
Abstract
Sexual trauma is prevalent among women veterans and associated with health risks including hazardous drinking, intimate partner violence (IPV), and post-traumatic stress disorder (PTSD). Safe and Healthy Experiences (SHE) is a computerized intervention to reduce these health risks. SHE was pilot tested in an open trial (N = 20) with women veterans with a history of sexual trauma and associated health risks. Women reported high satisfaction with the intervention and computerized delivery and they evidenced reductions in hazardous drinking, IPV, and PTSD at 4 months. SHE appears to be satisfactory, feasible, and potentially beneficial to women veterans.
Keywords
Women are one of the fastest growing demographics seeking treatment at the VA, with the current generation of women veterans seeking care at younger ages and higher rates than prior generations (Frayne et al., 2014). Among women veterans receiving care at the VA, 51–57.5% have experienced lifetime sexual trauma (Polusny et al., 2008; Sadler et al., 2012), and up to 23.7% have experienced military sexual trauma (MST; Washington et al., 2015). Among women veterans, lifetime sexual trauma—particularly MST—has a strong association with greater hazardous drinking (Hankin et al., 1999; Langdon et al., 2016), intimate partner violence (IPV; Gerber et al., 2014), and post-traumatic stress disorder (PTSD; Middleton & Craig, 2012).
Although the VA screens all veterans verbally for MST, PTSD, and hazardous drinking at certain intervals (Department of Veterans Affairs, 2018), a computer-delivered screening and intervention may increase the identification of high-risk women veterans and potentially have a high reach at a low-cost. Women veterans may feel more comfortable reporting health risks via computerized screener, than an in-person interview with a health care provider (Newman et al., 2002). Furthermore, computerized intervention may overcome numerous health care provider barriers to screening and intervention for lifetime sexual trauma and associated health risks (Richens et al., 2010). These barriers include lack of time and support resources, low level of confidence in screening and intervening, lack of education and training, and fear of offending the patient (Brown & Weisler, 2011; Humphreys et al., 2011; Iverson et al., 2013; Rhodes et al., 2007; Sprague et al., 2012).
This study evaluated the satisfaction, feasibility, and potential promise of Safe and Healthy Experiences (SHE), a brief modular computer-based intervention for women veterans reporting lifetime sexual trauma and one or more health risks (i.e., hazardous drinking, IPV, and PTSD). The content of the SHE intervention is theory-driven and consistent with past studies’ determinations of effective interventions for women with health risks of hazardous drinking, IPV, and PTSD (Seal et al., 2012; Weir et al., 2009). The content is also consistent with motivational interviewing (MI), a widely used and disseminated model of behavior change that is considered effective across a span of mental health and behavioral issues (Weir et al., 2009). MI aligns with the Transtheoretical Model (TTM; Prochaska & DiClemente, 1984) that outlines different stages of change and procedures aimed at evolving readiness to change. The nonconfrontational nature of MI is ideal for reducing health risks in women with histories of sexual trauma because it is consistent with the recommended empowerment model for survivors of IPV (Dutton & Hemphill, 1992) that promotes self-efficacy and focuses on identifying the women’s strengths and successes (Motivational Interviewing and Intimate Partner Violence Workgroup, 2010). SHE has three brief intervention modules on each of the health risks of hazardous drinking, IPV, and PTSD. We hypothesized that our novel intervention (SHE) would be satisfactory to women veterans and feasible in a VA primary care setting, research procedures would be feasible, and that participants would show reductions in the targeted health risks of hazardous drinking, IPV, and PTSD, respectively, in the 4 months following completion of SHE.
Method
Participants and Procedures
Participants
A nonrandomized trial was conducted with 20 women seeking VA primary care. Inclusion criteria included female gender, veteran status, age between 18 and 65 years, a lifetime history of sexual trauma defined as at least one occurrence of childhood sexual trauma, adult sexual trauma or MST during a woman’s lifetime, and at least one health risk factor: hazardous drinking, IPV, or PTSD within the last 12 months. Exclusion criteria included an inability to understand study procedures in English, and an active suicidal or homicidal crisis state warranting imminent hospitalization. Participants in the study sample were mostly U.S. Army veterans (95%; see Table 1 for demographic information).
Demographics of Study Sample (N = 20).
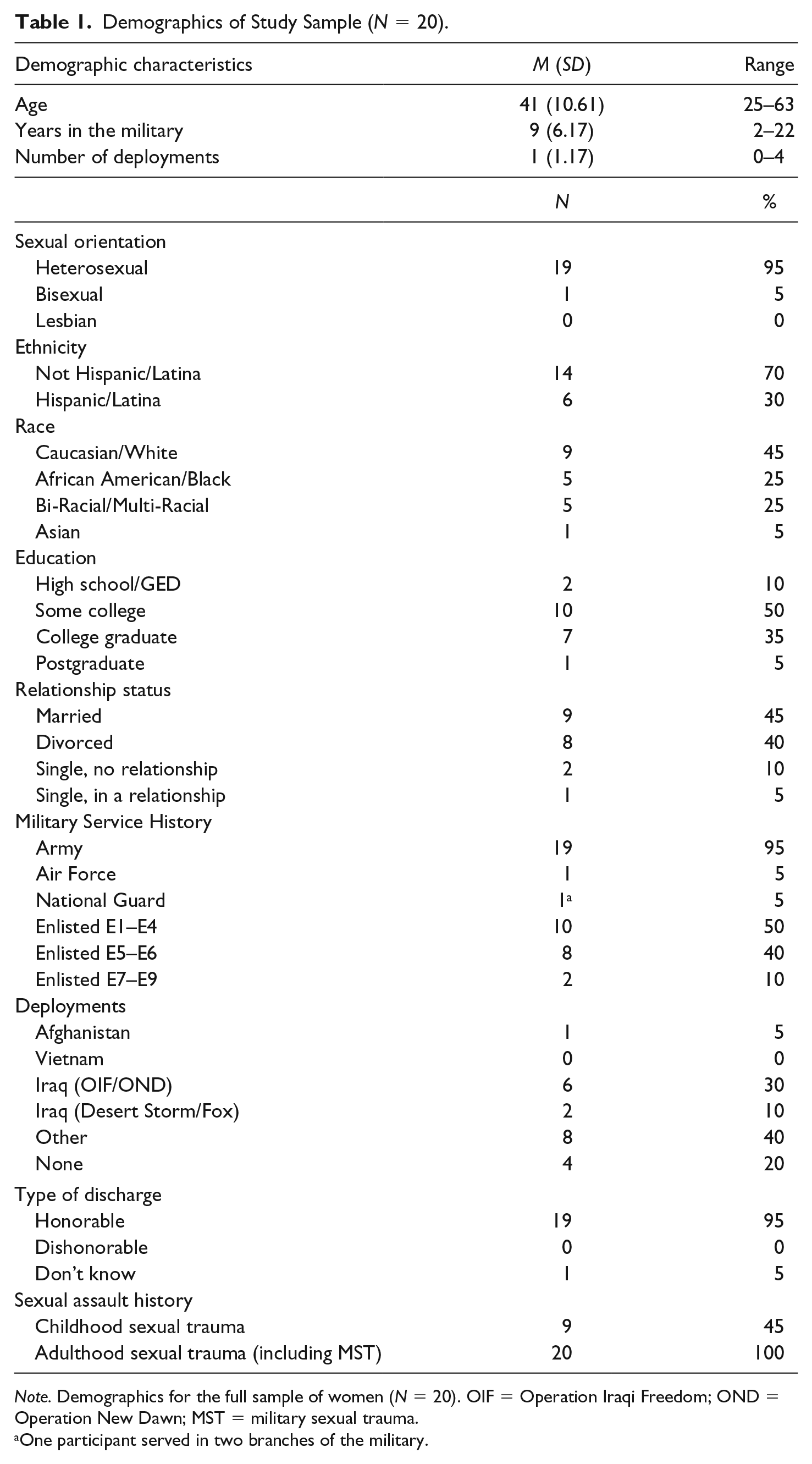
Note. Demographics for the full sample of women (N = 20). OIF = Operation Iraqi Freedom; OND = Operation New Dawn; MST = military sexual trauma.
One participant served in two branches of the military.
Procedures
Participants were recruited from a women’s primary care clinic at a large VA hospital in the southern United States. The primary method for recruitment was in-person recruitment in the clinic waiting room; study personnel handed out flyers and asked each woman in the waiting room if they were interested in hearing more about a study to “examine the mental health and stress of women veterans.” Flyers were also posted throughout the hospital. After initial recruitment, all research procedures took place in a private research office within the clinic. Screening: Women who agreed to complete the screener (approximately 45 min) provided informed consent and were screened for eligibility—including history of lifetime sexual trauma and at least one of the associated health risks—on an iPad, given a discreet list of mental health resources (that did not identify sexual trauma), and received compensation in the form of a US$10 gift card for their time and effort. Women who screened eligible for the study were invited to participate in the open trial, either by beginning the baseline and intervention immediately, or scheduling an appointment for the baseline and intervention within 6 weeks to ensure data accuracy. Baseline assessment: Eligible women who elected to participate in the open trial provided informed consent and were administered the computerized baseline assessment. Intervention: Immediately following the baseline assessment, participants received all of the relevant SHE intervention modules for which they screened eligible (i.e., hazardous drinking, IPV, and/or PTSD) on the iPad (using headphones), as well as corresponding psychoeducational resource handouts on the relevant health risk(s).
Intervention Content
At the beginning of each SHE intervention module, participants receive a personalized profile based on their responses during the baseline assessment. For example, a participant who screens positive for the IPV health risk would receive a summary of her relationship safety and general information on IPV. In each module, participants are shown videos of women veterans with the same risk factor discussing their experiences and utilization of resources and/or skills to reduce their risk. Some of these videos were from the VA website, maketheconnection.net (Department of Veterans Affairs, 2011/2018), and featured women veterans discussing their experiences, and some were produced for the SHE intervention with actors portraying women veterans. The module then prompts women to indicate their readiness to change. Participants reporting readiness to change are presented with goal setting including affirmations about utilizing information from the module and the psychoeducational resource handouts. Participants reporting ambivalence to change receive targeted feedback and a list of example pros and cons. Next, the program offers participants the option to view information about steps toward change. This includes allowing the participants to consider their biggest motivators for improving health and safety such as “it would be better for my mental health” and “I would feel more safe and secure.” Finally, a motivational video with affirmations is presented. At the end of each intervention module, participants evaluate satisfaction with the intervention content and computerized software, respectively. Follow-up: Participants returned for 45-min computer-based follow-up assessments at 2 months and 4 months from the date of their baseline appointment. Participants were compensated up to US$140 in gift cards for their time and effort completing assessments.
Measures
Eligibility screening measures
Women completed screening measures on history of lifetime sexual trauma, hazardous drinking, IPV, and PTSD. Lifetime sexual trauma was determined by a history of childhood sexual trauma, adulthood sexual trauma, and/or MST. Childhood sexual trauma was assessed with the Childhood Sexual Victimization Questionnaire (CSVQ; Finkelhor, 1979), which defines sexual trauma as unwanted exposure to another’s genitals, genital touching or fondling, and attempted and completed oral, vaginal, and anal rape before age 14. Adulthood sexual trauma was assessed with the Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2007), comprising seven behaviorally oriented items that assess victimization experiences including unwanted sexual touching, and attempted and completed oral, vaginal, and anal rape since age 14. MST was assessed with the VA’s two-item MST screener, in which participants are asked to respond “Yes” or “No” to the following two questions: (a) When you were in the military, did you ever receive unwanted, threatening, or repeated sexual attention (e.g., touching, cornering, pressure for sexual favors, or inappropriate verbal remarks)? and (b) When you were in the military, did you have sexual contact against your will or when you were unable to say no (e.g., after being forced or threatened or to avoid other consequences)? (Kimerling et al., 2007, 2008). Hazardous drinking was assessed with the Graduated Frequency Measure (GFM; Hilton, 1989), which assesses the quantity and frequency of alcohol use over the past month. Women screened positive for potential hazardous drinking if they reported having four or more drinks on any single day in the past month, which is the quantity that exceeds the national daily limit for low-risk alcohol use for women (Dawson, 2000; National Institute on Alcohol Abuse and Alcoholism, 2004). IPV in the last 12 months was assessed with the Woman Abuse Screening Tool (WAST), and a score of 4 or greater was considered a positive screen for IPV (Brown et al., 2000). PTSD was assessed with the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5; Weathers et al., 2013), and a score of 33 or greater was considered a positive screen for PTSD (Bovin et al., 2016).
Baseline, 2-Month, and 4-Month Assessment Measures
Participant characteristics
Background characteristics were measured with a standard demographics questionnaire assessing age, race, ethnicity, marital status, educational history, sexual orientation, and military history.
Hazardous drinking
The Alcohol Use Disorder Identification Test (AUDIT; Saunders et al., 1993) is a 10-item measure of hazardous drinking. The AUDIT assesses current drinking behavior on a 5-point Likert-type scale ranging from 0–4; higher scores reflect greater alcohol use. Individuals were classified as engaging in hazardous drinking if the total score was greater than or equal to 8 (Conigrave et al., 1995). In a sample of people with substance abuse, the AUDIT showed high test–retest reliability (r = .86; Babor et al., 2001). Internal consistency values were averaged across 10 different studies within a systematic review of the AUDIT and the mean value indicated good internal consistency (α = .80; de Meneses-Gaya et al., 2009). Internal consistency for the AUDIT in the current sample was good to excellent (α = .84–.93).
IPV
The Composite Abuse Scale (CAS) is a multidimensional measure of partner abuse that assesses four factors of abuse, including (a) severe combined abuse, (b) emotional abuse, (c) physical abuse, and (d) harassment (Hegarty et al., 2005). The assessment has 30 items quantified with a 6-point response scale ranging from 0–5; higher scores are indicative of greater abuse (Hegarty et al., 2005). Items assessed the frequency of a series of actions by their current intimate partner within the past 12 months. Individuals were classified with the IPV risk factor if their total score was greater than or equal to 3. Outcomes from a study of the four factors by Hegarty et al. (2005) showed good internal reliability (α ≥ .85) with the majority of subscales ≥ .9 and high corrected item-total correlations (>.5). Internal consistency for the CAS in the current sample was excellent (α = .96–.98).
PTSD
Symptoms of PTSD were assessed using the PCL-5 (Weathers et al., 2013). The PCL-5 is a widely used measure (Blevins et al., 2015) including 20 items on the four symptom clusters of PTSD: re-experiencing, hyperarousal, avoidance, and negative mood/beliefs. Scores on each item range from 0–4 and higher scores reflect greater symptoms. A positive screening for PTSD was classified by a cumulative score greater than or equal to 33 (Bovin et al., 2016). Outcomes from a study conducted by Bovin et al. (2016) show excellent internal consistency (α = .96) and good test–retest reliability (r = .84) for the PCL-5 when administered to a sample of veterans receiving care in the VA. A psychometric analysis of the PCL-5 administered to a sample of 912 military service members seeking treatment also reported strong construct validity (Wortmann et al., 2016). Internal consistency for the PCL-5 in the current sample was excellent (α = .97–.98).
Intervention Measures
Satisfaction
Immediately after completing each intervention module (corresponding to their identified health risks of hazardous drinking, IPV, and/or PTSD), participants completed the satisfaction measures. The Client Satisfaction Questionnaire (CSQ; Larsen et al., 1979) is an eight-item questionnaire which measures participants’ satisfaction regarding an intervention. The CSQ showed excellent internal consistency (α = .93) in a sample of 62 patients receiving mental health care at an urban community clinic (Attkisson & Zwick, 1982). Internal consistency for the CSQ in the current sample was excellent (α = .94). The SHE intervention was developed with the Computerized Intervention Authoring Software (CIAS; Ondersma et al., 2005). Satisfaction with the computerized software itself was assessed with the CIAS Software Scale (SCSS), which was created by the authors of the CIAS for evaluating participant satisfaction (Ondersma et al., 2005). The SCSS assesses participant satisfaction in terms of likeability, ease of use, interest, and respectfulness using a 1–5 Likert-type scale (1 = not at all, 5 = very much). Internal consistency for the CIAS in the current sample was good (α = .80).
Results
Participants
The open trial was conducted over a period of 2 months. During this time, 222 women were approached about the study as they were waiting to be called for their primary care appointments, 34 completed the screening procedures, 22 were eligible to participate in the study, and 20 women (91% of those eligible) elected to participate in the study (see Figure 1, CONSORT table). Twenty women participated in the open trial of the SHE intervention, and 19 women (95%) completed all of their assigned intervention modules. Participant retention at the 2-month follow-up was 19 women (95%) and retention at the 4-month follow-up was 18 women (90%).
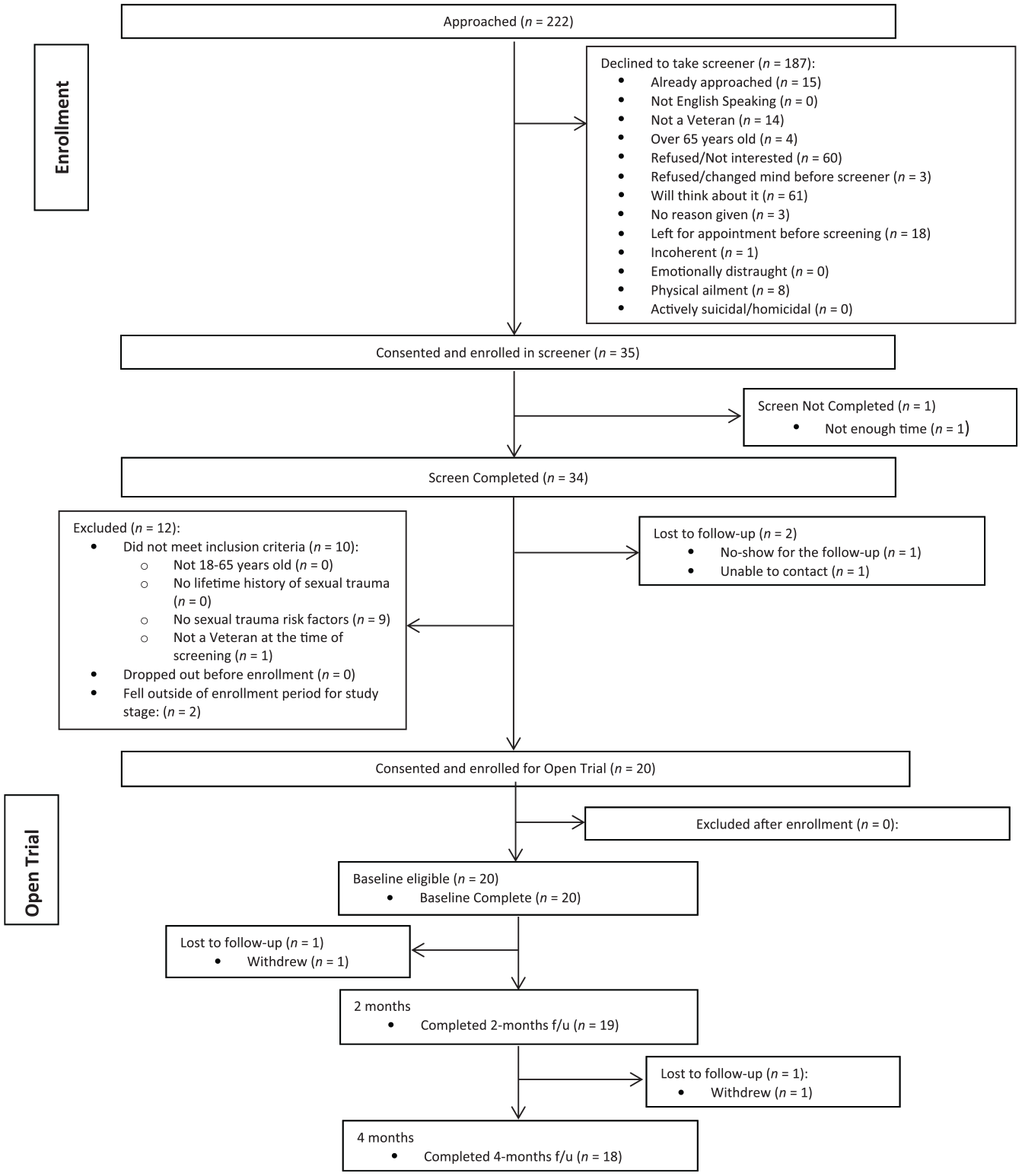
CONSORT table for the open trial of the SHE intervention.
Intervention Satisfaction
Participants rated their satisfaction with the intervention content and with the computerized software specifically. Participants rated intervention satisfaction and software satisfaction for each intervention module they completed; thus, women with multiple health risks completed these measures in reference to each module, respectively. In terms of satisfaction with the intervention content, the full sample of participants (N = 20) collapsed across the three interventions (hazardous drinking, IPV, and PTSD), provided an average item rating of 3.2 (SD = 0.7) on this 0- to 4-point scale, reflecting moderately high satisfaction scores. When participants were examined by group, the PTSD group reported the highest item satisfaction rating with an average rating of 3.47 (SD = 0.66), followed by the IPV group, and hazardous drinking group, respectively (see Table 2). Notably, 81% of participants reported they would recommend the intervention to a friend. In addition, 74% of participants indicated they would come back to this intervention in the future. See Table 3 for mean ratings on the intervention satisfaction items.
Satisfaction With SHE Intervention.

Note. The items of the Client Satisfaction Questionnaire (CSQ) are scored on a 4-point Likert-type scale, with higher numbers indicating greater satisfaction. Item mean values are presented. The Satisfaction with CIAS Software Scale (SCSS) is rated on a 5-point Likert-type scale (total score range = 7–35), with higher numbers indicating greater satisfaction. Note that participants completed the CSQ in reference to the intervention content, and the SCSS in reference to the computerized software after each module; thus, women with multiple risk factors completed these measures in reference to each module, respectively. The satisfaction questionnaires were completed a total of 27 times by the 20 study participants.
Item Ratings for Satisfaction With the SHE Intervention Content.
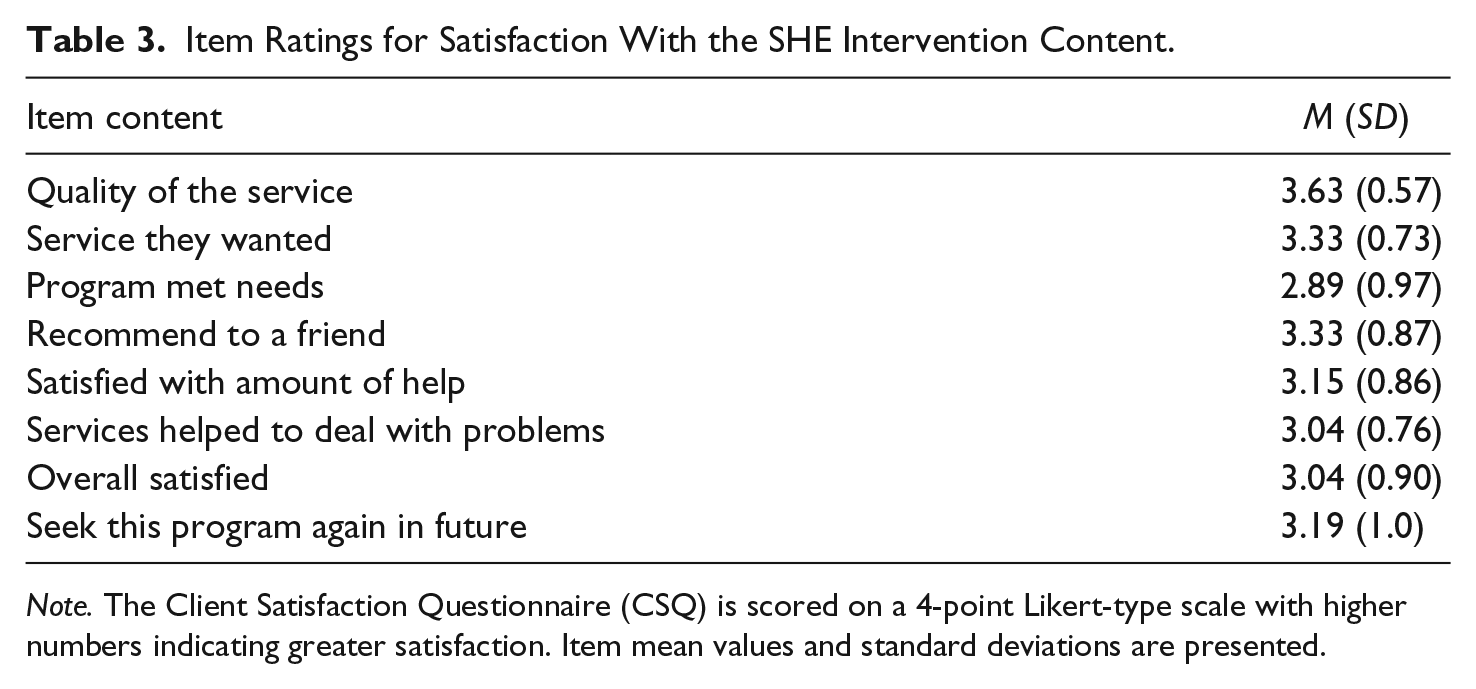
Note. The Client Satisfaction Questionnaire (CSQ) is scored on a 4-point Likert-type scale with higher numbers indicating greater satisfaction. Item mean values and standard deviations are presented.
In terms of satisfaction with the computerized software, the full sample of participants collapsed across the three interventions provided an average total rating of 29.96 (SD = 4.52), reflecting high scores on this 35-point scale. Again, the PTSD group reported the highest satisfaction with an average total rating of 31.43 (SD = 4.52), followed by the IPV group, and hazardous drinking group, respectively (see Table 2). Participants rated the software highly on “easy to use,” “understandable,” and “respectful.” For additional details on the software satisfaction ratings, see Table 4.
Item Ratings for Satisfaction With the Computerized Software.
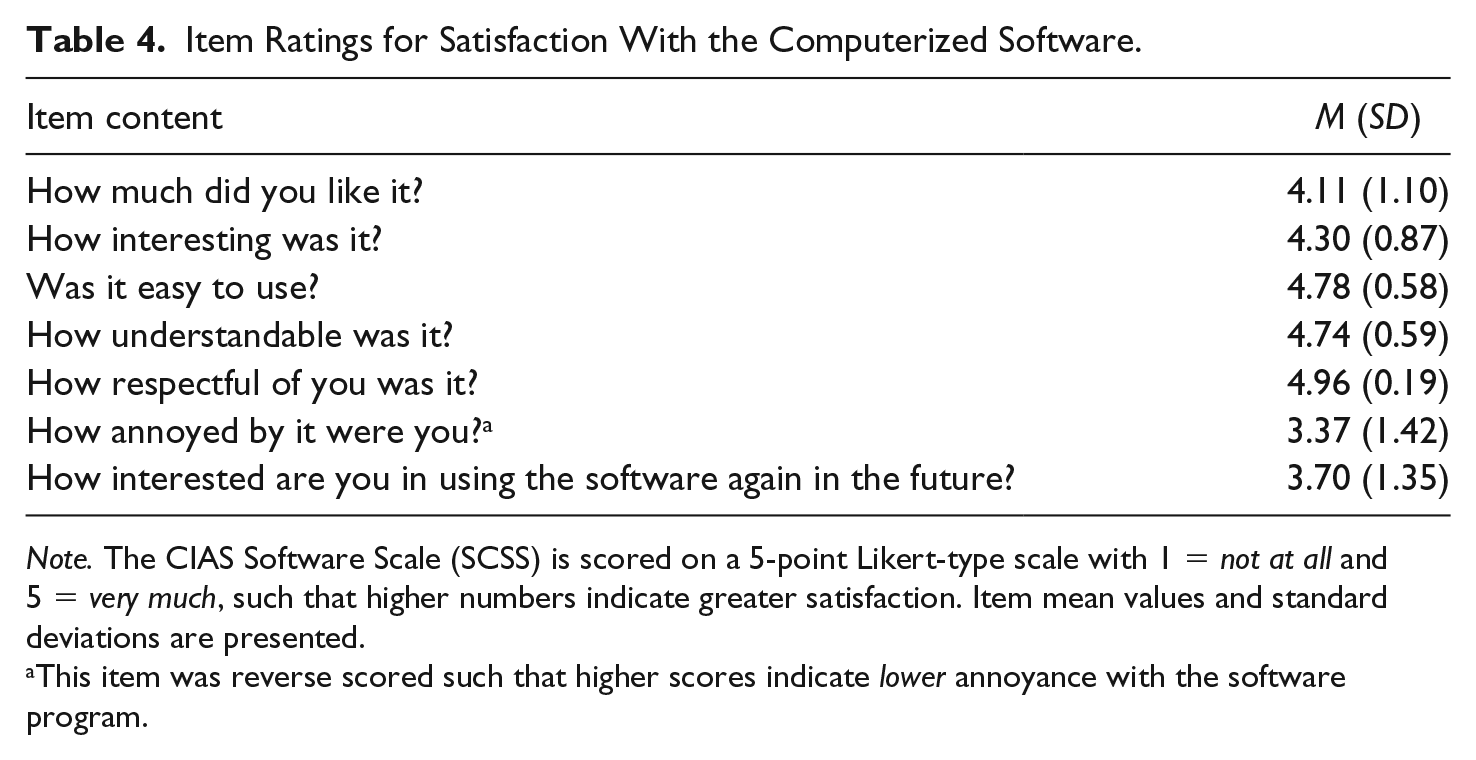
Note. The CIAS Software Scale (SCSS) is scored on a 5-point Likert-type scale with 1 = not at all and 5 = very much, such that higher numbers indicate greater satisfaction. Item mean values and standard deviations are presented.
This item was reverse scored such that higher scores indicate lower annoyance with the software program.
Health Risk Outcomes
Given the limited number of participants in each group, preliminary analyses were conducted on the mental health outcomes of hazardous drinking, IPV, and PTSD. Scores on the outcome measures were then used to evaluate whether women continued to meet criteria for each health risk across time from the baseline, to the 2-month, and 4-month assessments. Results are presented for each health risk, respectively. For a summary, see Tables 5 and 6.
Health Risk Scores for Combined Sample (N = 18).

Note. Combined data (i.e., not divided up by health risk group) are presented for the 18 participants who completed all three assessments, at baseline, 2 months, and 4 months. In this study, the hazardous drinking health risk was defined as a score greater than or equal to 8 on the AUDIT, the IPV health risk as a score greater than or equal to 3 on the CAS, and the PTSD health risk as a score greater than or equal to 33 on the PCL-5. IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
Baseline, 2-Month, and 4-Month Health Risks by Group.

Note. Data are presented by health risk group for the 18 participants who completed all three assessments, at baseline, 2 months, and 4 months. Note that 10 women (55.5%) reported more than one health risk and thus are included in multiple groups. In this study, the hazardous drinking health risk was defined as a score greater than or equal to 8 on the AUDIT, the IPV health risk as a score greater than or equal to 3 on the CAS, and the PTSD health risk as a score greater than or equal to 33 on the PCL-5. IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
Hazardous drinking
At baseline, eight women met criteria for the hazardous drinking health risk. All the assumptions for parametric tests were met except sphericity was violated, so the Greenhouse-Geiser correction was employed. A repeated measures analysis of variance (ANOVA) test on hazardous drinking indicated that there was a nonsignificant trend toward a decrease in hazardous drinking over time, F(1.12, 7.90) = 4.13, p = .07, η2 = .42. At baseline, eight women met criteria for this health risk, which decreased to four women at the 2-month follow-up and to two women at the 4-month follow-up.
IPV
At baseline, 10 women met criteria for the IPV health risk. The data for this group violated the assumption of normality, thus data were log-transformed to correct this issue. A repeated measures ANOVA on IPV indicated a significant decrease in IPV over time, F(2, 18) = 5.83, p < .05, η2 = .38. Follow-up contrasts indicated that the majority of this reduction occurred between the baseline and 2-month follow-up, with scores decreasing by an average of 12.9 points (SD = 16.56, 95% confidence interval [CI] = [1.06, 24.74]) in this time period, and an average of only one point (SD = 0.47, 95% CI = [−0.34, 0.34]) between the 2-month follow-up and 4-month follow-up. The reduction in IPV between baseline and 2-month follow-up was statistically significant, F(1, 9) = 7.2, p < .05, η2 = .56. There was no change in IPV between the 2-month and 4-month follow-ups, F(1, 9) = 0, p = .99. At baseline, 10 participants met the criteria for IPV, which decreased to five women by the 2-month follow-up and stayed constant at five women at the 4-month follow-up.
PTSD
At baseline, 13 women met criteria for the PTSD health risk. All assumptions for parametric tests were met. A repeated measures ANOVA test on PTSD indicated a statistically significant decrease in PTSD over time, F(2, 24) = 5.98, p < .01, η2 = .48. Follow-up contrasts showed that the majority of this reduction occurred between the 2-month and 4-month follow-ups, with scores decreasing by an average of 11.31 points (SD = 17.0, 95% CI = [0.99, 21.62]) in this time period, and only 3.77 (SD = 17.01, 95% CI = [−6.51, 14.05]) points between baseline and 2-month follow-up. There was no difference in PTSD symptoms between baseline and 2-month follow-up, F(1, 12) = 0.64, p = .44, and a statistically significant decrease in PTSD symptoms between 2-month and 4-month follow-ups, F(1, 12) = 5.70, p < .05, η2 = .50.
Discussion
Women veterans are a rapidly growing demographic of VA health care users who also present with high rates of lifetime sexual trauma exposure and a cadre of related health risks including hazardous drinking, IPV, and PTSD symptoms. Women are already verbally screened by VA health care providers at certain intervals for these health risks; however, computer-based screening followed by brief intervention could increase provider capacity, reduce barriers to care, and improve health outcomes. This study is the first study, to our knowledge, to develop and assess a brief computer-based intervention (or any intervention) that specifically targets health risks (i.e., hazardous drinking, IPV, and PTSD) among women veterans with lifetime sexual trauma exposure. Results suggest that the study procedures including in-person recruitment of women from the primary care clinic, use of an iPad for assessments and intervention, content of the intervention, and process of returning to the clinic for follow-up appointments were satisfactory to women veterans, feasible to complete in the expected time periods, and did not place an undue burden on participants. In terms of the feasibility of delivering this intervention in a primary care setting, the setting was accessible for women veterans, allowed for the recruitment of an adequate sample of eligible participants, and the study procedures blended into the daily clinic procedures without disrupting patient care. The SHE intervention, therefore, has the potential to fill a unique gap in care for women veterans.
Although their numbers are growing, recruiting women into research studies at the VA can be a challenge because some VA hospitals have too few women, and women often have work and child care obligations that limit their time (Yano et al., 2010). In the current trial, 222 women were approached to enroll 20 eligible women in a period of 2 months. As women were approached while they waited to be called for their primary care appointments, some of the common reasons for declining to participate included medical illness, conflicting medical appointments, not having time to stay at the VA that day, and needing to leave right after the medical appointment to go back to work or to pick up children. These are many of the same barriers that have been cited in larger studies of women veterans. Despite these barriers in this study, in-person recruitment within a high-volume women’s primary care clinic was a successful strategy. Enrollment and completion data for the open trial also indicate the study procedures were satisfactory to participants and feasible in this setting, suggesting use of computer-based screening, assessment, and intervention is a promising methodology for addressing women’s health concerns. Participants also reported a high level of satisfaction with the SHE intervention. Although testing in a larger sample is needed, given that prior work has found that women reported VA mental health services did not fully meet their needs (Kimerling et al., 2015), the current results suggest that it is worth evaluating whether SHE can serve as an avenue for delivering high-quality, gender-sensitive mental health care at the VA.
Study findings must be interpreted in light of several important limitations including low power due to the small sample size, lack of a control group, and lack of a randomization trial design. However, the goal of the current open trial was to determine whether study procedures were satisfactory and feasible and whether there was preliminary support for the hypothesis that SHE would lead to reductions in the targeted health risks of hazardous drinking, IPV, and PTSD. We are currently conducting a fully powered randomized controlled trial comparing the SHE intervention to a screening and referral-only control group.
Implications for Practice and Policy
Results from this study indicated that women who completed the SHE intervention evidenced reductions in hazardous drinking (48% reduction), IPV (53% reduction), and PTSD (29% reduction), at 4 months postintervention. These are promising findings for an intervention that uses a novel and brief delivery method. The computerized approach addresses several patient barriers to seeking treatment for sexual trauma-related concerns which include stigma, and competing work and child care obligations (Richens et al., 2010). Providers often struggle to address sexual trauma concerns in a trauma-informed and gender-sensitive manner (Iverson et al., 2013). Findings from this study suggest the SHE intervention with its patient-centered and collaborative approach may reduce health risks associated with sexual trauma exposure in a manner that addresses some of the barriers and challenges faced by both patients and providers.
Conclusion
Despite growth in the number of women veterans receiving care at the VA and growth in research on women veterans, intervention research with women who have experienced sexual trauma has consistently lagged far behind observational studies (e.g., Danan et al., 2017; Goldzweig et al., 2006). The present findings from this open trial of the SHE intervention, and the randomized clinical trial of SHE currently underway, offer a novel intervention to meet the needs of women veterans experiencing highly stigmatizing and sensitive health risks related to lifetime sexual trauma exposure. Women veterans have distinct health care needs that call for high-quality, trauma-informed and gender-specific interventions. Results from the present open trial suggest the satisfaction and feasibility of the SHE intervention, as well as promising reductions in hazardous drinking, IPV, and PTSD.
Footnotes
Authors’ Note
ClinicalTrials.gov identifier: NCT02957747.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Zlotnick has one conflict of interest to report; her spouse, Dr. Gordon, has served as a physician advisor consultant to a technology company, Soberlink. This company manufactures breathalyzer equipment. Soberlink technology was not used in this study. The authors have no other conflicts of interest to report. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. Government.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Department of Defense, W81XWH-14-1-0368. The writing of this manuscript was partially supported by the Office of Academic Affiliations Advanced Fellowship Program in Mental Illness, Research, and Treatment, and the VISN 17 Center of Excellence for Research on Returning War Veterans.