
Abstract
We explored the challenges and lived experiences of intimate partner violence (IPV) survivors during the COVID-19 pandemic by interviewing 53 U.S.-based IPV advocates between June and November 2020. Advocates described how the COVID-19 pandemic limited survivors’ abilities to meet their basic needs. The pandemic was also described as being used by abusive partners to perpetrate control and has created unique safety and harm reduction challenges. IPV survivors experienced compounding challenges due to structural inequities. IPV must be considered by local, state, and federal governments when developing disaster planning policies and practices, including in the context of pandemics.
Keywords
Introduction
Intimate partner violence (IPV), defined as physical violence, sexual violence, stalking, and psychological aggression by a current or former intimate partner, is a pervasive public health problem impacting one out of three adults in the United States and almost one out of three women who have been in a relationship globally (Breiding et al., 2015; Smith et al., 2018). IPV has myriad negative health and wellbeing impacts on survivors (Campbell, 2002; Miller & McCaw, 2019). IPV exists within a broader context that includes political, social, and environmental influences (Centers for Disease Control and Prevention, 2016). As such, the experience of IPV may be impacted by significant societal events such as infectious disease pandemics and natural disasters. The United Nations Development Program (2015) noted increases in gender-based violence during the 2014–2016 Ebola epidemic in West Africa, an outcome they attributed to increased economic strain on the household and restrictions on movement. Similarly, past studies have demonstrated increases in frequency and severity of IPV after natural disasters that, similar to the 2019 novel SARS-CoV-2 coronavirus disease 2019 (COVID-19) pandemic, may disrupt ongoing social services. For example, a study of 186 women living in a shelter after the 2008 earthquake in Sichuan, China, found that women reported higher rates of IPV for the post-earthquake period than during the year preceding the disaster (Chan & Zhang, 2011). In a study of 123 postpartum women who lived through Hurricane Katrina in 2005 and gave birth in 2006 or 2007, strong associations were found between experiencing storm damage and physical IPV (Harville et al., 2011).
The severity and breadth of the COVID-19 pandemic including impact of shelter-in-place orders in the United States have fueled interest in the intersection between pandemics and IPV. Multiple major journals as well as lay press (e.g., New York Times, National Public Radio, Washington Post) have published articles describing the urgent need to support IPV survivors during the COVID-19 pandemic (Connor et al., 2020; Evans et al., 2020; Ragavan et al., 2020a). The United Nations Secretary-General has emphasized: “Making the prevention and redress of violence against women a key part of national response plans for COVID-19” (United Nations, 2020).
Aligned with these research priorities, studies in the United States and globally have focused on elucidating the prevalence and severity of IPV during the COVID-19 pandemic. Police report data from Los Angeles and Indianapolis showed an increase in IPV reports after shelter-in-place orders while reports of other crime types examined stayed the same or decreased (Mohler et al., 2020). Another study conducted by the Guttmacher Institute from April 30 to May 6, 2020, showed that in a sample of 2,009 cisgender women, 16% had experienced IPV in 2020; one-third of these women indicated having trouble or being unable to seek services in response to the violence they experienced (Lindberg et al., 2020). Globally, similar studies are emerging. For example, a survey of 560 women in India, conducted between May 11 and 18, 2020, showed a 33% increase in IPV since shelter-in-place began (Pattojoshi et al., 2020). A study using 5 years of crime records and 2 years of calls-for-service data from London's Metropolitan Police Service showed an 8.1% increase in abuse by current partners and an 11.4% decrease of abuse by former partners during shelter-in-place (Ivandic et al., 2020). A report by Vision Point (2020) notes increased calls to IPV hotlines in multiple countries, including the United States. These reports suggest IPV continues as a significant public health problem during the COVID-19 pandemic.
Data on the frequency and severity of IPV during the pandemic is important but provides only one perspective on the ways that the COVID-19 pandemic may impact IPV survivors. IPV is often rooted in abusive partners’ assertion of power and control through isolation, threats, abuse, and discrediting of their partners (Dichter et al., 2018). Substance use coercion and reproductive coercion, as well as partner interference with health care and service seeking, are also less well-recognized aspects of IPV (McCloskey et al., 2007; Miller et al., 2010; Ragavan et al., 2020a, 2020b, 2020c). COVID-19 pandemic stressors including loss of employment, limited childcare options, and disruption of social supports may further exacerbate abusive relationships and may create unique opportunities for abusive partners to perpetrate abuse. To date, this is an underexplored aspect of the impact of the pandemic on IPV survivors. Additionally, the COVID-19 pandemic has hindered access to social support services, such as mental health care (Pfefferbaum & North, 2020), resources for survivors living with substance use disorders (Melamed et al., 2020), and basic needs such as housing, food, and transportation.
The COVID-19 pandemic may also create unique challenges for IPV survivors from marginalized and minoritized communities. Decades of literature demonstrate how structural inequities—including racism, xenophobia, poverty, and transphobia—intersect with IPV to create unique challenges for some survivors (Crenshaw, 1991; Sokoloff & Dupont, 2005). For example, poverty disproportionately impacts IPV survivors, and the negative impacts of IPV and poverty compound upon each other. IPV survivors experiencing poverty may also experience more economic abuse and face unique challenges (e.g., housing insecurity), limiting survivors’ ability to seek safety and heal from an abusive relationship (Bybee & Sullivan, 2005; Goodman et al., 2009; Klein et al., 2019). Additionally, concerns about racism and police brutality impact whether IPV survivors feel safe engaging with law enforcement, thus limiting safety planning (Decker et al., 2019; Monterrosa, 2021). Practices and policies rooted in xenophobia and transphobia may further restrict immigrant and gender and sexual minority IPV survivors from accessing resources (Gamarel et al., 2020; Ragavan et al., 2020a, 2020b, 2020c). The interwoven relationships between COVID-19, structural inequities, and IPV can be viewed through the lens of a syndemic framework (Mendenhall, 2017). Syndemics have been used to describe the interaction between diseases and the social, environmental, and economic factors that worsen and amplify intersecting conditions such as IPV, SARS-CoV-2 infection, and health. As a syndemic, the COVID-19 pandemic, structural inequities, and IPV must be addressed concurrently rather than in silos. Little work has used a syndemic framework to examine how IPV survivors from marginalized communities have been impacted by the COVID-19 pandemic.
Existing evidence suggests that IPV survivors, particularly those belonging to marginalized communities, are facing unprecedented challenges during the COVID-19 pandemic. To effectively address the impact of COVID-19 on IPV survivors and inform the provision of prevention and intervention services, it is critical that we better understand the specific ways in which the pandemic may be affecting survivors. The use of qualitative methodologies, which allow for a deep exploration into challenges and lived experiences is a useful strategy to understand survivors’ needs and reality. In particular, interviews with IPV advocates, defined as “anyone who responds directly to help abused women in an institutional context” (Davies et al., 1998, p. 2), provide deep knowledge about IPV (Wood, 2017) and can add information about how the COVID-19 pandemic is impacting IPV survivors, without creating safety concerns inherent in conducting data collection with IPV survivors during a pandemic (UNICEF, 2020). To that end, in this study we performed qualitative interviews with U.S.-based IPV advocates to explore their perspectives on (1) stressors faced by IPV survivors during the COVID-19 pandemic; (2) how IPV survivors kept themselves safe during the pandemic; and (3) unique challenges and protective factors for IPV survivors belonging to marginalized communities.
Methods
Study Design and Study Team
This article describes results from a larger project examining the impact of the COVID-19 pandemic on family violence and related service provision. We conducted semi-structured interviews with U.S.-based IPV advocates. We selected a qualitative approach because our goal was to understand the challenges and lived experiences of IPV survivors during the COVID-19 pandemic. Qualitative methods are ideal for examining complex topics with limited prior research, generating hypotheses, and providing a framework for further quantitative studies (Patton, 2015). We used a generic qualitative inquiry approach, whereby qualitative methods are used to ask open-ended questions to solve problems, improve programs, or develop policies (Patton, 2015). Generic qualitative inquiry was aligned with our goal to examine IPV survivors’ lived experiences to ensure service providers and policy makers provide support to IPV survivors and their families during this and any future pandemics.
The full study team comprised a multi-disciplinary group with unique expertise including four IPV researchers, a representative from the American Academy of Pediatrics, two representatives from the Centers for Disease Control and Prevention, a representative from the violence prevention organization Futures Without Violence, an IPV advocate, and three trained research assistants. We used our diverse team to ensure representation of various concerns and insights, continuously check the process for potential bias, and triangulate interpretation and analysis of the data from multiple expert and experiential perspectives, as described throughout the methods section. The University of Pittsburgh Institutional Review Board approved this study.
Participants
To be included in this study, a participant had to: (1) identify as an IPV advocate as defined above; (2) work directly with IPV survivors as an IPV advocate; (3) be aged 18 or older; and (4) speak and understand English. Participants self-identified as IPV advocates. Participants who did not spend time engaged in direct work with families experiencing IPV (e.g., development or administrative staff) were excluded. We focused on IPV advocates because they have advanced training in responding to IPV and provide direct services to survivors, thus have unique insight into the study topics. We chose to not directly interview IPV survivors due to safety concerns about virtual interviews, particularly for survivors cohabiting with abusive partners.
Participant Recruitment
Participant recruitment occurred through announcements on listservs, word-of-mouth, and networking. Outreach was facilitated by Futures Without Violence, a non-profit organization that is connected to multiple U.S. IPV agencies. Prior to recruitment, we created a sampling matrix to ensure inclusion of IPV advocates who work with marginalized survivor groups including survivors who identify as (1) Black; (2) immigrant and English learner; (3) gender and sexual minority; (4) living with a disability; and (5) Indigenous. We ensured that at least one advocate worked with a majority of IPV survivors from each of the above categories (see Table 1 for the number of advocates recruited from each group). We also sought to sample IPV advocates from various states and purposively included advocates who worked with underrepresented or marginalized populations. We relied heavily on professional networks, especially those of Futures Without Violence, to ensure equitable representation from IPV advocates serving marginalized survivors. Eligible participants emailed or called to set up an interview. Participants were told that this research centered on their experiences working with IPV survivors during the COVID-19 pandemic.
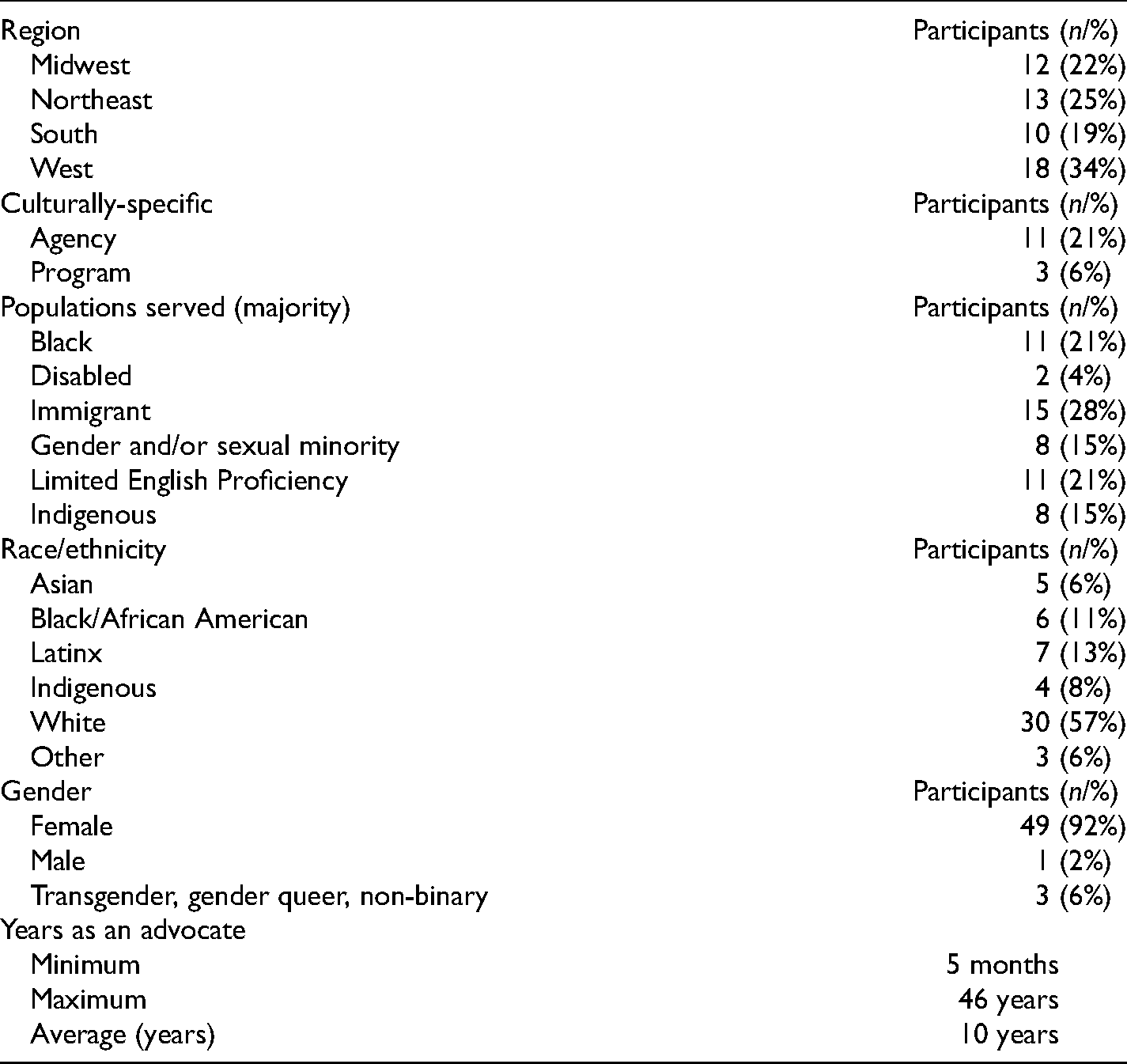
Demographic Characteristics of Intimate Partner Violence Advocates (Total n = 53) Who Participated in Interviews.
Development of the Interview Guide
We developed an interview guide aligned with our research objectives and the Center for Global Development conceptual model of the pathways between pandemics and IPV (Peterman et al., 2020). This model hypothesizes several direct and indirect pathways by which pandemics impact IPV, including (1) poverty-related stress; (2) social isolation; (3) disaster and conflict-related unrest and instability; (4) exposure to exploitative relationships; (5) inability of survivors to temporarily escape partners; (6) violence due to being infected by the virus; (7) reduced health care access; (8) exposure to violence in response efforts; and (9) violence against service workers (Peterman et al., 2020). In this article, we focus on pathways 1 through 6; forthcoming articles will examine the impact of COVID-19 on IPV advocates and agencies.
We asked 12 open-ended questions addressing: (1) specific challenges faced by IPV survivors during the pandemic; (2) how the COVID-19 pandemic was being used to perpetrate violence against IPV survivors; and (3) strategies to keep survivors safe during the pandemic. Aligned with the syndemic framework, we also asked participants about unique challenges and lived experiences of IPV survivors from marginalized communities, particularly those identifying as Black, Indigenous, immigrant, disabled, and gender and sexual minorities. The interview guide was developed by the research team and revised after pilot testing with one IPV advocate.
Data Collection
Virtual interviews were conducted June through November 2020 by a study team member via Zoom. Interviewers were the first author or a research assistant (CH, JT, LR), who had qualitative methods training prior to conducting interviews. Participants provided verbal consent prior to their interview, including a reminder that interviews were confidential. Interviews were audio-recorded, conducted in English, and lasted 45–90 min. The interviewer also obtained advocates’ demographic information including race/ethnicity, gender identity, region of the country, and number of years working at the agency. To identify advocates serving diverse IPV survivor communities, we asked advocates whether they worked with marginalized groups of IPV survivors, as described above, as well as whether they worked at a culturally specific IPV agency (self-identified). Participants received a US$30 gift card after interview completion. Interviews continued until data saturation was reached (i.e., no new themes emerged; Guest et al., 2006) and when the research team recruited at least one advocate who worked with each group of marginalized IPV survivors.
Data Transcription and Analysis
The research team used an inductive, thematic-analysis approach for coding and analysis (Braun & Clarke, 2006). Specifically, the codebook was developed based on participants’ perspectives rather than using a predetermined structure or set of themes. Audio recordings were transcribed verbatim and uploaded into the Dedoose software program (version 7.5.16) to support the organization of codes. The coding team included the first and second authors, as well as an IPV advocate, and two trained research assistants. Two coders independently coded each transcript line by line (Braun & Clarke, 2006; Dedoose, 2016; Patton, 2015), iteratively developing a codebook containing codes and their definitions. A third coder would then review the coding and note all discrepancies. The coding team met weekly, led by the first author, to review the codebook, discussing and resolving each discrepancy to address inter-rater reliability. After coding 25 transcripts, the coding team identified only minimal discrepancies; therefore, we shifted to co-coding every third transcript. The full team met weekly to review emerging codes, make iterative changes to the interview guide, and consolidate codes into themes. Quotes were chosen by the team to include in this article, ensuring that quotes from at least half of the advocates were included to guard against selective use of data.
Our large and multidisciplinary team of researchers, public health practitioners, and representatives from victim services agencies served as a point of triangulation. Representatives from our collaborative partners reflected with the researchers on the data weekly and shared their perspectives on how the emerging data aligned with their lived experiences working on this topic. To further triangulate our emerging data, we held monthly meetings with a group of 25 stakeholders who work at victim services agencies around the United States. Emerging codes and themes were shared with these stakeholders and they helped us shape the results based on their experiences. For example, initially, our safety planning questions were geared more toward safely leaving abusive relationships; the stakeholders reminded our team of the importance of harm reduction strategies used while survivors are cohabiting with abusive partners. We therefore modified the interview guide to better examine the range of harm reduction strategies offered and employed.
Results
We conducted interviews with 53 IPV advocates, working in 25 states in the United States. The majority (84.9% or 45) identified as female. Advocates described a range of racial and ethnic backgrounds including Black (11% or 6), Latinx (13% or 7), Asian (6% or 3), Indigenous (8% or 4), and White (57% or 30). Eleven (21%) advocates stated they worked at a culturally specific agency (self-defined); an additional 3 (6%) worked at a culturally specific program within their agency. Advocates served survivors from a variety of marginalized and minoritized communities. Please see Table 1 for more information about the advocates and the communities they serve.
We identified six major themes expressed by advocates: (1) the COVID-19 pandemic compounds challenges of IPV survivors meeting basic needs; (2) the pandemic is being used by abusive partners to control IPV survivors; (3) COVID-19 pandemic mitigation strategies need to be balanced with trauma-informed practices; (4) harm reduction and safety planning requires adaptation during the COVID-19 pandemic; (5) the COVID-19 pandemic impacts IPV survivors’ mental health, stress, and resilience; and (6) structural inequities and discrimination impact marginalized IPV survivors during the COVID-19 pandemic. While structural inequities relate to every theme, we decided to present them separately to reflect their importance during interviews. Representative quotations are provided throughout the results section.
COVID-19 Compounding Challenges of IPV Survivors Meeting Basic Needs
Advocates described how the COVID-19 pandemic made it difficult for IPV survivors to meet basic needs, which was already a pre-pandemic challenge. Housing was viewed as one of the most pressing challenges, with the pandemic exacerbating difficulties in access to safe and affordable shelter: “I think that one of the biggest things that I've seen is that there were housing barriers and difficulty with housing. Those all were exacerbated because of COVID.” Another advocate noted how even when housing could be secured, it was crowded and created challenges in maintaining needed physical distancing: A couple of my clients were living in another congregant living situation where there were many, many, many, many people living there. Two of them had such high anxieties, they were just saying, “We would rather be homeless on the street than living here.” It was really horrible for them to live in that place. Some people where they were living didn’t take this seriously, so they were not wearing masks in the hallways, still hanging out around the hallways, not taking any precautions. They would call me crying and having anxiety attacks about getting COVID-19.
Advocates also described COVID-19 pandemic-related barriers survivors face when accessing technology, transportation, and employment that enable them to meet basic needs. These new barriers are compounded by pre-existing IPV-related challenges to meeting needs. Accessing technology, particularly cellular phones and Internet, was problematic for many: “There's a lot of technology restraints for families. They didn't have internet at home. They didn't have the capabilities as far as having a cellphone, a laptop, or an iPad.” Childcare challenges were discussed frequently: “A lot of our parents, they still have to go to work because we work with a lot of families that do work in the service industry. Then, it was like the question of who's going to look after the kids.” Additionally, financial stressors, particularly centered on losing employment, plagued survivors, further compounding IPV-related and other pre-pandemic worries and concerns. An advocate explained: “There is the barriers that people are facing with the economic crisis and loss of jobs. I work with women who say, ‘I am juggling work and childcare,' but they’re also juggling an abusive partner or ex-partner and everything else that everyone else is facing. The financial aspect of this has been really challenging on clients.” Another advocate noted how some gender and sexual minority IPV survivors may face unique challenges: “LGBTQ community are folks who are either working in essential jobs or folks who are doing work that requires an audience or to be in person. Some examples, aside from working in the food industry are people working at night clubs, or doing drag shows, or even sex work was something that was hugely impacted.”
The COVID-19 Pandemic is Being Used by Abusive Partners to Control IPV Survivors
Many advocates described how both the health concerns and economic ramifications of the COVID-19 pandemic were used by abusive partners to control IPV survivors. An advocate summed this up by saying: “It’s just about power and control. COVID has given some abusers the power and control and they’re using COVID as part of the controlling mechanism.” Advocates provided various examples including (1) using the pandemic as a way to further isolate IPV survivors, (2) financial abuse, including taking stimulus checks, and (3) purposeful exposure of an IPV survivor to the SARS-CoV-2 virus or limiting access to personal protective equipment (PPE).
The physical distancing required to mitigate the COVID-19 pandemic provides a unique opportunity for abusive partners to isolate IPV survivors and keep them away from their support networks. An advocate described: “A lot of times, the abuser will use quarantine against you and say, ‘You are not allowed to see any of those people. It’s unsafe.'” Another advocate, shared a similar opinion, stating: One thing that we heard a lot in the beginning was partners using COVID in a way to keep the survivor at home, or just saying, “Well, you wouldn’t want to get COVID. You wouldn’t want to expose yourself. You wouldn’t want to expose our child. You can’t leave the house.” That almost just fueled a little bit isolation.
Advocates also noted abusive partners were purposefully exposing IPV survivors to the COVID-19 virus or keeping them from seeking medical care. An advocate shared another perspective, noting how an abusive partner was purposefully not using proper PPE and putting her in danger of contracting the SARS-CoV-2 virus: “He is exposing himself to COVID. He goes out. He doesn’t use masks. He doesn’t use anything. Then he comes back, and he says, ‘I don’t care. You can get sick. I don’t care.’”
Advocates also described how abusive partners were using uncertainty and instability around employment and finances to assert control. One advocate explained what an abusive partner said to one of her clients: “‘You can't go get a job right now. You have to stay here with me, and I'm gonna control the money’. Yeah, it totally impacts people's feelings of autonomy and independence, so further emphasizing the control and lack of options.” A COVID-19-specific form of financial abuse was taking stimulus checks for IPV survivors who were eligible for this resource: “I have a client—her stimulus check, the money for their kids was put right into their joint bank account that she has zero access to. She's still been trying to get her share of the money back.”
COVID-19 Pandemic Mitigation Strategies Need to be Balanced With Trauma-Informed Practices
Some advocates discussed how public health measures that prevent transmission of SARS-CoV-2 may be traumatizing or triggering for IPV survivors. An advocate who works with gender and sexual minority survivors explained: The survivors I work with have experienced a distancing from their families due to being part of the LGBTQ community. I think everyone is experiencing a lot of isolation as an impact of COVID. This can either exacerbate isolation that they’ve already been experiencing, or could put them—for some people, be a re-traumatizing experience where the impacts of COVID have been reminding them of the impacts of abuse that they’ve experienced.
Another advocate noted that regulations from shelters and other residential services may also be traumatizing for IPV survivors: Having precautions put into place, just in case somebody was exposed [to COVID-19] or somebody might get sick … has been a challenge because people don’t want to be that restricted. It’s leaving one jail for another jail, almost. I hate to say it that way, but when you’re told, “Yes, we want you to have a safe place to come, but you can’t leave your bedroom unless you have to go to the bathroom,” it’s very, very hard.
A few advocates also described triggers related to PPE, such as using masks. “A lot of our sexual assault victims said, ‘I feel re-victimized wearing this mask. I am claustrophobic.’” Other advocates described how the disinformation campaigns and disregard of public health guidelines and messages reminded some survivors of manipulation they experienced from their abusers: One thing I’ve noticed survivors experiencing that I think will increase will be … where they’re behaving in a very cautious way [to protect against COVID-19], and then hearing from friends or social media or neighbors, that they don’t have to be so worried. They don’t have to take these precautions, that they should be doing these other things. I think a lot of the survivors I’ve been working with have been experiencing that as—again, like a re-traumatizing experience where they’re reminded of the ways that their abuser would gaslight them.
Harm Reduction and Safety Planning Requires Adaptation During the COVID-19 Pandemic
Advocates described multiple ways that survivors displayed strength, creativity, and resiliency to keep themselves safe during the pandemic. Many described the importance of prioritizing harm reduction to keep IPV survivors safe while they were often forced to co-exist and cohabitate with abusive partners. An advocate explained how they support survivors in finding safe places within their homes: “Talking a lot about how to stay safe in the situation, things like the safest areas of the house to be in. To avoid places with things that could be used as weapons or tools or kitchen things, bathrooms, hard surfaces.”
IPV advocates described the importance of facilitating privacy and security when communicating with IPV survivors, especially when using virtual platforms. Advocates had several ideas for maintaining privacy, including using code words, switching from phone to texting platforms, and providing emergency cellular phones. Some folks still want to speak with us, but we are fully aware they are cohabitating with an abusive person, and so we've needed to be a little more boundaried. Either reducing the amount of time that we're speaking to people or speaking in code or trying to find different times to support them.
Another advocate described several strategies being used: A lot of people that we've been working with, we've given them emergency phones, which are basically old cell phones that you can call 911. A lot of people are talking to their family members about what's going on and giving their family code words or phrases to let them know that they're in danger and need law enforcement, or for their family member to go over. We're definitely having to think out of the box since a lot of people are at home 24/7.
Survivors’ Mental Health, Stress, and Resilience
Advocates described survivors’ mental health challenges, emerging from their experiences of IPV and stress during the COVID-19 pandemic: “Survivors are thinking … if I don't die at the hands of the perpetrator, am I sick with COVID, or will I lose my job? Then they start with all of this other anxiety. We just work with their emotions.” Another advocate expressed a similar opinion, explaining that IPV survivors have always faced stress, but the pandemic has exacerbated it: “Client challenge is something that I’m very used to, but I think that the compounding stress that the pandemic has caused on everyone, it changes the challenges a little bit. It’s been a learning process for sure.” Advocates also reminded us that IPV survivors, like everyone else, were losing loved ones in the pandemic, further compounding their trauma: It's just like trauma on top of trauma. I have had a few clients that have said, “I've had a close family member, or a friend passed from COVID or be very ill with COVID.” That has then just been another barrier and trauma to deal with at this point in time.
Despite the incredible challenges brought by the COVID-19 pandemic, advocates were struck by survivor resilience. An advocate who works with gender and sexual minority survivors described: “There have been so many survivors and members of our community, of our LGBTQ community, who have utilized social media kind of to uplift their situation and be like, ‘Hey, let's crowd source. We all haven’t been impacted equally, so why don’t we share some of our resources?’” Reminding us about the strength of survivors both in the past and during the current pandemic, an advocate explained: “Folks have been surviving for years. They don't need us. We're just here to support and maybe encourage and guide and advocate for. Just reminders that there's nothing inherently wrong with any of us and with our survivors that we work with specifically.”
Structural Inequities Impacting Marginalized Survivors During the COVID-19 Pandemic
A cross-cutting theme that emerged was how structural inequities such as racism, transphobia, xenophobia, and poverty compounded with IPV and the COVID-19 pandemic to create unique challenges for marginalized groups of IPV survivors. Advocates described how racism and related police brutality negatively impact safety planning options for survivors of color. An advocate who works with gender and sexual minority survivors of color said: I think especially when talking about the black trans women that we serve, in combination with COVID and IPV and what's going on in the US right now, we just—we don’t want someone to call our hotline and our first response to be call the police. I think they’ve just been impacted so much because it’s terrifying to interact with the police right now for them. A lot of times it makes the situation worse in multiple ways.
Another advocate shared a similar plan about interactions with law enforcement, noting that these challenges predated the pandemic: Even before the pandemic, survivors who were either women of color, their experiences with regards to navigating even things like safety planning weren’t—there were differences because sometimes it would be like, “It doesn’t feel safe to call the police because last time I called the police, they were very violent to me and really scared my daughter.”
Advocates working with immigrant and limited English proficiency IPV survivors noted barriers rooted in xenophobia, which were particularly challenging for these survivors. An advocate shared how immigrant survivors might be less likely to be able to fulfill their basic needs: “People were still waiting for work authorization. Some people were working under the table at the various South Asian restaurants. When they closed, they found themselves unemployed and could not work, and of course, no access to benefits because they were either working temporarily or for cash jobs.” Another advocate who works with undocumented immigrant IPV survivors noted how abusive partners used immigration abuse to keep survivors from seeking medical care during the pandemic: If folks are undocumented, many times they’re being told [by the abusive partner] … again, we hear this pre-COVID, but I think right now, the fear's a lot greater. Saying, “If you go to the doctor, and you’re not documented, they’re writing down your name and you’re gonna be deported.”
Survivors living in poverty faced numerous struggles, many of which were detailed in the theme related to basic needs. Advocates noted that while poverty has always been a challenge, the COVID-19 pandemic has exacerbated unmet needs: The biggest chunk of our clients living in poverty has just been crushing, soul-crushing for these clients. A lot of them are forced to stay with their abusers out of necessity. A lot of the people that would have been trying to leave during this time [COVID-19 pandemic] have had to stay because they don't have those natural support systems. The amount of people that are having to stay in an unsafe situation because they just don't have the resources to leave right now is sort of horrifying.
A few of the advocates who worked with gender and sexual minority survivors noted similar barriers rooted in homophobia and transphobia. An advocate noted how issues with housing access have been exacerbated for gender and sexual minority survivors: “It's difficult to get into shelters when they're trying to manage COVID and on top of that, we've already had challenges before of getting queer and trans people into shelters. Because of discrimination against trans women and all of those type of things, so yeah, that's another heightened situation.” Another noted that much-needed medical care for trans survivors may be delayed during the pandemic: Specifically, for transgender people who are transitioning, that's an area where some of them have put off things related to their transition, who are really wanting to continue their transition at this point. If COVID cases don’t go down, there may also be long-term impacts of the delays of them proceeding in their medical transition.
An advocate who works with survivors living with disabilities shared a similar perspective: “I think it’s just put a strain on people with disabilities because it’s already difficult for them to access resources. With COVID, it’s like a whole additional layer of difficulties.”
Advocates working with marginalized IPV survivors noted incredible survivor and community-level resilience. An advocate who works with Native Hawaiian survivors described: I can speak for the survivors, the amazing women that I work with, and definitely, for native Hawaiian survivors they are so at one with the land. Such a spiritual people and being able to be at—we’re all supposed to be at home and they’re telling me, “Hey, I planted something and for native the plant, is such an important part of our culture.” It’s amazing that for so many of them, they are finding peace out on the land.
An advocate who works with Indigenous survivors noted community-level perseverance to fight on behalf of murdered Indigenous women even during the pandemic.
We did a drive-through in our community. We decorated our cars and put masks on it, and we asked people to wear red and to just wave to us if they wanted to see us and whatnot. The turn-out for that was just amazing. It’s sad, but it really showed, I think, who we are as a people, and that we come together in that like, “We see you. We see you. We’re here for you. We’re in this together.” I think it just showed the strength of us as a community, and I think that that was really great.
Discussion
The COVID-19 pandemic has resulted in considerable concern about escalation of IPV and the resulting negative impacts. Our results address a critical gap in our current understanding of the impact of an infectious disease pandemic on IPV by examining specific ways that COVID-19 has affected survivors. Our work demonstrates that pre-pandemic challenges faced by IPV survivors, such as isolation and inability to access housing, have been exacerbated by the COVID-19 pandemic and that approaches to IPV safety planning may need to be adjusted during the pandemic. Our findings may inform responses to the ongoing and future pandemics, particularly those requiring physical distancing and shelter-in-place strategies for infectious disease mitigation.
Safety strategies, including safety planning, harm reduction, and engaging informal and formal networks are well described (Parker & Gielen, 2014). Our work demonstrates that similar strategies are being used during the COVID-19 pandemic, although some harm reduction strategies, such as leaving the home and engaging support from friends and family, may be unavailable for some survivors. Advocates described further barriers to safely accessing formal and informal resources due to confidentiality concerns inherent in virtual service delivery. Using technology to control and manipulate survivors is well-documented, particularly monitoring technology use (i.e., email, cellular phones), use of location-based services to track IPV survivors, and cyberbullying (Emezue, 2020; Freed et al., 2017). This study demonstrates the need to consider technology-related abuse and adopt technology-specific safety strategies that facilitate the use of virtual services with IPV survivors.
Our findings suggest that the health and economic ramifications of the COVID-19 pandemic may be used to manipulate IPV survivors. This aligns with an understanding of IPV being rooted in the intent to maintain power and control over the IPV survivor. Our study shows that the COVID-19 pandemic offers unique opportunities for manipulative and controlling behaviors within intimate relationships. Study participants described abusive behaviors that centered on limiting access to health care, threatening to infect a survivor, or challenging a survivor's belief about the need for mitigation strategies such as physical distancing. These findings expand our understanding of how health concerns may be used to extend power and control over an intimate partner. Past literature describes abusive partners controlling survivors’ reproductive choice (i.e., reproductive coercion), manipulating attitudes about and access to HIV medication, and limiting access to health care providers (McCloskey et al., 2007; Miller et al., 2010; Ragavan et al., 2020a, 2020b, 2020c). A novel finding from our study is also how PPE, particularly masks, have exacerbated trauma experienced by IPV survivors; abusive partners may not wear masks, thereby putting survivors at risk, and masks may be difficult to wear for survivors who have experienced certain types of abuse. To our knowledge, past literature has not described how PPE can be used to control and manipulate survivors.
Our findings suggest that the COVID-19 pandemic adds another layer of intersectional challenges for IPV survivors, highlighting how three critical public health problems—IPV, COVID-19, and structural inequities—compound upon each other to create staggering difficulties, aligned with a syndemic framework (Mendenhall, 2017). For example, the COVID-19 pandemic has caused economic devastation globally, creating new opportunities for perpetration of financial abuse, as well as complicating existing barriers for survivors to meet basic needs such as jobs, housing, and technology. Similarly, our study demonstrates how structural racism, transphobia, xenophobia, and poverty have created barriers for marginalized survivors during the COVID-19 pandemic. Unique solutions leveraging survivor resilience and addressing IPV and the COVID-19 pandemic within the context of pre-existing structural inequities are needed to support marginalized IPV survivors.
IPV survivors often experience isolation and loneliness; both have been exacerbated during the COVID-19 pandemic given the critical role of physical distancing in COVID-19 mitigation strategies. Isolation is a well-documented strategy that abusive partners use in perpetrating control and violence (Goodman & Epstein, 2020). This study builds on pre-COVID-19 literature by describing how mandatory stay-at-home orders may be used to further isolate and control IPV survivors. Further, the near-global shelter-in-place orders during the COVID-19 pandemic, with dynamic opening and closing of businesses, schools, and other services, have exacerbated isolation already experienced by IPV survivors. Additionally, advocates noted how regulations, put in place by shelters to mitigate risk of SARS-CoV-2 transmission, further heightened isolation felt by IPV survivors. Although shelters and other residential services are deeply important to promote survivor safety, even pre-pandemic emerging literature demonstrated how confidential shelters create challenges for survivors in maintaining their social support (Goodman & Epstein, 2020; Kulkarni, 2018). Strategies to mitigate survivor isolation that balance the need for privacy and confidentiality (e.g., virtual support groups) are important for pandemic planning, especially when concurrent physical distancing is necessary.
We recognize several limitations to this study. First, we interviewed IPV advocates rather than survivors themselves due to safety concerns with virtual interviews for IPV survivors. Although advocates work with survivors on a daily basis and are aware of challenges they face, future work interviewing survivors is needed to triangulate these findings. Additionally, advocates can only share perspectives about the IPV survivors with whom they interact; therefore, this work likely does not capture the perspectives of IPV survivors who do not engage with IPV advocates. The COVID-19 pandemic has rapidly shifted in the United States from this project's inception in April until the time of manuscript submission. The results primarily focus on advocates’ perspectives about the lived experiences of IPV survivors, rather than strategies and solutions IPV agencies incorporated during the pandemic. Additional work will examine the impact of the COVID-19 pandemic on IPV agencies and review innovative approaches employed by agencies to ensure the continuation of prevention and intervention services during the pandemic. The results we present focus on adult IPV survivors; additional work examining the impact of the pandemic on other populations affected by IPV (e.g., adolescents, children) is needed. Finally, these results are limited to the United States; we appreciate and recognize our colleagues conducting similar work in other countries. Further work is needed to examine the potential global generalizability of findings from this and others’ work.
Implications
This study has implications for both the current COVID-19 pandemic and any future pandemics or natural disasters. Chief among these is the need to support services to address the ways in which the current pandemic compounds pre-pandemic challenges faced by IPV survivors, including isolation and meeting basic needs. Service providers in the health care, legal, child protective services, and other sectors should be aware of the unique challenges and safety needs faced by IPV survivors during the pandemic. For example, if health care teams understand and consider the health impacts of abusive partners’ use of COVID-19 mitigation strategies to control health care access and PPE use, they will be able to better create trauma-informed spaces and support IPV survivors. Health care providers and systems may also consider partnering with IPV agencies to conduct warm handoffs or referrals for IPV survivors needing care. Further, it is critical to consider privacy concerns when providing services virtually as many sectors (e.g., health care, courts, schools) are using virtual technology more frequently. The use of code words and text-based platforms may be important means of ensuring private and confidential virtual service provision in fields such as health care.
Perspectives shared by advocates are also relevant for future pandemics and natural disasters. Addressing IPV can be integrated into disaster planning, particularly when shelter-in-place mandates are necessary. Integrating a trauma-informed approach into disaster planning, including when considering how public health measures (such as PPE) may be triggering for some survivors, will help support IPV survivors during a pandemic. Modifications to safety planning and harm reduction resources for IPV survivors cohabitating with abusive partners, as well as expanding options for housing, are critical to supporting IPV survivors during a pandemic and natural disasters. Further, attention should be given to the needs of IPV survivors from marginalized groups, many of whom are disproportionately affected by pandemics due to the compounding nature of disparities created by systemic issues such as racism and poverty.
Footnotes
Acknowledgments
The authors acknowledge Cynterria Henderson, Rebecca Garcia, and Kelley Premeo for their help with data collection and analysis.
Declaration of Conflicts of Interest
The authors do not have any conflicts of interest to disclose. The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Funding
This study was funded by a cooperative agreement from the Centers for Disease Control and Prevention (NU38OT000282).