vary not just across world regions (cf. Linos et al., 2014), but also across provinces in the same country (Andersson et al., 2010). This variation points to the interaction between individual and social factors in their association with help seeking for IPV.
Support Selection
The third step in Liang and colleagues’ (2005) model, support selection, refers to deciding from whom to seek support. Women are most likely to seek informal sources of support for initial disclosure (Abrahams & Jewkes, 2010; Erulkar, 2004; Kenya Demographic and Health Survey, 2008-2009; Liang et al., 2005; van Rensburg, 2007). The reactions of informal support providers (e.g., bystanders) are particularly important and influence whether the woman moves to disclose the violence to formal sources of support that can provide services to address the physical and emotional consequences of the violence or institute legal action to stop the violence (Fanslow & Robinson, 2010).
Experience of structural stigma has been shown to influence support selection. Paralegals, working in the same urban slums as the current research, report that the severely limited economic options for single mothers, the absence of safe shelters or enforcement of court orders, and multiyear delays in court actions result in women rarely pursuing either divorce or criminal action against a violent husband (Barnett et al., 2016). In the face of such structural stigma, women and NGO staff reported that responses to IPV centered primarily on participation in support groups where women developed and shared tactics for maintaining their family and limiting the violence (Barnett et al., 2016).
These findings are not unique because a context of gendered economic dependency (Umubyeyi, Persson, Mogren, & Krantz, 2016), absence of services, and corruption and delay in the criminal justice system (Andersson et al., 2010; Mannell et al., 2015; Odero et al., 2014; Umubyeyi et al., 2016) have been identified as structural barriers to help seeking across other lower-resourced countries. Linos and colleagues (2014) explicitly call for increased attention to the structural determinants of help seeking, finding that levels of development and violence against women in different states are significantly associated with rates of help seeking among women in those states. This emerging focus on structural influences on disclosure is consistent with Barnett and colleagues’ (2016) articulation of the structural component of GBV stigma, as evidenced in the systematic disadvantage or institutional stigma experienced by women survivors of GBV.
Stigma Challenges
Theoretically, if stigma is a “community process of instrumentally organized behavior” (Barnett et al., 2016, p. 459) to maintain existing inequalities, then challenges to stigma interfere with this process. Challenges to stigma might occur across moral, cognitive, interpersonal, or structural components. Laws criminalizing GBV, for example, may be understood as structural challenges to stigma. While bystander intervention in support of survivors or to counter IPV is typically examined as an interpersonal challenge, it may also be understood as a moral and, potentially, structural challenge to stigma.
The three key types of bystander action identified by Moynihan and colleagues (2015) challenge and disrupt the stigma processes of social control at the interpersonal, moral, and structural levels. Active bystanders may (a) intervene in the social reproduction of IPV norms (e.g., publicly speaking against IPV), (b) intervene in potential or actual violent situations (e.g., calling the police), and (c) engage in supportive, prosocial responses to IPV disclosure (Moynihan et al., 2015). Engaging in supportive, prosocial responses to IPV disclosure or intervening in potential or actual violent situations challenge stigma at the interpersonal level. Bystander responses may also challenge stigma at the structural level if bystanders advocate for victims when reporting IPV to police, local leaders, or health providers. At the moral level, the very act of intervening provides an alternative normative narrative and disrupts the social reproduction of IPV norms, particularly when bystanders speak publicly against IPV. IPV bystander researchers and theorists have identified bystander interventions as both contributing to shifts in the moral order related to IPV and resulting from such shifts (Gracia & Herrero, 2006; Jewkes, Flood, & Lang, 2015; Schuler & Nazneen, 2018; Voith, 2019). Research on “social support” and help seeking indicates that encouragement from informal support people such as bystanders is the second most common reason for disclosure to formal sources of support (Fanslow & Robinson, 2010) and that there is a significant positive association between having discussed violence against women with someone and seeking help for GBV (Andersson et al., 2010). Importantly, Naved et al. (2006) also point out that women sometimes receive help from those to whom they have not directly disclosed experiences of violence, usually family members. Taken together, these findings indicate that bystander action may increase help seeking from formal sources, reduce the responsibilization of women for seeking help to deal with the violence to which they are subject, and contribute to change in the social norms related to IPV, each of which challenges the stigma process.
Current Study
The foregoing review of empirical evidence organized by synthesizing Barnett et al.’s (2016) model of GBV stigma with Liang et al.’s (2005) model of IPV help seeking demonstrates that moral, cognitive, interpersonal, and structural elements of stigma have been identified as key barriers at each stage of help seeking in both qualitative and quantitative research across the globe. Many studies of disclosure/help seeking, however, do not frame these barriers as “stigma” per se and/or they focus on only one aspect of stigma. The current analysis addresses this gap by examining the association between disclosure and IPV stigma as conceptualized and measured across these four elements. The current study also assesses the role of challenges to stigma, particularly by active bystanders in the slum neighborhood, in this process. To our knowledge, the current analysis is the first to assess interrelationships among GBV stigma, challenges to stigma (particularly bystander action), and disclosure.
Method
This study used a subset of cross-sectional survey data collected for a multimethod research project on IPV, help seeking, and their correlates among women living in urban slums in Kenya.
Study Samples and Recruitment Procedures
Research was conducted in three urban slums (Mukuru, Thika, and Nakuru settlement) located in cities of different sizes, economic profiles, and mixes of ethnic groups. Two groups of participants were recruited from each site to complete surveys: a sample of 181 women who had participated in NGO-sponsored support groups for IPV survivors for at least 3 months (referred to as client women) and a sample of 174 women resident in randomly selected households (referred to as community women). Client women were informed about and invited to participate in the research by NGO staff, and community women were provided with information and an invitation by local community health volunteers. Community women were a representative sample of the population of interest. Client women comprised a convenience sample of women participating in NGO-sponsored support groups for IPV survivors. It is important to note that in this context support groups were often informal and semiautonomous.
Inclusion criteria for the research project were as follows: being married or in a marriage-like relationship; age 18 years or above; living in Mukuru, Thika, or Nakuru settlement; and able to communicate in English and/or Kiswahili. The subsample used in this study consisted of the 77 client and 54 community women who reported experiencing IPV in the 6 months prior to the survey.
Survey Administration
Invited women came to a local community center to participate in the research. On arrival, their eligibility to participate was established, the purpose and procedures of the study were explained, consent to participate was obtained, and they completed surveys in a private room in face-to-face structured interviews in a combination of English and Kiswahili. Survey completion required 20-48 min with a mean of 36 min (SD = 6 min). Nonparametric statistics were used to compare responses based on completion time divided into ordinal categories within 2 and 3 standard deviations of mean time. No significant differences were found between client and community women or in responses to questions based on the time to complete surveys. Question responses were entered directly into a survey database using tablets and PC survey software. Consistent with procedures typically used in research in these areas, women who completed surveys were provided with vouchers valued at 500Ksh. None of the women eligible to participate declined or withdrew from the study.
Research assistants who administered the survey were all experienced interviewers employed by Gmaurich, a Nairobi-based research company with extensive experience in diverse forms of data collection and research topics. All were women and received training specific to this research, including asking sensitive questions and dealing with potential difficulties that participants might have when recalling their experiences of IPV. The training also addressed self-care for the interviewers who would be hearing about violent experiences. A trained trauma counselor was available throughout the data collection period. Interviewers recommended the counselor to participants who expressed difficulty, and all participants were informed of the counselor’s availability and were encouraged to use these services. As use of counseling services was confidential, we do not have a count of how often these were used, but reports from the field indicate that this was frequent.
The study received ethics clearance from the University of Windsor and AMREF, Kenya.
Survey Development
Procedures used in survey development to “maximize instrument fidelity” are fully described by Onwuegbuzie, Bustamante, and Nelson (2010). Briefly, measures were developed based on a review of the literature and major surveys in use in the area (e.g., Kenya Demographic and Health Survey), a prior study that used focus groups with women survivors of IPV and consultations with NGO staff and researchers familiar with the field context and topic of research. The survey was pilot tested using both qualitative and quantitative methods, and procedures for sampling and administration were developed for the final research project. A multimethod approach was used for analysis of the pilot data (see Onwuegbuzie et al., 2010). Kiswahili was used as the reference language in question development, with fidelity to meanings in Kiswahili maximized through back translation.
Measures
Measures consisted of demographic characteristics, experiences of IPV in the past 6 months, variables indicating disclosure of recent IPV to formal and informal supports, experiences of stigma, challenges to stigma, and decision-making related to household finances.
Demographic characteristics
Included were self-reported age in years, completed education (0 = none, 1 = some primary school, 2 = completed primary through Grade 8, and 3 = more than completed primary), whether the participant had children (0 = no, 1 = yes) and how many, and ethnic group. The remainder of the demographic characteristics included whether the participant was a single mother, lived with her husband, and was unemployed (all coded 0 = no, 1 = yes).
Recent IPV
Women were asked whether they had experienced any of five forms of IPV in the past 6 months. These included threats to beat; hitting, kicking, dragging, or beating; forced sexual intercourse; throwing out or trying to sell her things; and withholding household money. Eligibility for inclusion in this study required a response of “yes” to at least one of these forms of IPV. “Being hurt so badly that hospital care was needed” was used to indicate severity of the IPV.
Dependent variables
Disclosure of IPV to informal contacts was dichotomized as 1 = disclosure to mother, father, sister(s), brother(s), female or male friends and 0 = no report of disclosure to any of those listed. Disclosure to formal contacts was dichotomized as 1 = disclosure to community health volunteer, health center or hospital, chief, religious leader, community activist or paralegal, police and 0 = no report of disclosure to any of these.
Independent variables
There were three types of independent variables: stigma, challenges to stigma, and participation in decisions about household finances.
Stigma
Direct experience of stigma was measured as 1 = having experienced structural, interpersonal, or cognitive stigma in the form of lost housing, lost job, or people would not buy from me, told to forget about the IPV and move on, told to be quiet about the IPV, excluded from community gatherings, avoided by friends or family members and 0 = no report of any of the listed forms of stigma. The moral dimension of stigma was measured based on a woman’s endorsement of any of nine reasons that justified a husband disciplining his wife. In focus group discussions preceding survey development and during piloting of the questionnaire, participants stressed that “a husband disciplining” his wife was the appropriate way to inquire about physical, economic, and emotional forms of IPV. The multiplicity of Kiswahili words for discipline included normative, or socially moral, forms of physical discipline. In contrast, words for beatings, assaults, hitting, and so on, outside reference to discipline, indicated inappropriate forms of violence. Endorsement of norms was measured dichotomously as 1 = endorsement of any of nine reasons justifying a husband disciplining his wife (e.g., she didn’t properly care for the children, she refused sex to her husband, she spent too much time with friends) and 0 = lack of endorsement of any of these reasons. Finally, awareness of IPV stigma in the community was measured as 1 = knowing of an IPV survivor who had been stigmatized in any of the ways listed in the experienced stigma questions, 0 = no such knowledge.
Challenges to stigma
Awareness of challenges to stigma at the communal or structural level included three measures. First was awareness of laws criminalizing various forms of IPV (1 = reporting awareness that any of six actions, such as a husband beating his wife, refusing to allow her to seek employment, or forcing his wife to have sexual intercourse, are illegal, 0 = no awareness of illegality on any of the items). Second was knowing a community leader had helped women who experienced IPV (1 = reporting such knowledge for any of the six items listed in the awareness of laws question and 0 = no such knowledge on any of the items). Third was knowledge of another woman reporting her IPV experience to the police (1 = knowledge of such reporting with respect to any of the six items listed in the awareness of laws question and 0 = no such reporting for any of the items).
Interpersonal experience of challenges to stigma was measured by experience of positive outreach by a bystander (1 = reporting that someone in the neighborhood had engaged in any of five helping activities, including asking the survivor what they wanted them to do; gathering others to help; informing a community activist, police, or other authority; encouraging the survivor to talk to someone else; or talking to the husband; and 0 = not reporting any of these activities).
Household financial decisions
Women’s participation in financial decision-making in the household was used as an indicator of the woman’s power in the household (1 = the woman reported that she made financial decisions related to household expenditures on her own or jointly with her husband, 0 = the woman reported her husband made these decisions).
Data Analysis
The 77 client and 54 community women who reported having experienced any one of six forms of IPV within the past 6 months comprised the sample of 131 women used in this study. Chi-square analyses were used to examine similarities and differences of the client and community groups on demographic characteristics (Table 1), IPV experiences (Table 2), and on each of the independent variables (Table 3).
Profile of Women Reporting IPV in the Past 6 Months.
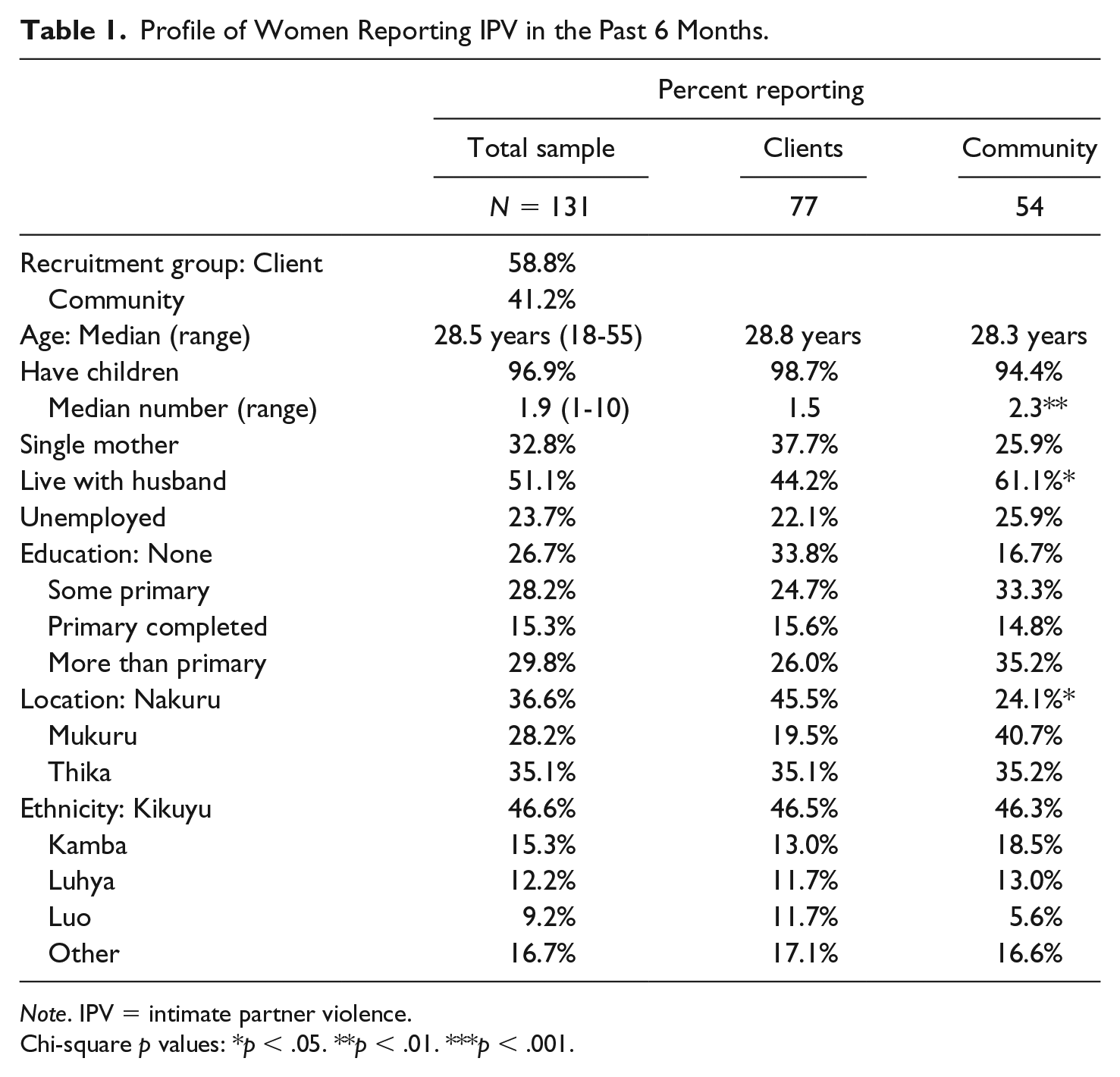
Note. IPV = intimate partner violence.
Chi-square p values: *p < .05. **p < .01. ***p < .001.
IPV Experience in the Past 6 Months.
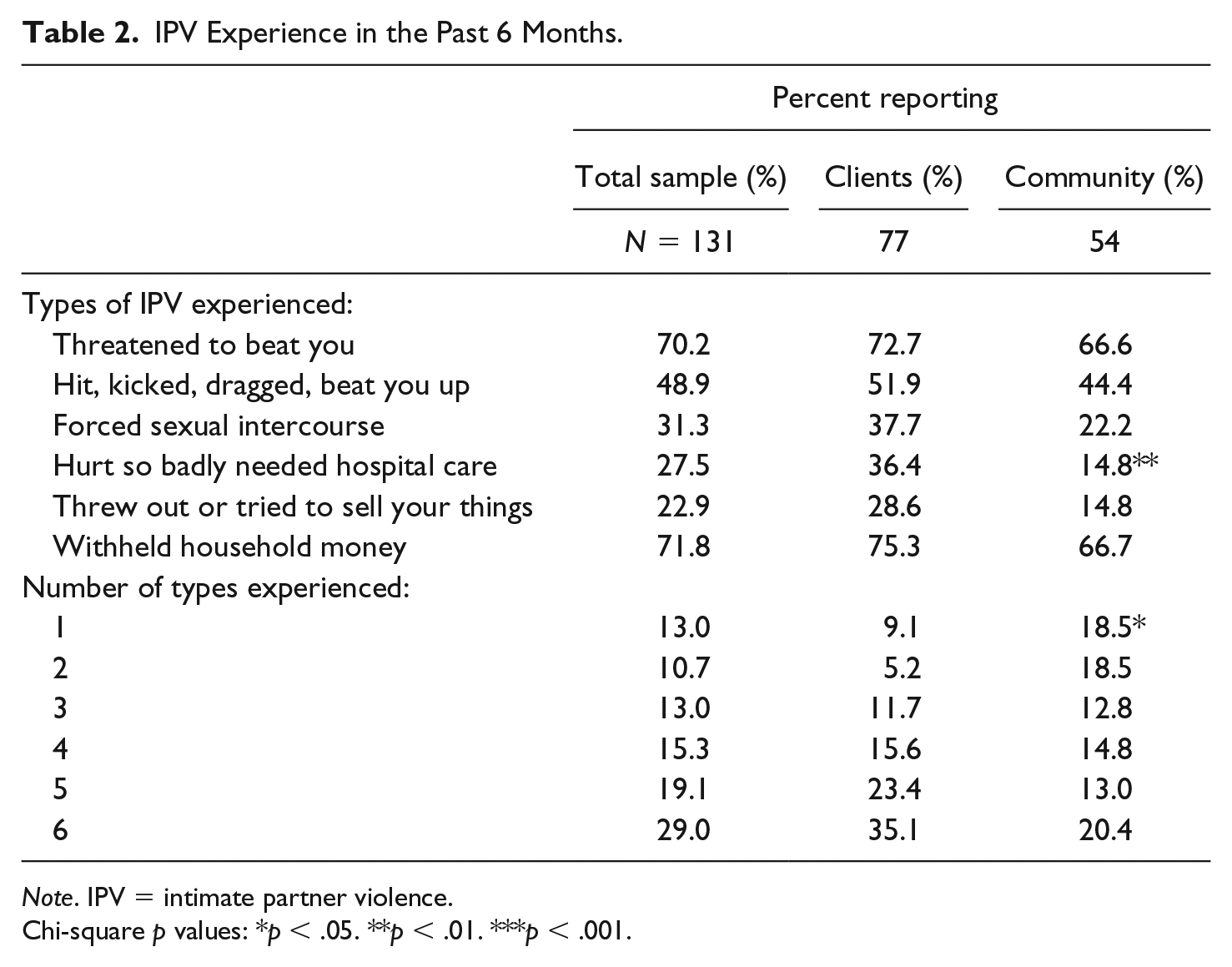
Note. IPV = intimate partner violence.
Chi-square p values: *p < .05. **p < .01. ***p < .001.
Percent of Respondents Endorsing Concepts of Interest.

Note. IPV = intimate partner violence.
Chi-square test p values: *p < .05. **p < .01. ***p < .001.
Following Liang et al.’s (2005) theory and extant research on disclosure or help seeking, we explored the associations between stigma, challenges to stigma, severity of IPV, women’s participation in household financial decisions, and informal and formal disclosure. Based on the work of Peduzzi, Concato, Kemper, Holford, and Feinstein (1996), combining the two groups into a sample of 131 created a sample of adequate size to support logistic regression with up to three independent variables for informal disclosure and six independent variables for formal disclosure. Bivariate logistic regression was used to measure the independent influence of each variable on either informal or formal disclosure. Formal disclosure was also regressed on informal disclosure. Given the exploratory nature of this study and sample size limitations (Peduzzi et al., 1996), we proceeded to a forward stepwise logistic regression for each form of disclosure on all other variables of interest. Goodness of fit of the final multivariate models was assessed using the omnibus chi-square, –2 log likelihood, Nagelkerke R2, Hosmer–Lemeshow chi-square, and percent of cases correctly classified. Results for regression analyses were interpreted with caution as they combined two groups of women who shared a residential context, a lifetime and recent history of IPV, and were similar on multiple demographic characteristics but who were sampled differently and represent different subgroups of urban slum-dwelling women with recent IPV experience.
Results
Profile of Sample
Table 1 presents a profile of the sample. More clients (58.8%) than community women (41.2%) from the full research project reported some form of IPV in the past 6 months. Comparing the subsample of client and community women who experienced IPV in the past 6 months, women in both groups were similar in age (18-55 years, median between 28 and 29 years), the proportion who were mothers (96.9%), status as a single mother (32.8%), level of education (26.7% no education, 70% primary or less), and employment (23.7% unemployed), with proportions in each ethnic group similar to ethnic distribution in the population (Kenya Demographic Health Survey, 2008-2009). Client women had significantly more children than community women (median = 2.3 and 1.5, respectively) and fewer lived with their husbands (44.2% and 61.1%, respectively).
When considering experiences of IPV in the past 6 months (Table 2), client women reported experiencing a significantly greater variety of forms of violence and a higher proportion required hospital care because of IPV. Among both groups, the two most common forms were a threatened beating and withholding funds for household expenses (70.2% and 71.8%, respectively). Just under half of the women reported having been hit, kicked, dragged, or beaten in the past 6 months. Other forms of violence were reported by 23-31% of the women.
Disclosure of the violence was common (81.7%; Table 3), with this most often being informal disclosure (75.6%). Formal disclosure was more common among client (58.4%) than community (31.5%) women. A large majority of women experienced both moral stigma (75.6% endorsed IPV norms) and some form of cognitive, interpersonal, or structural stigma (69.5%), with a significantly higher proportion of client (86.3%) than community women (57.1%) reporting these. Women were also aware of and experienced challenges to stigma at the interpersonal, community, and structural levels. Bystander action was reported by over 73% of the women. High proportions of women knew of structural challenges to stigma through laws that made IPV illegal (97.7%) and community leaders taking action against IPV (79.4%), and a high proportion were aware of challenges in the community, such as women reporting IPV (89.1%). At the same time, the high proportion who knew of a woman who had been stigmatized because of IPV (98.7% of client and 88.9% of community women) is evidence of widespread awareness of the community’s use of stigmatization. Finally, although most women (67.9%) reported participating in household financial decision-making, 71.8% had household funds withheld by their husbands (Table 2).
Table 4 provides results of bivariate logistic regressions for informal and formal disclosure. Unfortunately, the extremely high levels of awareness of laws (97.7%) and stigmatization of other women (93.1%) precluded their inclusion in regression analyses. Except for the significant difference in formal disclosure between community and client women already evidenced in Table 3, no other demographic variables had a statistically significant association with either form of disclosure. Among the other variables, only a bystander offering help and experiencing stigma had significant associations with informal disclosure, with each increasing the odds of disclosing to friends and/or family nearly fourfold. For formal disclosure, a bystander helping, informal disclosure, experiencing stigma, requiring hospital care as a result of the recent IPV, knowing other women who had formally disclosed, and participating in decisions about household spending were each positively associated with formal disclosure, with increases in the likelihood of disclosure ranging from more than twofold for financial decision-making and requiring hospital care to more than fourfold for experiencing stigma and a bystander offering help.
Bivariate Logistic Regressions of Disclosure of Recent IPV to Informal and Formal Contacts.
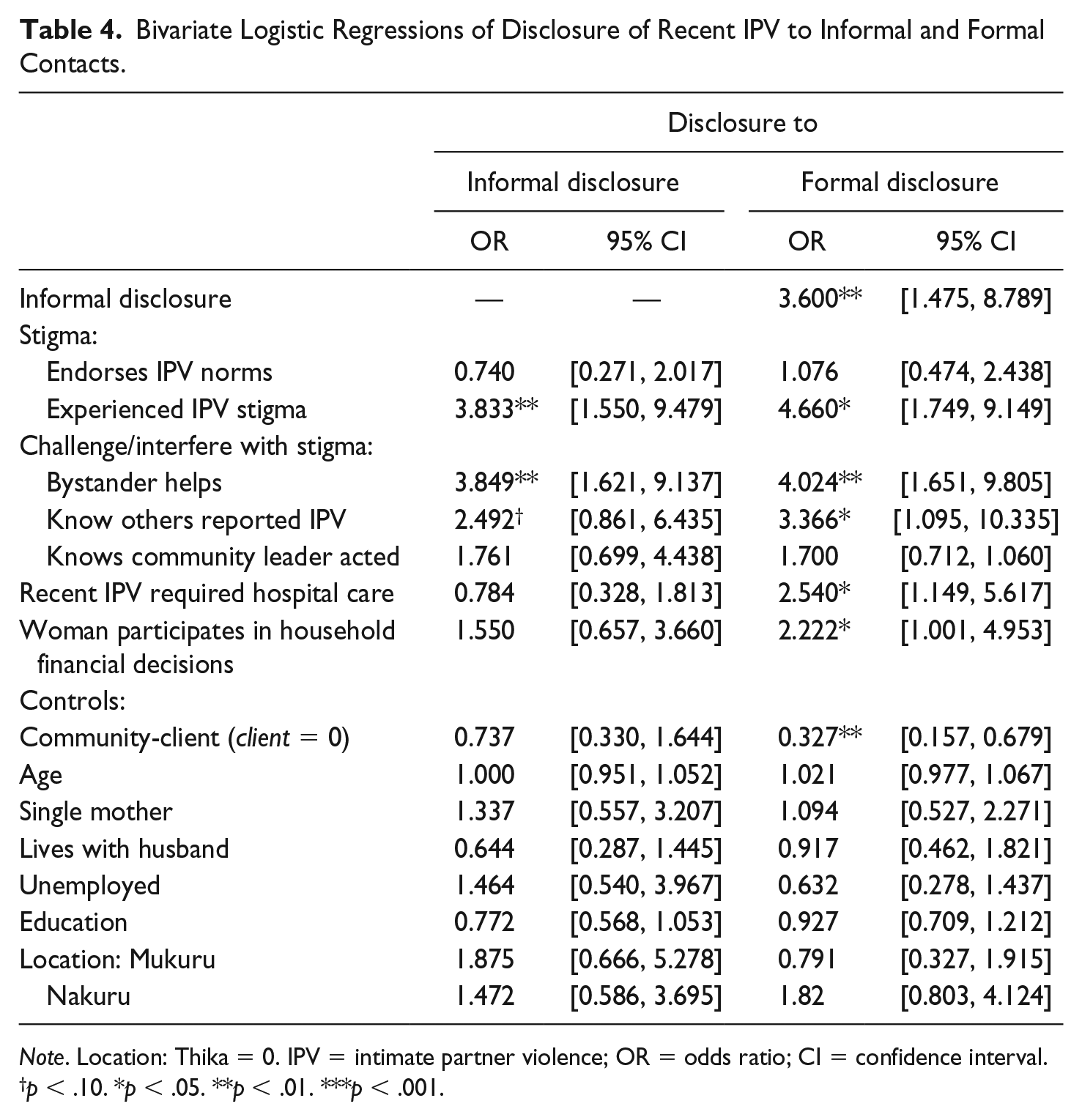
Note. Location: Thika = 0. IPV = intimate partner violence; OR = odds ratio; CI = confidence interval.
p < .10. *p < .05. **p < .01. ***p < .001.
Table 5 displays results for the final models in forward stepwise multivariate logistic regression analyses. Informal disclosure was positively associated with both a bystander offering help and experiencing stigma, with the association with bystander assistance stronger than that of stigma. For formal disclosure, four variables that were significant in bivariate analyses were retained. A bystander offering help had the strongest association, followed by having experienced stigma, participating in financial decision-making, and being a client, with the latter three not significantly different from each other in their degree of association.
Final Models in Forward Stepwise Multivariate Logistic Regressions of Disclosure to Informal and Formal Contacts.

Note. AOR = adjusted odds ratio; CI = confidence interval; IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
Goodness-of-fit indicators show a good fit to the data for the final multivariate models. In both cases, the omnibus chi-squares indicate that the overall models were statistically significant and the change in –2LL showed a statistically significant gain over the null models. The Hosmer and Lemeshow test suggests that there would not be a statistically significant gain in adding more variables (e.g., interaction effects) to the models. The Nagelkerke R2s and the percent of correctly classified cases suggest that a smaller proportion of the variance is explained (18.3% vs. 26%) but a higher percentage of cases are correctly classified (75.6% vs 68.7%) for informal than for formal contact.
Discussion
The current study helps us better understand associations between stigma, challenges to stigma, and disclosure or help seeking by integrating two theoretical frames: Barnett and colleagues’ (2016) multimodal conceptualization of GBV stigma as a process of social control and Liang and colleagues’ (2005) model of help seeking. The relationships between different components of stigma; challenges to stigma as social control at the interpersonal, community, and structural levels; and both informal and formal disclosure demonstrate a contested social terrain. There are conflicting “push–pull” factors affecting women’s disclosure. Importantly, the variables significantly associated with disclosure were those characterizing the social landscape in which women exercise choice.
Stigma, Challenging Stigma, and Disclosure
Experience of cognitive, interpersonal, or structural stigma and direct experience of a challenge to stigma by a bystander were both significantly associated with informal and formal disclosure. The moral aspect of IPV stigma, endorsement of norms supporting IPV, however, was not. A community-level challenge to stigma, knowing other women who had reported IPV, was also significantly associated with formal disclosure, although it was not retained in the stepwise procedure. The results for a positive association with bystander action were consistent with prior research (Andersson et al., 2010; Fanslow & Robinson, 2010; Naved et al., 2006), and those for the absence of an association of the moral aspect of IPV stigma were consistent with other research in sub-Saharan Africa (Linos et al., 2014; Okenwa et al., 2009). The positive association between experiencing stigma and disclosure was at odds with Liang and colleagues’ (2005) help seeking model and contrary to results of prior research (Overstreet & Quinn, 2013).
One explanation of this difference from previous work may lie in differences in the operationalization and measurement of stigma or the “third stage” of help seeking (Liang et al., 2005), support selection. The current study measured stigma across four conceptual levels: moral, cognitive, interpersonal, and structural. Other studies rely on different conceptual groupings (e.g., anticipated stigma) and associated measures. These often mix what we call “moral stigma” (for which no association was found when measured separately in this study) and what we call “cognitive” or “interpersonal” stigma. They rarely include structural components. In addition, previous works examining associations between stigma and disclosure have been overwhelmingly qualitative in nature. These provide insight into how women themselves or the researchers analyzing their narratives make sense of women’s decisions about disclosure and help seeking. They do not provide information about reliable associations within a sample or population.
Williams and Mickelson (2008) provided a rare inferential analysis using measures of stigma that go beyond IPV norms (the moral component). They found a positive association between “perceived stigma” and “indirect support seeking” (seeking support without disclosing) and no association between perceived stigma and direct support seeking (no distinction was made between informal and formal targets). This result is one of no association, not a negative association, and similar to the current finding, is based on correlational data.
Three substantive explanations are also possible. First, in the context of challenges to stigma, as evidenced in bystander actions and awareness of laws criminalizing IPV, community leaders acting against IPV, and women in the community reporting IPV, the experience of stigma may act as a signal that motivates disclosure. Associations between stigma, stigma challenges, and disclosure have not been previously tested. The prevalence of both IPV stigma and challenges to IPV stigma in these communities creates a contested terrain for women to navigate. In such a contested terrain, stigma may function less effectively as a social control that creates a barrier to women seeking resolution to IPV through formal channels. It may even encourage such help seeking because stigma challenges show women that alternative sources of support are available at a time when previous forms of social support and economic stability are being retracted through the stigmatization process. While not directly addressed by those who have identified the reflexive relationship between bystander actions and community norms (Gracia & Herrero, 2006; Jewkes et al., 2015; Schuler & Nazneen, 2018; Voith, 2019), their work supports a stage or process model where contradictory norms and actions may coexist during certain stages of the process.
Second, given the moral codes that frame IPV as a family matter that is not to be disclosed (Barnett et al., 2016) and the cross-sectional nature of our data, experiences of stigma may be a result of disclosure. Thus, disclosure results in stigmatization. Further predictive research is required to clarify this association. Third, most prior investigations of the relationship between help seeking and stigma (beyond IPV norms) have been conducted in the global north. Different sociocultural and economic settings may set the stage for different associations. Comparative research is warranted.
Support Groups, Economic Empowerment, and Disclosure
Being a client and participating in household financial decision-making were also significantly associated with formal disclosure. The former result may appear inconsequential, that is, women who have formally disclosed in the past are doing the same in the future. However, the exclusion of disclosure to an NGO or support group from the measure of formal disclosure and the overwhelmingly negative and injurious experiences reported in an earlier study by women from these same urban settlements as a result of previous formal disclosure (Barnett et al., 2016) suggest that this result is of consequence. Support groups and bystander action are both examples of direct, interpersonal challenges to stigma. Their influence on formal disclosure is consistent with Fanslow and Robinson’s (2010) identification of such supports as encouraging formal disclosure.
Participation in household financial decision-making has been taken as an indicator of women’s power in the household and consequently reduced vulnerability to IPV (Donta, Nair, Begum, & Prakasam, 2016; Okenwa et al., 2009). The high proportion of women who reported that husbands withheld household funds as part of IPV distinguishes participation in decision-making from control of finances. Women who participate in household financial decision-making may be considered as more empowered than women who do not, but our results support the observation that they are not necessarily in control of funds. In other words, their husbands may include them sometimes in decisions about how money is spent and at other times withhold funds, including those necessary for survival. Power is not a zero-sum phenomenon. It is important that this distinction be recognized in future research.
Study Limitations
There are several limitations to generalization of these results. First is the self-report nature of the measures. While Onwuegbuzie et al.’s (2010) procedures were used to maximize what they term the fidelity of the measures, results are based on women’s reports and interpretations. Second, although the sample used in this study was large enough to support the analyses undertaken, it was too small for consideration of potential interactions and additional associations that could clarify complexities evident in the relationships among variables. Also, while the method of sampling of community women contributes to confidence in their representation of women living in these slum communities, the same cannot be said for client women who were a convenience sample of women receiving services. The merging of the two groups for logistic regression means results must be understood as based on a convenience sample and interpreted as suggestive. Third, compared with experimental research, field research imposes limitations on drawing definitive conclusions about causality. Issues of potential confounders, time ordering, and reciprocity of influence are among the challenges posed in field research. Yet, not all topics lend themselves to experimental designs, as is the case in this study. Finally, given the location and context of this study, results cannot be generalized beyond Kenya’s urban slums.
Conclusion
The results of this study contribute to theory, programming, and directions for future research. They support the integration of a multimodal theory of stigma with a theory of help seeking and call attention to the complexity of relationships between intimate partner relationship norms, social controls to enforce norms, resistance to norm enforcement in these relationships, and help seeking, and the associated need to more fully incorporate these into theory. The results for the influence of stigma and challenges to stigma at the interpersonal, community, and structural levels suggest that such interference may reduce the power of stigma as a social control and should be incorporated into theory. Findings that being a client, participating in household financial decision-making, and receiving support from a bystander were associated with disclosure indicate that a woman’s relative social empowerment, or the degree to which her exercise of agency is supported by others, is strongly associated with disclosure of IPV, particularly to those formal supports who may provide health care, protection from future violence, or legal redress. This aligns with Campbell and Mannell’s (2016) call for conceptualizing social networks and institutions as two dimensions of agency. These should be examined in future work on disclosure.
The strong positive association between a bystander offering help and both informal and formal disclosure provides rationale for antiviolence programming to focus on increasing bystander action at the community level. Given previous findings that active bystanders are themselves stigmatized (Barnett et al., 2016; Odero et al., 2014), this must also be addressed in interventions promoting bystander action. Addressing IPV stigma as a multimodal process of social control should work to destigmatize both survivors and bystanders. In accordance with the theoretical model used here (Barnett et al., 2016), this means addressing norms that justify IPV and frame those who disclose and challenge IPV as “trouble makers,” while proactively reframing challenging IPV as in line with the moral order because it better ensures access to “what matters most” in a community.
IPV is recognized as a global issue that occurs in diverse social and cultural settings. The complexity of the relationships evidenced here, and the diversity of results found in other settings, calls for additional research that takes account of different social and cultural settings to more fully understand IPV as a social phenomenon.
Footnotes
Acknowledgements
The authors thank staff at Trocaire, Kenya, their partner organizations, and Gmaurich for their work on this project. The authors especially thank the research participants for taking the time to participate.
Authors’ Note
Neither Irish Aid nor Trocaire, Kenya, is responsible for the analyses, interpretations, or conclusions presented in this article. The first two authors made equal contributions to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported with funding from Trocaire, Kenya, Irish Aid, and the Canada Research Chairs Program.