
Abstract
The Structured Assessment of Protective Factors for violence risk (SAPROF) has recently been developed as a risk assessment tool to focus solely on protective factors for (sexual) violence risk. Research on protective factors for sexual offending is very limited and most risk assessment tools for adult sexual offenders do not incorporate protective factors. The current study investigates the applicability and predictive validity of the SAPROF for forensic psychiatric patients who have sexually offended. For a sample of 83 hands-on sexual offenders, risk assessments were carried out retrospectively with the SAPROF, the Historical Clinical Risk Management–20 (HCR-20) and the Sexual Violence Risk–20 (SVR-20). Results show good interrater reliability and negative correlations between the SAPROF and both risk tools. Predictive validities of the SAPROF protective factors for reconvictions of general and sexual violence were good for short-term (1-3 year) as well as for long-term follow-up (15 year). Moreover, the SAPROF remained a statistically significant predictor of future violence and sexual violence even after controlling for the HCR-20 and the SVR-20. Implications of these findings and recommendations for future research are discussed.
Introduction
The quest for optimal risk assessment for reoffending of sexually violent offenders is an ongoing challenge for forensic mental health care professionals. Although we may be approaching a statistical ceiling in the predictive accuracy of risk assessment tools, the introduction of more dynamic empirically grounded tools brings an innovative approach to risk assessment. At the very least, dynamic tools offer more treatment guidance, likely resulting in greater risk reduction and better violence prevention (Skeem & Monahan, 2011). For sexual offenders treated in inpatient forensic psychiatric hospitals in the Netherlands, routinely repeated assessments with the Sexual Violence Risk-20 (SVR-20; Boer, Hart, Kropp, & Webster, 1997) are mandatory. However, despite good findings on its predictive abilities (see de Vogel, de Ruiter, van Beek, & Maed, 2004), the clinical utility of the SVR-20 is somewhat limited due to the low number of factors in this tool that are able to show improvement during treatment. For adult sexual offenders, dynamic tools such as the STABLE (Fernandez, Harris, Hanson, & Sparks, 2012) have been valuable recent assessment developments, which provide more direction to the treatment and risk management of sexually violent offenders.
Most sexual offender risk assessment tools only focus on risk factors and altogether ignore the potential value that patient strengths and positive environment factors may have for the assessment and treatment of adults who have sexually offended. The inclusion of protective factors could be a promising new contribution to (sexual) violence risk assessment, which might still increase predictive accuracy and could possibly offer additional guidelines to the often difficult and lengthy treatment of violent and sexually violent offenders (de Ruiter & Nicholls, 2011; Ullrich & Coid, 2011). In their reflection on assessing risk of sexual recidivism, Mann, Hanson, and Thornton (2010) concluded that future developments of risk assessment tools should strive to measure risk and protective factors embedded within plausible (and testable) models of offender recidivism risk. Griffin, Beech, Print, Bradshaw, and Quayle (2008) also stated that the inclusion of strengths is important when assessing the risk of future sexually violent behavior. Protective factors could bring more balance to risk assessment and offer positive treatment goals, possibly leading to higher-quality offender treatment and more accurate decision making. As such, protective factors could provide an important contribution to violence prevention.
Although the literature on protective factors for general violent offenders is limited, literature on specific protective factors for sexually violent offenders is even scarcer (de Vogel, de Vries Robbé, de Ruiter, & Bouman, 2011). In their attempt to present a richer way of intervening with sexual offenders, Ward and Laws (2010) brought together the (sex) offending desistance approach and the strengths-based rehabilitation and reintegration framework for sexual offenders the Good Lives Model (Ward, 2002). They argue that in attempting to persuade sexual offenders to give up criminal activities, rather than simply eradicate, control, or manage risk it is advisable to build up offender and environment strengths. Effective positive rehabilitation strategies should not only focus on enhancing positive personal skills, but need to also enforce the aid of practitioners in the desistance process. Through offering a variety of different resources in a holistic approach, health care professionals are advised to attempt to enhance sound therapeutic alliance and create social support, future opportunities, and personal life significance (Ward & Laws, 2010).
Protective Factors in Risk Assessment
As far as we know, there are no sexual violence risk assessment tools available that focus specifically on protective factors for sexual violence risk. However, a tool intended for the assessment of protective factors for general violence risk was recently developed: the Structured Assessment of Protective Factors for violence risk (SAPROF; de Vogel, de Ruiter, Bouman, & de Vries Robbé, 2009, 2012). Most of the protective factors in the SAPROF are potentially changeable and aim to provide opportunities for positive treatment interventions and risk management. Although most of the empirical support for the 17 protective factors in the SAPROF stems from general violent offender studies, the SAPROF was intended to be applicable both to violent and to sexually violent offenders. As most commonly assessed risk factors are valid for general violence as well as sexual violence (see also Hanson & Morton-Bourgon, 2004), it was also expected that most protective factors would be valid for non-sexual violence as well as for sexual violence. Nevertheless, as the SAPROF was not specifically developed for sexual offenders, its factors may neither be fully applicable to sexual offending, nor may this list of protective factors be exhaustive for those who have sexually offended.
Validation research with violent offenders showed good interrater reliability for the SAPROF factors as well as good concurrent validity with the Historical Clinical Risk Management–20 (HCR-20; Webster, Douglas, Eaves, & Hart, 1997) and good predictive validity for no violent reconvictions at different follow-up times after discharge from forensic psychiatric treatment (de Vries Robbé, de Vogel, & de Spa, 2011). Incremental predictive validity was found when the SAPROF was used together with the HCR-20. Prospective clinical evaluation also showed good predictive validity for the absence of violence to others and the absence of self-harm during treatment (Abidin et al., 2013). A first exploration of the usefulness of the SAPROF for sexual offenders was done by Yoon, Spehr, and Briken (2011). They found a significant correlation between the SAPROF and the sexual violence risk assessment tool, the SVR-20. Higher SAPROF ratings were related to lower SVR-20 ratings. However, no significant correlation was found with the Static-99 (Hanson & Thornton, 1999), which according to Yoon and colleagues was likely due to the historical nature of the Static-99 versus the dynamic nature of the SAPROF. The present study investigated the additional value of the SAPROF when combined with the HCR-20 and the SVR-20 for a sample of discharged forensic psychiatric patients with a history of sexually violent offending.
The protective factors in the SAPROF are in line with several of the proposed protective factor domains in an exploration study of protective factors supporting desistance from sexual offending by de Vries Robbé, Mann, Maruna, and Thornton (2014). In that paper, the limited available research specifically on protective factors related to desistance in adult sexual offenders is explored, and eight empirically supported potential domains of protection for sexual offending are proposed. Most of the proposed domains concern general life functioning and are considered valid for violent offenders as well as for sexual offenders. However, the domain Healthy sexual interests specifically addresses issues related to sexual offending and is not covered in the SAPROF. In future studies on protective factors for sexual offending, it would be valuable to include this potentially important domain as an additional factor. If indeed, this domain shows a strong relationship with desistance from sexual violence, it may provide for a valuable additional protective factor to the SAPROF for assessing the risk of sexual offending.
Present Study
The aim of this study was to provide a validation for the SAPROF protective factors for assessing the risk of future general violence and of future sexual violence in sexual offenders. First, the interrater reliability of the tools as well as the concurrent validity between the tools was assessed. Second, the predictive validity of the different tools was examined. To study the ability of the SAPROF, the HCR-20, and the SVR-20 to predict (desistance from) future violence, discharge ratings on each tool were related to violent and sexually violent recidivism at different follow-up times. It was expected that the SAPROF protective factors would be able to significantly predict desistance from future violence, especially for the short-term follow-up. Moreover, it was expected that the SAPROF would add incremental predictive validity to the HCR-20 in predicting future violence and to the SVR-20 in predicting future sexual violence.
Method
Participants
The present study involved 83 male sexual offenders who had been admitted to two different Dutch forensic psychiatric hospitals and were discharged between 1984 and 2006; 65 patients from the Van der Hoeven Kliniek hospital in Utrecht and 18 from the Van Mesdag Kliniek hospital in Groningen, both in the Netherlands. All sexual offenders discharged to the community from either hospital during this time period, for whom sufficient file data were available regarding the final stage of treatment (6-12 months prior to discharge) to be able to retrospectively rate the different dynamic risk and protective factors in the tools, were included in the present sample. Patients from the two hospitals were merged together to afford a larger sample size for studying the predictive validity for recidivism. All participants had previously committed sexually violent offenses for which they had been sentenced to a tbs-order (“terbeschikkingstelling”) by criminal court, randomly assigned to a Dutch tbs-hospital. A tbs-order is a judicial measure that allows for the mandated treatment of violent offenders who are not held fully responsible for their offenses due to severe psychopathology. The order is in effect for as long as deemed necessary by the court, with the aim to rehabilitate patients safely back into society. Although naturally interventions changed over the 20-year course that the different patients in this study were admitted in, treatment at both hospitals typically involved intensive inpatient treatment following a cognitive behavioral and relapse prevention model through an eclectic approach. Among the many aspects of treatment patients generally received psychiatric support, individual psychotherapy, group-based interventions, (psycho)education, social network involvement, work skills development, and engagement in leisure activities. All activities aimed to assist with a safe and successful reintegration into society. Most patients gradually reintegrated into the community, before being discharged.
The average treatment length was about 5.4 years (SD = 2.5, range = 1-16). Median age at release was 30 years (SD = 7.5, range = 18-51). A large proportion of patients suffered from Axis II personality disorders (45%) or traits (29%), particularly cluster B disorders. Only 3% of the patients suffered from a psychotic disorder (e.g., schizophrenia) and 14% of the patients had a diagnosis of a sexual disorder (mostly pedophilia). One in four patients had committed a sexual offense involving at least one child victim; the other patients only had adult victims. Almost half of the sexual offenders in this study had also been convicted for a non-sexual violent offense in the past. At the end of treatment, 56 patients were discharged without any further court conditions, 26 were discharged under court conditions, and 1 had recidivated shortly after discharge and was therefore admitted to another institution. The most commonly imposed court conditions at discharge concerned prolonged supervision by the probation service and court-ordered outpatient treatment, with or without mandatory use of androgen deprivation medication.
Measures
SAPROF
The SAPROF is a relatively new tool specifically developed for the assessment of protective factors for (sexual) violence risk. The SAPROF was designed according to the Structured Professional Judgment (SPJ) approach and intended to be used in addition to risk-focused tools like the HCR-20, its recent revision the Historical, Clinical, Risk Management: Version 3 (HCR-20V3; Douglas, Hart, Webster, & Belfrage, 2013), or the SVR-20. However, the protective factors in the SAPROF could also be assessed in addition to dynamic actuarial risk tools such as the STABLE. The 17 SAPROF items are rated on a three-point scale (0-2), with higher scores indicating the presence of a protective factor for the assessed individual. The SAPROF items are organized in three scales: Internal factors, Motivational factors, and External factors. Items 1 and 2 are static; items 3 through 17 are dynamic and potentially changeable during treatment. Items of particular importance to the individual may be marked as “key,” items considered most relevant for further treatment interventions can be marked as “goal.”
HCR-20
For the assessment of risk factors for general violence (including sexual violence) the HCR-20 was used. The HCR-20 contains 20 risk factors: 10 static (Historical factors) and 10 dynamic items (5 Clinical factors and 5 Risk management factors). Items are scored on a three-point scale (0-2), with higher scores indicating the presence of a risk factor.
SVR-20
To specifically assess the level of sexual violence risk the SVR-20 was also included in this study. The SVR-20 consists of 20 factors in 3 different domains: 11 psychosocial adaptation items, 7 sexual offending items, and 2 items relating to future plans. Only the last four items are dynamic, the other items are static. Items are scored on a three-point scale (0-2), with higher scores reflecting the presence of a sexual violence risk factor.
In addition to rating the 17 SAPROF protective factors and recognizing the most important factors for the individual, an overall Final Protection Judgment is made on the level of available protection for the individual that reduces the risk of (sexually) violent recidivism (low, moderate, or high protection). Next, the results from the SAPROF protective factors assessment are integrated with the results from the HCR-20 risk factors for violence and with the results from the SVR-20 risk factors for sexual violence to come to an integrated Final Violence Risk Judgment for future general violent behavior (including sexual violence) and an integrated Final Sexual Violence Risk Judgment specifically for future sexually violent behavior.
Procedure
The SAPROF, the HCR-20, and the SVR-20 were coded from patients’ hospital files, which generally included case history information, clinical documentation, court evaluations, treatment progress reports, and discharge plans. Because of the dynamic nature of most SAPROF items, it was important to have sufficient information concerning the final phase of treatment (the last year prior to discharge). Dynamic factors were rated based on file information that was available on the last 12 months of treatment. A maximum of four missing items for each tool was allowed. Missing items were prorated for each participant by taking the participant’s average item score on a tool and appointing this to any missing values on that tool. Ratings were performed while all raters were blind to recidivism outcome data as recidivism data were collected after the file codings had finished and none of the raters coded files for patients they were familiar with. For all patients, the Psychopathy Checklist–Revised (PCL-R; Hare, 2003) had previously been coded, either retrospectively or prospectively and results from the PCL-R ratings were used to code the psychopathy items in the HCR-20 and the SVR-20. In the present study, 7 trained psychologists coded the SAPROF, the HCR-20, and the SVR-20 retrospectively for all cases at the end of treatment based on all available file information. To be able to assess the interrater reliability, 30 cases were rated by 2 independent raters randomly divided over the 7 raters in altering pairs. After the individual ratings, a consensus rating was done for these cases. The consensus ratings were used for the predictive validity analyses.
In addition to the final protection and risk judgments, for the purpose of this study, total scores were composed for the 20 HCR-20 general violence risk factors, for the 20 SVR-20 sexual violence risk factors, and for the 17 SAPROF protective factors, as well as for the subscales of each tool. In clinical practice, only the final judgments are composed, based on integrating and interpreting the findings from the different tools used in the assessment. Thus, when carrying out risk assessments with these SPJ tools in clinical practice no adding of scores is used in the process. However, when using the tools in research empirically, it is informative to also analyze the item scores in an actuarial fashion. As this study aimed to investigate the joint predictive abilities of the risk tools and the SAPROF protective factors, in addition to the separate total scores on each tool, two overall total scores of risk and protection were composed reflecting violence risk corrected for available protection: (a) subtracting the SAPROF total score from the HCR-20 total score resulted in the HCR-SAPROF index for general violence risk; and (b) subtracting the SAPROF total score from the SVR-20 total score resulted in the SVR-SAPROF index for sexual violence risk.
Statistical Analyses
The interrater reliability of the SAPROF, the HCR-20, and the SVR-20 was examined by means of reliability analysis using the intraclass correlation coefficient (ICC) with two-way random effect variance model and consistency type, single measure (McGraw & Wong, 1996). The critical values for single measure ICCs are as follows: ICC ≥ .75 = excellent; .60 ≤ ICC < .75 = good; .40 ≤ ICC < .60 = moderate (Fleiss, 1986). To determine the correlations between the SAPROF, the HCR-20, and the SVR-20 Pearson’s correlation analysis was used. Pearson point-biserial correlation analysis was utilized to examine the correlations between the scores on the different tools and violent as well as sexually violent recidivism at different follow-up times. For the final judgments, Spearman’s rho correlation analysis was applied. Partial correlation analysis was done to examine the correlation between the SAPROF and violent outcome while controlling for the HCR-20 and the SVR-20. To assess the predictive validity for violent and sexually violent recidivism of each tool individually and of the combined HCR-SAPROF index and the combined SVR-SAPROF index, Receiver Operating Characteristics (ROC; Mossman, 1994; Rice & Harris, 2005) analyses were conducted resulting in Area Under the Curve (AUC) values. AUC values of .70 and above are considered moderate to large, AUC values of .75 and above are considered large (Douglas, Blanchard, Guy, Reeves, & Weir, 2010). Further analyses were done using the ROCTools statistical software for comparison of ROC curves (Allaire & Cismaru, 2007) that applies the DeLong, Delong, and Clarke-Pearson (1988) method for determining significant differences between AUC values. This method uses chi-square analysis to establish whether two ROC curves differ significantly. In addition, hierarchical logistic regression analyses were carried out to assess the incremental predictive validity of the SAPROF over the risk tools. To control for follow-up time, for the long-term follow-up Cox regression analysis was used instead. Finally, logistic regression analyses were carried out for the final judgments and violent as well as sexually violent recidivism at different follow-up times.
Outcome
For all patients, criminal records were collected from the Judicial Documentation register of the Dutch Ministry of Justice. In the predictive validity analyses (sexually) violent recidivism was used as outcome measure for the HCR-20 and the SVR-20 and non-recidivism in (sexual) violence was used as outcome for the SAPROF. Violent recidivism was defined as any new conviction after discharge for a violent (sexual or non-sexual) offense. Sexually violent recidivism was defined as any new conviction for a sexually violent offense after discharge. Thus, sexually violent recidivism is part of general violent recidivism in this study. All patients in the study had a follow-up time of at least 3 years after discharge. To be able to compare predictive validities at fixed follow-up times, official reconvictions within 1 and 3 years after release were included in the analyses. In addition, analyses were also carried out on the maximum follow-up time available for each patient: On average this long-term follow-up was 15.1 years (SD = 5.3, range = 3-24). None of the participants was incarcerated for more than a year for a non-violent offense during the follow-up. As the exact incarceration time for non-violent offenses was often unclear from the criminal records and overall follow-up time was sufficiently long, no corrections were carried out for time not at risk due to possible temporary imprisonment for non-violent offenses. General violent recidivism rates (including sexual violence) were: 7% for 1-year, 17% for 3-year, and 45% for long-term follow-up. Sexually violent recidivism rates were much lower: 2% for 1-year, 7% for 3-year, and 19% for long-term follow-up. Given the low sexual violence recidivism rate for the 1-year follow-up, predictive validity analysis was not carried out for this outcome for the 1-year follow-up.
Results
Interrater Reliability
The SAPROF showed good interrater reliability for the total score (ICC = .85) as well as for the Final Protection Judgment (ICC = .73). All individual factors had moderate to excellent interrater reliabilities with ICCs ranging from .57 (Self-control) to .91 (External control), all significant (p < .01). Good interrater reliability was also found for the HCR-20 total score (ICC = .86) and the SVR-20 total score (ICC = .85). For the integrated Violence Risk Judgment and the integrated Sexual Violence Risk Judgment, interrater reliability was moderate (ICC = .62 and .55, respectively).
Descriptive Statistics and Convergent Validity Correlations
Table 1 shows the mean total and scale ratings for the HCR-20, the SVR-20, and the SAPROF. Table 2 shows the distribution of final judgments. The SAPROF total score demonstrated a strong negative correlation with the total score on the HCR-20 (r = −.83) and the SVR-20 (r = −.39). The correlation between the total scores on the HCR-20 and the SVR-20 was positive (r = .63). Similarly, the Final Protection Judgment had a strong negative correlation with the Final Violence Risk Judgment and with the Final Sexual Violence Risk Judgment (rs = −.72; and −.67, respectively), whereas both risk judgments were also strongly correlated (rs = .88).
Descriptive Statistics for the SAPROF, HCR-20, and SVR-20 (N = 83).
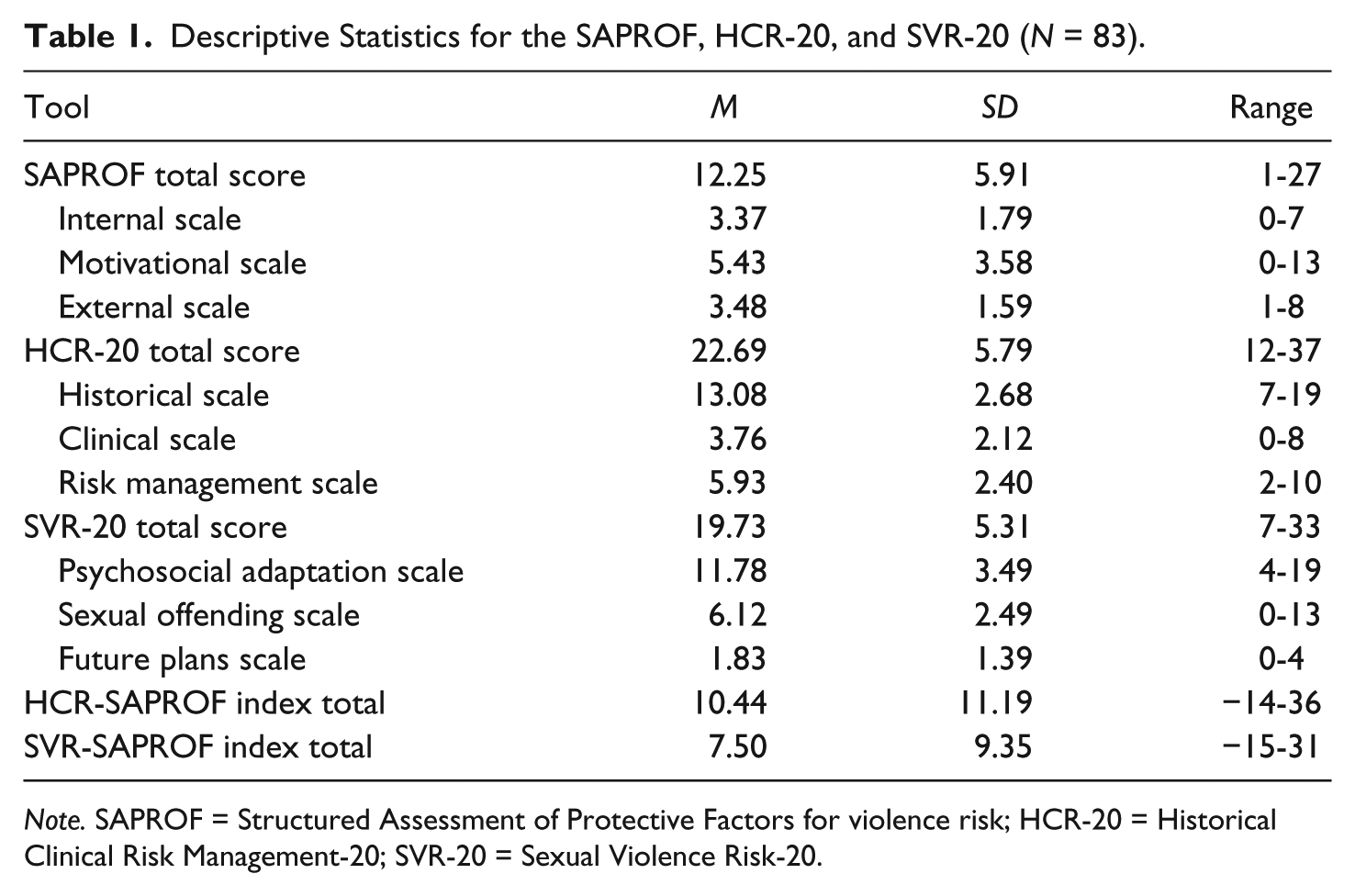
Note. SAPROF = Structured Assessment of Protective Factors for violence risk; HCR-20 = Historical Clinical Risk Management-20; SVR-20 = Sexual Violence Risk-20.
Final Protection Judgment Versus Final Risk Judgment and Final Sexual Risk Judgment (N = 83).
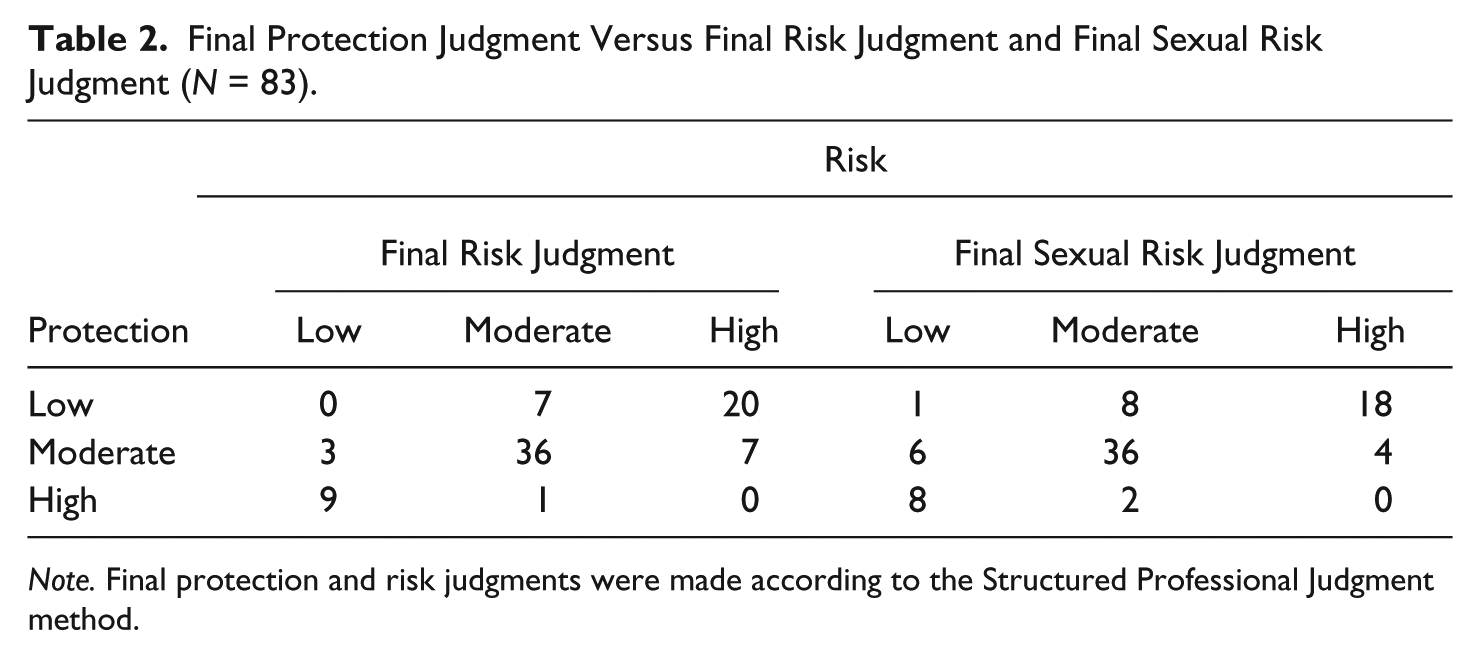
Note. Final protection and risk judgments were made according to the Structured Professional Judgment method.
Predictive Validity
Table 3 shows the correlations between the risk assessment tools and violent as well as sexually violent outcome at the different follow-up times. Correlations between the total scores on the three tools and general violent outcome were significant for all follow-up times, except for the SVR-20 at long-term follow-up. The correlation between sexually violent outcome and SAPROF score was significant at both 3-year and long-term follow-up. However, no significant correlation was found between sexual violence and the total scores on the HCR-20 and the SVR-20. The correlation between violent recidivism and the HCR-SAPROF index, the SVR-SAPROF index and the final judgments, was significant for all follow-up times. The correlation between these measures and sexual violent recidivism was significant only for the long-term follow-up, except for the SVR-SAPROF index which was also significant for the 3-year follow-up. Partial correlation analysis showed that the correlation between the SAPROF and general violent outcome remained significant for long-term follow-up when controlled for the HCR-20 and the SVR-20 (rpb = −.29, p < .01). The correlation between the SAPROF total score and sexually violent outcome was found to remain significant after controlling for the HCR-20 and SVR-20 total scores for 3-year (rpb = −.26, p < .05) as well as long-term (rpb = −.35, p < .01) follow-up.
Correlation Matrix for SAPROF, HCR-20, SVR-20, and (Sexually) Violent Recidivism at Different Follow-Up Times (N = 83).
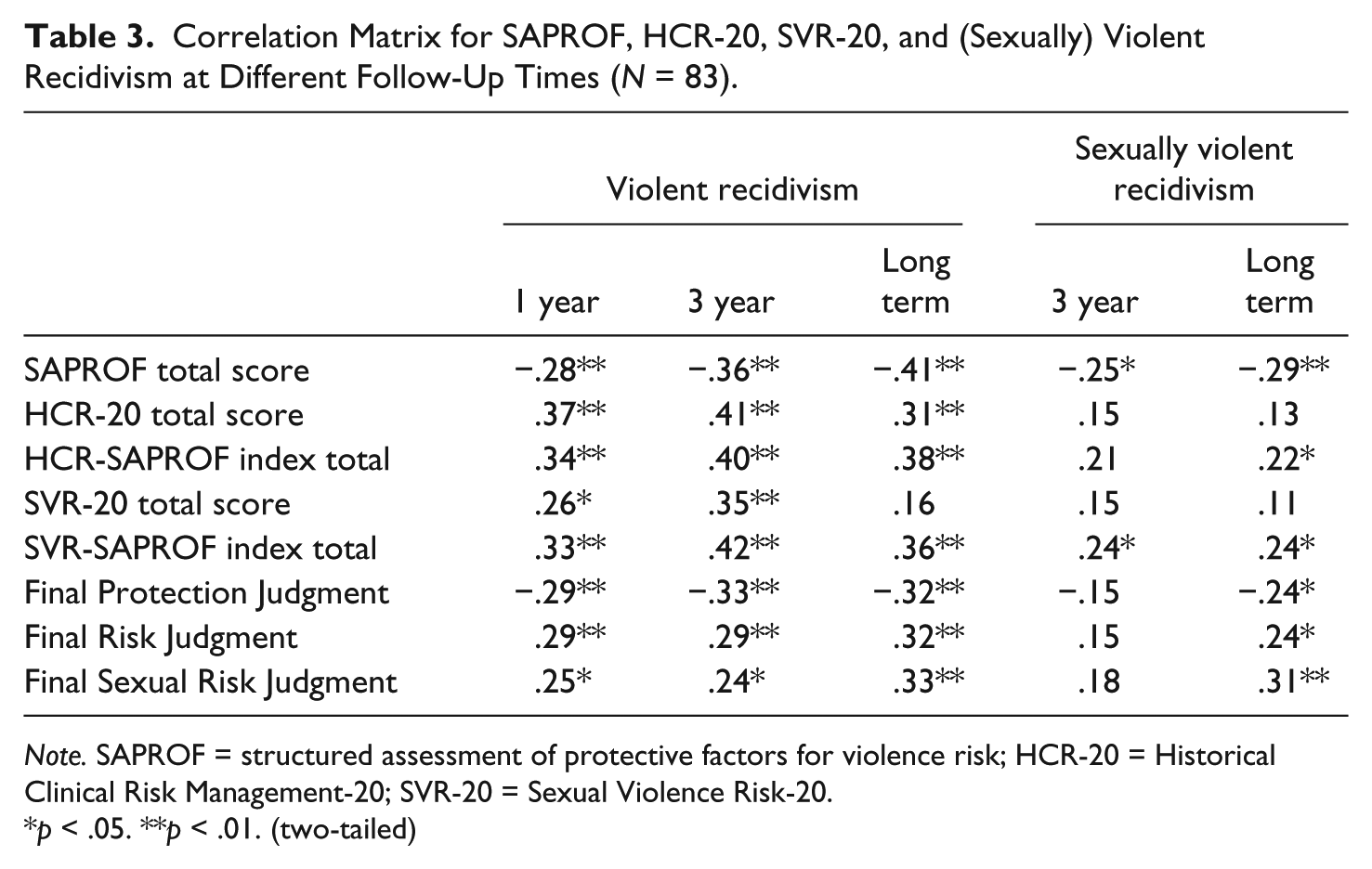
Note. SAPROF = structured assessment of protective factors for violence risk; HCR-20 = Historical Clinical Risk Management-20; SVR-20 = Sexual Violence Risk-20.
p < .05. **p < .01. (two-tailed)
In Table 4, results are shown from the ROC analyses for violent and sexually violent recidivism at the different follow-up periods, for the ratings on the risk assessment tools at discharge. Ratings on the SAPROF are related to non-recidivism in (sexual) violence, those on the HCR-20 and the SVR-20 to violent recidivism. Table 4 shows good predictive validities for the SAPROF protective factors total score for violent reconvictions with short- as well as long-term follow-up after discharge from treatment (AUC = .83 - .74).
AUC Values for SAPROF, HCR-20, and SVR-20 Ratings Upon Discharge for General Violent Recidivism and Sexually Violent Recidivism (N = 83).

Note. The values for the HCR-20/SVR-20 and Final Risk Judgments concern recidivism, the values for the SAPROF and the Final Protection Judgment concern non-recidivism. AUC = area under the curve; SAPROF = Structured Assessment of Protective Factors for violence risk; HCR-20 = Historical Clinical Risk Management-20; SVR-20 = Sexual Violence Risk-20.
p < .05. **p < .01. ***p ≤ .001. (two-tailed)
The HCR-20 also predicted future violence well for the short term; however, at long-term follow-up the SAPROF and the combined HCR-SAPROF index both showed significantly better predictive validity than the HCR-20 total score, χ2(1, N = 83) = 4.24, p < .05, and χ2(1, N = 83) = 6.96, p < .01, respectively. In general, the SVR-20 (not designed for the prediction of general violence) had lower predictive validity for general violence compared with the SAPROF and the HCR-20. At 1-year follow-up the SVR-SAPROF index predicted future violence significantly better than the SVR-20, χ2(1, N = 83) = 4.15, p < .05. The predictive validities of the final judgments were slightly lower than those of the total scores.
Table 4 shows the results from the ROC analyses for sexually violent recidivism at 3-year and long-term follow-up. As sexually violent recidivism rates were very low for the 1-year follow-up, this follow-up period was not included for the sexual recidivism analyses. The ROC analyses for sexual violence risk outcome showed good predictive validity for the SAPROF protective factors total score for reconvictions for sexual violence for 3-year as well as long-term follow-up after discharge from treatment (AUC = .76 - .71). Both the HCR-20 total score and the SVR-20 total score (specifically designed for the prediction of sexual violence) were unable to significantly predict future sexual violence at either follow-up time. However, the HCR-SAPROF index produced a significant prediction of sexual violence at long-term follow-up.
The Final Protection Judgment was slightly less accurate in predicting future sexual violence than the SAPROF total score. However, the integrated Final Sexual Risk Judgment was slightly more accurate in predicting sexual violence compared with the SVR-SAPROF index total score. The integrated Final Risk Judgment predicted sexual violent recidivism equally good as its total score equivalent: the HCR-SAPROF index. Both final risk judgments were able to significantly predict future sexual violence at long-term follow-up, however the Final Sexual Risk Judgment was able to predict sexual violence significantly better than the Violence Risk Judgment, χ2(1, N = 83) = 7.11, p < .01.
To further test the predictive validity of the SAPROF while controlling for both risk tools for violent and sexually violent recidivism, hierarchical logistic regression analyses were carried out on the 1-year and 3-year follow-up times. For the long-term follow-up, Cox regression analysis was carried out to control for the influence of time-at-risk for each participants. In all regression analyses, the HCR-20 and SVR-20 total scores were entered in Step 1 of the analyses and the SAPROF total score was added in Step 2. Similar to the results from the ROC analyses for the violent recidivism outcome, for the long-term follow-up, the violent recidivism prediction model in the Cox regression improved significantly when the SAPROF was added, Δχ2(1, N = 83) = 5.41, p < .05. However, addition of the SAPROF did not show significant improvement to the logistic regression model for the 1-year and 3-year follow-up times. For sexual violent recidivism, adding the SAPROF improved the logistic regression model significantly for the 3-year follow-up, Δχ2(1, N = 83) = 5.90, p < .05, and improved the Cox regression model significantly for the long-term follow-up, Δχ2(1, N = 83) = 10.84, p < .01.
Finally, odds ratios (ORs) were calculated for the final judgments. For violent recidivism, ORs were higher for all three final judgments for the 1-year follow-up (Final Protection Judgment OR = 10.75; Final Violence Risk Judgment OR = 10.37; and Final Sexual Violence Risk Judgment OR = 5.68), then for the 3-year follow-up (OR = 4.74; OR = 3.45; OR = 2.79) and for the long-term follow-up (OR = 3.06; OR = 2.74; OR = 2.95). These values indicate that, for example, when a patient received a rating of “moderate protection” instead of “low protection” (one category difference), his likelihood to become violent within the year after discharge was 10.75 times smaller. ORs for sexual violent recidivism showed an opposite pattern: slightly lower values were observed for the 3-year follow-up (OR = 2.35; OR = 2.38; OR = 3.09) than for the long-term follow-up (OR = 2.70; OR = 2.73; OR = 3.79).
Discussion
Given the limited number of empirical studies on protective factors for sexual offending, this article aimed to provide insight into the potential value of protective factors for the assessment and treatment of sexual offenders and for reducing violent and sexually violent reoffending. The SAPROF is currently the only risk assessment tool that solely focuses on protective factors for violence risk, developed for use with adult violent as well as sexually violent offenders. This study investigated the applicability of the SAPROF protective factors for the risk assessment of patients with a history of sexual offending. The HCR-20 and the SVR-20 were also examined to reflect common risk assessment practice with the SAPROF alongside risk-focused tools. The inclusion of the three tools made comparison possible between protection-focused and risk-focused factors for the assessment of general and sexual violence risk.
The interrater reliability was found to be good for all three tools, although the values were lower for the final judgments. Perhaps making final judgments retrospectively based on patient file information only, was more difficult than rating the items in the tools. Future retrospective file studies should consider more intensive training of raters regarding the making of final judgments. Correlations between the tools showed significant concurrent validity. The protective factors in the SAPROF were negatively correlated to the risk factors in both the HCR-20 and the SVR-20. The overlap between the SAPROF and the SVR-20 was sufficiently small to conclude that these tools may add substantially to one another, which was expected given the predominantly static nature of the SVR-20 and the predominantly dynamic nature of the SAPROF. This result is in line with findings by Yoon and colleagues (2011). The strong negative correlation between the SAPROF and the HCR-20 suggests that there is a bigger overlap between the concepts within the HCR-20 and those in the SAPROF. Although skeptics might interpret this as both tools virtually measuring the reverse of the same constructs and may only view protective factors as clinically relevant, several other findings in this study may provide an argument for the individual empirical value of assessing protective factors. First, both correlation and regression analyses revealed the SAPROF as a significant predictor of violence and sexual violence after controlling for the HCR-20 and the SVR-20, indicating that the SAPROF had an independent relationship with violent recidivism. Second, the predictive validity analyses for sexually violent recidivism revealed significant results for the SAPROF, but not for the HCR-20 and the SVR-20. Finally, significantly better predictive validities were found for the combined HCR-SAPROF index and the combined SVR-SAPROF index than for the HCR-20 and the SVR-20 alone. These findings suggest that the SAPROF contains sufficient independent value to be empirically complementary to the HCR-20 and the SVR-20. That being said, the main value of the SAPROF likely lies in the prospective guidance of positive treatment efforts for violent and sexual offenders, which was not studied in the current retrospective research design.
Predictive Validity
For the short-term (1-year and 3-year) as well as for the long-term (average 15-year) follow-up, the predictive validity of the SAPROF total score was good for general violent reconvictions. This finding is in line with the results found for violent offenders (de Vries Robbé et al., 2011). The HCR-20 predicted violent outcome well for the short term, but was a weaker predictor for violence at long-term follow-up. The SVR-20 showed significant results for the short-term prediction of general violence but not for long-term predictive validity. Overall, final judgments predicted general violence slightly less accurate than the total scores on the tools. Only the SAPROF showed to be able to provide good predictive validity specifically for sexually violent offenses. Neither the HCR-20 nor the SVR-20 total score was able to significantly predict future sexual violence. For the long-term follow-up, the integrated Final Violence Risk Judgment and the integrated Final Sexual Violence Risk Judgment were significant predictors for sexual violence. The latter being the better predictor.
In general, the predictive validity findings for the SAPROF in this study are higher than what is internationally being demonstrated in terms of predictive accuracy of SPJ risk assessment tools. A meta-analysis of SPJ tool performance by Guy (2008) including 113 disseminations reported an average AUC of .74 for violent and .59 for sexually violent behavior. Long-term predictive values were found to be lower than short-term ones in the present study. This was not surprising as, in general, it is harder to predict events further away in time than in the near future, especially given the fact that all tools in the present study also incorporate potentially dynamic factors which may be sensitive to external influences and life events. The lower long-term follow-up predictive validity in the current study of the HCR-20 compared with the SAPROF was somewhat surprising given the fact that half the HCR-20 is comprised of historical static factors. Static factors could be expected to serve as better predictors for the long term as dynamic risk- and protective factors might be more susceptible to change for the worse after treatment. However, the current findings suggest that the predictive value of dynamic factors may be more enduring than previously assumed. It may be the case that positive evaluations of the dynamic “markers” (the dynamic risk- and protective factors) also indicate well-developed underlying psychopathological traits (e.g., enduring good self-control, coping, and social integration may in fact have changed someone’s general anxiety and/or hostility). More treatment-focused research is needed to be able to draw conclusions regarding the effects of different treatment efforts on dynamic risk and protective factors, psychopathology, and ultimately violence risk.
The weak performance of the SVR-20 in this study for general violence was not surprising as the tool was developed for the prediction of sexual violence. In their meta-analysis on risk assessment tools for sexual offenders, Hanson and Morton-Bourgon (2009) also found that tools designed for sexual violence are less suitable for the prediction of general violence in sexual offenders compared with tools designed for general violence. However, the finding that the SVR-20 did not significantly predict sexual recidivism was unexpected given the good results that had previously been found with the SVR-20 in a similar sample of Dutch sexual offenders (de Vogel et al., 2004). The different findings may be due to the fact that the sample used by de Vogel and colleagues had been discharged between 1974 and 1996 and had much higher recidivism base-rates.
Interestingly, combining the SAPROF protective factors with the HCR-20 in the HCR-SAPROF index and combining the SAPROF with the SVR-20 in the SVR-SAPROF index produced significantly better results for general violent recidivism compared with predictions by both risk tools alone. For sexually violent recidivism, the HCR-SAPROF index and the SVR-SAPROF index also produced better predictions than the HCR-20 and the SVR-20 on their own, which was not surprising as the SAPROF was the only significant total score predictor for sexual violence. Finally, regression analyses demonstrated that the SAPROF remained a significant predictor of violence and sexual violence even after controlling for the variance accounted for by the HCR-20 and the SVR-20. These findings provide back-up for the assumption that the predictive accuracy of risk assessment could be increased by adding protective factors to the violence risk equation.
Clinical Use
It is common practice to use item and total tool scores when studying the psychometric properties of SPJ tools. Yet, the empirical evidence resulting from this actuarial approach of the tools may be difficult to translate to the SPJ use in clinical practice. In treatment, the final judgments, composed based on the factors in the different risk assessment tools, are the most relevant outcome for guiding interventions and risk management strategies. The predictive validities for the final judgments that were shown in the present study and the ORs presented aimed to provide some insight into the decreased or increased likelihood of reoffending when patients fall into different protection or risk categories, which may be helpful for the interpretation of the present results in SPJ guided practice.
Despite the apparent overlap with well-established risk factors in some of the protective factor domains and the undisputable value of these risk factors in offender treatment, in our view, the simple “reversed” scores on risk factors are unable to replace the assessment of protective factors on the same domains, as the approach in risk-focused tools is ultimately different. Offender desistance from violence is nourished by a positive approach to treatment and reintegration efforts (see also Ward & Laws, 2010). Focusing on the development of strengths through positive treatment guidelines provides for valuable intervention alternatives to the repression of risk factors. A greater focus on positive treatment goals could enhance offender as well as practitioner motivation, provide meaning to life for the offender and inspire non-criminal future planning, which in turn is likely to positively influence desistance from offending. Furthermore, stimulating the development of personal strengths can provide offenders with more personal resilience against relapse and greater emphasis on external and situational protective factors may be able to enhance risk management strategies.
Although traditional treatment efforts have focused primarily on risk factors, more recently, clinicians have increasingly adopted strength-based approaches. Protective factors need to become embedded in treatment efforts to become manifest over time and have a risk-reducing effect. Ward and Stewart (2003) argued that the therapeutic focus in sexual offender treatment should be on implementing offenders’ good lives plans rather than simply managing risks. By focusing on providing offenders with the necessary conditions (e.g., skills, values, opportunities, and social supports) for meeting their human needs in more adaptive ways, their assumption was that sexual offenders would be less likely to harm others or themselves. In their development of the Good Lives Model—Comprehensive sexual offender treatment approach, Ward and Gannon (2006) conclude that the primary goal is to help offenders to live better lives and thereby reduce their likelihood of committing further crimes. In addition, they comment on the crucial role that context or ecological variables have in the process of rehabilitation and on the importance of the development of offender skills and resources to be able to function successfully in their environment. They state that context and relationship variables play an essential role in effective sexual offender treatment and should be addressed accordingly. To be able to effectively use strengths-based interventions, it is our belief that positive treatment goals should be derived from the periodical assessment of empirically related protective factors.
The promising findings in the present study on the potential value of the SAPROF factors for guiding treatment interventions need to be consolidated. A recent study into the changeability of the dynamic protective factors during the treatment of violent and sexual offenders, showed that most of the factors in the SAPROF are indeed changeable during clinical intervention and that improvements on these factors during treatment are related to reduced recidivism after treatment (de Vries Robbé, de Vogel, Douglas, & Nijman, 2014). A further prospective validation study on the predictive validity of protective factors for inpatient aggression also provided good results for violent and sexual offenders alike (de Vries Robbé, de Vogel, Wever, Douglas, & Nijman, 2014). However, more prospective studies specifically on sexual offenders in different treatment settings are needed. The true potential value of dynamic protective factors for treatment atonement and risk management planning can only be assessed prospectively in clinical and community follow-up studies. Promising dynamic developments in dynamic violence risk assessment practice, such as the HCR-20V3 for general violence risk, and the STABLE for sexual violence risk, should be included in these studies to provide insight into the additional value each of these tools has for sexual offender risk assessment.
Limitations
Although the extensive follow-up time of this study makes long-term predictive validity analysis possible, the downside of this retrospective file study design is that dynamic factors are challenging to code on file information and that it was impossible to seek after missing data. Although patient files were generally extensive and sufficiently informative, information on the presence of the dynamic factors in the final stage of treatment was less detailed than the information would be in prospective studies. However, by carefully scanning the files beforehand and only including cases for which sufficient file information was available on the last year of treatment before discharge, it was attempted to overcome this limitation.
Another limitation from the retrospective design is that treatment changes over time. The fact that on average patients were discharged from treatment 15 years ago, means that the treatment that was received by the patients in this study does not reflect the state-of-the-art best practice sexual offender treatment of today. Not only the content of sexual offender treatment has changed, release decision making has also become stricter, resulting in longer treatment duration, less discharges, and consequently also lower recidivism rates. Given the fact that the time span of the discharges in the current study was about 20 years and participants originated from different hospitals, even within the study sample, some noticeable variability was present in treatment efforts and discharge decisions, which is a limitation to the study. However, in our opinion ensuring a sufficiently large participant sample for the present study outweighed these limitations. Although the sample consisted of patients from two different hospitals, both were high secure treatment facilities and the participants included in the study formed a fairly homogeneous group of offenders with high historical risk profiles.
A further limitation of this study is the low base-rate of registered sexually violent recidivism. Out of the 85 discharged patients, at 1-year follow-up only 2 people had recidivated with a sexual offense. At 3-year follow-up, 6 patients had committed a new sexual offense (7%); at long term, 15 had recidivated sexually (19%). Given the low base-rate of short-term sexually violent recidivism, for this outcome, the predictive validity was not analyzed for the 1-year follow-up. Although the predictive validity for the 3-year follow-up was reported in this study, the fairly low recidivism base-rate for this follow-up (7%) should be taken into account when interpreting the results for this time frame. The same should be said for the 1-year predictive validity for general violent recidivism, which was also present in only 6 cases (7%). It is possible that the low base-rate is influenced by a “dark figure” of unreported or unprosecuted sexual offenses, although the long-term follow-up is likely to compensate for this to some degree. Nevertheless, a low sexual violence reconviction base-rate seems to point to a positive treatment result, which is of course desirable for society and for the offender. At the same time, low base-rates make validation research of risk assessment tools somewhat difficult. It would be expected that, given the professional development in sexual offender treatment over the past decade and the increasingly strict decision making on community discharge, if the same study were to be repeated with currently discharged patients, sexual violence recidivism rates would even be lower and the validation of these tools more difficult. Hart (1998) argued that in fact if we do our job as professionals correctly by letting risk assessment guide decision making in clinical practice, it becomes increasingly challenging to validate tools as high-risk cases simply are not being discharged and thus little differentiation remains in the risk levels of discharged patients. Although ultimately, it seems like we are doing our risk management job well when high-risk cases remain in treatment, the threshold for release decision making remains a difficult issue. Tolerance in society for potentially violent individuals has rapidly decreased, inspiring politicians to instate more repressive and punitive measures rather than solution-focused treatment and rehabilitation promoting initiatives. This also means more stringent decision making on community discharge and as a result, a higher number of offenders that are subject to potentially unnecessary lengthy interventions. Besides the short-term negative and possibly unethical effects this has for the offenders, this development likely also leads to adverse long-term effects on successful offender rehabilitation and as a result high financial burden for society.
Implications
The findings from this study support the potential value of the inclusion of protective factors in sexual offender risk assessment and treatment. The evidence presented demonstrates an increase in risk assessment accuracy when the SAPROF is administered for patients with a history of sexual offending. From a risk assessment point of view, this supports the emerging notion that protective factors should be more incorporated in risk assessment procedures for sexual offenders. From a treatment point of view, this demonstrates the importance of attending to protective factors in clinical practice and the potential value that protective factors have for evaluating the treatment effectiveness of sexual offenders. The findings in this study are in line with those found in previous studies on protective factors for violent offenders. Future multi-phase prospective studies on protective factors will have to confirm their promising clinical value for different patient and offender populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michiel de Vries Robbé and Vivienne de Vogel are both authors of the SAPROF, however they receive no financial benefits from this tool.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.