
Abstract
This case study aims to determine the efficacy of a program based on drama therapy, theater of the oppressed, and psychodrama to reduce psychological malaise (post-traumatic stress disorder [PTSD], depression, anxiety) and sexist stereotypes, and improve self-esteem, quality of life, life purpose, and communication skills in women victims of intimate partner violence. A pretest and a posttest were administered to a single group using psychometric instruments; in addition, an evaluation of the process was done using participatory observation. Findings show a statistically significant reduction of depression and increase in life purpose. Qualitative analyses suggest development of personal and social competencies and the elaboration of trauma.
Keywords
Intimate partner violence (IPV) manifests as a continuum of behaviors and patterns aimed at acquiring control over one’s partner or the subservience of one’s partner in a relationship. It is the most common type of violence endured by women worldwide. In a situation comprising abuse, the violence can be physical, psychological, or sexual, or even the threat of suffering any of these types of violence (Durfee, 2018).
Both woman abuse and IPV occur in a social context dominated by structures that can have a differential effect on women, especially in patriarchal cultures or in the case of women suffering double discrimination because of their ethnic origins, nationality, or socioeconomic condition; discrimination is not always only predicated on gender, and exclusion conditions make it more difficult for certain women to end the situation of suffering in which they find themselves (Durfee, 2018; Segura, 2010).
The interpersonal dynamics in an abusive relationship have been explained by Walker (1980, as cited in Durfee, 2018) in a description of the cycle of violence, a theorization corroborated by other studies such as that of Osborne (2009). According to Walker’s explanation, the cycle starts with an initial phase of tension building, with the survivor adopting a submissive attitude to calm her partner, followed by an explosion or battering incident phase, and then a honeymoon phase in which the abuser makes promises, apologizes, and is affectionate and attentive toward the survivor; after that, the cycle starts again.
Authors such as Stark (2009, as cited in Durfee, 2018) propose that the cycle of violence explanation simplifies IPV, reducing it to the personal and interpersonal realm, thus strengthening myths and stereotypes. As an alternative, these authors focus on coercive control, presenting a more complex dynamic that is not limited to observable phases and behaviors. The abuser exerts significant coercive control over their partner, undermining the autonomy of the survivor and sometimes using subtle actions that are based on (shared) gender stereotypes that sustain the inequality and submission of the woman in the social context.
Following the same impulse, M. Johnson (2008) makes a distinction between four kinds of IPV and their associated dynamics. First, intimate terrorism occurs when one member of the relationship commits violent actions against the nonviolent partner. Second, violent resistance occurs as a result of the frustration felt from previous abuse. Third, Johnson describes situational couple violence as the response of one partner when dealing with frustration and the inability to resolve conflict. Finally, in the case of mutual violent control, each of the partners employs violence to obtain power and try to subjugate the other.
According to the World Health Organization (WHO), 30% of women worldwide suffer physical and/or sexual violence from their intimate partners. The lifetime prevalence varies by region: 23.2% in the high-income countries, and 24.6% in the WHO Western Pacific region, 37% in the WHO Eastern Mediterranean region, 37.7% in the WHO South-East Asia region, 36.6% in Africa, 25.4% in Europa and 29.8% in WHO Americas region (World Health Organization, 2013).
The results of a national macro survey in Spain (the country where the program evaluated in this study was implemented) show that 78.2% of women 16 years old or older living in the country have suffered some form of violence from their current or former partners. Of those victims, 78% mentioned that the consequences included harm to their physical and psychological well-being (Delegación Gobierno para la Violencia de Género, 2015).
Psychological Impact of IPV on Women
Most studies of IPV survivors mention a significant deterioration of physical health with self-perceived decreases in energy and vitality as well as increased psychological distress, demand for medical services, and morbidity and suicide risk (Boughima & Benyaich, 2012; Chen et al., 2009; Da Fonseca et al., 2011). Some studies point out depressive episodes and disorders in women abused by their partners as prevailing mental health concerns (Bowland et al., 2012; Crespo & Arinero, 2010; Ersoy & Yildiz, 2011), and other studies (Duros, 2009; Hebenstreit et al., 2015) report that post-traumatic stress disorder (PTSD) is a common ailment among victims of gender-based violence.
Depression and PTSD in women victims of gender violence usually go together with anxiety disorder and episodes of psychological distress, such as feelings of rage or guilt, somatic discomfort, sexual dysfunction, declining self-esteem, affective isolation, difficulty concentrating, addictions or substance abuse, eating disorders, feelings of hopelessness, and difficulties establishing relationships (Bermúdez et al., 2009; García, 2010). Another study conducted in Spain by Labrador et al. (2011) described significant levels of depression, PTSD, and low self-esteem.
Drama Therapy, Psychodrama, and Theater of the Oppressed
Drama therapy can be defined as “the intentional use of healing aspects of drama and theatre as the therapeutic process. It is a method of working and playing that uses action methods to facilitate creativity, imagination, learning, insight and growth” (Hollaway et al., 2011, p. 3). Currently, there are several approaches in the field of drama therapy, each with different theories and methods supporting them.
Among the studies that have offered empirical evidence about the use of drama therapy with women who have suffered from IPV, Campbell (2015) used pretest and posttest evaluations and a control group to suggest the effectiveness of drama therapy interventions in combination with other expressive arts therapies.
Psychodrama is a psychotherapeutic technique developed by Jacob Levy Moreno intended to promote spontaneity and resolve psychic conflicts. Group sessions in psychodrama begin with a warm-up activity that creates the atmosphere while choosing a theme and protagonist; then, at the action phase, participants enact the conflict and its aspects. At the final phase of sharing, the director leads the debriefing and ensures closure. There are multiple currents and schools of psychodrama, and it is considered one of the roots of drama therapy (García & Richard, 2009).
In a study about the transformations of traumatic events using art therapy, systemic psychotherapy, and psychodrama, Lai (2011) outlines the therapeutic possibilities of those techniques for domestic violence survivors and their daughters. Leeder and Wimmer (2007) have described similar healing benefits with incarcerated women in a treatment program using writing exercises and techniques from theatrical and drama therapy groups that assisted the participants in establishing new approaches for relating to themselves and others without the stigma of being incarcerated. To prevent gender-based violence in teenagers, Fong (2007) used drama therapy and psychodrama in a study with promising results. These techniques have also been shown to help participants overcome stigma and sexual stereotyping in studies by Moller (2013) with women and by Edell (2013) with teenage girls in situations of exclusion.
The theater of the oppressed is a constructivist pedagogical strategy developed by Augusto Boal. The process consists of improvisations about the life experiences of one or more participants who have suffered oppression. These participants direct others in their described roles and, during an improvisational portion, numerous variations are played out; finally, a forum discussion takes place to analyze the conflict of power and the possibilities for change (Boal, 2004).
In one recent study that employed strategies of the theater of the oppressed, Rich (2010) described his 10-year experience on a university campus in California. Using the theater of the oppressed, he focused, from a pedagogical perspective, on understanding gender-based violence and sexual violence in relation to the gender roles that perpetuate such violence. This intervention has also been applied in other university populations to prevent rape and sexual violence against women (Ahrens et al., 2011). In similar studies, Belknap et al. (2013), also by means of the theater of the oppressed, conducted a program with adolescents of different genders. A decrease in the acceptance of gender violence in dating was observed.
Considering the high worldwide incidence rate of domestic violence against women, the corresponding psychological malaise suffered by the victims, and the limited amount of research on interventions based on theater and drama therapy with women victims of IPV, we think it is imperative to keep cementing the empirical foundation on the effectiveness of these techniques.
For that purpose, we aimed to determine the effectiveness of a specific program that pursued the following objectives:
Reduce psychological malaise (PTSD, depression, anxiety).
Increase the indicators related to self-esteem, quality of life, intercommunication skills, social interaction, and life purpose.
Reduce the sexist stereotypes that sustain inequality and gender-based violence.
Method
Design
To evaluate the program, we followed the proposal found in Yates (2012), with the first step being the creation of an initial statistical description of the population to design a program meeting the needs of the participants. An evaluative study was designed with the interpretative goal of a group case study using a mixed procedure that was both qualitative and quantitative and employed a pretest–posttest design.
The program’s activities were subjected to a process evaluation during the intervention using an interpretative phenomenological analysis (IPA; Smith & Shinebourne, 2012). For that purpose, during the sessions, the participants were asked open-ended questions that encouraged them to reflect on the therapeutic experience, perform a participatory evaluation of the program’s activities, and verify the activities’ suitability to help the participants reach the objectives set forth. For this analysis, the comments by the participants were explored, and the participants were asked to connect the benefits and difficulties they attributed to the session to specific activities and situations.
Procedural assessment was also carried out to analyze the process to offer support or appropriate intervention by modifying the initial strategies if required (Pino-Juste, 2011). For this reason, an observation register was maintained, as was a recording of the final group discussion and evaluation of every session. In this way, the phenomenological analysis performed with the participants could afterward be compared with the observational register completed by the facilitator during the session and the break that took place prior to the end of the group discussion for each session; this procedure allowed for an evaluation of the activities and reorientation of the design of subsequent sessions as needed.
Participants
The participants were selected by nonprobability convenience sampling. The criteria for inclusion in the sample were being of legal age, currently suffering or having previously suffered from IPV, and accepting participation in the study by signing an informed consent form. The participants lived in the autonomous community of Galicia in Spain and attended two centers that offer help to women victims of domestic violence (Women’s Information Centers) located in two urban areas.
The initial sample included 25 participants, eight of whom left the treatment, reducing the final sample used to evaluate the program to 17. In the final sample (n = 17), the ages of the participants ranged from 21–52 years, with an average age of 49; most of the women (58.8%) had no job, and 64.7% had incomes below the national minimum wage. In addition, 58.8% did not have any kind of vocational training or had not even completed the basic formal education that is compulsory in Spain.
All of the participants in the sample were Spanish nationals and had children, with a maximum of four children per participant and a mode of two children. Regarding their relationship status, three were single, three were separated and had filed for divorce, six were divorced, and eight were married. Of the eight married women, five currently lived with abusive husbands.
Procedures
Initial assessment
An initial assessment was carried out to obtain information about the knowledge or content that the participants had incorporated before the intervention (Pino-Juste, 2011). For the initial evaluation, the following instruments were used:
– An ad hoc survey: socioeconomic information; type and duration of the violent situation.
– The Severity of PTSD Symptoms Scale, comprising three subscales (re-experiencing symptoms, avoidance symptoms and hyperarousal symptoms) and a total of 17 items based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria for the diagnosis of PTSD. The scale was designed and standardized for the Spanish population (Echeburúa et al., 1997). The reliability of the scale for the sample used in the present study was acceptable, with a Cronbach’s alpha of .899.
– The Quality of Life Survey Sf-12 v1, Spanish version by Alonso (1996). This test was composed of 12 items with different answer modalities on a Likert-type scale. The scoring incorporated three factors: physical health, mental health, and a global component of quality of life. The reliability of this scale in the sample was acceptable, with a Cronbach’s alpha of .792.
– The Ambivalent Sexism Inventory (ASI), Spanish adaptation by Expósito et al. (1998). The components measured by the scale are benevolent sexism (11 items), hostile sexism (11 items), and the sum of the two, understood as ambivalent sexism. This inventory yielded a Cronbach’s alpha of .847 in the study sample.
– The Purpose in Life Test (PIL), Spanish adaptation by Noblejas de la Flor (1999) based on the original by Crumbaugh and Maholick (1964). The PIL is a self-administered scale of 20 Likert-type items, with answers ranging from 1–7. The scale’s constructs are based on the basic principles of logotherapy by Victor Frankl. The test has four factors: perception of meaning, experience of meaning, goals and tasks, and a destiny-freedom dialectic. This test obtained an acceptable reliability for the study sample with a Cronbach’s alpha of .834.
– The Beck Depression Inventory II, Spanish adaptation (Sanz et al., 2003). This is an instrument used for the diagnosis of depression, comprising 21 self-reported items, with an interpretation of minimal depression when there are no or few diagnostic criteria met (0–13), mild depression when there are 14–19, moderate depression when there are 20–28, and severe depression when there are 29–63. The Cronbach’s alpha for the sample was .908.
– The Rosenberg Self-Esteem Scale, Spanish adaptation (Vázquez et al., 2004). This instrument consists of 10 items that assess feelings of self-respect and acceptance. For the study sample, this scale obtained a Cronbach’s alpha of .860.
Design of the program
Content and structure
The studied program was divided into 40 hr, distributed over 20 sessions of 2 hr each. Each session was divided into three phases corresponding to the psychodrama method: warming-up, action, and sharing (referred to below as group discussions).
The subjects the program dealt with were based on two transversal axes: a psychotherapeutic intervention axis to reduce psychological malaise and an axis from the perspective of critical pedagogy that aims to question sexist stereotypes and develop social and personal competences and skills. Thus, the content of the program was based on objectives focused on developing competences or reducing symptoms. The content was clustered in different stages of the program, which are described in Table 1.
Program’s Contents, Activities, and Number of Sessions.

Note. A more detailed description of the program can be found in Mondolfi (2017).
Method
The therapeutic axis was addressed from the role method drama therapy approach (Landy, 2009). The aim was for the activities to promote the training through roles (see Table 1) and thus expand the behavioral repertoire and spontaneity of the participants. Thus, this method was influenced by Landy’s theory as a frame for the procedural analysis.
In the same way, techniques from psychodrama were employed (Lemoine & Lemoine, 2009; Moreno, 1974; see Table 1); these techniques include the use of an empty chair for the projection of psychodramatic and psychosomatic roles and sociodrama.
The pedagogy axis incorporated the methodology of the theater of the oppressed (Boal, 2002, 2004). Many of the drama games and physical warm-up exercises detailed in Table 1 matched those proposed by Boal.
The body language exercises were performed with music and very few prompts to encourage the spontaneity of the participants. The breathing and voice warm-up exercises were usually employed in an actor’s training to learn the correct use of the voice (Stanislavski, 2010). For this program, such activities for the warm-up phase of the session were derived from several possibilities that both psychodrama and drama therapy offer.
Improvisation exercises are part of an actor’s training (Grotowski, 2002; Stanislavski, 2010); in the program, they were used in conjunction with the activities to reach training in roles and, later, were used to pursue a collective construction in which improvisations started with minimal guidelines and evolved into scenes with more complex dramatic content.
For relaxation activities, the technique of autogenic training (Linden, 2007; Schultz & Luthe, 1959) was used because, together with Jacobson’s progressive relaxation (Bernstein et al., 2000; Jacobson, 1987), such activities may improve de-rolling and foster competencies to deal with anxiety.
The group discussions at the sharing phase had a double purpose: They promoted the development of competencies of elaboration and interpretation building and simultaneously allowed the assessment of the activity’s effectiveness as part of the processual evaluation.
Implementation and assessment of the program
The program was guided by a female clinical psychologist with a postgraduate degree in theater and performing arts and was implemented in two government assistance centers for women victims of gender-based violence. The sessions were held weekly between October 2014 and July 2015.
Procedural assessment
The observation register was based on a 5-point Likert-type scale of the competencies and skills that were supposed to be developed throughout the program. The content evaluated in the observation register was as follows: anxiety, depression, meaning of life, social interaction and emotional bonding, communication skills (verbal and body language), awareness and insight, and self-esteem. The process of each participant was evaluated at the end of each session using the scales of the observation register completed by the person in charge of guiding the program.
The final discussions at the closure (sharing) stage of each session were recorded with voluntary informed consent from the participants. These discussions had an open format and were normally introduced by questions such as “How did you feel in today’s session? Have you learned something, and if so, what?” This content was used to analyze the therapeutic process and was categorized for further content analysis.
Final assessment
The final assessment made it possible to determine whether the objectives were achieved, as well as to analyze the learning outcomes and results of the entire process (Pino-Juste, 2011). The psychometric instruments administered in the initial assessment were applied again in the final assessment.
Data analysis
A descriptive analysis of the sample was performed using the averages and typical deviations gained from the pretests to obtain their initial level in the psychometric tests and compare the pretest and posttest results. A descriptive analysis of the group averages obtained in each session in the observation register was also performed.
To establish whether there were differences between two dependent groups, the Wilcoxon signed rank test was applied. A bilateral Z contrast with a .05 significance level was applied using the positive ranks to determine the significance of values that decreased between the pretest and the posttest and the negative ranks for those that increased. The quantitative data analysis was performed using SPSS (version 22).
The qualitative analysis of the closing discussions was performed using what authors such as Kvale (2011) call bricolage analysis; that is, we combined the terms used by the participants with our nomenclature and terminologies as researchers to generate the categories and subcategories used to codify the information and perform the interpretative analysis.
For the qualitative analysis, we followed the participatory evaluation approach. During the discussion with the participants, the participants’ evaluations were returned. To verify that the message they wanted to transmit had been properly understood, we shared the analytic categories (generated by the researchers after each session and by the facilitator during the discussion) with them, discussing the best way to classify the responses and verifying that the words used actually transmitted what the participants wanted to say.
In the case of the data from the observational register, the mean obtained from the group of participants in each session was calculated, and those data were analyzed as the group evolution during the program.
Results
The effectiveness of the program was first determined by analyzing the association of the data before the program (pretest) and the evaluation once ended (posttest). We verified a reduction in the averages of the psychological symptoms of depression and PTSD and in the stereotypes of ambivalent sexism, including both hostile sexism and benevolent sexism. An increase in the averages of favorable indicators, such as self-esteem, quality of life (physical and mental), and the global scale of life purpose, was also found in three of the factors.
Using the descriptive data in Table 2, we can surmise that the program has had favorable results. Furthermore, by analyzing the pretest–posttest differences with statistical significance, we see a marked improvement in the total of purpose in life (Z = −2.043; sig = .041) and in the factor perception of meaning (Z = −3.623; sig = .000), interpreted as improvements in the participants’ perception of reasons and motivations to live and value their own lives. There was also a statistically significant decrease in the factor experience of meaning (Z = −2.330; sig = .020), which refers to participants’ feelings that their personal existence was filled with positive aspects in everyday life.
Descriptive and Contrast Statistics Between Pretest and Posttest Based on Wilcoxon’s Signed Rank Test.

Note. PTSD = post-traumatic stress disorder; PIL = Purpose in Life Test.
Significant at the .05 level based on the positive ranks. bSignificant at the .05 level based on the negative ranks.
In addition, the changes in the case of depressive symptoms, which were reduced after the implementation of the program (Z = −2.393; sig = .017), were statistically significant. For context, it must be added that in terms of the diagnosis of depression, before the intervention, 64.7% of the participants were in a state of severe depression, and afterward, only 29.4% were in that state, while 23.5% suffered from moderate depression, 17.6% suffered from mild depression, and 29.9% did not meet the criteria for a diagnosis of depression.
The statistically significant changes in purpose in life and depression match the data obtained in the observation register during the sessions. Both variables show constant improvement in the registers, as shown in Figure 1.

Group averages of the observation register on anxiety, depression, purpose of life, and self-esteem.
Although they were not statistically significant, the PTSD indicators with the highest reduction were those of physiological activation. This matches the reduction in the group averages of the observation register for the category of anxiety (Figure 1) because the indicators that made it necessary to register this category during the sessions were mainly related to physiological activation (tendencies toward hypervigilance or difficulty in reducing the rhythm of breathing and eliminating muscular tension during the relaxation exercises).
The reason PTSD does not show a statistically significant reduction, we believe, is due to the continuous presence of violence from partners and ex-partners, which, as the participants explained, cannot be avoided because they have children in common or a restraining order cannot be enforced. As a result, harassment as a form of violence continued or there was a constant reminder of a traumatic event due to close contact with the aggressor. These facts are reflected in the testimony of some participants: Participant 16/Session 7: Sometimes I wonder if I should leave the girls with my parents and take myself out because I can no longer bear what the father of the girls does to me. However, I think I shouldn’t do it, because I worry about my daughters. Who would they stay with? My family is a bunch of miserable people, and the father is even worse. I have no support from my family, they are now on very good terms with the father of the girls, my father and brothers are in business with him, and the father of the girls is there . . . Participant 21/Session 7: I am sitting at a coffee shop and he goes by once, and they tell me it is just pure chance. However, he comes around again, staring at me, and I get nervous . . . I have a restraining order, but they keep telling me it is just a coincidence . . . he also goes to the children’s school.
In the second narrative, the participant references the fact that her former partner constantly violates the restraining order, running into her at the children’s school or seeing her in a public place, returning several times to the same spot instead of avoiding her. We chose this comment because it is representative of the most frequent complaint by the participants: the restraining orders were not observed, so seeing their abusers is a constant threat.
To specifically understand the content related to the variables that improved after the intervention, we also analyzed the frequencies of the categories in the analysis of the testimonies during the group discussions held after each session (see Table 3).
Categories and Subcategories of Content of Participatory Evaluation.

Note. F refers to the frequency of participants revealing each content. PTSD = post-traumatic stress disorder.
As seen in Table 3, relaxation is one of the activities with a higher positive valuation. The effectiveness described by the participants matches the improvement in anxiety symptoms found in the observation register (Figure 1).
In regard to the category of depression, the participants described their improvement process during the program, mainly mentioning the use of humor and an increase in physical energy, as described by one of the participants after finishing the sessions: Participant 12: I get home feeling very well. The other day I left, and after coming back, they told me: you are beaming (Session 3); You leave this place with more energy (Session 4).
Regarding the category of communication in Table 3, some of the comments of the participants mention their skills in verbal communication, their awareness of their difficulties in that aspect and their improvement during the process, as seen in the following testimonies: Participant 7/Session 4: I feel quite more at ease today, because we are so few; I feel more confident to speak, because I have troubles speaking in public. Participant 3/Session 19: Each day brings a new experience, each day we tell something new and I have lost my fear of the stage . . . I used to be fearful of speaking, and now I feel a little bit more emboldened; I speak more.
Regarding nonverbal communication and body expression, the participants describe their awareness of their difficulties. These difficulties were confirmed in the observation, because during the activities, the participants were reluctant to use their body to express themselves, requiring several guiding instructions and alternatives (such as changing the rhythm of the music, reducing the light, and working in pairs) to help them to participate. In their own words, the participants said the following: Participant 2/Session 10: Sometimes you want to, but you cannot do it. I like music, but I can’t, I go back home, and I wonder: Why can’t I? It must be because I am paying attention to what is in front of me and behind me. Participant 10: I think we need more physical contact (Session 2); It was good for me to interact with the others, just interacting with the body is hard for me, lowering the intensity of the light was helpful, taking into account the embarrassment of interacting only with the body (Session 5).
According to the observation register, self-esteem was improved within the group (Figure 1), and despite there being no statistical significance between the pretest and posttest, after the intervention, this variable increased in 11 (65%) of the participants. On a qualitative level, the participants attributed this improvement to the development of self-confidence and the reduction of embarrassment or a recovery of spontaneity, as illustrated by the following testimonies: Participant 4/Session 4: I find myself more open, I don’t care that much that others can see me. Participant 10/Session 5: At the beginning it was harder because of the fear of being seen, but now it’s starting to be easier.
During the processual evaluation, we also found, as qualitative content linked to an improvement in self-confidence, that the participants started having positive thoughts about themselves and creating purpose for their lives. That process can be illustrated with the following testimony: Participant 3/Session 16: It’s just not letting your thought limit you, you can, because you control the situation.
Talking was also helpful; catharsis is a therapeutic method for dealing with trauma, as seen in the following comments: Participant 3/Session 15: It’s good; it’s a way to escape, to talk. Participant 1/Session 8: It was quite relaxing because that is something I carry alone, by myself, without family or anything else. I have nobody to talk to, but it was helpful to tell somebody, just spill it out, like getting rid of a huge weight you carry. . . . It’s hard, because I am quite timid, very shy. It’s hard, but step by step, I still have time.
The second participant manifested diagnostic criteria for PTSD in the pretest and a remission of the disorder in the posttest, and her testimony references a scenic exercise that she correlated with her own life and personal experiences.
Positive valuations by the participants that also mention improvements in their ability to communicate and interact match the observations of the therapist and the group averages in Figure 2.
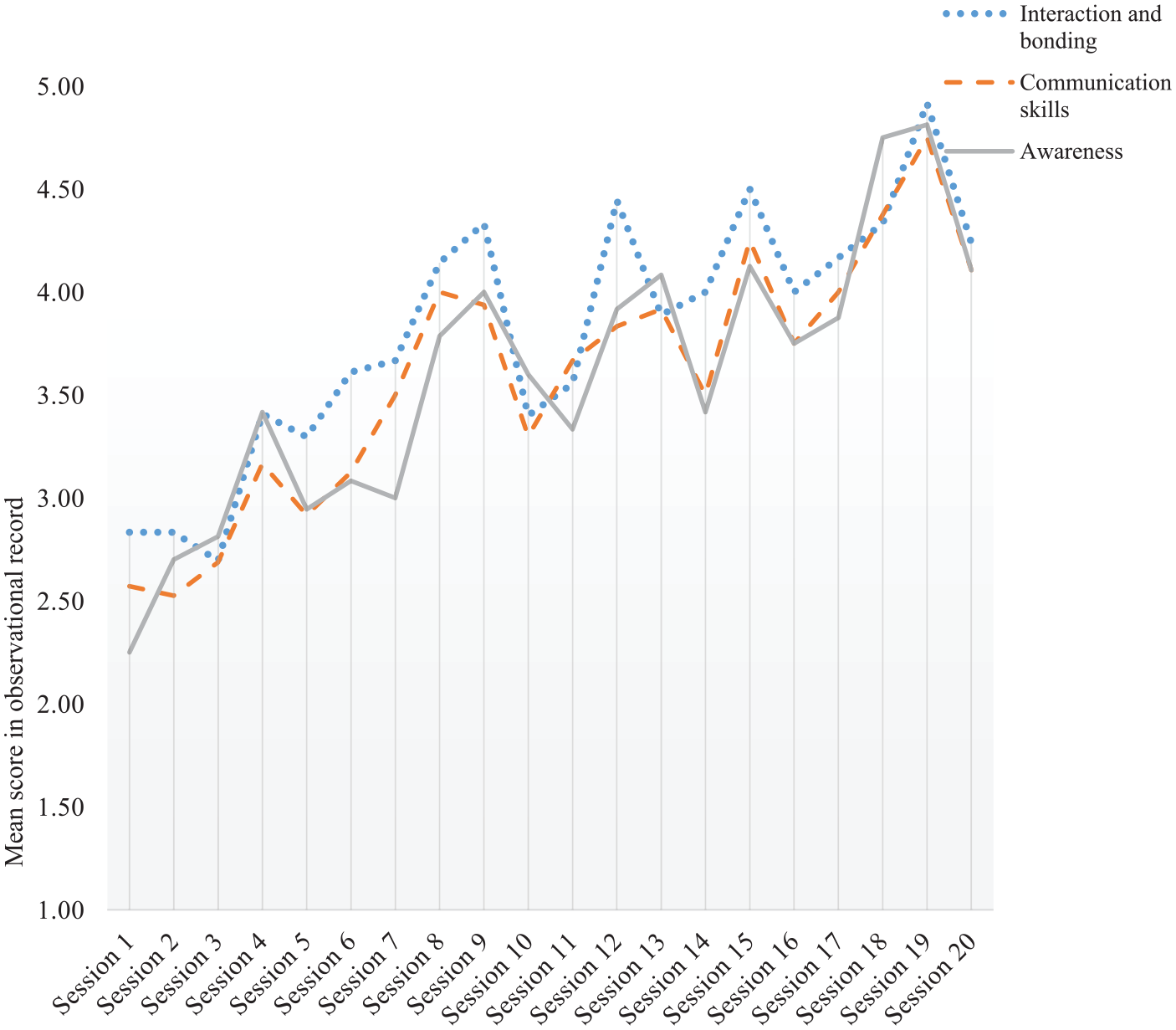
Group averages of the observation registers on interaction, communication skills, and awareness.
In the observation register in Figure 2 for the category of awareness, we find a progressive group increase over the 20 sessions. In that respect, in parallel to the development of communication skills and cathartic expression, a process of elaboration of trauma in relation to violence was carried out; that is, the therapeutic work was not limited to simply expressing and remembering the process of victimization. In that regard, some of the testimony of the participants in the closing discussions suggests an understanding of the cycle of violence and a decrease in symptoms of re-experience linked to trauma, as seen in this example: Participant 12/Session 8: When I come here, he tells me, why are you going if you are already well? I told him: I go like you go to the gym, while looking at him to see how he was going to react, because they have their cycles and I observe them, for when it comes the time to leave him, that’s it, but it’s not that moment yet. Starting here has been very helpful to me because I used to cry because I couldn’t forget. Now no more images come to my mind. I would be very sorry if I have to stop coming here.
In the previous quotation, Participant 12 referenced having constant flashbacks about situations of infidelity and abuse by her partner; in the discussion, the comments made the participants consider participation in the sessions as a form of self-care, making them feel stronger and reducing the episodes reliving traumatic memories connected with the abuse. The discussion also sparked comments about control by the abusers, which was, for some of them, a barrier for continuing attendance at the sessions.
In the same vein, other testimonies, such as the one quoted next, suggest an elaboration following more symbolic processes leading to the development of a stage we have categorized as awareness and purpose in life: Participant 3/Session 18: I made a comparison with daily things, with what each day can be like, the storm, moments of stress, moments of friction, a strike, something broken, something that can’t be glued back together, that sometimes the best option is a separation. . . . Suddenly we found something new: the wind like paragliding. Sometimes I felt like breaking in the middle. The adventure of life. I even danced a little bit with it, because we smiled a bit; we broke a little piece because there can be friction and then life goes on, everything goes back to its place and everything goes back to normal if that is what we want and that’s my story. I keep thinking about life, that we learn everything since we are children and that the emotional behavior can be learned, and you realize that these things teach those sensible details, that a thing and something else distract you in the same way and they help you solve aspects that the mind didn’t use. Now, you use them. Today I get so much out of the most trivial things. . . . The children first must be happy, that’s the lesson you have to learn in life.
The above testimony was given following a body-expression exercise. In the exercise, the participants danced in pairs, waving plastic painter’s sheathing following the rhythm of music and ambient sounds of nature. During the discussion, the participants metaphorically connected their movements and their situation in life. In the case of the woman above, the embodiment seems to have led her to a reflection on how to overcome difficulties and assimilate the learning from experience to promote spontaneity and a playful disposition. The same participant reflected on the process during the last session: Participant 3/Session 20: You came to me just at the right time, this fits like a glove, because you made me see many things and it was very helpful for making the decision I had to make and doing what I had to do, maybe a long time ago, but this was the time and you came to me just at the right moment.
In the above, she is referring to filing for divorce while participating in the program.
Finally, one of the initial requests of the participants during the therapeutic contract of the first session dealt with the socioaffective support. That expectation seems to have been totally met in the case of all participants in the program, as they verbally expressed this success during the sessions, mainly at the last one, during which they validated the categories of analysis in a participatory manner. Some testimonies of the progressive and complete fulfillment of this therapeutic request include: Participant 11/Session 2: If I let myself go, I spend the day crying, but I go out, I try to enjoy myself. This weekend I went out with them, the friends I have now; they are so cool (she refers to other participants). Participant 3/Session 12: After this I am going to miss you. Participant 1/Session 20: For me it should be more, more hours . . . see more solutions, see my friends with their problems and always a smile on their faces; we help each other. Participant 6/Session 20: I believe I have learned new things, I am very satisfactorily surprised. Things I didn’t know about, and I think it’s very helpful to know them, many of the group activities, and you learn to play a little with your feeling, but in a good way. . . . Besides, meeting you all, that was great, I am very happy.
In terms of the goals of the participatory research, the group mood of comradeship and fellowship was confirmed. Such an effect can be taken as a benefit of the group experience, especially in the case of people who are usually isolated from social contact by their abusers.
In other testimonies, the participants mentioned the benefits of experiencing therapy in a closed group that was homogeneous as victims of gender-based violence. The participants mentioned that aspect of the group as something that allowed them to be at ease to deal with that form of violence and made it easier for them to learn strategies for coping and understanding that others have had the same experience: Participant 3/Session 6: It’s very helpful, even if only for common sense, to spin it and see other perspectives. Participant 1: For self-esteem, I feel that the best is to talk, but not to tell somebody that didn’t live it, because they won’t believe you, but somebody that suffered the same, you go and tell her, and you perceive that person needs you, and at the same time she helps you and you help her, because she understands what you are saying (Session 9); For me, seeing these things is what makes me be again, and the group was very helpful (Session 19). Participant 8/Session 20: I think it’s great, because you create a space to talk, to discuss a bit what could be happening to us and each one of us adds her own experience with its own point of view, and thanks to that, you can search for alternatives and think of new situations that can solve that circumstance.
Discussion
The assessment of the program suggests its effectiveness in reducing depression and increasing life purpose, specifically oriented around the perception of meaning, motivations and reasons to live, and the value of the participants’ own lives.
The marked reduction in the experience of meaning may be due to the fact that reflecting on their lives during the therapeutic process led the participants to be aware that their daily experiences were not gratifying. The participants frequently mentioned unfavorable socioeconomic conditions as a cause of daily distress and an obstacle to recovering their independence. According to Graham-Bermann et al. (2011), socioeconomic deprivation is an aggravating factor in the recovery of victims of gender-based violence.
The participants also mentioned contact with the aggressor as a source of distress in their lives; in our program, this aspect seems to have been an obstacle for the remission of PTSD, as was the case in the study by D. Johnson et al. (2011) on cognitive-behavioral therapy with abused women.
In the initial statistical description of the population, before starting the program (Mondolfi & Pino-Juste, 2019), it was observed that in these cases, a longer relationship was associated with an increased level of violence, starting with the psychological violence, in time adding physical and sexual violence. The participants mentioned that increased violence as a means of submission was compounded by a lack of financial means to be the main cause preventing them from breaking off their violent relationships.
The abandonment of the program was also analyzed as part of the research project. Among the women who left the program, there was a significantly higher rate of more severe violence in the relationship, more acute symptoms of PTSD, higher levels of ambivalent sexism, and the presence of a history of mistreatment and child abuse (Mondolfi & Pino-Juste, 2018).
Therefore, following the constructs of the instrument used for the evaluation, we think that the difference between the perception of meaning and the experience of meaning can be understood as part of the therapeutic process in which the participants gain insight and become conscious of the situations causing distress in their lives, simultaneously perceiving compelling motives to change those situations.
The evolution of the program did not show a statistically significant change in the reduction of sexist stereotypes, but it yielded qualitative changes regarding understanding of the cycle of violence and the function of sexist stereotypes in gender inequality. This suggests the possibility that the participants become their own agents of change, starting from being conscious of their situation and understanding it after becoming audience members and interpreters of common problems through drama and theater as the means of symbolization.
Among the qualitative evidence, we can underline the importance of the group experience in recovering from psychological malaise and the elaboration of psychic trauma because the interaction with other women who have suffered similar experiences helped participants meet therapeutic demands or initial expectations of the need for social and affective support. This coincides with the results of Fong (2007) on group belonging, comradeship, and a sense of achievement as part of the benefits of drama therapy interventions on gender-based violence.
One of the challenges of working with this group, which required special work, was to promote the recovery of spontaneity and the use of one’s body as a communication channel and a symbolization and reaffirmation of self-confidence. For this, drama therapy and theater-based techniques were the right means because they favor embodiment and facilitate insight during the therapeutic process. Even so, the verbal final discussions showed the development of the awareness needed in the participants’ everyday lives and elaborations and competencies acquired, provided that the experiences of the session are used as a starting point.
As for the intervention strategies that promote the interdisciplinarity of drama therapy, the relaxation techniques during the sessions promoted improvement in symptoms of anxiety, as suggested by previous researcher (Echeburúa & Redondo, 2010; Michalopoulou et al., 2015) in interventions with this population. Following the recommendations of Jones (2015) about starting a dialog through drama therapy with other disciplines, our case used psychology and pedagogy.
Study Limitations
This study lacked a control group, so the influence of other variables external to the program that can affect the improvement or worsening of psychological malaise could not be measured. Although there was some attrition from the program, as is usual with this population, it is necessary to point out the irregular attendance of the participants in the final evaluation of the program.
These are limitations inherent to the social reality of the studied population, starting with the difficulty of finding a sample in small cities, where IPV victims avoid being singled out as such in front of the rest of the community and fear retaliation from their abusers. In addition, there are socioeconomic limitations that, in many cases, are an obstacle to attending the program.
Due to the reservations of the participants to engage in any situation that could potentially compromise their anonymity, the therapist-researcher had to do the observation register a posteriori, limiting the reliability of the data and preventing triangulation in the observation process.
Conclusions and Recommendations
The quantitative evaluation suggests that a program based on drama therapy and theater is beneficial in reducing depression and increasing life purpose. Regarding participatory research, the similarities between the observation register of the therapist and the evaluations of the participants suggest benefits for reducing anxiety and depression, increasing physical well-being and bonding, and developing communication competencies and symbolic construction.
The qualitative evidence allowed us to confirm and understand the statistical dimensions and generate an interdisciplinary dialog that offers empirical evidence of the effects of drama therapy and theater-based intervention on women victims of domestic violence in Spain, a country where these types of disciplines and interventions are not very well established or recognized.
Our recommendation is to continue researching these therapeutic and pedagogic strategies with victims of domestic violence because widening the studies to different contexts can offer invaluable data about cultural diversity and evidence-based considerations for professional practice and data obtained from case studies, where, whenever possible, all extraneous variables should be controlled. It is deemed essential that social services foster conditions that favor independence in this population and offer guarantees of personal and social safety that in turn facilitate adherence to the treatments, their freedom from violence, and their total recovery. This recommendation comes from the initial statistical description, finding that the longest-lasting relationships were correlated with more severe violence, this being in turn a factor associated with abandonment of the program, and acknowledgment by participants that their socioeconomic situation and insecurity were deterrents to leaving their current or former partners, as well as for the remission of the psychological malaise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.