
Abstract
Indigenous intimate partner violence (IPV) advocates are essential for Indigenous women experiencing IPV who seek support amidst personal and historic trauma. IPV advocates work with and on behalf of clients to identify resources and promote resiliency. Indigenous advocates share their personal IPV experience. They provide individual ways they halted intergenerational trauma, moved toward becoming healthy, and made changes in their personal lives which affect services provided to their clients. This study fills a literature gap as it examines the intersection of Indigenous IPV advocates’ personal journey of ending intergenerational trauma as a path to promoting resiliency among their clients.
Intimate partner violence (IPV) against women is a global epidemic. The World Health Organization (WHO) (2021) states IPV is a violation against women's rights with long-lasting major public health problem. In their 10-year study across 161 countries, WHO (2021) reported one in three women experience some form of IPV. The Centers for Disease Control and Prevention (2021) report that in the United States, nearly one in five women experience IPV. Of the 1.8 million Indigenous women in the United States, 1.5 million Indigenous 1 women in the United States experience some form of violence, including physical violence, sexual violence, stalking, or psychological aggression in their lifetime (Rosay, 2016). Of this number, physical violence by a partner account for 55.5% of the violence and 66.4% is psychological aggression by a partner. Rosay (2016) further states 56.1% of Indigenous women experience sexual violence and 48.8% have experienced stalking in their lifetime. Violence against Indigenous women by intimate partners is linked to the impacts of colonization such as historical trauma and historical oppression (Bubar & Thurman, 2004; Burnette, 2016). Colonization has shaped violence against Indigenous women and continues to promote the ongoing violence (Weaver, 2009) by changing the ways in which Indigenous women are seen in their communities and how they are valued. 2 Specifically, colonization shaped the violence wielded against Indigenous women by non-Indigenous and Indigenous others. Prior to contact with settlers in the United States, Indigenous women were seen as equals, particularly in matrilineal societies (Herring, 2001). Indigenous women have been historically dehumanized by the impacts of colonization through federal policies, sterilization, and other structural-level violence (Weaver, 2009) however those conversations are beyond the scope of this article. The focus of this article will explore the impact historical trauma has had on the rates of IPV against Indigenous women and investigate how advocates encourage resiliency.
Literature Review
Literature regarding the intersection of historical trauma, Indigenous women who experience IPV, and advocates who promote resiliency is growing. The three concepts are individually important, however, a cross-section of all three can provide background knowledge on historical trauma for advocates working with Indigenous women who experience IPV. More literature is needed so Indigenous individuals, communities, and practitioners can effectively address historical trauma and its contribution to IPV and promote Indigenous survivors’ resiliency. From a scan of the literature, only one other study focuses on the connection of recovering from IPV and IPV survivor advocates that emphasize resilience (Crann & Barata, 2021) when advocating on behalf of survivors. In addition, insight is also needed into how Indigenous IPV advocates, specifically within the context of historical trauma, approach their advocacy work with clients. Colonization is the precursor to genocidal acts which has been termed historical trauma. Historical trauma is the culmination of events that ultimately leave lasting effects such as high rates in IPV in Indigenous communities (Yellow Horse Braveheart, 2006), particularly IPV against Indigenous women (Weaver, 2009). The following section connects literature on historical trauma, IPV, and resiliency.
Historical Trauma: Connection to IPV Among Indigenous Women
Colonization created historical events or forces that caused historical trauma. The historically traumatic events lead to the imposed violence such as the high rates of IPV against Indigenous women. The traditional teachings and values held by Indigenous communities prior to contact with white settlers were much different than today (Baskin, 2020). While Indigenous women are still held in high regard in many Indigenous communities, the once held beliefs, practices, and respect for Indigenous women were different before colonization as they were once highly regarded as life givers and the foundation for Indigenous tribal Nations, particularly among matrilineal tribes (Burnette, 2015b; Burbar & Thurman, 2004; Weaver, 2009). The connection between historical trauma and IPV is evident beginning with the beliefs and practices by some white settlers. Colonizers’ beliefs and sexist attitudes (Braveheart-Jordan & DeBruyn, 1995) contradicted the traditional views of Indigenous values. Their attitudes, in some cases, forced or influenced some Indigenous communities and their perception of Indigenous women (Baskin, 2020; Murray, 1998). Historical trauma and oppressive acts, such as land disposition, boarding schools—which nearly severed the family structure—and near loss of Indigenous traditional teachings have also contributed to contemporary societal factors that negatively impact Indigenous women (Burnette & Hefflinger, 2017; Weaver, 2009). These acts are considered historical trauma, the result of historical events or historical forces that negatively impact the current living situations of a population (Brave Heart, 2000; Weaver, 2009; Varcoe, et al., 2021).
Literature on IPV in relation to Indigenous women suggests they experience higher rates of violence when compared to their non-Indigenous women counterparts (Burbar & Jumper Thurman, 2004; Chenault, 2004, 2011; Evans-Campbell et al., 2006; Tehee & Esqueda, 2008; Willmon-Haque & Big Foot, 2008). Despite the trauma Indigenous women face, they continue to be resilient as they maintain their roles as caregivers, earn degrees, build businesses (Institute for Women's Policy Research, 2020), and strive to carry on traditional Indigenous ways.
Resiliency as Part of Recovery From IPV Among Indigenous Women
Little is known about how the concept of resiliency can help practitioners, but survivor-advocates may hold the answer to understanding how resiliency is a component of a woman's recovery from IPV (Crann & Barata, 2021). Helping others has been found to be part of the recovery and resilience process for women who experience IPV (Crann & Barata, 2021; Senter & Caldwell, 2002). Understanding resiliency can allow researchers to focus on the ability of advocates to work against oppressive systems by broadening the knowledge of their resilience (Slattery & Goodman, 2009). According to Tsirigotis and Luczak (2018), resilience and resiliency are often intertwined and interchangeable. Resilience is defined as the continuation of healthy or productive adaptation despite adversity (Martinez-Torteya et al., 2009). Tsirigotis and Luczak (2018) indicate that resilience is a concept used to define the ability of an individual or group of people to positively face adversity even when the environment is damaging. It allows individuals or groups to respond to everyday demands despite adversities faced throughout their life, resulting in a combination of individual attributes (Tsirigotis & Luczak, 2018). Resilience has two dimensions: (a) resistance to adversity protects the integrity of a person under pressure and (b) the person maintains the ability to build a life worth living despite adverse circumstances (Labronici, 2012). Greene (2008) defines resilience as a person's ability to adapt to challenges and becoming better with greater skill prior to adversity.
For advocates who went through their own healing, resiliency is an important factor to their recovery. Sharing their own experience with IPV helped the advocates’ own personal recovery and gave a sense of self-dignity and purpose (Crann & Barata, 2021). Advocates may hold insights on resilience that can aid in the recovery process. In particular, resiliency in the context of Indigenous people is essential to the conversation because of this groups’ unique relationship to collective trauma.
To date, most of the research regarding resiliency and Indigenous people has focused on understanding what cultural and familial factors are correlated with children and elders’ strength of resiliency. Literature on resiliency and Indigenous people focuses on children and youth (Garrett et al., 2014; Swanson & Saus, 2013; Ulturgasheva et al., 2014) and older people and elders (Ramirez & Hammock, 2014), while other literature focuses on all age ranges (Goodkind et al., 2015; Wexler, 2014; Willmon-Haque & BigFoot, 2008). Goodkind et al. (2015) focus on the importance of cultural resilience to move beyond trauma as a way to reconnect to traditional ways. In a more recent study, Burnette et al. (2020) focus on the Family Resilience Inventory to gather information on participant's current families and their families of origin to assess family protective factors. Wexler (2014) examines three generations and how they understand colonization, or “cultural suppression” based on their generation.
Other literature on resiliency among Indigenous people provides a connection to resiliency as a path toward healing. For instance, Garrett et al. (2014) review resiliency while paying attention to historical trauma and its effects on Indigenous people. They highlight the many strengths and resilience of the youth to bring forward positive ways of helping them heal from intergenerational trauma. Goodkind et al. (2015) indicated that youth did not find Western behavioral health services useful in their healing process. Most of the parents/caregivers and elders used prayer as a coping mechanism. All participants identified land of their ancestors as important to their healing and well-being. As a result of identifying place as vital to healing, the authors conducted another interview to map out areas of significance. Swanson and Saus' (2013) participants indicated that they use the concept of historical trauma when working with children. They found that historical trauma can lead to both negative and positive aspects of the children's lives and that colonization has led to modern-day struggles. Ulturgasheva et al. (2014) conducted a cross-comparison study among Indigenous youth from five different arctic communities. The researchers proposed a sliding scale of positive and negative influences and how each can move between being a resiliency factor or a vulnerability.
Interestingly, Willmon-Haque and BigFoot (2008) examine the effects of violence and trauma within Indigenous populations and the subsequent results of such violence and trauma. They describe historical trauma as a pathway to experiencing psychological disturbances. Willmon-Haque and BigFoot (2008) conclude trauma still has lasting impacts on Indigenous people, despite their resilience. They identify culturally congruent services, both Native and mainstream, currently assisting Indigenous people to identify and raise awareness of issues affecting the Indigenous population. In addition to individual level resiliency, there are many tribal Nations using their traditional ways to help heal from all forms of trauma (Burnette, 2015b; Lewis et al., 2021) and promote resilience at the community and nation levels.
Historical trauma experienced by Indigenous people can be addressed by focusing on resilience or positively facing adversity. Resiliency within Indigenous communities, particularly among women who experience IPV, can be increased by advocates who work with and on behalf of these women. The advocate's role is essential to the client's overall successful healing.
Role of Advocacy: Fostering Resiliency
Advocates in the IPV field must be knowledgeable regarding many aspects of IPV from the impact of trauma, to access of resources, to implications of local and federal policies (Sullivan & Goodman, 2019). They work with and on behalf of IPV clients to identify resources to aid in honoring the client's responses and desires (Goodman et al., 2016). IPV advocates have been instrumental to the advocate-client relationship (Wood, 2017) and promoting resiliency. Their role can include but is not limited to emotional support, ensuring safety, and protecting the client's rights (Sullivan & Goodman, 2019). Advocates promote resiliency through a variety of ways, but relevant to this article, they focus on opportunities for survivors to reclaim control over their lives and support and strengthen their coping strategies (Goodman et al., 2016). Goodman et al. (2016) also identified both cultural humility and historical context as central to effective advocacy. Indigenous IPV advocates have a unique connection which can promote resiliency as they have also experienced historical trauma and oppression. The shared experience and understanding of their clients can build a relationship and the trust needed for an effective relationship (Asian Pacific Institute on Gender-based Violence, n.d.) thus promoting resiliency.
Literature that focuses on the cross-section of historical trauma, IPV, and resiliency is limited. Additional research should be conducted on the role advocates play in understanding the impact of IPV in relation to historical trauma. It is also vital to understand the impact of resiliency when advocates work with Indigenous women who experience IPV. Collectively, the concepts can provide a connection between IPV advocates and survivors of IPV.
Present Study
This study seeks to bridge this knowledge gap by listening to the lived experience of Indigenous IPV advocates to understand how the study participants promote resiliency with the clients they work with. The participants, tribally enrolled Indigenous women who were advocates that work with Indigenous women experiencing IPV, were asked about their perceptions on how to support resiliency in their clients.
Method
This study, as part of a larger research study (Holder, 2015) to learn more about the relationship between historical trauma and IPV among Indigenous1 women, focused on the experience of promoting a resilience response. The present study sought to explore the following research question: Research Question 1: What do advocates believe has been most effective in helping Indigenous women experiencing IPV?
Participants
Purposive sampling technique was used to recruit participants and to gather more participants. Initial recruitment began with internet searches to identify tribal social service departments located in the Midwest region to see if they had IPV departments and advocates. Emails and phone calls were made to share the study with directors. After information was provided, the researcher asked if a flyer could be shared with advocates. If potential participants were interested in participating in the study, they were asked to email the researcher. After initial contact was made, an interview time and location were determined to suite participant needs and to ensure privacy. Participants received a human subjects-approved consent form. Most interviews were conducted in person with the exception of two which were done over the phone because of distance between the researcher and participant.
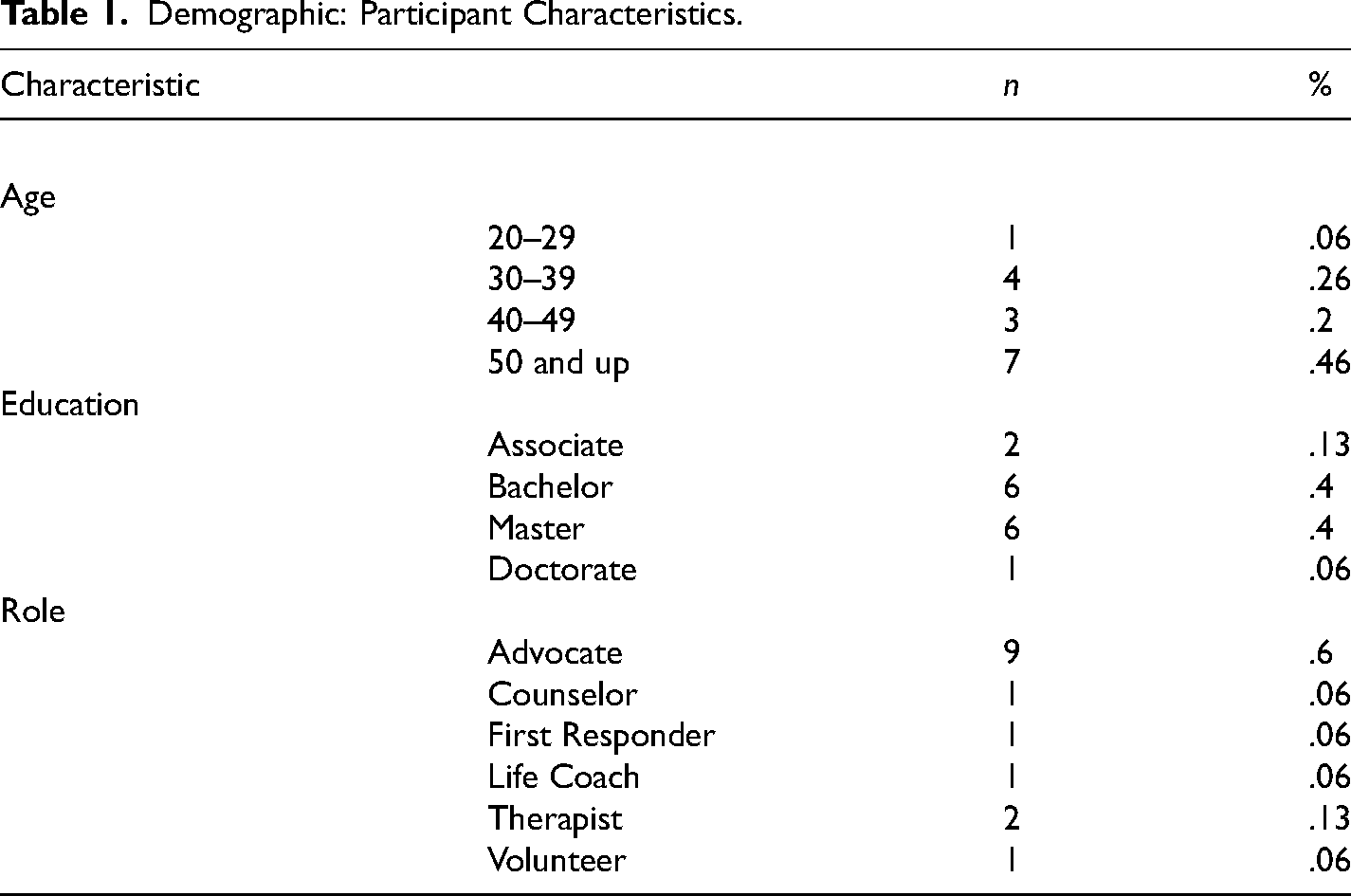
The criterion for participants to be selected included: female regardless of gender assigned at birth, an enrolled member of a Native American tribe, and be a professional or volunteer advocate with experience helping Indigenous women to cope successfully with their past experience of IPV. Participants self-identified as tribally enrolled Indigenous women who were advocates or practitioners who worked with Indigenous women who experienced IPV. Their ages ranged from late 20s to mid-60s, with the average age 47 years old (see Table 1 for participant characteristics). Most of the participants held a higher educational degree (N = 13). Two of the participants indicated their highest degree earned is an associate degree. Six participants have a bachelor's degree. Six other participants have a master's degree, five of which have their master's in social work. One has her doctorate degree. Most of the participants call themselves advocates (N = 9), while two are considered therapists because of the type of service they offer clients, and the remaining are either called life coach, first responder, or counselor. The majority (N = 12) worked in tribal communities or urban areas and only three worked in their home communities. The shortest amount of time in the IPV field was three years, while the longest amount of time was 28 years. Due to the narrow focus of the criterion, the researcher had difficulty getting enough participants, so the use of a referral process by current participants was utilized. The same selection process was used with those referred to be potential participants.
Demographic: Participant Characteristics.
Reasons for Selecting the IPV Field
It is important to understand how the participants got into the field of IPV because it helps lay the foundation for their commitment to the IPV field. Personal or family history of IPV was a motivating factor for entering the field, as Linda shares: I think growing up in a home with my own experience as a child probably led me to this work. I did not know at the time, I was so young, but I just finally came to terms with, “Hey, my mother was an abuse victim.” My father was in a wheelchair, and he was paralyzed from the waist down, but he could still be abusive in certain ways to myself and my brother and my mother. I really didn’t think I would go into this field; I really tried to stray away from the mental health field.
Using a naturalistic inquiry approach along with an empowerment-based framework (Creswell, 2009; Patton, 2002), an IRB-approved semi-structured interview guide with open-ended questions was used. Interviews ranged from 45 min to 2 h. Interviews were audio recorded and then professionally transcribed and then once again reviewed by the researcher for accuracy and to remove all personal identifying information. Pseudonyms were assigned to each participant to ensure anonymity. The researcher conducted member checks to verify further accuracy. The member checks clarified unclear points or filled in missing information from the first interview. Follow-up member checks lasted approximately 20 min.
Data Analysis
According to Lincoln and Guba (1985), data collection and analysis are inseparable until the final report therefore the researcher began initial meaning and tentative meaning during the interview process and continued to reduce themes until the final version of the report. The analysis began with transcribing verbatim the audio recordings of each participant interview by a professional transcriber. The text of the audio recording was checked by the researcher for authentication purposes. In accordance with Patton (2002), coding of data occurred next to begin examining and evaluating transcriptions for trends and themes. Tentative coding occurred to help determine the main ideas based on the insights garnered from the transcripts and the first few participant interviews. Inductive coding was utilized as it allowed the analysis to develop without pre-determining themes though the research question influenced the emphasis of analysis in a deductive manner. Upon examination of the text, broad themes emerged from the patterns of the data itself. The remaining transcripts were coded into the broad themes which made the data more manageable for the researcher. The coding guide was then refined to check for usefulness as it applied to all data (Lincoln & Guba, 1985). ATLAS-ti was used to code the themes. The themes from the findings emerged inductively and included subthemes.
It was necessary to plan for methodological trustworthiness to accurately reflect participant experiences and perceptions. The four original criteria identified by Lincoln and Guba (1985) include: credibility, transferability, dependability, and confirmability to support the rigor of design. Patton (2002) later added authenticity and integrity or faithfulness as criteria to be consistent and support an empowerment approach. In addition to the audio recordings the following were maintained by the researcher to support the rigor of design: a personal journal, summary sheets of participant interviews, and an organized audit trail. The audit trail included electronic and paper files, audio recordings, interview transcripts, researcher reflective notes, interview records, consultant panel notes, and the interview guide (Lincoln & Guba, 1985; Creswell, 1994). An external auditor reviewed the audit trail during three different points in the research process. The first occurred during code category development, the second during the theme development, and the third review was conducted to confirm the final findings. Additional audits of the research process and results were conducted by a colleague.
Findings
Participants were asked to share their views regarding how they promote Indigenous women's resilient responses to IPV. They discussed factors that enabled a continued path toward their own personal recovery toward intergenerational healing. From this study, participants revealed they witnessed violence in their home or origin or experienced IPV themselves. None of the participants were directly asked if they were abused or if they witnessed abuse. Out of the 15 participants, 9 talked about their own personal experiences with IPV however, this section provides information from seven of the participants. Of these, several discussed in detail the type of abuse they experienced and the effect it had on them, but they also shared their own journey and identified how their own path led them to resiliency. In turn, this promoted resiliency among their clients. Following under the larger theme of breaking intergenerational trauma, the following subthemes emerged: making a change, becoming healthy, and hope and belief. The findings section shares ways in which participants began to break intergeneration trauma to aid their own healing and lead to ways they can build resiliency among their clients.
Breaking Intergenerational Trauma
Breaking intergenerational trauma emerged as a major factor influencing the participant's path toward healing which led to the advocates building resiliency among their clients. Participants discussed intergenerational disruption between and across generations. Harmful beliefs and behaviors were learned in families and then transmitted across generations (BigFoot & Braden, 2007). The coding process revealed a relationship of the themes such as making a change, becoming healthy, and hope and belief as ways to halt intergenerational trauma. The participants discussed how their personal experience with IPV and witnessing IPV parallels their client's path. The participants’ path toward healing and stopping intergenerational trauma began with making a change, becoming healthy, and hope and belief.
Making a change
The process of making a change is a conscious decision to either improve or do something differently than previous efforts. Some participants (N = 5) decided to make a change while others witnessed a family member make a change. Sasha found strength through her mom's change, “And so, you know, if my mom could change her life around, and who else knows whose lives changed around, by role playing of just being educated on something.”
The decision to make a change began for some at an early age. Betty shared about her desire to leave home at a young age to escape the violence. I can only speak for myself right now, because I have to relate it to this. I wanted to leave because I got tired of listening and seeing and hearing and just living in that destruction and that violence at the very young. I wanted to leave forever and never come back, which happened for me when I went to boarding school. [I] never went back. I never saw that again. So, the fear that I never tackled was the violence, you knew, that I grew up with. So, going through school was my fear. I was like, “If I don’t succeed, I’m going to end up over here.” “If I don’t go through school, I’m going to end up over here.”
[name deleted] was a boarding school mentality, and I was still safe; but I didn’t know I was very unhealthy, meaning not well mentally—you know? And so getting into a relationship that wasn’t well, we both and the same type of childhood. And so when we started our family is when I finally realized, “Hey, one of us needs to get well.” My children were raised without drugs and alcohol and violence, you know? It's hard. It's hard to be that kind of parent.
Joyce also made a conscious decision a change her life for her children.
And I wanted my life to be different. I had a daughter at the time, and she was five, and I wanted life to be different for her. I didn’t want her—and, actually, for—you know, my son came along years later, but I strived to make life different.
The decision to make a change helped the participants adapt to adversity when the environment is damaging (Tsirigotis & Luczak, 2018). The advocates can help the clients make a decision to leave their abuser or to remove negative aspect of their life.
Becoming healthy
Participants (N = 4) found that becoming healthy was the next natural process in the path toward healing and halting intergenerational trauma expressing through acts of IPV. Becoming healthy is the process of learning healthy ways of life. It can feel unfamiliar to women who have either witnessed or been abused for a long time. Joyce, an advocate who also experienced IPV, talks about her thoughts on becoming healthy. And you can’t tell me that where we’re at today, where we have low self-esteem, that we were born that way. I don’t think so. I think that we have learned that. We have learned a lot of unhealthy behaviors; and by the same token that we have learned those, we can unlearn them. But we have to know what it is that we’re trying to unlearn, because so much of it has been enmeshed in our lives now. And violence is commonplace.
How do we grasp on to what healthy is, you know? And so, when I was in the therapy world out there, my focus always was, “How do you get well?” I, myself, didn’t get well until I was 30 and I was forced into treatment. I took care of myself. I was already starting my new family, but part of me had one leg in and one leg out, and I wanted it both to be in. How was I supposed to know that and grasp what healthy was?
Deanne shares her experience about leaving unhealthy ways behind,
Everybody's different. And you know what? Five years after my divorce, finally—I can only describe it this way: my old self, Deanne, came back; because Deanne in the marriage and stuff—I had joy of the Lord, but now I just feel like my old self.
Becoming healthy can include learning traditional ways which is an aspect of cultural resiliency (Goodkind et al., 2015). For others becoming healthy can mean receiving culturally appropriate counseling or therapy, both of which can provide techniques that can act as protective factors to prevent psychological disturbances (Willmon-Haque & BigFoot, 2008).
Hope and belief
The participants (N = 3) identified hope and belief as another important aspect of halting intergenerational trauma. Hope and belief provided the participants with positive feelings about the future and the belief that their decisions have made a positive impact for upcoming generations. Christine talked about her belief in herself and for her children. But I’m just saying, you know, if I believe in something, no door will close on me. That's how it's always been. Because I believe in something so much, people respond to that. And I believed in myself more than anything. And I believe in my children.
…I appreciate the fact that I did go through that because I’m a stronger, healthier person. When a person is finally done and says, “That's it. Never going to happen again.” Because it finally got to that point where I remember the last hit I took, and I said, “No more. That's it. I’m done.”
Participants find hope and belief not only in their own personal life, but also for future generations. Joyce explained how she has hope for her grandchildren.
I look at my grandchildren, and I want a brighter future for them. I want them—I am so thankful that my grandchildren have never seen their grandfather drunk. They don’t know what it is. Our children shouldn’t have to go through that. They shouldn’t have to grow up before their years. Our children shouldn’t have to be scared. They shouldn’t have to hide.
Participants share their experience and encourage their clients to be hopeful about the future. As their clients make the necessary adjustments and learn new skills to address new challenges, the clients will believe they can construct a life worth living despite everyday adversity (Labronici, 2012).
Discussion
Participants who work as IPV advocates were asked how they promote resiliency among their clients and to provide recommendations on how to promote resiliency for other helping professionals who might also work with Indigenous women who experience IPV. They were specifically asked to share examples of their experience in identifying what works best. None of the participants were asked if they themselves experienced IPV, but many of them revealed they have either witnessed IPV or are survivors of IPV. The results indicate that the participants used their personal experience with IPV to promote resiliency among their clients. They found their own path was the most useful information in building relationship with their clients. Under the overall theme of breaking intergenerational trauma, there are three subthemes of making a change, becoming healthy, and hope and belief.
Participants shared personal experiences of how historical trauma has impacted the IPV they experienced or witnessed. Their personal experience addressed the research question of how they promote resiliency by providing examples of leaving a situation, becoming healthy, and having hope and belief. In doing so they recognized the necessity to make changes in their own lives. For example, when Betty and her partner started a family she told him, “Hey, one of us needs to get well.” Together they made a conscious decision to end the abuse they both witnessed as children. Other participants such as Sasha gave credit to her own mother's decision to make a change by leaving her abuser. In turn, this resulted in Sasha making better decisions in her own life for her family. After leaving a situation or making a change, the participants found they needed to become healthy to address the trauma they experienced or witnessed. They identified the need to unlearn generations of unhealthy behavior commonplace after colonization. Joyce shared “… but we have to know what it is that we’re trying to unlearn, because so much of it has been enmeshed in our lives.” As participants move forward with becoming healthy, they found hope and belief as part of their path to healing. Many found hope in their children and wanting to be better parent. Others believed they deserved a better life that does not entail IPV.
In line with expectations, the participants identified the correlation between historical trauma and the high rates of IPV against Indigenous women (Burbar & Jumper Thurman, 2004; Chenault, 2004, 2011; Evans-Campbell et al., 2006; Tehee & Esqueda, 2008; Willmon-Haque & Big Foot, 2008; Weaver, 2009). Participants shared that generations of unhealthy behaviors, due to colonization and the changing beliefs about Indigenous women (Baskin, 2020; Burnette, 2015b; Burbar & Thurman, 2004), have led to historical and intergenerational trauma (Brave Heart, 2000; Weaver, 2009; Varcoe et al., 2021). Intergenerational trauma in this study is displayed through the normalization of IPV in some Indigenous communities. IPV advocates who also experience or witness IPV provide a sense of sameness and can be vital to building relationship with their clients (API, n.d.). Their personal resilience acts as a foundational knowledge base to promote resiliency among their clients. Resiliency is a newer concept when it comes to IPV advocates (Crann & Barata, 2021), but is effective in the healing process (Tsirigotis & Luczak, 2018).
This article has contributed to the IPV body of knowledge by highlighting personal experiences of Indigenous IPV advocates who work with Indigenous women who experience IPV. The focus of this article is important because of the dearth of literature on IPV that focuses on Indigenous women, the limited curriculum focused on Indigenous people specifically the correlation between historical trauma and IPV, and the lack of practical knowledge about Indigenous women who experience IPV. The literature that does exist regarding IPV and Indigenous women is growing (Burnette, 2015a; Burnette & Cannon, 2014), yet there is a scarce amount that focuses on the importance of recognizing the impact of historical trauma on the high IPV rates. This article supports previous literature that addresses the impact of historical trauma and the impact on IPV in Indigenous communities (Baskin, 2020; Burnette, 2015a; Burnette & Hefflinger, 2017; Burbar & Thurman, 2004; Weaver, 2009). It also provides support to the idea that the survivor advocates’ role and experience as being vital to the client's healing process (Goodman et al., 2016. Further, the information shared in this article is in line with the limited amount of research concerning the promotion of resiliency among women who experience IPV (Crann & Barata, 2021).
The findings from this study provide new insight into the IPV advocacy field. It provides a unique relationship by combining three concepts: historical trauma, Indigenous women, and resiliency. It achieves this by offering the personal experiences of Indigenous women who are IPV advocates. Their unique perspective and experience offer practitioners the opportunity to understand the correlation of historical trauma to IPV, while emphasizing the importance of breaking cycles of intergenerational trauma through resiliency.
Implications
The results of this study are valid in exploring the intersection of historical trauma, Indigenous women, and resiliency in the realm of IPV. The study offers new insight into this connection that supports existing literature on the individual concepts or the combination of a couple (e.g., historical trauma and IPV, or Indigenous women and IPV, or resiliency and IPV advocates) and provides new information regarding the link between all three. It is beyond the scope of the study to address the question of current social conditions that impact rates of IPV or address other avenues to healing beyond resiliency such as traditional Indigenous ceremonies.
Advocates at the practice level who work specifically with Indigenous women who experience IPV should recognize potential intergenerational trauma their client has faced. The recognition of historical trauma will allow the advocate to better understand the background of the client (Weaver, 2009). Understanding the connection can build trust which can allow the client to be more receptive to the advocate's assistance. Practitioners can use the concept of resiliency (Slattery & Goodman, 2009) to promote healing among their clients who experience IPV regardless of their racial or ethnic background. They can aid in the process of helping their clients become resilient as they encourage clients to, when ready, make changes to their lives. Once changes are made, they can provide techniques through counseling or therapy that serve as protective factors (Martinez-Torteya et al., 2009). Advocates can also engage in culturally appropriate approaches to align with their client's way of life (Goodkind et al., 2015). Clients who move forward despite everyday challenges (Tsirigotis & Luczak, 2018) will continue to build their hope for a brighter future and belief that they deserve a healthy life.
The information provided by the participants has the potential to address practice, social work (and related fields) curriculum, and research. It is recommended that both educators and practitioners (Indigenous and non-Indigenous) use the study's findings to guide their work. Schools of social work or human service fields seeking to incorporate both the history of Indigenous people as well as the resiliency of Indigenous people can incorporate the participants’ experience into case studies within the curricula. The focus of the study can help social work students benefit from understanding the lived experience of the IPV advocates in this study, and the implications of practice with Indigenous people and IPV survivors explicitly. Since this study centers on the experience of Indigenous peoples and the connection of historic trauma to modern-day trauma and events, such as IPV, students can become more compassionate practitioners who will aid in the healing process and promote resiliency.
Limitations
There are many limitations to this study. One limitation is the overall research design. The research design used a naturalistic and empowerment-oriented approach which requires the use of a consultant board. While the consultant board was used throughout the study, they could have been used in the final stages of both delivering the findings to appropriate communities and reviewing the article. The naturalistic approach provided information on the lived experiences of the participants, however, other methods or frameworks such as a feminist methodology could have also been used to provide balance and address any potential power differentials. Other culturally focused methodologies such as Indigenous methodology could also empower Indigenous people and aim to decolonize the research process.
The sample size is relatively small; however, this is typical in naturalistic studies to have a smaller number (Patton, 2002). A larger number of participants could possibly provide additional insights that vary from the current participants’ experience. A quantitative exploration or mixed methods approach is needed to understand the specific practices of other populations due to narrow participant criteria. Additionally, the demographics of participants are very narrow and focus on Indigenous women located in the Midwest who specifically work with Indigenous women. While intentional, it limits the focus of the study to a certain subset of the population. Future studies can include a variety of approaches that differ from the current study. For instance, future studies can explore the experiences of Indigenous IPV advocates who are male that work with Indigenous men who experience IPV. Other studies can focus on non-Indigenous advocates who work with Indigenous people who experience IPV. The research can be taken a step further and explore the voices about resiliency from other frontline workers who assist survivors. Further research is required to establish whether resiliency is a factor in relation to Indigenous advocates who work with Indigenous women experiencing IPV. Researchers can take the current research a step further and inquire about specific uses of traditional ways of resiliency such as storytelling.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.