
Abstract
The present study investigated the relationships between the scales of the Personality Assessment Inventory (PAI) and variables relevant to recidivism risk and criminogenic need to inform clinicians’ use of the PAI for purposes of treatment planning and risk management. PAI profiles, risk measure and domain scores, and recidivism data were collected for 158 males who have been convicted of sexually offending. Data were analyzed to investigate whether select clinical scales of the PAI correlated with conceptually relevant domains of risk and/or recidivism. Our findings demonstrated that the antisocial scales were consistently associated with risk constructs and recidivism, while very few clinical and personality scales showed relationships with risk constructs. The PAI seems to include select scales that represent risk-related needs, but also, other scales that may be more related to responsivity issues, and therefore may have utility to address two of the risk, need, and responsivity principles.
Reducing the prevalence of sexual violence, and its subsequent negative impact on victims, is possible with the appropriate management and treatment of males who have sexually offended. This is the underlying premise of the risk-need-responsivity (RNR) model, which outlines three critical principles for effective rehabilitation of individuals who offend (Andrews & Bonta, 2010; Andrews, Bonta, & Wormith, 2011). Research has demonstrated that adherence to this model is an effective way of reducing the probability of future violence (Bonta & Andrews, 2007) and the likelihood of sexual and nonsexual violent recidivism for males who sexually offend (Hanson, Bourgon, Helmus, & Hodgson, 2009).
At the present time, there is a great deal of attention drawn to identifying and assessing criminogenic needs. Criminogenic needs can be defined as personal or situational characteristics that are associated with offending (Andrews et al., 2011). Eight criminogenic needs have been identified by Andrews et al. (2011), which are predictive of general future offending (e.g., antisocial associates, antisocial cognitions, antisocial personality pattern). Central to the discussion of criminogenic needs is the necessity of measures that can validly assess the needs of each individual. In the past two decades, the field has seen the emergence and validation of several tools for the assessment of sexual violence. These tools have repeatedly demonstrated their utility for the prediction of sexual recidivism (Hanson & Morton-Bourgon, 2009); however, these measures have also been criticized for their inability to assess factors that speak to the cause of the offending behavior (Mann, Hanson, & Thornton, 2010). While the prediction of violence is important, both for the implementation of the risk principle of the RNR model and from a public safety standpoint, the reduction of violence should be the ultimate goal (Wong & Gordon, 2006). According to the RNR model, we have the greatest likelihood of achieving this with the use of treatment programs that are tailored both to an individual’s level of risk and his criminogenic needs (Andrews et al., 2011). As such, it follows that assessment tools that measure criminogenic need and are empirically related to violence risk have high utility for informing the management and treatment of individuals who sexually offend.
There are several psychological assessment tools available to clinicians to aid clinical decision making and treatment planning. For pragmatic reasons, including their cost-effectiveness and ease of administration, norm-referenced, self-report inventories are popular among clinicians. Although they were not designed to predict criminal recidivism, nor to identify criminogenic treatment needs, these inventories are frequently administered in forensic and correctional settings to inform decisions regarding treatment and management for males who offend. Among these tools is the Personality Assessment Inventory (PAI; Morey, 1991, 2007), a measure of clinical characteristics and psychopathology. The efficacy of the PAI in forensic settings has been empirically investigated, and the results have been favorable. For example, Douglas, Hart, and Kropp (2001), in their investigation of the validity of the PAI for forensic assessments, concluded that the tool has utility in measuring key forensic-related domains, including violence, personality disorder, and psychosis. Furthermore, numerous studies have indicated that certain PAI scales, typically those conceptually relevant to violence (e.g., antisocial features, aggression, and dominance), are useful predictors of institutional misconduct (e.g., Hopwood, Baker, & Morey, 2008; Newberry & Shuker, 2012; Reidy, Sorensen, & Davidson, 2015; Walters, Duncan, & Geyer, 2003), violent behavior (e.g., Crawford, Calhoun, Braxton, & Beckham, 2007; Edens, Poythress, & Watkins, 2001), and recidivism (e.g., Salekin, 2008; Salekin, Rogers, Ustad, & Sewell, 1998). These findings also hold up with samples of men who sexually offend, with evidence to show that a number of PAI scales are useful predictors of technical breaches (Boccaccini, Murrie, Hawes, Simpler, & Johnson, 2010) and institutional misconduct (Boccaccini, Ruffino, Jackson, & Murrie, 2013; Buffington-Vollum, Edens, Johnson, & Johnson, 2002; Caperton, Edens, & Johnson, 2004). Recently, the PAI has also shown some promise for predicting violent nonsexual and nonviolent recidivism among men who have been convicted of sex offences (Boccaccini et al., 2010).
A recent meta-analysis (Gardner, Boccaccini, Bitting, & Edens, 2015) concluded the following summary points about the current state of science with respect to the PAI: (a) Scores from the antisocial features and aggression PAI scales are the most robust predictors of all types of misbehavior (e.g., institutional misconduct, violent behavior, and recidivism); (b) PAI scores have stronger predictive effects among incarcerated men (i.e., in correctional settings), compared with men in treatment settings; (c) the PAI is better able to predict institutional misconduct in studies that utilize longer follow-up times (i.e., greater than 1.5 years); and (d) the PAI is better at predicting institutional misconduct than recidivism. With regard to this last point, the authors noted that even though the PAI had weaker predictive power for recidivism in comparison with institutional misconduct, in direct comparisons the tool has performed comparably with other assessment measures that are conceptually related to violence (e.g., Psychopathy Checklist–Revised; Walters & Duncan, 2005) and measures that were developed for the purpose of the predicting violence (e.g., Static-99; Boccaccini et al., 2010). Thus, they concluded that further research looking at the PAI and recidivism is needed. Gardner et al. (2015) also had important conclusions regarding the use of the PAI for managing individuals who offend. Gardner et al. concluded that while only a small number of scales seem to explain most of the variance of misbehavior, other PAI scales still provide important information. For example, when attempting to reduce the likelihood of future violence, two men with seemingly identical risk may respond differently to interventions depending on their psychological profiles (i.e., their differences in scores of treatment rejection, anxiety, suicidal ideation, substance abuse, etc.; see discussion of responsivity issues in Jung & Dowker, 2016).
The literature suggests that the PAI has utility as a treatment and management planning tool for individuals who offend, in general, and it may not be difficult to surmise that its application would also extend to individuals who sexually offend. In addition to the evidence supporting the PAI’s utility and ability to predict violence and misconduct, the PAI may also have the advantage of being comprehensive. That is, it contains numerous scales relevant to a wide range of clinical conditions and treatment attitudes. Recently, the comprehensiveness of an assessment has been identified as an important feature to capture psychologically meaningful factors (i.e., factors associated with the cause of offending) that predict sexual recidivism (Mann et al., 2010). Specifically, it has been argued that these causal factors should be the focus in the assessment and treatment of men who sexually offend.
The Current Study
This study aims to further explore the use of the PAI for purposes of treatment planning and risk management by examining the relationships between the scales of the PAI and the variables that are relevant to the risk and criminogenic need of men who sexually offend. Given that the majority of previous studies have utilized samples of individuals who commit nonsexual offences, used relatively short follow-up times, and measured outcomes of nonsexual violence and institutional misconduct, the aim of this study is to contribute to the body of literature with a sample of men who have been convicted of sexual offences, and uses a longer follow-up period and outcomes that include sexual recidivism. In light of past research, it is predicted that selected PAI scales will be significantly associated with sexual violence risk scores and differentiate among individuals who have sexually reoffended and those who have not.
Method
Participants
Data were obtained from a forensic outpatient agency and an affiliated secure forensic psychiatric hospital where individuals who have been adjudicated for sexual offending are referred for court-ordered assessment and treatment. Adult males who were convicted of sexual offences and evaluated between 2001 and 2009 were identified, and their patient files were archivally coded for relevant variables. Of the total 474 available files, 158 males convicted of sexual offences had completed the PAI and therefore were included in the present study. The average age of this study’s sample was 39.5 years old (SD = 13.71), with an education level of 11.7 years (SD = 2.38). At the time of the index offence, 35.4% (n = 56) were single, 52.5% (n = 83) were married or common-law, and 7.6% (n = 12) were separated or widowed. A small number of individuals had a prior psychiatric hospitalization (9.5%; n = 15). The sexual offending behaviors in their index offence were diverse and included sexual offences against children (47.5%; n = 75), sexual assault against adolescents and/or adults (36.7%; n = 58), indecent exposure (8.2%; n = 13), possession/making/distributing sexual exploitation materials (0.6%; n = 1), and other sexual crimes, such as voyeurism or property offences (7%; n = 11).
Measures
Demographic variables, T-scores for each scale on the PAI, and items from the Static-99R and 2002R were coded from files. Recidivism outcomes were coded from criminal records.
PAI
The PAI is a 344-item self-report personality measure that assesses treatment attitudes and psychopathology (Morey, 2007), and has 22 non-overlapping validity, clinical, treatment attitude, and interpersonal scales. The PAI has been demonstrated empirically to have high construct validity when compared with corresponding life events of psychiatric individuals (Slavin-Mulford et al., 2012). Slavin-Mulford et al. (2012) found support for the construct validity of these scales where psychiatric participants’ real-life events (i.e., medical history, legal history, current functioning) were correlated with scores on most PAI scales (alpha level of p = .05, but corrected for 100 correlations calculated, .05/100 = .0005). The PAI reliability coefficients for the clinical and treatment attitudes scales are high, with alphas ranging from .79 for stress and .94 for anxiety, implying the PAI has high internal consistency (Wise, Streiner, & Walfish, 2010).
For the current study, antisocial and related scales, along with other clinical, treatment, and interpersonal scales were included in the study. Specific antisocial-related scales were antisocial features (ANT), antisocial behaviors (ANT-A), egocentricity (ANT-E), stimulus-seeking (ANT-S), alcohol problems (ALC), drug problems (DRG), aggression (AGG), and dominance (DOM) scales. Specific clinical, treatment, and interpersonal scales that were examined included anxiety (ANX), anxiety-related disorders (ARD), depression (DEP), mania (MAN), paranoia (PAR), schizophrenia (SCZ), borderline (BOR), treatment rejection (RXR), and warmth scales (WRM).
Static-2002R
The Static-2002R contains 14 items grouped into five content areas (age at release, persistence of sexual offending, deviant sexual interests, relationship to victims, general criminality), and total scores can range from −2 to 13 (Helmus, Thornton, Hanson, & Babchishin, 2012; Phenix, Doren, Helmus, Hanson, & Thornton, 2008). Interrater reliability has been shown to be high with an intra-class correlation (ICC) of .98 (Helmus & Hanson, 2007); however, the authors noted that this was exceptionally high and should not be considered representative of the typical circumstances in which the Static-2002 would be used. Modest internal consistency estimates were found for the content area subscales (Cronbach’s αs for subscales ranged from .45 to .74 and for total score, .68; Langton, Barbaree, Hansen, Harkins, & Peacock, 2007). The Static-2002 has been shown to predict sexual, violent, and general recidivism with area under curve (AUC) values, ranging from .64 to .79, and has been cross validated in several studies, often showing that it can outperform the Static-99 (Bengtson, 2008; Langton, Barbaree, Hansen, et al., 2007; Langton, Barbaree, Seto, et al., 2007; Looman & Abracen, 2010; Stalans, Hacker, & Talbot, 2010).
The Brief Assessment of Recidivism Risk–2002R (BARR-2002R) comprises the age item and the general criminality score from the Static-2002R (Babchishin et al., 2016). The measure has shown to have large effect sizes in predicting nonsexual violent recidivism among men convicted of sexual offences (AUC = .74) and violent and sexual recidivism (AUC = .70), but had a smaller effect size predicting sexual recidivism (AUC = .60).
Static-99R
The Static-99R (Hanson & Thornton, 1999; Harris, Phenix, Hanson, & Thornton, 2003; Helmus et al., 2012) is a 10-item static risk assessment tool used to assess risk of sexual recidivism among adult males who have been charged with a sexual offence. The instrument includes 10 items, and total scores range from −3 to 12. The Static-99 has demonstrated excellent interrater reliability (ICC = .98 in Rettenberger, Matthes, Boer, & Eher, 2010; ICC = .90 in Barbaree, Seto, Langton, & Peacock, 2001), although one study found markedly lower values in an adversarial field setting (ICC = .64 in Murrie et al., 2009). The Static-99R also has good predictive validity for sexual, general violent, and general criminal recidivism (AUCs = .68, .70, and .72, respectively; Babchishin, Hanson, & Helmus, 2012).
Recidivism
To assess recidivism accurately, individuals were included in the analysis only if the follow-up period was longer than 2 years to allow for a minimal amount of time postrelease. Data from criminal records received from the Canadian Police Information Centre (CPIC) and the provincial Correctional Management Information System (CoMIS) were analyzed to determine whether there were any (a) new offences including community supervision violations that led to a new conviction, (b) new violent offences, and (c) new sexual offences, in the form of charges and convictions.
Procedure
The present research was reviewed by two institutional research ethics boards (REBs); one of these REBs is designated to review research proposals addressing the use and disclosure of health information. Clinical files were reviewed by trained research assistants. Each file varied in its contents, potentially containing presentence reports, referral information from the courts and/or the probation officer, criminal records, demographic information, police reports, general documentation about the individual, and any previous criminal justice and/or mental health reports. Some files also contained victim impact statements and victim descriptions. Because PAI scale scores were directly coded from the psychological test protocol, interrater reliability was less relevant in the coding procedure. However, interrater reliability of the Static-2002R for the larger study was examined on a subset of files (n = 29) and reported in a previous published work (see Jung et al., 2017). The ICC was .89 for the total Static-2002R score.
Results
To investigate the use of the PAI scales to identify treatment needs and to predict recidivism, several analyses were conducted. To examine the association between overall risk and PAI scales, Pearson correlation coefficients were calculated. To examine the predictive validity of the risk scales and subscales and the PAI scales, the area under the receiver operating characteristic curve (AUC from ROC analyses; Rice & Harris, 2005), which is the most commonly used and recommended effect size statistics for recidivism prediction, was used (Helmus & Babchishin, 2017). Incremental validity was examined using a series of logistic regression analyses. An alpha of .05 was used to examine significance of the findings.
Prior to analyses, the individuals’ PAI profiles were examined for their validity on PAI validity indicators, that included the inconsistency (ICN; ≥ 73), infrequency (INF; ≥ 75), negative impression (NIM; ≥ 92), and positive impression (PIM; ≥ 68) scales. If they had T-scores that exceeded the cutoff according to the PAI manual (Morey, 2007), then those profiles were excluded (n = 25). The means for each of the included scales and subscales did not change significantly when these cases were removed from the analyses.
Association Between PAI Scales and Risk
Pearson correlation coefficients are listed in Table 1 between the risk measures (totals and subscales) and the antisocial and antisocial-related scales on the PAI. When we examine the correlations between the antisocial and related scales, the total scores of the Static-99R, Static-2002R, and BARR-2002R significantly and positively correlated with the antisocial scales, including the overall antisocial scale and its subscales, antisocial behaviors, egocentricity, and stimulus seeking. The total scores were significantly associated with the drug problems scale and the dominance scale as well. The BARR-2002R total score also showed significant positive associations with alcohol problems and aggression scales, although the Static-99R and Static-2002R were not correlated with these latter PAI scales.
Pearson Correlation Coefficients Between Risk Measures and Domain Scales and the Antisocial Scales of the PAI for the Sample That Excludes Invalid Profiles.
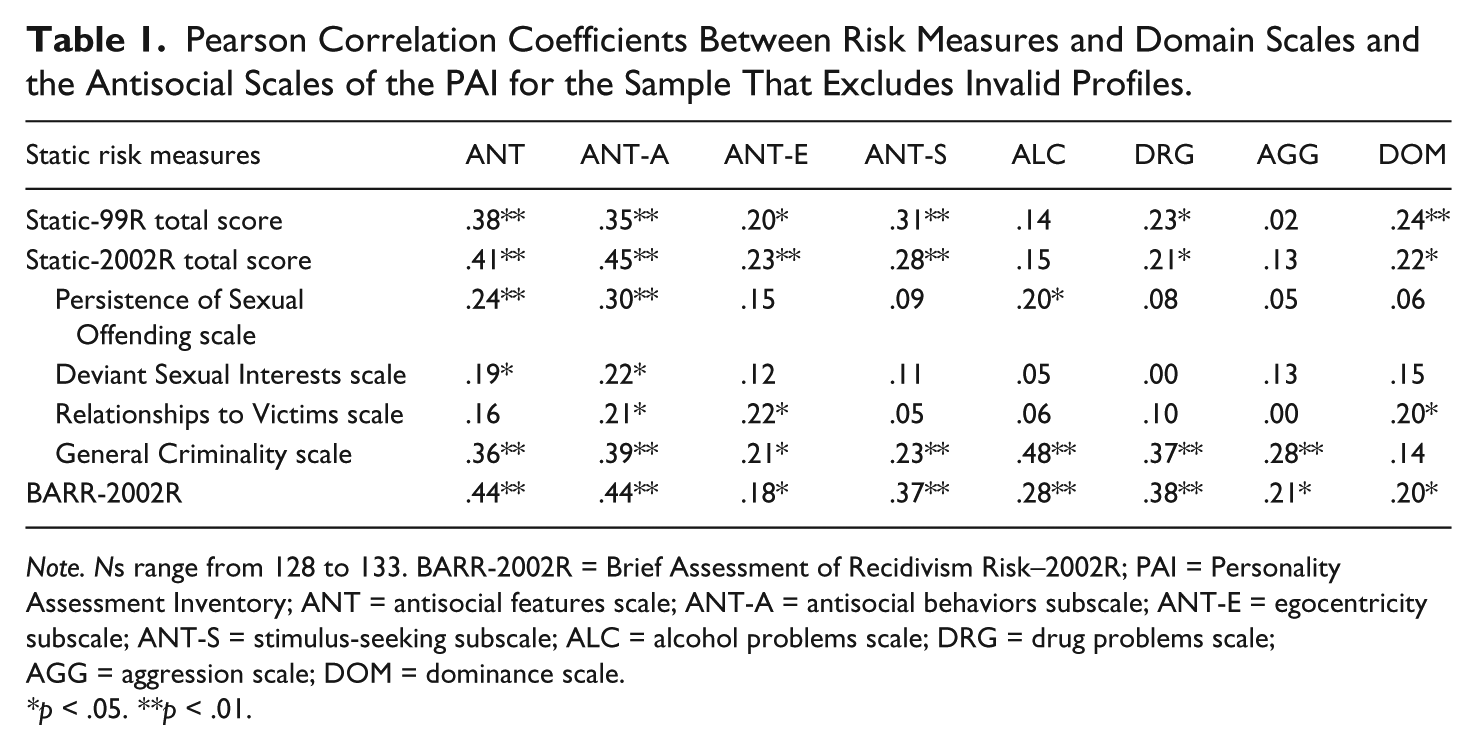
Note. Ns range from 128 to 133. BARR-2002R = Brief Assessment of Recidivism Risk–2002R; PAI = Personality Assessment Inventory; ANT = antisocial features scale; ANT-A = antisocial behaviors subscale; ANT-E = egocentricity subscale; ANT-S = stimulus-seeking subscale; ALC = alcohol problems scale; DRG = drug problems scale; AGG = aggression scale; DOM = dominance scale.
*p < .05. **p < .01.
When we examine the domain scales on the Static-2002R, the persistence of sexual offending and deviant sexual interests scales were associated with the overall antisocial features scale and the antisocial behaviors subscale of the PAI. Persistence of sexual offending scale was also significantly related to the alcohol problems scale of the PAI. The relationships to victims scale were significantly correlated with two of the antisocial subscales, namely, antisocial behaviors and egocentricity, and also the dominance scale. Similar to the BARR-2002R (which comprises the age item and the general criminality items), the general criminality scale was positively associated with the antisocial scale, its three subscales, the alcohol and drug problem scales, and the aggression scale; however, it was not correlated with the dominance scale.
Pearson correlation coefficients were calculated to examine the associations between the risk measures and selected clinical, treatment, and interpersonal scales of the PAI, and these are listed on Table 2. There were very few significant correlations between the risk measures and these PAI scales. The total scores from the Static-99R and Static-2002R were only positively associated with the mania scale of the PAI. The relationships to victims scale was negatively associated with the anxiety-related disorders scale, indicating that the higher the score on the Static-2002R subscale, the less endorsement of anxiety-related problems, and positively associated with the treatment rejection scale, suggesting that those with unrelated victims are more likely to reject treatment. The BARR-2002R and the general criminality subscale were significantly and positively associated with paranoia and borderline features scales of the PAI. The persistence of sexual offending and deviant sexual interests scales were not significantly associated with any of these selected scales.
Pearson Correlation Coefficients Between Risk Measures and Domain Scales and the Clinical, Treatment, and Interpersonal Scales of the PAI for the Sample That Excludes Invalid Profiles.

Note. Ns range from 130 to 133. BARR-2002R = Brief Assessment of Recidivism Risk–2002R; PAI = Personality Assessment Inventory; ANX = anxiety scale; ARD = anxiety-related disorders scale; DEP = depression scale; MAN = mania scale; PAR = paranoia scale; SCZ = schizophrenia scale; BOR = borderline scale; RXR = treatment rejection scale; WRM = warmth scale.
*p < .05. **p < .01.
Predictive Validity
In addition to examining the associations between the PAI scales and the risk measures, associations between the PAI scales and actual recidivism were also investigated. AUCs are typically preferred over other measures of predictive accuracy because they are less affected by the base rate of recidivism (Rice & Harris, 2005). AUC values between .5 and 1 indicate prediction exceeds chance, and Rice and Harris (2005) have noted that AUCs of .56 correspond to a small effect, while .64 reflects a moderate effect, and .71 reflects a large effect. Three recidivism outcomes (general, violent, sexual) were included in the analyses, and the average follow-up time was 5.44 years (SD = 1.83). It is important to note that the base rates for each recidivism outcome were quite low, so the statistical analyses may be biased. The overall rate for any recidivism was 15% (17 of 113), for violent recidivism was 8% (9 of 113), and sexual recidivism was 5.3% (6 of 113).
AUCs were calculated using the Static-99R total score for each of the three recidivism outcomes and are reported on Table 3. The average Static-99R total score is 3.01 (SD = 2.20). The Static-99R showed large effect sizes for all three outcomes (any new offences, any new violent offences, and any new sexual offences) with AUCs of .84, .79, and .80, respectively). For the Static-2002R, the average total score is 3.18 (SD = 2.52). The Static-2002R also revealed large effect sizes for all three outcomes (AUCs = .86 for general, .83 for violent, .82 for sexual). All AUCs were significant.
AUCs for the Static-99R, Static-2002R, and PAI Scales on Any, Violent, and Sexual Recidivism Outcomes.

Note. AUC denotes area under the ROC curve. 95% confidence interval is listed in brackets. Statistically significant findings are bold-faced (i.e., 95% confidence interval does not include .50). AUC = area under curve; BARR-2002R = Brief Assessment of Recidivism Risk–2002R; PAI = Personality Assessment Inventory; ROC = receiver operating characteristic.
The selected PAI scales were examined for their ability to predict the three recidivism outcomes. As seen on Table 3, the antisocial features scale and its three subscales showed moderate to large effect sizes, demonstrating an association with general, violent, and sexual recidivism (e.g., AUCs for antisocial features = .76, .79, and .84, respectively). The dominance scale also predicted violent recidivism (AUC = .69). None of the other three antisocial-related PAI scales (alcohol and drug problems, aggression) predicted any of the recidivism outcomes (i.e., confidence intervals included chance). Of the clinical scales of the PAI, three scales demonstrated effect sizes in the moderate to large range for at least one recidivism outcome. Specifically, the mania scale predicted violent and sexual recidivism (AUCs = .70 for both outcomes), and the paranoia (AUC = .83) and borderline features (AUC = .76) scales of the PAI demonstrated significant and large effect sizes in their association with only sexual recidivism. None of the other PAI scales were significant as their confidence intervals included chance.
Incremental Validity
The incremental validity of PAI scores over the Static-99R and over the Static-2002R was examined. Given the low base rate for sexual recidivism to adequately conduct regression analyses (i.e., seven offenders had been reconvicted for sexual offending), violent recidivism was used. For this analysis, the total score from the Static-99R was entered as a single predictor in the first model and subsequently the PAI scale scores of antisocial features, paranoia, and borderline features scales were entered in the second model. None of the PAI scales demonstrated incremental validity over the Static-99R in the second model, as shown in Table 4. In the next model comparison, the Static-99R was entered as a single predictor and compared with the Static-99R combined with the PAI scale scores of the antisocial subscales, antisocial behaviors, egocentricity, and stimulus seeking. Again, none of the subscales showed incremental validity over the actuarial measure (see Table 4).
Logistic Regression Analyses Examining the Incremental Validity of PAI Scales Over the Static-99R and Static-2002R in Predicting Violent Recidivism.

Note. PAI = Personality Assessment Inventory.
p < .05. **p < .01. ***p < .001.
Similar analyses were conducted using the Static-2002R, as shown in Table 4, entering the PAI scale scores of antisocial features, paranoia, and borderline features in second model for the first analysis, and then the antisocial behaviors, egocentricity, and stimulus-seeking subscales in the second model for the second analysis. None of the PAI scales for either analysis demonstrated incremental validity over the Static-2002R.
Discussion
The rationale for this study was to examine the use of the PAI as a measure of risk-related constructs, and we examined the PAI’s potential use as a treatment planning and risk management tool with a sample of men who were convicted of sexually offending. Our results were congruous with past research that involved samples of men who were convicted of general and sexual offending. We found that selected scales from the PAI were strongly associated with constructs of risk and with recidivism outcomes, although on its own, PAI scales did not add incremental validity to existing actuarial measures of sexual violence risk.
Of particular note, the antisocial scale and all three antisocial subscales were strongly associated with assessed risk, as measured by extant sexual violence risk measures, the Static-99R and Static-2002R, and the derived violent risk measure, BARR-2002R. Many of the domains on the Static-2002R demonstrated strong relationships with the antisocial scores on the PAI. The antisocial features scale, which captures personality and behavioral features relevant to constructs of antisocial personality and psychopathy, was associated with all domain scales except for the relationships to victims scale. The antisocial behaviors subscale (ANT-A) of the PAI, which assesses the presence of antisocial acts during adulthood and adolescent and a history of difficulties with authority or society norms, was associated with all four of the Static-2002R scales. The egocentricity subscale (ANT-E) assesses callousness and lack of empathy and was associated with the relationships to victims and general criminality scale of the Static-2002R. The stimulus-seeking subscale (ANT-S) only demonstrated a relationship with general criminality as measured by the Static-2002R. In addition to the relationship between the antisocial scales and subscales of the PAI and assessed risk, significant relationships emerged with various recidivism outcomes. Our findings are consistent with published research indicating that the antisocial scale is able to predict criminal recidivism and institutional infractions (see meta-analysis by Gardner et al., 2015), and sex offender registry violations (Boccaccini et al., 2010). Although these associations are meaningful, the antisocial scales and subscales do not add incremental predictive validity to existing actuarial measures. A report by Boccaccini et al. (2010) also reported similar findings using the Static-99. Our study’s findings are also consistent with studies by Reidy et al. (2015), who found a relationship between the antisocial, aggression, and Violence Potential Index (VPI) scales of the PAI and institutional misconduct.
When we examined other antisocial-related constructs, the drug abuse and dominance scales were associated with the sexual violence risk measures, Static-99R and Static-2002R. These PAI scales, along with alcohol problems and dominance interpersonal scales, were also associated with the BARR-2002R (which includes the general criminality items). Although we found relationships between these antisocial-related scales and assessed risk, these relationships did not necessarily include actual recidivistic behavior. In fact, none of the scales were associated with behavioral indicators of recidivism, except for the dominance scale which was associated with violent recidivism. These findings were somewhat surprising given the importance of the central eight in predicting general recidivism, which includes substance abuse problems (Andrews & Bonta, 2010). Moreover, the aggression scale has been found to be a robust predictor in Gardner et al.’s (2015) meta-analytic study and the strongest predictor in Boccaccini et al.’s (2010) study with men who had been civilly committed for sexually offending. It is important to note that the current study had a small sample size of 158 compared with the size of the sample used in Boccaccini et al.’s study (N = 1,412 civilly committed sexual offenders). Beyond sample limitations, it is also relevant to acknowledge the dynamic nature of several of these scales. The PAI was completed by offenders at intake in our study, and therefore change that occurs post-assessment as a result of potential substance abuse and emotional management treatment is not accounted for when examining the substance abuse and aggression scales. This should be a consideration for future studies to control for related interventions when examining the predictive validity of PAI scales. With regard to the dominance scale, although we found a relationship with the total scores on the risk measures and violent recidivism, past studies have not consistently shown it to have an association with recidivism outcomes (e.g., Boccaccini et al., 2010; Douglas, Hart, & Kropp, 2001; Ruiz, Cox, Magyar, & Edens, 2014).
In addition to examining the antisocial and antisocial-related scales from the PAI, we explored several clinical, treatment, and interpersonal scales. Very few relationships emerged between these scales and assessed risk or recidivism. For example, the mania scale of the PAI was associated with sexual violence risk, paranoia and borderline scales were associated with the BARR-2002R (and the general criminality scale, but its items are also in the BARR-2002R), and the anxiety-related disorders and treatment rejection scales were negatively and positively, respectively, associated with the Static-2002R’s relationships to victims scale. What was remarkable was that the mania, paranoia, and borderline scales were also associated with sexual recidivism (the mania scale also predicted violent recidivism as well). In Boccaccini et al.’s (2013) study, they found that the borderline scale predicted institutional misconduct; however, these scales did not emerge as predictors in other studies with individuals who have sexual offended. Despite the association between these scales with sexual recidivism in this study and not general recidivism, incremental analysis of the paranoia and borderline features scales (which had the largest effect sizes) did not add to the predictive validity of the actuarial measures. This could reflect the small sample size (i.e., low power), but it could also simply be the case that much of the variance is better explained by statistically created measures of risk rather than clinical scales that were never developed for this purpose.
Our results further affirm that the Static-99R, Static-2002R, and BARR-2002R are valid tools for informing the risk principle. This research particularly contributes to validation of the Static-2002R because there is relatively less empirical research in light of the continued use of the Static-99R over the Static-2002R (see McGrath, Cumming, Burchard, Zeoli, & Ellerby, 2010). Unlike the Static-99R, the Static-2002R assesses criminogenic needs. In this study, the results indicate that the PAI has some utility as a tool for assessing the status of some needs that are potentially criminogenic for men who sexually offend. Our results show that numerous PAI scales/subscales are associated with the risk domains of the Static-2002R; however, the vast majority of PAI variables that demonstrated significant relationships were associated with the general criminality domain of the Static-2002R. Indeed, from an RNR perspective, several PAI scales are indicative of “central eight” criminogenic needs, which are predictive of general recidivism (Andrews & Bonta, 2010), and meaningful associations can be drawn between the central eight and the PAI scales. One of the central eight, antisocial personality patterns, can be assessed by the antisocial scale (ANT), its subscales (ANT-E; ANT-S), and other relevant scales, such as dominance (DOM, which assesses tendency to be controlling and forceful in relationships and exhibits little tolerance for those who disagree) and borderline scales (BOR, which assesses poor control over emotions, intensive and combative interpersonal relationships, impulsivity by engaging in self-destructive behaviors). A history of antisocial behaviors can be appropriately assessed using the antisocial behaviors scale (ANT-A), and substance abuse can be assessed with the drug and alcohol problems scales. Criminal attitudes could be drawn from the paranoia scale (PAR), which assesses a tendency to be resentful and hold grudges, and a readiness to identify inequities in how one is treated by other people. However, despite the utility of these associations with general criminogenic needs, our results indicate that, consistent with the face validity of the PAI, it does not include content that is directly relevant to criminogenic needs associated with sexual deviancy.
Hence, the PAI can potentially be a helpful part of a larger battery that includes valid risk instruments, well-conducted interviews, and validated psychometric measures. Differing from other risk tools, the PAI’s utility is relatively convenient, given the self-report nature of administration and the availability of computer scoring. Others have concluded that the PAI has the potential as a screening tool for areas that require a more thorough assessment (Douglas et al., 2001). The PAI is a good broad measure for this purpose with some obvious limitations. It contains a wide range of scales, many of which are theoretically, if not statistically related to the criminogenic needs of men who sexually offend. In that sense, the PAI should be viewed as a potentially useful inclusion in an assessment battery, but should not be relied upon as a stand-alone measure of risk, nor should it be the sole source of information for identifying relevant criminogenic needs. Further examination of the PAI as a measure of dynamic criminogenic needs may be useful, although it is beyond the scope of this article. Currently, we are moving into the fourth generation of risk assessment, and the PAI may be helpful, upon further investigation, as an adjunctive measure of change.
In addition to assessing criminogenic needs, others have highlighted the need to assess specific responsivity concerns as per the third principle of the RNR model (Jung & Dowker, 2016; Looman, Dickie, & Abracen, 2005). An assessment of notable responsivity issues should be a starting point to determine the most effective treatment approach and identify any adjunctive interventions that may be helpful. The existing literature does not have an approach to assess areas of responsivity, with the exception of using separate measures. It is important to use research appropriate, valid measures to evaluate responsivity and to consistently use these evaluative approaches to ensure communication and reliability among therapists. Given the ease of using the PAI in a clinical setting and its association with sexual violence risk, there are several scales on the PAI that may capture responsivity constructs that have been identified in previous literature (e.g., treatment motivation, borderline features, mental health concerns such as depression, psychosis, and anxiety; Jung & Dowker, 2016; Looman et al., 2005). An assessment of responsivity factors is needed to determine the most effective treatment approach and identify any adjunctive interventions and the PAI may be useful to assess some of these responsivity issues. Further development of this area is needed and perhaps empirical work that examines treatment success and change in selected PAI scales, which capture specific responsivity issues, would determine the PAI’s utility for this purpose.
It is important to note any limitations of this study. For some of our analyses, the sample sizes were small, and particularly so when examining predictive validity where the number of recidivists were as small as seven of 129 and comparisons included groups as small as 17. A larger sample size is needed for us to make more definitive conclusions. Moreover, the study used a retrospective design where data collected from archival clinical files, and a more ideal methodology would involve a prospective study where data are collected and followed by an examination of recidivistic behavior. Unlike some previous studies (e.g., Boccaccini et al., 2010), the VPI of the PAI was not recorded and therefore not included in this research and the analyses, although the VPI was not one of the more robust predictors found in a recent meta-analysis (Gardner et al., 2015).
In conclusion, the current study offers further support for the use of the PAI to assess risk-relevant targets with men who sexually offend. Reidy et al. (2015) contend that the PAI’s efficacy in predicting inmate misconduct and violent behavior is not merely an artifact of a few studies, but can make a modest contribution to overall risk assessment. They purport that the practicality of using the PAI makes it particularly appealing. Given the limited educational level of many prisoners, the fact that the PAI requires only a fourth-grade reading level makes it amenable for use as a self-report inventory. More importantly, the PAI identifies relevant clinical factors of interest to prison officials needing to manage the mental health and behavioral needs of a diverse inmate population, and concerns about assessing the accuracy of inmate self-report are addressed by the PAI’s inclusion of several response-style indices (e.g., carelessness, random responding, and minimization or exaggeration of symptoms). In addition to the practical use of the PAI with men who are in correctional settings and/or being supervised in the community, the PAI has been demonstrated to modestly be associated with relevant offending behaviors.
The PAI has the potential to make a valuable contribution to the assessment and treatment planning of individuals who sexually offend, in light of its ability to assess criminogenic risk factors, such as antisociality, substance abuse, and emotional dysregulation, and even responsivity as shown in other studies. The PAI has some promise for assessing constructs that are dynamic in nature and may serve as a good adjunct to actuarial measures, although it should not replace these tools when assessing sexual violence risk, and the PAI may be useful when clinicians are limited in their resources to conduct a comprehensive risk evaluation. Of particular note, the PAI can be most helpful identifying obstacles engaging offenders in treatment thereby capturing any responsivity issues early on when providing rehabilitative services. Hence, it can be helpful to administer the PAI as part of a more comprehensive assessment for those who sexually offend.
Footnotes
Acknowledgements
We gratefully acknowledge the support provided by the Northern Alberta Forensic Psychiatry Services, the Faculty of Arts and Science and the Research Office of Grant MacEwan University, and the Integrated Threat and Risk Assessment Centre. We also thank Alberto Choy and Tarah Hook for their earlier assistance in the development of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.