
Abstract
Emergency departments (EDs) providing care and forensic examinations for sexual assault (SA) survivors are often supported by SA patient advocates. This study explored advocates’ perspectives regarding problems and potential solutions in SA patient care through a focus group with 12 advocates. Thematic analysis identified two major themes: provider–patient interactions and ED–hospital systems. Challenging aspects of provider–patient interactions included (a) provider attitudes and (b) disempowering behaviors. Within ED–hospital systems, themes included time constraints, efficiencies, and hospital preparation. Advocates surveyed were optimistic about an increased presence of SA nurse examiners and enhanced protocols and provider training to improve survivors’ experiences.
Introduction
Emergency departments (EDs) serve as a primary point of care for patients with a myriad of unplanned acute medical needs, often playing a key role in a healthcare system's ability to serve patients with barriers to other sources of outpatient care (Greenwood-Ericksen & Kocher, 2019; Pines et al., 2016). Demand for ED care frequently leads to high patient volumes, which must be carefully mitigated to prevent deterioration in the quality of care (McKenna et al., 2019). Among patients served in EDs are survivors of sexual assault (SA), who receive acute care to address SA-associated mental and physical health issues (Dworkin et al., 2017; Saltzman et al., 2007). However, seeking and obtaining medical care can be challenging for SA survivors. Only ∼20% of United States hospitals provide survivors with comprehensive services, including SA crisis counseling, sexually transmitted infection management, emergency contraception, and HIV management (Patel et al., 2013). Furthermore, completing an SA Examination Kit to obtain forensic evidence is inherently invasive and includes swabbing the vagina, rectum, and mouth, plucking and combing head and pubic hairs, and obtaining fingernail scrapings and blood samples (Ingemann-Hansen & Charles, 2013; Muldoon et al., 2018). Negative interactions can leave survivors at higher risk of posttraumatic stress symptomatology and reluctant to seek further medical and legal assistance (Campbell & Raja, 1999, p. 2005; McQueen et al., 2020).
One approach to support survivors in the development of SA Response Teams consists of SA patient advocates and/or SA Nurse Examiners (SANEs). SA patient advocates are volunteers or sexual violence center staff members who are trained to be dispatched to EDs (Zajac, 2011). Their role includes helping the survivor navigate the legal and medical process in the ED and serving as first-response crisis counselors (Greeson & Campbell, 2013). Training standards are defined and implemented at a state level (Wahab et al., 2021). For example, in Illinois, this includes a minimum of a 40-h crisis intervention training organized by a certified rape crisis center or the Illinois Coalition Against SA. SANEs are registered nurses organized through SA Forensic Examiner Programs who are trained in trauma-informed approaches to survivors’ medical needs, conducting forensic examinations, and providing forensic documentation in legal cases (Cole & Logan, 2008; Ledray et al., 2001; SANE-A, 2019). While SANEs’ roles overlap with those of SA patient advocates as liaisons in crisis intervention, safety planning, and referrals to follow-up services, SANEs are not always available to care for SA survivors (Delgadillo, 2017). In many of these cases, non-SANE-trained ED staff provide care, and SA patient advocates serve as liaisons (Ullman & Townsend, 2007).
Even with SA Response Teams assisting ED staff, providing care for SA survivors in the context of other demands in the ED is challenging (Campbell, 2013; Maier, 2008, p. 2012). Quality improvement research incorporating the perspectives of care team members offers the opportunity to address these challenges and develop more ideal models of care (Pope et al., 2002; Yang et al., 2017). As active observers of ED interactions and systems, patient advocates often have insight into the factors that affect the care of SA survivors and are key contributors to quality improvement research. While other studies have explored the perspectives of SA patient advocates, these studies have broadly surveyed patient advocates’ experiences in medical, legal, and mental health systems rather than focusing on their experiences in EDs (Campbell, 1998; Maier, 2008). Furthermore, no studies have provided updated perspectives from patient advocates on ED care after cultural changes of the last decade, including the #MeToo movement, have led to changes in the care of SA survivors in other medical fields (Campbell, 1998; Maier, 2008). Additionally, patient advocates’ views on potential areas of improvement in survivor care have not yet been described in the existing literature. The aim of this study, therefore, was to explore patient advocates’ perspectives regarding interpersonal and systemic factors that both support and impede the provision of trauma-informed care to SA survivors in the ED. Additionally, this study presents patient advocates’ novel quality improvement proposals for SA patient care.
Methods
Qualitative Approach and Research Paradigm
This explorative, descriptive qualitative study collected data about SA patient advocates’ experiences and perspectives. A focus group was utilized to explore the experiences of being a patient advocates in the ED setting (Wright et al., 2016). Our methods and results are reported according to the Standards for Reporting Qualitative Research (O’Brien et al., 2014).
Researcher Characteristics and Reflexivity
The research team consisted of three female medical students who were also trained as SA patient advocates (KDC, RP, and NED). While RP was a former co-volunteer with some study participants, she did not have an evaluatory or supervising relationship with them. The team also included three physicians/medical educators with experiential expertise in caring for SA survivors in both EDs and outpatient settings and in instructing medical trainees in trauma-informed care.
Context
After being paged by an organizing rape crisis center when an SA survivor checks into the ED, the patient is given the option to accept or reject services from an SA patient advocate. If the patient selects to have an SA patient advocate present, the patient advocate will often be present in the exam room for the entirety of the patient's medical care and forensic examination. SA patient advocates are valuable resources when evaluating ED care because, unlike survivors, they are usually not directly experiencing emotional trauma, and therefore conducting focus groups with them presents a lower risk of retraumatization (Campbell, 1998). In addition, patient advocates offer a wide perspective because they can draw observations of multiple experiences with different survivor identities, medical personnel, and medical centers.
Sampling Strategy
Focus group participants were recruited through volunteer email listservs through one of the two major rape crisis centers in the Chicago area. The rape crisis center is a nonprofit organization that partners with 17 hospitals. The focus group event was held during a regularly scheduled patient advocate meeting and participation was voluntary. Approximately 5% of active patient advocates attended the focus group. Participants were not provided with financial compensation but were given refreshments.
Ethical Issues Pertaining to Human Subjects
The University of Chicago Institutional Review Board approved the study procedures and ensured that ethical principles were applied to research activities. All participants gave informed written consent. Nonidentifiable demographic data was collected via a secure online survey.
Data Collection Methods
The focus group was held in December 2018 at the organization's headquarters. The focus group was conducted in a private conference room and lasted 48 min.
Data Collection Instruments and Technologies
A semistructured focus group guide was developed in collaboration with an SA patient advocate volunteer coordinator to explore patient advocates’ observations of survivor experiences in EDs. A review of the relevant literature was used to frame questions addressing barriers and facilitators to trauma-informed care in the ED, including both ED staff- and systems-level factors (Ahrens et al., 2000; Campbell, 2013; Campbell et al., 2005; Girardin, 2005; Kallio et al., 2016; Maier, 2008, p. 2012; Patel et al., 2013). Solutions to barriers to trauma-informed care were also discussed. Major topics covered in the interview guide included sources of retraumatization and how to mitigate them, the impact of SANE nurses, ED protocols, and potential areas for additional training. The interview guide was reviewed by an emergency medicine physician (KC), a family medicine physician specializing in domestic violence (SO), and a sexual violence crisis center coordinator. The focus group was facilitated by RP and was audio recorded.
Data Processing
The focus group was audio recorded and transcribed verbatim by two research team members (RP and NED). All identifying information was removed during the transcription process.
Data Analysis
Emergent concepts were identified by KDC, RP, and NED using an open coding and thematic content analysis approach (Bazeley, 2013; Braun & Clarke, 2006; Pope et al., 2000). Steps to codebook development were as follows: initial codes were derived from study goals and interview questions; codes were adapted and augmented by a review of a quarter of the initial transcriptions; codes were tested on additional transcriptions by all coders; and the codebook was edited as appropriate until a complete code list was reached. Coders were blind to each other's coding and all differences were resolved by discussion until 100% agreement was reached. During synthesis, coded excerpts were summarized into themes.
Techniques to Enhance Trustworthiness
A member check was performed by presenting a summary of themes to the original focus group members. The member check consisted of presenting tables of major themes, associated examples, and quotes. Participants used Likert scales to indicate their level of agreement with each of the five major themes. They were also provided with text boxes to express their opinions on the themes.
Results
The focus group included 12 SA patient advocates. Participant demographics are reported in Table 1. Of note, 8 of the 12 participants provided demographic information.
Participant Demographic Data.
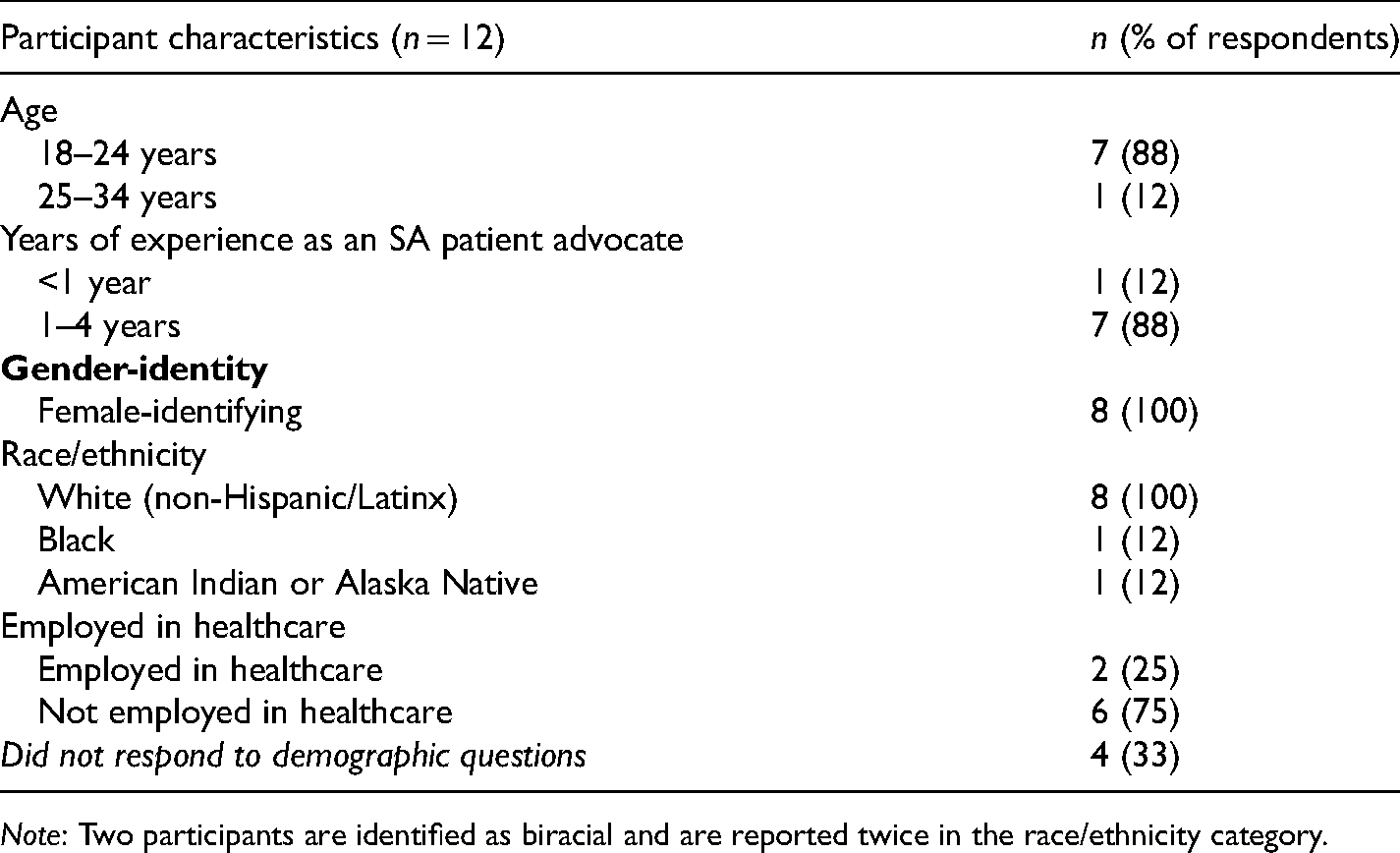
Note: Two participants are identified as biracial and are reported twice in the race/ethnicity category.
Of the eight participants who completed the member check survey, seven respondents agreed or strongly agreed that all the five major themes accurately represented their perspectives. One respondent agreed or strongly agreed with the four major themes and was neutral regarding the final theme (Hospital Preparation).
During the focus group, SA patient advocates described their experiences interfacing with survivors and healthcare providers in the ED. Two major categories of themes emerged from the discussion: (a) provider–patient interactions and (b) ED and hospital systems (Table 2).
Major Themes in Barriers and Facilitators to Trauma-Informed Care of SA Survivors and Proposed Solutions.

Provider–Patient Interactions
There were two major aspects of the interactions between healthcare providers and survivors that patient advocates perceived as factors influencing the provision of trauma-informed care: (a) provider attitudes, including the impact of provider assumptions, biases, and emotional valence, and (b) empowering or disempowering provider behaviors, or specific provider actions that influenced patient autonomy and shared decision making (Table 2).
Provider Attitudes
Many focus group participants emphasized that provider attitudes were a primary factor in survivors’ ED experiences. ED staff established that they believe the survivor was a key factor and both passive and active skepticism of the survivor's experience was described as damaging: Even if the doctor or nurse hasn’t said anything directly to the patient, usually the second they leave the room, the patient goes “I know they don’t believe me.” They’ve communicated it to the patient whether they intended to or not with the way that they’re treating and with the words they are saying to them. They also do sometimes say the words.
Participants noticed increased provider skepticism toward patients belonging to marginalized groups, including patients with psychiatric illnesses, patients working as sex workers, patients identifying as transgender, or male survivors of SA: I’ve worked with a survivor who wasn’t a woman, and there was a lot of skepticism and like, “Oh I don’t understand how that is sexual assault.”
Patient advocates also described scenarios in which providers assumed an investigative role by asking medically irrelevant questions. This behavior “translates to how they treat the person in the room and … creates a culture where the person is already under suspicion of not being believed.” Provider comments were also sometimes characterized by advocates as victim blaming, suggesting that the patient's actions, such as walking alone, caused the assault: Like, “Oh honey, but what were you doing there at that time?” or like, “Next time make sure you have a friend with you.”
Patient advocates also described a lack of respect for patient privacy. Examples included ED staff not involved in patient care loudly discussing the survivor's case and nonessential providers coming into the survivor's room out of curiosity: There’s a lot of curiosity from the other healthcare workers, respiratory therapists, phlebotomists, CNAs, security guards. They all want to know what the story is, ‘cause it’s like, interesting.
In contrast, patient advocates noted that an environment of professionalism and prioritization of the patient’s medical needs created a more supportive atmosphere. ED staff avoiding language such as “alleged assault” and “rape kit” and, instead of using neutral language, such as “evidence collection kit” or “the kit” was also identified as a method of conveying a supportive attitude.
Empathy was also identified as critical to trauma-informed interactions between providers and patients. Observed barriers to expressing empathy included a lack of time to spend with each patient leading to providers having a rushed demeanor could contribute to a negative experience for patients: It is so uncomfortable when [providers] walk in and are like, “Ok, I have 2 minutes, let’s do this.” That’s (the genital exam) just such a sensitive part of the exam and I feel like they just treat it like, “Let’s get this over with.”
When providers did have the time and/or emotional resources to express empathy, patient advocates observed that this created a supportive environment. It makes such a big difference when people (providers) are present and they are connecting with someone as if they are a human. And aware that this is a really traumatic event and that that person (survivor) may be emotional and that it’s okay.
Empowering or Disempowering Provider Behaviors
Focus group participants also expressed that providers’ behavior influences a survivor's ability to make well-informed decisions. Patient advocates described interactions where care and evidence collection were poorly explained: [The provider has] just been like, “Here take these pills.” And then after [the survivor is] like, “So, what did I just take?”
Patient advocates were concerned about interactions in which the providers provided such minimal information that survivors did not understand that all parts of the exam and medications are optional. In these instances, patient advocates felt that survivors were not being given the opportunity to properly provide consent. Time constraints also led to situations where patient advocates described how some providers became visibly frustrated when the survivor exhibited hesitation or asked for additional information: If the survivor is reluctant about any step in the process, especially like a fear of needles, not wanting to swallow big pills, things like that, I’ve seen so many nurses and doctors get intensely frustrated with the survivor and act extremely pushy like, “No, you have to do this. I’m not gonna sit around and wait for you to do this, you have to do (it).”
However, when providers had adequate time, patient advocates also observed the potential of explanation of options and consent for patient empowerment and shared decision making: …explain what every medication is for and make sure that they are getting a choice about whether to take that medication and understanding why they would or wouldn’t want to take that medication.
Finally, patient advocates observed providers pressuring survivors to speak to the police and burdening them with the responsibility of preventing potential future assaults: I’ve seen doctors and nurses telling the patient they must speak to the police ‘cause, “If you don’t tell the police he could do this to someone else.” (Some providers) really try to take it upon themselves to convince the (survivor) to talk to the police which is not their job and not necessarily what’s best for that survivor.
To empower survivors to make their own, well-informed medical and legal decisions, patient advocates emphasized the positive impact of providers that “slow down” and “make sure everything gets explained and consent is had.” Patient advocates noted that prior experience and training facilitated empowering provider behaviors: If you’ve done that kit before and you are trained then you know that everything is optional and so they know to be like, “You don’t have to do this,” and “Do you want to do this? Is this okay?” They will check in about consent the entire time.
Provider–Patient Interactions: Solutions
When discussing solutions to improve provider–survivor interactions, patient advocates stressed the importance of training providers in being “professional.” This included not commenting on nonmedically relevant topics and respecting patient privacy: The only advice that is a good thing to give is medical advice. I believe you, it’s not your fault, and you have options.
Patient advocates acknowledged that providers often intended to provide survivors with appropriate care but lacked specific skills. For example, one patient advocate proposed “support[ing] staff in the language they use” in response to the ingrained challenges such as “the processes and the way we think about assault in general (making) staff always assume the perpetrator is a male.”
In response to the discussion on barriers to provider compassion, patient advocates perceived lapses in empathy to be connected to providers’ desensitization to trauma: This is [the provider’s] day-to-day life and I think that they sometimes forget that this is the most unusual day, I mean, of this patient’s life.
Therefore, focus group participants proposed “enabling doctors and nurses to say that they didn’t want to take a patient because they were not feeling equipped to.” However, patient advocates acknowledged that this would be difficult to enact. Patient advocates acknowledged that many barriers to trauma-informed provider–patient interactions were caused by the systemic factors in the ED context (see below).
ED and Hospital Systems
Time Constraints
Patient advocates acknowledged that the barriers to trauma-informed provider attitudes and behaviors discussed above must be considered in the context of systemic problems in ED settings. Patient advocates discussed the link between time constraints inherent to the ED and problems such as lack of provider empathy, explanations, and consent. As explained by one patient advocate, patients will be prioritized based on acuity and survivors may be less medical urgent relative to other patients: Someone is like literally dying two doors away and our nurse was trying to save their life and (the survivor) is not the priority right now.
Efficiency
Receiving care in the ED can also subject survivors to process inefficiencies. Most notably, patient advocates were concerned about potential retraumatization caused by survivors having to repeat their stories to multiple members of the care team: There have been quite a few instances where I’ve noticed the survivor just feeling really exhausted by having to say the same thing over and over again.
Patient advocates observed that experienced team members explaining to the survivor what to expect at the start of the encounter were a simple way to mitigate this potential source of retraumatization: The first nurse they interact with was like, “[Telling your story] happens during the kit, if you don’t want to keep retelling it that’s fine just say so and we can just go over it then…don’t feel obligated to talk about it now”
Lack of care coordination also led to frequent interruptions and what patient advocates perceived as too many providers in the room at one time. They described the impact of this as “disruptive” and “exposing.”
Patient advocates also observed how inefficiencies can impact the experience of providers caring for survivors, creating what patient advocates perceived as a dynamic that harmed the provider–patient interaction: I was told by the nurses that they hate getting sexual assault cases because it means hours of paperwork, a very slow evidence collection … then it’s a problem for them … and they get really frustrated.
Finally, delays in discharge were emphasized as impacting survivors because spending additional time in the ED is not conducive to survivors feeling safe after an assault: How many times have we all sat in an emergency room and all of a sudden you just hear screaming or shrieking or something? That’s also absolutely retraumatizing.
Hospital Preparation
Patient advocates highlighted that patients receiving care at hospitals that are “well-versed” in the care of SA patients benefited from the care team's confidence: Any nurse in those hospitals is like, “Been there, done this. I have the kit down.” Not in an awful way. They know what they are doing. They are comfortable.
In contrast, patient advocates noted that receiving care from an underprepared hospital could make survivors feel even more vulnerable: A lot of the times [providers] do nothing to hide the fact that this is the first time they are seeing [a sexual assault survivor] and they completely rock that person’s world.
The importance of hospital preparation extended from the comfort of individual providers to the logistical preparedness of the system as a whole: I was in a call where the hospital didn’t even have a kit … They were calling other hospitals to ask, “Do you have a kit we can pick up?” Like this did nothing to inspire confidence.
Patient advocates also noted that some survivors experienced EDs that were underequipped to connect survivors with necessities such as clothing, transportation, and emergency housing: The survivor is there for medical care, but their biggest concern was where they are going to sleep that night.
These situations highlighted that EDs may not have the resources to address survivors’ basic needs, such as clothing, transportation, and safe housing, after discharge.
ED and Hospital Systems: Solutions
Patient advocates acknowledged that some of the provider–patient problems, such as rushing, were caused by the systemic factors in the ED context. For this reason, patient advocates emphasized that SANEs and SA patient advocates can support patients despite challenges precipitated by rushing, lack of provider training, or lack of care coordination.
Similarly, patient advocates explained the importance of making sure the patient is aware of the role of all team members. For this reason, patient advocates stressed the importance of providers introducing themselves and their role in patient care. Patient advocates also proposed giving the survivor options about who to engage with: As much as possible, make fewer people enter the room. I know that sometimes there have to be trainees, but sometimes just one trainee, or give them (the survivor) the option. Make sure they have options the entire time.
To address inefficiencies, patient advocates suggested increased involvement of healthcare workers, such as SANEs, who have developed ways to operate efficiently in the current system: The first thing [the SANE nurse] did was say like, “Let’s talk about STI concerns right now.” And she put [orders] in because she knew it was going to take 2 to 3 hours to get it from the pharmacy.
Standardized protocols and checklists were proposed as another way to support providers in improving efficiency. However, patient advocates stressed that developing protocols and disseminating logistical information is not enough; hospital staff must be trained in trauma-informed care: I think a universal training for everyone in the hospital on crisis intervention would be great. It’s not just a list of how do you communicate belief and not make it worse.
Discussion
In this study consisting of a focus group of SA patient advocates, we found EDs sometimes fall short when providing complex care, collecting forensic evidence, and connecting survivors with ongoing resources in a compassionate and empowering manner. Importantly, our results show that lapses in trauma-informed care often reflect systemic failures to provide ED staff with adequate training and time to care for this patient population.
The unfamiliarity and low self-efficacy in caring for this patient population observed by patient advocates have been documented in wider samples of providers (Amin et al., 2017; Marshall et al., 2018). Lack of training could be an underlying factor in negative interactions because (a) providers do not feel confident in providing SA patient care and project this lack of confidence to their patients and (b) the lack of training makes the encounter take longer, adding to both provider and patient frustrations. Additionally, ED staff are not immune to widely held misconceptions about SA and may be at risk of expressing disbelief, victim-blaming attitudes, and insensitivity (Campbell, 2005; Campbell & Raja, 1999; Harland et al., 2021; Maier, 2008). These behaviors were confirmed by our sample of patient advocates, who also suggested that these harmful behaviors are more prevalent when survivors do not fit stereotypes associated with prototypical SA survivors.
However, patient advocate perspectives suggest that these attitudes and behaviors can be modified through provider education. Initial implementation of educational interventions and collaborative training between ED staff and SANE nurses show great promise (Auten et al., 2015; Glowa et al., 2002; McLaughlin et al., 2007; Milone et al., 2010; Slaughter, 2018). Specifically, in the Chicago area, a SANE-led program for emergency medicine residents including a didactic lecture, two standardized patient cases, and a forensic pelvic examination simulation increased the provider's self-perceived ability to avoid retraumatizing patients and conduct forensic examinations (Chandramani et al., 2020). These results confirm our focus group members’ recommendation that increasing collaborative training between ED staff and SANE nurses will improve the quality of SA patient care.
Problems attributable to lack of provider training in SA patient care were exacerbated by the ED context. Competing priorities for time are a barrier for even well-trained ED staff. Our results suggest that additional care coordination and emotional support from SANE nurses integrated into care teams is key. Patient advocates’ observations of SANEs elevating the quality of care align with prior studies documenting that EDs with SANE programs provide comprehensive medical services and proper completion of forensic examinations at higher rates than EDs lacking SANE nurses (Patterson et al., 2006; Schmitt et al., 2017). Numerous studies have also demonstrated that receiving care from a SANE “humanizes” the survivor experience and that survivors are more likely to report receiving compassion, clear explanations, and choices (Campbell et al., 2008; Fehler-Cabral et al., 2011).
Beyond increased provider training, solutions to ED efficiency challenges proposed by patient advocates are well-aligned with the tools utilized in initial quality improvement projects in the ED care of SA survivors. Training in standardized protocols and checklists improves provider self-efficacy, decreases patient wait time, and improves the quality of care (Ciccone, 2020; Marshall et al., 2018). For example, implementing a computerized charting system detailing new care protocols for SA survivors improved the proportion of survivors receiving optimal medical care from 10% to 90% (Gilles et al., 2019).
Our study was limited by its single-organization status. Although focus group attendees collectively had experience at 17 Chicago-area hospitals, the SA patient population at these hospitals is not necessarily representative of other Chicago communities, and other urban or nonurban patient populations. Future studies should explore if disparities in SA patient ED experience exist in these different populations. Additionally, theme saturation was limited to perspectives from a single focus group study. Validation of these themes established in this study with wider groups should be performed.
Implications for Practice
This study suggests that increased training of ED staff and the allocation of resources including specifically trained SANEs are critical to improving ED care for SA survivors. Despite our qualitative study adding to an existing body of evidence that SANEs are effective in improving SA patient care, SANEs are frequently not available (Delgadillo, 2017). In the state-wide context of our study, only 32 of Illinois’ 10,000 ED nurses are certified SANEs (Bowen, 2018; Delaney et al., 2019). Our results suggest that increasing the ranks of SANE-trained providers should be prioritized in tandem with enhanced ED staff training. Particularly given the financial and logistical strain on EDs caused by COVID-19, pragmatic and feasible goals must be developed to create a future healthcare workforce that is well-equipped to meet the unique needs of SA patients in this setting (Sohrabi et al., 2021).
Conclusions
Our results highlight how both interpersonal and systemic factors contribute to the ED experiences for SA survivors. Specifically, a lack of hospital preparedness, both in the form of provider training and well-established protocols was identified as a major problem. Conversely, patient advocates reflected on how positive survivor experiences were facilitated by staff who were trained in caring for survivors, specifically SANE nurses.
Our results offer novel perspectives on ways to improve survivor experiences in the ED drawn from the experiential knowledge of SA patient advocates. Patient advocates noted that features of these interactions were often related to more systemic issues including time constraints and lack of provider education rather than unmalleable factors. For this reason, patient advocates were optimistic about the presence of SANE nurses and/or SA patient advocates as well as enhanced protocols and provider training to improve survivors’ experience in the ED.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bucksbaum Institute for Clinical Excellence.