
Abstract
Developed with the goal of preventing recidivism, contemporary sex offender supervision models focus on collaboration between probation officers and therapists. This exploratory study used focus groups to examine the working relationships between probation officers and therapists from two large U.S. urban probation departments. Overall, both probation officers and therapists were quite positive about their working relationships; they valued each others’ roles and agreed that regular, accurate, and timely communication occurred frequently. Not all relationships, however, were effective. Several probation officers and therapists expressed dissatisfaction with poor communication, conflicts between the goals of therapy and probation, a lack of resources, and deficits in the policies they needed to adequately implement components of their supervision model (the containment model). Our findings suggest ways to structure sexual offender supervision that integrate the distinct orientations of probation officers and therapists into a collaboration that promotes public safety and work well for all.
Few individuals who have committed sexual crimes seek treatment without criminal justice involvement. Intensive supervision is effective in directing individuals into services, but surveillance and threats of punishment cannot, on their own, be expected to change individuals’ risk relevant propensities responsible for the persistence in sexual crime. Prosocial change is most likely to occur in a relationship of trust, with professionals skilled in providing hope, challenging dysfunctional thoughts, and promoting effective self-regulation (English, Pullen, & Jones, 1996; McGrath, Hoke, & Vojtisek, 1998). Consequently, many correctional systems consider treatment services an integral part of their response to individuals with a history of sexual crime.
Given that the culture and training of probation officers in the United States is often quite different from that of therapists, constructive relationships between these professions cannot be taken for granted (McGrath, Cumming, & Holt, 2002). There are good reasons, however, for making these relationships as strong as possible. Some research has suggested that the combination of intensive/enhanced supervision and therapeutic treatment is more effective in reducing sexual offender recidivism and enhanced functioning than a surveillance-only approach (McGrath et al., 1998; Stalans, 2004; Turner, Bingham, & Andrasik, 2000; R. J. Wilson, Stewart, Stirpe, Barrett, & Cripps, 2000), although the case is not yet closed on the increased effectiveness of supervision over treatment-only (Morrissey, Fagan, & Cocozza, 2009).
The Containment Model as an Alternative to Standard Probation
As an alternative to standard probation, many jurisdictions across the United States have developed specialized sex offender probation programs, often based on versions of the containment model. The containment model of supervision is a well-known, victim-centered, intensive community-based probation and parole model developed specifically for supervising sex offenders. A major goal of this approach is to enable sex offenders to be in the community—yet prevent them from committing new sex offenses. Containment model advocates argue that meeting these goals requires effective collaboration between probation officers, therapists/providers, police, victim advocates, and polygraphers. Collaboration has been defined as a mutually beneficial and well-defined relationship entered into by two or more organizations to achieve common goals (D’Amora & Burns-Smith, 1999).
The containment model comprised five components: (a) victim- and public safety-centered philosophy, (b) multidisciplinary collaboration in the form of intra- and inter-agency and interdisciplinary teams made up of probation officers and therapists (who communicate frequently and share important information), as well as polygraph professionals, and victim rights advocates, (c) the use of a variety of containment strategies such as intensive community supervision (e.g., frequent office/home visits, low caseload numbers, use of GPS technology), sex offender-specific treatment emphasizing cognitive behavioral and relapse-prevention group therapy, and post-conviction and maintenance polygraphs, (d) informed and consistent public policies and agency protocols regarding sex offender management, including consistent funding for treatment, the use of actuarial risk-assessment tools for the assessment of dangerousness and recidivism potential, and (e) quality control mechanisms such as regular, multiagency case review meetings, sophisticated collection of data tracking offenders who fail in treatment or commit new crimes, dropout-revocation rates and staff training, to name a few (D’Amora & Burns-Smith, 1999; English, 1998; English, Heil, & Veeder, 2016; English et al., 1996). Both probation sites involved in this study used the containment model of sex offender supervision.
Description of Project and Sites Involved
The current study was part of a larger study examining the effectiveness of a specific risk-assessment tool (the Sex Offender Treatment Intervention and Progress Scale [SOTIPS]; McGrath, Lasher, & Cumming, 2012). One of the goals of risk assessment in corrections is to help professionals form a common understanding of individuals in their care, and to help such individuals understand the common goals of treatment and community supervision (Lasher, McGrath, Wilson, & Cumming, 2015). To examine whether the introduction of the SOTIPS improved communication and collaboration between probation officers and therapists, we examined the nature of their existing relationships prior to introduction of the SOTIPS measure.
Two probation locations were examined: (a) Arizona: Maricopa County Adult Probation Department (including Phoenix) and (b) New York City (NYC): NYC Department of Probation (composed of the five boroughs of NYC—Manhattan, Bronx, Brooklyn, Queens, and Staten Island). The probation department sites were responsible for implementing the dynamic risk-assessment tool, SOTIPS, at baseline, 6- and 12-month follow-up, and collecting additional data from adult men on probation for sexual offenses. As a part of the SOTIPS’ evaluation, focus groups were conducted with probation officers and treatment providers from both sites. This study presents the results of the qualitative baseline focus groups, not the larger quantitative study, which is still in process.
Description of the Two Probation Department Sites
The two probation department data collection sites were selected for study because they provided uniform, specialized, jurisdiction-wide sex offender supervision and treatment services for 300 to 500 probationers, serviced socioeconomic and racially diverse populations, and had a probation department that collaborated with sex offender treatment agencies.
Maricopa County (Including Phoenix)
In 2012, when we collected our focus group data, the Maricopa County Adult Probation Department employed 80 probation officers with different specialties (e.g., field officer, GPS monitoring) who supervised 2,132 individuals on probation for sexual crimes, 1,518 (71%) of whom were in treatment. The average officer had a caseload of 53 individuals. Probation officers averaged 10.7 years with the department (Broderick, 2012). Maricopa County is a mostly urban jurisdiction, with more than 2.5 million people living in the Phoenix metropolitan area; approximately, two thirds of the state’s population resides within the county.
In 1987, the state legislature passed a law mandating lifetime probation for individuals convicted of crimes against children. The county adult probation department’s response included intensive supervision, subsidized treatment and assessment, and services for victims and their families as part of a “dynamic” containment model. Probation officers supervised offender’s progress with behavioral and life issues and their compliance with probation conditions. In 1997, the probation department formally adopted the containment model for probationers. These probationers were required to participate in sex offender treatment provided by providers who met specified competency requirements selected by the Maricopa County Adult Probation Department via a Requests for Proposals (RFPs) process (Maricopa County Adult Probation Department, 2012, Program Narrative, grant submitted to Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking [SMART]).
NYC
In 2012, the NYC Department of Probation was one of the largest in the United States, employing approximately 500 probation officers who supervised 1,068 people on probation for sex crimes. Probation officers had worked for the probation department an average of 15 years (New York City Department of Probation, 2012, Promoting Evidence Integration in Sex Offender Management: Project Narrative). NYC had a population of 8.3 million people residing in five boroughs and comprised 43% of the state’s population.
Unlike Maricopa County, there was no lifetime probation mandate, but, similar to Maricopa County, the NYC Department of Probation adopted the containment model. After conducting a review process to identify the best supervision model for sexual offender probationers (New York City Department of Probation, 2012, Program Narrative, grant submitted to Office of SMART) and relying heavily on a Department of Justice study (English, Pullen, & Jones, 1997), NYC probation selected the containment model as their approach for supervising sex offenders in the community in 2007 (Cumming & McGrath, 2005). To meet these requirements, specialized officers supervised probationers through in-person office and community meetings. The NYC Department of Probation selected providers with the Professional Code of Ethics and the Practices Standards and Guidelines (Association for the Treatment of Sexual Abusers, 2014) in mind. Sex offender treatment providers were selected based on their certification as sex offender treatment providers and their ability and willingness to operate within the containment model.
Description of Maricopa County, Arizona, and NYC Treatment Agencies
There were four Maricopa County and five NYC treatment agencies that provided sex offender treatment to probationers within the containment model approach. Between April and August 2013, program directors from each of the nine treatment agencies completed a 60-item survey designed by the Safer Societies Foundation (McGrath, Cumming, Burchard, Zeoli, & Ellerby, 2010), which provided information on their practices in sex offender assessment, treatment, and management during the 2012 calendar year.
The nine treatment agency program directors reported treating a total of 4,092 adult male offenders who committed stranger and statutory sexual assaults, intrafamilial and extrafamilial childhood sexual abuse, non-contact offenses, and viewed child pornography; Maricopa County treated 2,172 offenders and NYC 1,920. Offenders participated in cognitive behavioral group treatment an average of 24.3 months (SD = 12.8 months) ranging from 4 to 40 months; M = 21.5 and 25.3 months for Maricopa County and NYC, respectively. All nine agencies offered aftercare programs and provided an average of 24 months (SD = 18.7 months) of aftercare (“step-down”) treatment ranging from 6 to 60 months per offender (M = 25.5 and 22.0 months for Maricopa County and NYC, respectively). All nine treatment agencies also used psychological testing, plethysmography, and polygraphy to secure a complete sexual history and to periodically monitor compliance with probation regulations. Every treatment agency had considerable experience providing sex offender treatment (M = 14.4 years, SD = 8.7 years), especially in Maricopa County where the agencies reported treating probationers for over two decades (M = 21.5 years SD = 7.1 years); in NYC, the average was 8.8 years (SD = 4.8 years).
All agency program directors reported that they collaborated with their respective probation departments by allowing probation officers to observe treatment groups; no agency reported that probation officers co-led group with therapists. Due to Maricopa County’s contractual relationship with their four therapy agencies, they more tightly controlled the referral process than NYC, which, on occasion, allowed probationers to select their own private therapist/psychiatrist outside of the approved network of agencies. Collaboration with other treatment stakeholders was common as five agencies utilized risk management teams (composed of mental health, law enforcement, and corrections professionals) and collaborated with victim advocates. The majority of agencies involved family members in their treatment process.
There has been some research investigating the importance, value, and frequency of the probation–therapist relationships, and even speculation that close communication between probation officers and treatment staff contributes to lower rates of sexual reoffense (McGrath et al., 2002). In this qualitative study, we examined how probation officers and therapists from two probation departments in two large metropolitan areas of the United States described their collaboration, communication, and experiences while working together to supervise and treat sexual offenders using the containment model of supervision. They each identified the characteristics of high and low quality working relationships, as well as deficits in resources and policies needed to adequately implement a variety of containment components. Utilizing focus groups, we examined relationships within these systems to highlight significant themes that emerged from the experiences of probation officers and therapists as they engaged in the supervision of probationers who have committed sexual offenses.
Method
This study was part of a multisite project funded by the United States National Institute of Justice (NIJ) in collaboration with the Office of SMART (2012-AW-BX-0153) to investigate the validity and reliability of the SOTIPS (McGrath et al., 2012) when compared with the Static-99R/Static-2002R risk-assessment tools (Helmus, Thornton, Hanson, & Babchishin, 2012). The study was approved by the Human Subjects Review Committee, Social and Behavior Science Research at the University of Minnesota, Institutional Review Board (IRB) Study 1301S26422.
Recruitment and Sample
Maricopa County and NYC probation supervisors and program directors provided a list of all probation officers and therapists who supervised and treated probationers in their departments. All probation officers and therapists were contacted by email asking them to participate in a 2-hr focus group; we were aiming to recruit 10 to 12 participants per focus group. Two focus groups of 2 hr were held at each site: one for probation officers and one for treatment providers (both groups contained both frontline staff and supervisors). The numbers in each focus group were as follows: probation officer focus groups (n = 18, Maricopa County; n = 12, NYC) and therapist focus groups (n = 13, Maricopa County; n = 10, NYC). No monetary incentives were provided to participants but supervisors encouraged their attendance during their regular workday. Focus groups were held at the Maricopa County and NYC probation offices in April and August 2013.
Focus Group Procedures
In total, 13 semi-structured questions were developed for probation officers and therapists. Questions focused on how offenders were supervised and treated, how treatment and probation progress were monitored and assessed, and how termination decisions were made. Parallel questions for probation officers and therapists were developed to assess similar concepts. For example, probation officers were asked the following questions: What is your relationship with your client’s treatment providers/therapists? How involved are you in treatment? Therapists were asked as follows: What is your relationship with your client’s probation officers/supervising agents? How do you work with them? How involved are they in treatment? Additional clarifying probes were used to encourage participants to elaborate on their responses (see the appendix). Participants sat around tables and were digitally audio-recorded using Olympus DS-2 and DS-20 digital audio recorders with two external microphones. The moderators ended the focus groups on time after 2 hr. The third author transcribed the recordings from Maricopa County; transcripts from NYC were prepared by Verbal Ink—a professional transcription service specializing in complex terminology and sensitive audio material. All focus group participants gave first names to introduce themselves, enabling us to track their comments throughout the focus groups. Identifiable information was removed upon transcription.
Data Analysis
Qualitative analysis of the focus groups was conducted by coding transcripts for themes in NVivo10. Coders used line-by-line open coding for all transcripts (Glaser, 1998). The coding strategy was based on social constructionism, a theory used to interpret reality out of the lived experiences of subjects. To achieve reliability and validity, coders identified terms and concepts and clarified thematic meanings throughout the writing process (Charmaz, 1990). The first and third authors read the transcripts multiple times and independently developed broad categories/nodes based on participant responses. Then, both raters met to review, merge, and agree on the broad categories/nodes. After these categories were agreed upon and defined, both coders independently coded all parts of the transcript again and met together to identify subthemes emerging out of the combined themes. Finally, the first three authors met and coded the transcripts using the final categories/nodes and subthemes—creating a final description of the characteristics that facilitated or impeded collaboration between probation officers and treatment providers.
Results
Qualitative analysis of the focus groups revealed several important themes: (a) probation officer perspectives on working relationships with therapists, (b) treatment provider perspectives on working relationships with probation officers, and (c) difficulties/frustrations with important factors in containment model implementation. We edited all quotes for brevity, clarity, and readability.
Probation Officer Perspectives on Therapy, Therapists, and Collaboration
Probation officers were asked to describe their relationship with treatment providers, as well as to give their opinions about the effectiveness of treatment. They identified the characteristics of high and low quality working relationships with therapists.
Characteristics of high quality relationships—Regular, timely, accurate, face-to-face communication
Regular, timely communication was identified by probation officers as an important characteristic that contributed to a high quality relationship with therapists. This was reflected in comments about the frequency of contact among probation professionals: . . . the more contact you have with them, the more you’re gonna find. The supervision and treatment together works better than an assessment. That’s my belief, because I’m actually having a physical contact, I’m seeing them in their environment, when they come to the office its basically they’re blowing smoke up your tail tellin’ you what you wanna hear . . . (Probation officer)
In addition to the frequency of communication, probation officers reported on interactions they believed improved communication. Face-to-face interactions were especially valued: A lot of the times the treatment providers are in our building, so all we have to do is walk downstairs, you know, they come right to the office . . . They’ll have the counselor in the office with the probationer there so they can discuss what’s going on, so it’s a really, really, really, really close relationship. (Probation officer)
Noting the importance of in-person communication, many probation officers identified the benefits of structured containment meetings designed to facilitate collaboration: I feel is very vital to the probation officer to maintain contact with the clinician. The containment meeting is vital. Whether they’re in treatment, whether they’re making progress or they’re not making progress, we have containment meetings to show positive as well as negative. But it’s a good idea that that’s the approach that we take. And I think it does work for monitoring progress. (Probation officer)
Valuing treatment
Probation officers who valued treatment and recognized the importance of the therapeutic process reported having higher quality relationships with therapists; they spoke passionately about the importance of treatment to the rehabilitation process: I think treatment is very, very important! Unfortunately, it took violating the law to get into treatment, but I wish everybody could be in treatment, cuz . . . these guys . . . they have really helped their lives and relationships that have all been possible because they’re in treatment. And as a probation officer I feel like I’m kind of—I’m just a facilitator, like, making sure I’m the eyes and the ears of the court, making sure that they’re following their conditions of probation, but if you were to take out the treatment component, to me it would just be a waste of time. (Probation officer)
Probation officer opinions about treatment were rooted in experiences with specific probationers who made significant strides while benefiting from therapy. One officer mentioned the dramatic changes probationers make during treatment: . . . and I can’t count the number of guys that have told me that treatment has saved their life. Uh, those who dig in and really worked hard that it’s made an enormous difference in every aspect of their life. Some of them would say the same thing about us, some wouldn’t. I think treatment is priceless if it’s done right and you can get the buy-in from the client. (Probation officer)
Positive changes in probationers while in therapy were often considered significant. This probation officer credited participation in therapy for this change: I agree with everyone else that the treatment is very, very important. Sometimes it surprising to see the insight that they get once they’re in there, when they come to us and they’re saying “I didn’t commit this crime at all” and they’re in complete denial and then to see them change, um, through treatment. (Probation officer)
Role adherence
Probation officers discussed the importance of knowing and adhering to their respective roles within the supervision system: . . . from the probation standpoint, we have a certain job, . . . we have certain things that we are supposed to do as officer, we are not therapists, even those who have specialized degrees, that is a separate entity, . . . I think it’s important that you have both the community supervision side and the therapeutic side looking at their risk, cuz I don’t think one side can do it accurately. Because unfortunately, we in probation may be a little more jaded to certain things than the therapeutic side . . . so I think it’s really gonna be a 50/50 to get an accurate profile. (Probation officer)
One probation officer opined that when probation officers and therapists do their respective jobs, probationers are better able to concentrate on treatment: I think when they’re invested in [treatment] . . . their role is a lot more important . . . [our role is to] motivate them and get them to that level where then treatment can focus on getting them on track. (Probation officer)
Characteristics of low quality relationships
In the focus groups, probation officers were questioned about the challenging aspects of their relationships with treating therapists. Poor communication, not valuing treatment, and working with ineffective therapists were characteristics noted by probation officers as contributing to low quality relationships with therapists.
Poor communication
Infrequent, late, poor quality, and inaccurate information from therapists about their work with probationers led to poor quality relationships between probation officers and therapists.
One probation officer contrasted therapists who were good communicators with others who were not: . . . some of them will communicate really well, and quite well and they’ll call and they’ll email, they’ll let you know, they’ll keep you in the loop. Others you’ll forget that they work for that agency until your defendant comes in with complaints . . . (Probation officer)
Another probation officer identified poor timing and generic quarterly reports as detracting from good communication with therapists: . . . the quarterly report as I’ve experienced them, are the ones that tend to arrive a year late are often the very best, but they are of no use because they’re too old. The one’s we get instantaneously are the cut and paste, . . . there is no thought in em so they’re timely but they’re of no use . . . we often get after the fact, so if there was something we were going to miss, we wouldn’t know about it for 9 months. (Probation officer)
Not valuing treatment
Several probation officers stated their belief that therapy does not work and questioned its effectiveness: I think it [supervision] is very important. We’re doing a wonderful job through supervision, and I think it is more helpful. It is better. We get compliance better than through treatment. I’m not a fan of therapy. I think we get more done through supervision and putting the fear into them. (Probation officer)
Another probation officer criticized treatment for not motivating probationers to take responsibility for their sex offenses and questioned therapist motivations: I’m not gonna knock the whole program. I’m gonna say maybe there’s one person or two in there that you do have a group of individuals that come back and say, “I enjoyed it, I acknowledge what I did. I am deeply sorry.” You get good reports, but on the whole, the majority of the times—we have people [therapists] that just want the money. I’m sorry. (Probation officer)
Characteristics of ineffective therapists
Probation officers identified inexperience as an important characteristic of ineffective therapists. One probation officer described a visit to a treatment group, citing the therapist’s passivity and unwillingness to confront offenders as problematic: . . . you will be able to decide and determine how good the therapist is, because there been times when I’ve gone into group to address certain problems and the therapist will just sit there and I’ll just take over. (laughter) It’s true! And then you ask the other group members to their response is to his behaviors and they’ll look at each other like, what’s he talkin about? You know, he’s been doing great, well obviously he’s not because I’m sitting in group and I’m calling him out and the therapist just sits there. (Probation officer)
Another probation officer cited a frustration with private therapists who don’t have specific sex offender treatment training: Because if you’re a private therapist and I need him to go to sex offender treatment and therapy and you don’t know what you’re doing, then you’re not addressing the need, you’re not addressing the need, you’re not addressing the offense, you’re not addressing the issue . . . (Probation officer)
Most had experience with both high and low quality therapists. A probation officer summarized this point by stating, “Some of our treatment providers are bordering on brilliant, some are truly imbeciles.”
Therapist Perspectives on Probation, Supervision, and Collaboration
Therapists were also asked to discuss their relationship with probation officers. They identified the characteristics of high and low quality working relationships.
Characteristics of high quality relationships—Regular, timely, face-to-face communication
Similar to probation officers, therapists described the importance of regular, timely, face-to-face interaction. One therapist described the personal relationship he tried to have with probation officers: I make it my business to know who every PO is if it’s on my list of clients. That way if I do have concerns and if I see a downward spiral going on in somebody’s behavior, I go to that PO and I make them aware of it. And I don’t wait until the end of the month for that progress note. Because, given 30 days, you never know what could happen . . . if you have that communication established, then that’s very valuable . . . (Therapist)
Another therapist appreciated the fact that the probation office and therapy office were in the same building: Same building, same office. So we’re able to maintain that type of communication, and that’s excellent. I mean, we find things out. The clinician will go over to the probation officer or what have you and say, “Look, this is what I know.” Or, as a former probation officer, I may go into someone’s house and I may see things in that house, like magazines or what have you, and then I’ll go back to the clinician and say, “You know what? You know there’s photos and stuff. Let’s put together a containment meeting. We’ll address the issue before it actually becomes a bigger issue.” So being an on-site provider has that communication that we can go back and forth between the probation officer and so forth. (Therapist)
Similar to probation officers, therapists saw the containment meeting as a valued mechanism for increasing face-to-face communication: . . . we also have the same meetings [containment meeting] for positive behaviors to reinforce what’s going on in group, how they’re doing, complying, whether they merit a step down for relapse aftercare, once a month, twice a month. All this is addressed in containment. The SPO may come back with other issues that the clinician may not be aware of, and vice versa. And it’s a meeting of the minds. We’re all at the same table at the same time. (Therapist)
Valuing supervision
Like probation officers, therapists who valued supervision and recognized the importance of the supervision process reported having higher quality relationships with probation officers: . . . it would occur to me that the skill set that those people possess [probation officers] is the kind of skill set that we need to be engendering and fostering in the folks that are supervising the guys on the primary caseload . . . we’re clearly in this together, and the exchange of information back and forth is free flowing and spontaneous and dynamic and the kind of stuff that really lends itself to wanting to do this stuff. (Therapist)
Therapists appreciated the safety that supervision provides: I came into this line of work and ended up staying in Arizona instead of moving back to California because of the opportunity to work closely with probation . . . I feel I get to go to sleep comfortably at night because I made a phone call to a PO . . . who’s gonna watch the person I’m worried about, . . . ah, those are all priceless to me. (Therapist) . . . the safety of all the kids and families that are out there trying to live productive lives. And it’s vital to have a PO doing an intense monitoring as a part of the community monitoring and therapeutic approach. And without the POs or the Department of Probation, the populations that we treat would be dropped down to maybe one percent of what we have now. (Therapist)
Some saw their role as teaching clients how to work with and value the probation: . . . I listen to what probation’s saying whether or not I agree with it or not, and I try to take it and make something productive out of it, I go back to the client and say “Ok, your probation team is really, really worried about this.” . . . and then the client says, “well, I haven’t done that in 2 years” and I say, “ok, well, what can we do to relieve probation?” And if that means you save up and take a specific polygraph around X so that your probation team can relax around that, then that’s what we need to do. (Therapist)
Characteristics of low quality relationships
In describing their relationships with probation officers, therapists identified harsh probation officers and conflict around roles and treatment goals as descriptive of low quality relationships.
Tough, unrealistic probation officers
Probation officers with unrealistic expectations for probationers made working relationships with therapists difficult: . . . there’s some POs that are more stringent and a client will miss a group and they never miss a group so maybe I won’t tell the PO cuz I’m—I don’t want them to call. I feel like they’re always looking for . . . something wrong or to arrest em on, kinda like what you talked about before, um, with some type of—allowing them to make mistakes, sometimes they’re gonna make mistakes and obviously it’s all from reoffending to, like, a friend showed them porn on their phone, sometimes they [probation officers] overreact and then some it’s like they’re not involved at all. (Therapist)
Another therapist expressed frustration with a probation officer who refused to be flexible with a low-risk offender and stated, “They [offender] have to be on house arrest for 3 years and, you know, they are [a] very low-risk client, so I think that’s really hard to work with.”
Conflict between therapy and probation goals
The quality of the working relationship between probation officers and therapists often deteriorated when treatment and supervision goals competed: . . . I think, ah, for me personally, the early part of treatment seems to be the most important . . . learning about their . . . sex offence cycle, learning about the, uh, early events of life that created some of this movement, trauma, . . . the education social, intimate part of how they’re developed and how they maybe aren’t developed . . . they [probation officers] wanna focus on one thing but we’re trying to do something else so, you know, it kinda ties our hands to how we wanna move with a client . . . (Therapist)
Additional Probation Officer and Therapist Struggles Implementing the Containment Model
Probation officers and therapists discussed the resources they needed to adequately implement a variety of containment components—components discussed earlier as major components of the model. They identified problems in five areas: caseloads, use of GPS technology, informed and consistent public policies and agency protocols, consistent funding for therapy, and actuarial risk assessment.
High Caseloads
Implementation of the containment model requires that probation officers work intensively with probationers and collaborate with the multidisciplinary team. Probation officers complained that high caseloads made it difficult to devote sufficient time to intensive community supervision and collaboration: But the problem happens . . . when the caseloads go so high you don’t have time to sit and say let me take a look at your cell phone or let me search that computer or let me go through, let me do a thorough walk-through of the house because you don’t have time to do that. You gotta meet your compliance standards, it’s on to the next case. So once the caseloads go above 25 or 30, I think sometimes things get lost in the crack because you don’t have that time. (Probation officer)
Technology
Probation officers identified problems with GPS monitoring in terms of the amount of time necessary to monitor probationers, as well as which probationers were sentenced to electronic surveillance. Two probation officers discussed their frustration with GPS monitoring or implementation: . . . I’m spending at least an 8-hour day just doing GPS, which is just running the GPS because they don’t have the money. They have GPS on these clients but they haven’t added enough personnel to actually monitor the GPS and watch where they’re going. Watching the computer, which I think is crazy; I’d rather have real eyes on the problem in the field . . . (Probation officer) One of my issues is just that the way the law divides or separates the GPS. We have guys that are on probation for a computer crime that happened at their home and yet they’re sentenced to GPS. And to me it’s just, almost a waste for probation to supervise that person when the crime was committed at their home . . . (Probation officer)
Informed and Consistent Agency Protocols and Public Policies
Probation officers and therapists identified frustrations with inconsistencies, changes in policy, and the politics involved in the supervision of offenders. One therapist expressed frustration with the frequent reorganization of probation caseloads: . . . about every few months, they reorganize the probation caseloads based on where people are relocating and they do it by zip code, so one day a guy will be with a PO, mister A . . . and the next day he goes to probation officer B . . . (Therapist)
Another therapist expressed frustration with the variability between probation officers in their interpretation and enforcement of supervision rules and suggested the need for investment in the development of consistent policies and procedures: . . . “oh, I just spent two weeks in Vegas.” “good for you, how’d you do that?” “Oh, my PO let me go.” So you get just crazy variations. I think the biggest problem for the department . . . they need to invest some dollars in some policy and procedure, um, they say they have it, I’ve never seen it. Cuz the problem is the variability is really tremendous from PO to PO. Just depends on their own personal style . . . (Therapist)
A probation officer noted their frustration with criteria for classifying high and low-risk offenders for community notification: I would definitely like to just, revamp that [community notification], if that could be changed where they were really notifying on people that are the true deviant sex offenders . . . the 19 year old guy that’s on the caseload for having sex with a 16 year old, they’re notified their whole life, they can’t find housing, and then, the person . . . who’s 40 years old and has 200 victims, he’s not notified on. His neighbors have no idea. (Probation officer)
Finally, a probation officer expressed frustration with an administrative decision to modify the containment model, “The containment model went away as far as we were concerned when the [new] administration came in.”
Consistent Funding for Treatment
Probation officers and therapists expressed frustration with the lack of dedicated funding for sex offender treatment. One officer expressed frustration for mandating offenders who cannot afford to pay for their treatment: Some of my initial observation is being in treatment, the state should have mandated that the treatment be free. I got a problem where cases that can’t pay, they’re dropping out of the treatment. What do I do, what is the next step? (Probation officer)
Another therapist complained that it was easier to get treatment for a chemical dependency problem than for sexual offending risk: . . . it’s easier for us to get a person into a program who has no money if he also smokes marijuana . . . the city then will pay for their sex offender counseling because we’re putting them in one program that’s gonna do both [sex offender and drug treatment]. (Therapist)
Helpful Actuarial Assessments
Probation officers and therapists expressed general dissatisfaction with the assessment instruments and process used to measure and track risk, progress, and recidivism potential. One probation officer reflected on the variability of assessments: . . . an assessment’s only as good as the person doing it, so, I’ve seen, we go off the Static-99R. Two of them in one file that are different from each other, and that’s very concerning . . . (Probation officer)
One therapist expressed frustration with the imperfect science of assessments: I’m not satisfied, because it’s not, it’s not a real science . . . it’s not black and white, nothing is, and there’s a lot of risk pressure on them, on us, to be “successful.” . . . you learn how to do the best you can and be as satisfied as you can . . . (Therapist)
Another therapist would like to see a more rigorous process developed for determining graduation criteria: Is the guy being terminated for problematic behaviors? That one I’m pretty ok with the process and the methods that I think we employ to make those kinda decisions. I struggle with the other decision, though, about releasing the guys from treatment because they’re doing well, but they’re still gonna be on probation. And I struggle with that for this reason—because I don’t think we collectively have ever sat around and really come up with, by and large a consensus, of what they should look like and what that should consist of and how we go about making that decision so that we’re collectively making that decision in a way that’s fairly consistent. (Therapist)
Discussion
Our study examined the collaborative working relationships between probation officers and therapists who supervise and treat adult sexual offenders in two large metropolitan areas in the United States: Maricopa County, Arizona and the NYC Department of Probation. Probation officers and therapists in our study identified important characteristics that they believed promoted effective collaborative relationships, as well as high quality supervision and treatment within the containment model framework implemented in their respective sites. The containment model of supervision is anchored in the ability of probation and treatment professionals to work effectively in collaboration and in partnership with each other (English, 2003; English et al., 2016).
Summary of Study Findings
Positive collaborative relationships
Overall, both probation officers and therapists were quite positive about their collaborative partnership. The majority of probation officers and therapists agreed that regular, accurate, and timely communication between the probation officer and the treating therapist—preferably face-to-face—frequently occurred and was essential for providing good supervision and treatment to probationers. These findings confirm previous research on the importance of “frequent and substantive two-way communication between treatment providers and POs about information that will assist in reducing an offender’s risk to the community” (McGrath et al., 2002, p. 62) and communication “as a pivotal concept and tool in developing positive inter-organizational relationships between community corrections and community treatment providers” (Monico et al., 2016, p. 497). Probation officers and therapists also emphasized how much they valued each other’s roles—including appreciation for the fact that they believed that both probation officers and therapists usually operated within the established parameters of their professional responsibilities. The fact that probation officers and therapists were so positive about their relationships in spite of well-established differences between probation officer and therapist professional orientations cannot be taken for granted; probation officers and therapists have different professional perspectives that unless well-coordinated could present challenges to implementing collaborative approaches such as the containment model. When working together collaboratively, probation officers and therapists often need to set aside their preconceived ways of operating and integrate their different professional perspectives into their practices and relationships with their sex offender clients (D’Amora & Burns-Smith, 1999). Our findings suggest that the majority of the probation officers and therapists successfully navigated these differing professional perspectives and developed healthy collaborations.
Barriers to collaboration
Not all probation officers and therapists who took part in our focus groups perceived their working relationships across discipline as fully successful. These participants perceived barriers to collaboration due to infrequent, late, poor quality, and inaccurate communication; conflicts between the goals of therapy and probation; probation officers who did not value treatment or who were too tough, unrealistic, and confrontational; and therapists who were inexperienced, lacked sex offender-specific training, did not value probation, or were not confrontational enough. Day (2014) found that law enforcement officers held more negative attitudes about sex offenders than did therapists. D’Amora and Burns-Smith (1999) noted that probation officers were more likely to be focused on maintaining order and control over offender behaviors; in contrast, therapists were likely to be working to engage sexual offenders in increasing their autonomy in the change process. These differences in professional focus may still exist even though the attitudes of probation officers involved in the rehabilitation of sex offenders tended to be more positive than those not involved in rehabilitation (police and correctional officers; Day, 2014; Ware, Galouzis, Hart, & Allen, 2012). Clear and Latessa (1993) noted that probation officers sometimes struggled with competing “enforcer” and “social worker” roles within themselves. Some of the probation officers and therapists in our study described troubled collaborative relationships partially due, we believe, to these differing professional perspectives. Such problems are not unique to the sexual offender field and reflect the common tension between the contrasting professional perspectives of law enforcement and treatment professionals in corrections and forensic mental health (Day, 2014; Hogue, 1993). Clear and Latessa (1993) described how conflict can exist between the probation officer’s “law enforcer” role, which places emphasis on enforcing the legal requirements of supervision, and the therapist’s “social worker” role, which places emphasis on assisting the offender with community adjustment and reintegration. Interestingly, A. B. Wilson and Draine (2006) observed greater collaboration between corrections and mental health when mental health services for offenders were led by corrections.
As the present results indicate, however, it is quite possible for these roles to be mutually enhancing. Many productive relationships, such as boss, coach, and parent, work best when they effectively combine support and control. The potential problems we observed arose when the enforcement and support roles were poorly coordinated, or when one partner was not playing their expected role.
Additional Struggles Implementing Aspects of the Containment Model
Probation officers and therapists discussed five deficits in resources and policies that interfered with adequate implementation of the containment model: (a) high probation officer caseload size, (b) complexity and time intensiveness of GPS technology and monitoring, (c) inconsistent probation agency protocols/policies characterized by frequent changes in policy and the destabilizing effects of politics and politicians, (d) lack of a consistent funding source to pay for mandated sex offender treatment, and (e) inconsistent and absent actuarial risk assessment. Political influences are a major factor that affects these deficits. Sex offender management policies are guided by emotion and not informed by empirical data (Miner, 2007). Empirically driven sex offender management policies would adhere to Risk-Needs-Responsivity principles (Andrews & Bonta, 2006) and would involve interventions that have demonstrated impact on public safety. Adhering to the risk principle would mean directing intensive interventions for high risk offenders and providing less intensive interventions to those at low risk—this would allow the limited resources available for sex offender management to be more effectively targeted. Containment approaches and long-term mandated sex offender treatment would be limited to the few sexual offenders whose actuarially measured risk is highest; few resources would be directed toward serving the majority of sexual offenders—whose risk of reoffense is quite low (Hanson, Thornton, Helmus, & Babchishin, 2016). Resource-intensive interventions, such as GPS monitoring, would only be used if they have been shown to be effective in maximizing public safety. To date, there is little evidence that GPS monitoring affects rates of reoffending in sexual offenders (Payne & DeMichele, 2011)—thus, the staff resources allocated to such monitoring might be better spent in other activities.
Strategies for Reinforcing the Positive and Addressing the Negative Factors
Although our research showed that collaborative relationships between probation officers and treatment providers generally seemed strong, these good working relationships should not be taken for granted. Systems or protocols requiring regular communication and collaboration, as well as practices that help probation officers and therapists gain a better understanding and appreciation of each other’s roles, are essential to maintain and build strong relationships. Research examining “linkages” through both formal and informal means was an evidence-based method used to foster collaboration between probation officers and chemical dependency treatment providers; one successful “linkage” was the use of regular cross-trainings where probation officers and treatment providers attended drug court-related trainings together (Welsh et al., 2016). Additional “linkages” that could be borrowed from the drug court system and applied to the supervision of sex offenders include the following: using case management services, resource sharing, joint assessment of clients, joint planning of client service goals, mutual sensitivity to concerns of the other agency or program, sharing of information about clients, and staff meetings (Wenzel, Turner, & Ridgely, 2004). These linkages would require a system-wide commitment from probation departments, including allocating necessary resources, and require identifying barriers to collaboration, and a commitment to resolving them. To address inter-agency collaboration, systemic changes in how probation and treatment agencies communicate, coordinate treatment, and make supervision decisions may be needed.
Other suggested linkages arising more directly from our research include providing additional opportunities for probation officers and therapists to meet and run into each other—perhaps by housing probation officers and therapists closer together—even in the same building or in buildings near each other. Probation officers could regularly participate in quarterly or yearly reviews and regularly scheduled containment sessions. When conflicts arise, protocols could be in place to resolve conflicts and monitor collaboration. Finally, using common, dynamic assessment instrument(s) that require probation officers and therapists to jointly rate or score together may provide a regular structure and reason for probation officers and treatment providers to meet together regularly and collaborate. The Sex Offender Intervention and Treatment Protocol (SOTIPS) is an example of one such tool developed to track supervision and treatment progress over time; the recommended scoring protocol suggests that probation officers and treatment providers score SOTIPS together (Lasher et al., 2015; McGrath et al., 2012).
Limitations
Krueger and Casey (2015) described the optimal size of noncommercial focus groups as five to eight participants and 10 to 12 participants for marketing focus groups. The Maricopa County probation officer (n = 18) focus group was considerably larger than optimal, which may have made it more difficult for Maricopa County participants to express their thoughts. To manage the higher numbers, we cut back on some of our questions and probes to give participants more time to answer questions and attempted to direct our questions to quieter probation officers. The space provided for the NYC focus groups had distracting environmental conditions (e.g., fan noise and a lack of air ventilation/air conditioning) that may have interfered with participants’ responses, including making it more difficult for participants and facilitators to hear each other, as well as affecting transcription quality.
As with any study involving a small sample of volunteers, it is unlikely that the participants were a random sample of any predefined population. Although we were fairly confident of the themes identified, it is possible that there were voices who did not find expression, either because they were systematically excluded (by themselves or others) or simply by chance. Consequently, it is unlikely that our results reflect the opinions and experiences of all therapists who treat sex offenders in either location.
Another limitation is that some lines of questioning did not yield any interpretable findings. Specifically, respondents were unable to answer questions concerning the specific criteria they used to determine when offenders were ready to graduate treatment or to have reduced supervision requirements. This should not be entirely surprising because the scientific evidence on these topics is relatively weak and local policy is rarely specific about what constitutes an acceptable risk (see Hanson et al., 2017).
Implications for Research
A central tenet of the containment model is the importance of good communication between the various team members working with sexual offenders, especially probation officers and treatment providers. It is clear from our research that the probation officers and therapists working in Maricopa County and NYC valued high quality and frequent communication and interaction, as well as the importance of respecting and valuing each others’ role. One obvious question is whether these findings would be replicated in other probation jurisdictions. Another question is whether the quality and quantity of communication and interaction between probation officers and therapists affects important supervision and treatment outcomes, such as reduced offending and enhanced functioning. Does the quality of their working relationships influence their sex offender clients’ adjustment in the community? Residential and employment stability? Social relationships? Successful completion of probation? Conversely, are these working relationships related to offender motivation for treatment and their degree of preexisting prosocial orientation? It is quite likely, for example, that certain probationers are experts at splitting teams, and that dysfunctional teams do little to promote effective rehabilitation. Research could focus on finding the optimal level, type, and quality of probation officer and therapist communication and contact, as well as on the best methods for helping probation officers and therapists gain a better understanding and appreciation of each other’s roles. Such research would help substantiate the theorized importance of these key components of the containment model.
Conclusion
Our research informs the supervision and therapy system conditions necessary for effective collaboration between probation officers and therapists. In particular, rules and procedures should seem reasonable, not arbitrary and rigid, and should fit into a coherent, coordinated vision. Effective collaboration between therapists and probation officers is possible, but it is fragile and should not be taken for granted. Those involved in these collaborations, and their administrators, need to invest in building, monitoring, and maintaining these professional relationships. These collaborations work best when there are few barriers to informal communication, competent practitioners, and respect for, and understanding of, each other’s roles.
Footnotes
Appendix
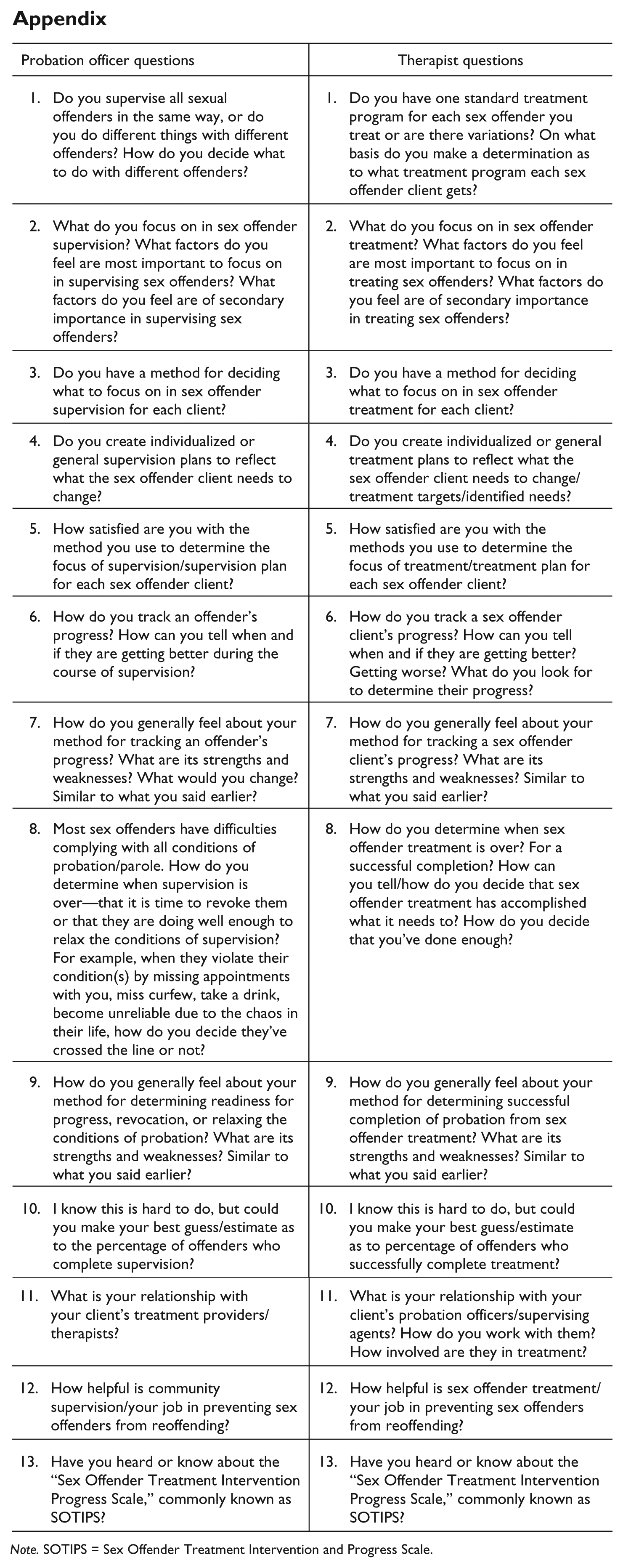
| Probation officer questions | Therapist questions |
|---|---|
| 1. Do you supervise all sexual offenders in the same way, or do you do different things with different offenders? How do you decide what to do with different offenders? | 1. Do you have one standard treatment program for each sex offender you treat or are there variations? On what basis do you make a determination as to what treatment program each sex offender client gets? |
| 2. What do you focus on in sex offender supervision? What factors do you feel are most important to focus on in supervising sex offenders? What factors do you feel are of secondary importance in supervising sex offenders? | 2. What do you focus on in sex offender treatment? What factors do you feel are most important to focus on in treating sex offenders? What factors do you feel are of secondary importance in treating sex offenders? |
| 3. Do you have a method for deciding what to focus on in sex offender supervision for each client? | 3. Do you have a method for deciding what to focus on in sex offender treatment for each client? |
| 4. Do you create individualized or general supervision plans to reflect what the sex offender client needs to change? | 4. Do you create individualized or general treatment plans to reflect what the sex offender client needs to change/treatment targets/identified needs? |
| 5. How satisfied are you with the method you use to determine the focus of supervision/supervision plan for each sex offender client? | 5. How satisfied are you with the methods you use to determine the focus of treatment/treatment plan for each sex offender client? |
| 6. How do you track an offender’s progress? How can you tell when and if they are getting better during the course of supervision? | 6. How do you track a sex offender client’s progress? How can you tell when and if they are getting better? Getting worse? What do you look for to determine their progress? |
| 7. How do you generally feel about your method for tracking an offender’s progress? What are its strengths and weaknesses? What would you change? Similar to what you said earlier? | 7. How do you generally feel about your method for tracking a sex offender client’s progress? What are its strengths and weaknesses? Similar to what you said earlier? |
| 8. Most sex offenders have difficulties complying with all conditions of probation/parole. How do you determine when supervision is over—that it is time to revoke them or that they are doing well enough to relax the conditions of supervision? For example, when they violate their condition(s) by missing appointments with you, miss curfew, take a drink, become unreliable due to the chaos in their life, how do you decide they’ve crossed the line or not? | 8. How do you determine when sex offender treatment is over? For a successful completion? How can you tell/how do you decide that sex offender treatment has accomplished what it needs to? How do you decide that you’ve done enough? |
| 9. How do you generally feel about your method for determining readiness for progress, revocation, or relaxing the conditions of probation? What are its strengths and weaknesses? Similar to what you said earlier? | 9. How do you generally feel about your method for determining successful completion of probation from sex offender treatment? What are its strengths and weaknesses? Similar to what you said earlier? |
| 10. I know this is hard to do, but could you make your best guess/estimate as to the percentage of offenders who complete supervision? | 10. I know this is hard to do, but could you make your best guess/estimate as to percentage of offenders who successfully complete treatment? |
| 11. What is your relationship with your client’s treatment providers/therapists? | 11. What is your relationship with your client’s probation officers/supervising agents? How do you work with them? How involved are they in treatment? |
| 12. How helpful is community supervision/your job in preventing sex offenders from reoffending? | 12. How helpful is sex offender treatment/your job in preventing sex offenders from reoffending? |
| 13. Have you heard or know about the “Sex Offender Treatment Intervention Progress Scale,” commonly known as SOTIPS? | 13. Have you heard or know about the “Sex Offender Treatment Intervention Progress Scale,” commonly known as SOTIPS? |
Note. SOTIPS = Sex Offender Treatment Intervention and Progress Scale.
Acknowledgements
The authors thank the New York City and Maricopa County probation departments, particularly the probation officers and therapists who participated in the focus groups. They also thank Donna Vittori, Jennifer Ferguson, Regan Daly of the Maricopa County Probation Department, and John Corrigan and Mike Caputo of New York City Department of Probation who assisted with the coordination of the data collection. Much appreciation to David Thornton for his assistance with focus group questions and guidance throughout the process. Thanks to the University of Minnesota Department of Family Medicine and Community Health, especially Heidi Fall for her editing and formatting, Rebekah Pratt for her assistance with qualitative analysis and NVivo training, Sarah Loeschke for coding and organization, and Cathy Strobel-Ayers for coordination. Finally, thanks to the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking (SMART) and the National Institute of Justice (NIJ) for funding and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Award No. 2013-AW-BX-0153, awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusion or recommendations expressed in this publication are those of the authors and do not necessarily reflect those of the Department of Justice.