
Abstract
Current evidence about the impact of specialized sex offender treatment on reoffending remains inconsistent, drawing attention to the need to focus more on those program characteristics that potentially moderate outcome. This review considers current professional perspectives and evidence on two defining aspects of treatment: its intensity and timing. It is concluded that insufficient evidence currently exists to articulate best practice in this area and there is a pressing need to collect empirical evidence about the effectiveness of different intensity treatments offered at different stages of sentence.
The last 10 years have seen the publication of a number of evaluation studies and reviews that address the overarching question of whether treatment is likely to be effective in reducing reoffending in known sex offenders (e.g., Collaborative Outcome Data Committee, 2007; Mews, Di Bella, & Purver, 2017; Mpofu, Athanasou, Rafe, & Belshaw, 2016; Schmucker & Lösel, 2015). Many of these make the important observation that the existing evaluation data are still not particularly strong. For example, one meta-analysis by Långström and colleagues (2013) reported major weaknesses in research designs that, in their view, should preclude any substantive conclusions being drawn about the overall effectiveness of treatment. They emphasized that this is largely a result of the lack of randomized controlled trials, while noting the practical and ethical challenges that are inherent in such designs (e.g., withholding treatment to create a control group may create unknown risks to the community; using treatment refusers as a control group creates an inherent bias in motivation for intervention; trying to produce identical environmental conditions for comparison groups, especially in outpatient settings, may be nearly impossible).
One set of variables that has been less frequently considered is the differential impact of the treatment itself, although there does appear to be some consensus that treatment is likely to be more effective when it is tailored to the risks, needs, and offense dynamics of individual offenders (Przybylski, 2015). Hanson and Morton-Bourgon (2009), for example, concluded that treatment programs that adhered to Risk–Need–Responsivity (RNR) principles showed the largest reductions in recidivism, arguing that these “should be a primary consideration in the design and implementation of intervention programs for sex offenders” (p. 25). Schmucker and Lösel’s (2008) review is also important as it classified cognitive behavioral therapy (CBT)–based and behavioral interventions as “the only approaches to have significant treatment effects, with the cognitive orientation of the treatment program . . . [adding] . . . significantly to the explanation of effect size variance” (p. 15). It is, nonetheless, difficult to provide firm advice when more specific questions about the types of treatment that are likely to be effective are asked. For example, evidence is simply not available about whether different modes of treatment (individual or group) have similar effects (Fernandez & Marshall, 2000), or on the impact of a range of other issues such as homogeneous versus heterogeneous group membership, therapist qualifications, and therapist to client ratios. This article seeks to synthesize current evidence and professional thinking about two defining aspects of the structure of treatment: its duration and timing. In light of what is a limited evidence-base to answer questions about the optimal structure of sex offender treatment, a summary of current expert opinion on the available data, in our view, is important for responsible decision making about which types of program should be invested in.
Treatment Duration
Smid, Kamphuis, Wever, and Verbruggen (2015) have noted that not only are recommendations about the preferred treatment duration for sex offenders scarce, but that advice on such matters is also inconsistent. Yates (2013) has similarly observed that practice in this area still varies substantially across jurisdictions. Suggestions about optimal treatment length can, however, be found in the professional practice literature. W. L. Marshall, Jones, Ward, Johnston, and Barbaree (1991), for example, recommended that treatment should be delivered across two sessions a week over 3 months for low-risk offenders, with high-risk offenders requiring three sessions a week over 9 months. Hanson (2009, cited in Smid et al., 2015) later described a high-intensity treatment consisting of daily group treatment sessions amounting to 15 hr per week for 8 to 12 months and a low-intensity treatment consisting of 2 to 5 hr of group sessions per week for 4 to 8 months. Treatment standards, such as those from the International Association for the Treatment of Sexual Offenders (IATSO; n.d.), are also often used as the basis for assigning offenders to treatments of different intensity levels, although the empirical foundations for these standards is rarely articulated.
A particular issue is the extent to which the intensity and duration of treatment should be matched to the characteristics of the individual offenders, with some programs recommending that moderate risk offenders receive between 80 (Beech & Mann, 2002) and 120 contact hours (e.g., W. L. Marshall, Marshall, Serran, & Fernandez, 2006), and others that high-risk offenders receive between 160 to 195 contact hours and approximately 300 hr of treatment contact (Correctional Service Canada, 2000). For Olver and Wong (2013), the basic mandate of high-risk sexual offender programs, as indicated by their label, is to provide high-intensity treatment, that is, programs that have both a longer duration and more treatment contact. Olver and Wong argue that high-risk sexual offenders frequently present with a range of treatment specific issues or responsivity considerations that require longer treatment (e.g., low motivation, denial, cognitive impairment, and literacy deficits). According to the Correctional Services Canada (2009) national guidelines, high-risk sexual offenders (i.e., those allocated to high-intensity treatment) attend five 3-hr sessions per week for 6 to 9 months. This results in a true “dosage” of between 360 and 540 treatment hours per program. Moderate-intensity programs run for 4 to 5 months (at 10 hr per week), resulting in a total of 160 to 200 hr per program. Low-intensity programs run for 2 to 3 months (at 3 to 5 hr per week), or a total of between 24 and 60 hr per program. These dosage levels are described as broadly similar to those employed in the H.M. Prison Service which provides treatment for sexual offenders in prisons in England and Wales. The prison service core treatment program, for example, is a basic program for medium risk or higher offenders in custody (with an IQ of 80 or higher) which lasts for an average of 6 months, and involves 84 sessions (up to five per week, 2.5 hr per session) delivered in 20 blocks. There is also an extended program for “high” or “very high” risk offenders who have successfully completed the core program which involves another 76 sessions (6 months; up to four sessions per week; 2.5 hr per session, delivered in nine blocks). These correctional programs, however, may still be substantially lower intensity than treatment provided by forensic psychiatry services. Smid, Kamphuis, Wever, and Van Beek (2016), for example, have described a Dutch mandatory inpatient sex offender treatment program which is offered by health providers following the completion of a prison sentence. The average treatment duration for the offenders in this program was reported to be 8 years and 4 months (SD = 42.6 months), although this did include time as offenders progressively gained more extended forms of leave, including access to “halfway houses.”
Yates (2013) has reported evidence that 100 contact hours is sufficient to reduce recidivism for general offenders presenting with moderate risk and few criminogenic needs, 200 hr was more effective when offenders were either high risk or had multiple criminogenic needs, and that 300 contact hours or more was required to reduce recidivism among offenders who were both higher risk and who had multiple criminogenic needs. Based on research pertaining to general offenders, as well as the results of evaluations of accredited treatment programs, Hanson and Yates (2013) recommended no specialized treatment for low-risk sexual offenders (the bottom 10% to 20% of the risk distribution), 100 to 200 contact hours for moderate risk sexual offenders, and a minimum of 300 hr for sexual offenders presenting with high risk and high needs (the top 10% to 20% of the risk distribution).
A specific issue concerns the dosage of treatment for those offenders who present with traits indicative of psychopathy, perhaps suggesting that psychopathic violence is a more resistant form of pathological behavior (Reidy, Kearns, & DeGue, 2013). This is in light of evidence that psychopathic offenders drop out of treatment more frequently than nonpsychopathic offenders, with treatment dropout associated with higher rates of subsequent violent and sexual reoffending (Polaschek & Daly, 2013). Such findings are the basis for recommending that treatment for psychopathic offenders can be improved through the development of more tailored treatment approaches, in combination with higher intensity programs. For example, highly psychopathic offenders are often described as presenting substantial challenges to effective treatment, with early research even suggesting that treating psychopaths may increase risk even in those who demonstrate good treatment behavior (Hart & Hare, 1997; Rice, Harris, & Cormier, 1992; Seto & Barbaree, 1999). Polaschek and Daly (2013) have, however, suggested that the professional perspective on this issue may be changing and Olver and Wong (2013) have argued that it is a matter of further scientific inquiry as to the extent to which a sexual offender with a high Psychopathy Checklist score is, de facto, less treatable than other high-risk offenders. A key point here, however, is that the prevalence of psychopathy (as measured by the Psychopathy Checklist-Revised) among sex offenders has been reported to be 10% to 15% among child molesters and 40% to 50% for rapists and those with both child and adult victims (Hare, 1999). There is also evidence that the strongest predictor of sexual reoffending is a combination of high levels of psychopathy and the presence of deviant sexual interest or arousal, which can be defined as arousal to sexual activities with children or coercive sex with nonconsenting adults (Hanson & Morton-Bourgon, 2009). One meta-analysis, by Hawes, Boccaccini, and Murrie (2013), found that the presence of both psychopathy and sexual deviance was associated with a more than threefold increase in sexual recidivism. A particularly worrying subset of offenders presents a combination of high levels of psychopathy and sexual sadism (Mokros, Osterheider, Hucker, & Nitschke, 2011), defined as a paraphilia characterized by recurrent and intense sexual arousal from the physical or psychological suffering of another person, as manifested by fantasies, urges, or behaviors (American Psychiatric Association, 2013). Not only have sexually sadistic offenders been shown to have higher rates of sexual recidivism, but the nature of their sexual offending can be especially severe (Dietz, Hazelwood, & Warren, 1990; Langevin, 2003). In short, blanket rules about treatment dosage or category of sexual offense are unlikely to lead to the delivery of treatment that is matched to the risk and need profiles of every offender.
Available Evidence
The evidence to support such practice guidance does not, however, appear to be particularly robust—drawing, in part, on differential outcome evidence from Canadian evaluations reported by Mailloux and collegaues (2003). These concluded that generally, those at high risk and having high needs should be allocated to higher intensity programs, whereas those with moderate risk and needs should receive moderate intensity treatment, and those with low risk and needs should enter a low-intensity program. Friendship, Mann, and Beech (2003) also reported that high-risk sexual offenders did not respond to a 160-hr treatment program, but that the same program was very effective in reducing rates of reconviction for medium-risk offenders. They also suggest that rapists and sexual murderers require longer treatment than the 160-hr program, in the context of continuing needs relating to dysfunctional thinking patterns and socioaffective difficulties.
Some of the most compelling empirical evidence about treatment intensity comes from Schmucker and Lösel’s (2015) meta-analysis. This not only reported that treatment duration did not influence treatment effect size (there was even a nonsignificant negative relation, r = −.15, p = .47, between length of treatment and reduced reoffending) but that offender risk did not substantially influence these results. This finding contrasts with those from studies that have investigated the impact of different intensity treatment on reoffending outcomes in general offender populations. Sperber, Latessa, and Makarios (2013), for example, reported data from a sample 689 offenders discharged from a community treatment program over a 3-year period. Dosage was defined as number of group hours per client, but their sample specifically excluded sex offenders. A subsequent extension study by Makarios, Sperber, and Latessa (2014) concluded that there is evidence that higher risk offenders will require much higher dosage of treatment; and as a “rule of thumb,” this should equate to 100 to 150 hr for moderate risk and 200+ hr for high risk. However, these effects seem to diminish over 300 hr even for high-risk offenders and dosage of around 100 hr for high-risk offenders appears to have little effect. These data raise the possibility that the benefit of treatment does not improve (and may diminish) when treatment dosage goes beyond a certain threshold, even for those classified as at high risk. It has further been suggested that a general aim of sex offender treatment is to not exceed the duration of 2 years in total length, because of doubts about the added value of treatment (Verschuur, 2012). Concerns about the possible iatrogenic effects of “over-treating” sex offenders appear to be rarely discussed and yet appear to warrant further consideration, especially in light of the move away from the open-ended treatment models that were available in the 1980s to the time-limited approaches that characterize contemporary practice.
Methodological Constraints
A potentially useful way to synthesize the available evidence on the impact of treatment duration would be to classify those programs identified as “successful” (such as those described in the Schmucker & Lösel, 2015, meta-analysis) in relation to their relative intensity, and compare with those programs identified as “unsuccessful.” However, for such comparisons to be meaningful, the key variables of “treatment” and “dosage” need to be consistently defined, and this is unlikely to be the case. For example, treatment is sometimes conceptualized as including aftercare and postrelease components (as in the Smid et al., 2016, study), and maintenance programming (see Day & Casey, 2010).
W. L. Marshall and Yates (2005) have further argued that the true intensity of the treatment offered is contingent on offender need and the completion of any ancilliary programs. Treatment might also be best conceptualized as commencing with the assessment, which typically does begin at the start of the sentence. In an important sense, these two activities cannot, and should not, be separated. Thus, the finding of differential effectiveness may relate to other factors (such as number of programs) rather than the actual dosage of treatment. Similarly, Birgden and Griffiths (2013) made the observation that intensity of treatment matched to risk level does not simply mean high risk (more treatment), moderate risk (some treatment), and low risk (no treatment), but also relates to the differing length and frequency of sessions, the participant to facilitator ratio, duration of treatment, complexity of treatment targets, depth of treatment discussions and assignments, and aftercare and supervision requirements (see also Stinson & Becker, 2013). It is also sometimes the case that while some aspects of treatment are clearly structured and time-limited, other components continue until sufficient progress has been achieved. These definitional issues require attention before any meaningful comparisons between studies can be made.
Treatment Timing
Decisions concerning the timing of treatment appear to currently be based primarily on a clinical rationale relating to the environment in which treatment is offered, rather than specific evidence about differential outcome. In fact, our searches revealed no studies that have directly compared the outcomes of similar treatments delivered at different stages of sentence, and it is thus not possible to separate clinical opinion about when treatment should be offered from the empirical evidence. Thus, the only available reference point for decision making about this issue come from recognized experts in the field, with commentary often seeking to simply articulate a rationale for delivering treatment at a particular time. Accordingly, the references below do not relate to empirical evidence regarding the differential outcomes of offering treatment at different times.
It has been suggested that the provision of treatment early in a sentence can mean that there is too long between completion of the program and release from the prison system during which the effects of the prison environment minimize treatment gain. Olver’s (personal communication, October 12, 2016) Canadian research shows that when time from the end of program to actual release is used as a covariate in outcome studies, there is little impact on the overall treatment effect size. The ideal scenario here may be to start treatment early with core programs and then strengthen gains made and promote the generalization and transfer of learning through ancillary programs and security reductions. The high-intensity sex offender programs in Canada, for example, are typically augmented by school, work, constructive leisure, and then general nonspecific sex offender groups (e.g., substance abuse). This may not be the case, however, in other jurisdictions where specific legislation (e.g., notification laws and/or residence restrictions) impact on the offender’s ability to engage with these activities.
The logic for providing treatment toward the end of sentence, as far as can be inferred, is that sex offenders benefit more from treatment offered closer to their exposure to risky environments (i.e., postrelease). This perhaps suggests that some treatment programs continue to draw heavily on relapse prevention models of change, despite Yates’s (2013) observation that this model lacks research support. It is also the case that sex offenders do have the opportunity to rehearse new skills in custody (and do engage in sexually deviant behavior) and the prison environment does provide the opportunity for new ways of relating, thinking, and acting relevant to the reduction of risk. Similarly, although relatively little is known about sex offenders’ sex lives in custody, they are still sexually active, and early intervention could address issues like masturbation to deviant sexual fantasy.
Some potential benefits of offering treatment early in a sentence are that there is often increased motivation to change (resulting from the distress generated by conviction and incarceration), fresher memories of the offense and its determinants, and reduced vulnerability to embellishment or altered recall of past offending. In addition, for most serious offenders, significant time is needed to establish a therapeutic alliance and for an interest in treatment to emerge, and it becomes possible to intervene progressively as interest in treatment increases. Treatment may also be valuable for reducing risk in ways that will allow a prisoner to move to a lower security classification. This would conform with the principle of the right to least restrictive environments, and might offer greater access to other programs that are not available in high security settings.
For those who commence custodial treatment early, there is a need for ongoing maintenance (if there is improvement) throughout the sentence if often identified. However, a review of these programs by Day and Casey (2010) revealed little empirical evidence to support this practice, and the underlying rationale of maintenance programs was not always clear. This is surprising given the widespread recognition that follow-up and support services are vital if the changes made in treatment are to be sustained over time. Taxman and Bouffard (2000), for example, have suggested that the implementation of transitional and/or support services (including relapse prevention, booster sessions, support groups, employment assistance, vocational training, and counseling) is critical to the rehabilitative process. Day and Casey (2010) concluded that maintenance programs are likely to be more successful if they are able to link offenders into environments in which they experience stronger and more positive relationships, antisocial attitudes are not supported, they can reduce levels of negative affectivity, and they can develop a positive and valued sense of personal identity. More recently, Youssef, Casey, and Day (2016) have argued that maintenance programs should be conceptually based on models of the desistance process and offered postrelease to support community reintegration. This would potentially lead to a reconceptualization of the treatment process, such that rehabilitation and reintegration efforts are more closely aligned.
Discussion
The aim of this review was to collate the empirical and professional practice evidence that might be relevant to “best practice” decisions about both the duration and timing of sex offender treatment. This is important from both a policy and practice perspective, and especially relevant to case reviews of serious re-offenses following the completion of treatment. In such circumstances, questions are inevitably raised about the adequacy of the treatment that was provided. However, it is evident from this review that drawing firm conclusions about best practice in this area continues to be premature, primarily because of the limited knowledge that currently exists about treatment effectiveness and those factors that are associated with treatment outcome. While there is a clear need to link program development to current research knowledge, there is a corresponding danger of creating rigid paradigms that constrain practice and potentially result in less effective and less efficient interventions. Furthermore, the very notion that best practice is possible may instill a false sense of confidence in the effectiveness of current approaches. In short, it is evident that the strength of evidence required to translate current knowledge directly into clear practice standards is still not available, and more research is required to understand why specific programs either succeed or fail to bring about their expected outcomes. As a starting point, it would seem reasonable to directly compare the structure and content of the most effective programs against those what have been shown not to work.
Given that sexual offenders often commit nonsexual re-offenses, there is also a case for collecting and applying evidence of differential treatment outcome from the general offending literature (Sperber et al., 2013; Yates, 2013), rather than rely on sex offender specific research. This body of research, however, is also not without limitations even though it is possible to note general professional acceptance of the idea that level of risk should be matched with the intensity of treatment. There is, for example, some evidence that 100 contact hours is sufficient to reduce recidivism for general offenders who are at moderate risk and present with few criminogenic needs, 200 hr is more effective when offenders are either high risk or have multiple criminogenic needs, and 300 contact hours or more is required to reduce recidivism among offenders who are both higher risk and who have multiple criminogenic needs. There is also a professional view, informed by indirect evidence, that specialist treatment should not be offered to those who present a low risk of sexual reoffending (the lowest 10% and 20% of the risk distribution), and it has been suggested that a general aim of sex offender treatment should be to not exceed 2 years in total length. It is nonetheless apparent from this review that the evidence to support such recommendations is, however, not particularly strong.
Decisions about the timing of treatment are currently based primarily on a clinical rationale relating to the organizational environment in which treatment is offered, rather than any substantive evidence about differential outcome. While there are views that early treatment can potentially be of benefit, there is no evidence to suggest that this is more effective in reducing reoffending than treatment that is offered later in sentence. The major concern appears to relate to the practicalities of delivering sufficient treatment for those high-risk offenders with multiple areas of criminogenic need who commence treatment toward the end of sentence. An important consequence of providing treatment early in the sentence is that long-term maintenance programs are then required. Evidence for the effectiveness of such an approach does not currently exist, with the limited knowledge about treatment maintenance restricted to that which occurs in the community (i.e., postrelease) settings. It is also not clear what long-term maintenance in a custodial setting would entail, given the risk of treatment fatigue and the restricted opportunities to implement risk management plans.
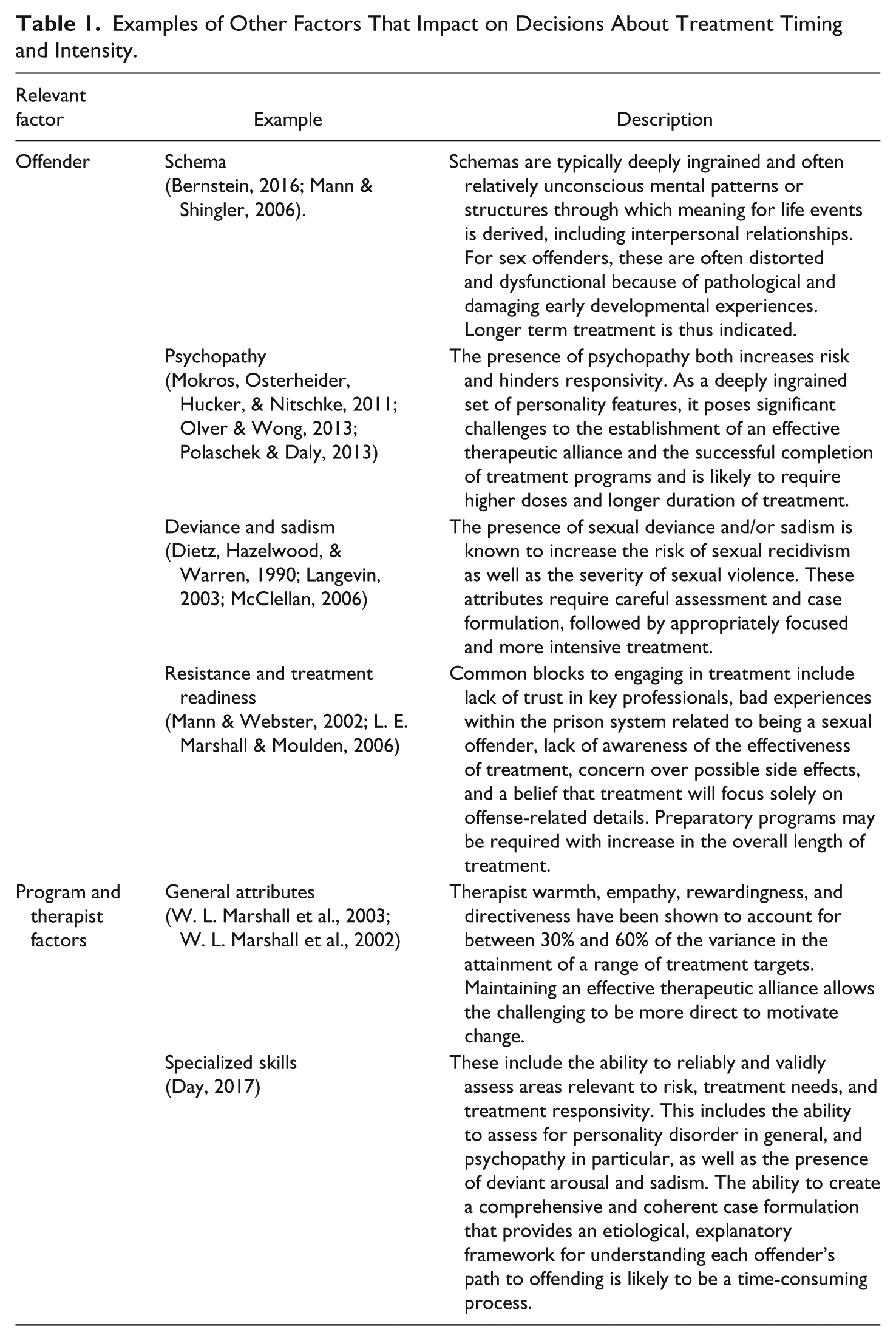
In an important sense, the type and timing of treatment should be matched to the specific needs of each individual offender and the skill set of treatment staff. It is reasonable, for example, to expect that different types of offender will require different treatment approaches. And yet, in the absence of supporting empirical data, this is, in our view, a clinical (rather than actuarial) decision that has to be informed by a careful assessment of a number of factors that impact dosage, timing, and treatment effectiveness. This includes those related to the offender, as well as factors to the treatment program staff (Table 1).
Examples of Other Factors That Impact on Decisions About Treatment Timing and Intensity.
In conclusion, the challenges associated with developing evidence-based practice in sexual offender treatment are immense. It is unlikely that any jurisdiction will have the capacity to conduct controlled trials which compare different intensities of treatment offered at different stages of sentence and the clinical, administrative, and financial implications of providing a suite of programs that are matched to the personal characteristics of offenders and the resources and abilities of treatment staff. And yet, such an approach is clearly needed if we are identify optimally effective treatment programs. This review nonetheless highlights some of the problems associated with the demand among policy makers for “evidence-based” policy information and illustrates how conforming to a “status quo” (or established practice) about key aspects of program delivery can develop. The underlying assumptions of program structure appear to rarely attract the level of scrutiny that might be expected, not only in relation to timing and intensity but also session content, staff skills, and the setting in which treatment is provided. This has implications for the veracity of evidence-based and “best practice” information, as well as how what is envisaged by policy makers may be influenced by organizational, practice, and service delivery interfaces. In our view, and in the absence of any clear empirical evidence about program timing and intensity, an important perspective that can also inform debates about program timing and intensity will inevitably come from those who have expertise and experience in providing treatment. Regardless, from both a program development and policy perspective, there is a need for much greater clarity about the type of program that should be provided.
Recommendations
There is a need for greater standardization in terms of how dosage is calculated, as well as when treatment commences and is finalized. Information that can help evaluators to disentangle the effects of other interventions, including posttreatment and postrelease programming, should be routinely reported as an industry-wide standard.
Programmatic moderators of treatment effectiveness should be the focus of evaluation activity going forward, including the use of randomized evaluation designs where possible, along with further consideration of the impact of offender and staff characteristics on outcome.
High-risk offenders require careful assessment and effective case formulation before decisions about when to begin treatment and how long it should last for can be made. Treatment programs should start sufficiently early in the course of incarceration to allow time for this to occur, and to protect against the further erosion of treatment readiness that can result from the prison environment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.