
Abstract
The intersecting issues of intimate partner violence (IPV) and alcohol abuse in South Africa are often characterized as “disasters.” Ethnographic research among women in Soweto demonstrates the different manifestations of IPV, perceptions of abuse, and coping mechanisms to manage harmful domestic relationships. Findings suggest a consistent relationship between excessive drinking patterns and IPV—most significantly, physical and emotional abuse—while indicating that domestic violence measures should include questions about stress. The authors also argue against pathologizing the relationship between IPV and alcohol abuse, to instead center the structured, sedimented ways that violence within the home has become a “normalized” disaster.
Looking back, I could say that my husband did abuse me to a certain extent physically. […] He was really into alcohol at the time. The abuse only stopped one day when I decided to fight back. I also asked him how he could beat me up if he said that he loved me. I told him that that was no way to treat the one that you love. [Siphokazi (pseudonym), widow, age 49]
Siphokazi's story introduces the complex relationship between intimate partner violence (IPV), alcohol use, and love, the fights that frequently occur between romantic partners and which many associate with problematic drinking in South Africa. South Africa has long labored under the onerous honorific of “Rape Capital of the World” (Human Rights Watch, 1995), a title tied to histories of colonization, racial oppression, and gendered violence, a longue durée which many argue served to “normalize” a culture of violence (Brankovic, 2019; Campbell, 1992). Within the continuum of gender-based violence (GBV), IPV represents the most prevalent form of violence experienced by women, estimated to impact one in three South African women in their lifetime (Abrahams et al., 2006). Attempts to diagnose why IPV is so common in the country have often dwelt upon the influence of illicit substances, particularly, alcohol. In fact, South Africa has one of the highest per capita rates of alcohol consumption in the world (Eaton et al., 2014; Parry, 2010; Parry et al., 2005; Rehm et al., 2003). The prevalence of risky or problematic drinking, coupled with the high incidence of alcohol-related harms in the country, has become so significant that alcohol now represents a “kind of disaster” to South African public health (Herrick, 2012).
This catastrophic framing around alcohol abuse is paralleled by the designation of GBV and intimate femicide as a “national emergency” issued by South African President Cyril Ramaphosa in November 2018 (Madisa, 2019). When considering the co-occurring crises of problematic drinking and IPV, it is important to foreground how the mundane aspects of everyday life help to illustrate the nuances of how IPV is experienced by South African women. Although the prosaic may appear at odds with the spectacular framing of emergency, the ordinariness of drinking must be contextually understood in order to complicate overly deterministic assessments blaming high rates of violence solely on South African drinking habits. Ethnographies of the particular (Abu-Lughod, 1991), in this context, serve to elaborate on the historical, political, economic, cultural, and interpersonal processes that play out in the homes where these disasters are felt most acutely.
This article seeks to situate and investigate the complex and internecine relationship between alcohol use and IPV in the South African context by drawing upon ethnographic research conducted with women in Soweto between 2012 and 2017. These women were interviewed about lifetime exposures to violence and adverse experiences, providing integrated narratives of childhood upbringing, intimate partnerships, domestic conflict, township violence, and substance use. The illustrative life histories offered by these women allow for a critical engagement with the social and political ecologies of substance use and GBV in the country. By drawing upon the personal to elucidate trenchant historical and structural productions of suffering, we can better understand the occurrence of heavy drinking among certain populations, and the conditions in which violence between partners is routinized and expected as everyday, ongoing disasters.
Social and Political Ecologies of Alcohol and Violence
The sentiment of “alcohol-as-disaster” (Herrick, 2012) in South Africa can be attributed to having one of the highest alcohol consumption rates per capita in the world (Eaton et al., 2014; Parry, 2010). In the 2016 Demographic and Health Survey, 25%–35% of men demonstrated behaviors related to risky drinking, and 11%–18% of men engaged in what would be considered problem drinking (Department of Health, 2016). Although these numbers represent a small proportion of the South African population, evidence suggests that “a relatively large proportion of those who drink appear to engage in risky drinking regularly” (Smit, 2014, p. 16). Drinking patterns among South African men are characterized by periods of heavy episodic drinking (Eaton et al., 2014; Herrick, 2012). Women demonstrate fewer symptoms of alcohol-related problems (Willliams et al., 2019), but a 2014 study found that 19% of women in townships reported weekly binge drinking (Eaton et al., 2014). Most scholarship and policy initiatives around substance use in the country target local shebeens or taverns (Parry, 2010; Smit, 2014; Wojcicki, 2002), but research suggests that 59.9% of heavy drinking occurs in homes, followed by pubs (15.3%), nightclubs (2.2%), and restaurants (1.1%) (Tragenstein et al., 2018). These dynamics of drinking within the home—where getting drunk is more easily hidden—are important to consider given that home is often where IPV takes place.
A great deal of epidemiological research has shown associations between alcohol abuse and injuries related to IPV, as well as intimate femicide in the country (Seedat et al., 2009). Dunkle et al. (2006) found that South African men who report being violent toward their intimate partners are also more likely to drink heavily. Other studies indicate that men who abuse alcohol report more behaviors associated with IPV (Abrahams et al., 2006). Women who have experienced abuse from male partners are also more likely to endure harmful psychological effects which may lead to later unhealthy drinking habits or increased vulnerability to future incidents of violence (Pitpitan et al., 2012). Despite this, the epidemiological literature on the relationship between IPV and alcohol abuse is often framed around discourses of risk and vulnerability, a language of social determinants (Yates-Doerr, 2020) that needs to be complicated by a less linear and prescriptive model of victim and perpetrator.
Anthropological studies of substance use and addiction seek to complicate pathological framings of alcohol, foregrounding the historical and structural milieu within which alcohol and drinking patterns draw their meaning (Raikhel & Garriott, 2013). Rather than reducing alcoholism or substance dependency to psychological determinism or the pathological failure of individuals, a political-economic approach to drinking interrogates the creation of a market for alcohol, the connections between drinking and capitalist forms of labor, and the social fields in which heavy drinking has come to be synonymous with more masculine forms of identity (M. Singer et al., 1992). This political-economic approach is salient in the South African context, where policies around alcohol control, restriction, and controlled consumption were strategically employed as a tactic of social control and suppression since the early Dutch and British colonial settlements of the Cape (Crush & Ambler, 1992).
Scholars of GBV similarly emphasize an ecological approach in understanding the drivers of violence and vulnerabilities of certain individuals and populations to violence (Heise, 1998). This integrated model considers not only the personal history of a survivor or a perpetrator of violence, but also the cultural context in which they are raised, the customary and formal legal system undergirding a social system of justice, and the political-economic context in which interpersonal violence occurs (Heise, 1998). The interplay between GBV and alcohol consumption, therefore, must be situated within the political-economic and cultural frameworks of South African constructions of hegemonic masculinity, particularly one in which violence against women is deemed an appropriate and acceptable strategy to reassert male power (Jewkes et al., 2011; Morrell et al., 2012). Such power is enacted in two critical ways: situational couple violence (Johnson, 2008)—where violence occurs after alcohol consumption, leading to aggressiveness and fights—and coercive controlling violence (Stark, 2009), where alcohol consumption and violence co-occur, which is the primary focus of this article.
Discussions of hegemonic masculinity in the country similarly situate contemporary manifestations of violence and binge drinking (coercive control) in the changes precipitated by the layered histories of colonialism, apartheid, and postapartheid liberalism. South African scholars often describe the conditions of apartheid as emasculating (Hunter, 2010; Morrell et al., 2012), having stripped away crucial elements of men's ability to serve as patriarchs and breadwinners for their family, a domestic role perceived as central to one's identity as a respectable man. The apartheid system essentially treated Black and colored South Africans as minors, politically undermining the basic human rights of innumerable South African citizens, while state agents employed violence to demonstrate absolute control over bodily autonomy of their subjects (Moffett, 2009). In the process of postapartheid reconciliation, therefore, scholars argue that South African men have struggled to reclaim power and dignity, particularly given the widespread unemployment and poverty that still impact broad swaths of the population (Hunter, 2010; Wood et al., 2008). In the absence of economic or political enfranchisement, some men have sought to reassert their power through the use of violence, disciplining wives and intimate partners through coercive controlling violence to reinforce a gendered hierarchy of power (Jewkes et al., 2011; Posel, 2005).
Within this hierarchy, women are often expected to be passive, deferring to partners or husbands and attending to domestic duties like cooking and cleaning (Gqola, 2007). If women speak out of turn or contradict their partner's authority, violence is perceived to be justified (Wood et al., 2008). Within this ecology of attitudes and cultural mores around violence, alcohol can exacerbate conflicts between intimate partners, or, as Hunter (2010) puts it, “bestows courage and sometimes leads to violence. […] This dialectic of men's power and failures—one that becomes embodied through the physiological changes from alcohol consumption—is an important entry point into modern masculinities” (p. 158). In other words, societal beliefs around masculinity and aggressive behavior can lead to the use of alcohol as preparation for involvement in violence, or as a way of excusing violent acts. From this vantage point, alcohol can inflame preexisting patterns of abusive behavior which are reinforced by community perceptions about the “acceptability” of violence. This may include situational couple violence (abuse after drinking) or coercive behavior through and in drinking, which then becomes patterned.
But blaming alcohol for violence only further pathologizes drinking behaviors patterned by deep histories of exploitation, with few opportunities for relief. News reports circulated after the end of the alcohol ban instituted during the 2020 coronavirus lockdown blamed so-called “GBV hotspots” around the country on a return to previous drinking habits (Head, 2020; Vetten, 2020). This proposition presumes a unidirectional, determinative relationship between alcohol and violence, without addressing the syndemic drivers that undergird the two (Singer & Clair, 2003). The syndemic model moves beyond a model of co-morbidity or single causation to instead posit “synergistically interacting epidemics” (Hatcher et al., 2019, 4), which account for the biological, social, structural, and ecological conditions that produce co-occurring and mutually evolving diseases in certain populations. The SAVA syndemic (substance abuse, violence, and human immunodeficiency virus [HIV]/acquired immunodeficiency syndrome [AIDS]), which reflects both victimization and perpetration in the South African context, including the relationship between violence and alcohol intake among heterosexual men (Hatcher et al., 2019), has been particularly effective in the South African context in reframing public health understandings of risk and “responsibility” around drinking. This biosocial approach (Singer et al., 2017) takes the health effects of social inequity seriously while attending to historically and culturally embedded gender roles in disease vulnerabilities and outcomes, although greater care is needed in considering pathogenic framings of violence in the postcolonial context (Boonzaier, 2017; Sangaramoorthy & Benton, 2021). A gendered syndemic model also complicates binaries of chronic and crisis (Manderson & Smith-Morris, 2010), co-implicating the accumulation of slow violence with the more readily visible incidents of spectacular violence that disrupt everyday life (Nixon, 2011; Thomas, 2011).
Employing this ecological, syndemic approach to IPV and substance use serves to couch the two phenomena within contextual understandings of the dynamics of localized drinking culture, beliefs about gender roles, and the permissiveness of violence in particular relationships; systems of structural violence which may shape behaviors around pleasure drinking and intimate relationships; and historical trends that inform these patterns (Morrell et al., 2012). If violence is a communicative strategy employed to reiterate and stage someone's power over another, then drinking too communicates deeper social, economic, and biological needs that are not being met elsewhere. How alcohol use and IPV interact and speak to one another demands additional interrogation, particularly to contextualize the different kinds of IPV an individual might experience; how people respond to and make sense of violence in their day-to-day lives; and the local etiological frameworks marshalled to explain the relationship between IPV and alcohol use in the home.
Methods
This project involves 77 life history narratives from women who spent most of their lives in Soweto, a racially segregated township in Johannesburg, South Africa, where >1 million people reside. This project is nested within two longstanding cohort studies, including one associated with families over generations and another with breast cancer over the past decade. The 77 life stories analyzed here focus on the complex ways in which women remember, tell, and experience life through illness, specifically type 2 diabetes and breast cancer; the recruitment methods have been described in detail elsewhere (see Mendenhall & Norris, 2015; Mendenhall et al., 2019). In both projects, we called women eligible for our study who were already enrolled in the cohort studies; those who were available during our study period window met with us at our research center at Chris Hani Baragwanath Hospital in Soweto, where they routinely seek care and engage in other biological or treatment studies. We paid women for their transport (R150, around US$10), and provided separate consent forms for these studies, linked to approved reviews by the University of the Witwatersrand Ethics Committee.
Qualitative Data Analysis
Interviews were conducted in languages common in Soweto, and sometimes in multiple languages within one interview. All interviews and fieldnotes were transcribed verbatim into English, and interviews conducted in Zulu, Xhosa, Tswana, and Sotho were translated to English. Both studies involved 2–3 life history narrative interviews plus surveys about demographics and social history. The second and third authors had designed a codebook, applied codes, and analyzed the narratives for previous projects. For this project, we started with a new codebook to consider how women spoke about alcohol abuse and abuse linked to alcohol. The research team used a grounded theory approach to code the interviews, putting ideas like the relationship between love and violence in conversation with preexisting literature (Wood et al., 2008) to ensure an emic model of inductive analysis. The first author read through the field notes and transcripts to design a new codebook, with specific codes and definitions, which she talked through with the other authors. Then she developed the initial codebook, which was reviewed and independently confirmed by the second and last authors. In identifying and assessing the relationship between alcohol and IPV in South Africa, we realized that this dynamic was critical and common. Individuals were asked broadly about their experiences of violence within their lifetime and the relationships they found to be most rewarding or detrimental to their own sense of flourishing. The interviews illustrate self-reported experiences of violence, women's relationships with their husbands or intimate partners, exposure to violence during childhood and/or within the community, and perceptions on the role that alcohol plays in contributing to or inflaming dangerous domestic altercations.
The first author used the revised codebook to identify key themes across the 77 interviews, including different forms of violence interlocutors experienced over their life-course; support systems and coping strategies employed to manage periods of injury or hardship; and the impacts the experiences of violence had on the participants. Within the 16 primary codes developed to analyze the interview data, the category of abuse was broken into several sub-codes to document that different forms of abuse interlocutors identified in their lives. These sub-codes included sexual, physical, emotional, parental, and secondary abuse. Additional codes were added to the category of abuse based on the terminology interlocutors used to describe their experiences, including bullying and harassment. Codes for substance abuse, infidelity, and financial issues were included to identify self-reported intersections between drinking patterns, interpersonal conflict, and economic troubles to illuminate the various contours of what counts as IPV. Transcripts were subsequently coded in MAX QDA, allowing the research team to identify associations and patterns between codes, including links between mentions of a current or former husband or partner, abuse, stress, and substance use.
Results
Men are abusive too much. Physically and emotionally. They are abusers, sometimes they call you names. “Hey, bitch.” Yeah. Emotionally. “Hey, you bitch. What are you sleeping with, I want you sick.” They never keep quiet. [Zoleka (pseudonym), age 66]
The women in the study cut across multiple generations, from their late 20s to grandmothers in their 60s and 70s (see Table 1). Some elder women shared memories from the apartheid regime under the National Party prior to 1994, while others were part of the “Born Free” generation, having only lived under democracy in South Africa. Educational attainment ranged from no education to secondary education, some women having matriculated or completed tertiary degrees in university or through technical schools. A large sub-set of women were either unemployed or relied on a pension. South Africa has one of the largest social welfare grant systems in the world (Ferguson, 2015), including Child Support Grants and old-age pensions, grants many of the respondents used to supplement wages earned by family members, partners, or themselves through casual labor or contract work. However, the grant and income from casual labor were said to be insufficient, given that most households were not only poorer but also larger in size (Burns et al., 2005). Indeed, many women lived with extended family members, including adult children and school-aged grandchildren, who often required attention and caregiving. As part of ongoing cohort studies regarding breast cancer, chronic diseases, and mental illness (Bosire et al., 2020; Kim et al., 2019; Mendenhall, 2015; Mendenhall et al., 2019), experiences of violence were discussed in reference to comorbidities of depression, hypertension, cancer treatment, and antiretroviral therapy.
Demographics of Study Participants.
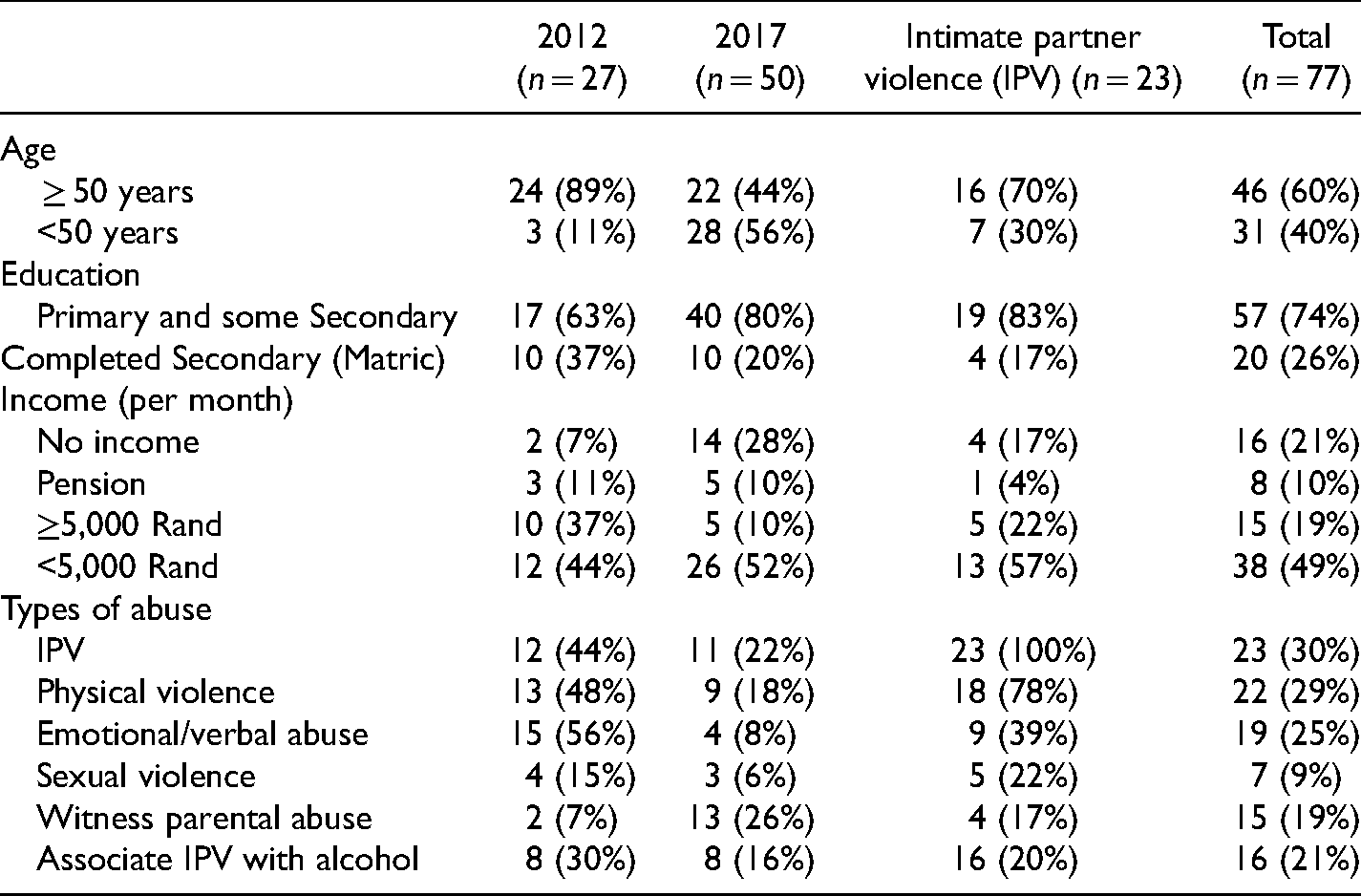
Findings from this study show that IPV was a major form of stress in many women's lives, despite overlapping chronic health concerns, caregiving responsibilities, and desperate financial circumstances. In total, 30% of the respondents reported having experienced IPV within their lifetime, with most of this violence exemplifying a coercive nature (synergistic abuse with drinking), and others situational couple violence (abuse after drinking). Within the sub-set of self-reported survivors of IPV (n = 23), 78% report having experienced physical violence—which could include beating, hitting, or choking—and 39% report having experienced emotional and/or verbal abuse from their current or former partner. In total, 17% mentioned having witnessed parental abuse growing up, or having a relative with an abusive partner. Alcohol use by an intimate partner, or an abusive family member, was a consistent through-line in women's testimonies, sometimes as a contributing factor to physical violence and infidelity and, in other instances, a habit that depleted the financial resources of families, constituting a form of economic abuse. In what follows, we detail the kinds of IPV participants described and the relationship between abusive partners and problematic drinking reported in their narratives.
Women's Experiences of Abuse
Women reported multiple dimensions of IPV, including physical violence, sexual violence, and emotional abuse. Some women described their husbands or partners as “bullies” who controlled their movements—including when, how, and to whom they were permitted to talk, a form of coercive control common in domestic violence. Women often linked episodes of physical violence to their perceived failures to carry out cooking or cleaning duties within the home, responsibilities wives and girlfriends are expected to perform. Verbal fights might escalate into physical altercations, bouts sometimes broken up or mitigated by the presence of children. Regular insults or negative comments were deemed as equally detrimental and damaging as physical violence. In the words of one woman, “So it is abuse even someone calls you names. My partner, he was abusing, he was stressing me too much. I was always crying.” In a comparative study of IPV in South Africa and Rwanda, researchers found that emotional IPV was one of the most common forms of violence in acrimonious domestic partnerships (Stern et al., 2019). Emotional IPV has also been linked to depression, fear, anxiety, compromised self-esteem, and even suicidal ideation among survivors (Gibbs et al., 2018; Stern et al., 2019), consequences less visible than physical violence but nonetheless harmful.
Gendered hierarchies of power and domestic duty also extended into instances of sexual coercion. One woman, Lerato, struggling with breast cancer (Bosire et al., 2020), was distressed by her husband's demand for sex, despite feeling ill: I was stressed because my partner, he sees that I’m sick but he still wants sex. I don't complain, he's a man, he won't be able to not have it, but it's not fair that he can see me struggling but still want sex, which means in other words, if I say I don't want to, he thinks he can go have sex elsewhere. The worst part this person will tell you, “You’re only sick at the top, not the bottom.”
This exchange elaborates multiple discourses about sexual privilege and access through her feelings of powerlessness to negotiate alternative sexual boundaries. Ongoing consent is presumed as part of their preexisting sexual relationship, and the threat of infidelity—complicated by concerns that unprotected sex outside their partnership could lead to HIV—is employed to prevent her ability to decline sex. IPV, thus, is not simply stochastic incidents of abuse or harassment within the home, but represents a totalizing system of psychological manipulation, emotional control, and physical intimidation, encompassing what some have referred to as intimate terrorism (Johnson, 2008).
Alcohol and IPV
Among those who reported having experienced violence from a current or former intimate partner, 70% attribute the violence to the man's alcohol consumption (coercive violence). In this context, alcohol drinking and violence often co-occurred in temporally patterned ways: the week was more peaceful, but once a paycheck was cashed and the weekend arrived, drinking was likely to ensue. As one woman described the pattern: “My husband, there was this thing that after he drank, when he comes into the house, we have to fight, the children cry and we have to fight, he would make a noise and he would hit me and I must leave the house running.” Another woman described similar circumstances, how her husband would come home from drinking and beat her, sometimes threatening the children. One night of violence after drinking was so severe, he knocked out her teeth. A woman with a husband who drank regularly related the story of losing two pregnancies to abuse, no longer capable of conceiving as a result: “My former husband abused me a lot. He used [to] hit me and he went on to hit me even when I was pregnant and that caused me to lose my two kids, a boy and a girl, as they were both born with fits and they didn't make it.” Other studies have indicated the increased vulnerabilities of pregnant women to violence within the home (Peltzer et al., 2013a; Shamu et al., 2011), with one study indicating that >20% of South African women have experienced a form of IPV during pregnancy (Groves et al., 2015). This woman's narrative similarly indicates that the abuse she suffered at the hands of her partner not only impacted her own reproductive capacities—a form of reproductive violence (see Fanslow, 2017)—but also contributed to the demise of their children. Even though she left her abusive partner, the violent consequences were felt within her body and impeded her ability to become a mother again.
Intergenerational Abuse
Several women who reported experiencing or witnessing violence as children connected this violence to their father's drinking habits. When asked to describe the most stressful experiences in her life, a respondent immediately discussed her experiences growing up: “The stress which I had from childhood was from my father because my father was drinking too much. He used to beat my mother a lot, so we were stressed. We would be stressed about how the weekend will end because he would always fight my mother.” Yet, participants did not necessarily link this to coercive control, but rather to situational couple violence which arose in the context of disagreements or arguments that escalated to physical violence. Research on GBV indicates that exposure to childhood violence increases the likelihood of victimization and perpetration of violence as an adult (Dunkle & Decker, 2013; Jewkes, 2013). Children raised in households where parents frequently fight to resolve arguments grow up with a particular model of domestic partnerships, one they might carry into their own intimate relationships as adults. Violence between a couple might be perceived as more acceptable because of these early life experiences, and women may be more likely to tolerate violence as adults because it was normalized in their childhood home. On the subject of violence within the home, one woman spoke at length about the consequences of growing up in a violent household: “I found that, because of lack of love, I was not loving. It's difficult for me to love someone because it's difficult to give something that you did not receive, that you don't have. I didn't grow in a loving environment, so it's difficult for me to love. To give love.” This woman related the absence of a caring childhood environment to her difficulty finding loving and supportive relationships as an adult, both romantically and platonically.
Witnessing parental abuse would sometimes escalate into threats against the life of their mothers. One woman, relating the frequency of her parents’ fights growing up, described, “he always wanted to fight my mother and wanted to kill her. At some point he came with his friend with knives, they just wanted to kill my mother.” Another described how her father killed her mother. The relationship was so rancorous that before she was killed, her mother requested not to be buried next to her husband. This experience affected current relationships as some of the women reported fear that they would be killed by a current or former intimate partner. For example, one woman reported her partner to the police when she was afraid he would kill her. Yet, many expressed mistrust of the criminal justice system, or stated that the police failed to protect them as they would hope or anticipated: “Always when we fight he chokes me, always when he hits me he chokes me and tells me he wants to kill me, he says he isn't afraid of jail.” Another woman lamented, “I was afraid to call the police because he would chase me home. I was even not working, even not earning anything. I was depending on him. That's why he was abusing me.” In this case, the woman was afraid that reporting to the police might lead to other consequences such as homelessness, which seemed more pressing than the daily abuse.
The relationship between IPV, substance abuse, and intimate femicide has been an area of concern in the country since the turn of the 21st century. The Medical Research Council (MRC) has undertaken studies to understand the role of alcohol in intimate femicide (Abrahams et al., 2013), showing that blood alcohol content is often higher for all causes of death, with the exception of gun homicide, and that those who killed intimate partners were often very drunk compared to those who killed non-intimate partners (Mathews et al., 2009, p. 323). Respondents also related stories of friends or family members with abusive partners who drank regularly. These narratives were situated within broader descriptions of violence within the community such as local gangs, youth who consumed alcohol and drugs, and proximity to shebeens.
Infidelity and Perceptions of Abuse
When discussing the harms associated with alcohol use by their partners, many women discussed the sense of hurt caused by their husband or partner's infidelity. As one woman put it, “He was abusing me with his girlfriends,” while another related, “He tormented me emotionally as he had affairs,” often bringing his mistress to the house after a night of drinking. Some partners outside of the marriage were seen as threatening the women's housing security, fearful that they might be kicked out of their homes and replaced by a new partner.
The perception that infidelity might constitute its own form of abuse—following the emic accounts of the female interlocutors—is important given the context and history of multiple, concurrent partnerships in South Africa. It's considered common for a South African man to have several sexual and romantic partners, even if he is legally married. Descriptions of hegemonic masculinity in the country often emphasize that the number of one's partners is seen to reflect someone's “manliness” and “success” (Hunter, 2010; Morrell et al., 2012).
On the other hand, men might accuse their partners of infidelity, an allegation they could use to justify a punitive form of violence for the woman's alleged transgressions. One woman described her case saying, “He hits me, he says he wants to kill me. I say, ‘kill me for what’ and he says because of other men and I tell him, how can I engage other men when I don't even go outside, when will I see these men? I’m always at home, he's the one in the streets.” Her partner's unwarranted suspicion that she might be sleeping with other men is employed as the rationale for his abusive behavior. Unlike the prestige for men of having multiple sexual partnerships, women do not necessarily gain social capital for engaging in multiple relationships. In fact, women might be accused of being “bad” or “loose” for the same behavior encouraged for men (Ross, 2010; Wojcicki, 2002; Wood et al., 2008). Despite the presumed normativity of multiple, concurrent partnerships for men, our participants' responses indicate infidelity is not necessarily tolerated.
Coping and Protective Strategies
From the start I was fighting to survive. I am still fighting to survive. (Karabo, age 44)
Not every woman experiencing violence necessarily left the relationship or moved out of the abusive home. Some displayed a form of acceptance of their situations and stayed because their partner provided them with consistent and stable housing, an option not necessarily available on their own. One woman, whose partner has since passed away, related, “I stayed because I was married and I had children with him. My children would at times try to stop him from hitting me. […] People had even advised me to divorce him, but I couldn't because I did not even have a house.” Affordable housing in South Africa, although promised as a central political priority by Nelson Mandela, has yet to materialize, leaving many to create their own homes in informal settlements and squatter camps, or find housing in the already crowded homes of friends or family members (Ross, 2010). Even emergency shelters for women in the country offer limited options—some will not admit women with children; others only provide housing for 14 days; and many shelters are under-resourced and over-crowded (Lopes et al., 2018).
Other women experiencing violence might choose to stay with partners out of fear of community judgment or stigma. One woman discussed how she and her partner separated but continued to reside in the same home: “I tried to bear it so that people wouldn't see what was happening. And staying together, so that no one would know.” The concern of how the neighbors might criticize her relationship served as a form of social discipline to continue to perform happy domesticity with her abuser. A widow, whose husband drank heavily and frequently beat her (situational couple violence), she chose to stay in the marriage until her partner passed away: “I could not leave him because traditionally a woman is not expected to run away from her marriage no matter how difficult it is.” Alternatively, some went to their neighbors, eager to see if they might intervene on her behalf. Often, these women did not find allies in their neighbors, as some neighbors feared for their own safety if they attempted to help.
Some women describe taking more punitive measures to prevent their partners from abusing them. Several sought help from the police in the form of protection orders and warrants for arrest. Yet, seeking help from the police rarely provided the anticipated results. The police in South Africa are widely mistrusted or deemed ineffectual (Fry, 2013). Although some evidence suggests that individuals who file for protection orders have positive outcomes when interfacing with the police (Peltzer et al., 2013b), police responsiveness and sensitivity to survivors’ needs vary drastically by province (GHJRU, 2014).
Seeking police assistance can also exacerbate preexisting tensions within the home, especially if the gambit to get the police involved fails to result in an arrest or adequate protections for the survivor. In some instances, the woman expressed that she was afraid to call the police; in these cases, fear of potential financial retribution contributed to a women's experience of entrapment. The feminization of poverty in South Africa (Bentley, 2004) is complicated by expectations in heterosexual relationships that men provide money, gifts, and other commodities as demonstrations of their love and affection (Moore et al., 2007; Posel, 2005). One way of addressing IPV as evidenced in these cases is through creating opportunities for women's financial independence. Although protection through the police represents a temporary solution to violence within the home, the criminal justice system does not address the economic drivers that might keep a woman in an abusive relationship if the relationship is financially reliable. On the other hand, abusive partners might spend the limited money they have on alcohol, jeopardizing basic needs like food and electricity. The monetary decisions around alcohol consumption, rather than the physical, emotional, or sexual abuse in these scenarios, could then be the precipitating factor that leads a woman to leave.
Situating Abuse in “Stress” Narratives
Collecting stories around GBV is historically challenging for a number of ethical and cultural reasons. Research guides advising best practices for qualitative or quantitative studies around violence recommend asking questions about behavior, rather than whether or not someone has experienced IPV (Backe, 2020; Garcia-Moreno, 2001). This approach is informed by the recognition that labels like domestic violence and martial rape may not be appropriate in certain cultural contexts (Mulla & Hlavka, 2011).
In order to address these social and linguistic variants, we asked respondents to identify stressful relationships in their lives. Oftentimes, this discussion of stress was the entry point during which respondents would articulate a troubled and violent relationship with a partner. In fact, when some respondents were asked whether or not they had experienced abuse, they initially said no, only to then go on and explain periods of bullying, harassment, verbal abuse, beating, and financial exploitation by their partners when prompted by the follow-up question of stress. Considering the complexities around asking women to disclose experiences of abuse, stress, and stressful relationships might be a more salient approach to collecting data on IPV.
Many of the women, even those who did not relay experiencing abuse or violence, identified relationships with current or former partners as the most stressful. This stress was articulated in a number of ways. Some women discussed the stress of economic uncertainty, financial loss, or the absence of monetary support provided by their partners. Others articulated the stress of domestic demands placed upon them by their partners, such as childcare. One woman related, “My partner, he was abusing, he was stressing me too much. I was always crying and I wasn't the cause with them. I was cleaning for them, I was cooking for them and doing everything I was supposed to be doing.” Part of the stress, in this situation, emerged from the fact that although she was abiding by traditional domestic expectations—what Gqola refers to as the “cult of femininity” (2007)—she was still subject to abuse within the home.
Here, we might consider the cultural scripts around “acceptable” and “unacceptable” violence, the idea that certain South African men are permitted to hit and “discipline” wives and partners if they do not fulfill domestic duties or defer to the male patriarch (Morrell et al., 2012). In this case, the respondent experiences stress because she is subjected to abuse, despite the fact that she abides by these cultural guidelines. This sentiment, however, serves to complicate other cultural narratives which depict violence as an expression of love in intimate relationships (Wood et al., 2008). In an ethnographic study of young South African relationships, youth portrayed beating as a demonstration of a partner's affection, that “showing roughness in a beautiful way” proved a man's commitment to the strength of the intimate relationship (Wood et al., 2008). The “stress” associated with these intimate partnerships, however, seems to indicate that coercion and sexual violence are less readily taken up as expressions of love. Indeed, one woman directly rejected her husband's violence: “I also asked him how he could beat me up if he said that he loved me and I was precious to him. I told him that that was no way to treat the one that you love.”
Breaking the Cycle
Several programs in South Africa have attempted to break cycles of alcohol abuse and IPV among men. A study of the One Man Can program implemented by Sonke Gender Justice demonstrated reduced alcohol intake and more healthy relationship dynamics among participants (Hatcher et al., 2014). Other studies of Stepping Stones similarly demonstrated positive associations between reduced alcohol consumption and decreases in violence (Gibbs et al., 2015). Evaluations note, however, that while some participants decided to reduce their alcohol consumption, drinking habits are difficult to adjust if friends and family maintain unhealthy drinking patterns. Hence, communities are crucial in enabling risky drinking or assisting with sobriety.
Moreover, little is known about the relationship between IPV and drinking as a coping mechanism for women at home—what is referred to as secret or “kitchen cupboard drinking” (Pretorius et al., 2009). Only seven of the women interviewed discussed drinking alcohol, which was often associated with coping with a husband's abuse. Women who frequent shebeens or drink publicly face moral approbation, so the low response rate could be attributed to concerns about stigma. Yet, previous research indicates that drinking might be used as a coping mechanism for violence, or as the result of trauma (Pitpitan et al., 2012). Indeed, one of the women discussed using alcohol to deal with her husband's abuse: “He was a very jealous guy—he would hit me just because I spoke to another male. He abused me a lot. I had to break up with him just to stay sane. In the interim, I turned to alcohol for comfort.” The urgency of IPV and alcohol abuse was renewed in March 2020 when the coronavirus crisis emerged in South Africa. Although alcohol was banned throughout the country during the height of the COVID-19 pandemic, home brewing practices soared (The Economist, 2020), and rates of violence in the home escalated. The lengths to which South Africans went to access alcohol under strict abstinence regulations suggests a much deeper, more complicated relationship with alcohol dependency, pleasure drinking, and abuse, one that needs to be treated with compassion and nuance.
Limitations
The key limitation to this article is that it draws its conclusion from ethnographic narratives from women living in Soweto while excluding men's perceptions on the high rates of violence and alcohol consumption in South Africa. Around 19% of women in townships reported weekly binge drinking (Eaton et al., 2014) and seven of our participants reported drinking alcohol, which may lead to some violence toward men or children. In addition, we focused on narratives from Soweto, a township in Johannesburg; this geographic context excises what happens in rural areas as alcohol drinking is reported in all provinces in South Africa. Future studies should look into these issues.
Conclusion
Rather than pathologizing drinking as a “social ill” (see Grobler, 2020), and treating domestic violence as a disease ameliorated primarily through medical interventions (Ticktin, 2011), we would do better to consider Arundhati Roy's provocation of the “pandemic as portal” (2020), revealing the historically grounded structural inequities and socialized suffering laid bare by the coronavirus. Although domestic violence has been declared a national emergency and a “shadow pandemic” within South Africa (Mlambo-Ngcuka, 2020), the language of emergency does not do justice to the routinized ways that IPV is tacitly condoned, overlooked, and even tolerated by the South African criminal justice system. Survivors’ accounts in this study evidence the disputes over childcare, domestic duties, interpersonal jealousy, and money that often contribute to and ignite violence within the home. Alcohol provides a permissive structure to violence, conditions detrimental to women's financial, emotional, and physical well-being. Yet, even in scenarios where their abusive partners did not drink, the women often felt incapable of fighting back or seeking alternative means of protection or remediation.
Nor does a discourse of emergency, which tends to elevate temporary fixes and short-term solutions (Abramowitz & Panter-Brick, 2015), address the sedimented ways in which colonial oppression, apartheid repression, institutional racism, structural violence, and economic dispossession contribute to both drinking patterns and expressions of violence meant to reassert masculine power. We must “overcome the tyranny of the urgent” (Smith, 2019) if we are to address the chronicity of violence within the home, as well as the proverbial “crisis of masculinity” driving problematic drinking habits among men who still struggle to access the affordances of democracy including stable work, sufficient economic income, and a sense of political efficacy. Although an emergency valence lends a sense of exigency to prevention and response initiatives, both IPV and alcohol abuse emerge from routinized, every day, and seemingly mundane struggles to make ends meet and fight to survive. It is only through a “descent into the ordinary” (Ndebele, 1986) through the very narratives of everyday life offered by the women of this study that we can begin to tackle the common and compounding structures of violence that suffuse conditions of survival, coping, and escape.
Footnotes
Acknowledgments
We would like to thank the following colleagues at the University of the Witswatersrand Developmental Pathways for Health Research Unit for support with the projects included in this analysis: Shane Norris, Hunadi Shawa, Meikie Hlalele, Phindile Mathe, Brooke Bocast, Nontlantla Mkwanazi, Victor Shandukani, Thandi Ma Sbong, Andrew Kim, Maureen Joffe, and Herman Cubasch.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding from the MRC/DFID African Research Leader Scheme (UK), the South African Medical Research Council, and the School of Foreign Service Summer Academic Grant and Provost's Pilot Research Project Grant at Georgetown University.