
Abstract
Current approaches to violence risk assessment are focused on the identification of factors that are predictive of future violence rather than factors that predict desistance. This is also true for the popular tools designed to predict adolescent sexual recidivism. Research on strengths-based variables with adolescents who have sexually offended that could serve a protective function is only recently underway. In the current prospective study, scores from clinician-completed assessments using the Estimate of Risk of Adolescent Sexual Offense Recidivism (ERASOR) and the parent-completed form of the Behavioral and Emotional Rating Scale (BERS-2) were evaluated in a sample of 81 adolescent males with at least one sexual offense. As expected, the ERASOR was significantly correlated with sexual recidivism over an average 3.5-year follow-up. In terms of a protective function, the Affective Strength scale of the BERS-2 was significantly negatively correlated with sexual recidivism, although it did not have incremental validity over and above the ERASOR. The BERS-2 School Functioning scale was significantly negatively correlated with nonsexual recidivism. The results are discussed in terms of previous findings and theoretical work on attachment in sexual offending behavior and implications for risk assessment practice.
Research in the area of violence risk assessment has been focused almost exclusively on the identification of factors that predict risk rather than on the identification of factors that predict desistance from reoffending (Rogers, 2000). It has been pointed out that this focus on risk-only factors in risk assessment tools has likely resulted in inaccurate and biased judgments by clinicians (e.g., Miller, 2006). Indeed, Farrington (2007) has recently stressed that researchers should now work to enhance the accuracy of violence risk assessments by identifying factors that are predictive of desistance.
There are several ways in which factors might predict desistance from reoffending (Luthar, 1993; Masten, 2001). In the editorial to this special issue, we consider this issue in detail. Here, we distinguish between two general processes. Some factors may have a direct relationship with the outcome. A direct relationship could be understood most simply as a positive correlation with the dichotomous classification of having not recidivated at follow-up (or a negative correlation with the dichotomous classification of having recidivated at follow-up). Farrington and Ttofi (2011) refer to factors with this direct association as protective factors. As we note in the editorial to this special issue, it could be argued that such protective factors are simply the obverse of risk factors. Certainly, this may be the case for some factors that could be conceptualized on a continuum (as one possible example, interest in mutually consenting, age-appropriate sexual activities through to interest in interpersonally exploitative and abusive sexual activities). For such factors, the value in recognizing a protective function in terms of enhancing the predictive accuracy and clinical utility of risk assessments may be simply the change in emphasis, moving beyond the scoring of risk factors as present (to whatever degree) or absent. At the “protective” end of the continuum, the factor is not “absent”; it is present and negatively associated with recidivism (without this empirically demonstrated negative association with the outcome of interest, of course, the factor would not be considered a protective factor even though, conceivably, it may function as a risk factor). The practical (and potentially theoretical) value of such protective factors will be more easily discerned if the protective factor can be shown to have incremental validity when used in conjunction with established risk factors or tools.
For other factors, there may be an interaction effect with known risk factors such that the protective factor can be shown to moderate the association between the risk factor and a recidivism outcome (that is, the protective factor reduces the strength of the risk factor’s association with a recidivism outcome, negating or partially negating the risk factor’s effect). Farrington and Ttofi (2011) have referred to such factors as interactive protective factors.
In addition to this distinction, it is important to be clear about the population and outcome for which the factors function as either protective or interactive protective factors. With a focus on adolescents who have sexually offended, a factor may be protective in terms of nonviolent recidivism, violent recidivism, or sexual recidivism, for example, but perhaps not all. Looking ahead for the field, any individual risk assessment would, ideally, incorporate empirically validated risk and protective factors (whether certain factors are conceptualized on a continuum or particular risk and protective factors are included as distinct items in a given tool) for each type of recidivism outcome, which are then used to support precise statements of the relatively likelihood of each outcome along with ways to lower these relative likelihoods.
Research on protective factors with adolescents who have offended sexually is currently at the germinal stage. One notable area that could usefully inform research efforts is the work on protective factors associated with desistance from general youth offending and violence. Of particular interest in this regard is the Structured Assessment of Violence Risk in Youth (SAVRY; Borum, Bartel, & Forth, 2006), a structured professional judgment risk assessment tool that has been shown to have moderate predictive validity, comparable with other widely used risk assessment tools for adolescent criminal recidivism (Olver, Stockdale, & Wormith, 2009). Unlike most of the available risk assessment tools for youth, the SAVRY includes, alongside 24 risk factors (in historical, social/contextual, and individual/clinical domains), a set of six protective factors, which the developers identified from the literature: Prosocial involvement, Strong social support, Strong attachments and bonds, Positive attitude toward intervention and authority, Strong commitment to school or work, and Resilient personality.
To date, however, only a few authors have examined the SAVRY-protective factors in follow-up research. Rennie and Dolan (2010) reported that the SAVRY-protective factors total score predicted desistance from any criminal recidivism among a sample of male adolescents (the percentage with historical or index sexual offenses was not reported). Lodewijks, de Ruiter, and Doreleijers (2010) reported that the SAVRY-protective factors total score predicted desistance from violent recidivism (including sexual assault) in each of three samples of male adolescents (3%-10% of which, the researchers noted, had an index offense that was sexual in nature). These researchers also found that the SAVRY-protective factors total score accounted for a unique portion of the variance in recidivism when combined with the SAVRY risk factors, and even served an interactive protective function too.
Schmidt, Campbell, and Houlding (2011) reported direct effects for the SAVRY-protective factors for both nonviolent and violent recidivism among male adolescents in their sample (again, the percentage with historical or index sexual offenses was not reported). Of interest, Schmidt et al. also examined sexual offending at follow-up but found the SAVRY-protective factors total score did not predict abstinence of this outcome. Similarly, in a study with adolescents with sexual offenses (rather than an undifferentiated sample of adolescent offenders), Spice, Viljoen, Latzman, Scalora, and Ullman (2012) found that none of the SAVRY-protective factors were related to desistance from sexual recidivism. One inference that can be made on the basis of these last two findings is that there may be protective factors that are predictive of desistance from adolescent sexual reoffending distinct from protective factors for nonsexual recidivism. This would not be surprising given that there are unique risk factors for adolescent sexual recidivism (Worling & Långström, 2006) and that risk assessment tools designed specifically for sexual recidivism typically outperform tools designed for general adolescent violent behavior when the target is sexual reoffending (Viljoen, Mordell, & Beneteau, 2012).
At this juncture for the field then, we would argue that it is in combination with an established risk assessment tool demonstrated to predict sexual recidivism that purported protective factors should be considered. For adolescents who have sexually offended, The Estimate of Risk of Adolescent Sexual Offense Recidivism (ERASOR; Worling & Curwen, 2001) and the Juvenile Sex Offender Assessment Protocol–Second Edition (J-SOAP-II; Prentky & Righthand, 2003) are among the most widely used tools designed to assist with predictions of future sexual reoffending (McGrath, Cumming, Burchard, Zeoli, & Ellerby, 2010), and both have been shown to have moderate levels of predictive accuracy (Viljoen et al., 2012). Importantly, these and other similar tools are made up almost exclusively of factors related to risk while efforts to develop assessment tools for use with adolescents who have sexually offended that consist of protective factors or that incorporate protective factors along with risk factors are only just beginning. In early work, Bremer (1998, 2006) developed the Protective Factors Scale (PFS) to assist with placement decisions for youth who had offended sexually; however, there is currently no empirical evidence to indicate that items on the PFS predict desistance or moderate the association between risk factors and recidivism outcomes. Efforts in the United Kingdom to develop an assessment tool comprised of both risk factors and strengths have resulted in the Assessment, Intervention and Moving on project (AIM2) (Griffin, Beech, Print, Bradshaw, & Quayle, 2008). But, again, empirical evidence is needed to determine its ability to predict desistance and whether its strengths moderate the association between risk factors and reoffending.
Thus far, we have concentrated our discussion on tools that are completed by the clinician or service provider. There are, however, several self-report and informant-completed questionnaire measures that are strengths-based and focus on protective factors, among which is the Behavioral and Emotional Rating Scales (BERS; Epstein & Sharma, 1998; BERS-2, Epstein, 2004). This tool has teacher, parent, and youth forms and is designed to assess the personal strengths a child or adolescent possesses according to their own or an informant’s perspective. The constructs measured form five scales tapping interpersonal strength, involvement with family, intrapersonal strength, school functioning, and affective strength (descriptions of these scales appear in the “Method” section). Although there has been little attention paid to the BERS-2 with adolescents involved in the youth justice system, preliminary findings are promising, and its potential utility with this population merits further investigation. Among a sample of 42 eighth-grade middle-school students, Epstein, Mooney, Ryser, and Pierce (2004) reported significant negative correlations between each of the Interpersonal Strength, Family Involvement, and School Functioning scales on the youth self-report form of the BERS-2 and both the Delinquent Behavior and Aggressive Behavior scales of the Youth Self-Report form (Achenbach, 1991). Pobanz (2000) found that both the School Functioning and Family Involvement scales had significant negative correlations with the seriousness of recidivism among 88 first-time juvenile offenders. The Family Involvement scale was also shown to account for a unique portion of the variance in serious recidivism in a regression model also containing risk factors. Notably, however, no statistically significant interaction effects between the risk and protective scales were found.
Given the dearth of research in the field, and the call to enhance the validity of risk assessments by including protective factors, there is a critical need to identify those protective factors that are predictive of desistance from reoffending by adolescents who have offended sexually. Furthermore, it is important that researchers investigate which outcomes purported protective factors actually exert their effect on. On the basis of the research on risk factors for sexual recidivism, we would expect there to be protective factors that are specific to sexual reoffending distinct from protective factors that are associated with desistance from other general types of recidivism; however, in light of mixed findings in the extant literature and the lack of clarity regarding what might be expected to protect against sexual recidivism, we do not advance specific hypotheses here. In the current study, we simply focus our investigation on main effects for purported protective factors and distinguish between sexual and nonsexual recidivism outcomes.
Method
Participants
Data were available for 81 adolescent males who had offended sexually. The youth were between 12 and 19 years of age at the time of assessment (M = 15.10, SD = 1.53), and they were convicted of and/or acknowledged criminal sexual behavior(s). These adolescents are a subset of those who were the subject of a larger prospective investigation that was focused on the predictive validity of the ERASOR (Worling, Bookalam, & Litteljohn, 2012). In particular, these 81 participants are those youth from the larger study for whom BERS data were available. Adolescents were assessed by 1 of 22 clinicians between January 2001 and October 2007 at one of five different agencies in Southern Ontario, Canada. ERASOR ratings were made immediately following comprehensive assessments which included clinical interviews, document review, psychological testing, and interviews with parents/caregivers. At the time of initial assessment, parents or caregivers were asked to complete the BERS as part of a comprehensive assessment of strengths and risks. For those youth who were placed away from home for a year or more, the primary residential staff or foster parent completed the BERS. Otherwise, parents or other familial primary caregivers completed the measure. For those youth who had been placed away from home for less than a year, and for whom both familial caregivers and residential staff completed the BERS, only those responses from familial caregivers were utilized. For the 81 participants in this investigation, therefore, the BERS ratings that were examined were provided by mothers (40), residential staff (26), fathers (7), foster parents (4), grandparents (3), or an aunt (1). None of the participants in this sample were residing in a secure custody facility at the time of assessment.
Measures
The ERASOR is a 25-item, single-scale instrument designed to structure professional judgments regarding the risk of sexual reoffending by youth aged 12 to 18. The ERASOR contains 25 risk factors: 9 static risk factors related to historical criminal sexual behaviors and 16 dynamic risk factors related to current sexual, familial, environmental, affective, and interpersonal functioning. As noted in our earlier investigation (Worling et al., 2012), the ERASOR was completed by clinicians immediately following comprehensive assessments that involved extensive interviewing with the adolescents, the completion of a number of tests and questionnaires, document review, and meetings with caregivers. In a recent meta-analysis of published and unpublished investigations, Viljoen et al. (2012) found that both a total score from the ERASOR and the ERASOR risk rating (low, moderate, or high) were significantly predictive of sexual reoffending. The moderate effect sizes for the ERASOR described by Viljoen et al. are comparable with the moderate effect sizes found in meta-analyses with adult risk assessment tools for sexual recidivism (Hanson & Morton-Bourgon, 2009) and with risk assessment tools for general adolescent criminal recidivism (Schwalbe, 2007). Two ERASOR predictors were examined in this investigation: the risk rating (low, moderate, or high) made by clinicians immediately following the assessment and the sum of risk factors rated Present.
The BERS–Parent Rating Scale (Epstein & Sharma, 1998; BERS-2, Epstein, 2004) was used to collect information from caregivers regarding the youth’s strengths. For those adolescents assessed between 2001 and 2003, the earlier version of the BERS was used in assessment; from 2004 until the end of data collection in 2007, the second edition of the BERS was used. It is important to note that there were no differences between the two versions of the BERS with respect to the test items or scales that were examined in this study. The second edition of the BERS has a 5-item scale that is focused on a youth’s career plans, and this was the only change to the item content of the BERS. These items were not addressed in the present investigation. The second edition of the BERS was normed on more than 2,000 participants from across the United States, and the test manual contains details regarding the reliability and validity of the test. For example, test–retest reliability (2-week) ranged from .85 to .99 for the individual BERS scales, and interrater reliability ranged from an r of .83 to .96. The test authors also report concurrent validity for the BERS scales utilizing additional adult-report measures of children’s behavioral and emotional functioning, and the results of a principal components analysis support the factor structure of the BERS scales.
There are five scales that are derived from the 52 items on the BERS. The Interpersonal Strength scale is based on 15 items, and it is designed to measure the youth’s ability to control their emotions and behaviors and to be respectful of others. Items on this scale are focused on issues such as respect for others, accepting responsibility, and the appropriate expression of anger. For the present study sample, an estimate of the internal consistency (Cronbach’s alpha) for this scale was .94. The Family Involvement scale measures the youth’s level of involvement with family members and the overall quality of family relationships. There are 10 items in this scale (Cronbach’s alpha of .85 for the present sample of 81 youth) related to relationships with parents and siblings, participation in family activities, and family communication, for example. The third BERS scale is Intrapersonal Strength. The 11 items (α = .85) that form this scale are designed to measure the youth’s view of their personal competence and outlook on life. Scale items are designed to tap issues such as self-confidence, popularity with peers, enthusiasm, and enjoyment. The School Functioning scale is based on 9 items (α = .89) and provides a measure of aspects of competence with school, including the youth’s ability to complete homework, attend school regularly, and study for tests, for example. The final scale is Affective Strength. The 7 items (α = .82) of this scale measure capacity for emotional intimacy, with a focus on the youth’s ability to give and receive affection, express feelings, show concern for others, accept closeness, and acknowledge painful feelings.
As noted in our earlier investigation, sexual recidivism data (criminal charges) for this prospective study were obtained from a national database of youth and adult criminal charges/convictions, a provincial database of adult (age 18 and over) criminal charges, and from reports from child welfare workers and/or probation officers when an adolescent had been criminally charged with a subsequent sexual crime. Unfortunately, we were not able to ascertain the dates of the sexual recidivism charges reported by the referral sources. Clinicians simply had data regarding whether the youth incurred subsequent charges for sexual offenses. Nonsexual recidivism was based on data from the national and provincial databases, as reports of subsequent charges for nonsexual crimes were not routinely collected from child welfare or probation offices. The follow-up period of this study ranged from 0.1 to 7.9 years (M = 3.66, SD = 2.08). Given that all of the youth in this investigation were living in the community, we felt that it was important to capture risk immediately following the assessment period. In recognition of the fact that it may take time for a sexual reoffense to be disclosed and investigated by authorities, however, we also examined separately the subsample of youth for whom there was a minimum follow-up period of 1 year.
Results
During the course of the follow-up period, the sexual recidivism rate for this sample was 8.6% (7 of 81), and the nonsexual recidivism rate was 11.1% (9 of 81). Table 1 contains the correlations among the five BERS scales, the two ERASOR variables, and both sexual and nonsexual recidivism. Mean scores for the BERS scale scores and the ERASOR sum of risk factors appear in Table 2.
Correlations (and Significance Levels) Among the Five BERS Scales, the ERASOR, and Recidivism (n = 81).
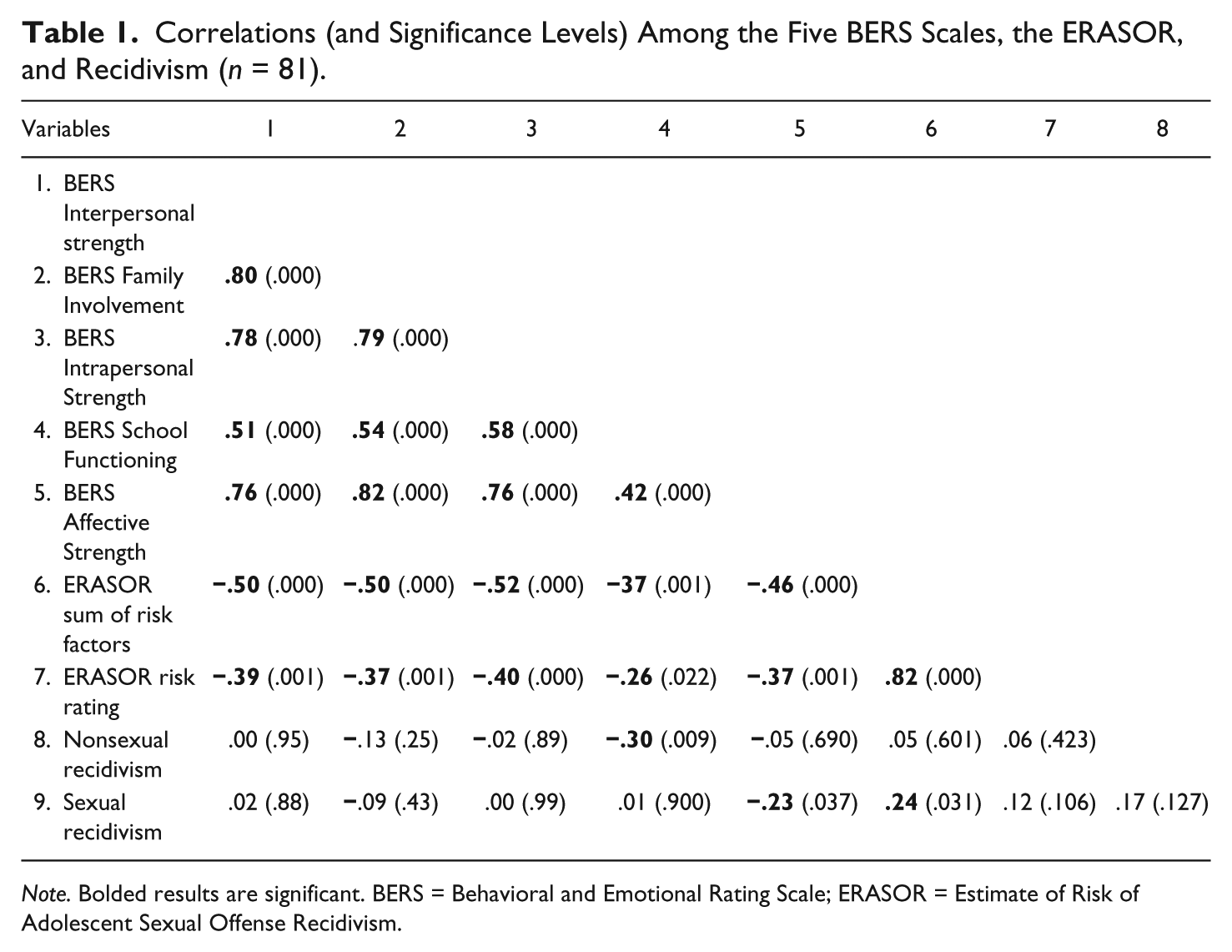
Note. Bolded results are significant. BERS = Behavioral and Emotional Rating Scale; ERASOR = Estimate of Risk of Adolescent Sexual Offense Recidivism.
Means (and Standard Deviations) for the BERS Scales and ERASOR Sum of Risk Factors by Recidivism Status.

Note. BERS = Behavioral and Emotional Rating Scale; ERASOR = Estimate of Risk of Adolescent Sexual Offense Recidivism; ERASOR sum = ERASOR sum of risk factors rated Present; BERS Is = BERS Interpersonal Strength; BERS FI = BERS Family Involvement; BERS IaS = BERS Intrapersonal Strength; BERS SF = BERS School Functioning; BERS AS = BERS Affective Strength.
Given the sample size and the relatively low recidivism rates, the area under the receiver operating characteristic curve (AUC) was calculated for each of the predictor variables (see Table 3); this statistic is reasonably robust with respect to base rates, selection ratios, and non-normative data distributions (Mossman, 1994). In their review of the accuracy of actuarial risk assessment tools for 81 samples of individuals who had offended sexually, Hanson and Morton-Bourgon (2009) reported a moderate average effect size of d = .67. This translates to a moderate AUC of .68 (Rice & Harris, 1995). As such, we anticipated that we should observe moderate predictive accuracy with the present sample.
AUC Values [and 95% CI] for the BERS Scales and the ERASOR Regarding Sexual and Nonsexual Recidivism for Two Follow-Up Intervals.
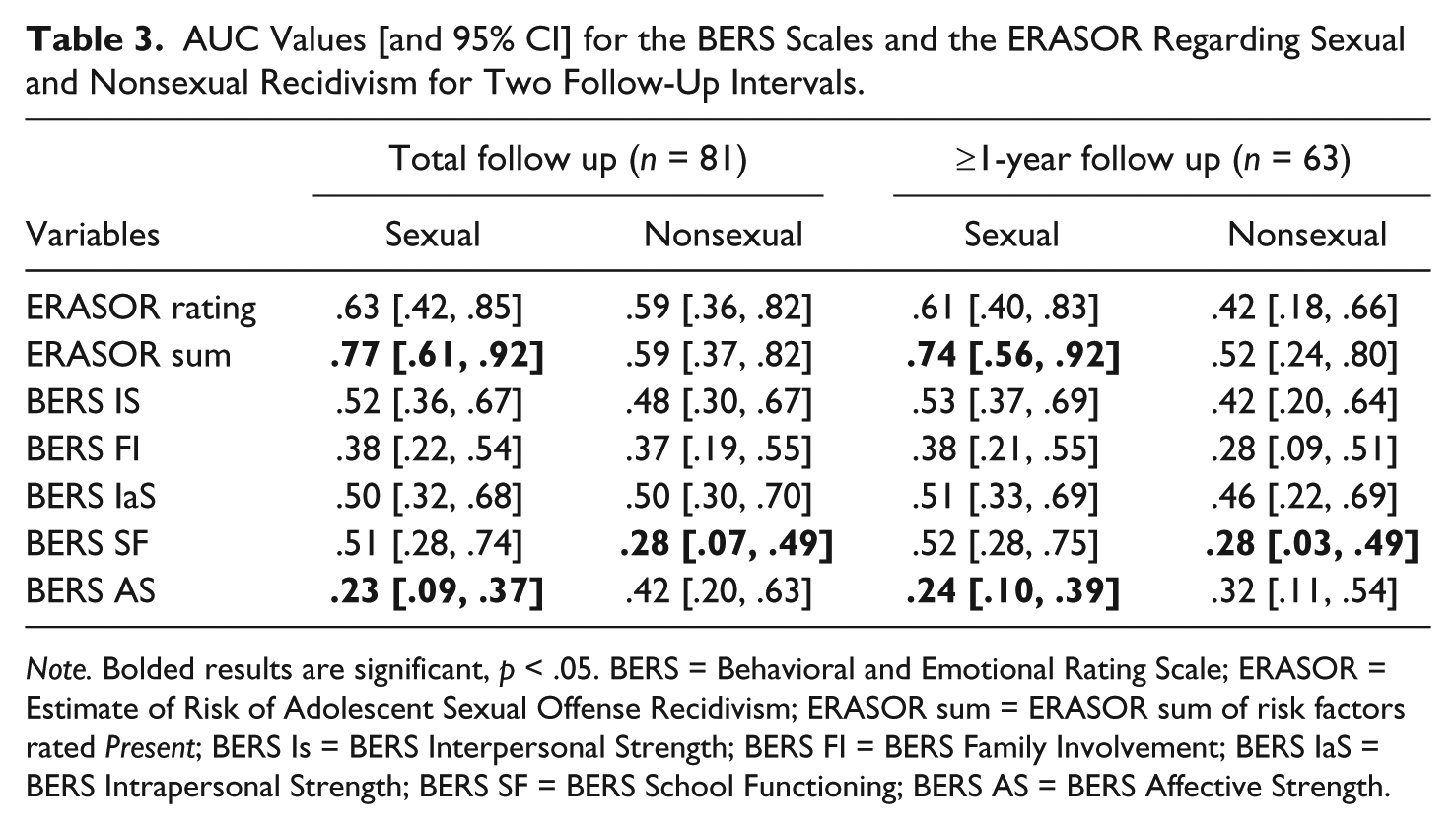
Note. Bolded results are significant, p < .05. BERS = Behavioral and Emotional Rating Scale; ERASOR = Estimate of Risk of Adolescent Sexual Offense Recidivism; ERASOR sum = ERASOR sum of risk factors rated Present; BERS Is = BERS Interpersonal Strength; BERS FI = BERS Family Involvement; BERS IaS = BERS Intrapersonal Strength; BERS SF = BERS School Functioning; BERS AS = BERS Affective Strength.
The BERS Affective Strength scale was found to be significantly predictive of desistance from sexual reoffending over the course of the entire follow-up period. The AUC of .23 indicates that 77% (i.e., 1-.23) of those who desisted from subsequent sexual crimes had a higher score on the Affective Strength scale relative to those adolescents who reoffended. As we found with the larger sample in our original study (Worling et al., 2012), the sum of risk factors rated Present on the ERASOR was also significantly predictive of sexual recidivism in this sample; 77% of those who reoffended sexually had more risk factors rated Present compared with those adolescents who did not reoffend sexually. There was no difference in the predictive accuracy between the ERASOR sum of risk factors and the BERS Affective Functioning score, z = 0, p = 1.0. For nonsexual recidivism, 72% (i.e., 1-.28) of those who desisted from nonsexual reoffending had higher scores on the School Functioning scale of the BERS. No other variables were predictive of nonsexual recidivism. As noted in Table 3, comparable results were obtained when analyses were limited only to those adolescents for whom we had follow-up data for a minimum of 1 year.
To determine whether information regarding strengths could add to the accuracy of sexual recidivism predictions beyond that provided by the ERASOR, a logistic regression was used where the ERASOR sum of risk factors was entered together with the BERS scales. The results for both sexual and nonsexual recidivism are presented in Table 4. The goodness-of-fit tests (Hosmer–Lemeshow) yielded a nonsignficant χ2 (8) of 13.79, p = .09, for sexual recidivism and a nonsignficant χ2 (8) of 7.47, p = .49, for nonsexual recidivism, which suggests that the resultant models fit the data well. Given the significant intercorrelations among the BERS scales, however, and the directional differences in the relationships between the BERS scales and the dependent variables in bivariate versus logistic regression analyses, it is possible that one or more of the BERS scales were operating as a suppressor variable. Therefore, we subsequently utilized stepwise logistic regression procedures to determine whether the BERS could account for unique variance beyond that already explained by the ERASOR. For sexual recidivism, the ERASOR sum of risk factors was a significant predictor, χ2 (1) = 4.72, p = .03. When the BERS Affective Strength scale was added at the next step, however, as it was the sole BERS scale correlated with sexual recidivism, it did not account for additional variance, χ2 (1) = 1.51, p = .22. Turning to nonsexual recidivism, the ERASOR sum of risk factors was not predictive of outcome when it was entered first in a stepwise logistic regression, χ2 (1) = 0.29, p = .60, and this is not surprising given that the ERASOR was not intended to be used to predict general criminal recidivism. When the BERS School Functioning scale was entered at the next step, as it was the only BERS scale correlated with nonsexual recidivism, it was a significant predictor of nonsexual reoffending, χ2 (1) = 6.94, p = .01.
Logistic Regression of ERASOR Sum of Risk Factors and BERS Scales on Sexual and Nonsexual Recidivism.
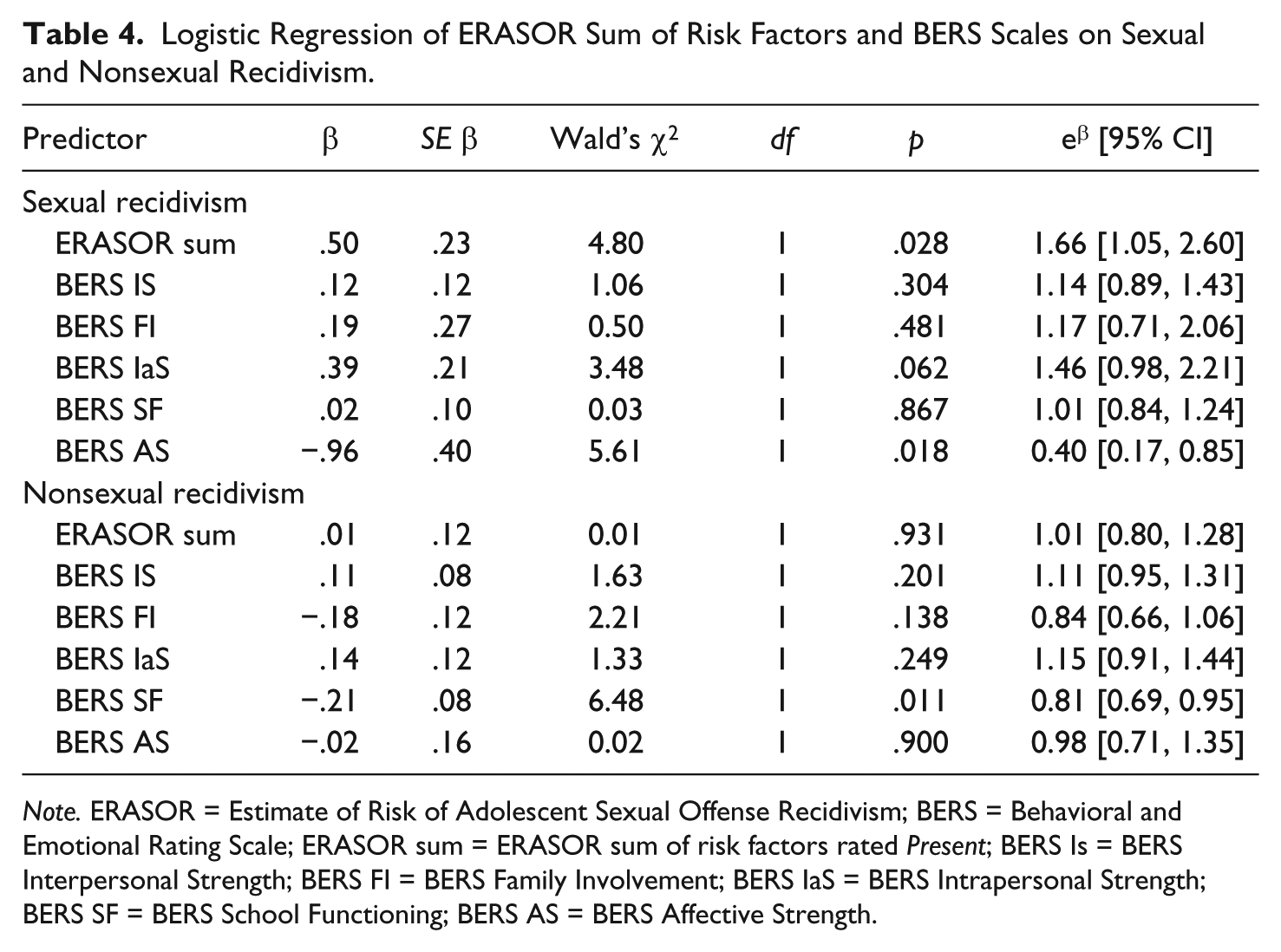
Note. ERASOR = Estimate of Risk of Adolescent Sexual Offense Recidivism; BERS = Behavioral and Emotional Rating Scale; ERASOR sum = ERASOR sum of risk factors rated Present; BERS Is = BERS Interpersonal Strength; BERS FI = BERS Family Involvement; BERS IaS = BERS Intrapersonal Strength; BERS SF = BERS School Functioning; BERS AS = BERS Affective Strength.
Discussion
The purpose of the present study was to determine if protective factors for adolescent sexual recidivism could be identified in a prospective investigation. During the course of a comprehensive assessment for a sample of 81 adolescent males, parents or caregivers completed the BERS—a norm-referenced measure of adolescents’ strengths. Immediately following each assessment, clinicians completed the ERASOR, which is an empirically validated, structured checklist of risk factors for sexual reoffending by adolescents. Recidivism data (criminal charges) were examined after an average follow-up period of approximately 3.5 years. It was found that the sum of risk factors rated Present on the ERASOR significantly predicted sexual reoffending. The BERS Affective Strength score was also predictive of sexual recidivism; however, it could not significantly enhance the predictive accuracy of the ERASOR. With respect to nonsexual crimes, the BERS School Functioning score significantly predicted desistance from continued nonsexual reoffending.
It is not surprising that different protective factors were related to sexual and nonsexual recidivism given that unique risk factors for adolescent sexual recidivism have been identified previously (McCann & Lussier, 2008; Worling & Långström, 2006). The BERS Affective Strength score was predictive of desistance from sexual reoffending in the present sample. This particular scale taps the capacity for emotional intimacy, as it includes a focus on expressing and receiving affection, acknowledging painful feelings, being concerned for the feelings of others, and accepting closeness with others. Affective bonding or attachment has proven a rich theoretical and empirical avenue for understanding human development and psychopathology across the life span (DeKlyen & Greenberg, 2008; Dozier, Stovall-McClough, & Albus, 2008). In research with adolescents, higher levels of insecure attachment have been found among those with serious substance use problems (e.g., Schindler et al., 2005), those involved in criminal behavior (e.g., Elgar, Knight, Worrall, & Sherman, 2003), and adolescents who have sexually offended against children (e.g., Miner et al., 2010).
This last finding is consistent with Marshall’s (1993) early theoretical work on attachment in sexual offending, in which he suggested that “childhood attachments and the adult capacity for intimacy are essential links in the chain of development underlying the emergence of an inappropriate sexual disposition” (p. 109). In essence, the absence of a secure attachment bond in childhood, in conjunction with other deficits in those who offend sexually, is thought to undermine the development of interpersonal skills needed to achieve intimacy with others in adolescence and adulthood (Rich, 2006). Certainly, among adults who have committed sexual offenses, intimacy deficits have been shown to correlate with sexual recidivism (e.g., Eher, Matthes, Schilling, Haubner-MacLean, & Rettenberger, 2012). The BERS Affective Strength score appears to provide an index of aspects of affective bonding that serve a protective function, having a direct association with desistance from further sexual offending among adolescents with sexual offenses.
It may, of course, be that other aspects of affective bonding serve a protective function for other general types of criminal recidivism among youth who have committed sexual crimes, but it is too early to know the extent to which operationalizations of constructs and measurement approaches impact findings. For example, Spice et al. (2012) found that the SAVRY-protective factor Strong attachments and bonds had a small but statistically significant negative correlation with nonviolent recidivism but not with sexual recidivism in their sample of 193 adolescents with sexual offenses. There simply is insufficient empirical work yet to draw firm conclusions about which constructs and measures of protective factors should be incorporated into comprehensive risk assessments with this population. At this stage, we would reiterate the recommendation we have made elsewhere that assessors consider strengths and purported protective factors within a comprehensive assessment, but that they refrain from adjusting appraised level of risk if such an adjustment or clinical override is not an explicit step in the process (Worling & Langton, 2012; see Rich, 2009, for an extended discussion of these issues).
Despite the lack of research regarding factors that would predict desistance from continued sexual offending, some authors have focused their attention on protective factors regarding the onset of sexual aggression. For example, Tharp et al. (2013) recently conducted a qualitative review of risk and protective factors for sexual aggression, and their analysis was limited to sexual aggression directed toward adolescents and adults (i.e., they excluded any analysis of child sexual abuse). The authors pointed out that very few protective factors could be identified given the lack of focused research; however, they suggested that potential protective factors for the onset of sexual violence may include empathy for others, a feeling that others care, and having grown up with parents who resolve conflict using reasoning. Although it is important to keep in mind that factors implicated in the onset of a behavior may not necessarily be the same factors linked to the continuance of the same behavior, it is interesting to note the conceptual overlap between some of Tharp et al.’s purported protective factors and aspects of the BERS Affective Strength scale.
It is not clear from the current data why there was no incremental validity when the BERS Affective Strength scale was included together with the ERASOR. It is possible that aspects of the Affective Strength scale are simply the obverse of risk elements already captured by the ERASOR. For example, whereas the BERS Affective Strength scale is designed to tap characteristics necessary for the formation of emotional intimacy, the ERASOR Lack of intimate peer relationships/Social isolation factor reflects a lack of close social connections. Although there are many reasons why an adolescent may lack intimate social relationships at the time of assessment, such as lack of opportunity, a recent change in residence, or depressed mood, for example, it is also possible that a lack of intimate connections with peers is the result of a diminished capacity to form intimate relationships. Perhaps an overlap such as this accounts for the lack of unique variance accounted for by the BERS Affecting Strength scale. It is also possible, of course, that the sample size in the present investigation simply did not afford the statistical power to detect the unique contribution of the BERS scales to risk prediction.
Our finding that the BERS School Functioning score significantly predicted desistance from continued nonsexual reoffending contrasts with that of Spice et al. (2012) who found that the SAVRY-protective factor Strong commitment to school was not statistically significantly correlated with any recidivism outcome (whether nonviolent, violent, or sexual in nature). Whether a methodological artifact or not, our finding is of interest in light of the link between various indices of school commitment, engagement, and functioning and criminal behavior more generally (e.g., Farrington & Ttofi, 2011) as well as criminal recidivism (e.g., Schmidt et al., 2011). In a large-scale, prospective study of a national sample of adolescents, Resnick, Ireland, and Borowsky (2004) found that positive scores on measures of school involvement measured at time 1 at the individual, family, and community levels all appeared to be protective factors in terms of self-reported violence at Time 2. Preliminary multi-site research from the Centers for Disease Control and Prevention (Hall, Simon, Lee, & Mercy, 2012) suggests that factors such as academic achievement and attachment to school (along with other factors including prosocial peer relationships and positive family management) may operate to reduce the onset of youth violence and criminality. These authors stressed, however, that firm conclusions regarding protective factors cannot be drawn given the current state of the limited research in the field. This caution applies equally to desistance research, given the relative dearth of empirical evidence on predictors of adolescents’ desistence from crime, especially adolescents with sexual offences.
This investigation is based on data from one of the only prospective investigations of criminal recidivism with a population of adolescents who have sexually offended. Furthermore, unlike most previous studies in which risk assessment tools were completed by research assistants who coded archival files, the ERASOR was completed by mental health professionals immediately following comprehensive assessments. It should also be pointed out that the BERS was completed by adult caregivers who lived with the adolescents, and multiple sources of recidivism data were obtained. Despite the strengths of this particular study, however, there were a number of limitations that should be highlighted.
The most significant limitation is that the overall sample size is relatively small, as is the absolute number of sexual and nonsexual recidivists. As well, we did not have precise dates of sexual recidivism to determine exact at-risk periods; this precluded the use of Cox regression analysis, which would have enabled us to control for unequal times-at-risk within the sample. It will be important to study additional samples and incorporate survival analyses before the generalizability of the results of the present investigation can be gauged.
Also worth noting, most of the adolescents who were the focus of this study were subsequently involved in specialized treatment focused on reducing their risk to reoffend. Given that treatment significantly reduces the risk of both sexual and nonsexual recidivism for adolescents (Reitzel & Carbonell, 2006), this likely affected the accuracy of predictions of future risk. Another limitation that pertains to most investigations in the field is that we had to rely on official documents regarding sexual and nonsexual reoffending. As we have noted previously (Worling et al., 2012), recidivism data based on criminal charges are dependent on the victim of the crime making a disclosure, the disclosure being reported to authorities, the report being investigated, the police laying a criminal charge, and the charge being entered into a database. It is likely that the actual reoffense rate is higher than that based on official data, and this is particularly true for sexual crimes, as sexual crimes are rarely disclosed to authorities (e.g., MacMillan, Jamieson, & Walsh, 2003).
Although it is clearly necessary to collect additional data from larger samples before we can identify factors that predict desistance from sexual reoffending, and establish how clinicians should integrate information regarding strengths and protective factors with information based on risk factors, the current study provides preliminary evidence to support further efforts in this regard.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.