
Abstract
Reproductive coercion (RC) refers to behaviors that interfere with contraception use or pregnancy and that limit reproductive autonomy. This article presents the results of a qualitative exploratory study of 21 young women in Canada who experienced RC perpetrated by an intimate partner along with the associated consequences. Results reveal that nonconsensual condom removal occurred more often in uncommitted relationships without violence, whereas pressure to become pregnant and pregnancy coercion occurred more often in committed relationships where other forms of violence were also present. Participants reported numerous repercussions on their psychological, sexual, and reproductive health and on their emotional and relational well-being.
Background
Intimate partner violence (IPV) and sexual violence are serious and widespread societal problems (World Health Organization, 2014). Proportionately more women than men report these forms of violence and suffer the consequences (World Health Organization, 2013). A more specific form of sexual violence called reproductive coercion (RC) occurs when reproductive health issues are combined with violence. It is defined as “a behavior that interferes with contraception use and pregnancy in ways that reduce female control over reproductive decisions” (Silverman & Raj, 2014, p. 2). A recent review of the U.S. literature reveals that RC prevalence varies from 5–13% for women aged 16–29 years who consult a family planning clinic (Grace & Anderson, 2018). In a population-based sample (Black et al., 2011), the prevalence was 9%. To our knowledge, no data on prevalence rates are available in Canada. Studies indicate that the majority of those who experience RC are women. In fact, RC can be considered a gendered behavior that has been facilitated by a long and ongoing history of female oppression. RC acts to intervene in women’s reproductive decisions about contraception, pregnancy, childbirth, child rearing, and other such matters (Chrisler, 2012).
Overview of the Literature
RC has been largely defined in terms of three categories of behaviors (Brodsky, 2017; Chamberlain & Levenson, 2012; Grace & Anderson, 2018; Miller & Silverman, 2010; Nikolajski et al., 2015). First, birth control sabotage includes acts such as condom damaging, nonconsensual condom removal during sex, and nonconsensual removal of a contraceptive device (vaginal ring, intrauterine device [IUD], or patch). Second, pregnancy pressure includes pressuring a sexual partner to become pregnant (e.g., threatening to be unfaithful or to leave if she does not comply). Third, pregnancy coercion includes forcing a reluctant partner to have an abortion or, inversely, forcing her to bring her pregnancy to term. Contraceptive interference is an emerging concept in the literature. It differs from RC in this aspect: the partner’s contraceptive decisions are ignored, but there is no deliberate intention of causing pregnancy. Still, a woman’s reproductive autonomy is undermined when a condom is removed without her knowledge. Alternatively, the male partner may pretend to wear a condom, even though the couple had already agreed to use a condom during sexual intercourse, as seen in RC (Katz et al., 2017; Katz & LaRose, 2019).
The known associated factors for increasing the risk of RC include ambivalent attitudes toward pregnancy (Patel et al., 2015), low socioeconomic status (Clark et al., 2014), visible minority status (Clark et al., 2014; Miller et al., 2010, 2014; Sutherland et al., 2015; Upadhyay et al., 2014), low education level (Miller et al., 2010, 2014; Upadhyay et al., 2014), and being single or in a dating relationship compared with being married (Clark et al., 2014; Miller et al., 2014). However, current or past history of IPV remains the strongest predictor of RC (Dick et al., 2014; Katz et al., 2017; McCauley et al., 2014; Sutherland et al., 2015). Nevertheless, some women report having experienced RC in the absence of IPV (Brodsky, 2017).
Studies have documented numerous harmful effects on the health and well-being of women who experienced RC. These include greater use of emergency contraceptives (morning-after pills) and abortions, more frequent unplanned pregnancies, and higher risk of sexually transmitted infections (STIs; Brodsky, 2017; Grace & Anderson, 2018; Holliday et al., 2018; Jones et al., 2016). Other studies have shown that RC restricts a woman’s choice, negotiation power, and use of contraceptive methods (Jones et al., 2016; Katz et al., 2017). For example, Jones et al. (2016) found that adolescents and young adults who had experienced recent RC reported lower ability to negotiate condom use, indicating problems in voicing their opinions and contraceptive choices. Similarly, pressure by their partners contributes to women’s ambivalent attitudes toward pregnancy and nonuse of contraception (Nikolajski et al., 2015). Furthermore, although the research focuses on physical health repercussions, women who have experienced birth control sabotage may also suffer psychological impacts such as fear, shame, and feelings of being deceived and abused (Brodsky, 2017). For example, in a qualitative study based on individual interviews and online forums, women who experienced nonconsensual condom removal (“stealthing”) felt that this act violated their bodily autonomy and trust (Brodsky, 2017). However, the knowledge in this area is limited, particularly concerning the different manifestations of RC and the relational contexts in which they occur. For example, studies have generally split the types of relationships into two opposing categories (single vs. in a relationship), although more recent studies have explored a broader spectrum of relational configurations (Rodrigue & Fernet, 2016). In addition, few studies have considered the different health components (physical, psychological, and sexual) of RC or the repercussions of RC on relational well-being.
RC: A Dynamic of Power and Control?
The IPV research has generally emphasized the concepts of power and control, domination and control, and coercive control (Hamberger et al., 2017). All these refer to systematic patterns of behavior meant to dominate another person through intimidation, isolation, threats of violence, or intimate terrorism (Dichter et al., 2018). Johnson (2008) proposes a typology that considers the context of domestic violence (i.e., IPV) not as a unitary phenomenon, but as a variegated and far-reaching social dynamic. This dynamic takes three main, conceptually distinct forms: intimate terrorism, violent resistance, and situational couple violence. The first two forms include coercive control. However, it is the third form (situational couple violence) that is reported more often in population surveys (Johnson, 2008). Coercive control in a couple relationship marked by IPV generates fear even when physical violence is absent (Crossman et al., 2016). It is a form of nonreciprocal authority that subverts the victim’s autonomy. In other words, it violates basic rights and freedoms (Stark, 2007). Coercive control follows two pathways. On one hand, coercion is effected through aggression, intimidation, harassment, stalking, threats, and humiliation. On the other hand, control is maintained through isolation, deprivation, exploitation, and imposed rules (Stark, 2007). Whereas coercive control was formerly thought to be based on physical violence (Johnson, 2008), more recent studies have demonstrated that all forms of coercive control behaviors raise the odds of violence in a relationship (Dichter et al., 2018; Graham-Kevan & Archer, 2008) as well as the risk for revictimization (Dichter et al., 2018). These findings concur with Blasco-Ros et al. (2010), who found that, compared with women who were exposed to both coercive control and physical violence, women who were exposed to coercive control alone were more likely to report persistent exposure 3 years later.
In the case of RC, a few studies have specifically addressed how control and coercion manifest, but they have neglected the relational context in which they occurred. Several questions remain unanswered. For instance, does RC manifest differently depending on the relational context? Is RC always accompanied by control behaviors? Do the consequences vary across forms of RC? To answer these questions, we gathered the perceptions of young women who experienced RC. This study examines the presence or absence of coercive control as reported by women who experienced RC, and in terms of the relational contexts and the associated repercussions. The objective was to better understand the different manifestations of RC and their consequences on health and well-being. This article (a) demonstrates how the relational context modulates the forms of RC; (b) identifies the main consequences of RC on physical, psychological, and sexual health and relational well-being according to the form of RC experienced and the relational context; and (c) based on the findings, discusses the boundaries of the concept of coercive control.
Method
Participants
The participants were 21 cisgender women aged 18–29 years (M = 24.85; median = 26; SD = 2.81). Of the sample, most (95.2%) held Canadian citizenship. The majority (71%) were Caucasian, and 10% had Caribbean origin, 10% North African origin, and 5% Asian origin (n = 1). Most identified as heterosexual (n = 15; 71%), with some bisexual (14%), queer (10%), or asexual (5%). At the time of the interviews, the majority were students (62%), 24% were employed full-time, and 13% were on social assistance. The majority (81%) had completed postsecondary studies.
Procedure
The study protocol was approved by the ethics committees of the main researcher’s university and of the 6 CEGEPs (Québec’s college equivalent) that participated. A purposive sampling procedure (Patton, 2002) was used according to the following criteria: age 18–29 years, has experienced RC in the last 2 years in the context of an intimate relationship involving or not an emotional attachment to a male partner, and French-speaking. The participants had to acknowledge that RC-related experiences or situations similar to those in the recruitment ads had occurred (e.g., “Has your partner ever sabotaged your birth control method without telling you?”; “Has he ever pressured you to get pregnant?”; “Has he ever forced you to terminate a pregnancy, or forced you to continue one?”). Prior to the interview, participants acknowledged that they had experienced RC as a form of violence, despite the fact that some felt responsible for the RC. One respondent did not self-identify as a victim or feel that she had been coerced (although she was disappointed and frustrated). Nevertheless, she indicated that it was a case of RC-associated behavior.
Participants were recruited in Montreal (Canada) via flyers placed in colleges and universities as well as ads and business cards posted in abortion clinics, via social media, and through several community groups that work with female victims of violence. Twenty-one participants underwent individual in-depth interviews from March 2017–May 2018. An additional 11 women initially contacted the team to participate in the study, but of these, two lost interest, six failed to confirm the interview appointment, one was younger than 18 years, and two did not meet the inclusion criteria. The 60- to 90-min interviews were generally conducted in a private office at the university, and all were audio-recorded. All participants received a monetary compensation of CAD$30. Prior to the interviews, they gave their verbal and written informed consent to participate.
Measures
Individual interviews
An in-depth interview guide was developed for this study. The themes included the participant’s representation of her intimate relationship; RC manifestations, chronicity, and crystallization over time; acknowledgment of RC; coping skills; and contacts with health professionals and/or community counselors. The interviews were semi-structured and contained open-ended, nonleading questions. The interviewers asked follow-up questions according to the participants’ responses to lead-off questions. After the initial interviews, we adjusted the interview guide slightly, because several participants mentioned how their resilience paths had been influenced by disclosure movements on social media (e.g., #BeenRapedNeverReported; #MeToo). After being interviewed, participants completed a brief questionnaire on sociodemographic characteristics.
Data Analysis
Verbatim transcriptions of the interviews were obtained. The data treatment comprised a thematic analysis (Braun & Clarke, 2006) using NVivo 11 (QSR International Pty Ltd.). Thematic analysis is a “method for identifying, analyzing, and reporting patterns (themes) within data” (Braun & Clarke, 2012). We began with an active reading of all transcripts. Next, we generated an initial coding and identified themes. After considering the themes and labeling them appropriately, we selected the extracts that best represented the analysis results. To improve the credibility and achieve consensus on the coding and analysis, we triangulated the results by soliciting the expertise of three analysts, and we held ongoing group discussions.
Results
The thematic analysis yielded a classification of the RC forms according to the relational context. Moreover, we identified control as a core element of RC whose focus varies according to the relational context. Based on the central theme, the relational context modulates the manifestations of RC, we identified four subthemes featuring control: (a) RC in a committed relationship with violence mainly concerns the control of the partner; (b) RC in a committed relationship without violence can also target partner control, but in a subtler way, passing for concern; (c) RC in a casual uncommitted relationship is about contraceptive disempowerment and control over the sexual relationship; and (d) RC in a long-term uncommitted relationship is about denying women’s reproductive choices. Another central theme was the repercussions of RC on health and well-being.
The Relational Context Modulates the Manifestations of RC
Women experience different forms of RC, and these forms differ according to the relational context. To understand RC according to the relational context, we created four categories of relational context. These relational categories, created by the research team, are based on the participants’ description of their relationships. They were asked questions about their relationship (How do you describe your relationship? Can you tell me a little more, followed by probes), which helped create an empirical corpus from which these four profiles emerged. They are (a) committed relationship with violence (i.e., generally referred to by the participants as a “couple,” where there is violence and a dynamic of power imbalance, violence and control), (b) committed relationship without violence (i.e., a romantic relationship where the participant does not report violence or power imbalance), and (c) casual uncommitted relationship (i.e., described by the participants as a casual/one-night stand, an occasional sex hook-up), and (d) long-term uncommitted relationship (i.e., described by the participant as a longer-term relationship without romantic commitment, but within which a link is present between the partners, for example, “friends with benefits”).
We classified the RC testimonials according to the relational context to obtain a more nuanced understanding of the associations between the manifestation and consequences of RC and the presence of IPV. In the committed relationships with violence, RC manifested in many forms and was accompanied by other forms of IPV. In the committed relationship without violence, RC manifested as control over the choice and use of contraceptive method. In the casual uncommitted relationships, RC manifested solely as nonconsensual condom removal, while various forms are present in the long-term uncommitted relationship. Table 1 presents the RC manifestations according to the relational context along with some illustrative extracts.
Manifestations of Reproductive Coercion Classified by the Relational Context.
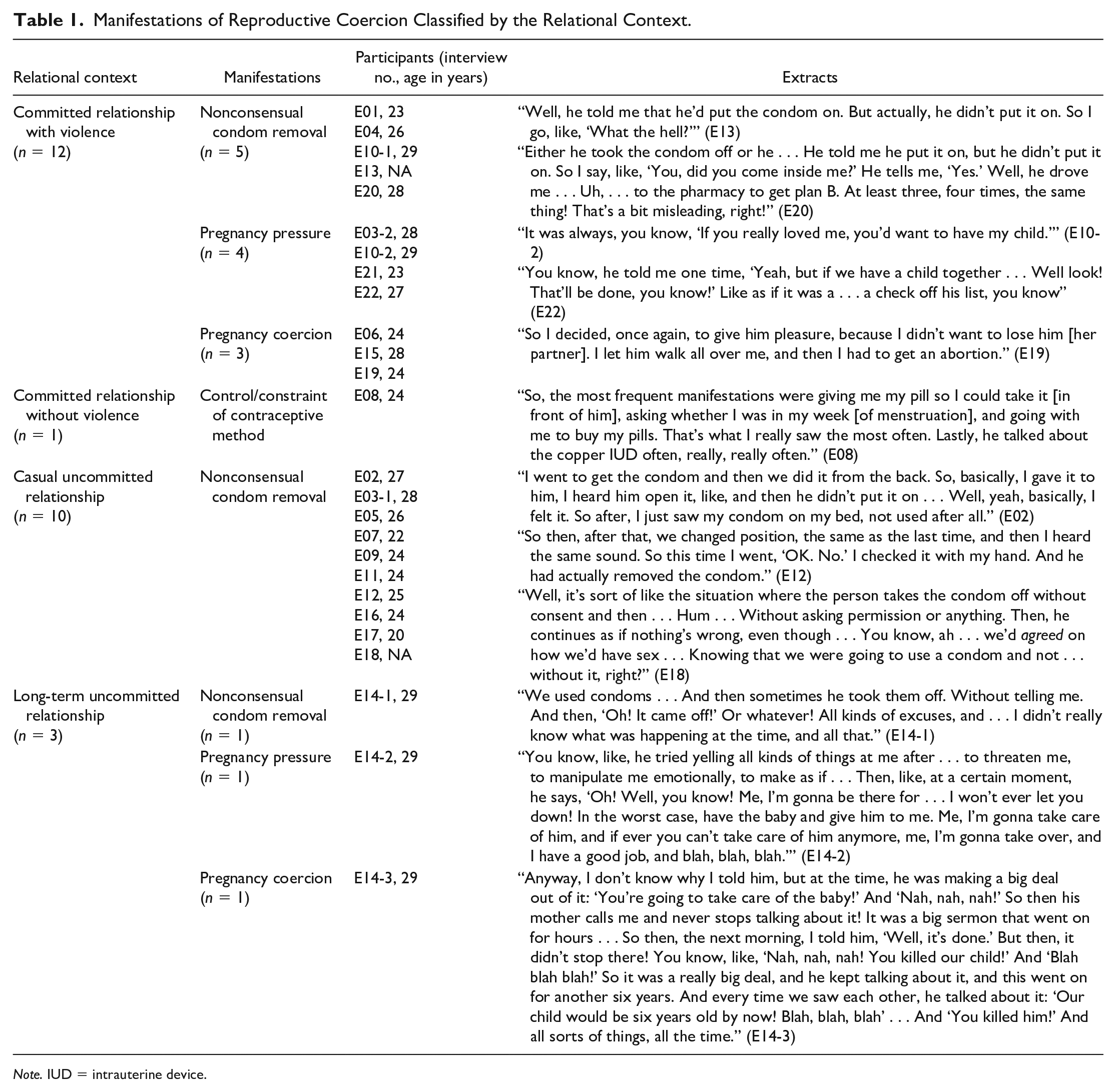
Note. IUD = intrauterine device.
RC in a committed relationship with violence mainly concerns the control of the partner
As mentioned above, various forms of RC, namely, nonconsensual condom removal, pregnancy pressure, and pregnancy coercion, were reported in the committed relationship with violence context. The analysis of the RC manifestations indicates that they occurred concurrently with coercitive control and other forms of violence (e.g., psychological, sexual, economic). Three participants who had experienced nonconsensual condom removal explained that their partner wanted to increase his sexual pleasure. However, unlike the case for uncommitted relationships without violence, these women were also insulted and/or belittled. Per example, one participant was often criticized for not being sexually exciting enough, making it harder to use a condom due to a weak erection (E01).
Pregnancy pressure sometimes manifested as recurrent comments about the partner’s desire to have a child. Male partners were insistent on this, and disinterested in the participant’s own reproductive preferences. For example, one participant said that her partner used emotional blackmail: “It was always like, if you really loved me, you’d want to have my baby” (E10). This psychological pressure was often accompanied by physical and sexual violence. For instance, one participant said that her partner forced her to have sex and threatened to be unfaithful if she did not give in. Pregnancy pressure could also manifest as monitoring fertility periods: “One time, he bought a pregnancy test, and then he kind of dipped it into the toilet after I peed” (E10).
The reported cases of coercion during pregnancy also included emotional blackmail by the partners, some of whom threatened to break up with the participant if she refused to have an abortion. One participant explained that she had told her partner she wanted to have a child, and he seemed to feel the same way. This was followed by unprotected sex. When it turned out that she was pregnant, her partner said that if she did not have an abortion, he would leave her (E06). When two other participants became pregnant unexpectedly (after contraceptive failure), their partners threatened to leave if they did not get an abortion. In all three cases, the partner allowed no discussion and threatened to end the relationship, forcing the participant to comply with his wishes. Nevertheless, one participant chose to keep her child, and thereby lost her partner (E19).
RC in a committed relationship without violence can also target partner control, but in a subtler way, passing for concern
Only one participant (E08) had been in a committed relationship without IPV, and she reported control over her contraception, a form of RC that appears to have been overlooked in the literature. In this exceptional case, the partner exerted pregnancy pressure by attentively supervising her birth control method. He watched her take her pill, monitored her menstrual cycle, checked to see that she got her period, and forced her to get emergency contraception if he thought there might be a risk of pregnancy. In addition, he tried to force his partner to use another contraception method (an IUD): “He asked me to use a contraception method that I considered invasive . . . a more long-term method. So that he could have another five years, like that [without a child]” (E08). This respondent initially had difficulty recognizing that her partner had restricted her reproductive autonomy. At first, she thought that he was simply “involved” in the contraceptive plan. Over time, however, she realized that his behavior was problematic. She became aware that her partner did not trust her, was overseeing her, was applying psychological pressure, and did not respect her contraceptive choices. With this observation came significant stress.
RC in a casual uncommitted relationship is about contraceptive disempowerment and control over the sexual relationship
The participants who had been in a casual uncommitted relationship reported nonconsensual condom removal as the only form of RC (n = 10). Although they had all told their partner that they wanted to use a condom before having sex, their partner put the condom on at first and then removed it later (and some just pretended to put it on), unbeknown to the participant. As one explained, At first, he wanted to start [sex] without a condom. I asked him, “Do you have a condom? Because I don’t really know you. I don’t know if you have something [STIs]; you don’t know if I have something [STIs].” . . . He’s probably clean, but I don’t know. So then he says, “Of course, I’ve got one.” He puts it on. . . . He did it behind my back. We were in a position where I couldn’t see what he was doing. At one point, I turned around, when we were changing position, and I realized he didn’t have the condom on anymore. (E03)
Here, the male partner reneged on the agreement to use a condom and deceived his sexual partner. These participants felt that their partners wanted to increase their own sexual pleasure, and they considered this behavior both irresponsible and disrespectful. Importantly, it also showed a complete disregard for the potential consequences, such as an STI or unwanted pregnancy. This act of contraceptive disempowerment carried a further mental burden: As one participant explained, “I was the only one who was responsible for not getting pregnant” (E16). Although the participants did not feel that their partner wanted to control their reproductive life, the partner’s behavior was viewed as taking control of the sexual relationship. Many participants acknowledged that their partner had controlled the sexual relationship by ignoring their wishes, which is equivalent to usurping their physical and reproductive autonomy.
RC in a long-term uncommitted relationship is about denying women’s reproductive choices
One participant (E14), who had been in a long-term uncommitted relationship, reported being exposed to three forms of RC: her partner had pressured her to have a child, he had repeatedly removed his condom without her consent, and he had tried to force her to continue an unwanted pregnancy. She reported that after she had an abortion, her ex-partner frequently tried to make her feel guilty about having the abortion (e.g., claiming that she had “killed their child” and reminding her how old their child would have been by now). These repeated accusations following the woman’s independent decision to have an abortion appear to have been attempts to control her physical and psychological integrity as well as her reproductive autonomy. This participant did not identify, at the time of the interview, the presence of violence in her uncommitted long-term relationship. However, the various examples and descriptions of her relationship shared during the individual interview led us to believe, as researchers in the field of violence against women, that IPV was indeed present.
The results presented in this section show that it is the common experience of violence between intimate partners that markedly distinguishes experiences of RC. Indeed, the two categories of relationships comprising IPV, acknowledged or not, reveal different forms of RC, whereas relationships without intimate violence present RC profiles in which the nonconsensual withdrawal of the condom predominates. Although this manifestation of RC is indeed a form of violence against women, the concept of control, as described by women, varies. In committed relationships, it is aimed at controlling the person, whereas in noncommitted relationships, it is primarily aimed at controlling sexual intercourse, which generates a loss of power over contraception, and cancels consent at the same time.
Repercussions of RC on Health and Well-Being
The participants reported diverse consequences of RC on their emotional and psychological health, their sexual and reproductive health, and their relational well-being. Table 2 presents the repercussions according to the relational context in which they occurred. The consequences presented in the top row were reported across all cases, regardless of the relational contexts in which RC was present. However, the relational context can modulate how the repercussion is understood or experienced, as evidenced by the results presented below. Lines 2 and 3 present the additional consequences that were specifically reported in committed relationships with IPV and in uncommitted relationships—whether ad hoc or long-term—respectively. The consequences reported by the participant in a committed relationship without violence are not distinct from the other relational categories, and therefore are reported in “across all cases,” which explains the absence of this category in the table.
Consequences According to the Relational Context (Total No. of Situations = 26).
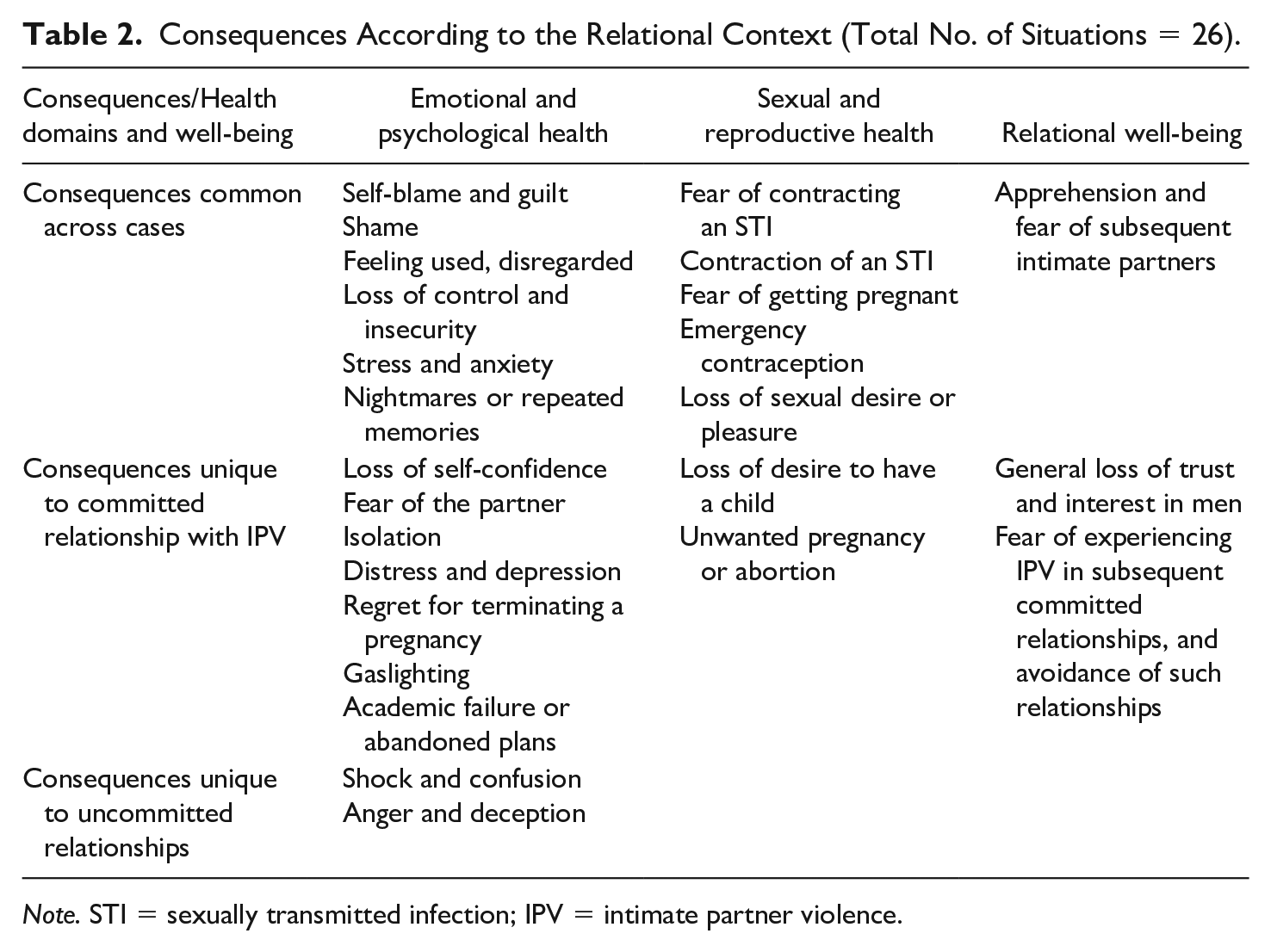
Note. STI = sexually transmitted infection; IPV = intimate partner violence.
Repercussions on emotional and psychological health
Across all cases
The consequences affected the participants’ emotional and psychological health. First, they felt guilty, especially when they had experienced one or more incidents of nonconsensual condom removal in an uncommitted relationship without IPV. The guilt specifically concerned having sex with a person whom they did not know very well, if at all. Many felt that they had put themselves at risk. As one explained, The first thing that came into my head was, you know, like, “You’ve got to stop getting into situations like this, and you’ve got to stop taking these risks.” (E05)
Those who had been in a committed relationship with IPV felt guilty about all the forms of violence they had experienced. One participant who had been pressured to get pregnant asked herself, “How come I didn’t try to stop him? Why couldn’t I stand my ground? How come I didn’t leave earlier?” (E10). Similarly, many participants who had been forced to have an abortion blamed themselves for ending their pregnancy instead of the relationship: “I felt guilty because I ended my pregnancy” (E19).
Many participants said that they had felt ashamed, which had prevented them from sharing their situation with their friends or a health professional. Some said that they were worried that other people would think of them as powerless, and it had discouraged them from opening up: I didn’t feel like sharing my story. I think there was some shame, yeah. I think that I didn’t . . . It’s like . . . I didn’t want to be “the girl who can’t say STOP” (during sex when she realizes he took off the condom). Maybe I felt weak, because I couldn’t take the initiative. (E07)
Many who had been in an uncommitted relationship said that they feared being judged for agreeing to have sex with someone whom they did not know very well, if at all. For those who had been in a committed relationship, shame, embarrassment in front of their friends, or looking vulnerable had inhibited them from speaking up. For example, one participant who had been pressured to get pregnant explained, I was afraid of how they were going to think of me, you know? My friends know me as, like . . . as having a personality that’s really strong. So to see that I wasn’t that person anymore . . . I think that it was . . . It was embarrassing. (E21)
Many felt despised and used. They felt objectified, as described by this participant who had experienced nonconsensual condom removal in a casual uncommitted relationship: The feeling of just being treated like an object. Like, I didn’t feel very good after. I felt disrespected. I didn’t feel . . . human. I was just . . . a piece of flesh. I was just there to get banged, and nothing more. (E11)
Because her consent had not been respected, she felt dehumanized by her partner’s behavior. Many of those who had been in committed relationships felt the same. One felt that her partner’s refusal to wear a condom following endless discussions came down to a lack of respect: “I felt really. . . uncomfortable. I was uncomfortable not using the condom. Him, he knew it! But like I said, he didn’t give a damn about me” (E21).
The majority of the participants felt that they had lost control when RC occurred. One who had experienced nonconsensual condom removal in a casual uncommitted relationship expressed herself as follows: “At the time, I felt sort of powerless. Or I felt naive, or . . . I don’t know. I just went ‘OK.’” (E07). There is some confusion about what consent means as well as the right to back out at any time. In this case, the misunderstanding of consent includes the notion of protected sex. The feelings of loss of control or insecurity can be accentuated by the power dynamic that operates in RC situations. Therefore, powerlessness can be exacerbated by many factors. For instance, being younger than one’s partner alters the balance: “Because he’s older, he’s the one who has to, like. . . . He’s the one who gets to decide . . . which means that, like, I shouldn’t question whatever he likes, if he wants to do it” (E17).
Another factor was being (or perceiving oneself to be) physically weaker: “I was better off not resisting, not putting up a fight; it would just be simpler! The other person is stronger than me, anyway!” (E12). In fact, diverse factors can influence the power in relationships. When these factors are expressed or implicit in sexual relationships, they nourish feelings of apprehension and fear, such that some participants were reluctant to state their wishes and boundaries. Feelings of loss of control were also present in the committed relationships, but they were expressed differently. One participant who had experienced pregnancy pressure was particularly worried about getting pregnant because it represented a loss of control over her own body: I felt like . . . I’d lost control. I lost control and I was just like “ok.” I was afraid. I was already unsure about what I was doing. I didn’t know what to do anymore. I didn’t know what I was doing anymore . . . I was really overwhelmed. (E21)
Four participants had nightmares and flashbacks following RC incidents, and stress and anxiety were also reported, for all forms of RC experienced. One participant who had experienced pregnancy coercion recounted: There were many times when I took a pregnancy test and I was really stressed out because I did them in secret. Like . . . I didn’t want him to be there, or, you know, if he found out. I went and threw them away in the park so he wouldn’t find them. . . . I think that I didn’t want him to know that I was pregnant. Because that left me more . . . you know, that left me more freedom to decide later, if it ever happened that I should get pregnant. (E10)
Committed relationships with IPV
Specifically, for committed relationships with IPV, the consequences included loss of self-confidence, social isolation, distress, fear of the partner, and lower motivation to carry out personal plans. For example, one participant recounted how her partner’s disrespect eroded her self-confidence: “It’s really destructive, being in a couple like that . . . for self-esteem. It destroys, like . . . It really makes me feel ashamed” (E22). Some participants said that their partner’s behavior led to social isolation. One explained how her partner had gradually controlled her outings so that she ended up being cut off from her friends and family: It’s sort of like everything is set up to control me, and that means to destroy . . . to take away my support, whether it’s, you know, my friends. He prevented me from seeing my friends a lot, from going out, and from going out without him, you know. (E10)
Three participants mentioned distress and depression, particularly in situations of pregnancy coercion, as explained by one participant who was forced to have an abortion: “I didn’t feel good; I was depressed; I was anxious . . . I spent six months locked up, crying every day” (E15). One participant who had been in a committed relationship with IPV explained that she was “gaslighted,” such that her memory was affected: This one memory, that I had. . . . It never came back completely clearly for me, because at the time, with the feelings, he was always doing this, you know: “You’re the one who’s mixed up,” or “You know very well it didn’t happen like that.” (E10)
In addition, some participants described failing in their studies or abandoning personal plans following RC incidents.
Uncommitted relationships
Specific consequences were reported by the participants who had been in uncommitted relationships. They described a state of shock and confusion when the behavior took place, which led to denial that could last for varying lengths of time, ranging from a few hours or days to several weeks or months. One participant described how shocked she felt after nonconsensual condom removal in an uncommitted relationship: I woke up the next morning; I honestly felt really bad, but I was so confused . . . I was actually really lost. I understood more as time went on. It was like I was all conflicted. That’s how it was. (E12)
Many participants also felt angry and frustrated with their partner. For some, this anger increased when they realized the consequences for themselves. In the words of one participant who had been in an uncommitted relationship: When I truly saw all the shit that I had to do: go to the drugstore (to get emergency oral contraception) . . . It was me who got stuck with all that. . . . It cost me money because it was the weekend, and I couldn’t go to the community health center. So I am the one who paid that money. I started to get mad when I realized the repercussions. Then also, when I thought about the notion of consent that was really uh . . . absent. (E16)
These stories illustrate the difficulty the participants had acknowledging the fact that they had been victims of an aggression, which sometimes led to denial. As described elsewhere (Lévesque & Rousseau, 2019), acknowledgment of RC varies according to the emotional bond with the perpetrator and the behaviors that were experienced. For example, nonconsensual condom removal was the most readily identified form of RC, whereas it could take longer to acknowledge pregnancy pressure and pregnancy coercion. In addition, it might take recurrent incidents before it was identified as a form of violence. Furthermore, it was easier to acknowledge RC when relationships were casual and uncommitted compared with romantic and committed.
Consequences for sexual and reproductive health
Across all cases
Regardless of the relational context, many participants said that they were afraid to catch STIs, which drove some of them to get screening tests. However, the screening procedures sometimes took time, and then the fear of being infected would persist: I started to feel a kind of psychological distress about my health, all because I didn’t know. And this distress hasn’t gone away, even today, because it’s been a month and a half, and HIV and other diseases like that, it can take up to two- two and a half months before they’re detected. So I take the tests every month and I don’t know if I’m sick or not. (E12)
These risks are real. One participant said she had contracted an STI after an incident of nonconsensual condom removal. Conversely, one participant who had been in a committed relationship in which she was pressured to get pregnant gave her partner an STI. Although she had informed him about her condition, he insisted on not using a condom (E21). This led to escalating violence: When we stopped using the condom, I gave him herpes and it was really not funny. He was crying, it hurt him and it also hurt me to see how he was because of me. After that, after every little argument, he made sure that I was to blame. So I felt terrible. I felt so, like . . . guilty . . . for giving it to him, because I was the one who brought it into the relationship. . . . After that, he started to insult me, to treat me like a slut! He called me names, bad names . . . very, very mean names. (E21)
Some also feared getting pregnant, as one participant who had experienced nonconsensual condom removal reported: “It’s a lot of responsibility, because after that, you have to wait for your period, so it’s a pretty stressful thing” (E16). Some participants who feared getting pregnant had to get emergency birth control. Using oral emergency contraception and then undergoing screening tests created additional mental and physical burdens for women, as one participant explained: “I had to go and get the morning-after pill, and that’s really . . . it’s a lot of time, a lot of energy out of your day” (E16).
Participants who had been in uncommitted relationships also reported lower sexual desire and/or pleasure after their partner had violated their sexual consent (n = 4). This participant said she completely lost desire for her partner: Him and me, we had been attracted to each other, but then what happened sort of stopped all that, actually. What happened de-eroticized him. I was quite disgusted when I thought about him, and what made it sort of worse was the fact that he didn’t use a condom, the fact that I had his sperm inside me as well, which was what really disgusted me. (E16)
It was similar for participants who had been in committed relationships. As one who had experienced pregnancy pressure explained: “I don’t feel like having sex. Because of that. He didn’t respect my decisions. He was very controlling. And, like, if I have sex, I could get pregnant” (E21). For some, the consequences of RC on sexual well-being were more long-lasting: In terms of my sex life, I think that’s the worst part [silence]. Well, to actually heal, I mean. To be able to feel my, you know, my libido, or my desire to have sex or not, as like, well, something that, you know, that belongs to me or is my right. (E10)
Committed relationship with violence
For some participants who had been in committed relationships with IPV, RC negatively affected their desire to have a child: And I still feel the aftereffects of all that. My biggest fear is that I’ll get pregnant without knowing it. . . . And since I’m anxious, it doesn’t help. So uh . . . I always check to make sure the condom doesn’t have a hole in it. (E13)
Participants who had experienced pregnancy coercion (e.g., unwanted pregnancy or unwanted abortion) reported negative impacts on their reproductive life.
Consequences on relational well-being
Across all cases
The participants reported numerous consequences that negatively affected their relational well-being. Notably, the experience of RC made some participants suspicious of their new partners: Since that time, I would say that I . . . I really pay attention to the condom. I’m really, like, vigilant. I would say that there’s a part of me that has problems just letting go, also because of that. . . . Well, for sure, let’s say that having gone through that sexual aggression, it also makes me be very careful when I’m having sex with somebody else. (E12)
Many participants said that they feared being victimized again, which heightened their caution toward intimate partners: “I think that I’ve got barriers because of this, so that I really have to build a relationship of trust with the person, because like, I don’t trust him all that much” (E02). To protect themselves, some participants avoided getting emotionally attached, especially when RC had occurred within a committed relationship: “You could say that I’m like . . . I’m stopped even before I can fall in love or get interested in somebody” (E15).
Committed relationship with violence
The consequences for relational well-being were observed specifically in participants who had been in committed relationships with IPV. These consequences therefore ensue from an overall context of violence, without necessarily being specific to RC. For one participant, RC had an impact on her intimate life and her desire for men: “I was single for two years, after. . . . I felt really lonely. You know, I wanted to be in a couple, but not with a guy” (E13). Similarly, one participant said that the consequences of RC were that she developed a fear of getting involved with another man (E01). The consequences of RC on subsequent relationships sometimes persisted. One participant said that her new couple relationship was sometimes tense, and she associated this with the repercussions of the RC she had experienced in a previous relationship (E10). Unlike the uncommitted relationships, the consequences of RC that took place in committed relationships appeared to endure, with longer-term effects on the participants.
Discussion
The main objective of this exploratory study was to identify manifestations of RC and its consequences on health and well-being according to the relational context in which it occurred. We also wanted to explore the influence of relational contexts on RC manifestations. Our results highlight the importance of considering the relational context when examining RC, because its manifestations vary accordingly. The different contexts in which RC behaviors occur were classified in terms of committed and uncommitted relationships, with or without IPV. However, despite the lack of commitment in the relationship, partners may see each other several times. We propose that the dichotomy that prevails in the literature precludes a thorough understanding of the various contexts that are associated with RC, at least, in the population of young adults who participated in the present study.
The results show that nonconsensual condom removal, which is a form of birth control sabotage, occurred mainly in casual uncommitted relationships. Although one of the risk factors for experiencing RC is being single or in a dating relationship compared with being married (Clark et al., 2014; Miller et al., 2014), this factor is less reflected in our results, because no participant was married. Therefore, the different relational contexts fall into either the single or dating relationship category. Indeed, the presence or absence of commitment in the relationship appears to have a strong influence on the form of RC experienced and its interaction with IPV. Nonconsensual condom removal also differs from the other forms of RC in terms of coercive control. According to Stark’s (2007) definition of coercive control, nonconsensual condom removal does not completely fit this conceptualization. In fact, this form of violence does not aim for domination of the woman—a key concept in Stark’s (2007) definition. Instead, it aims for control of the sexual relationship. According to the women we interviewed, the partner’s goal was not to completely restrict the woman from living freely and autonomously (Crossman & Hardesty, 2018), but rather to invalidate her needs and desires by placing the man’s needs and desires up front. Nevertheless, the aim is still subordination—another key concept for Stark (2007). Nonconsensual condom removal is a form of disempowerment that is associated with the partner’s sexual and reproductive health, as well as a disregard of her expressed choice to use a condom. We believe that contraceptive interference is a concept that should be further explored to better understand how these behaviors are operationalized. Although it shares some key elements of Stark’s (2007) framework, contraceptive interference appears to be a distinct form of RC. However, we should keep in mind that this proposal is based on the perceptions and statements of young women who were asked about the intentions of their partner. Notwithstanding, our results concur with Brodsky (2017), who analyzed the reports of men who had removed a condom without consent during sex and of women who had experienced this behavior. Further studies on nonconsensual condom removal are needed to corroborate this proposal.
In the committed relationships with violence, a wider variety of RC manifestations was identified. The participants shared stories of nonconsensual condom removal as well as pregnancy pressure and pregnancy coercion. In almost all these relationships, the male partner committed other forms of violence: physical, sexual, or psychological. This co-occurrence of different forms of violence suggests a coercive control dynamic on the part of the male partner, with RC being an additional form of control in the relationship. Moreover, the participants interpreted the RC in this sense. Some participants who had been in a relationship marked by violence experienced other forms of violence that were considered secondary to RC. In other words, these behaviors contributed to an atmosphere of contempt, belittlement, and threats.
All the participants reported significant consequences that affected their health and well-being. For instance, they were exposed to high risks of unwanted pregnancy or STIs, similar to the findings of previous studies (Brodsky, 2017; Holliday et al., 2018; Jones et al., 2016). Whereas Katz et al. (2017) showed that women who had experienced RC reported lower contraception use in their most recent sexual relationship, the results of the present study show instead that some women who experienced RC developed a highly cautious attitude toward condom use in their subsequent sexual relationships, and they appeared to be less trusting of new sexual partners.
The participants said that they felt very ashamed and guilty after incidents of RC. These feelings were associated with the relational context. Many felt that they had put themselves in “at-risk” situations by agreeing to have casual sex, or they felt that they could have been more assertive about condom use. Like many women who experience violence, they blamed themselves for what happened (Harned, 2005; Johnstone, 2016; Littleton et al., 2009). For example, Harned (2005) points out that some female sexual violence survivors assumed the blame because they believed that they had put themselves “at risk,” for instance, by flirting or by making advances to the aggressor, or else they had been under the influence of drugs or alcohol at the time. Other women blamed themselves for not being able to say “no” or to clearly state that they did not want to have sex (Harned, 2005). It is therefore essential to raise awareness among young women of their rights and the meaning of consent, as well as the perpetrator accountability. At the same time, men—and more broadly, society as a whole—need to be educated about all the situations that require obtaining the partner’s sexual consent. According to most of the participants who had experienced nonconsensual condom removal, their male partners were unaware (or heedless) of the seriousness of the situation and the negative impacts. These men prioritized their own sexual pleasure to the detriment of respecting their partner’s consent or using a condom, similar to the findings by Nikolajski et al. (2015). Clearly, both men and women need to be informed about matters of sexual consent, and their needs and preferences should carry equal weight. Furthermore, efforts should be initiated to raise awareness among women who experienced RC. In addition, education should be provided to perpetrators and the general public so that they can understand RC, a problem that remains largely overlooked and misunderstood.
Limitations
The results of this study should be considered in light of certain limitations. First, the small size of our sample precluded confirming all possible manifestations of RC, and our portrait is probably incomplete. However, we took care to construct a diversified sample within the limits of our inclusion criteria, in terms of sexual orientation, race, and the relational context (committed vs. uncommitted). Second, we compiled the data retrospectively, which can lead to memory bias. Given the exploratory nature of the study and the use of semi-directed interviews, it is plausible that some consequences were not reported. Instead of selecting the consequences of RC from a list, the participants shared the consequences that may have been the most significant or meaningful for them, regardless of the area in which they manifested. That said, the reported consequences were numerous and varied, as were the trajectories of the interviewed women.
Implications for Research and Practice
Despite these limitations, the findings have important implications. The results contribute to the literature on this form of violence. However, because our sample was not as diverse as it could have been, different populations should be investigated in future studies. In addition, qualitative methods could be used to more deeply explore the associations between IPV and RC, and in more diverse samples in terms of age, race, religious background, and social class. Moreover, studies on RC should systematically include the relational context to obtain a more informed analysis of how coercive control establishes itself. For example, future studies should investigate RC in diverse relational contexts, both committed and uncommitted, and in more diverse groups of women. Women who have had one or more children with their partner, women in a romantic but uncommitted relationship, and polyamorous women should be surveyed to identify the influence of various relational contexts on RC manifestations. Studies should also consider the partner’s pressure to use contraception or prevent pregnancy in ways that go beyond being involved in contraception or sharing the contraceptive burden. Because only one woman in our sample reported this situation, we were unable to obtain a thorough understanding of this form of RC. Although we have conceptualized the forms of the RC in terms of gender dynamics and from a feminist perspective that considers oppressive systems, we believe that cases reported by male victims are worth exploring, both in heterosexual and in LGBTQ+ (lesbian, gay, bisexual, transgender, queer) populations (Black et al., 2011).
The general lack of information on RC has significant implications for intervention strategies. On one hand, health professionals and counselors sometimes feel that they are poorly informed or equipped to assess, support, and help women who experience RC. As a result, the subject is seldom, if ever, broached during patient consultations (Burton & Carlyle, 2015; Zachor et al., 2018). On the other hand, many participants report being ashamed to reveal that they have experienced RC, which prevents them from getting the help they need. However, almost all of our participants were tested for STIs after RC in health clinics. This type of consultation provides opportunities for intervention. Knowing that women who experience IPV and those who visit health clinics are at higher risk for RC, health professionals and counselors need to be better informed and to have the necessary resources, including the intervention tools and training required to effectively identify potential RC situations (McCauley et al., 2017; Nikolajski et al., 2015; Park et al., 2016; Sutherland et al., 2015; Thaller & Messing, 2015; Zachor et al., 2018). This would better prepare health professionals to discuss RC issues with the women who use their services, and to provide more appropriate services.
Footnotes
Acknowledgements
We thank all the participants who generously and courageously shared their stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant awarded to the first author (S.L.) by the Fonds de recherche du Québec—Société et Culture (2017-P-200955).