
Abstract
Female sex workers (FSWs) face prevalent violence victimization and alcohol consumption at work, yet the bidirectional pathways between these factors are not well defined. Using cohort data from 232 venue-based FSWs in Pattaya, associations of violence and alcohol use were examined within a time period and prospectively via structural equation models. Within the time period, violence victimization and alcohol use were consistently associated; by contrast, violence was not prospectively associated with FSW alcohol use. Findings define alcohol as an important risk factor for violence in sex work environments. Alcohol safety interventions should be explored as a vital component of FSW violence prevention.
Introduction
Female sex workers (FSWs) are defined as women who regularly or occasionally receive money or goods in exchange for sexual services (United Nations Programme on HIV/AIDS [UNAIDS], 2002). Violence from clients (paying partners), human rights abuses from police, and frequent substance/alcohol use are often characteristic of the environments in which sex is sold (Decker et al., 2015; Li et al., 2010). Though alcohol use is often considered an individual behavior, in the sex work context, FSW alcohol use can be shaped by features of the work environment. For FSWs working in alcohol-serving venues such as bars or clubs, drinking alcohol with clients may be an encouraged or mandatory part of the job. FSWs may be pressured or incentivized by their managers to drink alcohol with clients (Markosyan et al., 2007; Nishigaya, 2002) or may choose to drink alcohol before sex to decrease inhibitions, increase enjoyment, or “numb” themselves to sex with clients (Kumar, 2003; Lancaster et al., 2018).
Violence victimization can be a consequence of, and a contributor to, alcohol use among survivors (Campbell, 2002; Eckhardt et al., 2015; Kilpatrick et al., 1997; Logan et al., 2002). This bidirectional relationship is defined through two primary pathways. First is the episodic pathway, in which alcohol use before sex can increase the risk of violence during that sexual encounter (Chersich et al., 2007; Decker et al., 2020; Logan et al., 2002; Testa & Livingston, 2009; Wang et al., 2007). Second is the prospective pathway, in which experiencing violence may increase the likelihood of future alcohol use among survivors to cope with their experiences (Campbell, 2002; Kilpatrick et al., 1997).
In the episodic pathway, alcohol can enable violence by decreasing FSWs' awareness and the ability to detect or escape a risky situation (Lancaster et al., 2018; Li et al., 2010; Okal et al., 2011; Wang et al., 2010). Qualitative research has shown that clients may encourage FSWs to drink alcohol to the point of inebriation or loss of consciousness, which leaves them vulnerable to rape (Panchanadeswaran et al., 2008; Schulkind et al., 2016). Additionally, for venue-based FSWs, who often meet their clients at an alcohol-serving venue, drinking alcohol with clients is common (Li et al., 2010). In these environments, clients also frequently become inebriated before sex (Li et al., 2010). Client inebriation also increases the risk of violence against FSWs via the episodic pathway, given the known risk of alcohol for violence perpetration (WHO, 2011).
In the prospective pathway, violence enables alcohol use through a survivor's approach to coping, in which a survivor may use alcohol as an avoidance coping mechanism after victimization (Hawn et al., 2020; Roth & Cohen, 1986). Longitudinal research among non sex working populations has shown that women's risk of alcohol and drug use increased significantly after experiencing violence, even among women who did not have a prior history of violence victimization (Campbell, 2002; Hedtke et al., 2008; Kilpatrick et al., 1997). Prospective studies examining violence victimization and substance use among FSW populations are sparse (Decker et al., 2020; Long et al., 2020). These studies include a Kenyan cohort study, which tracked HIV viral suppression in FSWs and found that history of partner violence was associated with current alcohol abuse (Long et al., 2020). Conversely, a recent US-based cohort study of FSWs found that daily drug injection contributed to the risk of violence victimization (Decker et al., 2020). More commonly, FSW studies are cross-sectional and show a clear, but nondirectional, association between violence victimization and FSW alcohol use (Leddy et al., 2018; Li et al., 2010; Wang et al., 2010; Zhang et al., 2013). Prospective studies are needed to unpack this widely observed but not fully understood relationship. In particular, research designs that can establish the temporality of exposure and outcome are valuable for informing alcohol and violence prevention interventions and programming in sex work settings.
Mental health factors play an important role in violence survivors’ coping processes and can affect the prospective pathway from violence victimization to alcohol use. Previous research from the general population of women has suggested that a violence survivor's later risk of alcohol abuse is mediated by psychosocial factors, such as depression levels, or psychological distress related to the violent incident (Fishbein et al., 2011; Kaysen et al., 2007; Luk et al., 2010; Miranda et al., 2002). A path analysis among college-aged survivors of sexual assault showed that violence victimization contributed to later alcohol use via its effect on increasing women's levels of psychological distress (Miranda et al., 2002). Comparable mediation analyses among FSWs using prospective data are lacking. However, cross-sectional data show that FSW depression is associated with both violence exposure (Sagtani et al., 2013; Sherwood et al., 2015; Ulibarri et al., 2013) and alcohol use (Li et al., 2010), making it a probable mediator of this prospective relationship in FSWs.
This study examines the temporal relationship between client violence victimization and FSW alcohol use before sex with clients using a prospective data set from Pattaya, Thailand. Specifically, this analysis will test the cross-sectional and prospective relationships between violence and alcohol use before sex using structural equation modeling across two time points. This design informs the context of FSW alcohol use as a contributor and/or consequence of violence victimization, with implications for addressing these pressing and intersecting health issues in the Thai sex work environment.
Methods
Data Collection
This study is a secondary data analysis from a quasi-experimental study designed to evaluate a safety promotion intervention among FSWs in Pattaya, Thailand. The parent study recruited 401 FSWs via proportional-to-size venue-based sampling from two sex work zones/hotspots in Pattaya assigned as intervention (n = 201) and control (n = 200) areas. The intervention entailed a specially trained outreach team that provided semiscripted messages on health and safety topics, including workplace safety, empowerment, and resources for violence-related support. All participants were assessed by interviewer-administered survey at baseline (May 2017) and at 14 weeks follow-up (September 2017). Study procedures were led by Mahidol University and approved by the Institutional Review Board at the Institute for Population and Social Research, Mahidol University, in Nakorn Pathom, Thailand.
At baseline, every known social venue (beer bars and dance clubs known as a-go-gos) in Pattaya (n = 142) was visited by data collectors; between two and six FSWs were sampled from each venue based on venue size. Within venues, consenting participants were selected based on availability and eligibility criteria. Participants were eligible if they were born female, were 18 years or older, spoke Thai, and had sold or exchanged sex for money or goods in the past three months in Pattaya. Data were collected face-to-face using electronic tablets and surveys lasted approximately 15–20 minutes. All baseline surveys were conducted in a private space at the venue where the participant worked.
As part of baseline data collection, all participants were asked for their contact information to be contacted for an additional survey at 3-month follow-up to reassess them on all baseline measures. Participants were contacted for a follow-up survey through a mixture of calls, texts, and in-person visits to the participants’ respective venues. Data collectors scheduled follow-up data collection at a time and location that was most convenient for the participants, including at bars, hotels, restaurants, or by phone. Of the 401 FSWs enrolled at baseline, data collectors located 232 (58%) of participants at follow-up. The primary reason for the loss to follow-up (LTFU) was that the participant moved at some point during the study period and was no longer working in Pattaya. This analysis used data from retained participants who have data from both baseline and follow-up timepoints (n = 232). This analytic sample includes 124 participants from the intervention and 108 participants from the control group.
Measures
All measures in this study are self-reported. Survey questions were drafted in English, translated and pretested in Thai by bilingual study investigators, and back-translated to ensure consistency of question meanings across languages.
Primary variables
A primary variable of interest in this study's model is FSW sex with clients while inebriated (SWI) in the past 3 months at baseline (T1) and follow-up (T2). SWI is measured as a binary variable for a participant who reported “always,” “often,” or “sometimes” having three or more alcoholic drinks before having sex with a client in the past three months vs participants who reported “never” or “rarely.” Inebriation depends on sex, weight, genetics, and other factors but occurs at blood alcohol concentrations around 0.08 g/dl (three to four drinks for women) according to the National Institute on Alcohol Abuse and Alcoholism (National Institute of Alcohol Abuse and Alcoholism, 2004).
The second primary variable is FSW experiences of client violence victimization in the past three months at baseline (T1) and follow-up (T2). Participants were considered to have experienced client violence if they responded “yes” to having “a client do any of the following things to you” in the past three months: “yelled at you,” “made you feel bad about yourself,” “hit, punched, slapped or otherwise physically hurt you,” “used violence, force, or threats to have sex or sex acts that you did not want,” “only paid for sex once, but then demanded to have sex multiple times,” or “brought more people to have sex with you than was agreed upon.” Response options are modeled after the well-tested revised Conflict Tactics Scale (Straus et al., 1996), and sex work-specific items were taken from previous literature describing violence against FSW (Panchanadeswaran et al., 2008; Wang et al., 2010; Zhang et al., 2013).
FSW depressive symptoms at T1 were measured by the two-question Patient Health Questionnaire (PHQ-2) depression screener (range 0–6) (Kroenke et al., 2003) and measured as a binary variable where participants who reported PHQ-2 score ≥ 3 were defined as being at risk of depression (Kroenke et al., 2003).
Adjustment variables
Potential confounders include demographic, psychosocial, social, and community environment variables measured at T1 that may be associated with the primary variables of interest in the model. Demographic variables included age, age of when the participant first sold sex, the primary reason why a woman entered sex work (e.g., coercion, enjoyment, to meet a need), marital status, education level, venue type (beer bar or a-go-go), primary living arrangement in the past three months (e.g., renting, living with partner), and average client number per week. Psychosocial variables included FSW self-efficacy related to condom use and safety. Each was measured as a participant's agreement to the statements “I am confident in my ability to negotiate condoms” or “stay safe during sex work” on a 5-point Likert scale (1 [strongly disagree] to 5 [strongly agree]). Social and community environment variables included FSW social support from co-workers, measured through a two-item abridged social cohesion scale from Kerrigan et al. (range 2–10) (Kerrigan et al., 2007; Lippman et al., 2010). Participants indicated their agreement on a Likert scale (1 [strongly disagree] to 5 [strongly agree]) to two statements assessing if FSWs felt they could “count on other sex workers” if they needed to talk about their problems or “borrow money.” FSW postviolence support from venue managers and police were each measured through FSW agreement on a Likert scale (1 [strongly disagree] to 5 [strongly agree]) with the statements “If I experienced violence, I could get help from my bar manager” or “from the police,” respectively. Lastly, the participant intervention group in the parent study was included and defined as a binary variable for intervention or control group.
Data Analysis
All analyses were conducted in STATA 15.0 (StataCorp, 2017). The significance level α was set at 0.05. Clusters are defined at the venue level, and all analyses are adjusted for venue-level clustering to account for likely nonindependence of participants (Huber, 1967; Jayatillake et al., 2011). Overall, missingness was low (<5%), except in SWI at baseline (9.4% missing). All variables with missingness were imputed at the sample mean and rounded to the nearest integer for binary variables. Models were run with both the imputed and nonimputed SWI variable in sensitivity analyses.
Attrition analyses were conducted to assess the baseline characteristics of participants who were lost to follow-up (LTFU) compared to those who were retained via cluster chi-squared tests (Herrin, 2012). Participants were similar, except that participants who were LTFU were more likely to have experienced client physical or sexual violence (5.9% vs. 2.2%, p = .05), report higher depressive symptoms (16.0% vs. 10.3%, p = .06), and have fewer clients (average 1 client per week vs. 2.2 p < 001) during the past 3 months at baseline compared to retained participants.
In preliminary analysis, all potentially confounding demographic, psychosocial, social, and environmental variables were assessed for association with client violence at T1 and SWI at T2 using clustered t-tests or chi-squared tests (Herrin, 2012). Variables that were associated with either client violence at T1 or SWI at T2, at the p < .05 level, were included as adjustment variables in structural equation models.
Main analysis: Generalized structural equation modeling
Generalized structural equation models (GSEM) were built to assess the temporal relationships between SWI and client violence during two time periods of baseline (T1) and follow-up (T2). The current GSEM models are estimated with maximum likelihood, Bernoulli distribution of endogenous variables, and logit link specified. The regression models include robust standard errors adjusted for venue-level clustering.
A series of GSEMs were built to assess the relationship between key exposure and outcome variables (client violence and SWI) at both time points. Firstly, a basic model was built to assess these relationships before adjustment, and then adjustment variables were added if they were associated with either client violence or SWI in the preliminary analysis. These variables include participant age, age of starting sex work, self-efficacy for condom use, client number, and intervention group (see Appendix A. Progressive GSEM models). The participant intervention group was not associated with violence exposure, but was related to alcohol use at work. Finally, depression was added as a mediator on the pathway from client violence (T1) and SWI (T2) (Fishbein et al., 2011; Kaysen et al., 2007; Luk et al., 2010). This approach also allows for the calculation of the proportion of the relationship between client violence and SWI that is mediated by depressive symptoms (mediated proportion = indirect effect via depression/ total effect) (Ditlevsen et al., 2005).
The final GSEM includes a system of equations to assess the relationship between client violence and SWI across two time points, adjusted for other variables in the system [Figure 1]. The model computes the difference in log odds of experiencing violence at T1 comparing those that reported SWI versus no SWI at T1 (λ7) and the difference in log odds of experiencing violence at T2 comparing those that reported SWI vs. no SWI at T2 (λ5). Additionally, the model computes the difference in log odds of SWI at T2 comparing those exposed to violence versus those not exposed at T1 without depression mediation (λ2) and with depression mediation (λ2 + λ4 × λ3). Other pathways of interest in the system include the relationship between violence across timepoints from T1 to T2 (λ6) and SWI across timepoints from T1 to T2 (λ1).
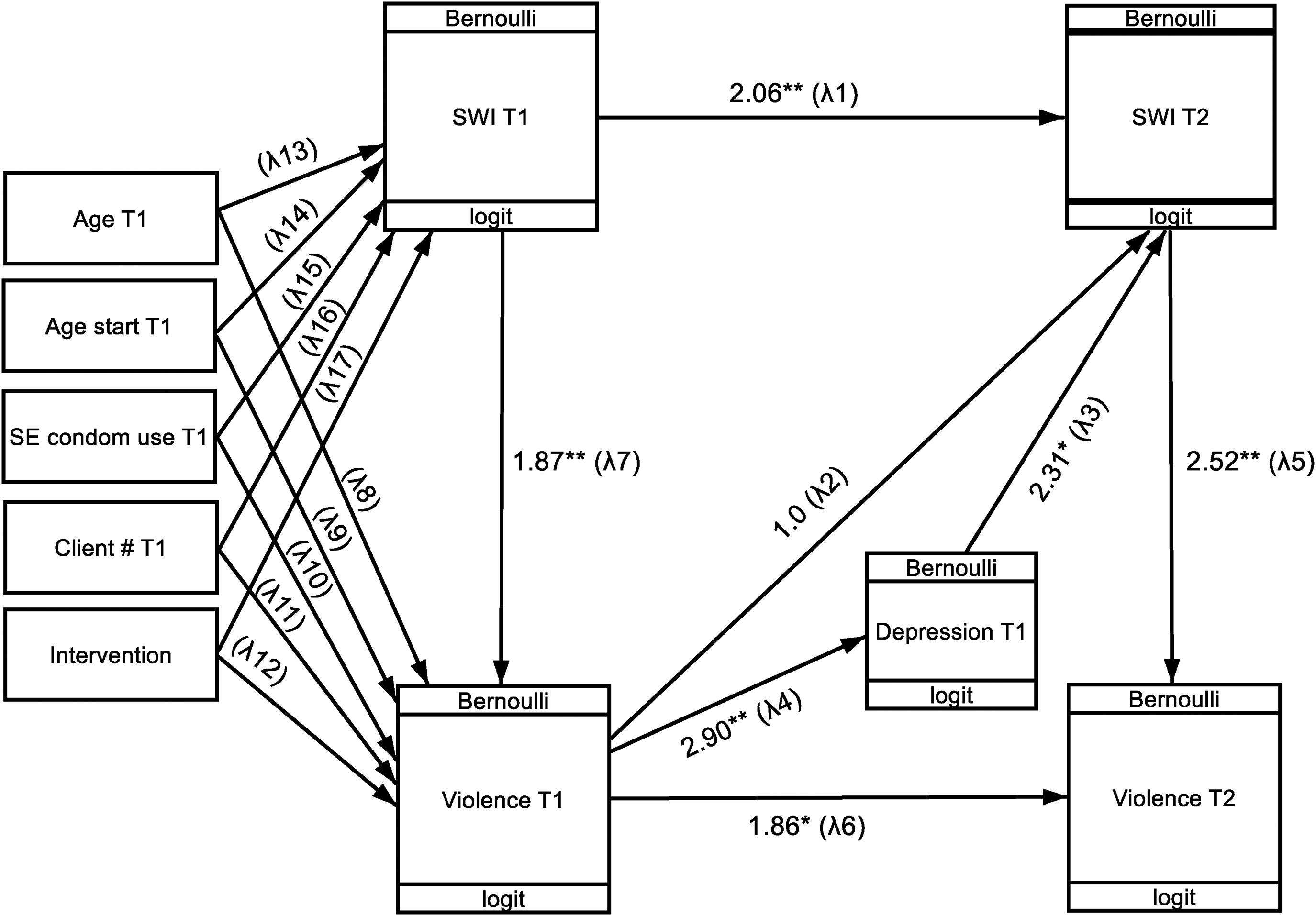
Structural equation model diagram of the relationship between experiencing client violence and having sex with clients (past 3 months) while inebriated in two timepoints. **Significant at p < .05 level. *Significant at p < .10 level.
Sensitivity analyses
For a sensitivity analysis, the final GSEM was rerun with nonimputed data of SWI at T1, dropping the sample size from n = 232 to n = 210 in imputed models (see Appendix B. GSEM sensitivity analysis nonimputed data). All other aspects of model specification remained the same. Additionally, because the directionality of the association between SWI and violence exposure within a time period is unknown, the GSEM was rerun with the direction of the cross-sectional association between violence and SWI reversed at both timepoints. Specifically, violence victimization was modeled as the exposure variable and SWI was modeled as the outcome variable within each time period (see Appendix C. GSEM sensitivity analysis reverse directionality).
Results
FSWs in this sample were an average of 33.8 years old, had started sex work at the age of 28.9, and had an average of two clients per week. The majority (62.5%) entered sex work to meet a basic need, were divorced or widowed (60.8%), worked at a beer bar (70.7%), and lived in a place they were renting or owned (87.1%). Participants had a mix of educational attainment, with about a third completing primary school or less (34.1%), secondary school (31.5%), and high school or more (34.5%). Overall self-efficacy for condom use (4.6, range 1–5) was higher than self-efficacy for safety (3.9, range 1–5). Postviolence support from bar managers (4.3, range 1–5) and family/friends (4.2, range 1–5) was higher than postviolence support from the police (3.7, range 1–5) [Table 1].
Sample Characteristics of FSWs Grouped by Violence Exposure and SWI in the Past 3 Months (n = 232).
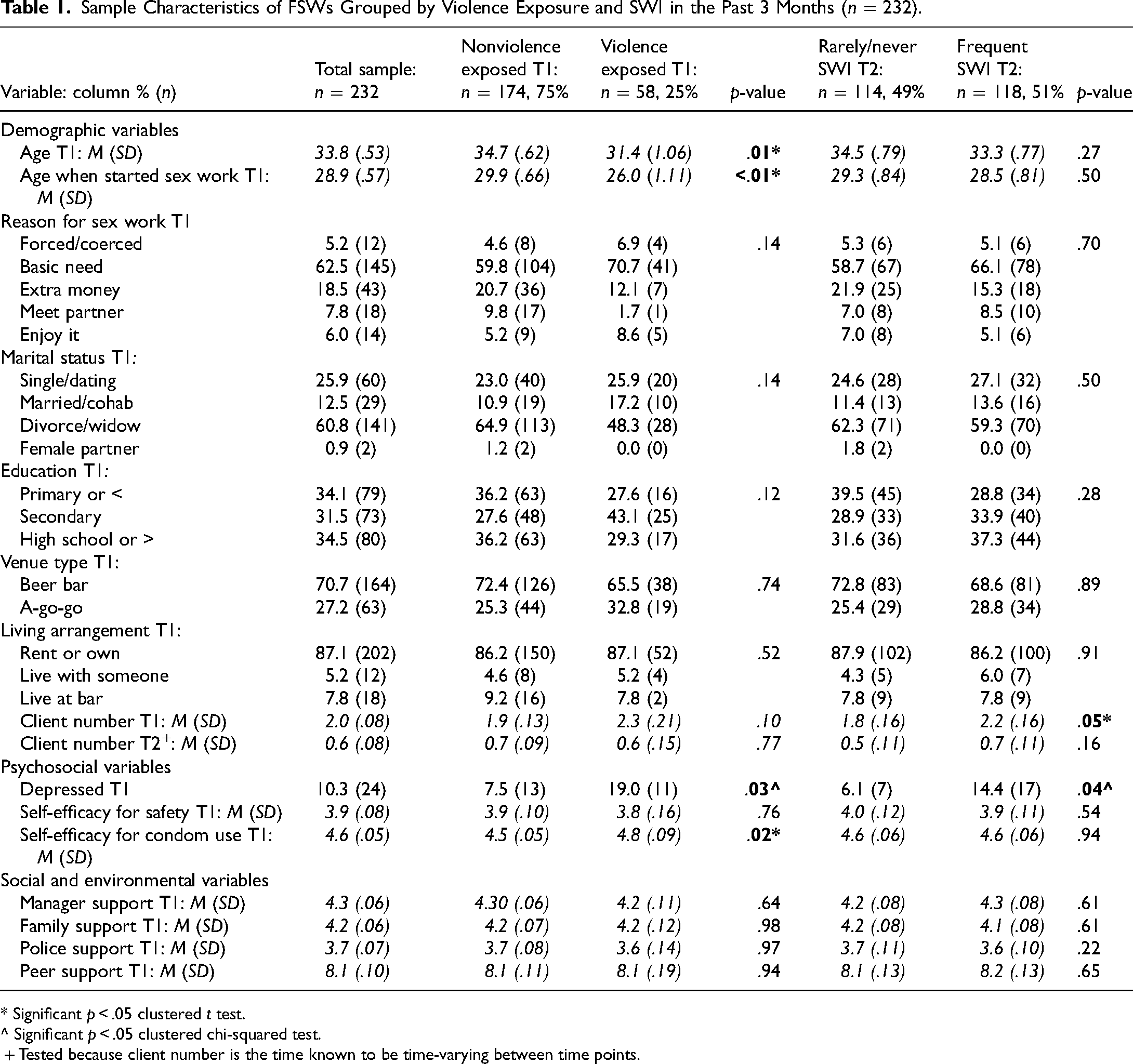
* Significant p < .05 clustered t test.
^ Significant p < .05 clustered chi-squared test.
+ Tested because client number is the time known to be time-varying between time points.
In this sample, 25% (n = 58) of FSWs reported experiencing violence. By category, 19% (n = 44) reported experiencing sexual threats such as clients bringing more people to have sex than was agreed or demanding sex multiple times, 11% (n = 26) reported verbal or emotional abuse such as being yelled at or made to feel bad, and 3% (n = 5) reported sexual or physical violence such as being hit, slapped, or forced to have sex. FSWs who had experienced client violence in the past 3 months at T1 were younger (31.4 years vs. 34.7 years, p < .05) and had started sex work at an earlier age (26.0 years old vs. 29.9 years old, p < .01). Women who experienced client violence at T1 were also more likely to have depressive symptoms (19.0% vs. 7.5%, p < .05) and had higher self-efficacy for condom use (4.8 vs. 4.5, p < .05) at T1. FSWs who experienced SWI in the past 3 months at T2 (n = 118, 51%) were more likely to have depressive symptoms (14.4% vs. 6.1%, p < .05) and had higher average numbers of clients per week (2.2 vs. 1.8, p < .05) at T1 (Table 1).
Generalized Structural Equation Model Results
Final GSEM results show the adjusted relationship between client violence and SWI with clients through the episodic and prospective pathways. In the episodic pathway, GSEM results show that both within time periods T1 and T2, SWI was significantly cross-sectionally associated with client violence. FSWs who reported SWI with clients in the past 3 months were more likely to have experienced violence by clients during this same time period both at baseline (aOR 1.87, 95% CI 1.04–3.37), and at follow-up (aOR 2.52, 95% CI 1.24–5.10). In the prospective pathway, examining the prospective relationship between client violence at T1 and SWI at T2, model results show client violence at T1 was not associated with SWI at T2 (total effect aOR 2.43, 95% CI 0.61–9.67) [Figure 1 and Table 2].
GSEM Model Results of the Relationship Between Experiencing Client Violence and Having Sex With Clients (Past 3 Months) While Inebriated in Two Timepoints (n = 232).
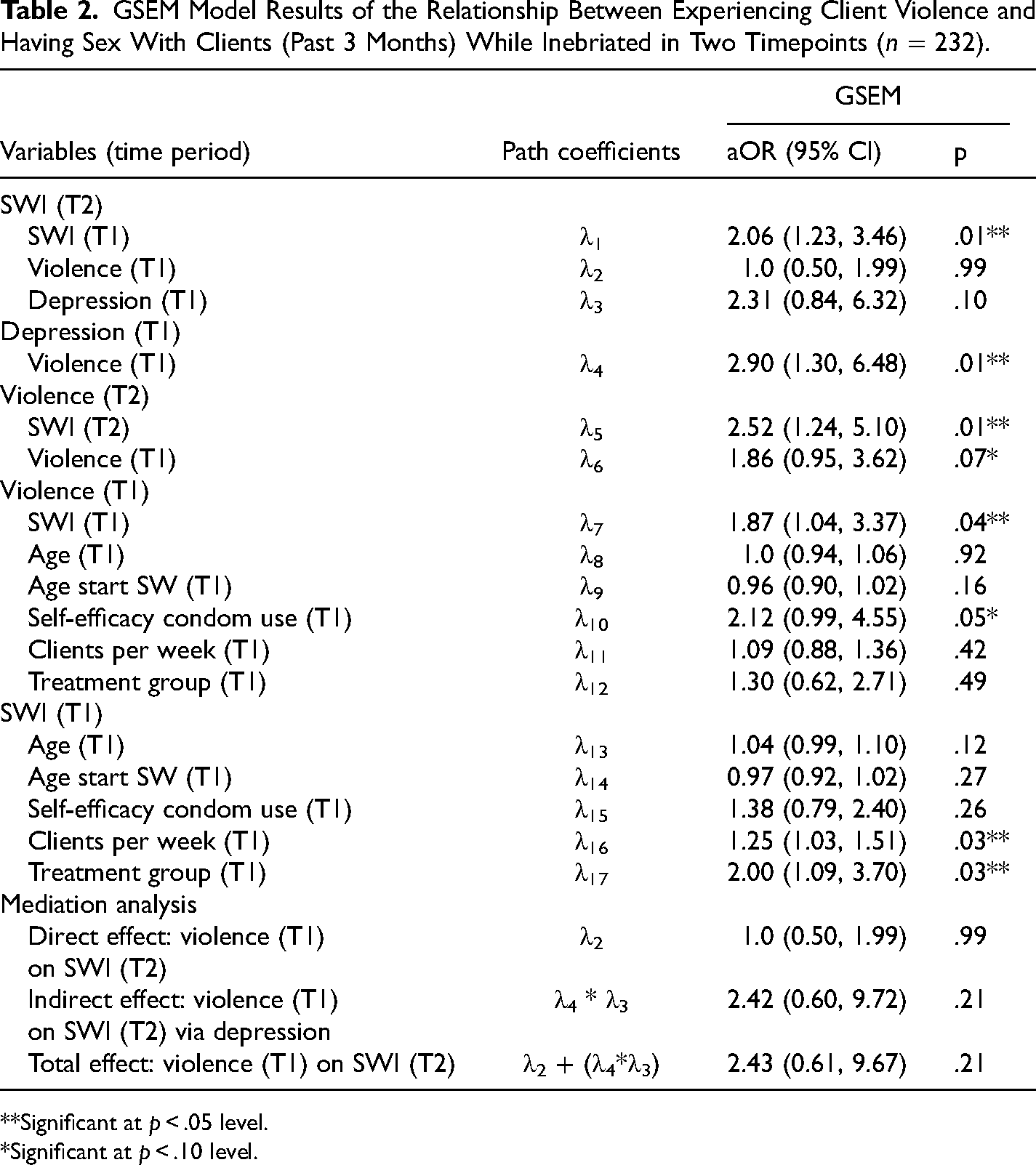
**Significant at p < .05 level.
*Significant at p < .10 level.
Along the prospective pathway, model results show that there was no direct relationship between violence at T1 and SWI at T2 (aOR 1.0, 95% CI 0.50–1.99), nor was there a significant indirect relationship between these variables via depressive symptoms (aOR 2.42, 95% CI 0.60–9.72) [Figure 1 and Table 2]. While no pathway was statistically significant, the observed relationship between client violence at T1 and SWI at T2 was almost fully mediated by FSW depressive symptoms (mediated proportion = 99%). In mediation analysis, the indirect effect of client violence at T1 on SWI at T2 via depressive symptoms (aOR 2.42) is divided by the total effect of client violence at T1 on SWI at T2 (aOR 2.43), showing a depression-mediated proportion of the pathway to be 99% (2.42 / 2.43 = .99).
Sensitivity Analyses
In the GSEM using nonimputed data for SWI at T1 (n = 210), all interpretations of path coefficients remained the same compared to the imputed model. Additionally, in the GSEM that reversed the direction of the association between violence and SWI (regressing violence on SWI at T1 and T2), all interpretations of path coefficients remained the same as the reported model.
Discussion
This study is among the first to prospectively examine the relationship between alcohol use and violence victimization in the sex work context. Results support an episodic relationship between alcohol use and violence victimization rather than a prospective relationship between previous violence and later alcohol use. Findings emphasize that the sex work venue environment is a risky setting for client violence that may be further facilitated by inebriation before sexual encounters. Venues can enable or prevent violence against FSWs depending on their alcohol and safety policies and practices. For example, venues which require or incentivize FSWs to drink alcohol with clients may be enabling violence. Conversely, venues can promote FSW safety by instituting strong alcohol safety policies which allow women to stop drinking alcohol if they desire and put in safety plans for women who will be leaving the bar inebriated to serve clients.
These results extend past work examining violence victimization and alcohol use among FSWs, which has left unanswered questions about the temporality and mechanisms of the relationship (Leddy et al., 2018; Li et al., 2010; Wang et al., 2010; Zhang et al., 2013). Our study supports the interpretation that alcohol use is a risk factor for client violence and implies that alcohol interventions may help prevent client violence in sex work settings. Our results build off a randomized controlled intervention trial among FSWs in Kenya, which tested the effects of a brief alcohol intervention on sexual risk factors (L'Engle et al., 2014). This study showed that an alcohol-reduction intervention significantly reduced FSW alcohol use and sexual violence from clients over a 12-month period. Researchers interpreted the reduction in client sexual violence to be a result of decreased alcohol use (L'Engle et al., 2014). Dissimilar to the Kenyan study, which measured “harmful” alcohol use in general (L'Engle et al., 2014), our study measures alcohol use before sex with clients in the venue setting. Our results add to the literature by showing that the sex work venue environment is both a risky setting for violence and alcohol use and an important setting for implementing alcohol and safety-promotion interventions.
In Pattaya, and other venue-based sex work settings, alcohol inventions could be designed based on internationally recognized alcohol messaging (WHO, 2001) and adapted based on community-generated messaging and safety strategies. Individual-level counseling sessions have previously shown promise in reducing FSW alcohol use (Carrasco et al., 2016; L'Engle et al., 2014). However, given the complexity of factors contributing to alcohol consumption in the sex work environment, community and venue-level alcohol programming would likely be more effective than individual-level interventions alone. For example, interventions could target venue managers with alcohol messaging and techniques to support the health and safety of their staff. Qualitative research has found that a primary reason why FSWs in Pattaya choose to work outside of venues is to avoid venue-mandated alcohol drinking with clients (Phuengsamran, 2007). Venues can support the safety of FSWs by eliminating any requirements for staff to drink alcohol. Venues can also support FSWs who want to stop drinking but are experiencing pressure from clients and can help implement safety plans for women who are inebriated after leaving the venue. To date, the majority of alcohol programming among FSWs is focused on FSW reducing their individual consumption (Carrasco et al., 2016; Li et al., 2010). This study highlights the violence-related risks of alcohol consumption in the venue environment and supports the development of venue-level alcohol interventions for FSW.
This study does not find a significant prospective association between client violence and later SWI with clients. These findings suggest that overall FSW alcohol use during sex with clients did not increase after victimization, contrary to our hypothesis of greater engagement in alcohol use to cope. This may be because FSWs in Pattaya drink alcohol at work for a variety of reasons, such as venue requirements, which made it more difficult to detect drinking related specifically to coping after violence. The null finding may also be related to our measure of client violence, which was relatively short-term (past 3 months) and did not encompass a woman's more frequent or longer-term exposure to violence. In comparison, other studies showing that alcohol use increased after violence victimization have focused on experiences of intimate partner violence (IPV) among non sex worker populations of women (Campbell, 2002; Devries et al., 2014; Ellsberg et al., 2008; Hedtke et al., 2008; Kilpatrick et al., 1997). IPV may constitute a more sustained or frequent exposure to violence compared to client violence. It may be that the alcohol-related consequences of violence are more likely to occur in the contexts of IPV or more sustained exposures to violence. Future studies on the impact of violence victimization on FSW alcohol use may consider measuring FSW alcohol use outside of work in addition to different lengths, frequencies, and severity of violence exposure.
A coping pathway from violence to increased alcohol use may still exist for some individuals based on other psychosocial or mental health factors not measured in this study. Alternatively, individuals may be using alcohol to cope more generally, outside of sexual encounters with clients, and this would not have been captured in our survey questions. Indeed, previous literature has shown that alcohol use increased post-victimization for survivors who had higher levels of psychological distress related to the incident (Miranda et al., 2002). Our models showed that depressive symptoms were a near full mediator of the relationship between violence victimization to SWI, despite the pathway remaining statistically nonsignificant. It follows that FSW mental health and psychological response to trauma may be a determinant of the relationship between violence victimization and later alcohol use. Our study, however, may be underpowered to see the effects of depression in mediation analysis. Future studies on the alcohol-related consequences of violence should examine the influence of depressive symptoms and other psychological factors that are related to FSWs coping after trauma.
Limitations
Design limitations include the lack of event-level data. Our cross-sectional data analysis shows a clear association between violence and SWI within the same time period, but we cannot determine if SWI and the experience of client violence occurred within the exact same episode of sex work. Additionally, the direction of cross-sectional association between violence and SWI in the GSEM is drawn based on theory and the true direction of the association is unknown. However, study findings are bolstered by sensitive analyses, which reversed the direction of the regression pathway, and showed that there was no change in the interpretation of the path coefficients.
There are also several limitations to the measures in this analysis. First, this study did not include any information from the client on violence perpetration or their alcohol use. Client's alcohol use is a known contributor to violence perpetration (WHO, 2011) and likely confounds the relationship between FSW alcohol use and violence victimization. Second, this study does not measure or adjust for venue requirements for FSW alcohol consumption at work, which likely impacted FSW alcohol consumption. Third, this analysis measures violence exposure as any client violence in the past 3 months, inclusive of verbal and emotional indicators of violence. Restricting this analysis to only those who experienced physical or sexual violence (n = 5) was not possible due to sample size but may have yielded different results. This measure of violence also does not record a woman's full history of abuse over her life, or violence from other types of perpetrators including nonpaying intimate partners. These forms of violence may represent other unmeasured confounders affecting FSWs' SWI. However, in this FSWs sample, few women (1.7%) reported experiencing violence from nonpaying partners.
Conclusion
This study provides greater clarity on the nature and timing of the relationship between alcohol and violence and informs prevention programming in the sex work context. Study results highlight the violence-related risks of FSW alcohol consumption before sex with clients. Alcohol interventions that target FSWs' work environments could be effective violence prevention in these risky settings. Given the social and environmental contributors to FSW alcohol use, alcohol interventions that target venue managers and improve venue policies on alcohol safety are likely to be more effective than those targeting FSW behavior alone. Scaling up interventions to improve the safety of FSWs’ work environments is a priority to uphold the health and human rights of this vulnerable population.
Footnotes
Acknowledgements
Thank you to the many participants who generously donated their time to take part in this research. Thank you to the dedicated data collectors from IPSR and outreach workers from SWING for their excellent work. Thank you to the Sexual Violence Research Initiative and World Bank Development Market-place for funding this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.