
Abstract
Bystander intervention has rapidly emerged as a strategy for preventing sexual violence. Yet, few studies have considered LGBTQ+ victim-survivor's experiences of bystander intervention, or LGBTQ+ community members bystander intentions and behaviours. This article presents findings from two exploratory surveys with LGBTQ+ victim-survivors of sexual violence and general community members based in NSW, Australia. Findings suggest that experiencing bystander intervention was not common for victim-survivors, and that sexuality did not significantly influence participants’ bystander intentions or behaviours, though being a victim-survivor of sexual violence did. We consider the implications of these findings for bystander intervention training and future research.
Introduction
Bystander intervention (BI) has rapidly emerged as a strategy for preventing and responding to sexual violence (SV), with a growing body of research and educational programs implemented in this space (Mainwaring et al., 2023). Bystanders are individuals who witness SV occurring or about to occur, or who witness the enactment of attitudes and norms that underpin SV, such as sexist ‘jokes’ (Banyard, 2011; Mainwaring et al., 2023). In such scenarios, bystanders have the choice to do nothing, to take action that exacerbates the violence, or to take action that prevents or interrupts the violence (Banyard, 2011). BI can also occur in the aftermath of SV. Thus, as Mainwaring et al. (2023) observe, BI can occur as forms of primary, secondary and tertiary prevention, and as direct intervention as SV is unfolding. BI constitutes a range of direct and indirect strategies (Hoxmeier & McMahon, 2021). These strategies are often represented through the ‘5D’ model: distract (where a distraction or diversion is created to disrupt a perpetrator's actions, such as striking up a conversation with their target); delegate (asking someone else to intervene, such as an authority figure); direct (confronting a perpetrator about their actions); document (recording what is happening); and delay (supporting a victim-survivor in the aftermath of SV). Importantly, BI aims to shift the responsibility of preventing or responding to SV away from victim-survivors by positing that we all have a role to play (McMahon, 2024).
However, as Hoxmeier and colleagues (2022) have recently observed, research and training on BI is overwhelmingly cis- and heteronormative in its approach (see also Coulter et al., 2024; Mainwaring et al., 2023). That is, scholarship and educational initiatives to date have been underpinned by the assumption that SV is almost exclusively perpetrated by cisgender heterosexual men against cisgender heterosexual women. To be clear, we do not dispute the gendered nature and drivers of SV or that cisgender heterosexual women are significantly impacted as victim-survivors. Nonetheless, a heteronormative framing is unable to account for diverse experiences of SV, including those of LGBTQ+ people (Erbaugh, 2007; Hindes et al., 2026; Ison et al., 2026; Mortimer et al., 2019). With a few recent exceptions, research in the field of BI has not examined LGBTQ+ people's bystander behaviour, intentions and readiness to intervene, or LGBTQ+ victim-survivors’ experiences of BI. It is these gaps that our studies aimed to address.
Simultaneously, a rapidly growing body of evidence demonstrates that LGBTQ+ people experience disproportionately high rates of SV (Hindes et al., 2026; Ison et al., 2026). In the Australian context from which we write, just under half (48.6%) of LGBTQ+ participants in the national Private Lives 3 study reported having ever experienced sexual violence (Hill et al., 2020), and these rates largely reflect international findings (e.g., Krahé & Berger, 2013; Potter et al., 2020). Given the high rates of SV experienced by LGBTQ+ people, it is imperative that we understand BI within this context. As we establish further in the ensuing discussion, it is currently unclear to what extent LGBTQ+ victim-survivors experience BI, or the extent to which LGBTQ+ community members have intervened, or are prepared to intervene, as bystanders. In contributing to this significant gap, we present findings from two exploratory, mixed-methods surveys with LGBTQ+ victim-survivors and community members and consider the implications for future research and practice in the field of BI.
Literature Overview
Effectiveness of BI as An Intervention/Prevention Strategy
While BI has emerged as a promising avenue for preventing SV and other iterations of gender-based violence, to date the overwhelming bulk of research has assessed people's perceptions of their readiness, confidence, and efficacy in intervening, and, to a lesser extent, whether they took action if they had an opportunity to do so (Banyard et al., 2016; Fileborn, 2017; Hamby et al., 2016; McMahon, 2024). There has been considerably less focus on the outcomes or impacts of intervening – something we aim to address in this work by exploring participants’ experiences of enacting and receiving BI (Banyard et al., 2019). Mainwaring and colleagues’ (2023) review found that bystanders are more likely to intervene in practice if they report a sense of responsibility and confidence to intervene. Training in bystander intervention has been associated with positive changes in participants’ knowledge and beliefs about sexual and other forms of interpersonal violence (Banyard, 2008; 2015; Lynch and Fleming, 2005; McMahon, 2015), and with reduced levels of SV (Coker et al., 2016; Cook & Reynald, 2016). However, a recent review of college-based BI training by Kirk-Provencher et al. (2023) found that few programs included content that explicitly addressed sexual and gender minorities (SGM) (see also Leone et al., 2024), and none of the identified program evaluations assessed the outcomes of training for SGM participants. As such, we know little about the efficacy of BI training for LGBTQ+ people as potential bystanders, and the content of contemporary training programs often obscures the possibility that LGBTQ+ people may use or experience SV.
There are currently few studies examining the use and impacts of BI in practice. Of the small number of studies investigating BI ‘in action’, findings are mixed. Studies from Hamby et al. (2016), Fileborn (2017), Hoxmeier and McMahon (2021), and Seo et al. (2022) suggest that BI does not commonly occur in practice. Seo et al.'s (2022) study found that participants who had witnessed different forms of violence were more likely to intervene for friends compared to strangers. Moreover, while BI can work to successfully intervene in sexual and other violence when it is occurring, it can also have unintended negative outcomes, such as exacerbating the situation or resulting in harm to the bystander (Fileborn, 2017; Hamby et al., 2016; Hoxmeier & McMahon, 2021). However, Fileborn's (2017) research on street harassment indicates that BI can help victim-survivors feel as though a sense of justice has been achieved, for instance because BI expresses disapproval of those who cause harm and validates victim-survivors’ experiences. BI can also facilitate a sense of safety in the aftermath of harassment. McMahon's (2024) qualitative study with victim-survivors who had experienced BI similarly found that intervention could provide support and validation, and in some cases successfully stopped the actions of the person using violence. Thus, while BI appears to be uncommon in practice and not always effective, there is evidence to suggest it can hold great value to victim-survivors.
Overall, there is a clear need for further research documenting the impacts and outcomes of BI in practice – and particularly so in the context of LGBTQ+ SV – something which our studies aimed to shed light on. As McMahon (2024: 576) observes, understanding the outcome of BI is important given these form part of the “feedback loops” conceptualised by Banyard (2015) that can impact whether bystanders intervene again in the future. Moreover, as BI is increasingly emphasised in educational and preventative initiatives, it is vital to understand whether – and in which contexts – BI is effective at preventing or disrupting SV.
Barriers to Intervention
In addition to the fact that BI appears to be rare in practice, there is a wealth of research demonstrating the significant barriers that potential bystanders can face in intervening. Diffusion of responsibility is a well-documented barrier, with bystanders assuming someone else will intervene, particularly in scenarios where it is unclear who has responsibility to act (Banyard et al., 2004; Cook and Reynald, 2016). Bystanders can lack the knowledge, skills or confidence to intervene (Banyard et al., 2004; Ovenden et al., 2019). For example, as a basic starting point, BI requires the ability to recognise when SV (or precursors to violence) is occurring. The potential for social embarrassment can also inhibit intervention, for example because a bystander believes that they are the only person who thinks something is wrong (Leone et al., 2024; Mainwaring et al., 2023). Bystanders may also hold concerns for their personal safety (Banyard et al., 2019; Ovenden et al., 2019), and it is of course important to acknowledge that intervention can be accompanied by significant personal risk. As Carmody (2009) suggests, ‘ethical’ BI necessitates foregrounding the bystanders’ safety.
Gendered norms also shape BI (Amar et al., 2014; Burns et al., 2019). Studies suggest that women are more likely to recognise and express a willingness to intervene in sexual and other violence (Banyard & Moynihan, 2011; Leone et al., 2024), although this is not a consistent finding across the literature (Mainwaring et al., 2023). Explanations for this gendered difference include women's higher likelihood of experiencing different forms of gendered violence, meaning they may be more likely to recognise this violence when it occurs, and to empathise with other victim-survivors (Hoxmeier et al., 2022; Leone et al., 2024). It is plausible that this explanation also extends to LGBTQ+ people, given the high rates of sexual and other violence experienced by these communities. Some evidence for this is provided by Hoxmeier et al. (2022), who found that SGM groups reported more opportunities to intervene than cisgender heterosexual participants. Conversely, overall, cisgender men are more likely to adhere to rape myths and misperceptions that narrow the scope of ‘what counts’ as SV (Baillie et al., 2022; Banyard, 2011; Cook & Reynald, 2016; McMahon, 2015). Gender can also shape the form that BI takes, with women tending to intervene in indirect ways, while men are more likely to respond using visible and direct tactics (Banyard, 2015; Mainwaring et al., 2023). BI is, thus, deeply entangled in the performance of gender, and may also serve to shore up the gendered norms and power structures that underpin SV. However, the role that gender plays in shaping BI for LGBTQ+ communities is less clear, particularly for individuals whose gender sits outside of the man/woman binary.
Current research on gendered norms and rape myths holds direct relevance for BI in relation to LGBTQ+ SV. As Graham and colleagues (2023: NP3982) observe, adherence to stereotypical gendered norms can “lead to the belief that only women can be victims and men can be perpetrators”, and this may function as a barrier to recognising and subsequently intervening in violence occurring in non-heteronormative relationship contexts. Similarly, norms pertaining to masculinity and sex can construct men as ‘unrapeable’, again impeding the potential for bystander intervention to occur (Graham et al., 2023; Kirk-Provencher et al., 2023). In short, heteronormative constructions of SV may render invisible the experiences of LGBTQ+ people as both victim-survivors and perpetrators of this violence. However, overall, much less is known about how diverse sexuality and gender shapes engagement in BI, or whether bystanders intervene in SV occurring outside of a heteronormative context (Coulter et al., 2024; Hoxmeier et al., 2022; Leone et al., 2024). Our studies aimed to shed light on the roles that diverse gender and sexuality might play in relation to BI.
BI and LGBTQ+ Communities
Recent research from Coutler et al. (2024) represents one of the only studies to explore SV knowledge, prevention behaviours, and care-seeking behaviours for people across diverse genders and sexualities. They found that women, gender diverse people and sexual minority participants had, overall, “greater SV knowledge, prevention behaviours, and care-seeking behaviours” compared to cisgender heterosexual men (Coulter et al., 2024:594). This included a higher likelihood of intending to intervene as a bystander. Graham et al. (2023) used audio vignettes depicting intimate partner violence (IPV) across different relationship configurations. They similarly found that LGBQ+ participants were more likely than heterosexual participants to intervene, as were participants with lower levels of rape myth acceptance and greater support for gender equality. Notably, participants in Graham et al.'s (2023) study were most likely to intervene in a vignette depicting heteronormative IPV. Conversely, Leone et al. (2024) hypothesise that (what they term) sexual minority groups may face additional barriers to intervening as a bystander, including an increased risk of experiencing violence. Hoxmeier et al. (2022) similarly found that while SGM participants reported more opportunities to intervene in sexual and intimate partner violence, this did not consistently translate into higher rates of bystander action. They found that cisgender bisexual women and cisgender gay men reported higher rates of intervention compared to heterosexual cisgender participants. Transgender and gender non-conforming participants reported a lower likelihood of intervention, something the authors attribute to the barriers faced by these groups, particularly the risk of experiencing violence themselves.
Beyond these important contributions, we know exceedingly little about BI and LGBTQ+ communities. This small body of work suggests that LGBTQ+ people may be more likely to intervene, but there is a clear need for further empirical research, and the few studies that have been conducted have predominantly drawn on US college student samples (Mainwaring et al., 2023). Studies that have included LGBTQ+ participants have tended to collapse diverse identities into a single ‘SGM’ group, with little work examining differences across the diverse LGBTQ+ communities (Hoxmeier et al., 2022). As we established earlier, a growing wealth of evidence illustrates that LGBTQ+ people experience disproportionately high rates of SV. Given this, there is a need for research that examines LGBTQ+ people's experiences of, and intentions in relation to, BI to inform education and prevention initiatives (see also Graham et al., 2023; Kirk-Provencher et al., 2023; Leone et al., 2024). Findings from our study suggest that LGBTQ+ people can face significant barriers to help-seeking, such as reporting to police or accessing crisis services, so BI may take on increased significance in this context (Fileborn et al., 2024; Layard et al., 2022). Further, little is known broadly regarding how victim-survivors’ experience bystander intervention, and this gap is even more acute for LGBTQ+ victim-survivors. Our study contributes towards this gap by examining LGBTQ+ people's experiences of receiving and/or engaging in BI and self-perceived intentions and readiness to help as a bystander for SV. Given that so few studies have specifically focused on the role of sexuality, we present findings on the role of diverse sexuality, and prior experiences of sexual violence, in shaping BI.
Methods
In this article, we draw on findings from two mixed methods surveys undertaken with LGBTQ+ communities in New South Wales, Australia. This project was undertaken in collaboration with ACON, a NSW-based LGBTQ+ community health organisation. Both surveys were exploratory in nature, and as such did not set out to test any specific hypotheses. Prior to commencing recruitment for both surveys, ethics approval was received from ACON and the University of Melbourne.
Study 1 Experiences of SV
The first survey explored LGBTQ+ people's experiences of SV across the lifecourse. This survey canvassed a broad range of topics that included participant demographics and experiences of SV across participants’ lives. Participants were then asked a series of more detailed questions about their self-defined ‘most impactful’ experience of SV. We focused on participants’ ‘most impactful’ experience to minimise the need to provide detailed accounts of multiple incidents of SV. This included questions relating to the identity of the person who used sexual violence, the context the violence occurred within, impacts, reporting, disclosure and help-seeking, and pathways to healing. The survey also contained several open-text response questions inviting participants to share further details of their experiences in their own words. Of direct relevance to this paper, the survey included a question asking participants whether “anyone else intervene[d] before, during, or after the incident” in relation to their most impactful experience. Response options included yes, no, unsure/don’t remember, and prefer not to say. Participants who responded ‘yes’ were invited to share ‘what the person/people [did] to intervene’ in an open-text response question. We present findings from these two questions.
Eligibility criteria required that participants were over the age of 18, currently lived in NSW, and self-defined as LGBTQ+ and as having ever experienced SV. In the context of this project, we drew on Kelly's (1988) continuum model of SV and utilised participant-centred rather than legal definitions. Participants were recruited online through ACON′s social media accounts. The survey had 330 respondents, and an overview of participants from Study 1 is provided in Table 1.
Demographic Data Study 1.
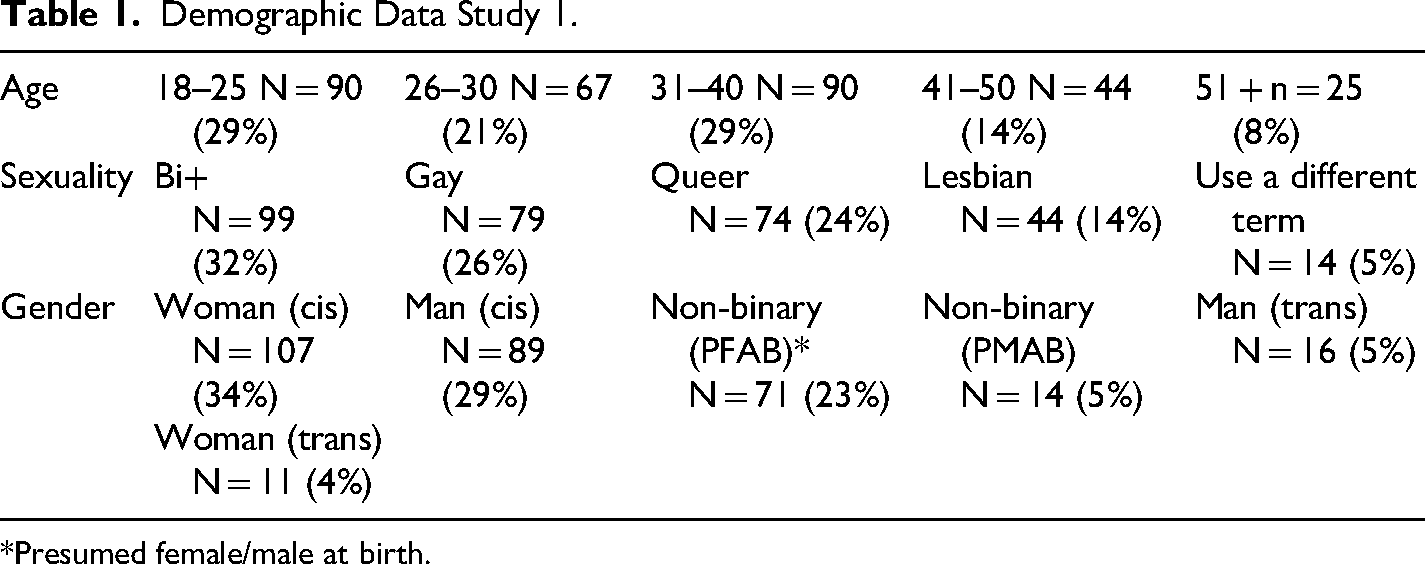
*Presumed female/male at birth.
We utilised several strategies to support participants’ safety and wellbeing when completing the survey. Contact details were provided for support services (including LGBTQ+ specific services) at regular intervals throughout the survey. A description of the survey content was provided on the survey welcome page, as well as information about the risks of participating, how participants’ data would be used, and explaining that participation was voluntary. The survey also contained regular ‘check in’ points that explained what questions would be on the next page, and to ask participants if they wanted to continue. Participants had the option to continue, to take a break and return later, or to withdraw from the survey and indicate if they consented to the responses provided thus far to be used. Participants indicated their consent to take part at the beginning of the survey. Except for eligibility questions, responses to all questions were optional.
Quantitative data was analysed using the Statistical Package for Social Sciences (SPSS). A descriptive analysis was undertaken employing frequencies and cross tabulations. Frequencies were employed to provide summary data, while cross tabulations were used to compare groups. In this case we were interested in the relationship between sexuality and experiences of sexual violence. Given the level of measurement (nominal and ordinal), Chi Square testing was undertaken to identify any statistically significant differences between groups and their experiences of sexual violence and BI.
Study 2 Perceptions of SV
The second study explored LGBTQ+ community members’ perceptions of SV against LGBTQ+ people. The survey contained questions covering participants’ demographic details and exploring their general perceptions of SV, help-seeking and support for LGBTQ+ people. The survey included several sections that explored bystander intentions, readiness to help, and bystander actions. Questions in these sections were adapted from Banyard's (2008) short form bystander measures, which have been widely used in the literature and have demonstrated construct validity. Response scoring was adapted to a 4-point scale for consistency with other measures used in the survey, aligning closely with the approach used by Baillie et al. (2022). This was followed by an open text response question asking participants if they had engaged in any bystander behaviour in the past (including prior to 12 months ago) and inviting participants to share these experiences.
Eligibility criteria included that participants were age 18 or older, currently lived in NSW and self-identified as a member of LGBTQ+ communities. As per Survey 1, participants were recruited via ACON's social media channels. In total, 183 participants were recruited for Survey 2, with 144 participants responding to the questions on BI. An overview of participants is provided in Table 2. The landing page for the survey provided a plain language statement which detailed the nature of the research, how participants’ data would be used, and that participation was voluntary. Participants indicated their consent to participate at the beginning of the survey. Other than eligibility questions, all responses were optional. Participants were provided with contact details for support services at the beginning and the end of the survey.
Demographic Data Study 2.
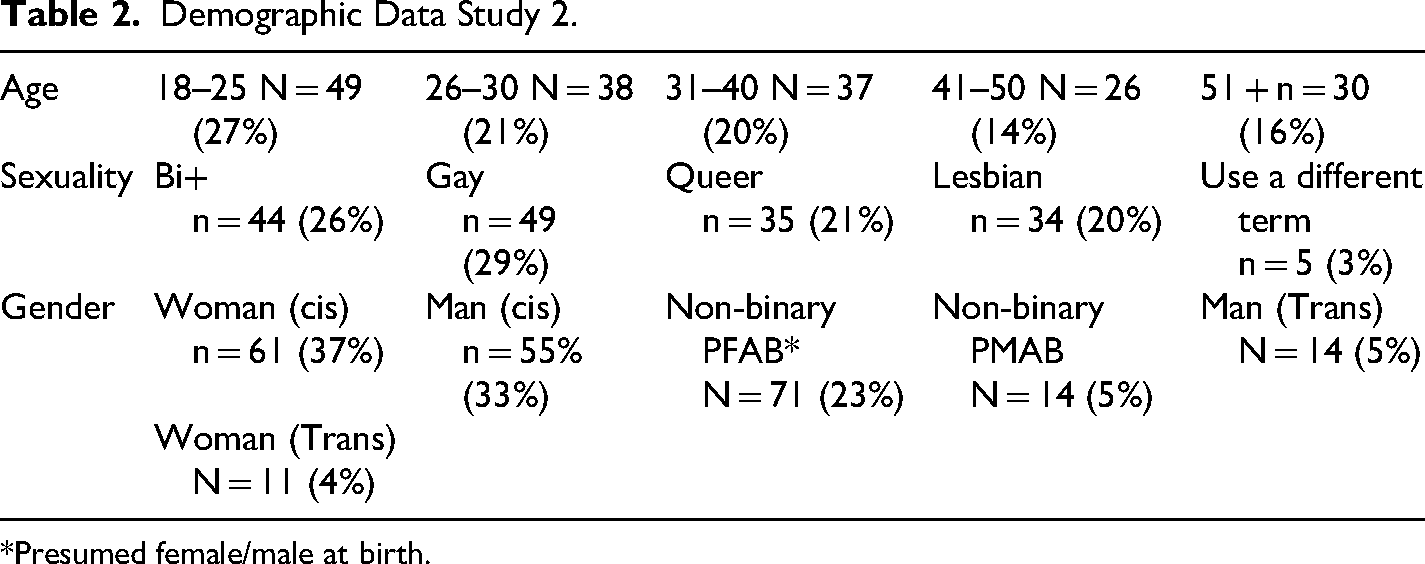
*Presumed female/male at birth.
Measures
Three measures were used to describe and understand participants’ intentions, readiness to help, and actions as bystanders in relation to SV (a definition of sexual violence in-line with Kelly's continuum model was provided to participants).
Bystander Intentions
Three items were used for this scale which addresses a respondents’ self-rated likelihood of undertaking different forms of BI: 1) If a friend told you that they had been sexually assaulted, how likely are you to show concern and offer to help them get support?; 2) If you saw someone surrounded by a group of people at a party, looking very uncomfortable, how likely are you to go over and see if they need help?; 3) If you heard a friend making excuses for forcing someone to have sex with them, how likely are you to speak up and say that is not ok?
A four-point scale from one (1) to (4) was utilised with 1 ‘Very unlikely’, 2 ‘Somewhat unlikely’, 3 ‘Somewhat likely’, 4 ‘Very likely’. A Cronbach's alpha score of .677 indicates modest internal consistency. The items used also differentiate between interventions involving friends (i.e., items 1 and 3) and those involving third parties (i.e., item 2). Items were summed to provide a total score (maximum=12), with scores ranging from three to twelve. The higher the score, the greater the likelihood of intervening in instances of SV.
Readiness to Help (RH)
Three items were also used for this scale, which aimed to assess participants’ awareness of and responsibility for intervening in SV: 1) Sometimes I think I should learn more about sexual violence; 2) I think I have a role to play in doing something about sexual violence; 3) I am planning to learn more about the problem of sexual violence against LGBTQ people.
A four-point scale from one (1) to four (4) was utilised to measure agreement with each item, with 1 ‘Strongly disagree’, 2 ‘Disagree’, 3 ‘Agree’, 4 ‘Strongly agree’. A Cronbach's alpha score of .799 indicates good internal consistency. Items were summed to provide a total score (maximum=12), with scores ranging from three to twelve. The higher the score, the greater the likelihood of learning more about SV.
Bystander Actions (ACT)
Five items were used to establish the extent to which respondents had utilised different forms of bystander intervention in practice: 1) I talked with a friend about sexual violence as an issue for LGBTQ people; 2) I confronted a friend who made excuses for abusive behavior by others; 3) I told a friend who had experienced sexual violence that I was available to listen and support, if they needed me; 4) I heard a friend joking about having sex with someone who did not want to, I spoke up against it and expressed concern for the other person involved; 5) I went with a friend who had been sexually assaulted to talk with someone (e.g., health service, police, crisis service) about their experience.
These items were dichotomous meaning the respondent could either indicate ‘no’ or ‘yes’ to each of the statements. Initially each statement included the response ‘I have not had the opportunity’. However, this was removed for analysis purposes as we were interested in whether any action was taken by those who had the opportunity to do so (n = 85). A Cronbach's alpha score of .621 indicated modest internal consistency. A total score was calculated indicating the number of times a respondent had intervened with a possible total score of five (Table 3).
Correlation Coefficients.
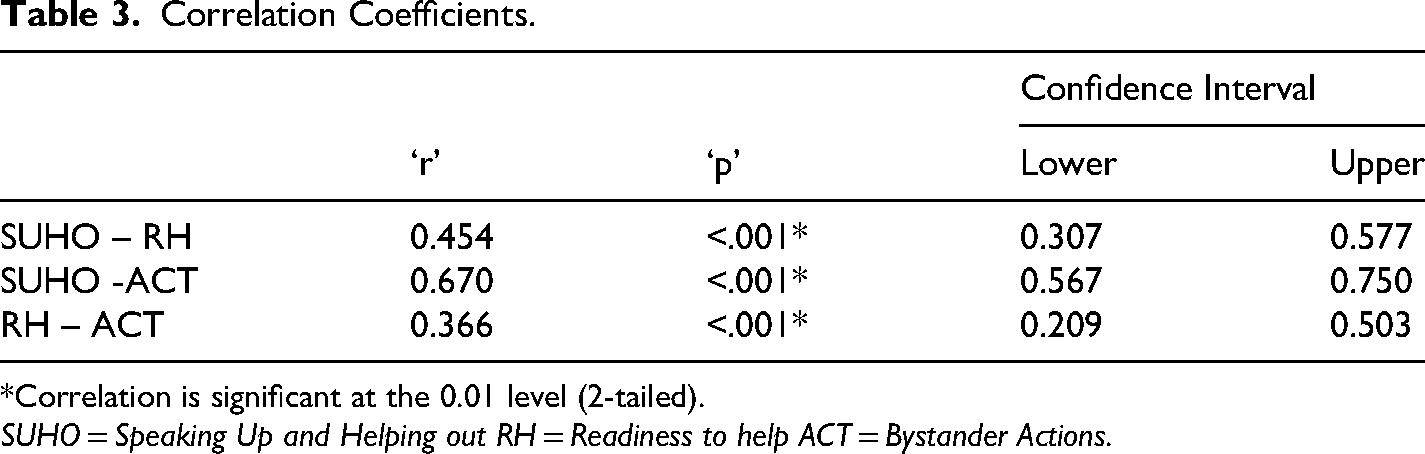
*Correlation is significant at the 0.01 level (2-tailed).
SUHO = Speaking Up and Helping out RH = Readiness to help ACT = Bystander Actions.
Analysis
Quantitative data was analysed using the Statistical Package for Social Sciences (SPSS). A descriptive analysis was undertaken employing frequencies and cross tabulations. Frequencies were employed to provide summary data, while cross tabulations were used to compare groups in relation to the impact of sexuality, gender and experience of sexual assault on ‘speaking up and helping out’, ‘readiness to help’ and ‘bystander actions’. In this paper we present findings from our analysis relating to sexuality and prior experiences of sexual violence, though we note here that there were no significant relationships between gender and BI.
Statistical Testing
Given an ordinal level of measurement, non-parametric tests were applied to the data. For sexuality, a Mann-Whitney U was utilised to identify any difference between the means of those who had experienced SV and those who had not in relation to bystander attitudes and intentions. For sexuality, which contained four categories, the Kruskal-Wallis H test was used to identify any statistically significant difference between the means of sexuality groups and bystander attitudes and intentions. While the Kruskal-Wallis H will identify a significant difference between groups, it does not identify which groups are different. In order to identify any differences between groups the Dunn test was employed. Where the data was nominal (i.e., bystander actions) chi square tests of independence were employed.
Findings – Study 1: Victim-Survivors’ Experiences of BI
Sexuality
No relationship was observed between sexuality and whether someone intervened either during or after SV, with 13% (n = 32) of all respondents indicating that someone did intervene. Lesbians (17%; n = 6) and those who identified as queer (18%; n = 11) recorded the largest proportions of participants who reported that someone else intervened, followed by those identifying as Bi+ (13%; n = 11) and those identifying as gay (6%; n = 4) (Table 4).
BI & Sexuality.

Qualitative Findings
Overall, our survey findings suggest that BI is not commonly experienced by victim-survivors, in line with past research. This may, at least in part, be accounted for by the fact that participants’ ‘most impactful’ experiences of SV typically occurred within a private residence (71%), meaning that there may not have been any opportunity for BI to occur (Layard et al., 2022). Further, BI may occur in ways that a victim-survivor is unaware of, such as a bystander talking privately to a person who uses violence. For the minority of participants who had a bystander intervene, responses to the open text question provided further insight into the intervention strategies that were utilised.
Supportive Intervention
Several participants described intervention strategies that occurred in the aftermath of SV. This included ‘checking in’ with the victim-survivor to “ask… if I was okay” (41, lesbian woman), while another participant said the bystander “supported me while I reported” (20, queer woman) the experience to a teacher. ‘Checking in’ could also work to immediately disrupt and intervene in the actions of someone using violence. As one participant recalled: I was in a crowd and I froze when it happened. So the girl next to me saw how terrified I looked after a few painful minutes of this person sticking their hands in my pants. She turned to me & asked if I was okay and the perpetrator immediately took their hands away…I also knew I could ask her for help if it happened again. I am endlessly grateful for her stopping to check on me, because I know the perpetrator would have just kept going. (23, queer, non-binary)
Another participant described how their “best friend stopped me from committing suicide right after from wanting to jump off the balcony” (24, pansexual, non-binary). Participants in this study reported significant levels of self-harm and attempted suicide as a direct result of experiencing SV (Asquith et al., 2024). The provision of mental health first aid is, therefore, a vitally important component of bystander intervention for LGBTQ+ victim-survivors.
Several participants described more direct forms of intervention. This included bystanders creating a diversion by saying “they needed to talk with me urgently in the kitchen” and then asking “if I wanted to be in the situation and when I said no, helped me leave through the back door” (44, lesbian woman). In another case, a bystander “pushed him off me” (34, queer woman), while another “removed the person from the venue” (47, pansexual woman). Finally, two participants reported that the person who used violence was banned from the venue the incident occurred within. For example, “I told them about it, and they banned that person from future events at that sex on premises venue” (26, bisexual woman).
Non- and Unsuccessful Intervention
While the examples in the previous section illustrate positive or supportive experiences of BI (though, in some cases the outcome of the intervention was ambiguous), other participants shared experiences where bystanders failed to intervene, or where the intervention was unsuccessful. One participant described how their family and friends provided support to help them leave their abusive partner. However, they said “equally, my ex-partner's own mother helps them keep these acts of violence a secret. There are bystanders on both sides, and both have been impactful” (27, queer, gender not disclosed).
In other cases, the actions of well-intended bystanders were simply unable to stop the actions of people using violence: Pulled him off me and told him to leave me alone (he came back later to continue) (31, pansexual, non-binary) I was too drunk to remember, but I believe friends tried to pull person away from me (didn't work). (25, queer, trans) Contacted the police – which was ultimately unsuccessful (28, bisexual, woman)
The final comment here also highlights the limits of relying on BI at the expense of systemic and institutional transformation. While this participant did not provide further detail as to why contacting the police was unsuccessful, it is important to situate this intervention strategy within a broader context of historical and contemporaneous police violence and abuse against LGBTQ+ communities (Dwyer, 2012; 2015; Leonard & Fileborn, 2018). BI tactics such as contacting an authority figure are unlikely to be successful when the ‘authority figure’ is unable or unwilling to respond ‘well’ to SV and may represent a source of harm to LGBTQ+ victim-survivors. This suggests that BI strategies must consider the identity of a victim-survivor, and the unique needs and experiences of different communities. Successful intervention strategies for some may be directly harmful for others.
Several participants shared experiences of BI that were overtly or unintentionally harmful. One participant, for example, discussed an experience when she was younger and experiencing abuse from a long-distance partner. Her father was going to accompany her to meet and confront the partner about their abuse. While this may appear supportive, the participant described how “at the time [I] was angry at him for interfering and not trusting my judgement”, and her father “ultimately…didn’t come with me” (30, bisexual, woman). This experience illustrates the importance of BI being responsive to victim-survivors’ needs, as even well-intentioned offers of support have the potential to cause harm. Two other participants described more overtly negative responses, including being “told…to forgive him as was my duty as a wife under god” (39, queer, non-binary) and “that I should get over it and move on” (24, bisexual woman).
Findings – Study 2
Bystander Intentions – Sexuality
No relationship was observed between sexuality and intention to act as a bystander (Table 5). An overall mean score of 3.92 (n = 184) indicated that respondents were very likely to indicate they would provide support and assistance to seek help (item = 1), with all sexuality groups scoring similarly to the total mean score. The total mean score (Table 5) was 10.94 (n = 184) out of a possible score of 12, indicating a high likelihood that respondents had a high self-reported intention to intervene and provide support to someone who had experienced/was experiencing SV. Each sexuality group scored similarly with no significant differences emerging.
Speaking Up and Helping out.

Interestingly, the mean score for item 2 (If you saw someone surrounded by a group of people at a party, looking very uncomfortable, how likely are you to go over and see if they need help?) was significantly lower than item 1 (Z = −6.893; p ≤ .001) (If a friend told you that they had been sexually assaulted, how likely are you to show concern and offer to help them get support?) and item 3 (Z = −3.522; p < .001) (If you heard a friend making excuses for forcing someone to have sex with them, how likely are you to speak up and say that is not ok?). While respondents were very likely to say they would support and seek help for a friend or confront a friend, they were less likely to report an intention to intervene if third parties were involved (item 2). This difference was observed for all groups.
Bystander Intentions – Prior Experience of Sexual Violence
Over 8 out of 10 respondents (87%; n = 153) in the community perceptions survey had also experienced self-defined SV. No differences emerged between sexuality groups and the experience of SV. While those identifying as gay recorded the lowest proportion experiencing SV compared to other groups, the difference was not significant. There was, however, a relationship between gender and SV (Chi-square 16.674; p ≤ .001), with 72% (n = 42) of men reporting sexual assault compared to 96% (n = 68; p = .001) of women and 92% (n = 44; p = .035) of those identifying as non-binary.
While differences between groups were not large, a relationship was observed in relation to the experience of SV and the extent to which an individual reported they would intervene and/or support a friend or stranger who was experiencing SV (Table 6). Those who had experienced SV were significantly more likely to report an intention to intervene or provide support (Total mean score 10.92; n = 177) than those who had not (Total mean score=10.00; n = 22). Mann Whitney U scores indicated a significant difference between each group (U = 758.500; Z = −2.055; p = .008).
Speaking Up and Helping out.
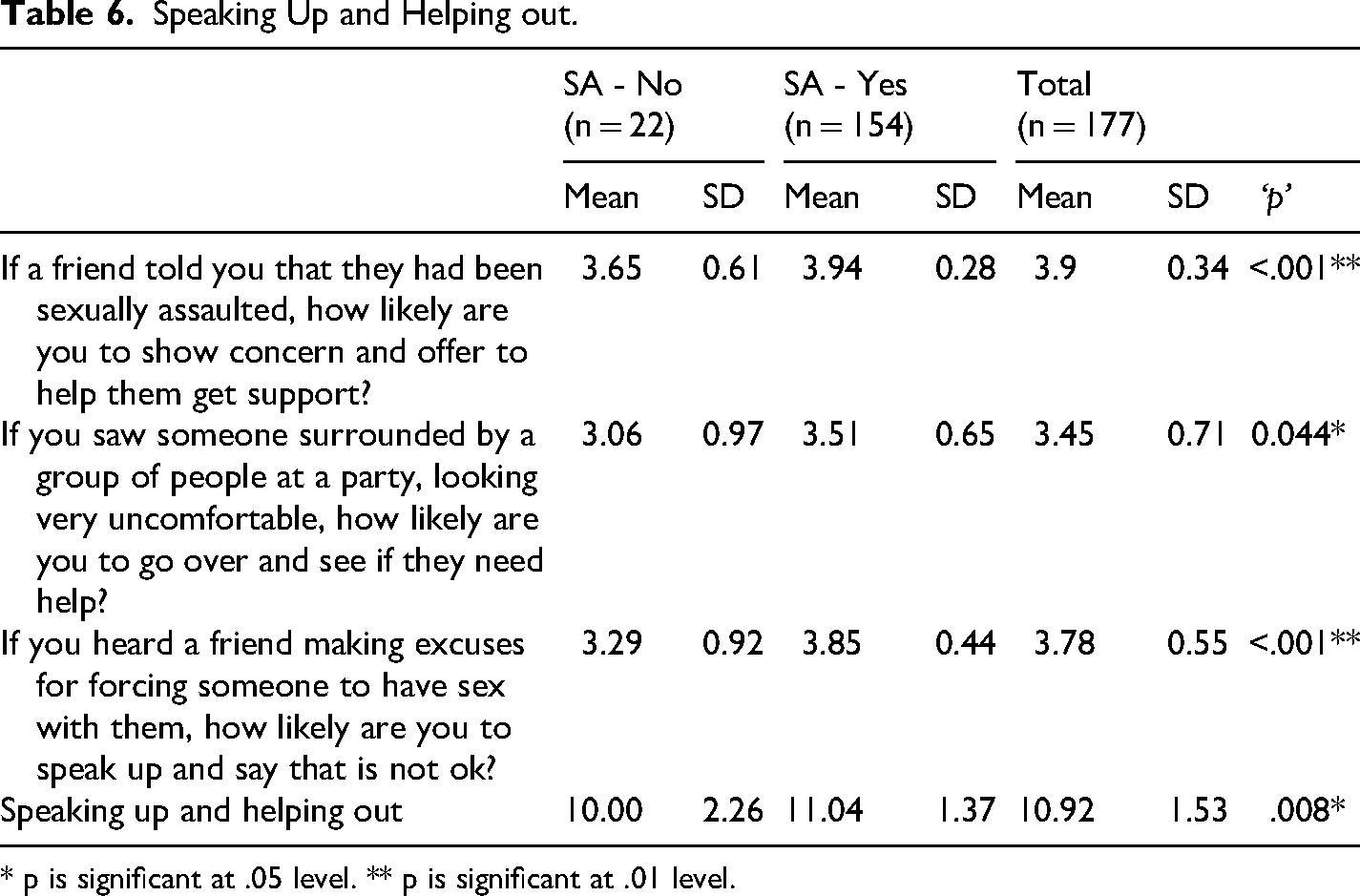
* p is significant at .05 level. ** p is significant at .01 level.
Those who had experienced SV were significantly more likely to say they would show concern and offer support (item 1), than those who had not experienced SV (U = 808.500; Z = −3.311; p < .001). Although not as strong, those who had experienced SV were significantly more likely to intend to intervene to help someone surrounded by others (item 2), than those who had not (U = 721.500; Z = −2.017; p = .044). Lastly, those who had experienced SV were more likely to indicate they would confront a friend (item 3) than someone who had not (U = 683.000; Z = −3.663; p < .001).
Readiness to Help – Sexuality
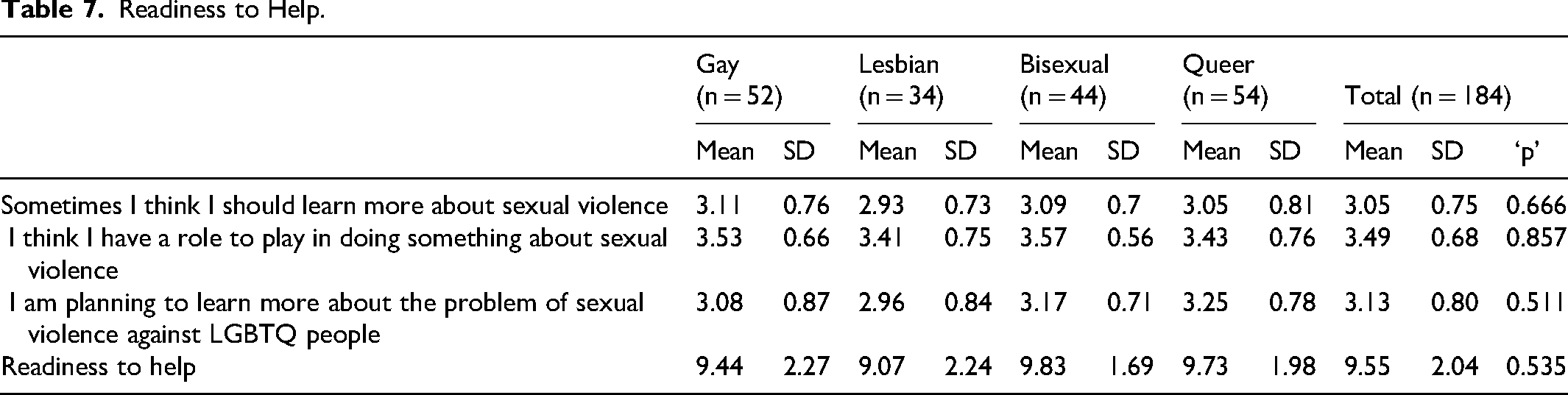
No relationship was observed in relation to sexuality and readiness to help with overall scores being similar for each group (Table 7). Thus, gay people recorded an overall score of 9.44 (n = 52) compared to 9.07 for lesbians (n = 34), 9.83 (n = 44) for bisexuals, and 9.73 (n = 54) for queer people. Total scores (Table 7) were also similar for each group ranging from 9.07 (n = 34) for lesbians to 9.83 (n = 44) for bisexuals, indicating a general willingness to learn more about SV and potentially playing a role in its prevention. As can be seen, ‘p’ values for each were non-significant.
Readiness to Help.
Readiness to Help – Prior Experiences of Sexual Violence
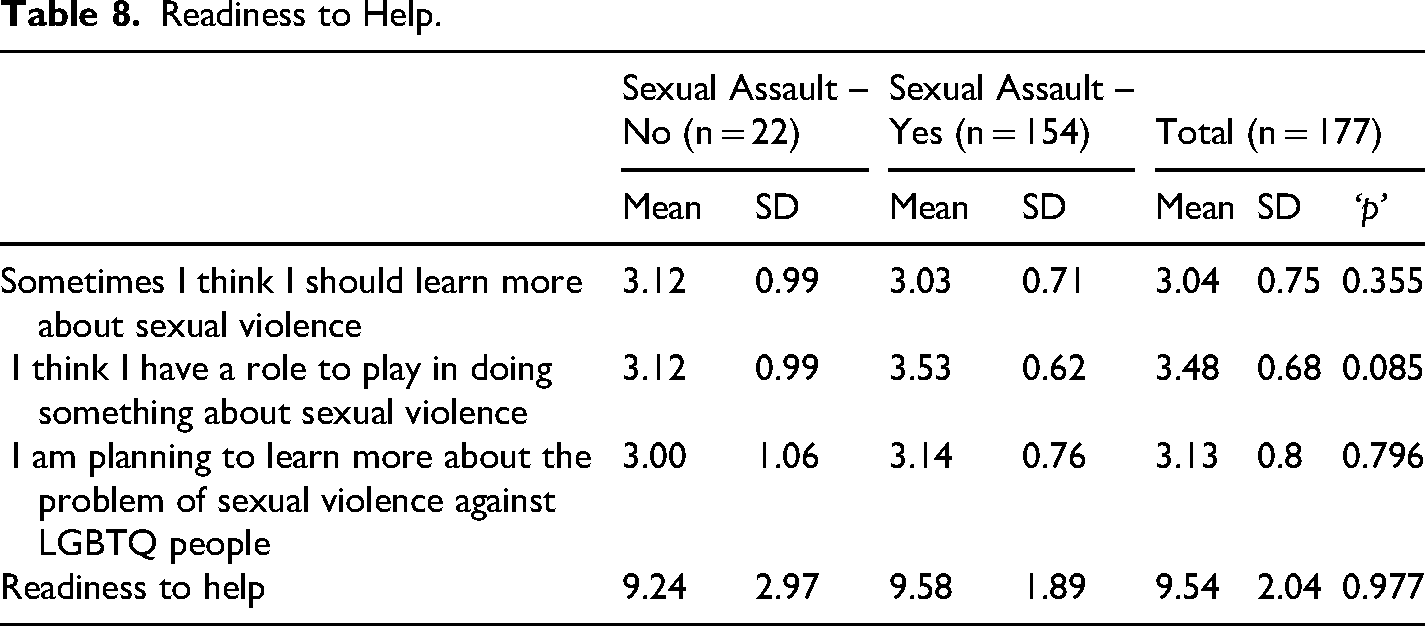
Overall scores for readiness to help reflected these results with those who had not experienced SV scoring 9.24 (n = 22) compared to 9.58 (n = 154) for those who had experienced SV (Table 8). Very little difference emerged between those who had experienced SV and those who had not in relation to readiness to help, with both groups scoring a mean score of 3 (rounded) for each of the items listed (Table 8). While those who had experienced SV scored higher for item 2 (3.53; n = 154) (I have a role to play) than those who had not (3.12; n = 22), the difference was non-significant (p = .085).
Readiness to Help.
Bystander Actions – Sexuality
No relationship was observed in relation to the number of times an individual intervened and sexuality (Table 9A) with a total mean score of 2.16 (n = 141) with similar scores being reported for each sexuality group. In relation to individual items no significant difference was reported between each sexuality group with the exception of ‘confronting a friend who made excuses for the abusive behaviour of others’ (Table 9). In this case queer people were more likely to challenge a friend (p = .033; n = 19) than gay people (n = 5). However, the sample size for those intervening (especially for gay people) is small so results should be interpreted with caution.
Bystander Actions (% Indicating ‘Yes’).
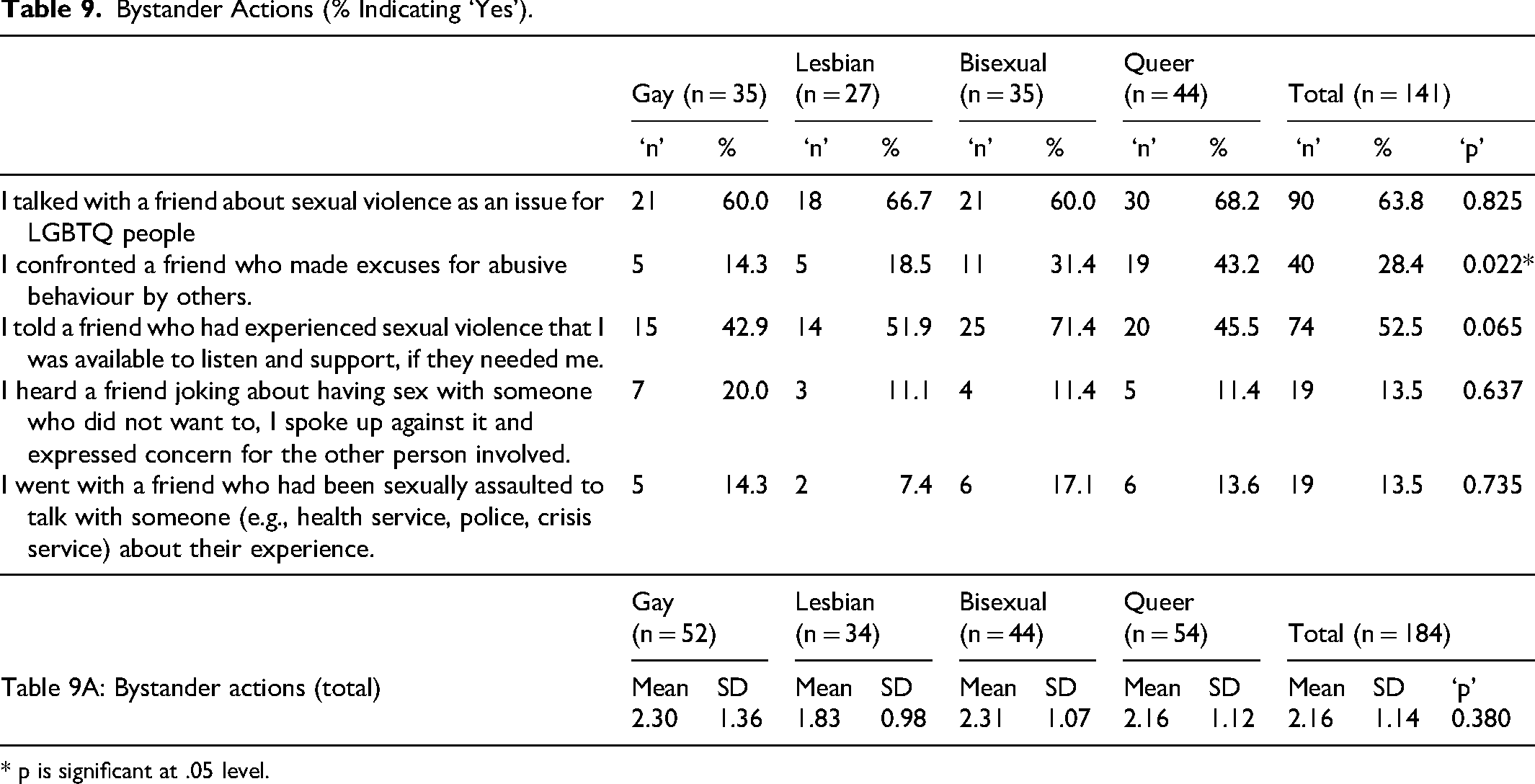
* p is significant at .05 level.
Bystander Actions –Prior Experience of Sexual Violence
A relationship was observed in relation to bystander actions and having experienced SV (Table 10A). The total mean score for bystander action was 1.75 (n = 177), with those who had not experienced SV (1.00; n = 23) reporting fewer interventions on average than those who had experienced SV (1.85; n = 154, U = 652.000; Z = −2.581; p = .010). In so far as individual items are concerned (Table 10) those who had experienced SV were significantly more likely to talk with a friend about SV as an issue (69.1%; n = 85; p = .006) than those who had not (35.3%, n = 6). However, the sample size for those who had not experienced SV was small so care should be taken when interpreting results. While the proportional difference between those who had and those who had not experienced SV was large for some items, the sample size for those who had not experienced SV was too small to be confident that any difference was statistically significant.
Bystander Actions (% Indicating ‘Yes’).
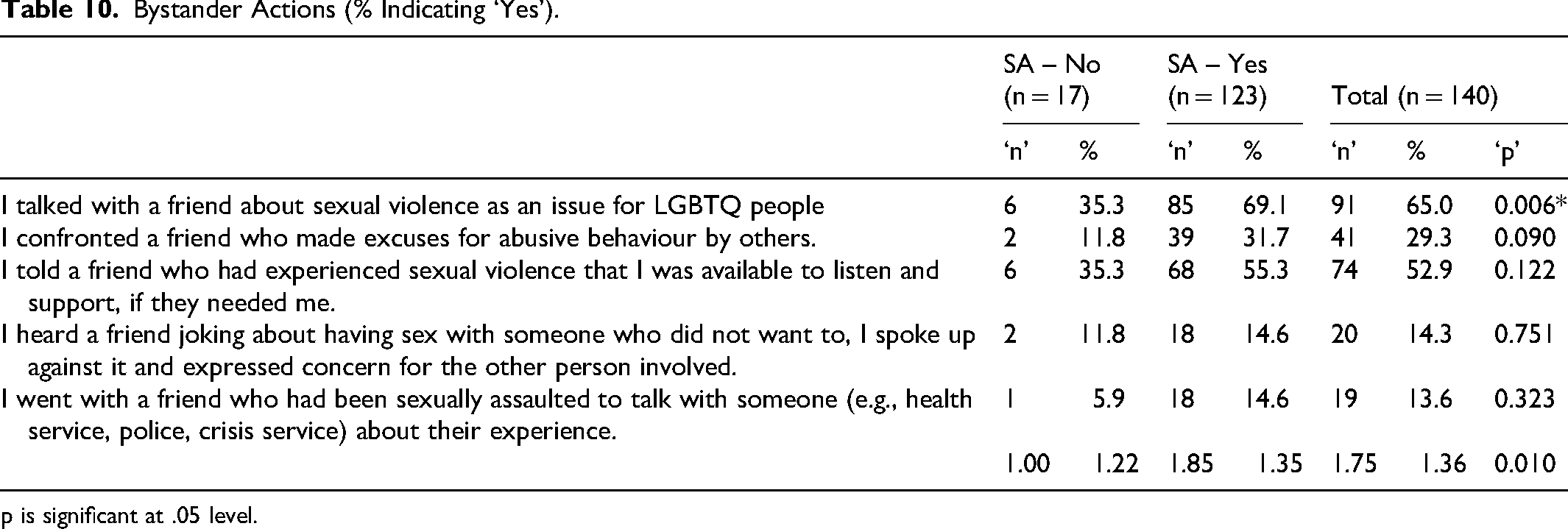
p is significant at .05 level.
Qualitative Findings: Bystander Actions
Offering Support
In their open text responses, participants provided further detail on the BI strategies they had used in practice. Offering support to a victim-survivor, typically in the aftermath of SV, was by far the most common form of intervention. In some cases, participants described providing responses to disclosures that occurred years after the incident, and there remains a question regarding the distinction between support as a form of tertiary intervention versus support as a response to disclosure. For example: My Bisexual friend was assaulted by another mutual friend while she was drunk. I offered her support and went no contact with the mutual friend who assaulted her. I respected her wishes to not contact the police but let her know that I would come with her to the police station to help her feel safer around the police if she ever wanted to report it. (22, queer, non-binary)
Support could also take more tangible forms, such as helping victim-survivors to exit abusive relationships and providing them with a safe space to stay: 1 supported someone who had faced continuous sexual violence, and helped them get out of a relationship with the perpetrator, and let them stay at my house (28, lesbian, woman)
Other participants discussed taking steps to keep the victim-survivor away from the person who used violence against them, such as letting the victim-survivor know if the person who used violence was attending a community event. In other cases, support involved referring or accompanying victim-survivors to crisis and other support services, to report to police, and providing a non-judgemental “ear to listen” (25, pansexual, woman).
Direct Intervention
While less common, participants also described more direct forms of intervention. Several participants indicated they had ‘called out’ violence-supportive beliefs and attitudes without providing further detail: Questioned a friend's attitude towards sexual violence. (31, gay, man) Spoke out when gay men have sexually harassed women by speaking about their genitals in a derogatory way in queer spaces (38, queer, woman)
One participant described in more detail the tactics they used in ‘calling out’ violence-supporting attitudes: I have stood up to a number of individuals who were “joking” about how they forced a number of LGBTQI+ individuals to have sex with them (so raped them). I asked the individual to explain how the joke was funny because I “didn’t get it”. After they failed to explain how it was funny I informed them that they committed an act of sexual abuse and violence against those people, that they raped those people (because no consent was given) and that I would be reporting them to the police (which I did, yet unsurprisingly nothing was done). (29, pansexual, non-binary)
While in most cases it was unclear in what context intervention was occurring within, the second and third quotes above provide direct examples of BI occurring within LGBTQ+ communities or involving violence against LGBTQ+ people.
One participant said they had “intervened when woman are being sexually harassed at queer parties by cis men” (38, queer, woman), although it was unclear what this intervention entailed. Two participants indicated they had engaged in forms of secondary prevention, “interject[ing] in situations where someone around me has been in danger of sexual violence” (25, lesbian, non-binary). A second participant provided more detail on the intervention they had provided, saying: At house parties and small events I've definitely spoken up for people who seemed too intoxicated or incapacitated to consent, including helping them getting home safely and being in touch with them in the days afterward. (28, bisexual woman)
No Opportunities
Participants who indicated they had ‘no opportunity’ to act as a bystander offered diverse reasons for this. As our project was conducted during the COVID19 pandemic, with parts of Australia placed under strict lockdowns at various points, some participants said they subsequently had not had any opportunity to intervene: With covid and isolation I have barely even seen my friends and they haven’t seen others. (49, man, sexuality not disclosed)
Another participant said he had no opportunity as his “confidence to speak up has only come lately” (19, gay man). However, another participant framed their lack of opportunity to intervene around the notion that SV is not an issue within their LGBTQ+ friendship group: Most of my friends are gay men and lesbians and tbh [to be honest] it's something of an unspoken rule that you don't joke about rape or whatever. It's just not cool and anyone who does it will find themselves uninvited (29, lesbian, woman)
While this may well be the case within this participant's friendship group, clearly such comments do not align with the experiences of others who had experienced SV, or ‘called out’ rape myths and stereotypes, within LGBTQ+ communities.
Discussion
In this paper, we have presented findings from two exploratory studies on LGBTQ+ people's experiences of, and self-rated intentions and readiness to intervene in relation to, BI. To the best of our knowledge, this is the first work to offer insights from both LGBTQ+ victim-survivors and general community members, and one of a limited number of studies to include an analysis across different sexualities rather than analyse LGBTQ+ respondents as a singular group. Our findings also aimed to further examine the relationship between experiences of SV and bystander intentions and action for LGBTQ+ people.
In line with previous studies exploring victim-survivors’ experiences of BI (Fileborn, 2017; Hamby et al., 2016; Hoxmeier & McMahon, 2021; Seo et al., 2022), our findings suggest that BI was not commonly experienced by LGBTQ+ victim-survivors. While there were no significant trends across different sexuality groups, lesbian, bi+ and queer participants reported higher levels of BI compared to gay participants. It is notable that majority of these experiences involved SV by cisgender men (Layard et al., 2022). This might suggest that BI is occurring within what might appear to be a heteronormative context, rather than for SV occurring within a queer relational context. At the very least, the occurrence of BI across these relational contexts of SV warrants exploration in future research. However, it is important to note that we only asked participants if BI occurred in relation to their most impactful experience of SV, and not whether they had ever experienced BI. Qualitative responses from both victim-survivors and the general LGBTQ+ community participants provided direct examples of successful BI in action, including BI that disrupted SV when it was occurring (direct intervention), removed vulnerable individuals from high-risk situations (secondary prevention), and provided support to victim-survivors in the aftermath of violence (tertiary prevention). Thus, while not common, our findings nonetheless indicate that BI can be effective or valued by victim-survivors in some contexts. However, in other cases BI was ineffective or actively harmful, a finding that reaffirms the small number of studies on BI in practice (Fileborn, 2017; Hamby et al., 2016; Hoxmeier & McMahon, 2021). The potential for BI to cause harm does raise some concerns about the extent to which it is currently emphasised in prevention and educational efforts around SV (Mainwaring et al., 2023), and there is a need for further research that aims to shed light on the contexts in which BI is most likely to be effective for LGBTQ+ communities.
Further, our findings suggest that effective or appropriate BI strategies must be tailored to the needs of different communities and contexts. In the case of our study, it was clear that mental health first aid could form a vitally important component of BI occurring in the immediate aftermath of SV for LGBTQ+ victim-survivors. While this is likely an important aspect of BI for all victim-survivors, LGBTQ+ victim-survivors in our study reported extremely high levels of self-harm and suicidality because of experiencing SV (Asquith et al., 2024; Layard et al., 2022), something that is likely compounded by living in a cis- and hetero-normative social context. This suggests that LGBTQ+ inclusive BI education should also include content on mental health first aid and supporting someone experiencing a mental-health related crisis. Other common BI strategies, such as calling an authority figure like the police, may be inappropriate for LGBTQ+ communities given ongoing concerns about police violence and hostility towards queer communities (something which is undoubtedly compounded for LGBTQ+ people of colour, first nations, sex workers and other multiply marginalised queer folk). Participants also described intervening in lateral SV perpetrated within queer communities, and it is unclear if this context of violence necessitates unique or tailored strategies. As such, we argue that BI research, education and strategies require a firm grounding in intersectionality (Crenshaw, 1991). Such an approach enables recognition of how our position within different structural locations shapes the structural drivers of SV, the forms that SV may take, our capacity to recognise SV when it is occurring, our capacity and safety in acting as bystanders, and the types of bystander strategies that are likely to be appropriate and safe. In other words, a ‘one-size-fits all’ approach is inappropriate, and likely to obscure the experiences of marginalised communities. In the case of BI for LGBTQ+ SV this requires an understanding of the roles that heteronormativity and cissexism play in driving SV, as well as attendance to the historical and contemporaneous forms of institutional violence and broader stigmatisation of queer communities.
At the very least, these queer-specific contexts of SV should be explicitly incorporated into BI training. Yet, as Kirk-Provencher et al.'s (2023) research highlights, LGBTQ+ people are rarely explicitly included in BI education and training, and it is unclear to what extent current BI training is effective for LGBTQ+ communities. Our findings add further support towards the urgent need for BI training to be inclusive of LGBTQ+ people, and for further research evaluating the outcomes and impacts of this training for LGBTQ+ communities. Given that victim-survivors in our study relied strongly on informal support systems (such as friends and chosen family), it is vitally important that LGBTQ+ people and their allies are effectively equipped to intervene as bystanders – though, as we discuss below, this should not occur in the absence of other structural and systemic changes. Some participants appeared to draw on myths about LGBTQ+ communities (e.g., that violence doesn’t happen in these communities), suggesting a need for training that is specifically tailored to dispel misperceptions about LGBTQ+ sexual violence (see Say It Out Loud, n.d., for a practice-based example). Misperceptions about LGBTQ+ SV are themselves entangled within a broader culture that positions at least some forms of SV as permissible, meaning that this work must occur alongside broader efforts to transform rape culture.
Findings from our community attitudes study shed light on LGBTQ+ people's self-rated intentions and readiness to help as bystanders, as well as their actual bystander behaviour. Overall, participants self-rated intentions to act as a bystander was high, though it is important to note that intentions to help do not always translate into direct action. In line with previous studies (Amar et al., 2014; Baillie et al., 2022; Bennett et al., 2017; Seo et al., 2022), participants expressed a stronger intent to intervene in situations where they knew the victim-survivor. There were no significant differences in bystander intentions, readiness or actions according to participants′ sexuality. However, most participants in Study 2 indicated they had experienced SV, and these participants reported higher levels of bystander intentions and readiness to help. Future research should aim to engage a broader cross-section of LGBTQ+ community members to enable further exploration of any differences in BI within and across these diverse communities, and to more fully explore the role of other intersecting structural factors such as race and disability.
While there can be a disjuncture between bystander intentions and behaviours, participants reported they had engaged in BI, with an average of just under two forms of BI reported per participant across the sample. This finding indirectly supports the notion that LGBTQ+ people may be more likely to act as bystanders and directly demonstrates that LGBTQ+ people do actively engage in BI. However, as the study did not include heterosexual cisgender participants, it is not possible to compare rates of BI across these cohorts – and this is an endeavour that could be taken up in future research to help better inform targeted BI interventions. There were no significant differences across the different sexuality groups included in this study. It is worth reiterating that, while not the focus of this paper, there were also no significant differences in BI according to gender. There are several potential explanations for this. For example, it may be the case that LGBTQ+ people are more likely to engage in BI regardless of their gender or sexuality, an explanation supported by Coulter et al.'s (2024) finding that SGM participants had higher levels of SV knowledge and intention to intervene as a bystander. As with bystander intentions and readiness to help, participants who had experienced SV reported more extensive bystander behaviours, and it may be that the high levels of prior SV victimisation reported by participants accounts for their propensity to have acted as bystanders.
Our findings provided further support to the notion that victim-survivors are more likely to engage in BI, though this finding is not consistent across previous studies (Mainwaring et al., 2023). However, it is challenging to disentangle whether rates of BI were high because participants were LGBTQ+, because they were victim-survivors, or a combination of these (and other) factors. Again, these relationships should be explored further in future research. Indeed, the apparent relationship between experiencing SV and engaging in BI raises questions about the extent to which BI truly positions us all as having a role to play in intervention and prevention, or whether the emphasis on BI inadvertently places this labour back onto victim-survivors. In a context where LGBTQ+ SV is excluded from or marginalised within policy and service responses to SV (Seymour, 2019), an over-emphasis on BI at the expense of systemic reform and resourcing of services may unintentionally further responsibilize LGBTQ+ communities for responding to SV. Furthermore, any reform and resourcing around BI should be operationalised in conjunction with wider educational work seeking to dismantle the broader culture around SV being permissible generally. This is especially important in a political climate where discussions about LGBTQ+ issues are being systematically erased from spaces where this is most possible, such as secondary schooling.
Limitations
There are several limitations of these studies that should be acknowledged. Firstly, questions on BI were asked in the context of two extensive surveys on SV, and we only asked a small number of questions on BI to prevent survey fatigue. We may have produced different results if the full versions of the short or long form bystander measures developed by Banyard and colleagues were used. The use of an online survey meant there was no opportunity to ask clarifying questions or seek out further detail from participants. Some of the written responses on BI were very brief, ambiguous or unclear – for example, it was not always apparent how an intervention was received by the victim-survivor or what the impact or outcome of an intervention was. Future studies could consider utilising interview-based methods to overcome this limitation, and to develop richer insights into LGBTQ+ people's experiences of BI. Further, it was not always clear if participants were referring to BI or rather to responses to disclosure. We also note that the difference between these concepts seems to be poorly distinguished in the literature, especially in relation to BI in the aftermath of SV – where does BI end and response to disclosure begin? Are there, for example, benefits or limitations to conceptualising response to disclosure as a form of tertiary BI? Similar slippages occur in relation to the concepts of ‘prevention’ versus ‘intervention’, particularly given the broad range of contexts that BI may occur within. While we do not have the scope to explore such questions here, we raise them as issues that could be considered in future work. Our participant sample was limited to New South Wales, and most participants lived in urban areas. As recruitment occurred through ACON's networks, this is likely to have shaped the sample, and it is unclear to what extent our findings are generalisable to the broader LGBTQ+ communities in Australia and beyond. Finally, our surveys were conducted during the height of the COVID-19 pandemic, during which time Australia had multiple phases of strict lockdowns. Participants in Study 2 had reduced opportunity to intervene as bystanders, and our findings may resultantly skew the true extent of BI engaged in by LGBTQ+ communities.
Conclusion
In presenting findings from two exploratory surveys with LGBTQ+ victim-survivors and community members, this article has sought to add to a small but growing body of literature on BI and LGBTQ+ communities. Given the high levels of SV experienced by LGBTQ+ people, we add our voices to the growing chorus of researchers arguing that it is imperative for research and prevention initiatives to be inclusive of queer communities. In the context of BI, this includes ensuring that LGBTQ+ experiences of SV are made visible, that the unique needs of LGBTQ+ communities are accounted for in bystander strategies, and that myths and misperceptions about SV which obscure LGBTQ+ experiences are challenged. While our study focused on LGBTQ+ people's experiences and perceptions of BI in relation to LGBTQ+ victim-survivors, it is also imperative for future work to explore the capacity of cisgender heterosexual people to recognise and intervene in SV against LGBTQ+ people. However, our findings also point to the limitations of BI as a prevention strategy: BI was rare in practice, not always effective, and may inadvertently serve to responsibilize victim-survivors and individual community members. Thus, efforts to encourage BI must, at the very least, occur alongside holistic structural and systemic interventions.
Footnotes
Acknowledgements
This project was supported with funding from the NSW Department of Communities and Justice, and ACON. The authors would like to acknowledge Eloise Layard, Teddy Cook and Joël Murray from ACON and Dr Shaez Mortimer for their contributions to this project. We also acknowledge the participants who so generously shared their experiences with us.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New South Wales Department of Communities and Justice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.