
Abstract
There is little information about the onset and the developmental course of child sexual behavior problems (SBPs), including sexually intrusive behaviors (SIBs). Using data from the Vancouver Longitudinal Study on the Psychosocial Development of Children, the current study examined the presence of distinct patterns of sexual development among children. A normative sample of preschoolers (N = 354) with a small clinical subsample were followed from age 3 to 8 with repetitive measurements of sexual behaviors using a revised version of Child Sexual Behavior Inventory. Semiparametric group-based modeling identified four distinct sexual development trajectories: the very low (10.5%), the low declining (27.8%), the moderate stable (48.3%), and the high-rate increasing (13.4%). In contrast to the other developmental trajectories found, the high-rate-increasing pattern showed that sexual behaviors became increasingly extensive after school entry. Children characterized by this developmental pattern, especially boys, were more likely to be involved in SIBs after elementary school entry than those in the other groups. Findings highlight the presence of multiple developmental trajectories of sexual development with significantly different behavioral patterns after school entry.
Keywords
In the past 20 years, there has been increased attention to the sexual behavior of children aged 12 years or younger by mental health systems and child welfare agencies (e.g., Elkovitch, Latzman, Hansen, & Flood, 2009). Such attention has been sparked by numerous factors such as (a) the presence of reports showing an association between child sexual abuse and sexualized behaviors (Friedrich et al., 1992; Letourneau, Schoenwald, & Sheidow, 2004; Tarren-Sweeney, 2008), (b) the growing popularity of theoretical and explanatory models of the cycle of abuse (e.g., Burton, Miller, & Shill, 2002; Longo, 1982; Widom & Ames, 1994), (c) the presence of clinical studies reporting that adolescents who perpetrated in a sexual offense are more likely to have been sexually abused and to present an atypical sexual development (e.g., Seto & Lalumière, 2010), and (d) claims that without early detection and early intervention, youth involved in a sexual offense will accumulate a tremendous number of offenses and victims over their life course (e.g., Abel, Osborn, & Twigg, 1993). The alarmist tone of some of the early reports on child sexual behavior and the perpetration of sexual offense has been criticized on the grounds of attempting to pathologize normative child sex play (e.g., Okami, 1992). These early reports, in fact, were clinical studies that virtually required that participants be involved in serious and/or frequent sexual offending, therefore providing a distorted view about all young persons involved in sexual offenses (e.g., see Lussier, 2017). Research, however, has shown that there is much heterogeneity in sexual development across children, and that only a small subgroup of children present evidence of SBPs with manifestations that are outside developmental and societal norms of what is considered to be sex play, curiosity, or exploration (e.g., Araji, 1997; Chaffin, 2008; Gray, Pithers, Busconi, & Houchens, 1999; Letourneau et al., 2004; Pithers, Gray, Busconi, & Houchens, 1998). Despite growing concerns over children showing atypical sexual development, there is surprisingly little research examining the origins and the developmental course of child SBPs over time. Beyond the relative absence of prospective longitudinal studies, there are three key issues and challenges that limit the understanding of the development of SBPs in children.
A Developmental Perspective on SBP: Issues and Challenges
The first issue concerns the understanding of what is meant by SBP, as the definition and the operationalization tend to vary from one study to another. The Association for the Treatment of Sexual Abusers (ATSA) task force proposed to define the children with SBPs as children 12 or younger “who initiate behaviors involving sexual body parts (i.e., genitals, anus, buttocks, or breasts) that are developmentally inappropriate or potentially harmful to themselves or others” (Chaffin et al., 2008; p. 200). The task force refers to developmentally inappropriate behaviors as low-frequency behaviors given the child’s developmental stage and culture, the extent to which sex and sexual behaviors have become a preoccupation for this child, and the persistence of these behaviors despite adult intervention. Furthermore, potentially harmful behaviors are described by the task force to refer to those involving the following: age/developmental differences for the children involved; the use of coercion, force, or intimidation; sexual behaviors causing emotional distress and/or physical injury, and; sexual behaviors that interfere with the child’s social development. Of importance, although SBPs refer to behaviors that have a sexual connotation, the intentions and motivations for these behaviors may or may not be related to sexual pleasure, gratification, or stimulation (e.g., Chaffin et al., 2008). Childhood SBP is not a psychological syndrome or a diagnosable disorder but a continuum of behaviors that fall outside societal norms (Elkovitch et al., 2009).
This definition highlights the issues and challenges in measuring the development of SBPs starting with the operationalization of SBP. Indeed, the ATSA task force’s definition of SBP encompasses a broad continuum of behaviors that are considered concerning due to their nature, their age-inappropriate quality, their frequency, and their persistence over time. Still, there is a lack of consensus as to which SBP manifestations are at each developmental stage and whether those stages are universal (e.g., Friedrich, Grambsch, Broughton, Kuiper, & Beilke, 1991; Heiman, Leiblum, Esquilin, & Pallitto, 1998). While there is a certain consensus about some low-frequency behaviors as reflective of SBPs (Bonner, Walker, & Berliner, 2001; Burton, Nesmith, & Badten, 1997; Carpentier, Silovsky, & Chaffin, 2006; Davies, Glaser, & Kossoff, 2000; Friedrich et al., 1991; Lindblad, Gustafsson, Larsson, & Lundin, 1995), other behaviors and manifestations have not been clearly addressed by researchers, such as behaviors that may cause harm, also referred to as SIBs (Baker et al., 2008; Friedrich, Davies, Feher, & Wright, 2003). In that regard, a significant challenge found in prior research has been the relative absence of an instrument measuring SBPs. Researchers have used instruments such as the widely used Child Behavior Checklist (CBCL; Achenbach & Edelbrock, 1983), but it includes a limited number of sexual behaviors manifested by children (e.g., Meyer-Bahlburg, Dolezal, & Sandberg, 2000). Another instrument, the Child Sexual Behavior Inventory (CSBI; Friedrich et al., 1991), was proposed to address this limitation by including a broader range of normative and nonnormative sexual behaviors, but this inventory was designed to determine whether a child had been sexually abused and not to describe the development of sexual behavior throughout childhood.
A second issue is that there is limited research on the development of normative and nonnormative sexual behaviors during the period prior to puberty (e.g., Burton et al., 1997). Evidence of preadolescent sexual behavior has been regarded as a symptom of child sexual abuse (Elkovitch et al., 2009). The normative sexual behavior in preteens caught researchers’ attention while investigating and comparing the behavior of sexually abused children with that of community samples of children with no evidence of prior abuse (Friedrich, Fisher, Broughton, Houston, & Shafran, 1998). This research has shown that preadolescent children are not asexual, as previously believed, and that sexual behavior may be observed in nonsexually victimized samples of children. Large-scale community-based surveys conducted with preadolescent children with no history of child sexual abuse have shown that sexual behaviors among children are common (e.g., Friedrich et al., 1991; Sandfort & Cohen-Kettenis, 2000). For example, in the Sandfort & Cohen-Kettenis, (2000) study of child sexual behaviors occurring mainly between 2 and 6 years old, several behaviors were observed and reported by more than half of the mothers surveyed, such as the child masturbates with hand (50%), plays doctor (60%), touches breasts (77%), and touches their own sexual parts (97%).
Normative sexual behaviors are considered by some to be those behaviors involving sex play and exploration that occurs spontaneously, infrequently, and is both mutual and noncoercive (Chaffin et al., 2008). Furthermore, preteen years are being described as years of frequent sexual exploration and experimentation rather than a period of dormant or “latent” sexuality (e.g., Josephs, 2015; Larsson & Svedin, 2002). Indeed, preschoolers have a very limited knowledge of sexuality, possessing only basic knowledge of genital differences, gender identity, and sexual body part functions (Brilleslijper-Kater & Baartman, 2000). In that regard, research investigating normative and nonnormative sexual behaviors generally relies on one of three sources of information: primary caregiver’s report (e.g., Friedrich et al., 1991), staff working at day care centers (e.g., Lindblad et al., 1995; Sandnabba, Santtila, Wannäs, & Krook, 2003), or staff working within preschool settings (e.g., Davies et al., 2000). Primary caregivers observe and report significantly more sexual behaviors than staff and educators at day care centers, suggesting that young children tend to explore their sexuality at home rather than in settings that are more structured and monitored (Larsson & Svedin, 2002). The findings from these survey studies also suggest that variations in child sexual behavior are not random and are associated with developmental, individual, familial, social, cultural, and contextual factors (e.g., Friedrich, Fisher, Broughton, Houston, & Shafran, 1998; Friedrich et al., 1991; Friedrich & Luecke, 1988; Friedrich, Sandfort, Oostveen, & Cohen-Kettenis, 2000; Gray, Busconi, Houchens, & Pithers, 1997; Josephs, 2015; Schoentjes, Deboutte, & Friedrich, 1999; Wurtele & Kenny, 2011). The link between preschoolers’ normative and nonnormative sexual behavior and later behavioral adjustments and outcomes, however, has not been firmly established due to a lack of prospective longitudinal studies (e.g., see Okami, Olmstead, & Abramson, 1997).
A third issue with the existing scientific literature is that most studies on children with SBPs are based on retrospective data with highly selective, clinical samples. Clinical research has identified a group of preadolescent children showing nonnormative sexual development, whether in terms of extent, nature, or frequency of their sexual behavior (e.g., Wieckowski, Hartsoe, Mayer, & Shortz, 1998). In a small sample of children with SBPs, the most common forms of SIBs were touching other children’s private parts, trying to undress children against their will, trying to have intercourse with another child or adult, and putting their mouth on another’s sex part (Silovsky & Niec, 2002). While research has shown on repeated occasions that children characterized by a nonnormative sexual development tend to have a history of child sexual abuse (Friedrich et al., 1992; Letourneau et al., 2004; Tarren-Sweeney, 2008), up to 62% of children with SBPs do not present such a history (e.g., Silovsky & Niec, 2002), suggesting multiple pathways toward SBPs (e.g., Baker et al., 2008; Friedrich et al., 1991; Lussier & Healey, 2010; Lussier, Tzoumakis, Corrado, Reebye, & Healey, 2011; Meyer-Bahlburg et al., 2000; Tarren-Sweeney, 2008). Some authors have argued that the comorbidity in the symptomatology of children presenting sexual problems, especially with respect to additional behavioral and emotional regulation issues, suggests only modest specificity in the clinical profile of this population (Meyer-Bahlburg et al., 2000). As a result, Friedrich et al. (2001) have noted difficulties discriminating the sexual development of psychiatric outpatients from sexually abused children. In line with these observations, there are reports suggesting some heterogeneity within the group of preadolescent children showing SBPs (Pithers et al., 1998), but the identified types showed considerable overlap, suggesting that they are not distinct taxons (Chaffin et al., 2008). Furthermore, it is difficult to draw conclusions about developmental patterns and trajectories because this prior research was based on cross-sectional data.
The few longitudinal studies on child sexual behavior come from studies based on clinical samples examining the impact of treatment programs/modalities. For example, Friedrich et al. (2005) examined stability of sexual behavior over a 12-month period in a small sample of preteens drawn from foster homes and a residential treatment program, and reported large correlations between the two assessment periods, suggesting that SBPs did not attenuate over time. However, clinical studies have shown that children generally respond well to treatment and interventions (e.g., Bonner et al., 2001; Pithers et al., 1998), and few are likely to escalate to adolescent sexual offenses (Carpentier et al., 2006). That said, not all children showing SBPs are detected and assessed by a professional. Furthermore, not all children respond well to treatment (e.g., Pithers et al., 1998). However, ultimately, as often mentioned by researchers (e.g., Silovsky & Niec, 2002), there is limited prospective longitudinal research examining the development as well as patterns of continuity and discontinuity of SBPs and SIBs over time in preteen-ager years in community-based samples.
Aims of This Study
Using a developmental perspective (e.g., Chaffin, Letourneau, & Silovsky, 2000; Elkovitch et al., 2009; Lussier, 2017; Lussier, Leclerc, Cale & Proulx, 2007), the current study aims to explore the development of SBPs, in particular SIBs in childhood. A guiding principle of the developmental psychopathology perspective is that maladaptive behavior must be approached and examined in the context of what is considered to be normative during a specific developmental stage. The need to understand the development of SBPs within a developmental psychopathology perspective has been stressed previously (e.g., Elkovitch et al., 2009). The current study, therefore, aims to fill this gap by exploring the developmental patterns of sexual behavior in a community/clinical sample of preschoolers using prospective longitudinal data. In doing so, the study examines the trajectories of sexual behaviors leading to SBPs, particularly SIBs. In the last two decades or so, key methodological and analytical advances have been made to study child development and maladaptive behaviors, more specifically developmental trajectories of maladaptive behaviors (e.g., Nagin & Tremblay, 2001). Therefore, using semiparametric group-based modeling (SPGM), this study aims to determine the number, nature, and shape of developmental trajectories of sexual behavior during childhood. Given the repeated observation that overt sexual behaviors generally decrease prior to school entry, the study is particularly concerned with SIBs beyond the elementary school entry period.
Method
Sample
The Vancouver Longitudinal Study on the Psychosocial Development of Children is an ongoing prospective study following a sample of preschoolers throughout childhood into adolescence (e.g., Lussier, Corrado, & Tzoumakis, 2012). All children included in the sample (N = 354), boys (n = 193; 54.5%) and girls (n = 161; 45.5%), were initially recruited between 2008 and 2011. Descriptive information about the sample is presented in Table 1. Of importance, the sample was culturally diverse, with Caucasians and Asians representing, respectively, 50.6% and 14.8% of the sample. On average, children were 4.3 (SD = 0.9) years old at Wave I, 5.4 (SD = 1.0) at Wave II, and 6.6 (SD = 1.2) at Wave III. Of note, only four children (prevalence = 1.1%) included in the sample presented evidence of (any) child sexual abuse or sexual assault as assessed through face-to-face and phone interviews conducted with the primary caregiver by the trained research assistants. This prevalence is within the expected range of early childhood sexual victimization in contemporary community-based samples of preschoolers. For example, Finkelhor, Turner, Shattuck, and Hamby (2013) found that the prevalence of any sexual victimization rate, as reported by the caregiver through a phone interview, was 1.1% for 2- to-5-year-olds in a large-scale study, including 4,503 children/youth (aged between 1 month and 17 years). For more information about the sample and children’s exposure to aversive familial experiences, see Cale and Lussier (2017).
Descriptive Information About the Sample.
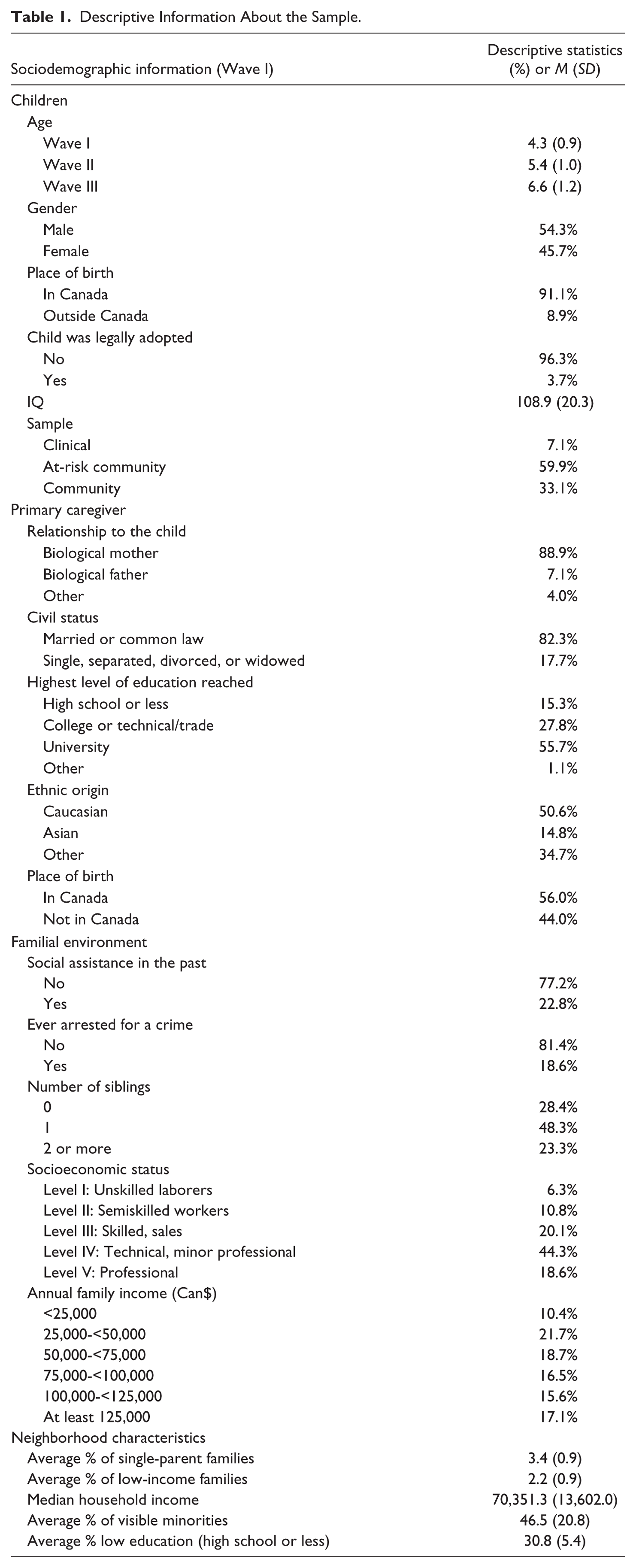
The current study sample comprises three groups derived from a clinical sample of children, an at-risk community sample, and a community sample (see also Lussier et al., 2012). The clinical sample (n = 25; 7.1%) was recruited from an Infant Psychiatric Clinic in British Columbia, Canada. Clinical practitioners informed the primary caregivers about the Vancouver Longitudinal Study. For the majority of this sample (58%), concern over the child’s aggressive behavior was one of the main reasons cited for referral to the clinic for assessment and/or treatment. Based on the clinical assessments conducted at the clinic, this sample of children was mainly characterized by attention deficit hyperactivity disorder (ADHD; 44%) and oppositional defiant disorder (ODD; 16%). The inclusion criteria were as follows: (a) the child was currently being assessed and/or treated for an externalizing disorder, (b) the child was between 3 and 5 years old, (c) both the child and the primary caregiver had a reasonable understanding of English, and (d) the child and the primary caregiver resided in and around the city of Vancouver and other municipalities in the Greater Vancouver Regional District (GVRD).
An at-risk community sample was selected for comparative purposes and was recruited from within more vulnerable socioeconomic neighborhoods in the city of Vancouver and six cities of the GVRD: Burnaby, Coquitlam, New Westminster, Port Coquitlam, Port Moody, and Surrey. In each of these cities, the neighborhoods that ranked in the lowest 25th percentile by two provincial surveys (Kershaw, Irwin, Trafford, & Hertzmann, 2005) were selected for sampling. The neighborhood rankings were identified by a composite score consisting of five components associated with a healthy childhood biopsychosocial development, namely physical health and well-being, social competence, emotional maturity, language and cognitive abilities, and communication skills. Each of the five components is associated with neighborhood socioeconomic status (SES; for example, percentage of low-income families; unemployment rate; Kershaw et al., 2005). It is important to stress that it was the neighborhoods that were sampled, not the families or children. It was therefore expected that, in spite of targeting vulnerable neighborhoods, the at-risk community sample would still include a wide range of families in terms of risk factors and vulnerability. Families recruited as part of this sampling procedure are referred to as the at-risk community sample (n = 212; 59.9%). Starting in February 2009, a comparison group of the children (n = 117; 33.1%) attending day care centers outside the catchment area was also recruited in the city of Vancouver following the same procedure. The day care centers were randomly selected from the remaining list of day care centers in Vancouver. In the present study, they are referred to as the community sample.
Ethics and Procedures
The research design was approved, and the research itself was conducted according to the ethical guidelines required by Simon Fraser University, the University of British Columbia, and the BC Children’s Hospital. Participants were either referred from the Child Infant Psychiatry Clinic at BC Children’s Hospital, or they responded to posters distributed in the community that described the project. Participation in the study was voluntary, and the participants were informed that they could withdraw at any time. The present study is based on the first three waves of data of the Vancouver Longitudinal Study. At Wave I, one in-person interview was conducted with the primary caregiver. Simultaneous interviews with the primary caregiver (i.e., the person most knowledgeable about the child) and the child took place during the Wave I data collection. Typically, the child’s biological mother was (89%) the primary caregiver. The average time for the primary caregiver interview was approximately 2.5 hr. The interview protocol was standardized across research participants, and the data were collected with a computerized questionnaire. The computerized interview involved a trained interviewer asking a series of standardized questions to the primary caregiver who responded directly to the interviewer. The child interview was completed in a separate room adjacent to where the primary caregiver interview was conducted and involved a standardized, developmentally appropriate assessment protocol. Graduate research assistants who had undergone extensive training conducted both the primary caregiver and child interviews. The primary caregivers were paid Can$40 for their participation at Wave I but not on subsequent waves. In addition, all participants signed a consent form indicating that the information they provided was confidential and collected for research purposes only. Two follow-up interviews were conducted, and they will be referred to as Wave II and Wave III. These follow-up interviews consisted of phone interviews with the primary caregiver and were conducted at approximately 1-year intervals from the preceding wave.
Measures and Instruments
The Wave I data were collected using a computerized interview protocol called the Cracow instrument (Corrado, 2002; Lussier, Corrado, Healey, Tzoumakis, Deslauriers-Varin, 2011), which is the main interview protocol of the Vancouver Longitudinal Study. The Cracow instrument collects information on a wide array of risk and protective factors associated with serious and violent juvenile delinquency: pre/perinatal risk; parental attitudes and behaviors; parenting styles; socioeconomic deprivation; individual and behavioral characteristics of the child; social/peer factors; as well as neighborhood factors, victimization, and community violence. A single informant, the primary caregiver, was utilized at this stage of the research to collect information about the child, which is not only optimal but also common for studies based on preschool children. Other studies have suggested that, for this population, using primary caregivers as single informants offers a valid and reliable source because they are familiar with their child’s behavior at home and across settings, especially at this developmental stage (e.g., Kerr, Lunkenheimer, & Olson, 2007). As part of the Wave I interview protocol, all children completed the Reynolds Intellectual Assessment Scale (RIAS; Reynolds & Kamphaus, 2003). The Composite Intelligence Index, which measures verbal and nonverbal intelligence, was also used and reported for this study.
CSBI
A revised version of the CSBI (Friedrich et al., 1991) was used to assess sexual behavior throughout the study period (Waves I, II, and III). The CSBI has been used with clinical samples in welfare settings, as well as with community samples (see Friedrich et al., 2005). The CSBI has also been used in different countries (e.g., Lussier & Healey, 2010; Sandfort & Cohen-Kettenis, 2000; Schoentjes et al., 1999) with different ethnic groups (e.g., Kenny & Wurtele, 2013; Thigpen, 2009). The CSBI has demonstrated good internal consistency (α coefficient = .82) in the original validation studies (Friedrich et al., 1991), as well as in subsequent studies with different samples (e.g., Sandfort & Cohen-Kettenis, 2000; Schoentjes et al., 1999). Higher internal consistency is not expected, given that the scale appears to include lower order factors or dimensions. Multidomain behaviors and factor analytic work have shown the presence of up to seven factors underlying the CSBI items (e.g., Schoentjes et al., 1999): shamelessness, sexual interest, boundary problems, gender-identity problems, sexualized play, sexual intrusiveness, and genital manipulation. The test–retest reliability after 4 weeks has been shown to be good (r = .85; Friedrich et al., 1992).
The CSBI is a clinical inventory used in a clinical setting mainly to determine whether a child has been sexually abused. In the current study, the instrument was not used for this purpose and, as a result, modifications had to be made to fit our study goals and objectives. For the purpose of the study, therefore, a 24-item revised version of the CSBI was used (the appendix) to measure the nature, extent, and frequency of sexual behavior during childhood. The CSBI is an inventory of conceptually related items and not an instrument measuring a psychological construct (e.g., depression, anxiety). Hence, the CSBI includes stand-alone items that can be analyzed separately for research purposes (e.g., trying to undress others against their will) without relying on an overall score produced by the inventory. The removal of items from the original CSBI instrument was justified by the fact that some did not measure a (sexual) behavior (e.g., knows more about sex), some were ambiguous (e.g., makes sexual sounds) or unclear (e.g., stands too close), while some items referred to nonsexual child behaviors (e.g., gets upset when adults kiss). Also, items related to gender-identity issues (e.g., wants to be the opposite sex) were not included in the study, given the limited correspondence with the concepts under study. After removal of these items, the average Cronbach’s alpha found for the 24 items used across age groups was .73 (SD = 0.05; range = 0.67-0.82). Parents reported the frequency of each of those behaviors in the past 12 months using a scale ranging from 0 (never) to 3 (very often). Consequently, the range of possible total scores for this revised scale varies between 0 and 72. A 1-year recall period was selected, given that our goal was to measure the behavior on a yearly basis to examine and describe child sexual behavior throughout childhood and into adolescence. While more frequent assessment periods are preferred to limit memory recall biases (e.g., every 6 months), they can introduce other potential biases (e.g., taxing research participants) while requiring significantly more resources. Data for all three waves were coded by taking into account the child’s age at the time of the interview to allow inspection of developmental trajectories. The sample size for the analysis was as follows: at 3 years old (n = 136); at 4 years old (n = 253); at 5 years old (n = 216); at 6 years old (n = 124); at 7 years old (n = 71), and at 8 years old (n = 45).
SIBs
An important aspect of the study included the measurement of SIBs. The operationalization of SIB stems directly from the work of Friedrich and colleagues (Baker et al., 2008; Friedrich et al., 2005) with the CSBI. In line with past research and factor analyses of the CSBI items, therefore, the current study includes eight CSBI indicators of SIB: touches another child’s sex parts; asks others to engage in sexual acts; attempts to undress others against their will; oral sex with another child; shows sex parts to children; touches an adult sex parts; tries to look at people in the nude/undressing; and tries to have sexual intercourse with another child. Cronbach’s alpha for the SIB scale was .63. To measure the presence/absence of SIB at two developmental stages, two measures of SIB were used in the current study: The first measure refers to the presence of at least one SIB prior to school entry (between age 3 and 5 years) and was simply coded as follows: (0) absent; (1) present. Similarly, the second SIB measure refers to the presence of at least one SIB after school entry (between age 6 and 8 years).
Marlowe–Crowne Social Desirability Scale
Given the focus of the study and its sensitive nature, the Marlowe–Crowne Scale (Crowne & Marlowe, 1964) was used. The short form consists of 20 items, with scores ranging from 0 to 20, measuring the participant’s tendency to respond in a culturally appropriate and acceptable manner (Strahan & Gerbasi, 1972). This scale has been widely researched, and study findings suggest that high scores indicate that participants’ responses may be influenced by a desire to seek approval (Crowne, 1979). This scale was also used given the multiethnic composition of our sample, the prevalence of first-generation immigrants, and prior research showing almost systematic cross-cultural differences in social desirability (Johnson & van de Vijver, 2003). It is noteworthy that, to our knowledge, this scale has never been used in conjunction with the CSBI in prior investigations in spite of the above-mentioned concerns. It was hypothesized that primary caregivers with higher scores on the scale would tend to present the sexual behavior of their child in a more normative and acceptable manner. All primary caregivers completed the scale during the Wave I interview. The mean score on the Social Desirability scale was 11.9 (SD = 3.8). Note that the scores of the Marlowe–Crowne Social Desirability Scale were not significantly associated with study attrition at Waves II (r = −.003, p = .961) and III (r = −.032, p = .562), demonstrating that participation in follow-up interviews was unrelated to social desirability factors.
Neighborhood-level variables
All neighborhood variables were obtained from the 2006 Statistics Canada Census. The 2006 census was selected because it represents the closest approximate time frame to the Wave I interviews that took place in the cohort study. Data were collected from Statistics Canada for each dissemination area. The dissemination areas associated with each neighborhood were subsequently aggregated to form neighborhood-level variables. Overall, data were collected for a total of 342 neighborhoods across Vancouver and the GVRD. Education, unemployment, and median family income were selected due to their association with SES, while the remaining two neighborhood-level variables (i.e., percentage of visible minorities and of single-female parents) were selected for their association with social disorganization. The education variable represents the percentage of individuals within a neighborhood between the ages of 15 and 65 years who had completed high school education or less. The variable unemployment represents the percentage of individuals 15 years of age or older within a neighborhood who were unemployed. The median income was selected, as opposed to the mean because the income distributions within neighborhoods were skewed. The percentage of visible minorities was calculated by dividing the total number of visible ethnic minorities by the total population of that neighborhood. This variable provides a proxy measure of the level of ethnic heterogeneity within a given neighborhood. Finally, a measure representing the percentage of female single parents was calculated by taking the frequency of female single parents with at least one child, dividing by the total population of that neighborhood, and multiplying the product by 100.
Follow-Up and Attrition
The sample size at Wave I included 354 participants. The Wave II interview took place about 1 year (M = 13.4 months; SD = 3.0) after the Wave I interview, and lasted between 30 and 45 min. Several tracking techniques were used to maintain a reasonable retention rate, and participants were contacted through different means (e.g., phone, email). For Wave II, each participant was contacted, on average, 5.6 times (SD = 4.0; range = 1-22). For Wave II, a total of 295 families were reached, and a phone interview was completed, indicating a retention of 83.3%. The Wave III interview was conducted, on average, about 1½ years (M = 20.1 months, SD = 8.2) after the Wave II interview, and lasted between 45 and 60 min as the interview protocol was more substantial than at Wave II. Each participant was contacted, on average, 6.2 times (SD = 3.4; range = 1-25). For Wave III, a total of 204 families were reached, and a phone interview was completed; that is, 69.2% of the Wave II sample and 57.6% of the original sample. In total, when combining data for all three waves with respect to the child sexual behavior data, 55.1% (n = 195) of the original Wave I sample had 3 data points, 29.1% (n = 103) had 2 data points, 15.3% (n = 54) had 1 data point, while 0.6% (n = 2) had no data point. 1 These two participants were excluded from the analyses because there were no data available at any age regarding their sexual behaviors as parents did not want to complete this section of the study. Attrition rates reported in similar studies varied between 29% and 85% (e.g., Bonner et al., 2001; Friedrich et al., 2005).
In the context of longitudinal studies, attrition refers to the loss of participation over time due to several factors, such as subjects declining further participation in the study or not wanting to be contacted again, the research team being unable to contact the participants to inquire about their willingness to participate in the study, subjects being temporarily unable to participate in the subsequent waves due to contextual factors (e.g., hospitalization, incarceration), or the participants having passed away since the last interview. Selective attrition was examined to determine whether child, primary caregiver, or familial characteristics influenced participation in Wave II and Wave III. In other words, several analyses were undertaken to determine whether missing data were missing not at random (MNAR). The covariates included in the study were all measured at Wave I, and the prevalence of missing data was not an issue, given that information was collected for almost all participants, meaning that data were available for at least 95% of the sample on all indicators. Of concern, however, was whether child sexual behavior measured at Wave II and Wave III was MNAR. A series of logit regressions were used to examine selective attrition. For Wave II, not only was the retention rate high, but the analyses conducted also confirmed that there was minimal issues of MNAR. Using child, primary caregiver, familial and neighborhood characteristics, several models (i.e., standard, stepwise, hierarchical) were conducted, and the findings consistently poorly identified the subjects lost to attrition. In fact, the percentage of correct classification of subjects lost due to attrition was below 8 across models. Wave III was more concerning, given that the attrition rate was higher. Regression models consistently showed that two indicators were related to attrition, holding constant all other factors: low annual family income (logged; odds ratio = 0.55, p = .011; 95% confidence interval [CI] = [0.35, 0.87]) and low SES (odds ratio = 0.62, p = .002; 95% CI = [0.46, 0.85]). Therefore, families with lower SES and lower annual family income were more likely to be lost due to attrition at Wave III. Subsequently, this prediction model was used to determine whether these factors were associated with the outcome of interest as measured by scores at the earliest waves where data were available. The statistical model of attrition was then used to predict CSBI scores for each of the age groups (3-8 years). None of the models examined (prediction model’s F values ranging from 0.07-1.56) were statistically significant (i.e., all models showed p values > .25) suggesting statistical independence between factors influencing attrition and the outcome examined.
Analytic Strategy
SPGM
First, the analytical strategy for this article involves the use of SPGM. This statistical technique, developed by Nagin and Land (1993), was used to identify the number and shape of sexual behavior trajectories that best fit the data. SPGM is considered a robust analytical method used to identify longitudinal patterns of development in children, adolescents, and adults, and is routinely used in various fields of research such as developmental psychology and psychopathology as well as criminology (e.g., Blokland, Nagin, & Nieuwbeerta, 2005; Broidy et al., 2003; Nagin & Tremblay, 1999). Frequency of sexual behavior, based on the revised CSBI total score, was measured from age 3 through 8 years. Trajectories were thus measured based on the frequency with which sexual behaviors were committed at each of these ages (i.e., a total of six measurement periods). An accelerated longitudinal design was used, and hence complete data (i.e., measures of sexual behavior at each age between age 3 and 8 years) were not available. 2 SPGM analyses were conducted in SAS 9.4 using the Proc TRAJ add-on developed by Jones, Nagin, and Roeder (2001).
Unlike cluster analysis and other grouping methods that rely on subjective classifications where individuals are sorted into predefined groups, the SPGM method allows developmental trajectories to emerge from the data (Nagin, 2005). In SPGM, the functional form of the trajectories is specified to estimate the distribution of the outcome of interest, in this case sexual behaviors, over age. Quadratic functional form specifies a more parsimonious distribution that captures one major change in the patterning of the outcome and is most appropriate for shorter measurement periods (Bushway, Thornberry, & Krohn, 2003), as was the case in the current study. A zero-inflated Poisson (ZIP) model with a quadratic functional form was used to estimate the distribution of sexual behavior trajectories. In keeping with Nagin’s (2005) recommendations and interpretations, the number of trajectories was first examined using Bayesian Information Criteria (BIC) values. BIC values closer to 0 indicate an improvement in model fit. The Bayes factor is calculated as eBICi − BICj, where values of Bij greater than 10 indicate strong evidence for model “i” according to Jeffrey’s scale (Nagin, 2005). Post hoc analyses can be used to interpret the reliability (i.e., posterior probability) with which individuals were assigned to the trajectory that best matched their pattern of sexual behavior frequency. There are three ways to examine classification accuracy: (a) lack of divergence between the estimated percentage of the sample described by each trajectory and the percentage of individuals assigned to each trajectory using the maximum probability rule, (b) average assignment posterior probabilities, and (c) odds of correct classification (OCC). OCC values, which are more conservative estimates of trajectory assignment compared with average posterior probabilities, were calculated as follows:
In this formula, AvePP g represents the average probability of correct assignment for a given trajectory, and ∏ g is the estimated size of group g (see Skardhamar, 2010). According to both Nagin (2005) and Skardhamar (2010), OCC values of at least 5 indicate excellent classification accuracy.
Cox proportional hazards model
The second key step of the analytical plan was to examine the empirical association between the identified developmental trajectories and the presence of SIB. In other words, the goal was to explore whether there is a developmental pattern more likely to involve the occurrence of SIB prior to and/or after school entry. Logistic regression was not selected, given that such analyses would provide potentially biased parameter estimates, given the presence of censored data. Indeed, logistic regression cannot account for the fact that some families were interviewed once, others twice, and some were interviewed thrice. Therefore, the prevalence rate does not account for varying observation periods across children and the fact that with additional interviews, some parents interviewed once or twice might have reported the occurrence of a SIB. Therefore, a series of Cox proportional hazards regression models (Allison, 2010) were used to account for the presence of censored data. The use of this statistical technique also allowed examining the relationship between the identified developmental trajectories and the presence of SIBs at 2 time points (prior to and after school entry), adjusting for potential confounding factors, such as child, primary caregiver, familial and neighborhood characteristics. For each covariate, the hazard ratio (HR; with 95% CIs) was inspected. Cox regression models were also used to examine the continuity and discontinuity of SIBs across developmental stages using two separate models. The first model examines the homotypic continuity of SIB by determining whether SIB between 3 and 5 years old predicts SIB after school entry (between 6 and 8 years old). The second model aimed to explore whether SIB after school entry is a manifestation of an underlying propensity/inclination toward SIB unfolding and/or a manifestation of a specific developmental trajectory of child sexual behavior unfolding over time.
Results
Model Identification and Interpretation
The first stage of the SPGM analysis involved identifying the number and shape of sexual behavior trajectories that best fit the data. Successive models were run, beginning with a one-group solution and evaluating changes in model fit as per BIC values. BIC values continued to increase through a five-group model which indicates consistent improvement in model fit. A five-trajectory-group model resulted in a BIC value of −2,241.53, which was closer to 0 than both a four-group model (BIC = −2,246.56) and a six-group model (BIC = −2,243.87; Table 2). To further examine the fit of the five-group quadratic model, Jeffrey’s scale of evidence based on the Bayes factor approximation was used to determine whether there were substantive differences in BIC values between models specifying a different number of trajectories. Bij values were greater than 10 when comparing the five-group model with both the four- and six-group models which supported the retention of the five-group model. However, there were also several more compelling reasons to retain a four-group model. Parsimony must also be considered in Bayesian statistics (Collins & Lanza, 2010). Nagin (2005) also suggested that BIC is not always a useful criterion for choosing a model and that parsimony and comprehensibility are preferred, and recommends selecting a model with no more groups than is necessary to communicate the distinct features of the data (also see Piquero, 2008). We therefore abided by Nagin’s principle of parsimony by retaining a four-group solution for the following reasons: First, the incorporation of a fifth trajectory did not appear to substantively add to the model. The addition of a fifth trajectory simply splits a moderate trajectory into two groups: This split resulted in one group with sexual behaviors that slightly declined toward the end of childhood and one group with sexual behaviors that remained stable over the same time period. Second, Table 2 shows that the median probabilities of assignment were highest for the four-group model compared with the five-group and six-group models. Furthermore, in SPGM, only an estimate of the percentage of the sample that each trajectory comprises is given, and divergence from this estimate is evidence of inaccurate classification. For both the four- and five-group models, very little divergence was observed between estimated and actual percentage of the sample comprising each trajectory. Taken together, the four-group model was selected for further analysis (Table 3).
Fit Indices Across Different Trajectory Solutions.
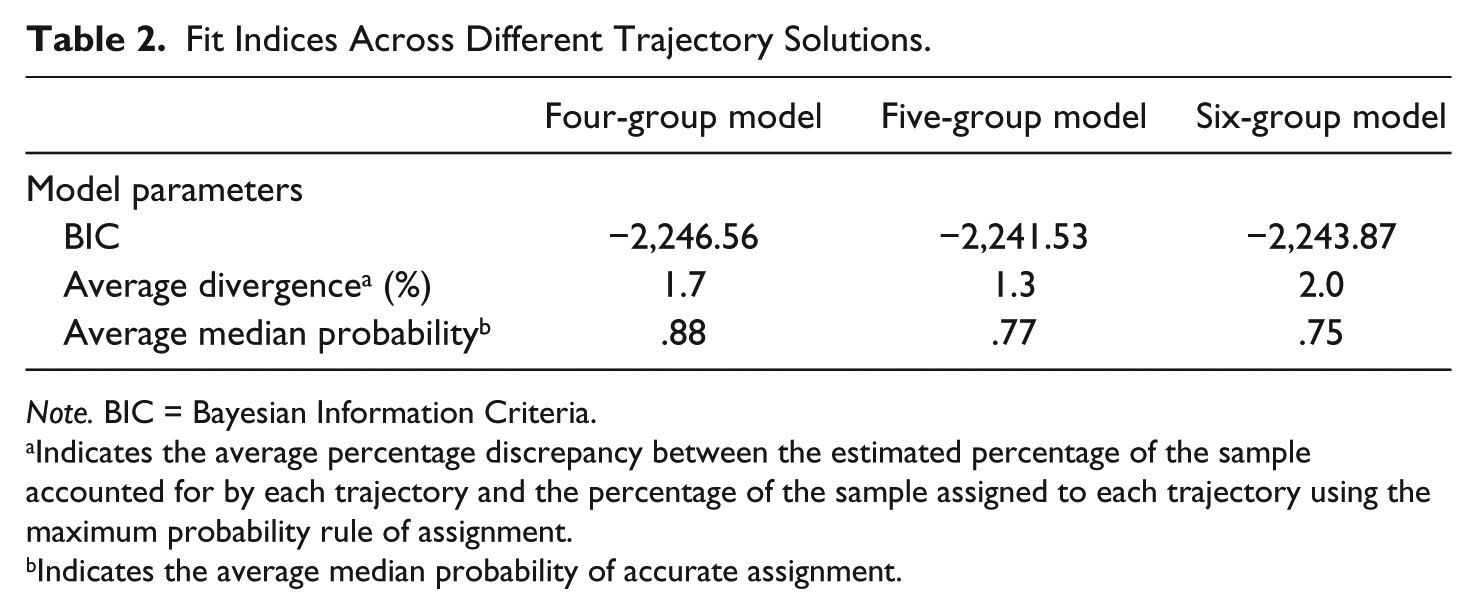
Note. BIC = Bayesian Information Criteria.
Indicates the average percentage discrepancy between the estimated percentage of the sample accounted for by each trajectory and the percentage of the sample assigned to each trajectory using the maximum probability rule of assignment.
Indicates the average median probability of accurate assignment.
Goodness-of-Fit Statistics of Semiparametric Group-Based Modeling.
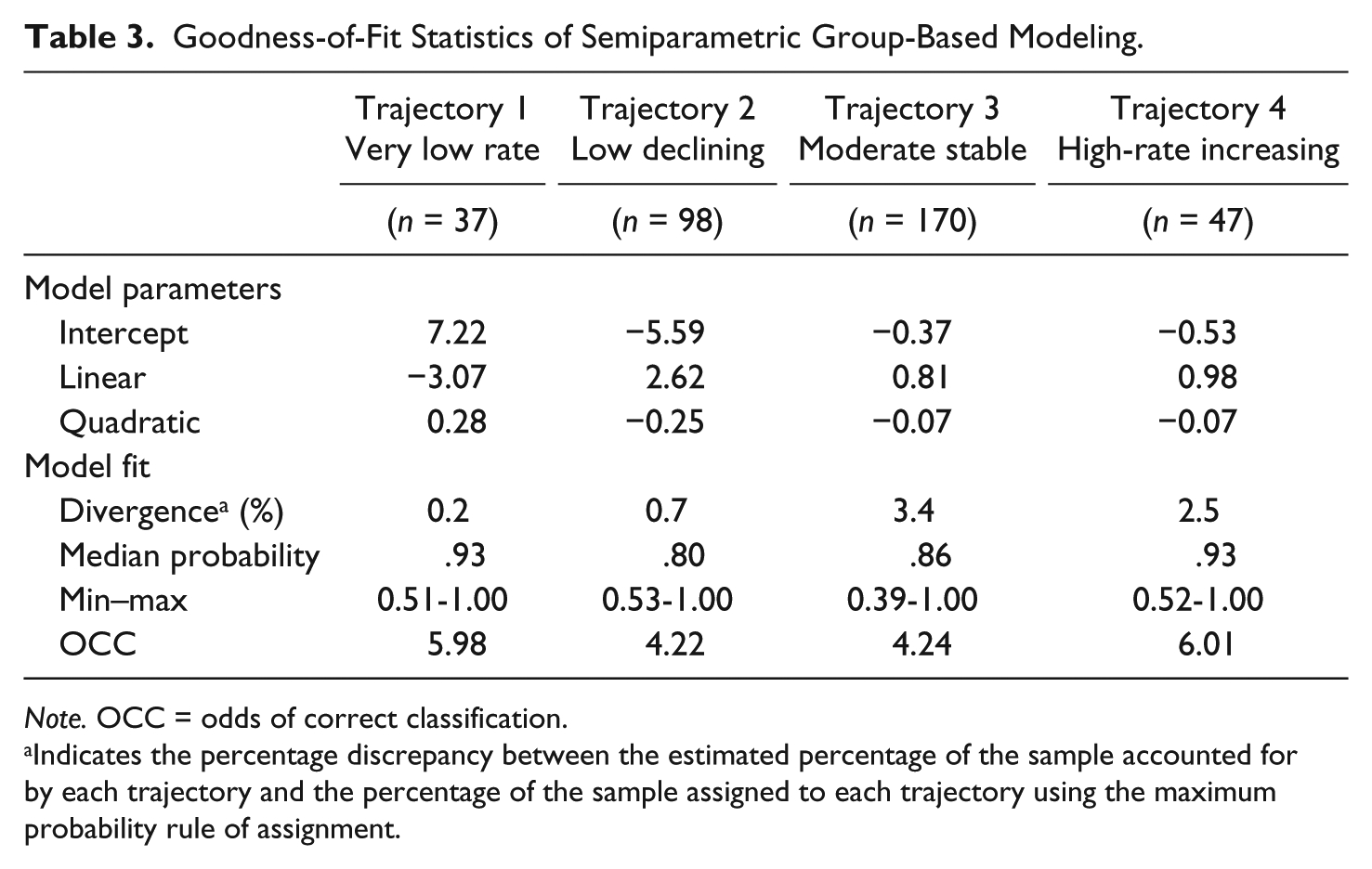
Note. OCC = odds of correct classification.
Indicates the percentage discrepancy between the estimated percentage of the sample accounted for by each trajectory and the percentage of the sample assigned to each trajectory using the maximum probability rule of assignment.
The four-group solution and the four associated trajectories of sexual behavior are shown in Figure 1. Trajectory 1 (10.5% of the sample) depicts a pattern involving the absence of, or at most, a very low level of sexual behavior from age 3 to 8 years. Trajectory 2 (27.8% of the sample) involves a bell-shaped distribution showing a low-declining longitudinal pattern of sexual behavior. Here, sexual behavior peaks at age 5; but by age 8, sexual behavior was very low and similar to that of the very low-rate trajectory. Trajectory 3 (48.3% of the sample) refers to a moderate-stable pattern that involves slightly more sexual behaviors at age 3 compared with the previous two groups. Similar to the low-declining trajectory, the sexual behavior increased thereafter, peaking around the school entry age. By the end of the study period, the sexual behavior of this third trajectory remains more frequent than the very low-rate and the low-declining trajectories.

Developmental trajectories of sexual behavior during childhood.
Finally, Trajectory 4 (13.4% of the sample) described a high-rate-increasing pattern showing the highest level of sexual behaviors compared with the other groups, with a gradually increasing frequency from 3 years of age onward, before somewhat stabilizing after school entry, at around 7 years.
To explore the presence of covariates of sexual behavior development, the four identified developmental trajectories were compared on a series of child, primary caregiver, familial and neighborhood characteristics (Table 4). The goal was not to identify predictors or risk factors, but rather to examine whether a particular developmental pattern was more (or less) prevalent across various subgroups or characteristics of the study sample. The findings showed more similarities than differences across developmental trajectories 3 with only four of the 20 child, primary caregiver, familial and neighborhood indicators examined showing statistically significant differences across groups. Children were statistically different on three interrelated characteristics, namely the primary caregiver’s ethnicity and birthplace as well as the percentage of visible minorities in the neighborhood. Children in the very low-rate trajectory were more likely to have a primary caregiver who is Asian, χ2(6) = 26.5, p < .001; a first-generation immigrant, χ2(3) = 27.9, p < .001; and to live in a neighborhood with a higher percentage of visible minorities, F(3, 339) = 3.9, p < .05. More precisely, children within the very low-rate group (M = 56.5%, SD = 19.7) were significantly more likely (p < .05) to reside in neighborhoods with a higher percentage of visible minorities compared with children within the low-declining (M = 48.0%, SD = 20.7) and moderate-stable groups (M = 44.1%, SD = 21.0). Finally, the analyses also revealed that the four groups were different on the primary caregiver’s scores for Marlowe–Crowne Social Desirability Scale, F(3, 339) = 8.8, p < .001, with caregivers of children in the very low-rate group showing significantly higher scores on the Marlowe–Crowne Social Desirability Scale. There were also additional differences, although not statistically significant (p > .05), where a statistical trend was noticeable for gender (phi = .14), IQ (eta = .14), number of siblings (Cramer’s V = .16), self-report lifetime arrest (phi = .14), and the neighborhood’s household median family income (eta = .14). In that regard, the low-rate trajectory (Trajectory 1) tended to include females, children with lower IQ, without any siblings, who lived in neighborhood with a lower median family income. In contrast, the high-rate-increasing trajectory (Trajectory 4) tended to include more boys as well as children with a parent who had least one prior arrest. Interaction effects between the primary caregiver’s ethnic origin and their scores on the Social Desirability scale were not statistically significant. Taken together, there were some differences across groups, but these differences were relatively modest and limited to one particular group of children.
Descriptive Comparisons Across Sexual Behavior Trajectories.
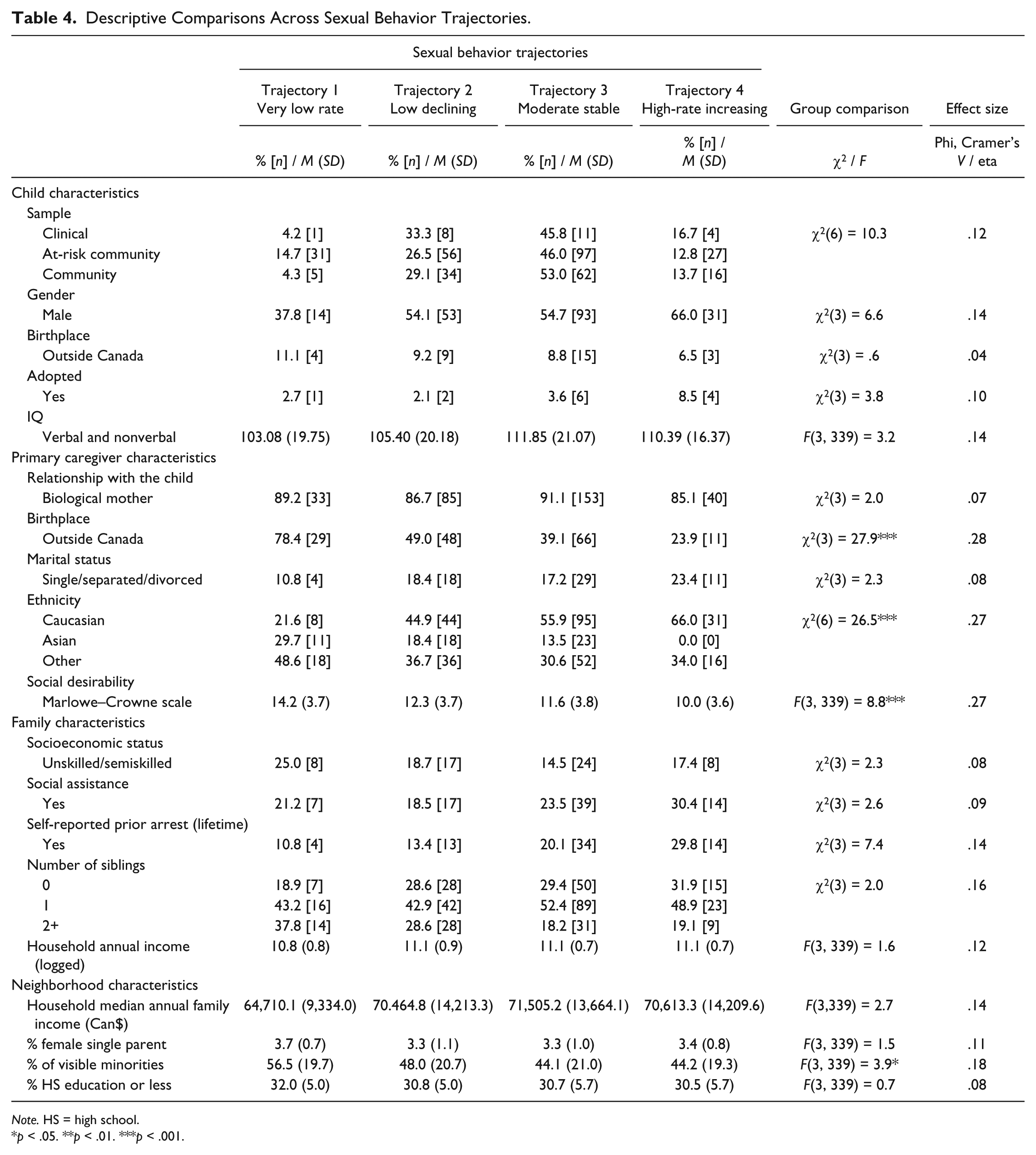
Note. HS = high school.
p < .05. **p < .01. ***p < .001.
During the study period, 93.7% of the sample manifested at least one sexual behavior included in the revised version of the CSBI. While the prevalence was high, children significantly differed in terms of the reported frequency of their sexual behaviors as shown by the SPGM findings. These findings, however, are not informative about the nature of the behavior manifested or the prevalence of SIB behaviors prior to and after school entry. Put differently, while the trajectories inform about the quantitative aspect of the developmental trajectories, they are not informative about the qualitative aspect of the manifested behaviors. To gain further insight, the presence and extent of SIB across trajectories were explored (Table 5). Based on the data collected during the study periods, 61.2% of the sample showed at least one SIB between age 3 and 5, while this prevalence dropped to 44.6% after elementary school entry. Of all the SIB items, instances of the child trying to look at people in the nude/undressing were endorsed most often by primary caregivers both prior to and after elementary school entry. Indeed, the prevalence of this SIB behavior was 51.5% prior to school entry but dropped to 38.3% after school entry. On average, children were involved in one SIB prior to school entry, but the mean dropped to 0.6 after school entry, suggesting that, for the most part, when SIBs were present, they were limited to trying to look at people in the nude/undressing.
Descriptive Information About the Four Developmental Trajectories of Sexual Behavior.
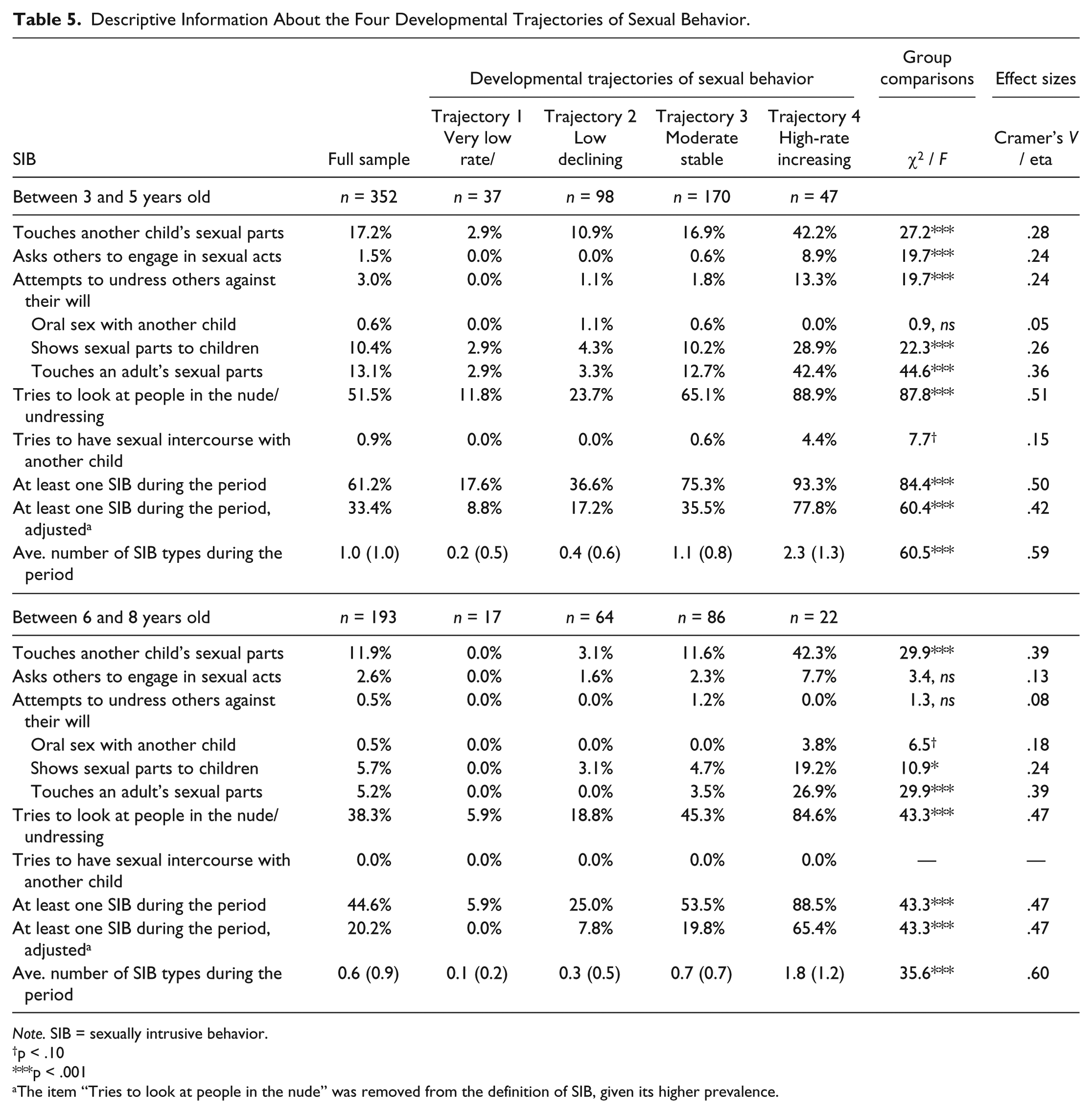
Note. SIB = sexually intrusive behavior.
p < .10
p < .001
The item “Tries to look at people in the nude” was removed from the definition of SIB, given its higher prevalence.
In addition, the inspection of SIB highlighted three key findings: (a) SIBs were rare for the very low-rate (Trajectory 1) and the low-declining (Trajectory 2) trajectories, and both showed a decreasing pattern of SIB as they aged; (b) the high-rate-increasing pattern (Trajectory 4), followed by the moderate-stable pattern (Trajectory 3), was more likely to be involved in SIB in both time periods; (c) the prevalence of SIB remained relatively unchanged after school entry for the high-rate-increasing trajectory (from 93.3%-88.5%), whereas it dropped for the other groups, including the moderate-stable trajectory. The three most common SIBs occurring after school entry that characterized the high-rate-increasing trajectory were as follows: trying to look at people in the nude/undressing (84.6%), touching another child’s sexual parts (42.3%), and touching an adult’s sexual parts (26.9%). Further analyses were conducted to determine whether group differences with respect to the prevalence of SIB were artificially created by a single item (i.e., Tries to look at people in the nude/undressing), given that the behavior is more common. As shown in Table 5, while the removal of this item affects the prevalence of SIB across groups, more than 60% of the children represented by a high-rate-increasing trajectory manifested at least one other SIB during both developmental periods.
Given the low prevalence of SIBs for the very low-rate and the low-declining trajectories, the two trajectories were combined to form the reference group to which the other two trajectories were compared. Findings reiterated the statistical association between developmental trajectory and manifestation of SIB prior to and after school entry. The findings reported in Table 6 show that children represented by a moderate-stable trajectory (Trajectory 3) were 2.3 times more likely than the reference group to get involved in SIB between 3 and 5 years old. This relative risk remained fairly unchanged after school entry (HR = 2.4). For the high-rate-increasing trajectory (Trajectory 4), this group was 3.2 times more likely to show evidence of SIB prior to school entry compared with the reference category, but the relative risk somewhat increased after school entry (HR = 4.1). The association between developmental trajectory and SIB remained relatively unchanged when adding child, primary caregiver, familial and neighborhood characteristics. Of note, prior to school entry, only two covariates emerged as significantly associated with SIB: IQ and annual family income. Children with higher IQ scores (HR = 1.02) and children from families with a higher annual income (HR = 1.3) were significantly more likely to show SIB. After school entry, however, these covariates were no longer predictive of SIB. Instead, boys (HR = 1.7) as opposed to girls and those who were younger at the start of the study (HR = 0.7) as opposed to those from the older cohort were more likely to be involved in SIB. 4
Developmental Trajectories and SIB Adjusted for Child, Caregiver, Familial, and Neighborhood Characteristics (n = 352).
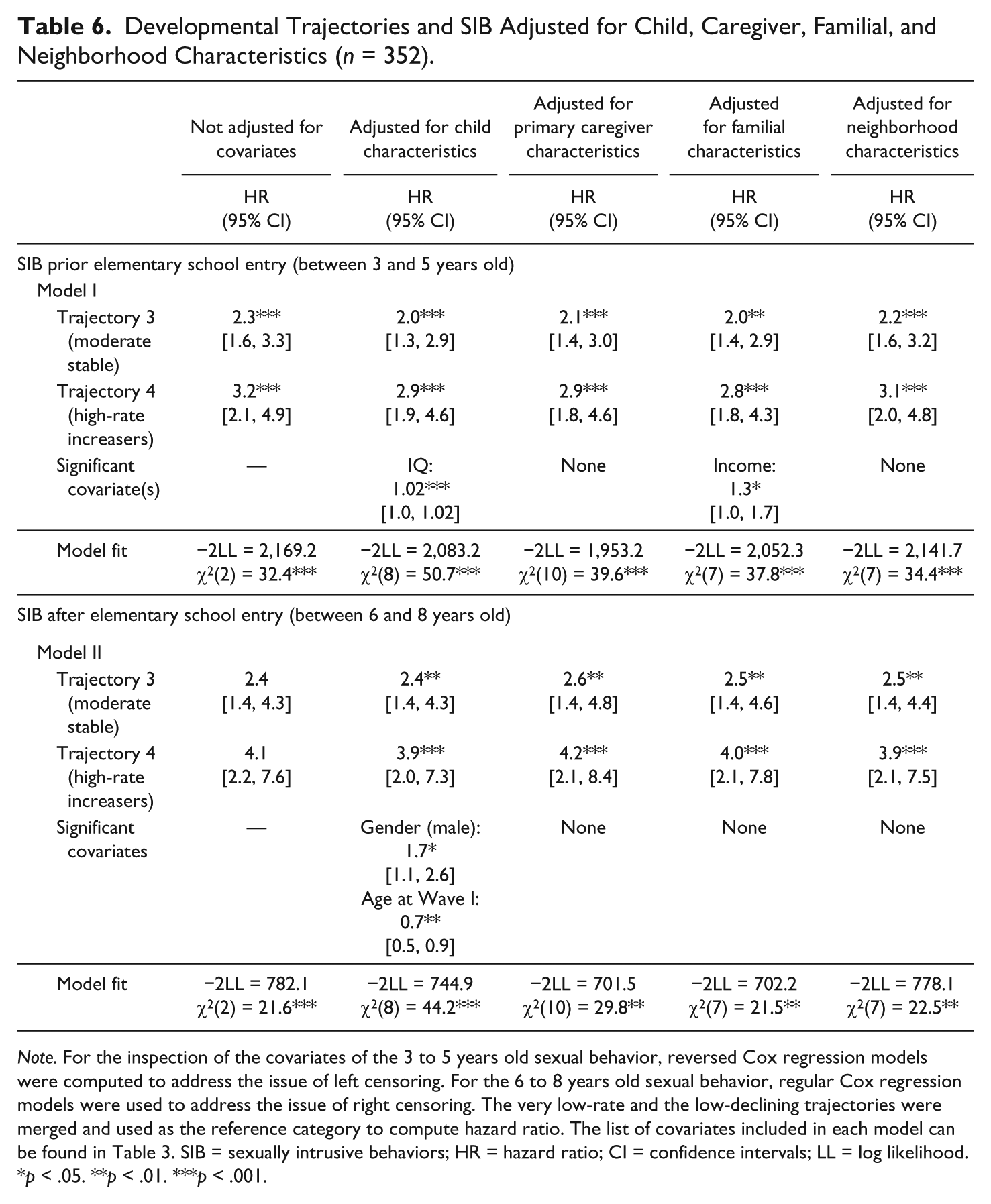
Note. For the inspection of the covariates of the 3 to 5 years old sexual behavior, reversed Cox regression models were computed to address the issue of left censoring. For the 6 to 8 years old sexual behavior, regular Cox regression models were used to address the issue of right censoring. The very low-rate and the low-declining trajectories were merged and used as the reference category to compute hazard ratio. The list of covariates included in each model can be found in Table 3. SIB = sexually intrusive behaviors; HR = hazard ratio; CI = confidence intervals; LL = log likelihood.
p < .05. **p < .01. ***p < .001.
Next, two Cox regression models were conducted to investigate the continuity and discontinuity of SIB across the two developmental periods. The findings are presented in Table 7. In Model I, one covariate, SIB between age 3 and 5, was added to the regression model to predict the presence of SIB between age 6 and 8 years. Not surprisingly, the model showed a significant statistical association between the SIB measures at 2 time points, taking into account the length of the observational period (HR= 1.95, p < .01). In other words, children involved in SIB between age 3 and 5 were about twice as likely to be involved in SIB in the following developmental period compared with those not involved in SIB between 3 and 5 years.
The Covariates of SIB Between 6 and 8 Years Old (n = 352).
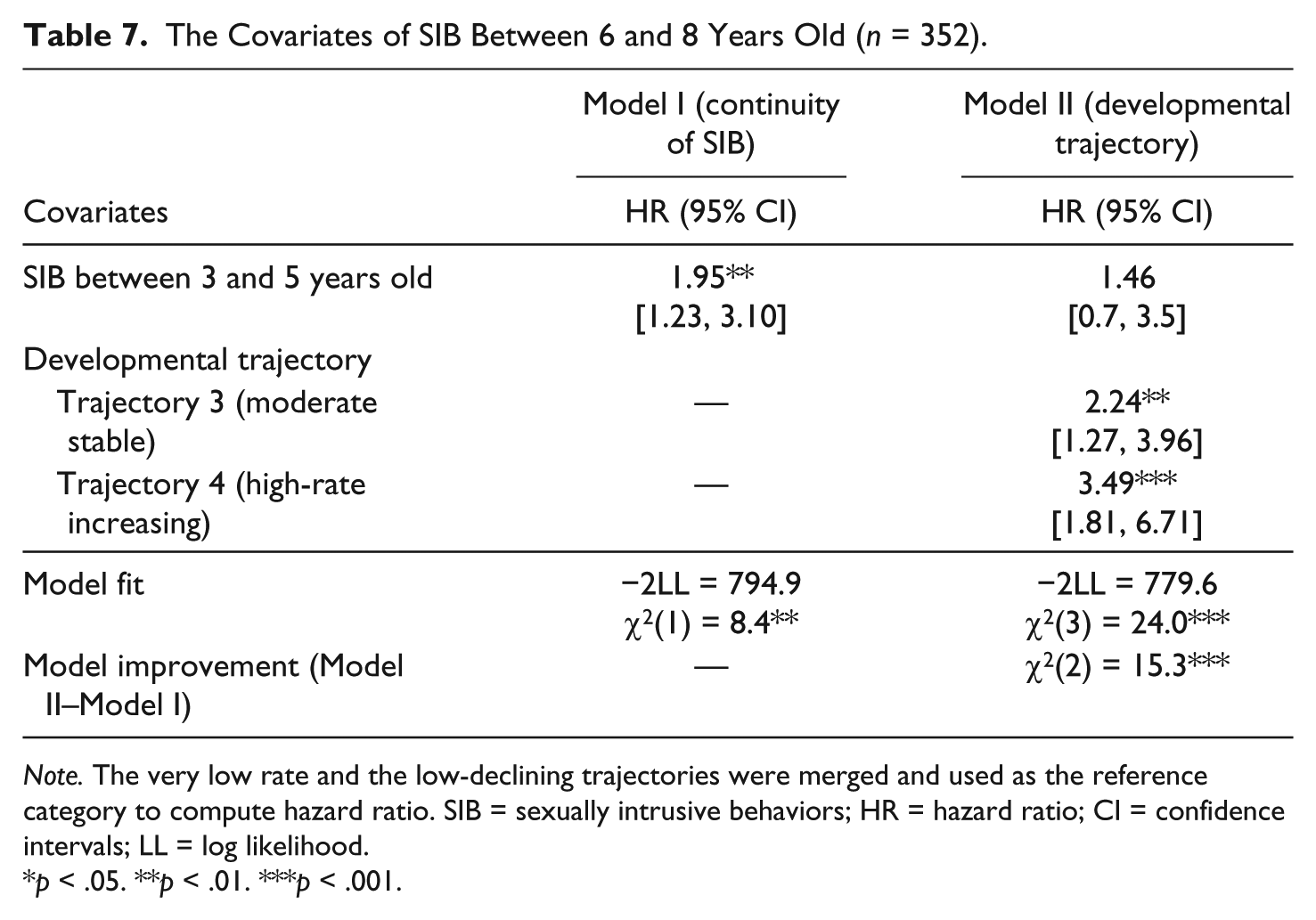
Note. The very low rate and the low-declining trajectories were merged and used as the reference category to compute hazard ratio. SIB = sexually intrusive behaviors; HR = hazard ratio; CI = confidence intervals; LL = log likelihood.
p < .05. **p < .01. ***p < .001.
In Model II, an alternative hypothesis was tested: SIBs after school entry are more reflective of a developmental pattern characterized by the unfolding of involvement in general sexual behaviors (i.e., trajectory) than reflective of an underlying predisposition toward SIB (as reflective of the presence of SIBs prior to school entry). To examine this hypothesis, Model I is tested again but indicators reflecting group membership to the four developmental trajectories found were added to the prediction model. The findings provided stronger support for the developmental trajectory hypothesis. Indeed, on one hand, when adjusting the prediction model by controlling for group membership to developmental trajectory, the indicator of SIB between age 3 and 5 years was no longer predictive of SIB after school entry (HR = 1.46, p > .05). On the other hand, the group of children characterized by a moderate-stable trajectory (Trajectory 3) was 2.2 times more likely to be involved in SIB after school entry compared with the very low-rate/low-declining group (Trajectories 1, 2). The high-rate-increasing group (Trajectory 4) was 3.5 times more likely to be involved in SIB after school entry compared with the reference group. These results held after controlling for two covariates of SIB after school entry: the child’s gender (male; HR = 1.80, p < .01) and age at the start of the study (HR = 0.72, p < .05). Hence, boys who were younger when the study started were more likely to be involved in SIB after school entry, irrespective of their developmental trajectory and the presence of SIB prior to school entry. Note that Marlowe–Crowne scores of social desirability were not predictive of SIB after school entry (p > .90).
Discussion
Framed within a developmental perspective (e.g., Chaffin et al., 2000; Elkovitch et al., 2009; Lussier, 2015), the current study aimed to explore the development of SBP, in particular SIB, during childhood. Longitudinal data were collected and analyzed to determine the number, shape, and prevalence of developmental trajectories of child sexual behavior. As such, the study focused on quantitative between-group similarities and differences as well as within-group stability and changes in sexual behavior of children between 3 and 8 years old. As a general rule, prior research suggests that childhood sexual behavior tends to peak around age 5 (Friedrich et al., 1998, 1991; Schoentjes et al., 1999) followed by a gradual decrease thereafter as children become aware of cultural norms and adjust their behavior accordingly. For some, the decrease is mistaken for a latency period as opposed to child sexual behavior becoming more covert and private as they age (e.g., Bancroft, 2006). Developmental models of normative sexual behavior, therefore, typically describe child sexual development as a single developmental pathway, and departure from this pathway is considered relatively nonnormative (e.g., Bancroft, 2006; DeLamater & Friedrich, 2002; Wurtele & Kenny, 2011). In line with the study findings reported by Thigpen (2009), the current study findings suggest that a single pathway model needs to be revisited, given the presence of significant heterogeneity in the development of childhood sexual behavior.
The inspection of longitudinal data helped identify four distinctive patterns of sexual development that varied in rate, shape, and prevalence. While the four patterns appeared quite similar at age 3, their developmental course subsequently differed. Only the low-declining group, which represented approximately 28% of the sample, mirrored the developmental pathway as typically presented in the scientific literature on child sexual development (i.e., a pathway characterized by a gradual decrease of child sexual behavior as they age). Furthermore, the very low-rate group, about 11% of the sample, presented a profile with very limited manifestations of sexual behavior throughout the study period. Of importance, this trajectory was overrepresented with Asian children. Compared with North Americans with a European background, Asians tend to be more conservative in their sexual attitudes and behaviors and in their willingness to discuss the subject (Futa, Hsu, & Hansen, 2001). It should be expected, therefore, that immigrants, especially those who are closely knit to their cultural background, are more likely to maintain their conservative attitude and behavior. In line with this hypothesis, the current findings showed that the very low-rate trajectory was not only associated with ethnicity but also higher social desirability scores, first-generation immigrant status of the primary caregiver, and a higher percentage of visible minorities in the neighborhood of residence. While prior research has examined cultural and ethnic differences in sexual behavior and reported findings suggesting developmental differences (Josephs, 2015; Kenny & Wurtele, 2013; Thigpen, 2009), we are not aware of clinical studies having investigated the impact of social desirability on reports of child sexual behavior by the primary caregiver. Without additional information, it is difficult to interpret whether the primary caregiver’s responses to the CSBI items reflected actual cultural differences in their child’s tendency to be characterized by a very low-rate trajectory or cultural differences in responding to the CSBI. Indeed, first-generation immigrants may not be familiar with what is considered to be normative and acceptable child sexual behavior in western culture, especially if they reside in predominantly Asian neighborhoods, and might have been somewhat biased toward lower reporting of child sexual behavior. Given that multivariate analyses showed both social desirability scores and ethnicity to be significantly associated with membership in the very low-rate trajectory, actual cultural differences in child development and social desirability factors may both be at play. In fact, similar conclusions have been reached to explain the significantly lower self-reported rate of sexual victimization in China (e.g., Finkelhor, Ji, Mikton, & Dunne, 2013). Clearly, more research is needed to disentangle these processes and clarify the role of ethnicity and culture in child sexual development.
The current study identified two trajectories of concern for the understanding of the developmental course of SBP during childhood. The first pattern, the moderate-stable trajectory, presented some concerning characteristics, particularly their likelihood of engaging in SIBs. In many ways, however, this pattern stood out from the high-rate-increasing trajectory which was distinct in three key ways: (a) as early as age 4, the high-rate-increasing trajectory showed a significantly higher annual frequency of sexual behavior in line with some of the clinical samples of children with SBPs as reported in prior studies (e.g., Baker et al., 2008; Friedrich et al., 1998); (b) they were characterized by a distinctive behavioral course after elementary school entry, their sexual behavior becoming more frequent and extensive to a level consistent with prior clinical studies conducted with children with SBPs (Friedrich et al., 2005); (c) they were significantly more likely to be involved in SIBs throughout the study period, not showing the same level of behavioral inhibitions after school entry compared with the children characterized by the other developmental patterns found. Therefore, the high-rate-increasing trajectory, representing about 13% of the sample, was associated with various behavioral aspects in line with what researchers have previously labeled SBP (e.g., Chaffin et al., 2008). In fact, in Friedrich et al.’s (1992) epidemiological study using a 25-item version of the CSBI, it was reported that a general population sample of 2- to 6-year-olds showed mean CSBI scores of about 3.0 (boys = 2.8; girls = 2.6), while the clinical sample (i.e., children with a confirmed history of sexual abuse) showed mean total CSBI scores of about 11.0 (boys = 11.3; girls = 10.9). In the current study, a 24-item CSBI version was used, and the trajectories found showed some interesting parallels with the Friedrich et al. (1992) study findings. Indeed, the low-declining trajectory showed a total frequency CSBI score in line with Friedrich et al.’s general population sample, whereas the high-rate-increasing trajectory shows scores in line with Friedrich et al.’s clinical sample of sexually abused children. While behavioral differences between the high-rate-increasing and the other trajectories gradually emerged during the preschool years, after elementary school entry such differences were more pronounced and significant. Such differences could suggest that these children (a) were more preoccupied with sexual themes than their counterparts, (b) experienced some difficulties modifying or redirecting their sexual behavior in response to societal norms, (c) were in a familial environment that directly or indirectly favored the expression of child sexual behaviors, and (d) showed some inclination toward potentially harmful sexual behaviors for themselves and others (e.g., touching others’ sexual parts, oral-genital sexual contacts) due to significant attachment issues and difficulties (Burton et al., 1997; Cale & Lussier, 2017; Tarren-Sweeney, 2008; Thigpen, 2009). Furthermore, there was a trend suggesting that boys were more vulnerable to developing a high-rate-increasing trajectory of sexual behavior, but the results were not statistically significant. In all, while these hypotheses are not contradictory, given the lack of theoretical and empirical research, firm conclusions cannot be drawn about them (e.g., see Elkovitch et al., 2009).
Generally speaking, it is suggested that SIBs, whether intrusive, aggressive, or imitative of adult sexual behavior, are low-frequency behaviors during childhood considered to be nonnormative and problematic (e.g., Elkovitch et al., 2009). In light of our findings, a more nuanced approach is necessary, given that more than 61% of the study sample showed at least one episode of SIB between 3 and 5 years old and 45% between 6 and 8 years old. Furthermore, SIBs were not exclusive to one particular developmental trajectory, and it reiterates the importance of contextualizing these manifestations within the child’s developmental stage. SIBs include a wide range of manifestations with some being more prevalent and age normative for preschoolers (e.g., trying to look at people in the nude/undressing); some behaviors are also common but are potentially concerning (e.g., touching another child’s sexual part), while other behaviors (e.g., oral sex/sexual intercourse with another child) are relatively rare throughout the study period (overall prevalence < 3%), but still concerning. Most SIBs included in the study, however, showed base rates that were relatively consistent with prior studies utilizing normative samples (e.g., Friedrich et al., 1998), but the current study is the first, to our knowledge, to examine this using longitudinal data and to show the dynamic aspect of SIB during childhood. Prior research provides little information about the cumulative percentage of children showing SIB during particular developmental periods, and the limited research on the issue suggests that, to some extent, immaturity and curiosity play a part in the manifestation of SIB, given that the prevalence of these behaviors is inversely related to age. For example, Schoentjes et al. (1999) reported that the prevalence of touching other people’s sexual parts was significantly more common among 2- to 5-year-olds than 6- to 9-year-olds. This pattern was also observed in the current study, as the prevalence of SIB after entry into elementary school was 26% lower compared with the earlier measurement period.
Although SIBs were relatively uncommon and their prevalence dropped as children grew older, this general rule did not apply to all children. Indeed, children characterized by a moderate-stable and a high-rate-increasing developmental trajectory were significantly more likely to show SIB prior to as well as after elementary school entry. This suggests that developmental trajectories representing the frequency and extent sexual behavior can inform to some extent about the presence and persistence of SIB during childhood. Other research has shown that school-aged children with SIB tend to be males (Bonner et al., 2001; Pithers et al., 1998), and our findings are consistent with these observations. After school entry, independent of their developmental trajectory, young boys were more likely to manifest SIBs. Specifically, while boys show more overt sexual behavior with age compared with girls (Sandnabba et al., 2003), particularly for aggressive sexual behaviors (Bonner et al., 2001; Friedrich & Luecke, 1988; Pithers et al., 1998), boys and girls tend not to differ in terms of more general sexual behaviors (e.g., Friedrich et al., 1991, 1992, 1997, 2001). The distinction between the expression of overt, aggressive, and intrusive sexual behavior and total sexual behavior is therefore consistent with our findings, and reiterates the importance of a gender-specific approach to understand the development of SBP, in particular, SIB. While the current study did not examine developmental risk factors associated with the development of SBP and SIB, research suggests that aside from the well-documented impact of child sexual abuse and abuse-specific factors (e.g., age of onset, perpetrator–victim relationship, duration of the abuse, seriousness of the abuse, presence of violence) on the child’s sexual development (e.g., Elkovitch et al., 2009; Friedrich et al., 2003; Kendall-Tackett, Williams, & Finkelhor, 1993), other developmental factors may play a role in the emergence and the developmental course of SBP. Past research suggests that children with SBPs present a developmental profile characterized by emotional and behavioral disturbances (e.g., externalization, internalization) resulting from exposure to aversive familial risk factors (e.g., neglect, abuse, violence), which may impede specific developmental tasks associated with their sexual development (e.g., Cale & Lussier, 2017; Friedrich et al., 2003; Silovsky & Niec, 2002). Consequently, intervening with a focus on childhood SBP alone without recognizing the presence of multiple developmental pathways leading to SBP and addressing such important child and familial risk factors potentially involved seems hazardous. Taken together, the study findings reiterate the importance of examining the developmental context in which SBPs emerge, and more specifically, extend the scope of research on SBP by investigating the role and importance of individual, familial, school, social, cultural, and neighborhood risk and protective factors (e.g., Elkovitch et al., 2009; Wurtele & Kenny, 2011).
Study Limitations
There are limitations to the present study: First, the current study oversampled families living in at-risk neighborhoods that are not representative of all families in British Columbia, Canada. This at-risk community sample, however, should not be confused with clinical samples of children (e.g., victims of child sexual abuse, children referred for assessment/treatment because of SBP) typically found in past research (e.g., Baker et al., 2008; Friedrich et al., 1992; Pithers et al., 1998). While our research findings did not provide empirical evidence that children with a particular developmental trajectory of sexual behavior disproportionally reside in at-risk neighborhoods, research should be conducted to further examine children’s exposure to socioeconomic adversities and its impact on the sexual development across childhood and into adolescence. Second, the youngest children were 3 years old when the study started; therefore, there was no available information about child sexual behavior prior to age 3 to inform about the onset of sexual behavior at the earliest developmental stage. Third, similar to the vast majority of studies on this issue, there was only one source of information (i.e., primary caregiver) about child sexual behavior. A more desirable approach would be to have reports from multiple sources and across multiple sites, especially for the purpose of clarifying cultural differences found across children. With that in mind, research has shown that the primary caregiver is the most knowledgeable person about the child’s development at this stage. In that regard, Larsson and Svedin (2002) reported the prevalence of child sexual behaviors by parents as observed at home and by day care workers as observed at day care, and found that parents report significantly more evidence of sexual behavior by preschoolers suggesting that children, for the most part, are more likely to explore their sexuality at home. Our findings are more in line with the findings reported by the parents in the Larsson and Svedin study than those reported by day care workers. Fourth, the study was based on a relatively small sample size that may have limited the identification of small but statistically significant effects (see, for example, Cohen, 1992), as well as unusual and uncommon developmental trajectories. Future studies should examine the presence of developmental trajectories of sexual behaviors using larger samples to confirm or refute the patterns found in the current study. Fifth, the current study did not include an examination of the impact of known risk or protective factors that could explain the presence and the course of the developmental trajectories identified. While several studies have shown that the child individual characteristics and psychopathology as well as experiences of abuse are some of the most important developmental correlates of child sexual behavior (e.g., Cale & Lussier, 2017; Elkovitch et al., 2009; Friedrich et al., 2003), there is little research on developmental risk factors and predictors of the course of sexual development during childhood. Finally, while SPGM is a robust analytical technique to identify trajectories, it is not without limitations (e.g., Skardhamar, 2010). Future research should examine the development of sexual behavior using different and alternative analytical strategies as well, such as latent growth curve and hierarchical linear modeling (HLM).
Conclusion
The current study examined developmental trajectories of sexual behavior in a sample of preschoolers followed up from age 3 to 8. Using SPGM, significant between-group differences across children and within-group stability and change of child sexual behavior were identified. Four developmental trajectories were identified with one developmental pattern, the high-rate-increasing trajectory, presenting some distinctive features more in line with the description of SBP. In fact, children presenting characteristics of a high-rate-increasing trajectory were at risk of presenting SIB behavior after school entry. The study findings highlight that the presence of SIB after elementary school entry is not reflective of the early onset of SIB or of an underlying predisposition for SIB but rather another manifestation of specific and concerning developmental trajectories. It is hypothesized that the most common forms of SIB prior to school entry are age normative, and most children learn to adjust or regulate their behavior as they come in contact with societal norms, whether at home or at school. A small subgroup of children, more specifically young boys characterized by a high-rate-increasing developmental trajectory, may have the most difficulties making such adaptations and transitions showing evidence of SIB after elementary school entry. It is important to keep in mind that, while SIBs are considered concerning when persistent and repetitive (e.g., Elkovitch et al., 2009; Wurtele & Kenny, 2011), its remains hypothetical at this time whether SIBs or some form of SIB are predictive of juvenile sexual offending (e.g., Burton, 2000; Carpentier et al., 2006; Letourneau et al., 2004; Lussier, 2015). The current study did not provide empirical evidence that a particular group of children are more at risk of sexual abusive or aggressive behaviors during adolescence (see also Okami, 1992; Okami et al., 1997). The findings do highlight, however, the heterogeneity of sexual behavior development, and future research will help inform about the developmental course and outcomes of sexual behavior into the teenage years. More research is needed to validate the developmental profile identified in the current study, to extend the analyses to the subsequent developmental stages to clarify what the developmental outcomes are, and relatedly, to explore their associated developmental characteristics. In that context, research should explore the child, familial, school, neighborhood, social, and cultural risk and protective factors across developmental stages of SBP, more specifically, SIB.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.