
Abstract
The current study (a) ascertained whether there is a relationship between sexual victimization (SV) and disordered eating (DE) among bisexual women, (b) assessed whether objectification theory explains the relationship, and (c) tested for group differences between bisexual and heterosexual women on SV, DE, and other objectification theory variables. Utilizing a sample of 164 undergraduate bisexual women, there was a significant positive relationship between SV and DE that was serially mediated by self-surveillance and body shame. In addition, bisexual participants endorsed more SV, DE, body shame, and interoceptive deficits than a comparison sample of 335 undergraduate heterosexual women. Implications are discussed.
According to the National Intimate Partner and Sexual Violence survey, bisexual women (75%) experience lifetime sexual victimization (SV) at higher rates than both heterosexual women (43%) and lesbian women (46%; Walters et al., 2013). In addition to increased risk for experiencing SV, results from recent studies suggest that bisexual women may also experience worse postassault outcomes (e.g., hazardous drinking, smoking, post-traumatic stress disorder [PTSD], depression) than women of other sexual orientations (e.g., Blosnich & Horn, 2011; Hequembourg et al., 2013; Hughes et al., 2010; Long et al., 2007). However, disordered eating (DE) has historically been understudied as a potential postassault outcome among bisexual women. The current paper presents theoretical and empirical rationales for understanding the association between SV and DE, as well as bisexual women’s disparate risk for DE, and presents results that address this gap in the literature.
Sexual Victimization and Disordered Eating
There is a growing body of literature that has established SV as a nonspecific risk factor for DE. The association between SV and DE has been demonstrated in a variety of contexts, including student (e.g., Capitaine et al., 2011; Dubosc et al., 2012; Holmes & Johnson, 2017; Williams & Gleaves, 2003), clinical (e.g., Racine & Wildes, 2015), community (e.g., Preti et al., 2006; Wonderlich et al., 2001), and nationally representative samples (e.g., Armour et al., 2016; Dansky et al., 1997). In addition, while most studies have been cross-sectional, several longitudinal studies have also demonstrated DE to be a postassault outcome (e.g., Johnson et al., 2002; Sanci et al., 2008). Despite the heterogeneity of this research, no study, to our knowledge, has explicitly assessed the relationship between SV and DE in a sample of bisexual women. It would be important to do so given bisexual women’s aforementioned disproportionately high rates of SV (Walters et al., 2013) as well as their greater endorsement of DE relative to their heterosexual and lesbian counterparts (Koh & Ross, 2006; Polimeni et al., 2009; Shearer et al., 2015). Consequently, research is needed to assess the possible relationship between SV and DE in bisexual women and, if such a relationship exists, ascertain its mechanisms.
Objectification Theory and Disordered Eating
One framework that may be pertinent to understanding the relationship between SV and DE in bisexual women is objectification theory, which was conceived in an effort to better understand the disproportionate rates at which women experience negative mental health outcomes, including DE (Fredrickson & Roberts, 1997). It posits that women are often treated as a body instead of a person and that the internalization of these sexually objectifying messages (often measured via self-surveillance; for example, Carr & Szymanski, 2011; Kozee & Tylka, 2006; Tylka & Hill, 2004) is associated with DE indirectly via several psychological consequences (i.e., body shame, appearance anxiety, safety anxiety, interoceptive deficits or reductions in internal bodily and emotional awareness, reduced flow; Fredrickson & Roberts, 1997). Overall, this model has been reliably substantiated as a means for understanding DE (e.g., Myers & Crowther, 2008; Noll & Fredrickson, 1998; Tiggemann & Slater, 2001; Tiggemann & Williams, 2012; Tylka & Hill, 2004) with body shame, followed by interoceptive deficits, garnering the most support as relevant mechanisms (Kozee & Tylka, 2006).
With regard to body shame, Fredrickson and Roberts (1997) posited that when women’s bodies are objectified and when these messages are internalized, women are more likely to assess the appearance, rather than the function of their body. When they inevitably compare it with the unattainable cultural body ideal propagated throughout Western culture, they are likely to experience shame that arises from believing their own body to be inferior. This body shame may then motivate them to engage in behaviors (e.g., restricting caloric intake, self-induced vomiting, excessive exercise, laxative misuse) aimed at narrowing the discrepancy between the cultural body ideal and their own body. To date, a number of studies have found support for this theorized relationship (e.g., Augustus-Horvath & Tylka, 2009; Holmes & Johnson, 2017; Kozee & Tylka, 2006; Noll & Fredrickson, 1998; Tiggemann & Slater, 2001; Tiggemann & Williams, 2012; Tylka & Hill, 2004).
With regard to interoceptive deficits, objectification theory (Fredrickson & Roberts, 1997) posits that when women internalize sexually objectifying messages, they may place so much of their attention and energy into their physical appearance that they lack resources to sufficiently attend to their internal experiences. Diminished awareness of some internal experiences (e.g., hunger/satiety, emotions) may result, in turn, in DE such as eating for emotional reasons rather than hunger, continuing to eat when full, and failing to eat when hungry. Studies that have supported the role of interoceptive deficits in DE have measured the construct in a manner that includes both emotional awareness and hunger and satiety cues (e.g., Holmes & Johnson, 2017; Myers & Crowther, 2008; Tylka & Hill, 2004). By comparison, studies that measured interoceptive deficits as a wide range of physical sensations, not specific to hunger and satiety (e.g., heartbeat, throat dryness), without assessing emotional awareness (e.g., Tiggemann & Slater, 2001) or studies that measured the construct as only emotional awareness (e.g., Muehlenkamp & Saris-Baglama, 2002) did not support a relationship between interoceptive deficits and DE. Consequently, it can be concluded that within the context of objectification theory, interoceptive deficits should be operationalized as internal awareness, inclusive of both awareness of emotions and hunger/satiety.
In addition, there are multiple studies (e.g., Holmes & Johnson, 2017; Tylka & Hill, 2004) that found support for the role of interoceptive deficits, but not in the manner specified by Fredrickson and Roberts (1997). More specifically, these studies did not find an indirect relationship between sexual objectification and DE via self-surveillance and interoceptive deficits. Rather, they found that that the indirect relationship occurred through self-surveillance, body shame, and then interoceptive deficits. Authors consequently speculated that, perhaps, interoceptive deficits were not the result of diminished resources to attend to internal states but rather the product of a woman distancing herself from her body in reaction to the shame she felt toward it (Holmes & Johnson, 2017).
Objectification theory is a well-established framework for understanding the relationship between sexual objectification and DE. It may also prove useful in elucidating the relationship between SV and DE, in women broadly and bisexual women in particular. However, much of the existing objectification theory literature does not answer these questions due to two limitations: (a) lack of focus on extreme forms of sexual objectification (i.e., SV) and (b) underrepresentation of bisexual women in samples utilized thus far.
Application of Objectification Theory to Sexual Victimization
When objectification theory was first conceived, Fredrickson and Roberts (1997) stated that sexual objectification could occur in everyday ways (e.g., leering, unwanted sexual comments) as well as in extreme forms (e.g., SV). However, few studies to date have explicitly examined SV, or extreme objectification. Several studies have employed the Interpersonal Sexual Objectification Scale (ISOS; Kozee et al., 2007) that predominantly measures everyday objectification. Although there are a couple of items that assess what could be considered extreme objectification, these items are not examined separately but rather are included in the full scale, which precludes authors from making any interpretations regarding SV specifically (e.g., Augustus-Horvath & Tylka, 2009; Kozee & Tylka, 2006). Other studies (e.g., Tylka & Hill, 2004) have utilized measures that do not include items that assess extreme objectification at all (e.g., Perceived Sociocultural Pressures Scale; Stice et al., 1996) and a great deal more do not assess sexual objectification of either form but rather start their models with self-objectification (e.g., Myers & Crowther, 2008; Tiggemann & Slater, 2001; Tiggemann & Williams, 2012). Notably, however, there is evidence from literature outside of objectification theory that implicates objectification theory variables (i.e., body shame, or related constructs such as body image) in the relationship between SV and DE (e.g., Connors, 2001; Preti et al., 2006; Tripp & Petrie, 2001), thus further bolstering the application of objectification theory to SV.
There are three studies, to our knowledge, that have explicitly examined SV within the context of objectification theory. The first two established significant positive relationships among SV, self-surveillance (as a proxy for self-objectification), and body shame (Carr & Szymanski, 2011; Davidson & Gervais, 2015); however, neither study examined interoceptive deficits or investigated DE as an outcome variable. The third, conducted by the current authors, largely supported the application of objectification theory to the relationship between SV and DE (Holmes & Johnson, 2017). Specifically, the role of body shame was consistent with that posited by objectification theory (Fredrickson & Roberts, 1997). With regard to interoceptive deficits, the results demonstrated an indirect relationship between SV and DE via self-surveillance, body shame, and interoceptive deficits, and through interoceptive deficits alone (Holmes & Johnson, 2017). Consequently, we discussed the possibility that in addition to the mechanisms relevant to everyday objectification (i.e., body shame may result in DE in an effort to more closely approximate the thin ideal and may cause women to distance themselves from their bodies, resulting in interoceptive deficits that put them at risk of DE), there may be trauma-specific mechanisms related to SV as well. For example, trauma survivors often feel disconnected from their own bodies and emotions (i.e., interoceptive deficits), which may occur because “attending to their current physiological state can evoke trauma-related reminders and subsequent distress and is thus avoided” (Cross et al., 2017, p. 116). When conceptualizing interoceptive deficits in this manner, it logically follows that it may arise after trauma exposure regardless of the extent to which the survivor internalizes sexually objectifying messages. Consequently, this particular indirect relationship, through interoceptive deficits alone, may not be relevant to everyday objectification, but rather specific to extreme objectification (i.e., SV) as it may be a trauma-specific response.
Objectification Theory and Bisexual Women
Most studies that test objectification theory utilize predominantly heterosexual samples (e.g., Carr & Szymanski, 2011; Holmes & Johnson, 2017) or do not report participants’ sexual orientation at all (e.g., Davidson & Gervais, 2015; Myers & Crowther, 2008; Noll & Fredrickson, 1998; Tiggemann & Slater, 2001; Tiggemann & Williams, 2012; Tylka & Hill, 2004). In fact, there are only a handful of studies, to our knowledge (Brewster et al., 2014; Engeln-Maddox et al., 2011; Kozee & Tylka, 2006; Watson et al., 2015) that have tested objectification theory in samples of sexual minority women. Generally, they found support for the indirect relationship between self-surveillance and DE via body shame. Results were mixed, however, with regard to whether there is a significant positive relationship between sexual objectification and self-surveillance (Kozee & Tylka, 2006; Watson et al., 2015) or not (Brewster et al., 2014; Engeln-Maddox et al., 2011). Of note, only one study (i.e., Kozee & Tylka, 2006) has assessed the role of interoceptive deficits in sexual minority women, finding in the final model that interoceptive deficits were not significantly associated with self-surveillance or DE. It is important to note, however, that of these four studies, only one examined bisexual women directly (Brewster et al., 2014) while two sampled only lesbian women (i.e., Engeln-Maddox et al., 2011; Kozee & Tylka, 2006), and one combined lesbian and bisexual women into a single group for the purpose of analyses (i.e., Watson et al., 2015). The latter reflects the field’s historical tendency to subsume bisexual women into other sexual minority groups, which has been a barrier for understanding bisexual women’s unique experiences of SV and its consequences (Hequembourg et al., 2013). Consequently, authors have put out “a call for more in-depth research into the unique vulnerabilities suffered by bisexual women” (Johnson & Grove, 2017, p. 436). As previously stated, there is only one study, to our knowledge, that addresses this by employing a sample comprised exclusively of bisexual women (i.e., Brewster et al., 2014). Although it demonstrates significant strengths, including a large sample size and inclusion of culturally relevant constructs (i.e., anti-bisexual discrimination, internalized biphobia), it did not assess the role of interoceptive deficits nor did it explicitly examine SV.
Applying objectification theory to the relationship between SV and DE in bisexual women is an imperative next step for this growing body of literature. The intersection of marginalized identities (i.e., woman, bisexual) may help explain this population’s increased risk for postassault outcomes such as DE. For example, some researchers have discussed the impact of hypersexualization of bisexual women, in which a woman’s bisexual identity becomes a vehicle through which she is dehumanized and denied agency, diminished to a trope in the straight male sexual fantasy repertoire and, consequently, ensconced in the straight male psyche as a constantly willing sexual plaything. (Johnson & Grove, 2017, p. 439)
This unique phenomenon, in combination with the sexual objectification to which all women are subjected, creates a cultural environment in which bisexual women are potentially multiply marginalized, necessitating the assessment of objectification theory in this population.
Current Study
In the previous study conducted by the authors (Holmes & Johnson, 2017) on SV, DE, and objectification theory, sexual minority women, the majority of whom were bisexual, reported significantly higher rates of DE than their heterosexual counterparts, requiring sexual orientation to be statistically controlled for in the primary analyses. This caused us to wonder about the application of the model to sexual minority women, and bisexual women in particular, as well as potential group differences on objectification theory constructs between bisexual and heterosexual women; however, the sample size precluded such analyses. The current study, therefore, sought to answer these questions and respond to the call for researchers to focus on the unique vulnerabilities of bisexual women (Johnson & Grove, 2017) by (a) identifying the relative rates of SV, DE, and other objectification theory variables in heterosexual and bisexual women; (b) assessing the potential relationship between SV and DE in this population; and (c) by testing possible explanatory mechanisms. A sample of undergraduate women was utilized, given their high rates of both SV and DE (Tripp & Petrie, 2001).
Specifically, we hypothesized that bisexual women would score higher than their heterosexual counterparts on SV (Hypothesis 1a [H1a]) and DE (Hypothesis 1b [H1b]), as has been found in previous research (e.g., Shearer et al., 2015; Walters et al., 2013). In addition, we predicted that bisexual women would score higher on variables related to objectification theory: self-surveillance (Hypothesis 1c [H1c]), body shame (Hypothesis 1d [H1d]), interoceptive deficits (Hypothesis 1e [H1e]), given the potential for hypersexualization because of their intersecting marginalized identities. We also hypothesized that there would be a significant positive association between SV and DE, as has been found in other studies with other populations (Hypothesis 2 [H2]; Armour et al., 2016; Dansky et al., 1997; Racine & Wildes, 2015). In addition, we hypothesized (see Figure 1) that the positive association would be accounted for by four indirect effects: (a) through self-surveillance and body shame, serially (Hypothesis 3 [H3]; Path A); (b) through self-surveillance and interoceptive deficits, serially (Hypothesis 4 [H4]; Path B), both of which were theorized by objectification theory (Fredrickson & Roberts, 1997); and (c) through self-surveillance, body shame, and interoceptive deficits, serially (Hypothesis 5 [H5]; Path C) as was found in several previous studies including the only other to apply objectification theory to the relationship between SV and DE (e.g., Holmes & Johnson, 2017; Tylka & Hill, 2004), and through interoceptive deficits alone (Hypothesis 6 [H6]; Path D) which is consistent with the conceptualization of interoceptive deficits as a form of posttraumatic avoidance (Cross et al., 2017) as well as the results of the previous study by the current authors (Holmes & Johnson, 2017).
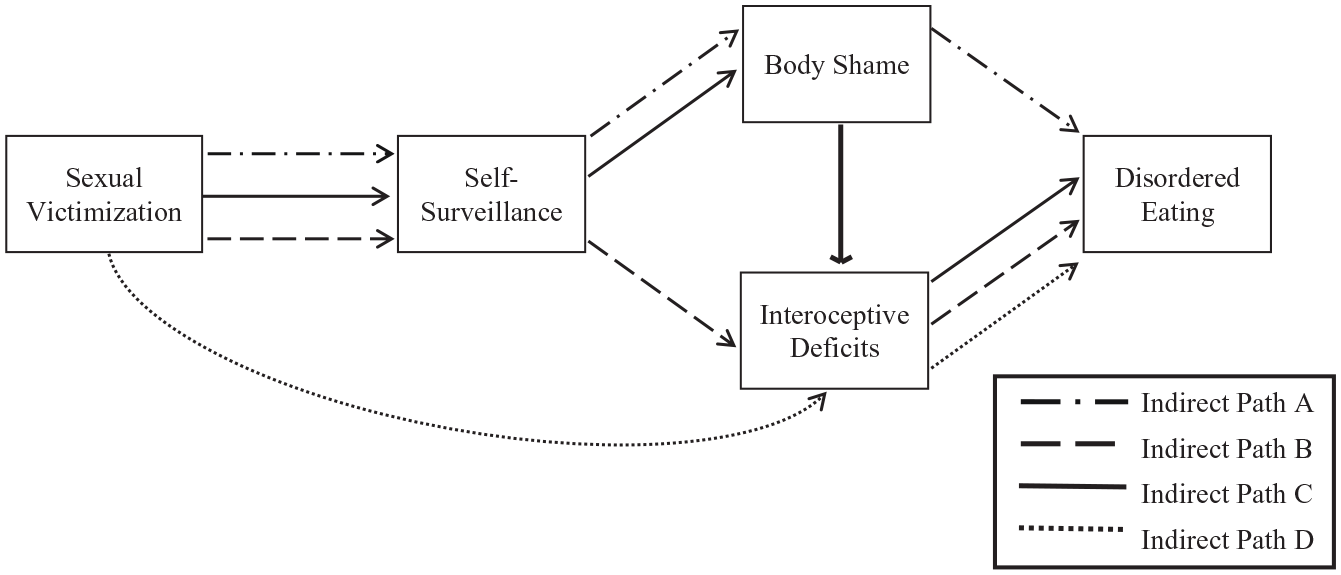
Hypothesized indirect paths between sexual victimization and disordered eating.
We also sought to assess the other potential indirect effects on an exploratory basis: (a) through self-surveillance alone, (b) through body shame alone, and (c) through body shame and interoceptive deficits serially. This decision is consistent with Hayes’s (2013) recommendation for testing parallel models of multiple mediation.
Method
Participants
The current study utilized two samples. The primary sample (N = 164) comprised undergraduate bisexual cis-gender women, ranging from 18–43 years (M = 21.34, SD = 3.55). Using the Kinsey scale ranging from 1–7, anyone who identified as a 7 (exclusively gay/lesbian) or 1 (exclusively heterosexual) was excluded from the sample, while those who identified their sexual orientation between 2 and 6 (2 = mostly attracted to the opposite sex but attracted to the same sex as well [45.1%, n = 74], 3 = some preference for the opposite sex but attracted to the same sex as well [17.1%, n = 28], 4 = equally attracted to both sexes [18.3%, n = 30], 5 = some preference for same sex but attracted to the opposite sex as well [10.4%, n = 17], 6 = mostly attracted to the same sex but attracted to the opposite sex as well [9.1%, n = 15]) are represented as bisexual for the current study. This operationalization is not uncommon. For example, the only other study to examine objectification theory in bisexual women similarly included women who identified as “mostly heterosexual” and “mostly gay/lesbian” (Brewster et al., 2014). In addition, it is “consistent with the conceptualization of bisexuality as a spectrum of nonexclusive sexual orientation and acknowledges that bisexual individuals may not experience equal attraction to both genders” (Brewster et al., 2014, p. 53).
The majority of the sample identified as White (73.2%, n = 120), followed by Multiracial (10.4%, n = 17), Black or African American (9.8%, n = 16), Latina or Hispanic (3.0%, n = 5), and Asian or Pacific Islander (2.4%, n = 4). Furthermore, 20.7% (n = 34) of participants reported current household incomes of less than US$10,000, 27.5% (n = 45) from US$10,000–US$29,000, 12.8% (n = 21) from US$30,000–US$49,999, 11.0% (n = 18) from US$50,000–US$74,999, 16.4% (n = 27) from US$75,000–US$150,000, 6.1% (n = 10) of greater than US$150,000, and 5.5% (n = 9) did not report their household income.
The current study also employed a comparison sample that comprised the cis-gender heterosexual subset (N = 335) of the sample from the authors’ previous study (Holmes & Johnson, 2017). These participants ranged in age from 18–60 years (M = 20.99, SD = 4.98). The majority of the comparison sample also identified as White (74.6%, n = 250), followed by Black or African American (11.9%, n = 40), Asian or Pacific Islander (4.5%, n = 15), Multiracial (2.4%, n = 8), Latina or Hispanic (2.4%, n = 8), Arab (2.1%, n = 7), other (1.5%, n = 5), and Indigenous or Aboriginal (.3%, n = 1) (one participant chose not to provide this information). Furthermore, 15.7% (n = 53) of participants reported current household incomes of less than US$10,000, 16.4% (n = 55) from US$10,000–US$29,000, 12.0% (n = 40) from US$30,000–US$49,999, 11.0% (n = 37) from US$50,000–US$74,999, 19.7% (n = 66) from US$75,000–US$150,000, 5.4% (n = 18) of greater than US$150,000, and 19.7% (n = 66) did not report their household income.
Measures
Extreme sexual objectification via SV
The Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2007) is the field’s gold standard in assessing SV. The seven primary items describe different types of unwanted sexual experiences (e.g., “A man put his penis into my butt, or someone inserted fingers or objects without my consent”), and participants respond by indicating the number of times they were victimized (0, 1, 2, 3+) as well as how the situation occurred (e.g., “showing displeasure, criticizing my sexuality or attractiveness, getting angry but not using physical force, after I said I didn’t want to,” “using force, for example, holding me down with their body weight, pinning my arms, or having a weapon”). The current study assessed SV across the lifetime and was scored dichotomously (0 = no SV history, 1 = SV history), such that any endorsement corresponded with having an SV history and negative responses to all items corresponded with no SV history. This scoring method allowed us to retain a greater number of participants than the severity-ranking score and has been used in previous studies utilizing the SES-SFV (Anderson et al., 2016; Holmes & Johnson, 2017).
Self-objectification via self-surveillance
The Self-Surveillance subscale of the Objectified Body Consciousness Scale (OBCS; McKinley & Hyde, 1996) measures the degree to which women monitor their bodies as an outside observer. It consists of eight items to which participants respond on a 7-point Likert-type scale ranging from 1 (strongly disagree)–7 (strongly agree). Sample items that are reverse scored include “I am more concerned with what my body can do than how it looks” and “I rarely compare how I look with how other people look.” The Self-Surveillance subscale of the OBCS has demonstrated adequate internal consistency reliability and test–retest reliability (McKinley & Hyde, 1996). Convergent validity has been documented with measures of public self-consciousness and appearance orientation (McKinley & Hyde, 1996), body esteem (McKinley & Hyde, 1996; Moradi & Varnes, 2017), and internalization of sociocultural attitudes toward appearance (Dakanalis et al., 2017; Moradi & Varnes, 2017). In addition, Smolak et al. (2014) established discriminant validity with a measure of enjoyment of sexualization. Cronbach’s alpha in the current sample was .86.
Body shame
The Body Shame subscale of the OBCS (McKinley & Hyde, 1996) assesses the degree to which women feel badly about themselves when they believe they have failed to meet culturally defined beauty standards. It comprised eight items to which participants respond on a 7-point Likert-type scale ranging from 1 (strongly disagree)–7 (strongly agree). Example items include “When I can’t control my weight, I feel like something must be wrong with me” and “I would be ashamed for people to know what I really weigh.” This measure has exhibited adequate internal consistency reliability and test–retest reliability. Convergent validity has been demonstrated with measures of body esteem (McKinley & Hyde, 1996; Moradi & Varnes, 2017), body dissatisfaction (Dakanalis et al., 2017), and internalization of sociocultural attitudes toward appearance (Dakanalis et al., 2017; Moradi & Varnes, 2017). Discriminant validity has been established between the Body Shame subscale and the Control Beliefs subscale (i.e., belief that effortful control can be wielded over body shape and size) of the OBCS (Dakanalis et al., 2017; McKinley & Hyde, 1996). In the current sample, Cronbach’s alpha was .88.
Interoceptive deficits
The Interoceptive Deficits subscale of the Eating Disorder Inventory–3 (EDI-3; Garner, 2004) assesses the extent to which participants have difficulties with internal awareness, including awareness of emotions (e.g., difficulty with emotional identification, confusion about internal states, feeling out of control) as well as hunger/satiety. The subscale consists of nine items to which participants respond on a 6-point scale, ranging from 1 (never)–6 (always). The Interoceptive Deficits subscale has demonstrated excellent internal consistency, test–retest reliability, and validity (Garner, 2004). Convergent validity between the Interoceptive Deficits subscale and emotion dysregulation as well as personal alienation (i.e., lack of self-awareness) has been established (Garner, 2004). Discriminant validity has been demonstrated by showing differentiation with divergent diagnoses such as anxiety and other phobias (Garner, 2004). Cronbach’s alpha was .93 in the current sample.
Disordered eating
The Eating Attitudes Test–26 (EAT-26; Garner et al., 1982) measures level of DE reported by participants. While the EAT-26 was intended to measure DE on a continuous scale rather than assessing the presence or absence of a clinical eating disorder, it has been validated on both clinical and nonclinical samples of women (Tylka & Hill, 2004). The measure comprised 26 items to which participants indicate how often they engaged in each behavior on a 6-point scale ranging from 1 (never)–6 (always). Sample items include “[I] am preoccupied with the thought of having fat on my body” and “[I] feel extremely guilty after eating.” The EAT-26 has shown good internal consistency, reliability, and test–retest reliability (Mazzeo, 1999). Convergent validity has been established with a measure of eating disorder risk (Garner, 2004) and a measure of bulimic behaviors (Kelly et al., 2012). Discriminant validity has been demonstrated by establishing divergence with measures of symptoms of depression and anxiety (Garner et al., 1982). In the current sample, Cronbach’s alpha was .89.
Procedures
With regard to the primary sample of bisexual women, 50 participants were recruited from a mid-sized public university in Ohio as part of the previous study by the current authors (Holmes & Johnson, 2017). All participants followed a link to Qualtrics, a secure online data collection tool, wherein informed consent was garnered prior to the participants completing the aforementioned surveys and demographic questionnaire. Participants received extra credit for psychology courses, when applicable. As previously mentioned, in this initial study, sexual orientation was significantly associated with the outcome variable (DE), and thus, it was controlled for statistically; however, there was not adequate power to analyze sexual minority women separately. Consequently, we continued participant recruitment specifically for undergraduate sexual minority women, which yielded an additional 114 bisexual participants, resulting in the final sample of 164. The comparison sample used in the current study consists of the 335 heterosexual women from the same prior study conducted by the current authors (Holmes & Johnson, 2017). Institutional review board approval was obtained prior to data collection.
Results
Preliminary Analyses
Data were inspected, and it was determined there were no issues with normality or multicollinearity and there were no multivariate outliers. Available item analysis (Parent, 2013) was used to handle missing data, provided that at least 80% of the items on the given measure were completed (Downey & King, 1998). After running zero-order correlations and t tests, there were no significant relationships between demographic variables and scores on the EAT-26, establishing that analyses could be conducted without controlling for covariates. Statistically significant zero-order correlations were demonstrated between the five variables and each of the other variables, except for SV, which was not significantly associated with either body shame or interoceptive deficits (see Table 1). DE demonstrated a strong relationship with body shame (r = .71, p < .001) and a moderate relationship with self-surveillance (r = .50, p < .001). In addition, body shame and self-surveillance were moderately correlated (r = .56, p < .001).
Means, Standard Deviations, and Correlations Among Measured Variables.
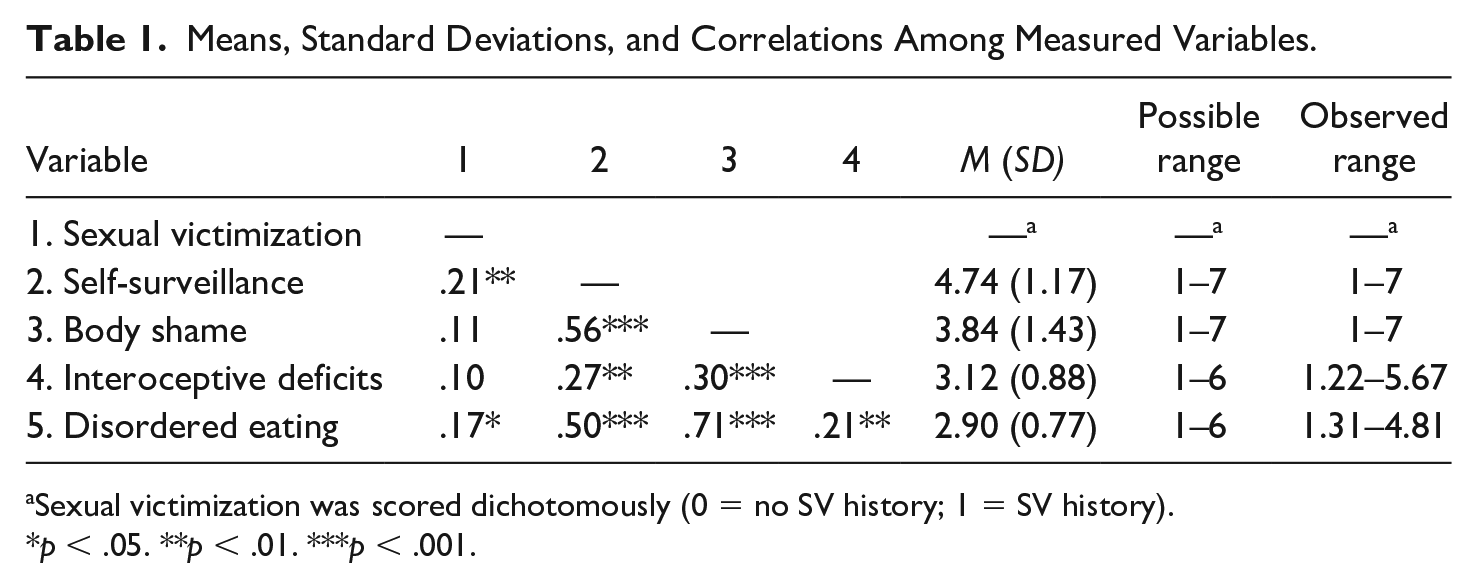
Sexual victimization was scored dichotomously (0 = no SV history; 1 = SV history).
p < .05. **p < .01. ***p < .001.
In the current study, 65.2% (n = 107) reported a lifetime SV history, defined as any form of unwanted sexual contact. Using this same definition, 49.1% (n = 78) reported SV occurring before the age of 14 and 61.3% (n = 98) reported SV occurring since the age of 14. Of those with a lifetime history of SV, 16.3% (n = 14) 1 reported unwanted sexual contact, 10.5% (n = 9) reported sexual coercion, 15.1% (n = 13) reported attempted rape, and 58.1% (n = 50) reported being raped. Among those who reported SV, the majority reported perpetration by men only (74.8%), 3.7% reported perpetration by women only, and 13.1% reported perpetration by both women and men (interestingly, but not uncommonly, 8.4% who answered questions indicating unwanted sexual contact stated, “I reported no experiences of victimization”).
Primary Analyses
Cross-tabulations were computed to compare rates of lifetime SV by sexual orientation. Supporting H1a, the prevalence rate of SV endorsed by bisexual women (65.2%; n = 107/164) was significantly greater than that reported by heterosexual women (55%; n = 186/335), χ(1) ≥ 4.29, p = .038. The remainder of potential group differences were tested by running a one-way multivariate analysis of variance (MANOVA). Results demonstrated a significant multivariate main effect for sexual orientation, F (4, 494) = 18.80, p < .001, Wilks’s Λ = .87,
Means, Standard Deviations, and MANOVA for Difference of Sexual Orientation on Disordered Eating Symptoms.
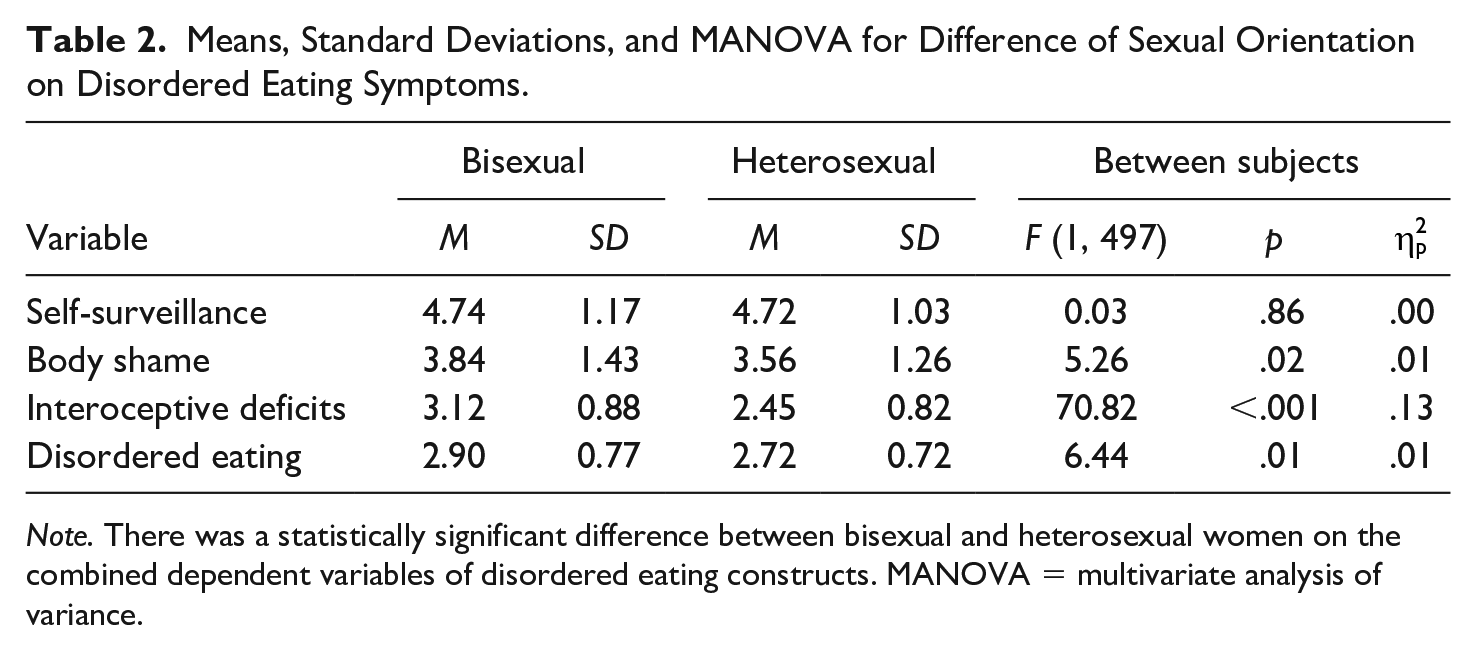
Note. There was a statistically significant difference between bisexual and heterosexual women on the combined dependent variables of disordered eating constructs. MANOVA = multivariate analysis of variance.
To address the remaining hypotheses, Model 6 of PROCESS for SPSS (Hayes, 2013) was utilized to conduct path analysis with 10,000 bootstrap samples. Overall, the model significantly predicted DE, F(1, 162) = 4.82, p = .030, R2 = .03. Supporting H2, the relationship between SV and DE was statistically significant, c = .27, t(165) = 2.19, p = .030. As hypothesized (H3), the indirect effect of SV on DE, via self-surveillance and body shame, was significant (see Table 3, Path A). None of the indirect effects that included interoceptive deficits as a mediator (H4–H6) were significant (Paths B, C, & D). Specifically, interoceptive deficits were not significantly associated with SV or DE above and beyond the other variables in the model (i.e., self-surveillance, body shame; see Figure 2). In addition, none of the exploratory indirect effects were significant (Paths E, F, & G). 2
Indirect Effects of Sexual Victimization on Disordered Eating.
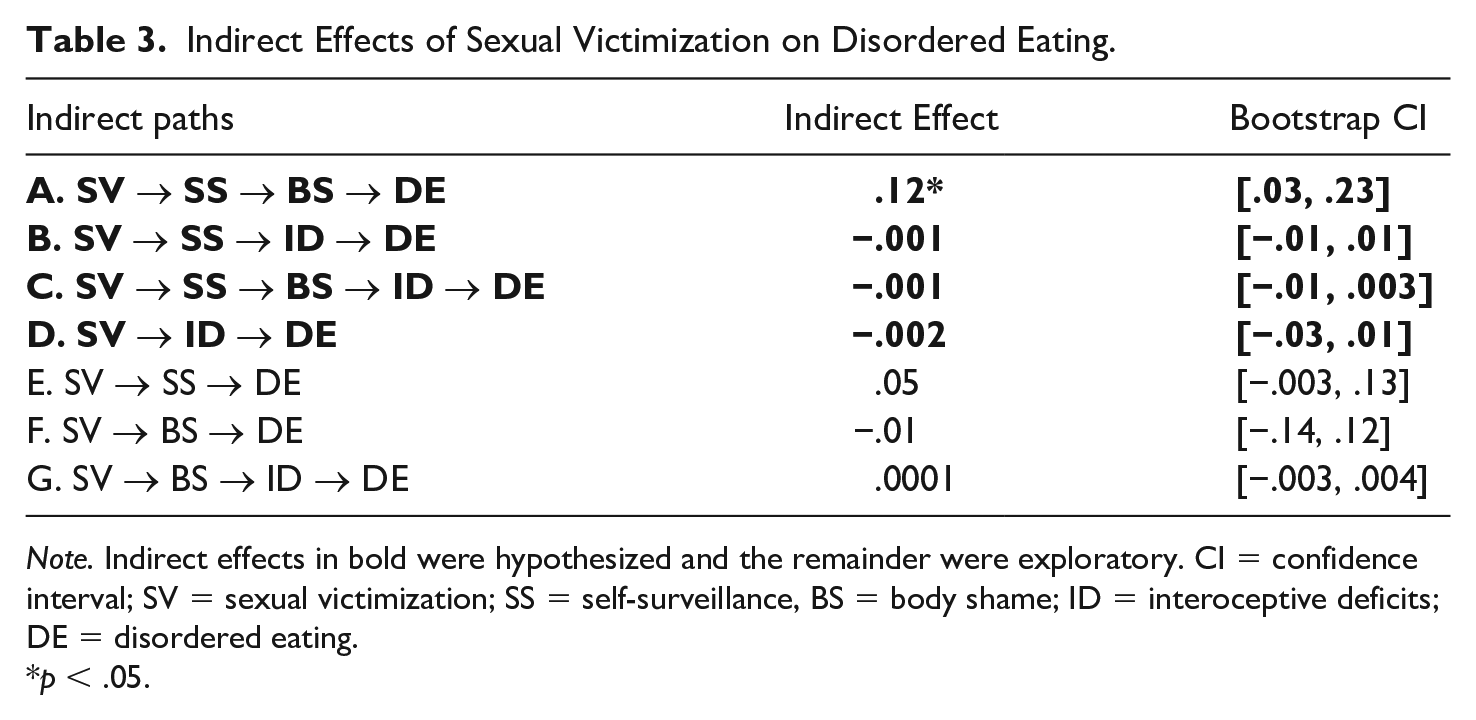
Note. Indirect effects in bold were hypothesized and the remainder were exploratory. CI = confidence interval; SV = sexual victimization; SS = self-surveillance, BS = body shame; ID = interoceptive deficits; DE = disordered eating.
p < .05.
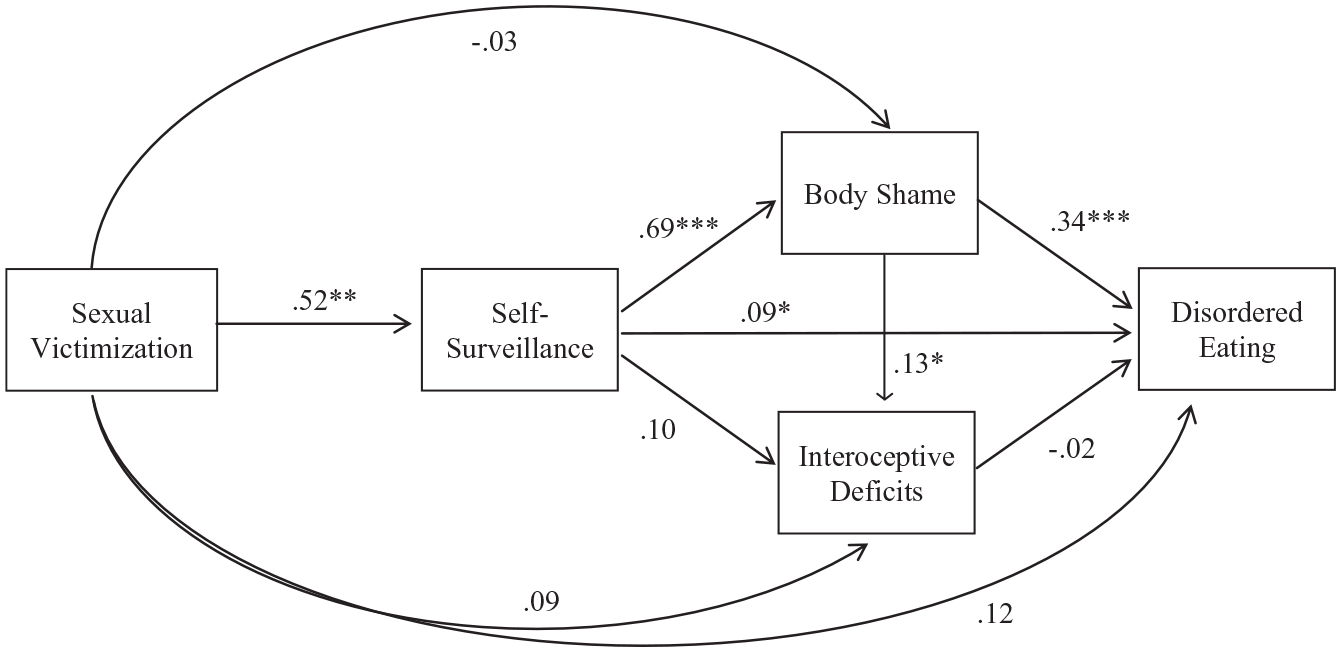
Relationships among variables in the proposed model of how objectification theory may clarify the relationship between sexual victimization and disordered eating.
Discussion
Consistent with other studies (e.g., Shearer et al., 2015; Walters et al., 2013), the rate of SV and degree of DE in the current sample of bisexual women was higher than that of heterosexual women. In addition to replicating these differences, the current study is the first, to our knowledge, to assess for potential differences on other variables relevant to objectification theory. Results demonstrated that bisexual women scored higher than their heterosexual counterparts on body shame and interoceptive deficits, but not self-surveillance. The general trend of bisexual women endorsing higher rates of SV and postassault outcomes (body shame, interoceptive deficits, DE) may be explained by their higher rates of SV victimization. It may also be due to their potential for being multiply marginalized, both as women and as bisexual individuals. While women of all sexual orientations are subject to sexual objectification and its sequela, as posited by objectification theory, bisexual individuals may be further hypersexualized due to the heterosexual male fetishization of them (Johnson & Grove, 2017). However, following this logic, one would also expect bisexual women to score higher on self-surveillance which they did not. Further research is needed to understand why bisexual women are more vulnerable to some postassault outcomes (i.e., body shame, interoceptive deficits, DE) but not self-surveillance.
The current study is also the first, to our knowledge, to establish a significant positive relationship between SV and DE among bisexual women, as it has been previously found among other samples of women (e.g., Armour et al., 2016; Dansky et al., 1997; Racine & Wildes, 2015). In an attempt to understand this relationship, the current study tested the application of objectification theory. This, too, is a vital inquiry given the historical underrepresentation of bisexual women in the objectification literature and infrequency with which extreme objectification (i.e., SV) has been assessed.
Consistent with objectification theory (Fredrickson & Roberts, 1997), the current study found support for the indirect relationship between SV and DE, via self-surveillance and body shame (Table 3, Path A). Although the results of this study are cross-sectional, and thus causality cannot be assumed, it is possible that SV facilitates internalization of objectification, which manifests as self-surveillance for bisexual women. Hypervigilance toward one’s body is then associated with body shame, which may be exacerbated if bisexual women blame their own bodies for their SV (Kearney-Cooke & Striegel-Moore, 1994). Body shame’s association with DE may occur for a number of reasons, including an attempt to attain the culturally prescribed body ideal, self-punishment, an attempt to diminish perceived attractiveness (i.e., through weight gain or loss of secondary sex characteristics), and so on (Fredrickson & Roberts, 1997; Kearney-Cooke & Striegel-Moore, 1994). Although Fredrickson and Roberts (1997) posited that this phenomenon would occur for girls and women broadly speaking, it may be especially salient for bisexual women, given the manner in which they are hypersexualized as a function of their sexual orientation (Johnson & Grove, 2017). For example, researchers have posited that the hypersexualization of bisexual women may result in worse social reactions following disclosure of SV due to bisexual-specific rape myths (e.g., “You were being affectionate with another woman but also flirt with guys. What did you think would happen?” “Is this another attempt for you to get attention, like when you kissed that girl?”; Johnson & Grove, 2017, p. 449). In fact, there is empirical evidence demonstrating that bisexual women do, in fact, receive fewer positive social reactions when they disclose SV, relative to heterosexual and lesbian women (Long et al., 2007). If bisexual women internalize these rape myths, they may become hyperaware of their bodies (i.e., self-surveillance), due to mistakenly blaming their bodies for their victimization (Holmes & Johnson, 2017), which, in turn, may result in body shame. As the current study did not assess for variables such as social reactions following SV disclosure or internalization of rape myths, it did not test this possibility; however, it may prove useful for future studies to do so.
The current significant indirect relationship between SV and DE via self-surveillance and body shame is consistent with studies examining primarily everyday objectification (e.g., Augustus-Horvath & Tylka, 2009; Kozee & Tylka, 2006) as well as the other study known to explicitly assess extreme objectification (i.e., SV) and DE (Holmes & Johnson, 2017). Notably, however, the only other study to test objectification theory among bisexual women did not support this. Specifically, Brewster et al. (2014) did not find the requisite significant relationship between sexual objectification and self-surveillance, which led them to conclude that, perhaps, bisexual women’s multiple marginalized identities result in them experiencing and interpreting sexual objectification experiences differently than objectification theory suggests. Given that the relationship between sexual objectification and self-surveillance is significant in the current study, however, it is possible that while everyday sexual objectification may not be related to higher levels of self-surveillance for bisexual women, more severe objectification (i.e., SV) is indeed related to self-surveillance.
In contrast, none of the hypothesized indirect effects, including interoceptive deficits (H3–H5), were significant (see Table 3, Paths B, C, & D). Specifically, interoceptive deficits were not significantly associated with SV, self-surveillance, or DE above and beyond the other variables in the model (see Figure 2). These results are contrary to the previous research that examined extreme objectification (Holmes & Johnson, 2017). However, they are consistent with the only other study that examined interoceptive deficits among sexual minority women, albeit lesbian women (Kozee & Tylka, 2006). Taken together, the results of the current study and that conducted by Kozee and Tylka (2006) can be interpreted as preliminary evidence that interoceptive deficits may function differently for sexual minority women. Neither study’s results are sufficient to explain why interoceptive deficits may function differently in this population; however, we explore possible explanations.
First, given bisexual women’s experience of multiple marginalization, they may experience a broader array of discriminatory experiences that may impact their ability to attend to internal states. To this end, Rogers et al. (2017) found that emotion dysregulation, a construct that conceptually overlaps with interoceptive deficits, was associated with nonsexual experiences of minority stress. Although it should be noted that emotion dysregulation and interoceptive deficits are not one in the same, they are related. As such, the measure of emotion dysregulation (i.e., Difficulties in Emotion Regulation Scale; Gratz & Roemer, 2004) utilized by Rogers et al. (2017) contains a subscale that assesses “lack of emotional awareness” which is core to interoceptive deficits. It is therefore possible that difficulty identifying and responding to internal emotions may be difficult for bisexual women for a number of reasons, and it may be less specific to their experiences of SV and DE. Notably, if this were the case, it would be a significant departure from the previous literature that has linked emotion dysregulation and interoceptive deficits to both SV and DE (e.g., Burns et al., 2012; Holmes & Johnson, 2017; Myers & Crowther, 2008; Racine & Wildes, 2015) in women not sampled for their sexual orientation. As such, additional research would be needed to confirm that interoceptive deficits do, in fact, function differently for bisexual women and, if so, ascertain why that might be.
Second, it should be noted that the analyses conducted in the current study assessed the seven possible indirect effects above and beyond one another. Notably, interoceptive deficits were associated with self-surveillance and DE in the zero-order correlations (see Table 1). It may be the case therefore that the indirect relationship between self-surveillance and body shame (see Table 3, Path A) is independently sufficient to explain the association between SV and DE in bisexual women. This possibility is further supported by the lack of significant direct effect above and beyond the indirect relationships tested (see Figure 2), which could also explain the null findings for the three exploratory indirect effects (see Table 3, Paths E, F, and G).
Implications
The current study is a response to the outstanding call for researchers to attend to psychosocial vulnerabilities of bisexual women (Johnson & Grove, 2017). First, it adds to the growing knowledge of adverse consequences (e.g., depression, PTSD, problematic alcohol use, smoking) of SV in bisexual women by establishing DE as an additional correlate. In addition, results suggest that self-surveillance and body shame are important constructs when understanding DE in sexually victimized bisexual women. Consequently, when clinicians work with bisexual women who are survivors of SV, they should thoroughly assess for the presence of DE, allowing for quicker detection and intervention. Similarly, when working with bisexual women presenting with DE, providers might consider the possible presence of an SV history and may address self-surveillance and body shame as more proximal clinical mechanisms. Doing so may provide clinicians with a clearer, more accurate theoretical conceptualization of their client. In addition, the current study, coupled with previous studies (e.g., Capitaine et al., 2011; Dubosc et al., 2012; Holmes & Johnson, 2017; Williams & Gleaves, 2003), supports the creation of tertiary prevention efforts that college campuses may make in an attempt to address the potential for DE development in female students of all sexual orientations.
Limitations and Future Directions
The results of the current study should be interpreted in context of its limitations. The most notable, perhaps, are the use of self-report measures and the study’s cross-sectional nature, which precludes any conclusions with regard to causality. Another limitation is the way in which bisexuality was operationalized. For the purposes of the current study, any participant who selected a response on the Kinsey scale item that endorsed both same- and other-sex attraction was retained in the sample; however, no data were collected on how they self-identify (i.e., do they in fact claim the term bisexual). This operationalization is consistent with the conceptualization of viewing bisexuality on a spectrum and is used in other studies (Brewster et al., 2014). However, given the discrepancy among various ways of conceptualizing sexual orientation (e.g., behaviors, attraction, self-identification; Savin-Williams & Vrangalova, 2013), there are limitations inherent to all operationalizations.
In addition, although the current study’s sample size was comparable with or larger than a number of other studies on objectification theory (e.g., Engeln-Maddox et al., 2011; Kozee & Tylka, 2006; Tiggemann & Williams, 2012), the relatively small sample size limits the strength of conclusions regarding the null findings. In addition, the undergraduate sample was utilized for its high rates of both SV and DE (Tripp & Petrie, 2001); however, its homogeneity limits generalizability to other samples of bisexual women. Future research, therefore, should attempt to replicate the results of current study with a longitudinal design and implementing other, larger samples of bisexual women, utilizing varying operationalizations of bisexuality.
In addition, some of the previous studies that have examined objectification theory among sexual minority women (Brewster et al., 2014; Watson et al., 2015) have found support for including population-specific minority stressor variables in the model (e.g., heterosexist events, internalized heterosexism). Future studies should test the applicability of these constructs in the context of extreme objectification. In particular, incorporating a measure that assesses experiences of being hypersexualized on the basis of sexual orientation, social reactions to SV disclosure, and internalization of bisexual-specific rape myths may be particularly helpful as it would allow researchers to empirically test our position that hypersexualization of bisexual women and its sequela may explain, in part, their higher levels of postassault outcomes relative to heterosexual women. In addition, it would be worthwhile for future research to examine how objectification theory may explain the association between SV and other symptoms that have been linked to sexual objectification (e.g., depression, sexual dysfunction, problematic substance use) given bisexual women’s heightened risk for psychological consequences associated with SV (Blosnich & Horn, 2011; Hequembourg et al., 2013; Hughes et al., 2010; Long et al., 2007).
Conclusion
In summary, the results of the current study demonstrate bisexual women’s heightened risk for SV and postassault outcomes as well as partially support the application of objectification theory to bisexual women’s experiences of SV and DE. These results demonstrate the necessity for clinicians to assess and recognize the potential for gender oppression–based consequences in bisexual women, especially when there is a history of SV. Further research is needed to better understand the differential function of interoceptive deficits in bisexual women and to assess other population-specific variables (e.g., heterosexist events, internalized heterosexism) within the greater objectification theory framework. Continuing in this line of research is imperative to understanding the unique psychosocial vulnerabilities of bisexual women and, ultimately, to provide culturally competent psychological care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work on this article by the first author was supported by National Institutes of Health (NIH) Grant T32 DA019426.