
Abstract
In the domestic violence field, a survivor-centered approach to services is a shared ideal, but there is little empirical work demonstrating its importance. This study filled that gap, focusing on a key outcome—safety-related empowerment. We gathered data from 177 intimate partner violence (IPV) survivors seeking community-based services, and after one session with an advocate, results revealed a significant change in two of three subscales of the Measure of Victim Empowerment Related to Safety (MOVERS) measure: Internal Tools and Expectations of Support. There was no change in Trade-Offs (pursuing safety causing new problems). More survivor-defined practice predicted greater changes in empowerment, over and above severity of violence, post-traumatic stress disorder (PTSD), and demographics.
The domestic violence (DV) field has long advocated a survivor-centered approach to working with survivors; that is, one that aims to maximize choice and address each survivor’s unique needs, contexts, and coping strategies in the framework of a collaborative partnership (Davies & Lyon, 2014; Goodman, Thomas, et al., 2016). Despite wide consensus about its importance, few studies have explored to what extent a survivor-centered approach contributes to survivors’ well-being. The concept has served more as a unifying value than as a measurable approach likely to increase particular outcomes. At the same time, evaluation has increasingly become a priority for programs, in that they must prove the impact of their work to funders (Sullivan, 2011). Thus, a philosophical link between survivor-centered practice and survivor well-being is not enough to justify programs’ activities; the link between them must be demonstrated empirically.
This study aims to establish just such a link by exploring the relationship between client perceptions of the degree to which they have received survivor-centered support in a single session and a key outcome that should be its result: a change in survivor empowerment. Although a single session may seem too short to produce long-term outcomes, single-session interventions are common in the field as survivors are managing multiple crises and complex risks. As such, while they cannot be conceptualized as the solution, one-time interventions can be a pivotal service in a survivor’s trajectory toward increasing safety (Davies & Lyon, 2014). If theory about its importance is correct, more survivor-centered practice should lead to an increase in survivor empowerment, which can increase survivor safety over time. Before describing the study exploring that assumption, we review the nature of both survivor-centered practice and empowerment, and the scholarship supporting their potential importance.
Literature Review
The Nature and Challenge of Survivor-Centered Practice for Intimate Partner Violence (IPV) Survivors
Multiple scholars have written extensively about the need for a survivor-defined approach to working with survivors, using a variety of terminology (e.g., woman/client/victim/survivor-centered or defined, empowerment-oriented, holistic; Davies et al., 1998; Davies & Lyon, 2014; Goodman, Thomas, et al., 2016; Nichols, 2013). Recommendations for steering practice in that direction have key points in common, as Kulkarni and colleagues (2015) note: 1) increasing opportunities for survivors to exercise meaningful choices; 2) listening deeply and amplifying survivors’ voices; 3) engaging in collaborative partnerships which seek to minimize power differentials; 4) crafting individualized solutions that build on survivors’ strengths; 5) providing validation and support of survivors’ experiences; and 6) addressing systemic elements that limit survivors’ opportunities and access to resources and justice. (p. 911)
Although service providers are likely to subscribe to the philosophy behind the practice, because there are significant obstacles to employing it, there may be inconsistent implementation. For example, one study (Kulkarni et al., 2012) noted the difficulty of implementing a survivor-defined approach because of the emotional strain of the job combined with limited resources and systemic obstacles. Hearing the full picture of survivors’ circumstances means taking into account the many layers of context over which advocates may have limited control: the behavior of friends, family and community, the responses of public institutions, and dynamics of racism and economics (Velonis et al., 2015).
In addition to emotional strain advocates may feel, the structure of many interventions meant to assist survivors can make survivor-defined practice more difficult. Indeed, across the DV field, researchers have documented numerous ways in which funder and system requirements impact the survivor-centeredness of the intervention (Cattaneo et al., 2013; Fisher & Stylianou, 2016; Messing et al., 2015; Nichols, 2013; Wood et al., 2020). For example, when funding streams set requirements regarding the number of victims served or the types of services delivered, following these imperatives may get in the way of advocates’ efforts to center the individual risks and needs of each victim. In sum, while there is substantial agreement about the value of survivor-centered practices, there are obstacles to implementing them. There is indirect but compelling evidence that overcoming these obstacles may be key to effective service.
Evidence Supporting the Importance of Survivor-Defined Practices
Until recently, there was no measure of survivor-defined practice to allow for the exploration of the approach’s effectiveness directly. Instead, researchers have demonstrated the relationship between survivors’ sense of voice in and control over IPV interventions and survivors’ satisfaction with and likelihood of using those services in the future in contexts ranging from police interactions (Cattaneo, 2010) to civil protection order cases (Cattaneo et al., 2016), criminal processes (Hotaling & Buzawa, 2003), and victim services more broadly (Zweig & Burt, 2007). This sense of being heard and having control in the process of seeking help predicts not only survivor satisfaction with services in cross-sectional research, in which survivors report on their feelings retrospectively, but it also predicts outcomes of interest in longitudinal work. Perceiving voice and control has been linked to using services when needed in the year following the interaction (Hotaling & Buzawa, 2003), to experiencing repeat violence after the prosecution of a criminal case (Ford & Regoli, 1992), and to depression and quality of life 6 months after completing criminal and civil court cases (Cattaneo & Goodman, 2010). As noted, however, these studies focused on voice and control—closely linked correlates of survivor-defined practice. Only recently has a researcher–practitioner team developed and validated a specific measure of survivor-defined practice itself, the Survivor-Defined Practice Scale (Goodman, Thomas, et al., 2016). The current study uses this measure to explore the degree to which survivors’ perception of a single advocacy session as being survivor defined is related to the degree of change in their self-perception of empowerment over the course of the session.
The Link Between Survivor-Defined Practices and Empowerment
Much like survivor-defined practices, survivor empowerment has been a unifying value since the early days of the DV movement, but has been inconsistently defined and measured (Kasturirangan, 2008; Woodall et al., 2012). Recent work by the first author has generated a model of empowerment (Cattaneo & Chapman, 2010), and then applied it to the specific context of DV (Cattaneo & Goodman, 2015). The model specified empowerment as an iterative process, in which survivors move toward their own goals, gathering or strengthening necessary resources. Survivor-centered practice, as it is centered on understanding and supporting the survivor’s movement toward her goals, should support this process.
Building on this framework, in a collaborative project, researchers and practitioners articulated safety-related empowerment as an outcome that is consistent with DV programs’ missions and the needs and goals of survivors (Goodman et al., 2015). This construct includes three components: Internal Tools, or the sense that the survivor knows what his or her goals are related to safety and feels capable of pursuing them; Expectations of Support, or the perception that the necessary resources for pursuing the survivor’s goals are accessible and helpful; and Trade-Offs, or the degree to which pursuing safety causes other problems in the survivor’s life (Thomas et al., 2015). While this concept prioritizes safety as opposed to other goals survivors might have, it allows for an individual definition of safety, and measures the extent to which this priority conflicts with others. A study building on the Survivor-Defined Practice Measure just described found that higher ratings on survivor perceptions of survivor-defined practices were correlated with a stronger sense of Internal Tools and Expectations of Support, but not a lower degree of Trade-Offs (Goodman, Thomas, et al., 2016). While this study provided the first direct evidence of the link between survivor-defined practice and empowerment, it did so with a cross-sectional design, precluding exploration of a causal relationship. The design also allowed for a great deal of variability in the services survivors had received, which introduces the possibility of confounding variables. Additional work is needed to test the link between service-defined practice and empowerment, contributing essential information to the knowledge base of both practitioners and scholars interested in best practices for IPV survivors.
The Current Study
Research has laid groundwork for the importance of survivor-defined practices but has not directly explored its impact on survivors’ safety-related empowerment. The current study fills this gap with a pre–post design, testing whether survivor-defined practice is related to greater client satisfaction (Hypothesis 1); and whether survivor-defined practice is related to improvement in survivor safety-related empowerment over the course of a single session, controlling for demographics, severity of violence, and post-traumatic stress disorder (PTSD) symptoms (Hypothesis 2). On an exploratory basis, the study also explores whether the components of safety-related empowerment (Internal Tools, Expectations of Support, and Trade-Offs) change to different degrees and relate differently to survivors’ perspectives of survivor-centered practices.
It is important to note that this study measures an approach—survivor-defined practice—not a specified model. This is purposeful: IPV survivors require individually tailored responses that are based on their own individual goals, needs, and circumstances, such that a one-size-fits-all model for serving such a diverse group would be impossible. Therefore, most interventions for this population are not—indeed, cannot be—standardized (Goodman et al., 2018). Nonetheless, scholars and practitioners strongly urge uniform approaches to the work, irrespective of the particular context, setting, or survivor presentation (Cattaneo & Goodman, 2015). The survivor-defined approach is recognized by practitioners in the DV field as the gold standard, and this study sought to understand whether survivors’ perspectives on adherence to this general approach resulted in a change in safety-related empowerment across a diverse sample of clients attending a single advocacy session.
Method
Procedure
This study was a collaboration between university researchers and a large, urban victim assistance organization. The organization operates four community-based programs serving survivors of abuse and violence, providing traditional community-based individual and group supportive counseling, safety assessment and safety planning, advocacy, information, and referrals. We surveyed survivors of IPV at two time points: before and after completing the first session with an advocate at one of the community-based programs. As a randomized control trial was not feasible for this study, the study utilized a pre–post design. We expected that there would be natural variance in the survivor-defined quality of interactions, given the many factors that make this approach challenging to implement. The study complied with American Psychological Association (APA) ethical standards in the treatment of participants and collection and management of data.
Staff training in the survivor-defined approach
Staff at the community programs consist of the advocates who work directly with clients, supervising social workers, and directors. All staff who participated in the study had completed the organization’s required 48 hr of in-house training on survivor-centered practice. The organization’s training model is based around four components of survivor-defined practice: engagement, safety assessment, safety planning, and information and referrals. A typical first session lasts between 30 and 75 min, depending on the needs and preferences of the client, with an average length of 45 min. In general, the advocate starts the interaction by introducing themselves and reviewing the organization’s confidentiality provisions. Next, the advocate engages the survivor in the safety assessment process. As the survivor identifies risks and needs, the advocate engages the survivor in identifying potential safety options and provides information and referrals as needed. Within this general structure, training emphasizes flexibility for staff to adapt practice based on the survivors’ needs. For example, in safety assessment, staff are trained to assess immediate risks facing survivors across a range of physical, emotional, financial, and other domains, exploring which risks the survivor believes are highest priority. Once the survivors’ risks and priorities are identified, staff are trained to collaborate with survivors to create survivor-centered safety plans. These plans identify specific strategies and articulate detailed information about the community resources necessary for addressing survivors’ unique risks. In sum, the training supports staff in employing a flexible approach based on the complexity of survivors’ situations.
In addition to the required 48 hr training, advocates take a range of in-house trainings to support survivor-centered practice: increasing system knowledge, acknowledging and understanding trauma reactions, managing their own vicarious trauma, and learning how to utilize reflective supervision. All staff receive bi-weekly individual supervision, monthly group supervision, and ongoing observations of their practice to reinforce the knowledge and skills in survivor-defined practice techniques. The organization provides a fidelity checklist for the approach for supervisors to utilize when conducting observations of their staff’s practice with survivors.
Recruitment
Survivors of IPV seeking services from the organization’s community-based programs were recruited for the study. On the days the organization’s evaluation staff were available, the evaluators reviewed the community program intake calendar for new appointments. The intake appointments were screened by the evaluators to see if the survivor met the criteria for the study. The criteria for the study stated that the survivor: (a) must be 18 years of age or older, (b) must report experiences of violence and/or abuse from a partner, (c) must speak either English or Spanish, (d) must not have received services from the organization in the past 12 months, and (e) must not be calling to request a paperwork appointment only (e.g., needing paperwork for a housing transfer as the only service request).
If the survivor met the requirements for the study based on the intake, the evaluator would alert the community program advocate. If the advocate was able to reach the client via phone to confirm the community program appointment, the advocate would also inform the survivor of the evaluation project and assess their interest in participating. If the advocate was not able to reach the client via phone, then the evaluator went to the site prior to the appointment, approached the survivor in the waiting room, explained the project, and asked whether or not the survivor wanted to participate. Survivors interested in participating were provided a description of the study, their rights as potential participants, and the incentives available. If the survivor agreed to participate, the evaluator reviewed informed consent with them. The informed consent highlighted that (a) participation was voluntary and that survivors had no obligation to participate, (b) whether or not survivors chose to participate would not affect the services they were receiving from the organization, and (c) survivors could refuse to answer any items or stop participation at any time. Survivors were provided with a US$20 gift card for the baseline data collection survey and a US$20 gift card for the survey completed immediately following the session with the DV advocate. In addition to the pre and post surveys, participants also consented to have their session with the advocate recorded and coded by the evaluation team, but that information was not included in this study.
A total of 261 survivors were asked to participate in the study, 73% (n = 191) of whom agreed to participate. Of the 191 survivors who participated in the study, 14 were dropped from the data set: four participants were later determined to be ineligible as they were not survivors of IPV, three participants did not complete the pre-surveys, and one participant requested to be dropped from the study after completing the session with the advocate. Six participants did not complete the post-survey, two because of difficulties in understanding it, and four because of time constraints. The final database for this analysis consisted of 177 survivors of IPV. Sites served between 13% (21) and 39% (69) of the sample and had between five and seven staff members each. The number of participants seen by any one staff member ranged from 1-21, with an average of 8.47 study participants per staff. Surveys took approximately 10-20 min to complete. The sessions ranged from 15-92 min, with an average length of 43 min. Unless there was a reason to include a measure in the pre-survey (i.e., if we expected that the session might influence participant scores on a particular measure), we put all measures in the post-survey to minimize our intrusion into the site’s schedule and flow.
Measures
The survey instrument was available in both English and Spanish. To translate survey items not already available in Spanish, a Spanish-speaking research team member first conducted a “forward” translation—translating the tool into Spanish. The translator focused on a conceptual translation and utilized language natural and acceptable for the broadest audience possible. Next, two native Spanish-speaking individuals reviewed the Spanish survey instrument and identified any inadequate expressions/concepts. Finally, the initial translator and the two native Spanish-speaking translators worked as a team to resolve any identified issues.
Demographic and service utilization variables
In the post-survey, participants responded to demographic questions including age, gender, race/ethnicity, sexual orientation, language, education, country of birth, and whether they had children living in their home. Presession, for descriptive purposes, participants also described the extent of previous service usage related to IPV.
PTSD
The Primary Care PTSD Screen (PC-PTSD; Prins et al., 2016) includes four items. It is not designed to give a definitive diagnosis of PTSD, but to assess whether a clinical interview should be carried out to assess for PTSD. The screening items are traditionally answered yes/no; we added a Likert-type scale to capture greater variability, from 1 (not at all/only one time) to 4 (five or more times per week). The four screening items reflect the four factors of PTSD: reexperiencing, numbing, avoidance, and hyperarousal. The scale demonstrated an acceptable level of reliability in this sample with a Cronbach’s alpha of .77. We administered this scale presession, so that it would not be impacted by the conversation with staff.
Experiences of violence and abuse
The Hurt/Insult/Threaten/Scream (HITS; Sherin et al., 1998) screening tool is a short instrument for screening DV, initially designed for family physicians. The four-item screen asks respondents how often in the past year their current/former partner physically hurt, insulted, threatened with harm, and/or screamed at them. Responses range from 1 (never) to 5 (frequently). Each item is scored from 1-5 and scores are summed to create an inventory range from 4-20. A score greater than ten signifies that the clinician should follow up with the patient for further assessment (Sherin et al., 1998). The scale demonstrated a moderate level of reliability among this sample with a Cronbach’s alpha of .79. For descriptive purposes, we added two items to the scale to assess experiences of sexual coercion, asking how often a partner “forced you to engage in sexual activities” and “how often did you engage in sexual activities with this person because you were afraid of what would happen if you didn’t?” The response items ranged from 1 (never) to 5 (frequently). For our analyses, we used the traditional four-item version of the scale. We administered it post-session, so that the conversation with staff, which might stir up memory of incidents, could inform reports.
Satisfaction
Post-session, we assessed participants’ level of satisfaction with services with two individual items, scored separately. Both used a 1-4 Likert-type scale. The first item asked, “If you had a friend in your situation, how likely would you refer them to [name of organization]?” The second item asked, “Thinking overall about your conversation with the staff member, how supported did you feel?”
Survivor-defined practices
The Survivor-Defined Practice Scale (SDPS; Goodman, Thomas, et al., 2016) is a nine-item measure that assesses respondents’ perception of the degree to which their advocates help them achieve goals they set for themselves, facilitate a spirit of partnership, and show sensitivity to their individual needs and styles. Items ask participants to rate on a scale of 1-4 (strongly disagree to strongly agree) how much they felt staff (a) help me to shape goals that work for me; (b) support my decisions; (c) do not expect me to be perfect; (d) support me even whether or not I agreed with them; (e) make sure that services are right for what I need; (f) offer choices; (g) believe that decisions about my life are mine to make; (h) respect the way I deal with things whether or not they agree with it; and (i) to what extent they felt respected by staff in this program. In the development study, results showed that the SDPS measures a single factor, and it demonstrated strong reliability in that racially and ethnically diverse sample (α = .93). Reliability was strong in the sample in the current study as well (α = .88).
Safety-related empowerment
The Measure of Victim Empowerment Related to Safety (MOVERS) scale (Goodman et al., 2015) was developed to assess safety-related empowerment of survivors and was validated in a multi-site study. Its three subscales are (a) Internal Tools (e.g., “I know what my next steps are on the path to keeping safe”), (b) Trade-Offs (e.g., “I have to give up too much to keep safe”) and (c) Expectations of Support (e.g., “Community programs and services provide the support I need to keep safe”). Response options ranged from 1 (never true) to 5 (always true). The full MOVERS scale demonstrated adequate reliability in this sample (α = .73). Cronbach’s alpha for the subscales was .80 for Internal Tools, .68 for Trade-Offs, and .74 for Expectations of Support. We administered this scale before and after the session to measure change.
Data Analysis
Hypothesis 1 was evaluated with a bivariate correlation. To evaluate Hypothesis 2 and our exploratory questions, determining whether changes in MOVERS scores were significant, a change variable was calculated for the overall MOVERS construct as well as for the subscales (Internal Tools, Expectations, and Trade-Offs). These change scores were used as outcomes in a multi-level analysis in which scores were nested within staff members. These unconditional models provided variance components that could be used to calculate Intraclass Correlation Coefficients. This approach reflects the fact that staff members were providing the services, and thus some of the change in outcome scores may have been due to the characteristics of particular staff members.
Building on these unconditional models, predictors were added. Categorical control variables were measured with dummy codes for using the Spanish version of the study instruments, being male, identifying as Black/African American, and identifying as Hispanic/Latin@. Continuous control variables were the client’s age, the severity of abuse, and PTSD symptoms. The main predictor of interest was Survivor-Defined Practice. All continuous variables were grand mean-centered.
Results
Participants
As is detailed in Table 1, the majority (88.1%) of the participants were female and heterosexual/straight (95.5%) with an average age of 36.7 years. The sample consisted primarily of individuals of color with 40.1% identifying as Hispanic/Latina, 32.2% identifying as Black/African American, 14.1% identifying as Other, and 13.6% identifying as White/Caucasian. Just over half of the sample was born in the United States (62.7%) with 69.7% reporting English and 21.7% reporting Spanish as their primary language. Over three quarters (79.1%) had children with 77.9% of participants with children reporting one to two children living in the home. Only a quarter (25.4%) of participants had less than a high school degree, and almost half (41.8%) had some college/associate/trade school. While eligibility criteria required that participants had not sought services from this organization in the past year, nearly all (94%) participants had a history of seeking services for IPV, including crisis hotline (44.1%), individual counseling (36.2%), legal advocacy (28.2%), support groups (22%), emergency or short-term housing (16.9%), services for children (16.4%), and transitional or long-term housing (11%).
Demographic Information.
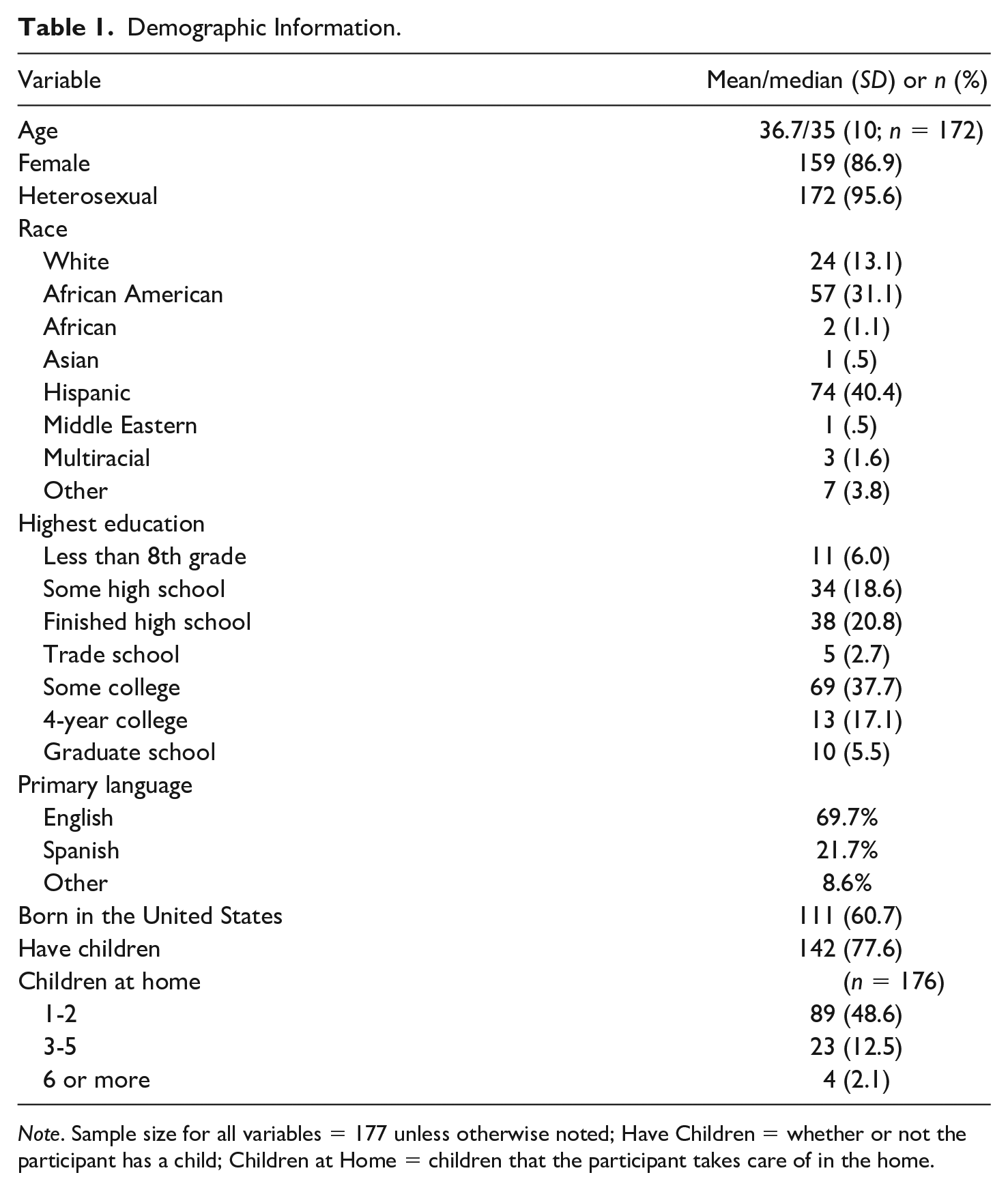
Note. Sample size for all variables = 177 unless otherwise noted; Have Children = whether or not the participant has a child; Children at Home = children that the participant takes care of in the home.
Descriptive Statistics
Descriptive statistics are presented in Table 1 and bivariate correlations for all variables are presented in Table 2. Based on traditional scoring of the HITS screening tool (see “Measures”), 91% of our sample would meet criteria for referral. As is typical of a sample seeking IPV services, the vast majority reported a history of physical abuse (81.5%). Almost all participants reported being insulted or talked down to (95.4%), or screamed and cursed at (96.6%), and most reported being threatened with harm (87%). About half of the sample reported having been forced to engage in sexual activities (53%), while about 57% reported experiences of sexual coercion. With regard to PTSD symptoms, the majority of participants (83%) would meet criteria for a referral based on the endorsement of three or more of the screening items. More specifically, at least once a week, 83% of participants reported nightmares and intrusive thoughts, 84% of the participants felt easily startled, and 82% reported feeling numb or detached.
Correlation Matrix.
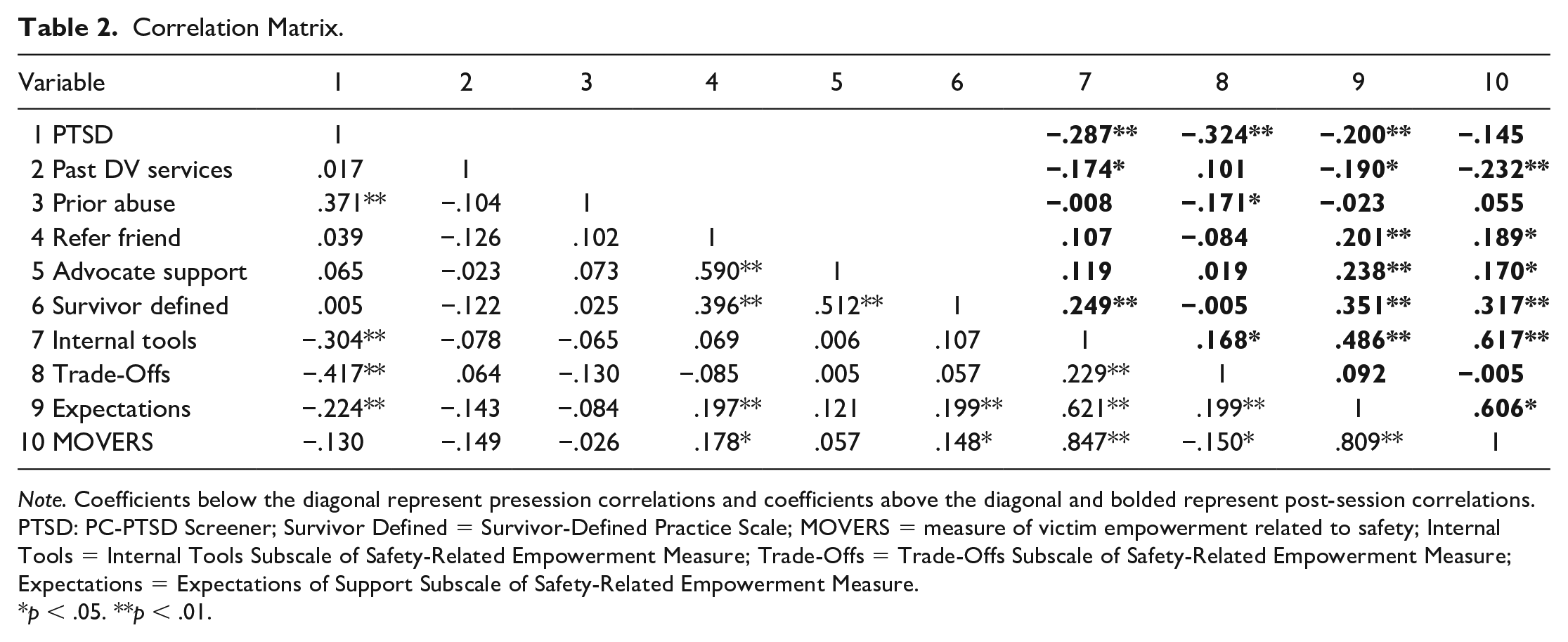
Note. Coefficients below the diagonal represent presession correlations and coefficients above the diagonal and bolded represent post-session correlations. PTSD: PC-PTSD Screener; Survivor Defined = Survivor-Defined Practice Scale; MOVERS = measure of victim empowerment related to safety; Internal Tools = Internal Tools Subscale of Safety-Related Empowerment Measure; Trade-Offs = Trade-Offs Subscale of Safety-Related Empowerment Measure; Expectations = Expectations of Support Subscale of Safety-Related Empowerment Measure.
p < .05. **p < .01.
On average participants reported that services were quite survivor-defined, with a mean of 3.53 out of 4 (SD = 0.45). This mean score is similar to the results of prior work with this measure (M = 3.47; Goodman et al., 2015). On average, participants rated their level of safety-related empowerment above the midpoint (M = 3.59; SD = 0.73; possible range = 1-5). Following one interaction with an advocate, the mean MOVERS score increased to 3.81 (SD = 0.71). On average, participants reported a high degree of satisfaction with services, with almost all (99%) survivors feeling supported or very supported (M = 3.71; SD = 0.50) and reporting they would be likely or very likely to recommend services to a friend (M = 3.76; SD = 0.50).
Bivariate Relationships
Relationships among study variables echoed prior literature, with PTSD symptoms related to prior abuse, and survivor-defined practice related to satisfaction. PTSD symptoms were related to both pre and post scores on safety-related empowerment: Those with more symptoms of PTSD reported a sense of lower Internal Tools for keeping safe, lower Expectations of Support, and more Trade-Offs associated with keeping safe. Similarly, those who had sought more help for IPV in the past reported a lower sense of Internal Tools and lower Expectations of Support, perhaps because they experienced less success through their prior efforts. Trade-Off scores did not have a significant relationship with the amount of services received in the past, suggesting that the sense of Trade-Offs might be less connected to the experience with providers.
Results of Hypothesis Tests
Relationship between survivor-defined practice and client satisfaction.
As hypothesized, participants’ reports of survivor-defined practice were positively correlated with both satisfaction items: The more the participant perceived the session to be survivor-defined, the more supported participants felt and the more likely they were to recommend services at this organization to a friend.
Change in safety-related empowerment
Because multiple participants were seen by each staff member, we investigated whether variance in safety-related empowerment was connected to the identity of the staff member working with the client. The MOVERS ICC (intraclass correlation) was .021, Internal Tools was .034, Expectations of Support was <.001, and Trade-Offs was .028. None of these ICCs were statistically significant, indicating that staffing differences did not account for a significant portion of the variance. It could be that the staff consistently offered survivor-defined services so that staffing differences in the treatment were minimized, or that the differential change that could occur due to the staff would need more time (and corresponding sessions) to accumulate. We nonetheless ran the models accounting for nesting, as that was the true structure of the data.
The ICC models include an intercept that represents the average amount of change for the four outcomes, providing a test of both hypothesis two and our exploratory question. The intercept for MOVERS was .155 (p = .001); for Internal Tools the intercept was .175 (p = .005); for Expectations of Support the intercept was .315 (p < .001). These indicate that the participants, on average, significantly improved in two of the three subscales. Trade-Offs did not evidence significant change, with an intercept of –.226 (p = .14).
Results of conditional models are presented in Tables 3 and 4. There was no clear pattern for the control variables except for the race/ethnicity variables. Participants who identified as Black/African American showed significantly less change for MOVERS total, Internal Tools, and Expectations of Support. Although participants who identified as Hispanic showed a similar pattern, their change scores were only significantly lower for Expectations of Support. We probed this pattern further and found that both groups had higher scores on the corresponding pretest scores but did not have lower posttest scores than participants of other races. This pattern of results suggests that participants who identified as Black or Hispanic changed less because they arrived at the session with higher scores, leaving less room for change.
Results of Hierarchical Linear Models Predicting Change in MOVERS Scores.
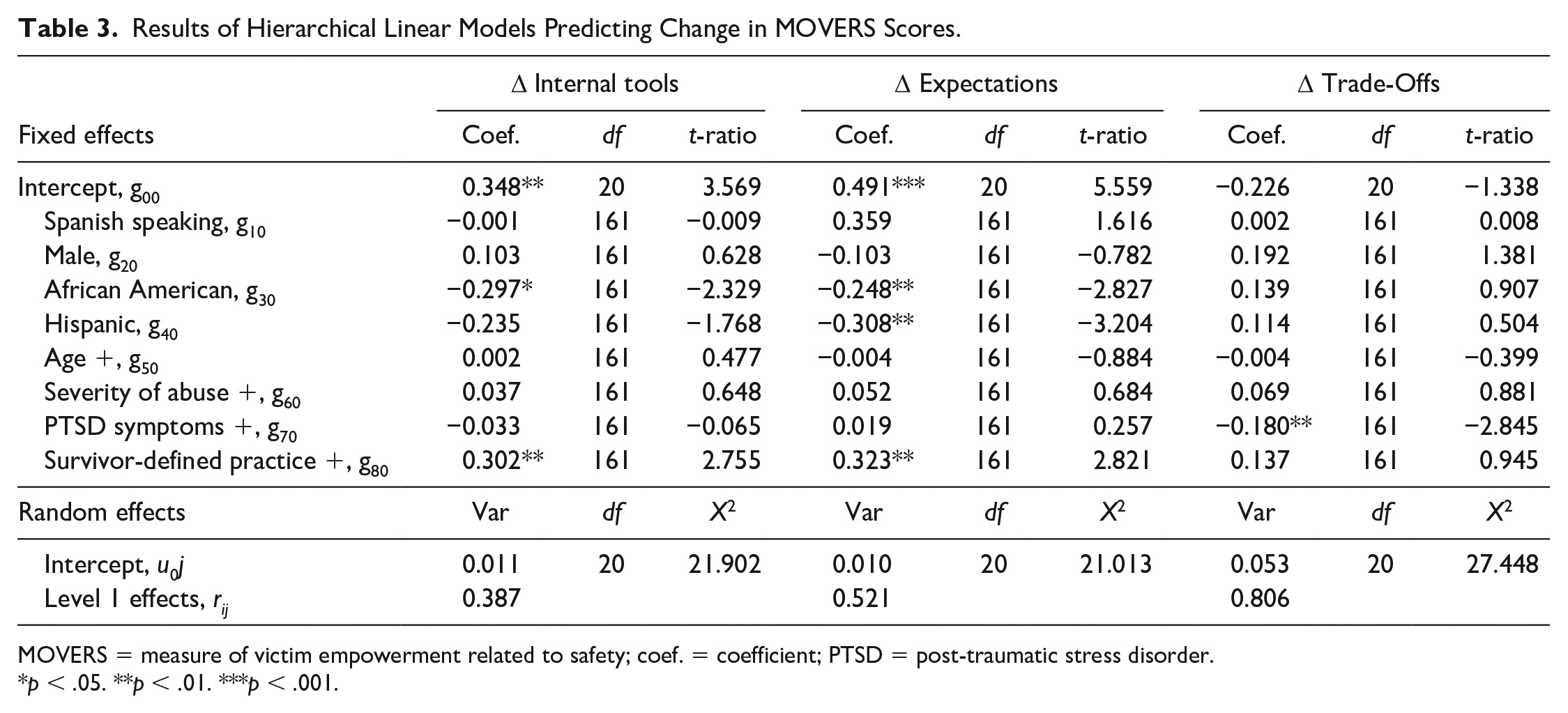
MOVERS = measure of victim empowerment related to safety; coef. = coefficient; PTSD = post-traumatic stress disorder.
p < .05. **p < .01. ***p < .001.
Results of Hierarchical Linear Models Predicting Change in MOVERS Scores.
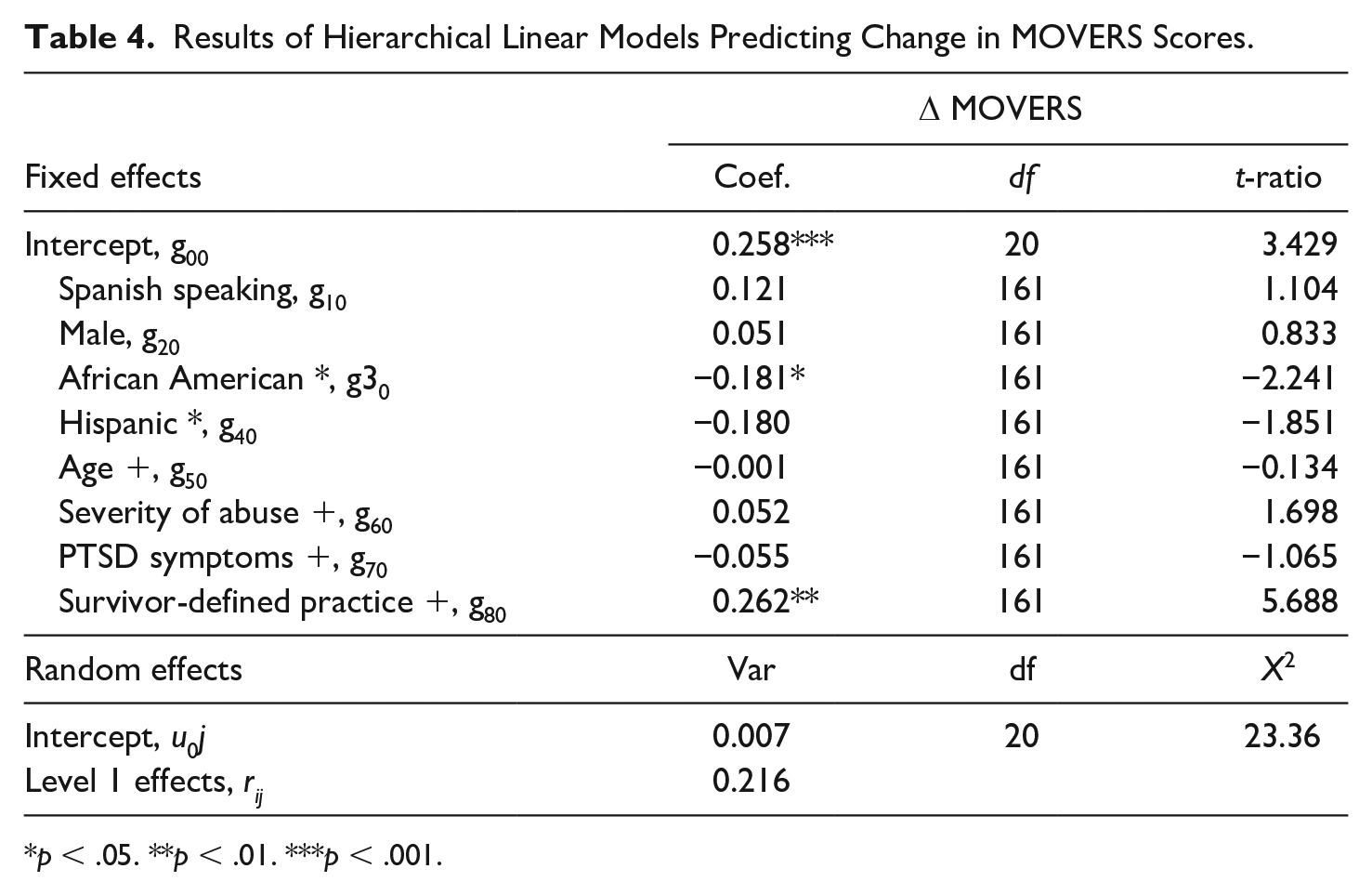
p < .05. **p < .01. ***p < .001.
The predictor of interest for this study was survivor-defined practice. Results indicated that survivor-defined practice was a significant predictor for MOVERS total change (b = .26), Internal Tools (b = .30), and Expectations of Support (b = .32). Survivor-defined practice was not a significant predictor of change in Trade-Offs (b = .14).
Discussion
While the field has theoretically supported survivor-defined practices as a critical approach in increasing survivor empowerment, only one study to date has empirically demonstrated the relationship between the two, and that study was cross-sectional (Goodman, Thomas, et al., 2016). This study supports and expands those findings. The results of this study provide evidence for the effectiveness of survivor-defined practices in increasing safety-related empowerment among survivors of IPV after one session from a community-based program.
Specifically, findings from this study indicated that on average, survivors increased their level of safety-related empowerment following the session. Similar to the cross-sectional study, this study found that these results were driven by change in two out of the three subscales: Internal Tools and Expectations of Support. Survivors did not significantly change their scores on the Trade-Offs subscale. Indeed, less than half (44%) of study participants had an improved Trade-Offs score following the session. The limited change in Trade-Offs is not surprising given the nature of the construct and the length of the intervention. Internal Tools are psychological; it is reasonable to believe that a helpful session might indeed shift a survivor’s sense of his or her own ability to move toward goals and confidence in doing so. The Expectations of Support subscale is directly related to the experience with providers of support, and thus might also be influenced in a single positive session. In contrast, Trade-Offs often involve forces beyond the control of both the advocate and the survivor. They include fears about financial security, threats to the safety and well-being of children and other loved ones, and the loss of housing and community (Thomas et al., 2015). These threats to well-being can be caused by systems and policies in addition to the actions of the abusive partner. Thus, it is not surprising that a single session might have less of an impact on Trade-Offs than the other two aspects of safety-related empowerment.
It is worth noting that while on average participants significantly increased their sense of safety-related empowerment as a whole and within two subscales, there was considerable variance among survivors. While 61% of the sample improved their safety-related empowerment following one session, 39% of the sample did not. Results also revealed a difference in these changes related to race. In particular, participants who identified as Black/African American indicated significantly less improvement in safety-related empowerment than did participants who identified as White. Upon further examination, results showed that participants who identified as Black/African American or Hispanic reported higher levels of safety-related empowerment on the baseline assessment than their White counterparts. With respect to the Black/African American participants, this finding is consistent with previous research that has found that female African American IPV survivors report significantly higher rates of empowerment than female White IPV survivors, even when there are no significant differences between IPV experiences (Peterson et al., 2002; Wright et al., 2010). As noted by Wright and colleagues (2010), the “Strong Black Woman” stereotype may impact African American women’s sense of empowerment either because empowerment serves as a protective factor among African American women or because the stereotype serves as a silencing factor among African American women. This finding was not as strong among women in our sample who identified as Hispanic, but the similar pattern suggests a need for further exploration. In the development study for the safety-related empowerment measure, which used a similarly diverse sample, there was no difference in scores by race. Future explorations of survivor-defined practices and empowerment should take racial and ethnic differences into account, to understand these conflicting findings.
Because the variance attributable to advocates was nonsignificant, it suggests that the approach is not sensitive to systematic differences among advocates; that is, it was the level of survivor-defined practice in a given session, rather than the identity of the staff member, that predicted change in empowerment. Future research might evaluate this (nonsignificant) finding further. As this study did not collect any specific information on the advocates—such as age, gender, education level, or years of experience—further research is needed to examine whether these variables are significantly associated with outcomes of interest.
Overall, while there was variance in the amount of change across participants, results showed that survivor-defined practices predicted increased safety-related empowerment. This finding held true for the full measure of safety-related empowerment and the Internal Tools and Expectations of Support subscales, even when controlling for demographic factors, severity of abuse, and post-traumatic stress symptoms. This is the first study examining the impact of survivor-defined practices on safety-related empowerment of IPV survivors using a pre–post design, and it provides empirical evidence of the theoretical connection between these constructs.
Limitations
Several limitations constrain the generalizability and interpretability of the study findings. First, the sample demographics present limitations in regard to external validity. The sample consisted of majority women of color receiving DV services in one city in the Northeast, which limits our understanding across other identities of survivors and across different geographic regions. Furthermore, nearly all (94%) participants had a history of seeking services for IPV from agencies other than the one collaborating in this study, thereby limiting our understanding of the results among truly first-time service seeking survivors. Finally, the majority (88.1%) of participants were female and heterosexual/straight (95.5%). The extent to which these findings are consistent for men or transgender survivors or among gay, lesbian, bisexual, or queer survivors needs to be explored.
With regard to the study methods, several limitations should be noted. The first methodological concern includes potential response bias. While participants were explicitly informed that results would not affect their participation in services or services received, survivors completed the survey on-site, and they were provided gift cards as an incentive; both of which could have led them to respond more positively to questions about services. The second methodological concern includes the short length of time between data-collection points. The post-survey was conducted immediately after the client’s first session. Notably, there was significant change even after that one session. However, it is possible that change might fluctuate after some time for reflection. This study could not evaluate that possibility, nor could it assess change after multiple sessions, in which a genuine relationship might develop between client and staff. Indeed, survivor-defined practice would ideally take place over many meetings, if the survivor wished it. Further research is needed to examine the relationship between survivor-defined practices and safety-related empowerment across a longer time period to allow for the entirety of the intervention and to determine how safety-related empowerment increases and/or decreases over a longer time period.
Implications for Research, Clinical Practice, and Policy
The results of this study support the idea that survivor-defined practice is best practice. Building on these findings, several questions for future research stand in sharp relief. First, the level of safety-related empowerment at the end of a single session is a proximal outcome. Research is needed to explore the connection between this proximal outcome and distal outcomes such as physical and emotional well-being, safety, stability, and long-term satisfaction with the role help-seeking played in survivors’ lives. Cross-sectional scholarship has found that safety-related empowerment fully mediated the link between therapeutic alliance and both PTSD and depression (Goodman, Fauci, et al., 2016). Thus there is some beginning evidence that this proximal outcome may lead to broader aspects of well-being; this possibility needs to be tested over time. Second, the survivor’s perception of the session is an important perspective, but certainly not the only perspective that might be weighed. Staff perceptions are also important to evaluate in understanding the nature and impact of services, as are the specific staff behaviors that might yield more positive survivor experiences, or the ways in which survivor behaviors contribute to the interaction. Further research is needed to examine the impact of survivor-defined practices from these additional perspectives. Third, scholarship has identified challenges and obstacles inherent in survivor-defined work (Kulkarni et al., 2012; Velonis et al., 2015); this study provides evidence that those challenges are important to address. Research might identify and test strategies to that end, to inform ongoing efforts to refine and support practice.
With regard to practice, this study offers DV organizations, such as the one involved in this project, evidence that devoting resources toward survivor-defined practice makes good sense. Results suggest that advocates’ ability to implement this approach is a key skill set that facilitates survivor empowerment. Those skills include the ability to demonstrate respect, support, and choice, and to work collaboratively with survivors in shaping goals, identifying needed services, and making safety-related decisions. Both training and ongoing feedback and support from supervisors are necessary to build and maintain those skills, and such efforts require resources. In short, DV organizations can utilize these findings to support the need to invest resources into training, supervision, and practice to increase staff’s capacity to utilize a survivor-defined approach to their work.
As noted earlier, in this study, Black/African American and Hispanic survivors reported higher levels of safety-related empowerment prior to the first session and therefore there was less room for growth on this outcome. Researchers can enhance the field’s understanding of survivor-defined practices by further exploring them from the viewpoint of survivors, across a range of intersecting survivor identities and contexts. Practitioners can seek to adapt survivor-defined techniques across racial and ethnic communities, along with other diverse populations. The field must continue to commit to leveraging our expertise, resources, and practice skills to better understand the needs of survivors from marginalized groups.
A final implication of these findings relates to the lack of change in Trade-Offs. The lack of change in this aspect of empowerment, consistent with prior research (e.g., Goodman, Thomas, et al., 2016), supports the idea that even a survivor-defined approach may not address the range of Trade-Offs survivors face when they seek help—e.g., the potential loss of financial security, housing, and community support. Trade-Offs likely cannot be addressed solely in individual work with survivors, but require advocacy, coalition building, and policy change. These efforts should build on the expertise of practitioners who, in working with many survivors over time, often have clear ideas about the Trade-Offs survivors most often face.
Conclusion
This study provides empirical evidence for an approach that is already understood by many practitioners and scholars to be best practice for facilitating survivors’ trajectory toward healing and safety, and also suggests its possible limits in addressing the myriad Trade-Offs that survivors face in seeking help. In our experience, a central challenge to working toward more survivor-centered approaches is its extraordinarily nuanced and time- and resource-intensive nature. It is our hope that this study bolsters DV organizations’ ongoing efforts to embrace these challenges as well as funders’ commitment to supporting them.
Footnotes
Acknowledgements
We would like to thank Liz Roberts, Dr. Lisa O’Connor, Juanito Vargas, Elizabeth Ebright, and the entire Community Program team at Safe Horizon for their dedication to and support of this project.
Authors’ Note
Amanda M. Stylianou is now affiliated with Rutgers University Behavioral Healthcare.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.