
Abstract
Many sexual victimization survivors disclose their experience; however, there is limited research investigating why women disclose this experience and how reasons relate to psychopathology. The current online study aims to further understand the experiences of 142 female survivors (aged 18–29 years) by identifying their reason for disclosure and investigating how reasons relate to self-reported depression and post-traumatic stress disorder (PTSD) symptomology. Qualitative analyses identified two reasons: intentional and elicited disclosures. Hierarchical linear regressions revealed that elicited disclosures were associated with higher PTSD symptomology than intentional disclosures above and beyond relevant covariates, suggesting that disclosure reason is an important factor in the recovery process.
At least 43% of women report experiencing some form of contact sexual violence (i.e., attempted or completed rape, forced penetration, sexual coercion, and/or unwanted sexual contact) in their lifetime, with the majority of women reporting that victimization first occurred in emerging adulthood (i.e., late teens through 20s; Arnett, 2000; Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, 2015). Specifically, 81% of completed or attempted rape survivors report experiencing their victimization before the age of 25 years (Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention, 2015). Sexual victimization survivors are at risk for a range of psychiatric disorders, including anxiety, substance use, and depression (Miller et al., 2011; Rothbaum et al., 1992; Sabina & Ho, 2014; Ullman, Townsend, et al., 2007). Furthermore, they are at a particularly elevated risk for developing post-traumatic stress disorder (PTSD), with 41.7% of rape survivors meeting criteria for PTSD compared with 11.5% of survivors of a nonsexual assault (Ullman & Peter-Hagene, 2014; Ullman, Townsend, et al., 2007).
Approximately two thirds to three quarters of female sexual victimization survivors ultimately disclose this experience to a recipient (Ahrens et al., 2007, 2010; Carson et al., 2019). However, little is known about why women first disclose these experiences and how this relates to mental health outcomes. Only one study known to these authors has identified specific reasons for disclosure of sexual victimization among adult female survivors and investigated how these reasons are associated with the well-being of the survivor (Ahrens et al., 2007). Expanding upon existing research, the goal of the current study is to further understand the disclosure process for emerging adult female survivors of sexual victimization (ages 18–29 years). This will be accomplished by identifying each survivor’s reason for their first disclosure and, subsequently, investigating if this reason for disclosure is associated with the survivor’s symptoms of PTSD and depression.
Emerging Adulthood
Emerging adulthood is a distinct developmental period, spanning ages from 18 years to mid-to-late 20s, during which individuals transition from adolescence to adulthood (Arnett, 2000, 2006). The United States Census Bureau (2017) estimates that as many as 50% of emerging adults are enrolled in college (Arnett, 2016), with higher rates among emerging adult females compared with emerging adult males (Arnett, 2016; National Center for Education Statistics, 2009). Emerging adulthood is, in general, a time period marked by transitions, exploration, and instability, making women especially vulnerable to unwanted sexual experiences during this time (Arnett, 2000, 2006). In fact, 81% of completed or attempted rape and 54% of stalking female survivors report that the incident occurred before the age of 25 years (Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Violence Prevention [CDC], 2015). Considering that women are at high risk for sexual victimization during emerging adulthood (CDC, 2015), and that a large percentage of these women are enrolled in college, it is important to examine unwanted sexual experiences in emerging adult, college-attending females.
Trauma Disclosure
Disclosure of a trauma involves telling someone about the traumatic experience verbally or in a narrative form (Pennebaker & Beall, 1986; Ullman, 2011). Individuals often experience signs of physical and emotional distress during and immediately following disclosure (Pennebaker & Beall, 1986; Pennebaker et al., 1988). However, in the long term, disclosure is associated with positive outcomes, including fewer visits to the doctor, lower levels of subjective distress, and healthier immune system functioning (Pennebaker & Beall, 1986; Pennebaker et al., 1988). Although research suggests that disclosure can be therapeutic, multiple factors can complicate the disclosure process for sexual victimization survivors, including contextual factors (e.g., private or social setting for disclosure), survivor characteristics (e.g., gender, age, culture, personality, attachment style, coping), and disclosure characteristics (e.g., voluntariness, modality, level of detail, timeliness; Ullman, 2011). Specifically, research with sexual victimization survivors has indicated that immediate disclosures, disclosures containing more detail and more personalization, and disclosures to female friends are associated with better mental health outcomes (Brown & Heimburg, 2001; Jacques-Tiura et al., 2010; Ullman, 2011). Alternatively, being African American, disclosing to a formal support provider, having many reasons for seeking support, and regretting disclosure are related to worse mental health outcomes (Jacques-Tiura et al., 2010; Ullman, 2011). One important variable influencing the relationship between disclosure and mental health outcomes is the survivor’s perception of the recipient’s reaction to disclosure. Research indicates that survivors report receiving both positive (i.e., emotional support or tangible aid) and negative (i.e., treating the survivor differently, distracting the survivor, taking control of the situation, blaming the survivor, or egocentric responses) recipient reactions to sexual victimization disclosure (Ullman, 2000). Overall, perceived positive recipient reactions are negatively correlated with survivors’ PTSD symptoms, and perceived negative recipient reactions are positively correlated with survivors’ PTSD symptoms (Dworkin et al., 2019; Ullman, 2011; Ullman & Peter-Hagene, 2014). While prior research has provided a strong framework for identifying specific disclosure characteristics that influence mental health outcomes, researchers have not fully investigated why women first choose to disclose and how reasons for disclosure may relate to the survivor’s subsequent psychopathology.
Reasons for Disclosure
A survivor’s motivation or reason for disclosing a sexual victimization experience may have an impact on their recovery. Research indicates that survivors often report experiences of sexual victimization to formal sources (e.g., police officers, doctors, mental health counselors) for support, medical assistance, or to seek justice (Ahrens et al., 2007; Ullman & Filipas, 2001). However, survivors’ reasons for disclosure to informal sources (e.g., friends, family members) have received less attention, and the influence of these reasons on survivors’ mental health remains unknown. Prior research suggests that specific reasons for nondisclosure (e.g., keeping the event to oneself due to shame or embarrassment) are associated with increased PTSD symptoms for the survivor, whereas other reasons for nondisclosure are associated with decreased PTSD symptoms for the survivor (Carson et al., 2019). There may be a similar pattern among disclosers of sexual victimization.
Only one research study (Ahrens et al., 2007) known to these authors has identified reasons for disclosure to both formal and informal sources among adult sexual victimization survivors and assessed how these reasons are related to survivors’ well-being. Through qualitative analyses of interviews with a community sample of rape survivors (M age = 34, SD = 10.05), researchers identified eight primary reasons for disclosing the event, which fell under two broad categories of “help-seeking” and “initiated by others.” Help-seeking disclosures were characterized by conscious decision-making of the survivor to actively seek support from others and consisted of survivors disclosing for: (a) emotional support, (b) catharsis, (c) tangible aid, or (d) to catch the rapist. Disclosures were categorized as initiated by others if the survivor clearly made the decision to disclose, but did not actively seek out support and was prompted by the recipient to disclose. This category consisted of survivors disclosing (a) to explain their behavior, (b) during a discussion about rape, (c) because they were asked what’s wrong, or (d) if the person was present at the scene. Ahrens and colleagues (2007) further investigated the disclosure process by examining the recipient of the disclosure (informal or formal support providers), reason for disclosure (help-seeking or initiated by others), the recipient reactions (positive or negative), and how the relationship between these variables predicts survivors’ self-reported general well-being (how hurt, angry, responsible, comforted, validated, supported, and unburdened the survivor felt following disclosure).
Prior research has provided a theoretical framework to suggest how Ahrens and colleagues’ (2007) specific reasons for disclosure, particularly disclosures initiated by others, may play a significant role in the recovery process for sexual victimization survivors. Sexual victimization experiences can be especially traumatic as they involve a loss of control over one’s body during the victimization, which, in turn, can influence the survivor’s beliefs about their safety and perceived control over their recovery (Janoff-Bulman, 1992; Perloff, 1983; Schepple & Bart, 1983; Ullman & Peter-Hagene, 2014). Research has consistently found that poor perceived control over recovery is associated with increased PTSD symptoms, and increased perceived control over recovery is associated with decreased PTSD symptoms (Frazier, 2003; Ullman et al., 2007; Ullman & Peter-Hagene, 2014). Similarly, reactions to disclosure that involve the disclosure recipient taking control of the survivor’s decisions are also associated with increased symptoms of PTSD and depression (Dworkin et al., 2019; Ullman, 2011; Ullman & Peter-Hagene, 2014). When a disclosure recipient initiates a survivor’s first disclosure, they are effectively taking the control surrounding the decision to disclose away from the survivor. This may further exacerbate a survivor’s perceived lack of control over their recovery, putting them at an increased risk for developing psychopathology. Conversely, disclosures that are initiated by the survivor may increase the survivor’s perceived control over their own recovery, decreasing their risk for developing psychopathology.
While Ahrens and colleagues (2007) have provided a strong foundation toward understanding why women first disclose their sexual victimization experiences, this research has not been replicated to see if these reasons are also relevant for emerging adult women, aged 18–29 years, who are at high risk for sexual victimization. Furthermore, although the researchers expected to find a significant relationship between the reason for disclosure and survivor well-being, their results did not support this hypothesis (Ahrens et al., 2007). Researchers noted that this may have been a function of the statistical analyses conducted (loglinear analysis), and called for future research to use continuous, quantitative measures to determine if a relationship exists between reasons for disclosure and survivor well-being. In addition, the levels of each variable included in the analysis were collapsed into binary responses, decreasing the variability in the data. Furthermore, researchers did not assess for specific PTSD or depression symptomology, but instead investigated the impact of disclosure reason on general survivor self-reported well-being following disclosure. In light of these limitations, the goal of the current study is to expand upon this research using hierarchical linear regressions to further investigate the relationship between reason for disclosure and well-being, specifically in regard to depression and PTSD symptomology, in emerging adult female sexual victimization survivors.
Current Study
The purpose of the current online study is to use qualitative analysis to identify reasons for disclosure among 142 college-attending female sexual victimization survivors (ages 18–29 years) and to investigate how these reasons are associated with self-reported depression and PTSD symptomology. Guided by the framework of Ahrens and colleagues (2007), we first hypothesize that the disclosure reasons identified in our study will be similar to their findings, and will fall into two broad categories of help-seeking/intentional (“intentional”) or initiated by others/elicited (“elicited”) and eight subcategories of possible reasons: (a) emotional support, (b) catharsis, (c) tangible aid, (d) catch/report perpetrator, (e) explain their behavior, (f) came up in discussion about sexual victimization, (g) asked what is wrong, or (h) person was present at the scene. After identifying the reasons for disclosure in the current sample, we aim to investigate whether reasons for disclosure are associated with symptoms of PTSD and depression, while controlling for relevant assault (e.g., drug use during victimization), disclosure (e.g., negative reactions to disclosure), and demographic (e.g., race, ethnicity) characteristics. Our second hypothesis is that intentional disclosures will be associated with fewer symptoms of PTSD and depression compared with elicited disclosures. The sample sizes for the individual subcategories were particularly small; therefore, associations between specific subcategories and symptomology were not examined.
Method
Participants and Procedure
Six hundred and four undergraduate women from two urban universities, one in New York City, NY, and one in Miami, FL, participated in an online study for psychology course credit in 2008 and 2009. They selected the current study among other available studies. All study procedures were approved by the university and institutional review boards. Women who chose to participate in the survey first completed a demographics questionnaire, followed by the Sexual Experiences Survey (SES; Koss & Oros, 1982). Women who endorsed an experience of sexual victimization completed the remaining measures. At the completion of the survey, participants were debriefed, thanked, and given referral information for mental health resources. Of these 604 students, 37% (n = 221) endorsed a history of sexual victimization (i.e., kissing, fondling, petting, attempted intercourse, completed intercourse). Of the 221 participants who experienced sexual victimization, 75% (n = 165) previously disclosed their experience. One hundred and forty-two of the women were between the ages of 18 and 29 years and were included in the current study. The participants in this study were a diverse group of undergraduate women. Of the 142 participants, 59.9% (n = 85) identified as Caucasian, 25.4% (n = 36) as “Other,” 7.0% (n = 10) as African American, 6.3% (n = 9) as multiracial, and 1.4% as Asian (n = 2). Of the 36 participants who identified as “Other,” 97.2% (n = 35) identified as Hispanic. The sample sizes for African American, Asian, and multiracial were small; therefore, to maximize power and make meaningful conclusions, all race categories were collapsed into two groups (White and People of Color). Ethnicity was also examined, which was a more appropriate way to investigate differences based on the diversity in this sample, with 68.3% of participants identifying as Hispanic and 28.9% identifying as Not Hispanic (see Table 1).
Demographics.
Measures
Demographics questionnaire
The demographics questionnaire asked participants to report their age, race, and ethnicity. Participants identified their racial background from a list of available categories and were able to select more than one category (African American or Black, American Indian or Alaskan Native, Asian or Asian American, Caucasian or White, Native Hawaiian or other Pacific Islander, and Other). Participants then indicated their ethnic background by selecting whether they identified as Hispanic or Non-Hispanic.
The SES
The SES (Koss & Oros, 1982) is a self-report measure of unwanted sexual experiences. Participants reported whether they experienced a variety of unwanted sexual experiences ranging from “sex play (fondling, kissing or petting)” to “sex (vaginal, anal or oral intercourse)” for multiple reasons, ranging from “because you were overwhelmed by a man’s continual arguments and pressure” to “because a man threatened or used some degree of physical force.” Data on the survivor–perpetrator relationship (stranger, acquaintance, casual date, romantic acquaintance, spouse, relative, or other) and disclosure recipient (formal or informal) were also collected. This survey has been used with a large number of college students (Koss et al., 1987; Koss & Oros, 1982) and in assessment of responses to sexual victimization disclosure (Ullman & Filipas, 2001). Prior research has established test–retest reliability with a reported mean of 93% agreement between the two administrations 1 week apart (Koss & Gidycz, 1985). This measure also has considerable validity with college women.
Disclosure themes
Disclosure themes were derived from experiences reported on the SES. Participants were asked to identify which sexual experience or experiences they considered to be the most traumatic. They were then asked if they had disclosed or talked with anyone about these events. Those who previously disclosed the victimization then responded to the following open-ended question regarding their first disclosure of the event: “Why did you choose to disclose to this person?” The reason the first disclosure was investigated here is because prior research has indicated that the first disclosure predicts the likelihood of further disclosures and of the survivor seeking support (Ahrens et al., 2007). Qualitative analysis of these reasons for disclosure was conducted to derive common themes. The content of these themes and how they were identified is discussed in more detail below in the “Data Analysis” and “Results” sections.
The Social Reactions Questionnaire (SRQ)
The SRQ (Ullman, 2000) is a 48-item self-report measure used to assess responses to disclosure of sexual victimization. It was modified to assess responses to the first disclosure experience. For each item, women reported how often they received different recipient reactions from the first person to whom they disclosed on a scale ranging from 0 (never) to 4 (always). The two positive responses to disclosure subscales were (1) emotional support and (2) tangible aid/information support. The five negative responses to disclosure subscales were (a) victim blame; (b) taking control; (c) distraction; (d) treating differently; and (e) egocentric reactions (i.e., focusing on the disclosure recipient’s needs and distress rather than on the survivor’s). Responses were totaled to create subscales assessing the frequency of which women received overall positive reactions and overall negative reactions to sexual victimization disclosure. Cronbach’s alpha was strong for both total positive response (α = .88) and total negative response (α = .77).
The Beck Depression Inventory, Second Edition (BDI-II)
The BDI-II (Beck et al., 1996) is a 21-item self-report measure that assesses a range of depressive symptoms, including sadness, anhedonia, hopelessness, guilt, and changes in sleep and appetite. Standard administration and scoring guidelines were followed. Participants chose a response for each item that best reflects how they have been feeling in the past 2 weeks from four possible options representing levels of severity of a symptom. Each item is scored on a 4-point scale (0–3) with possible total scores ranging from 0–63, with higher scores indicating higher levels of depressive symptomology. The BDI-II is a widely used measure with considerable reliability and validity (Beck et al., 1961, 1988), including with survivors of sexual victimization (Cheastey et al., 2002; Nikulina et al., 2016). In the current study, Cronbach’s alpha was .93 and survivors reported an average of 11.22 (SD = 10.4) symptoms, which indicates mild depression (Beck et al., 1996). Based on the standard cutoff score guidelines, 62% of participants endorsed minimal depression, 17% met criteria for mild depression, 15% met criteria for moderate depression, and 6% met criteria for severe depression (Beck et al., 1996).
The PTSD Symptom Scale (PSS)
The PSS (Foa et al., 1993) is a 17-item, self-report measure assessing participants’ symptoms of PTSD over the past 2 weeks. This measure is based on Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria; for the purposes of this study, the total symptomology severity was calculated. Responses are on a Likert-type scale ranging from 0 (not at all) to 3 (five or more times per week/very much/almost always) with possible total scores ranging from 0–51, with higher scores indicating higher levels of PTSD symptomology. Participants completed the assessment in reference to the most severe sexual victimization experience reported on the SES. The PSS has considerable validity and reliability, including with survivors of sexual victimization (Ahrens et al., 2010; Foa et al., 1997). In the current study, PSS has a Cronbach’s alpha of .91 and survivors reported 9.03 (SD = 9.04) symptoms on average, which is slightly lower than studies with similar populations (Ahrens et al., 2010). In addition, 49% of the current sample met the criteria for PTSD based on DSM-IV-TR criteria, and this rate is consistent with prior research (American Psychiatric Association, 2000; Ullman & Peter-Hagene, 2014).
Data Analysis
To test the first hypothesis and identify reasons for disclosure, a qualitative analysis was conducted, as recommended by Miles and Huberman (1994). An initial codebook was created using open coding guided by the subcategories previously identified in prior research (Ahrens et al., 2007; Miles & Huberman, 1994). The codebook included seven of the eight subcategories identified by Ahrens and colleagues as well as one additional reason (i.e., “pressure from an outside source”). The subcategory of “catch the rapist” identified by Ahrens and colleagues was not endorsed by any of the participants in the current sample and was not included in subsequent analyses. Two doctoral students (first and second authors) analyzed the content of the disclosure reasons provided by all participants and together coded 20% of the data to establish reliability (Syed & Nelson, 2015). They then independently categorized each reason into one of the eight subcategories. When the raters disagreed, other coauthors were consulted and the code was changed to reflect the category determined most appropriate by all coauthors. Interrater reliability was calculated on these codes using SPSS v. 25; the Kappa coefficient was .94, indicating an almost perfect interrater agreement on identified themes (Viera & Garrett, 2005). Prevalence rates of reasons for disclosure were computed by running frequencies for each of the categories using SPSS v. 25. Based on precedent established in prior research (Ahrens et al., 2007), these eight categories were then collapsed into two primary reasons (intentional and elicited disclosures), which parsimoniously represented the data. These two primary reasons were used in subsequent analyses.
All subsequent analyses were conducted with SPSS v. 25. Due to the disparate sizes of the two disclosure groups, cross-tabulation was used to also provide descriptive information for each group. To test the second hypothesis and investigate if intentional disclosures are associated with fewer PTSD and depression symptoms compared with elicited disclosures, independent t tests were run to first identify bivariate relationships between intentional disclosures and elicited disclosures in total symptoms of PTSD and depression. Adjusted t and p values were interpreted in analyses where Levene’s Test for Equality of Variances was significant. To identify whether the reasons for disclosure are associated with PTSD and depression symptomology after controlling for relevant assault characteristics (e.g., use of drugs during victimization), disclosure characteristics (e.g., reactions to disclosure), and demographic characteristics (e.g., ethnicity and school location), two separate hierarchical linear regressions were run. To reduce Type I error and maximize power, covariates were included in the regression models if they were significantly associated with the outcome measure (i.e., total depression or PTSD symptoms) in bivariate analyses (Hinkle et al., 1998). In Model 1 (predicting depression) and in Model 2 (predicting PTSD symptoms), assault and demographic characteristics and standardized overall negative reactions were entered as predictors in Step 1 and the reason for disclosure (intentional vs. elicited) was entered in Step 2. To assess significance and effect size of the associations between reasons for disclosure and symptomology, significance, beta values, and R2 change from Steps 1–2 were assessed.
Results
Hypothesis 1: Identifying Reasons for Sexual Victimization Disclosure
Using the method described above, we identified eight reasons for disclosure: (a) socioemotional support, (b) catharsis, (c) tangible aid, (d) discussion about sexual victimization, (e) person present at scene, (f) pressure from outside source, (g) explain behavior, and (h) asked what is wrong. These eight reasons were then condensed into two overall themes: (a) help-seeking/intentional disclosure (“intentional”) and (b) initiated by others/elicited (“elicited”) disclosure. The majority of the participants engaged in an intentional disclosure (n = 132) compared with elicited disclosures (n = 10; see Table 2 for frequencies of each primary reason and theme). It is important to highlight that sample size for elicited disclosures was particularly small, and there was a significant discrepancy in sample sizes across the two disclosure groups. However, as there is a dearth of literature on elicited disclosures and the subsequent recovery process, results are presented for both groups. In addition to providing inferential statistical analyses, descriptive data for each of the groups are presented in Table 3 and discussed below.
Frequencies of Reasons for Disclosure.
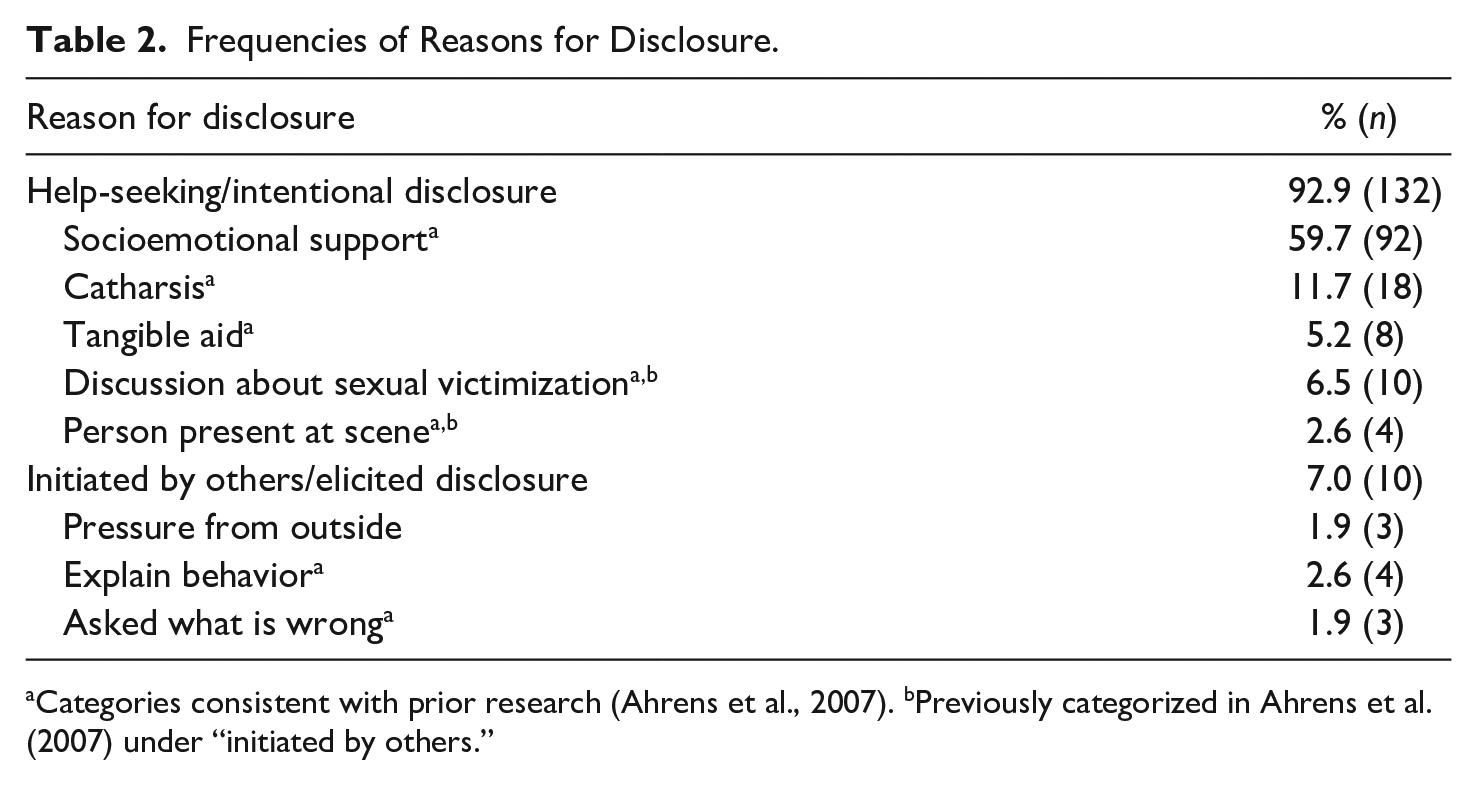
Categories consistent with prior research (Ahrens et al., 2007). bPreviously categorized in Ahrens et al. (2007) under “initiated by others.”
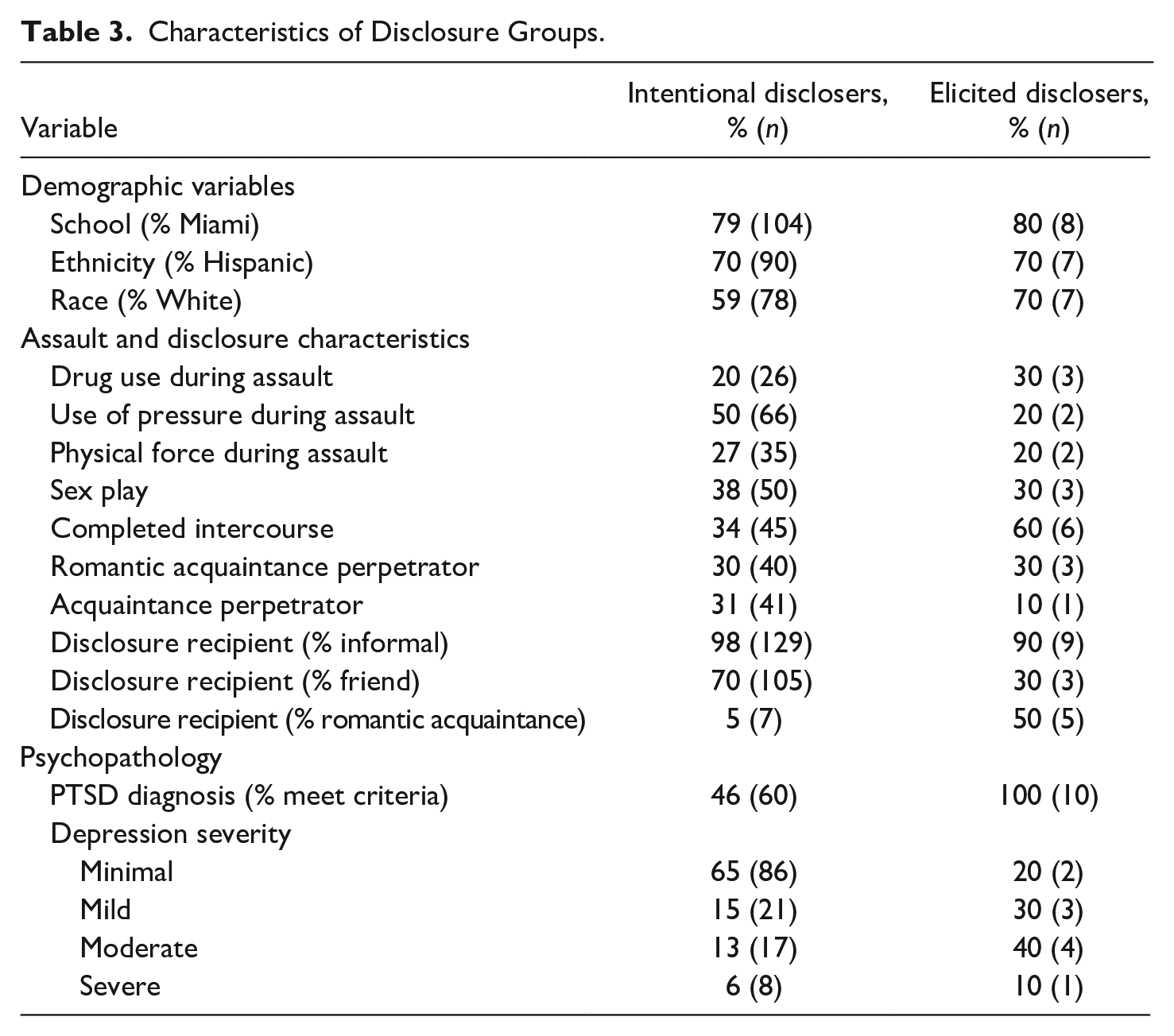
Characteristics of Disclosure Groups.
Following the methodology established by Ahrens et al. (2007), intentional disclosures were characterized by conscious decision-making on the part of the survivor to disclose their experience to actively seek support. In addition, this category included reasons that reflected a conscious decision to disclose in an attempt to help build a social relationship. While this general category consisted of multiple specific reasons, each reason had the same underlying theme. Specifically, all reasons were driven by a decision to disclose to seek help or to support someone else in some capacity. Examples of intentional disclosures included, “she is my best friend, someone I can turn to when I need her the most,” “they were there and I trust them completely,” “. . . I had to get it off my chest and I trusted this person,” and “she was my roommate at the time and she had the same experience with the guy. She opened up to me and then I broke down,” which were categorized as socioemotional support, person present at scene, catharsis, and discussion about sexual victimization, respectively. Disclosures were classified as elicited if they were in any way pressured or coerced by others and did not reflect the survivor’s deliberate decision to discuss the experience. In addition to being prompted by another individual, the specific content provided by the elicited disclosures demonstrated that these disclosures also differed from intentional disclosures in that they did not occur in the context of receiving or seeking support. Specifically, responses often demonstrated that the disclosure was not elicited due to the survivor’s observable emotional distress, but due to an egocentric concern from the disclosure recipient (e.g., “He wanted to know why I was not a virgin” and “He heard about the incident and asked about it.”).
As seen in Table 2, five of the primary reasons were categorized as intentional disclosures and three of the primary reasons were categorized as elicited disclosures. Of the 154 women who disclosed their experiences, 148 provided reasons for disclosure, including 132 intentional disclosures and 10 elicited disclosures. Six women provided reasons that the authors were unable to categorize due to limited content (i.e., “it was his other friend who did it to me.”) and were removed from subsequent analyses. Of the 142 women, 9 endorsed two themes. For parsimony, the reason that was listed first was considered more salient and used to categorize the reason. For example “I had to get it off my chest. And she was my friend” was categorized as catharsis. In all these cases, the two reasons were both part of the same broad theme of intentional disclosures. The distribution between intentional and elicited disclosures differs from frequencies identified in prior research with rape survivors in the community (Ahrens et al., 2007). Specifically, there were more intentional disclosures than expected in the current sample and fewer elicited disclosures than expected.
Hypothesis 2: Investigating Associations Between Reasons and Symptomology
Significant bivariate differences in symptomology were identified between intentional disclosures and elicited disclosures (see Table 4). Specifically, women who engaged in elicited disclosures endorsed significantly more depression symptoms (M = 19.4, SD = 9.52) than women who engaged in intentional disclosures (M = 10.12, SD = 10.11). In addition, 80% of women who engaged in elicited disclosures met criteria for mild, moderate, or severe depression, whereas only 35% of women engaging in intentional disclosures met criteria for depression (see Table 3). In regard to PTSD, women who engaged in elicited disclosures also endorsed significantly more PTSD symptoms (M = 22.80, SD = 5.88) than women who engaged in intentional disclosures (M = 8.40, SD = 8.69). Furthermore, 100% of women who engaged in elicited disclosures met criteria for PTSD compared with 46% of women who engaged in intentional disclosures (see Table 3).
Bivariate Associations Between Intentional and Elicited Disclosures.
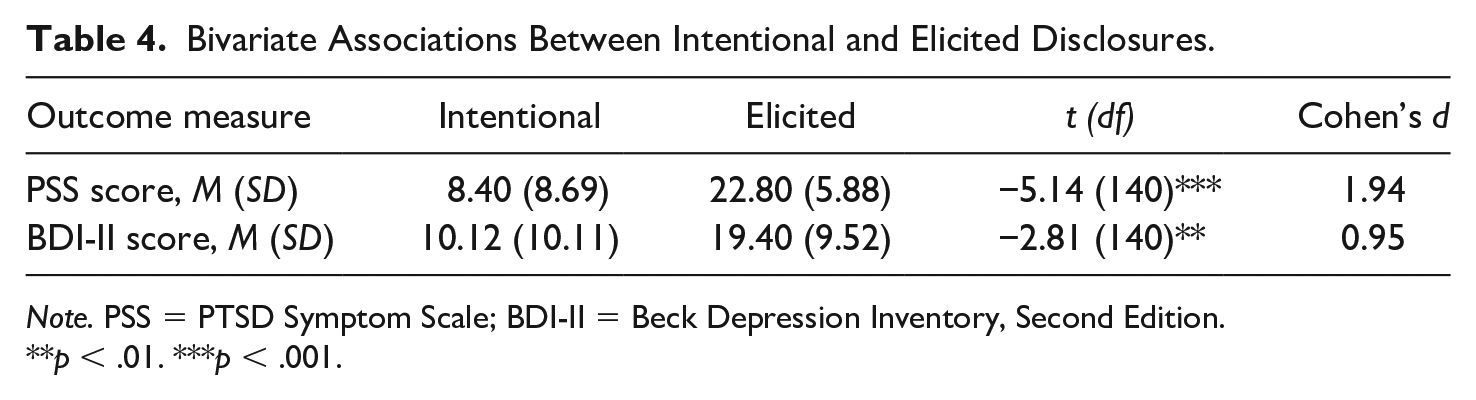
Note. PSS = PTSD Symptom Scale; BDI-II = Beck Depression Inventory, Second Edition.
**p < .01. ***p < .001.
Results from the hierarchical linear regressions suggest that reasons for disclosure are associated with survivor PTSD symptomology above and beyond the effects of recipient negative reactions to disclosure and other known risk factors (i.e., demographics and victimization characteristics). In the current sample, participants who were living in New York City endorsed higher PTSD and depression symptoms than those living in Miami, so this was included as a covariate. The regression analyses also included victimization characteristics, assessed in the SES, which reflect the type of assault instigator (i.e., pressure, authority, physical force, drug use). In bivariate analyses, the type of victimization (i.e., sex play, attempted intercourse, completed intercourse), perpetrator (i.e., acquaintance, romantic acquaintance, other), disclosure recipient (i.e., formal, informal), and positive disclosure reaction did not predict symptomology in this sample and, therefore, were not included as covariates. Descriptive data are included in Table 3 to demonstrate the distribution of these assault and demographic characteristics across the disclosure groups. As seen in Table 5, after controlling for covariates, elicited disclosures were associated with higher PTSD symptoms relative to intentional disclosures (β = .31, R2 change = .08). However, after controlling for covariates, reasons for disclosure were no longer associated with symptoms of depression (β = .13, B = 1.29, p = .17).
Regression Results for the Relationship Between Disclosure Reasons and PTSD Symptomology.

Note. PTSD = post-traumatic stress disorder; PSS = PTSD Symptom Scale.
Help-seeking disclosers were identified as the reference group.
p < .05. **p < .01. ***p < .001.
Discussion
The goal of the current study was to investigate why women first disclose experiences of sexual victimization and how these reasons for disclosure may relate to subsequent psychopathology. Prior research has identified various assault and survivor characteristics that are important to the disclosure process, influencing mental health outcomes for survivors. Results of the current study suggest that reasons for disclosure are also an important element in the disclosure process and may be associated with the development of PTSD.
Reasons for Disclosure
The themes for reasons of sexual victimization disclosure that were identified in the current sample were intentional (i.e., socioemotional support, catharsis, tangible aid, discussion about sexual victimization, and person present at scene) and elicited (i.e., pressure from outside source, explain behavior, and asked what is wrong). The two overall themes and seven of the eight primary reasons are the same as previously identified by Ahrens and colleagues (2007). Pressure from outside source was developed by the current authors to capture women who reported disclosing their experience after being coerced by another individual. In addition, discussion about sexual victimization and person present at scene were categorized as initiated by others in prior research, but were characterized under the intentional disclosures in the current study as the content of these reasons provided by the women in this sample more accurately reflected a conscious decision to disclose (e.g., “because she disclosed a similar situation to me and I felt like the experience would help her cope” and “she was with me at the time and I was scared and ran to her and told her what happened. She has been my best friend since pre-school”). The catch the rapist subcategory that was previously identified by Ahrens and colleagues (2007) was not endorsed by any of the participants in the current sample. This is likely due to the fact that the majority of the disclosures in the current sample were to informal sources and there were no disclosures to law enforcement, which is consistent with prior research indicating that less than 5% of college students disclose sexual victimization experiences to the police (Miller et al., 2011).
Despite the minor differences, these findings are largely consistent with prior research suggesting that many women make an intentional decision to disclose their experiences of sexual victimization to receive emotional support, tangible aid, or justice (Ahrens et al., 2007; Orchowski & Gidycz, 2012; Ullman & Filipas, 2001). However, these results also indicate that some women who disclose their experience do not do so intentionally, but share their experience for the first time with someone who has either pressured them or questioned them about their current behavior, emotional state, and/or relationship history. The underlying motivation driving these two types of disclosures is distinct and, understandably, may influence psychological outcomes differently. The distribution between the two types of disclosure was different than previously demonstrated, with more intentional disclosures than expected and fewer elicited disclosures than expected. This may be due to the differences in samples as prior research identifying reasons for disclosure used a community sample of rape survivors, with a mean age of 34 years (Ahrens et al., 2007). It is possible that the current sample of emerging adults has more resources available as all participants were enrolled in a 4-year college, increasing the number of help-seeking, intentional disclosures. As such, the field would benefit from additional studies examining reasons for disclosure to better understand these discrepancies, particularly in the emerging adult population.
Reasons for Disclosure and Associated Symptomology
The findings demonstrated that reasons for disclosure are associated with PTSD symptomology over and above relevant assault and demographic characteristics and the effects of negative recipient reactions received from disclosure recipients. This suggests that reason for disclosure is important for survivors’ well-being, particularly when looking at PTSD symptomology. It is important to note that the sample size for elicited disclosures was particularly small in the current sample. While this limitation cannot be ignored and inferential statistical differences are one key approach to understanding the data, interpreting the descriptive clinical implications is equally valuable. Notably, our findings indicate that albeit a small sample, 100% of women who engaged in elicited disclosures met criteria for PTSD. Prior research investigating understudied groups has established precedent for publishing results with unbalanced or small group sizes (e.g., Orchowski & Gidycz, 2012; Rascovsky et al., 2007; Widom et al., 2012). As there is limited research on the reasons for disclosure of sexual victimization, particularly in regard to the impact of elicited disclosures, it is important to present both the inferential and descriptive statistics. However, the results of the current article should be interpreted with caution.
While reason for disclosure may be an important variable in relation to depression outcomes for sexual victimization survivors, the current findings suggest it does not uniquely predict depression symptomology above and beyond relevant covariates. These findings are consistent with prior research demonstrating that while sexual victimization survivors are at an increased risk for developing both depression and PTSD, PTSD is the most common mental health outcome for survivors (Liu et al., 2017; Neilson et al., 2017). It is possible that the covariates, such as assault severity and social reactions to disclosure, that were controlled for in multivariate analysis, are better predictors for depression symptoms than the reasons for disclosure.
The reason driving a woman’s disclosure is one of the first steps in the disclosure process and may have a stronger association with mental health outcomes than other factors that have previously been examined in the literature. Why a woman first discloses this intimate experience may influence whom she tells, how the recipient reacts, the type of support the survivor receives, and ultimately the severity of PTSD symptomology. These findings highlight the complexities of the disclosure process. Prior research using structural equation modeling has identified various pathways explaining the relationship between sexual victimization experiences and PTSD by examining associations between trauma history, victimization characteristics, self-blame, avoidance coping, general social support, and recipient reactions (Ullman, Townsend, et al., 2007). These models suggest a bidirectional relationship between various risk and protective factors that are unique to the survivor and her experience (i.e., negative reactions may lead to avoidance coping and avoidance coping may elicit negative reactions, which in turn lead to PTSD). Reason for disclosure is another key element of the disclosure process that may further influence these pathways and can be an important target for intervention efforts. However, as this was a cross-sectional study, temporal relationship between these variables cannot be determined. It is possible that in some circumstances, survivors’ symptoms also drove the initial disclosure. For example, survivors who demonstrate higher levels of distress may prompt an elicited disclosure from a concerned loved one. Nonetheless, the content of many of the participant’s responses often indicated that the disclosure was not elicited due to observable emotional distress, but rather due to an egocentric concern of the disclosure recipient (e.g., “He wanted to know why I was not a virgin.”). Future longitudinal research should examine how reason for disclosure may fit in with previously identified models examining risk and protective factors involved in the relationship between sexual victimization and PTSD symptomology.
Prior research has suggested that many women disclose experiences of sexual victimization to receive support, aid, or justice (Ahrens et al., 2007; Ullman & Filipas, 2001). While our results corroborate these findings, we have also identified a subgroup of women who do not make the intentional decision to disclose this traumatic experience. Women who lose the ability to make the conscious decision to share this information are at risk for reporting higher levels of PTSD, even after controlling for the effects of negative reactions to this disclosure. The loss of control over one’s body that occurs during sexual victimization can influence the survivor’s beliefs about their personal safety and perceived control over recovery (Janoff-Bulman, 1992; Perloff, 1983; Schepple & Bart, 1983; Ullman & Peter-Hagene, 2014). Among sexual victimization survivors, perceived control over recovery has an inverse relationship with total PTSD symptoms (Frazier, 2003; Ullman, et al., 2007; Ullman & Peter-Hagene, 2014). Furthermore, lower perceived control over recovery has been found to mediate the relationship between negative reactions to disclosure and greater PTSD symptoms (Ullman & Peter-Hagene, 2014). By eliciting a nonvoluntary disclosure of a sexual victimization experience, disclosure recipients may further exacerbate a survivor’s feelings of limited perceived control over recovery, putting them at an increased risk for developing PTSD. In addition, prior research suggests that disclosure is not always beneficial for sexual victimization survivors and specific reasons for nondisclosure (e.g., lack of shame or embarrassment, minimizing the experience) are associated with decreased PTSD symptoms (Carson et al., 2019). These results highlight the significance of educating the general public as to the importance of not coercing or forcing a woman to share her experience and allowing the survivor to make the decision regarding if and when she would like to disclose her experience. Furthermore, half of the elicited disclosures in the current sample were prompted by the survivor’s romantic partner. Providing psychoeducational interventions on effective interpersonal communication strategies to emerging adult males and females may help reduce the prevalence of elicited disclosures. At a time when society has begun to give attention to experiences of sexual victimization, helping a woman to feel comfortable and safe enough to make the conscious decision to disclose her experience may be a successful approach to improving survivor well-being.
Furthermore, while this study focused solely on first disclosures, these findings also may have implications for future disclosures for sexual victimization survivors. Title IX is a federal law that prohibits discrimination on the basis of sex in any federally funded education program or activity (United States Department of Justice, 2015). Under Title IX at many universities throughout the United States, college faculty members are mandated to report any sexual assaults that occur on campus. If a female student discloses a sexual victimization experience to a trusted professor, the faculty member will likely be required to report this information, despite being told in confidence. While this legislation was created to protect survivors of sexual victimization, it may unintentionally have the opposite effect by forcing the student to share this information with more than just the person to whom she disclosed. It will be helpful for universities to be aware of the possible outcomes associated with coerced or forced disclosures to handle these cases in a sensitive manner. This may involve psychoeducation for policymakers and university faculty members, who can be trained to respond appropriately to distressed students.
Limitations
These findings should be considered in the context of study limitations. Participants were female undergraduates from two urban universities in the eastern United States, and findings may not generalize to different populations. High rates of sexual victimization are also seen among gender-nonconforming individuals (Hirsch & Mellins, 2019), and future sexual victimization research will benefit from including these populations to better understand their unique experiences. In addition, the majority of participants identified as Hispanic. While the percentage of Hispanic participants in the current sample is much greater than that of Hispanics in the general population, our rates are consistent with the percentage of Hispanic individuals living in Miami, Florida (United States Census Bureau, 2019), which is where a majority of our participants lived. As such, while this sample accurately reflects the population of Miami, results may not be generalizable to other cities with smaller Hispanic populations. While this may limit the generalizability of our findings, our high rate of Hispanic participants is also a strength of the current article. Prior research with Hispanic female sexual victimization survivors has noted that the Hispanic population is continuing to grow in the United States, and there is an increased need for research, services, and prevention efforts to address sexual victimization in the Hispanic community (Ahrens et al., 2011). Furthermore, researchers note that disclosing and discussing sexual victimization experiences is typically seen as taboo in Hispanic culture (Ahrens et al., 2011). The findings of the current article identifying reasons why women do disclose these experiences can be used to help guide future research with this underserved and understudied population.
Another key limitation is that there were few participants who identified as African American or Asian in the current study. To maximize power and make meaningful conclusions, race categories were collapsed into White or People of Color. However, the study does not intend to suggest that all women who identify as People of Color share similar experiences, and these results may not generalize to everyone who identifies as a person of color. In addition, the overwhelming majority of study participants disclosed to an informal source. These results may not be generalizable to formal source disclosures.
As previously mentioned, cross-sectional data collection limits interpretations about causality and direction of associations, which can be addressed in future longitudinal studies. In addition, few women identified the timing of the victimization, so this potential limitation could not be controlled for. However, a majority of participants reported that the perpetrator was someone they were dating, a romantic acquaintance, or a spouse, indicating that the victimization occurred when participants were at least of dating age. Furthermore, the current study data were collected in 2008 and 2009, and the findings may not be generalizable to the current time, particularly following the “Me Too” social movement encouraging survivors of sexual victimization to disclose their experience. However, while there may be different or additional reasons for disclosure for women who disclosed after the “Me Too” movement, it is likely that the reasons for disclosure identified here are still relevant for women today.
Furthermore, this study was conducted online and relied solely on retrospective self-report, limiting the data to the perceptions of each individual participant. However, one key benefit of online data collection is increased anonymity, providing a platform for women to more honestly report their victimization experiences compared with face-to-face interviews (Barr et al., 2017; Nooner et al., 2010). To ensure the quality of these online data, a consistency check was employed to screen for implausible demographic combinations (i.e., race, ethnicity, place of birth; Aust et al., 2013). No data were excluded following this technique. In addition, this online survey was restricted to undergraduate students to receive course credit, which reduced the likelihood of women participating multiple times and eliminated participants who search the internet for paid studies (Aust et al., 2013). Finally, the sample size for the elicited disclosure group was particularly small. However, to account for this, descriptive statistics were provided and effect sizes were also calculated, suggesting very large effect sizes for all significant bivariate analyses.
Despite these limitations, this is only the second study known to the research team to examine reasons for disclosure of sexual victimization and the first to assess the association between reasons for disclosure and psychopathology symptoms of PTSD and depression. With the increase in the societal focus on sexual victimization, it is important to draw upon research to educate the public about these experiences and establish an environment where the survivors feel comfortable and choose to disclose their experience to receive the support and help they may need.
Footnotes
Acknowledgements
The authors thank the women who participated in this study and shared their victimization experiences with the researchers. The authors also thank the psychology departments of the involved institutions for supporting this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Graduate Center, City University of New York (CUNY), who supported the first two authors with fellowship funding while working on this article. This work was sponsored in part by funding from the National Institute of General Medical Sciences (1 SC2 GM125547 01), Psi Chi (Mamie Phipps Clark Research Grant; Graduate Research Grant), and the Graduate Center, CUNY (Doctoral Student Research Grant). Support for this project was also provided by a PSC-CUNY Award, jointly funded by the Professional Staff Congress and the CUNY.