
Abstract
An empathy-related component has been included in most sex offender treatment programs since the 1980s; however, research linking empathy to sexual offending and/or to treatment outcome has produced mixed findings. This study examined the relationship between victim specific empathy, general empathy, and overall treatment change (determined by responses on a battery of psychometric tests) with static risk (Risk Matrix 2000 [RM 2000]) and sexual offense reconviction data in a sample of 105 offenders who completed treatment while in prison or in the community in England and Wales and followed up for an average period of more than 10 years. Victim-specific empathy improved from pretreatment to posttreatment and related to overall treatment change. A small group of offenders, whose victim empathy scores deteriorated from pretreatment to posttreatment, had higher rates of sexual recidivism compared with the rest of the sample. In contrast, neither were any reliable pretreatment to posttreatment changes noted on general empathy scores, except for an indication on the Interpersonal Reactivity Index Personal Distress Scale, nor was any relationship found to sexual recidivism. The implications of these findings are discussed in relation to treatment goals and sexual recidivism.
Introduction
The inclusion of empathy enhancement as a treatment component for sex offenders is long-standing. Abel and his colleagues were the first to report using an empathy enhancement component in sex offender treatment in the 1970s (Murphy, Abel, & Becker, 1980) and within a few years, most descriptions of treatment programs included an empathy component (Marshall, 1996). This rapid uptake came in the absence of strong empirical support perhaps because the idea that empathy inhibits behavior that harms others has such strong intuitive appeal. Indeed, Marshall and Eccles (1995) noted that “[n]o one has yet offered any evidence in support of these ideas, perhaps because they appear to be self-evident truths” (p. 302). Empathy has been found to be causally related to prosocial behavior supporting an empathy-altruism hypothesis (Piliavin & Charng, 1990). Farrington (2007), for example, argues that people are less likely to victimize others if they can appreciate and/or experience the others’ feelings. There is much evidence (see, for example, Beckett, Beech, Fisher, & Fordham, 1994) that sex offenders frequently fail to appreciate the damage they have inflicted on their victims and, thus, they often demonstrate little remorse for their crimes; they often blame victims for the offense and interpret victims’ behaviors as provocative. The assumption has been that this is a demonstration of a lack of empathy. However, this may be evidence of a range of “distorted” thinking patterns, justifications, and minimizations rather than an empathy deficit per se. Yet the assumed link between empathy and sexual offending is difficult to disregard. Mann and Marshall (2009) argue that a strong theoretical relationship between sex offending and empathy has developed, which means that empathy enhancement remains an essential component of sex offender treatment and rehabilitation.
That sex offenders have empathy deficits or exhibit lower levels of empathy than others has yet to be convincingly evidenced. Initially, and for sometime thereafter, most treatment programs focused on assessing and improving perpetrators’ generalized empathy skills; however, there is little evidence to suggest that sex offenders have generalized empathy deficits. See Brown and Walker (in press) for a recent review of the literature, which identified that only 6 out of 25 studies demonstrated that sex offenders had lower empathy than control/comparison groups, with the remaining studies finding mixed results, that sex offenders had higher levels of empathy or that there were no differences in empathy levels between sex offenders and control/comparison groups. Such equivocal findings may be related to a number of issues that surround the definition and measurement of empathy. In terms of the definition, it is not even clear if empathy should be viewed as a discrete or continuous variable. While we tend to measure empathy and treat it as a continuous variable in assessment and research, we also talk about offenders lacking empathy as if it were a discrete (i.e., we either have or do not have empathy) rather than a continuous variable. Furthermore, when generalized empathy is measured, it must be assumed that an individual’s empathy skills, or empathy levels, are applied equally to all people in all situations—that is, that empathy is a trait, rather than state characteristic, though this is rarely made explicit.
There has also been debate about whether empathy is a cognitive or affective construct (see, for example, Jolliffe & Farrington, 2004 for a review). The contemporary view tends to be that empathy includes both elements, as demonstrated in Marshall, Hudson, Jones, and Fernandez (1995) four-component model of empathy: (a) recognition of another person’s emotional state, (b) an ability to perceive the world from that person’s point of view, (c) an ability to replicate the emotional state of the other person, and (d) a change in behavior toward the other person. This model has, however, been criticized: for example, Pithers (1999) argued that the model is not able to explain an individual’s response to someone who is unconscious, as the unconscious person would have no emotional response to recognize or replicate. Furthermore, he points out that “merely” recognizing empathy is an inadequate treatment target if the offender recognizes empathy as, or after, he or she commits an offense: if empathy is to inhibit offending, individuals must be able to predict and respond empathically to an anticipated response before it happens.
Despite Marshall et al.’s model being reported in 1995, the entire model has not been systematically tested. Marshall, Hamilton, and Fernandez (2001) used the Child Molester Empathy Measure (Fernandez, Marshall, Lightbody, & O’Sullivan, 1999) to assess empathy in child molesters and Fernandez and Marshall (2003) used a modified version of the measure to test empathy in rapists. However, these measures assess the perspective taking and emotional response stages of the Marshall et al. model (Fernandez & Marshall, 2003) only. Hence, the first and last stages of the model have not been evaluated and these aspects of empathy are generally overlooked, even though they are fundamental stages in the empathy process. If offenders are not able to recognize others’ distress, for example, they will not apply the skills that may have been developed in treatment programs, which renders the treatment component ineffective. In 1993, Hudson, Marshall, Wales, and McDonald reported that sex offenders were deficient in recognizing emotions in others, especially anger, disgust, surprise, and fear and argued that treatment should include elements that enabled offenders to recognize these emotions; yet it is not clear that this element is included in most treatment programs or even what form effective intervention in this area should take.
The lack of agreement as to how the concept of empathy should be defined/modeled has the result that different measures of empathy are based on different conceptualizations. Of the three most commonly used generalized empathy measures, Hogan’s Empathy Scale (HES; Hogan, 1969) places greater emphasis on the cognitive element rather than the affective element. The Questionnaire Measure Emotional Empathy Scale (QMEE; Mehrabian & Epstein, 1972) measures the affective conceptualization of empathy, as the contents of the scale subsets are related to susceptibility to emotional contagion (Zhou, Valiente, & Eisenberg, 2003). The Interpersonal Reactivity Index (IRI; Davis, 1980, 1983) was designed to measure both cognitive and affective empathy. These differences limit the comparability of research studies that have used different measures, which may account for some of the differences in research findings. In addition, the reliability and validity of these scales has been challenged and is well documented (e.g., Blake & Gannon, 2008; Chlopan, McCain, Carbonell, & Hagen, 1985; Tierney & McCabe, 2001). The suitability of comparison/control groups in studies testing for empathy deficits in sex offenders has also been challenged (see, for example, Brown & Walker, in press).
That a person has a specific level of empathy that they apply equally to all people in all situations seems to be a fundamental flaw in the conceptualization of empathy generally and indicates that much more research and theoretical developments are required for this concept. The fact that the application of empathy varies from person to person, and situation to situation, is actually supported by some sex offender research and indicates that empathy is more closely tied to cognitions (attitudes, justifications, denial, minimization, etc.) than models and conceptualizations of empathy tend to suggest. Despite not finding evidence to suggest that sex offenders have generalized empathy deficits (Marshall et al., 1995; Marshall, Jones, Hudson, & McDonald, 1993), Marshall et al. (1995), Marshall, Champagne, Sturgeon, and Bryce (1997), and Fernandez et al. (1999) found that child molesters displayed empathy deficits toward children who have been sexually abused and even greater deficits toward their own victim(s). A small number of studies have provided support for the view that sex offenders display lower levels of empathy for nonspecific victims (with child molesters: Fisher, Beech, & Browne, 1999; McGrath, Cann, & Konopasky, 1998; Wood & Riggs, 2008; and in rapists: Hanson & Scott, 1995; Marshall & Moulden, 2001; Rice, Chaplin, Harris, & Coutts, 1994) and for their own victims (with child molesters: Webster & Beech, 2000; and rapists: Marshall & Moulden, 2001).
Teuma, Smith, Stewart, and Lee (2003), however, found that child molesters did not differ significantly from a nonoffender community sample in empathy levels for a sexual abuse victim of an unknown perpetrator. Similarly, Hanson and Scott (1995) did not find differences between sex offenders who had abused children and comparison groups (though, as noted above, differences were noted with rapists). Hennessy, Walter, and Vess (2002) found that rapists had higher victim empathy levels than controls. Moreover, no differences in this aspect of empathy were identified between child molesters and controls. Fernandez and Marshall found that rapists were not deficit in empathy toward nonspecific victims compared with nonoffenders, though they did have less empathy toward their own victims but were more empathic toward women generally. Buschman, Wilcox, Spreen, Marshall, and Bogaerts (2008) found that sex offenders reported less empathy for their own victim than a nonspecific victim but less empathy for a car accident victim than their own victim. Thus, although there seems to be more support for the view that sex offenders display lower levels of empathy toward their own victims, the findings are far from conclusive.
Studies show that empathy can be enhanced/developed in professional groups such as nurses (Wheeler & Barrett, 1994), psychology students (Hatcher et al., 1994), and medics (Chen, LaLopa, & Dang, 2008); however, the efficacy of programs that look to teach/develop empathy to sex offenders have demonstrated mixed results (Beech, Fisher, & Beckett, 1999; Marshall et al., 1997; Pithers, 1994; Ricci, Clayton, & Shapiro, 2006; Schewe & O’Donohue, 1993; Wastell, Cairns, & Haywood, 2009). Most treatment programs have many components and they are evaluated in their entirety and so there is a dearth of information about the efficacy of, and contribution to, overall treatment impact of each treatment component. Thus, it is not currently possible to assess the extent to which work aimed toward enhancing empathy and/or victim empathy links to treatment outcome.
When offenders are asked about their views of treatment programs, sex offenders report that they find the empathy component beneficial and that it has a large impact on them (Beech et al., 1999; Brown, 2000; Fentem, 2007; Wakeling, Webster, & Mann, 2005). This adds to the confusing picture with respect to this treatment goal and the reluctance to remove it from programs. In terms of the “link” between empathy and recidivism, however, the research evidence suggests that empathy is not related to sexual recidivism. In their meta-analyses that incorporate data from substantial numbers of offenders, Hanson and Bussière (1996, 1998) and Hanson and Morton-Bourgon (2004, 2005) found that victim empathy is not related to recidivism. This led some to question the importance of including an empathy component in treatment programs. However, there have been doubts about the quality, reliability, and validity of some of the measures of empathy employed by the studies incorporated into these meta-analyses and the variability of the measures included (Mann & Barnett, in press), such that “it may be overly hasty to conclude from Hanson and colleagues’ meta-analyses that deficits in victim empathy are unrelated to sexual offender recidivism” (Mann & Barnett, in press, p. 16).
The purpose of this study, therefore, was to examine the relationship between victim empathy, general empathy, static risk, treatment outcome, and sexual recidivism. It was hypothesized that treatment would have an impact on victim empathy and that change would be linked to overall treatment change. The potential moderating role of empathy on static risk level was also examined. Here, it was predicted that victim empathy would predict recidivism, but that empathy would moderate static risk.
Method
Settings
The sample consisted of offenders who had completed sex offender treatment programs in the United Kingdom during the 1990s in two settings: one group completed treatment in the community and one group in custody. The first community sample, 67 men, completed treatment in the early 1990s in probation service programs or a residential program that were evaluated by Beckett et al. (1994). The probation programs had between 47.5 and 60 treatment hours, whereas the residential program had 60 to 1,000 treatment hours. The incarcerated sample of 100 men completed the Core Sex Offender Treatment Programme (Beech et al., 1999; Mann, 1999) delivered in the English and Welsh Prison Service in the mid 1990s. Hours in treatment ranged from 74 to 160 hr. The samples were combined into one data set by Harkins and analyses using this data set have been reported by Harkins, Beech, and Goodwill (2010) in relation to denial, motivation, and risk.
Participants
The entire combined sample consisted of 167 adult male sexual offenders who had completed a treatment program in the United Kingdom. As some research suggests differences in empathy between offenders who abuse children and those who abuse adults (Hennessy et al., 2002; Pithers, 1999; Smallbone, Wheaton, & Hourigan, 2003), and that there was a comparatively limited number of offenders who abused adults in the sample, only those with a conviction for a sexual offense against children were included in the analysis (n = 159). Of these offenders, pre- and posttreatment victim and general empathy data were only available for 120 offenders and, of these, survival data were not available for 15. Analyses were therefore conducted on 105 offenders who had a mean age at index offense of 37.6 (SD = 10.7) and mean age at release of 44.4 (SD = 10.7). One third of the sample (n = 34; 42.4%) had been previously convicted of a sexual offense, one tenth (n = 11; 10.5%) of a nonsexual violent offense, and two fifths (n = 42; 40.0%) had been previously convicted of nonsexual nonviolent offenses. The majority (n = 68; 64.8%) of offenders had perpetrated against female victims, whereas one fifth (n = 23; 21.9%) offended against male victims and just above one tenth (n = 14; 13.3%) had perpetrated against both male and female victims. Three fifths of the sample’s (n = 63; 60.0%) victims were familial, one third (n = 35; 33.3%) extrafamilial, while the remaining offenders (n = 7; 6.7%) offended against both types of victims. For the community sample, the mean treatment hours was 183.8 (n = 63; SD = 218.6) and for the prison sample, the mean hours was 128.1 (n = 42; SD = 42.26). Although the number of treatment hours varied, there was no significant difference in the number of hours attended between those who showed treatment change (n = 29; M = 143.0; SD = 111.0) and those who did not (n = 75; M = 154.1; SD = 155.8), t = 0.35; df = 102; p = .726, or those sexually reoffended (n = 14; M = 157.9; SD = 185.7) and those who did not (n = 95; M = 149.3; SD = 137.4), t = −2.09; df = 103; p = .835.
Measures
Victim Empathy Scale (VES)
This is a 28-item scale (Beckett & Fisher, 1994) that measures sex offenders’ views of the impact of their offending on their victims. This questionnaire is filled out by offenders with their most typical victim in mind, or by using a general scenario. It examines the extent to which offenders believe victims enjoy, encourage, or are able to stop sexual contact; experience fear and guilt; and whether victims would want it to happen again in the future. A response can “score” between 0 and 3 or can be discarded because the response is “don’t know.” The whole test is scored by calculating the error score, which is the raw score as a percentage of the maximum possible total score (that is the maximum score possible after eliminating questions responded to with a “don’t know”). Scores are therefore reported as percentages, with lower scores indicating higher levels of victim empathy. The scale has high internal reliability with an alpha coefficient of .90 (Beech et al., 1999). Beech and his colleagues (1999) reported a test-retest reliability of .95 and an internal consistency of .89. The validity of the scale is confirmed by Beckett et al. (1994) who showed that there was a significant difference between the mean scores of offenders reporting on their own victims and nonoffenders reporting on a selection of vignettes.
Interpersonal Reactivity Inventory (IRI)
The IRI is a 28-item index (Davis, 1980, 1983) that measures four components of empathy: perspective taking (PT), empathetic concern (EC), fantasy (FS), and personal distress (PD) with lower scores indicating lower levels of empathy. The value of these subscales is their ability to divide empathy into its cognitive and emotional components (Beckett et al., 1994). PT measures the ability to assume, cognitively, the role of the other; EC measures feelings of warmth, compassion, and concern for another; FS measures the ability to identify with fictional characters; and PD measures the extent to which one feels anxious and uncomfortable when witnessing the distress of others. Each subscale contains seven items scored using a 5-point scale, ranging from 0 = does not describe me well to 4 = describes me very well. Hence, scores on each scale can range from 0 to 28, with lower scores denoting lower levels of empathy. A four-factor structure has been confirmed by Davis (1980) and Carey, Fox, and Spaggins (1988). The scale is internally consistent with alphas ranging from .71 to .77 (Davis, 1980). Test-retest reliabilities range from .62 to .71 (Davis, 1980).
RM 2000
This measure (Thornton et al., 2003) was developed to assess risk for sexual recidivism and is widely used in the United Kingdom as it has been adopted nationally by the Prison and Probation Services (now combined into the National Offender Management Service) and Police Forces. Risk is assessed by first placing individuals into low, medium, high, or very high risk categories based on three static risk factors: age at commencement of risk, number of court appearances for sexual offenses, and total number of criminal court appearances. This category is then moderated by four aggravating static risk factors: male victim, stranger victim, noncontact sexual offenses, and lack of a long-term intimate relationship. If two of these factors are present, the risk category is raised one level; if all four are present, raised two levels. A sample of 647 male prisoners at risk for at least 2 years and another group of 429 male prisoners followed up for 16 years were included in the construction data set. The area under the curve (AUC) statistic of 0.75 and 0.77 were reported, respectively, for the two samples, which indicates a good level of predictive accuracy.
Procedure
The original data set was developed by Harkins (2007) who determined Risk Matrix categories from the information contained for each offender in the data set and calculated the treatment change variable blind to the recidivism outcome data. To calculate the treatment change variable, principal components analysis with varimax rotation was used to examine the factor structure of the variables, which were the offenders’ scores on the battery of psychometrics used to assess offenders at pre-and posttreatment and included the Multiphasic Sex Inventory (Nichols & Molinder, 1984), Self-Esteem Scale (Thornton, 1989; Webster, Mann, Thornton, & Wakeling, 2007), UCLA Loneliness Scale (Russell, Peplau, & Cutrona, 1980), IRI PD Scale (Davis, 1980), the Social Response Inventory (SRI; Keltner, Marshall, & Marshall, 1981), Nowicki-Strickland Locus of Control (Salter, 1976/1988), Victim Empathy Scales (Beckett & Fisher, 1994), Beliefs About Children Scale (BACS; Beckett, 1987), and the Special Hospitals Assessment of Personality and Socialisation (SHAPS; Blackburn, 1982). Inspection of the scree plot and eigenvalues produced by a principal components analysis suggested that a four-factor solution was optimal. Principal axis factoring was then used to extract four factors, which together accounted for 65.3% of the variance in the data. The expected dynamic risk domains were accounted for reasonably well by the four factors. Factor 1 (accounting for 21.44% of the variance) contained measures related to the Socioaffective Domain. These measures were SRI Underassertiveness, IRI PD, Locus of Control, UCLA Emotional Loneliness, Self-Esteem Scale, and Multiphasic Sex Inventory (MSI) Cognitive Distortions. Factor 3 (accounting for 14.25% of the variance) contained measures related to the Sexual Interests Domain, particularly MSI Paraphilias, MSI Sexual Obsessions, and BACS Emotional Congruence. Items related to the Distorted Attitudes Domain loaded onto Factor 4 (accounting for 12.08% of the variance). These measures were MSI Justifications, BACS Cognitive Distortion, and Victim Empathy Scale. An overall treatment effect was measured by combining the scores on the measures for each domain and determining if the participant exhibited overall change on this domain. As the SHAPs was only assessed at pretreatment, it was not possible to identify treatment change in the second domain and so the individual was deemed to have demonstrated overall treatment change if he demonstrated change on two of the three remaining domains. To avoid circular findings in this study in comparisons with empathy measures, the original treatment change variable was recalculated, with the PD Scale of the IRI omitted from Domain 1 and the VES omitted from Domain 4.
For this study, the data set was examined to determine the links between empathy, treatment outcome, risk, and recidivism using a sample of 105 sexual offenders who were at risk in the community (i.e., with time returned to custody for nonsexual subtracted from the difference between release and follow-up) for at least 10 years (M = 10.2 years; SD = 35.8 months). Official reconviction data were collected from the Home Office Offenders Index (OI) and Police National Computer (PNC) in the United Kingdom, where the data revealed that 14 (13.3%) offenders were convicted of a sexual offense, 3 (2.9%) of a nonsexual violent offense, and 17 (16.2%) of a nonsexual, nonviolent offense.
To investigate the relationship between victim empathy, empathy, and recidivism, Kaplan-Meier survival analysis was employed as this method controls for time-at-risk by estimating the cumulative survival function at each time that an event (e.g., a sexual reconviction) occurs. This method appropriately incorporates censored data (Tabachnick & Fidell, 2001). Here, as per Harkins (2007), scores on the various measures were assessed as whether they were in the functional range (i.e., the range of scores more commonly found among nonsex offenders) of these scales pre-and posttreatment and whether they had moved to a clinically significant extent in and out of these ranges. Thus, offenders could be in three categories: (a) offenders who were in the functional range at pretreatment and remained there posttreatment, or started in the dysfunctional range at pretreatment and demonstrated clinically significant change being in the functional range at posttreatment, (b) offenders who started in the dysfunctional range pretreatment and remained there posttreatment, (c) offenders who were clinically significantly worse at posttreatment compared with pretreatment, ending in the dysfunctional range at posttreatment. This variable was used to compare time with sexual reconviction using Kaplan-Meier survival analyses. To examine the relationship between victim empathy, risk, and recidivism, hierarchical Cox regression was used as it is a type of survival analysis that relates one or more variables to the risk that an event (e.g., sexual reconviction) will occur (Wright, 2000).
Results
Pre- and posttreatment mean scores in the complete sample of 105 offenders were examined to assess whether the group demonstrated statistically significant treatment change in the VES and the four subscales of the IRI as shown in Table 1. It can be seen in Table 1 that VES scores improved considerably following treatment (t = 6.70; df = 102; p = .001) as lower scores demonstrate higher levels of empathy on this measure. In comparison, there were only very small changes in the mean scores across three subscales of the IRI, which were not statistically significantly different. Only the PD Scale demonstrated a statistically significant change (t = 2.54; df = 104; p = .013) in the desired direction (i.e., a lower score at posttreatment indicative that individuals are better able to feel negative emotions after treatment).
Group Means (and Standard Deviations) at Pre- and Posttreatment on the Four Subscales of the IRI and the VES and Pair t test t and p Values

Note: IRI = Interpersonal Reactivity Index; VES = Victim Empathy Scale.
Denotes a difference in the desired direction, that is, higher levels of empathy at posttreatment compared with pretreatment.
p ≤ .05. ***p ≤ .001.
When the pre- and posttreatment scores of the group of offenders who had demonstrated an overall positive treatment outcome were compared with the scores of the offenders who had not demonstrated such change (see Table 2), statistically significant differences were found at the 5% level for posttreatment VES scores (t = 2.56; df = 68; p = .013) and PD scores (t = 2.13; df = 102; p = .04). These findings suggest that levels of general empathy are not predictive of treatment change and that pretreatment VES scores could not be used to identify offenders who may be more responsive to treatment change. Posttreatment VES scores were not included in the treatment change calculation, so it is of interest to note that the group that demonstrated this change also had significantly higher levels of victim empathy posttreatment compared with the offenders who did not demonstrate overall treatment change.
Group Means (and Standard Deviations) Comparing IRI Subscale and VES Means at Pre- and Posttreatment in the Group That Demonstrated Overall Treatment Change With the Group of Offenders That Did Not Demonstrate Such Change
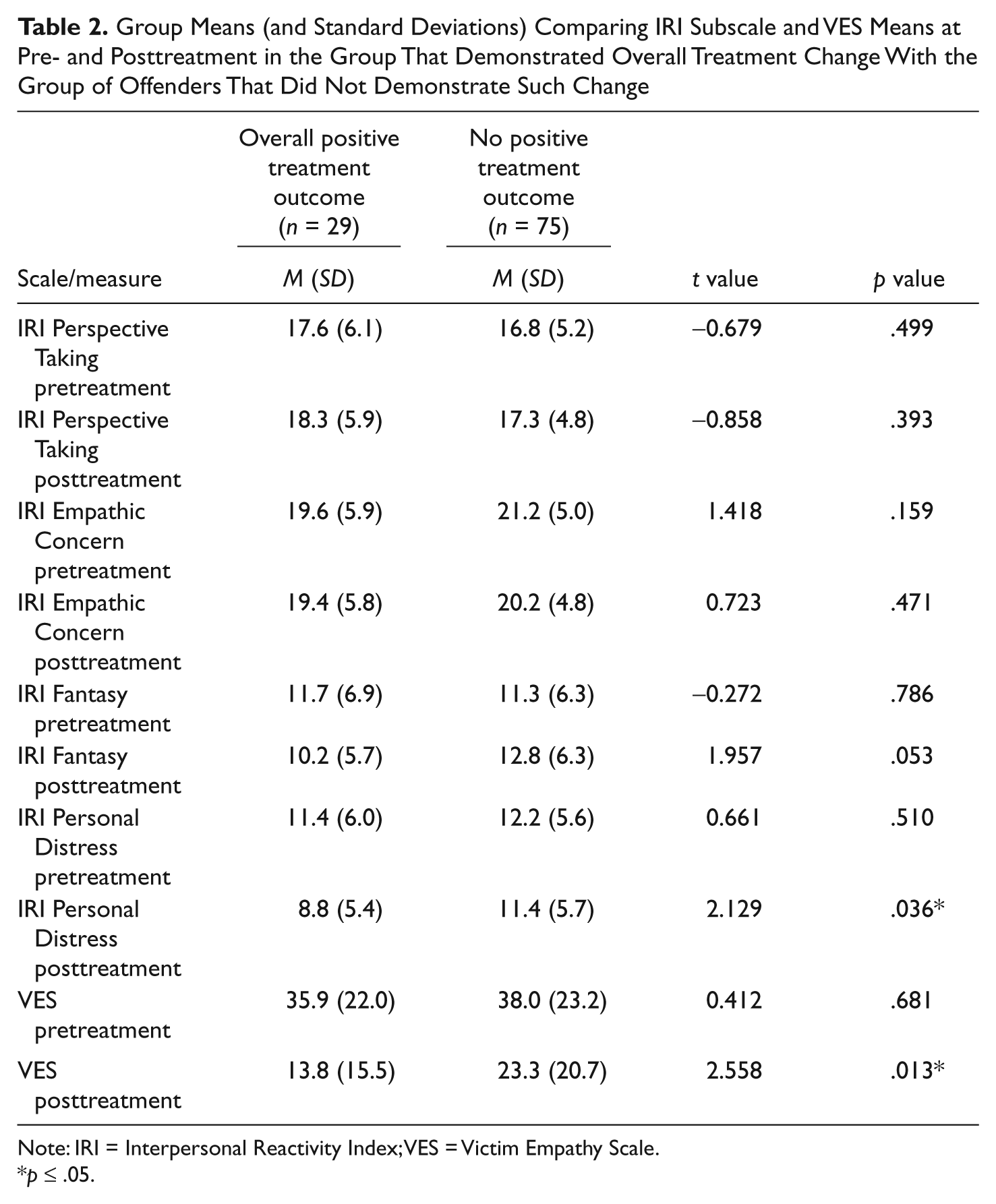
Note: IRI = Interpersonal Reactivity Index; VES = Victim Empathy Scale.
p ≤ .05.
Offenders who had sexually reoffended in the follow-up period were compared with those who had not using the VES and IRI data, as shown in Table 3. As only three offenders reoffended by committing a violent offense, comparisons between these offenders and the rest of the sample were not conducted. It can be seen here that only the posttreatment VES scores (t = −2.38; df = 103; p = .019) and pretreatment PT scores (t = 3.48; df = 17; p = .001) demonstrated statistically significant differences.
Group Means (and Standard Deviations) Comparing IRI Subscale and VES Means at Pre- and Posttreatment in the Group That Sexually Reoffended in the 10-Year Follow-Up Period With the Group of Offenders Who Did Not
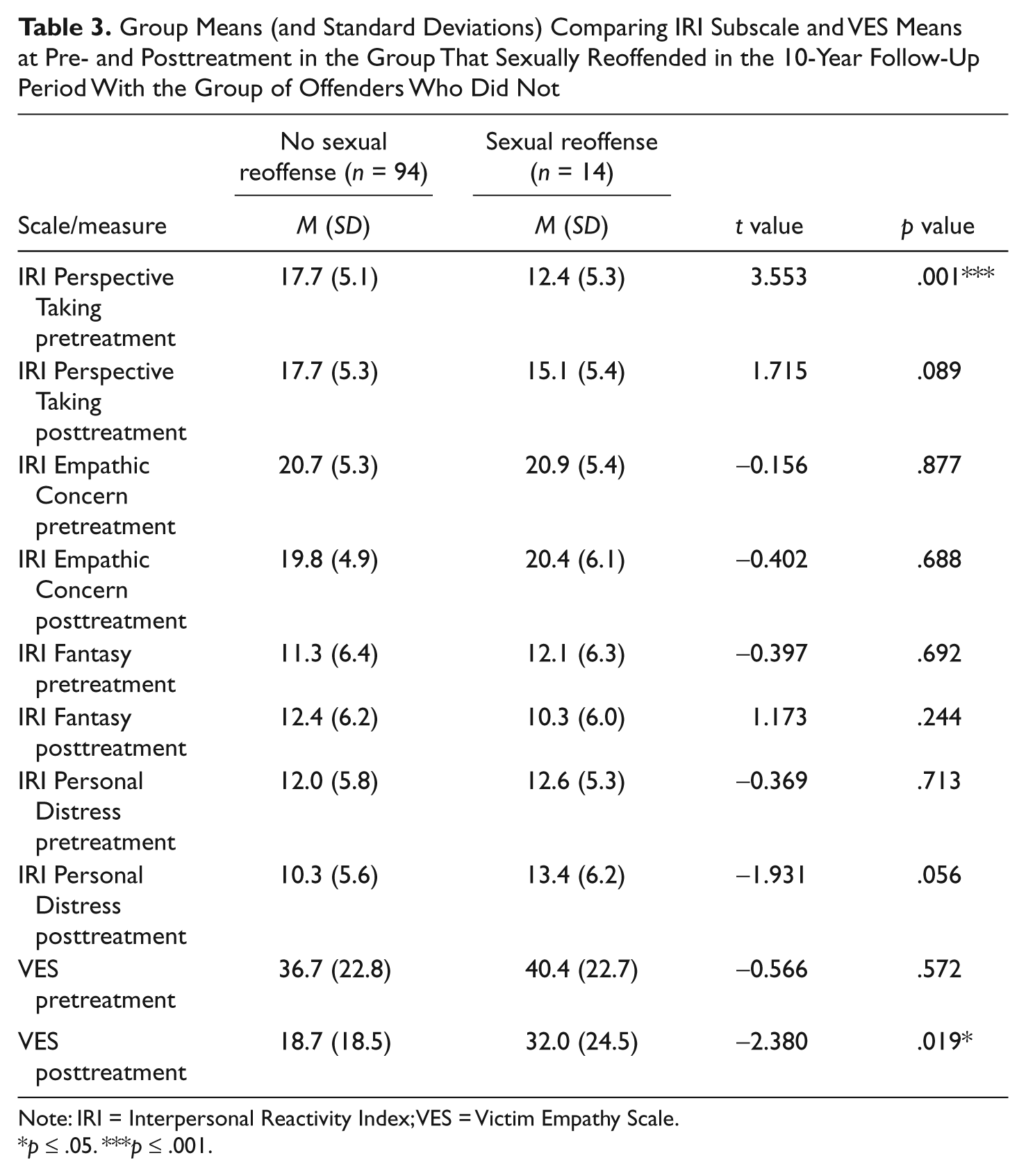
Note: IRI = Interpersonal Reactivity Index; VES = Victim Empathy Scale.
p ≤ .05. ***p ≤ .001.
As statistically significant treatment change was only demonstrated on the VES and the IRI PD scales, only these were included in the rest of the analysis, here the three categories of treatment response were used: (a) functional range at pre- and posttreatment, (b) dysfunctional range pre/posttreatment, (c) clinically worse, functional to dysfunctional after treatment. Post hoc pairwise comparisons revealed that there was a statistically significant difference between the clinically worse group (n = 10), compared with the functional group (n = 57; log rank = 7.85; p = .005). This variable was used to compare time to sexual reconviction using Kaplan-Meier survival analyses. Statistically significant differences were identified for the VES (see the survival curves in Figure 1). No statistically significant differences were found for the IRI PD Scale.

Kaplan-Meier survival curves for three groups of offenders categorized on presence of clinically significant treatment change and score on the Victim Empathy Scale in relation to the functional range of the measure
Finally, a hierarchical Cox regression analysis was conducted to assess if posttreatment VES scores could add anything to static risk as measured by the RM 2000 in terms of predicting sexual recidivism (see Table 4). Posttreatment VES scores made a contribution to the prediction of sexual recidivism at the 5% significance level.
Hierarchical Cox Regression Analyses Using Static Risk (Risk Matrix 2000) alone, and Static Risk and Posttreatment VES Scores to Predict Sexual Recidivism (n = 101)
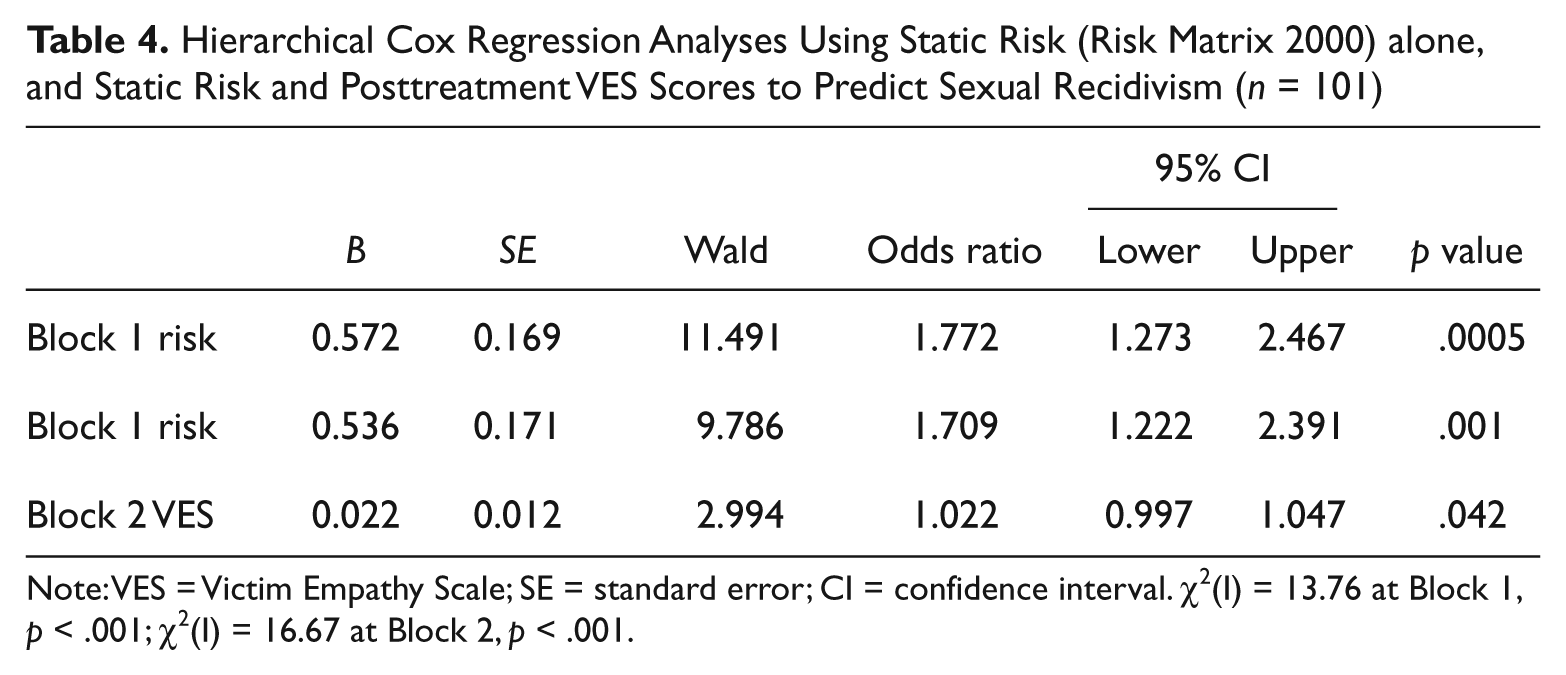
Note: VES = Victim Empathy Scale; SE = standard error; CI = confidence interval. χ2(I) = 13.76 at Block 1, p < .001; χ2(I) = 16.67 at Block 2, p < .001.
Discussion
These main results of the article support the usefulness of victim-specific empathy treatment goals, as the findings indicate that sex offender treatment did have an influence on offenders’ appreciation of the impact of their offending on their victims. The fact that victim empathy was affected, but general empathy was not, lends support to the studies of Marshall and Fernandez and their colleagues (Fernandez et al., 1999; Marshall et al., 1995, 1997, 2001) that revealed that sex offenders do not have general empathy deficits, but do demonstrate reduced levels of empathy in respect of their own victims. However, the findings are contradictory to those of Teuma et al. (2003) and the reason for the contradictory findings of the latter study is not clear. If it is the case that sex offenders do not have generalized empathy deficits but display low, or no empathy, toward their own victims, then this may be more related to cognition than empathy per se, as essentially offenders deny, or minimize, the need to feel empathy for their victim(s), perhaps because they believe that the victim(s) initiated the sexual encounter, deserved it, and/or wanted it.
There is some support for this view, for example, Webster and Beech (2000) found that total scores derived from participants’ “victim apology letters,” which were generated during the empathy component of treatment, did not correlate with general measures of empathy but did correlate with psychometric measures of cognitive distortions about offenders’ victims. Furthermore, Marshall et al. (2001) found that the level of empathy child molesters exhibited toward their victims was significantly correlated with their level of cognitive distortions. Moreover, Walker and Brown (in press) have demonstrated that nonoffenders apply similar strategies and cognitions as has been demonstrated in the sex offender literature, to “excuse” and “justify” the hurtful behavior of having an affair. This results in the overall impression of a lack of empathy, despite the fact that there was no evidence to suggest that participants had empathy deficits/difficulties per se. This issue needs further investigation but has important implications for treatment in respect of the model of change for victim empathy treatment goals and the links between these and goals related to cognition, justification, denial, attitudes, and minimization, all of which can influence whether, or to what extent, empathy is “applied” to a specific person in a specific context/situation.
This would also suggest that models of empathy need revision to take into account the fact that empathy is not trait-like characteristic and that individuals can apply different levels of empathy, or no empathy at all, to different individuals, in different situations in ways that may be related to a wide range of other variables. Some of these issues have been given consideration when empathy is considered in relation to prosocial behavior, for example, the number of bystanders influences the level of response given to an individual in distress, or attitudes toward the distressed individual might limit the helping response (see Dovidio, 1984 for a review of empathy research in relation to altruism). However, empathy has tended to be viewed more simply, with these variables not given due consideration when empathy, or its absence, is linked to the commission of negative behaviors.
This study also revealed that levels of victim empathy at posttreatment added some value to the prediction of sexual offense recidivism in addition to the assessment of risk. Assessing risk at posttreatment and taking account of treatment performance is currently very difficult and there are no evidence-based, widely used methods. This finding needs replication but it suggests that investigation of the extent to which posttreatment victim empathy responses link to risk and later sexual recidivism may aid in the development of postintervention risk assessment. Perhaps, of more immediate practical use, and linked to the previous issue, is the finding that sex offenders who show a clinically significant deterioration in their VES scores, such that they are in the dysfunctional range posttreatment, present a higher risk of sexual recidivism even compared with those who start and end treatment in the dysfunctional range. The small numbers of offenders in this group mean that this finding can only be tentative at this stage and it is not clear why this group in particular would present a higher risk—perhaps individuals who demonstrate such a pattern in their VES responses found treatment particularly difficult or did not wish to engage with it and/or became more antagonistic toward the victims of abuse as a result. Clearly, these suggestions are very speculative and much more research would be needed to investigate the link between victim empathy and treatment change. Nevertheless, it is an interesting finding that warrants further exploration as it may prove to be useful in terms of risk assessment, particularly in relation to including treatment change to assessments of risk, and/or completing risk assessment posttreatment, which remains a difficult area of practice.
The results of this study show, however, that general empathy, at least as measured by the IRI, is not linked to overall treatment change and is not predictive of sexual recidivism in a treated group of offenders who sexually offended against children. Furthermore, three scales of the IRI showed no overall treatment change in the sample. In relation to the PD Scale, change was demonstrated that indicated offenders were better able to deal with negative emotion, which would be expected posttreatment. These findings support the calls (see, for example, Marshall & Eccles, 1995) for, and growing trend in, sex offender treatment practice to move away from treatment goals targeting the enhancement of generalized empathy toward those targeting the development of victim-specific empathy.
Limitations and Directions for Future Research
Research examining the impact of sex offender treatment that includes a wide range of treatment goals/components on one specific goal/construct is rare, which means that although this research is novel, it is difficult to compare the findings of others studies in a detailed manner. The study also has a number of other limitations. Although the entire data set was relatively large, the extent of missing data and the need to exclude offenders who sexually offended against adults means that the sample included in the analyses is relatively small. In particular, the noteworthy group that is potentially at high risk is very small, meaning that further research is required to validate and extend the results of this study. Reliable recidivism data require that offenders are at risk for considerable periods of time and so this study, like many others, suffers from the fact that the treatment that was provided to the offenders in the sample has now been revised: nevertheless, revisions in relation to empathy have been made in respect of shifting treatment goals more toward victim empathy and so it is likely that the impact of such changes will be to support the findings of this study, though clearly this needs further investigation. While the offenders included in the study all offended against children, they were a heterogeneous group, for example, including intra- and extrafamilial offenders.
It should be noted that the nature of empathy itself is still relatively unclear, in terms of how it relates to cognitive distortions and other cognitive or affective traits and processes. This issue is potentially compounded by the self-report nature of the measures used, which could be seen as reflecting self-perception (or self-perception as filtered through impression management), as opposed to actual performance in empathetic functioning. Without a clear understanding of the construct of empathy, as applied to sexual offending and the treatment process, our efforts in this area remain somewhat murky. However, this issue has of course long been a problem for our field, and it is beyond the scope of the current study to provide definitive answers to these issues.
Conclusions
Work to develop empathy in sex offenders has been considered an important part of sex offender treatment programs since the development of early cognitive-behavioral treatment programs, although, more recently, many have suggested and many programs have been revised to focus more specifically on developing empathy toward sexual offense victims and perpetrators’ own victims. This study provides further support for these developments and suggests that general empathy is not related to sex offending, treatment change, and/or sexual recidivism. The fact that many offenders highlight the empathy component as an important and valuable aspect of treatment, no doubt alongside the similar views of therapists and treatment providers, has led to a reluctance to omit empathy work, despite the limited empirical support for its inclusion. This study, however, provides support for the continued use of empathy work, as offenders demonstrated change in victim empathy, although it cannot be shown that it was the empathy component of treatment per se that produced this change. Moreover it identified a specific group of offenders, those whose VES scores were clinically significantly worse at post-treatment compared to pre-treatment, ending treatment in the dysfunctional range, who were more likely to sexually recidivate compared to the rest of the sample. Furthermore, posttreatment VES scores contributed to the prediction of sexual offense recidivism in addition to the assessment of risk. Although these findings need validation, they may prove to be useful in assessing the posttreatment risk of offenders and/or in incorporating treatment progress into sex offender risk assessments.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.