
Abstract
This article describes an evaluation of the effects of an early version (1991-2001) of Rockwood’s prison-based Cognitive Behavioral Therapy/Risk–Needs–Responsivity (CBT/RNR) sex offender program that had emerging elements of a strength-based approach. This program was implemented under contract to Correctional Service of Canada (CSC) and continued to evolve in response to emerging evidence until it closed in 2013. Thus, the program as evaluated here did not involve a fixed approach as did the comparison CSC program (hereafter referred to as SOTP). Long-term reoffense data, from Rockwood’s program (n = 579), were compared with SOTP (n = 625) and with a group of untreated men (n = 107) sentenced for sex offenses. A modified brief actuarial risk scale (BARS-M) was used to control for baseline risk among the three groups, along with additional controls for age at release, victim type, and individual differences in the length of long-term follow-up period. Both treatment groups displayed lower rates of both sexual and violent reoffending when compared with the no-treatment offenders. Overall, the Rockwood program generated the lowest recidivism rates. The results demonstrate that prison-based sex offense–specific treatment can be effective. We discuss the strengths and limitations of the current design through the Collaborative Outcome Data Committee’s guidelines.
This report describes a comparative evaluation of two Canadian prison-based sex offender treatment programs. Both programs were operated under the jurisdiction of the Correctional Service of Canada (CSC), which is responsible for all offenders who have been sentenced to periods of incarceration of 2 years or more. Despite the obvious advantages of the rigor of random controlled trials, it was not possible to conduct such an evaluation under the operating circumstances of CSC, the aim of which was to treat all men federally sentenced for sex offenses. We made the best attempt we could under these restrictions.
There have been repeated attempts over the years to evaluate the effectiveness of sex offender treatment, the results of which have been incorporated into a series of meta-analyses, most of which have been summarized by Corabian, Dennett, and Harstall (2011) and by Lösel and Schmucker (2014). Although some meta-analyses have found no evidence of reductions in reoffending among treated men (Dennis et al., 2012; Långström et al., 2013), others have reported small, but meaningful benefits (Hanson et al., 2002; Lösel & Schmucker, 2005; Schmucker & Lösel, 2015). In these latter studies, it was shown that 10% to 12% of treated cases reoffended over the follow-up period, while among the untreated clients, reoffense rates ranged from 13% to 18%. This low base rate of recidivism among untreated men convicted for sex offenses places limits on the capacity to discern benefits derived from treatment.
Schmucker and Lösel (2015) concluded from their meta-analysis that overall community-based treatments showed more consistently positive results than did prison-based programs. Nine prison-based programs were included in their analysis. However, there have been positive reports from CSC prison programs that were not included in their study (Looman, Abracen, & Nicholaichuk, 2000; Nicholaichuk, Gordon, Gu, & Wong, 2000; Olver, Nicholaichuk, Gu, & Wong, 2013) and from a Minnesota prison (Duwe & Goldman, 2009). On the contrary, Abracen, Looman, Ferguson, Harkins, and Mailloux (2011) found no benefits for their prison program.
Issues in Outcome Evaluations
There are several methodological issues that may influence the outcome of sex offender treatment. Some of these features were made explicit by Olver et al. (2013), so we will not repeat most of them but we will note the relevance of two potentially important factors: matching of the groups and the nature of the outcome variable.
Matching should, as far as possible, result in the relative equivalence of the groups under consideration. This is typically done by showing that the groups are matched on established risk factors. However, this presents a problem in the present evaluation. Empirically based risk assessment tools were not available until near the end of the current period of the operation of the three groups and so participants were not scored on currently known risk factors. Furthermore, there is insufficient information available to allow us to complete scoring on these established risks. We will, therefore, employ a simpler risk scale that we have used in the past in retrospective evaluations to a satisfactory effect (Olver et al., 2013).
The second relevant issue concerns the nature of the indicator of long-term outcome. In studies of this kind, the usual index has been derived from official records of recidivism. This indicator, of course, suffers from the fact that official records do not reveal unreported crimes although there is no way of presently knowing the extent of these undetected offenses. Also, the simple identification of a crime reveals nothing about its seriousness, which may lie along continua of violence and harm. As reoffenders entering CSC prisons must have received sentences of 2 or more years, this, in the context of Canadian sentencing practices, provides a proximal indication of seriousness. We can, therefore, assume that the reoffense rates we will derive from official records indicate significantly problematic crimes. One advantage to our attempt to identify reoffending derives from the fact that the basis upon which we will rely is Canada’s official record of crimes (Canadian Police Information Center, CPIC). This information source is comprehensive as all charges and convictions for all crimes identified by police across the country must, by law, be entered into this system. The CPIC system is used in the present study to identify recidivists.
A Paradigm for Treatment
Although at least some of the meta-analyses reveal encouraging findings, it is also clear that not all programs entering these evaluations generated positive results. Perhaps this was due to the failure of many programs to adhere to principles that are known to underpin effective treatment with offenders of all types. We will, therefore, describe the features of a paradigm that embodies these principles.
The most soundly based approach for potentially effective treatment of offenders, including those who have sexually offended, involves the integration of the principles of the Risk–Needs–Responsivity (RNR) model (Andrews & Bonta, 2010) with a Cognitive Behavioral Therapy (CBT) approach (Meichenbaum, 1977). The RNR model was derived from Andrews’s earlier reports (Andrews, Bonta, & Hoge, 1990; Andrews, Zinger, et al., 1990) demonstrating that treatment for all types of correctional clients was more likely to be effective when (a) greater allocation of resources was devoted to the highest risk cases with correspondingly less resources offered to moderate- and low-risk clients, (b) treatment focused primarily on established dynamic risks (i.e., criminogenic factors), and (c) treatment was delivered in a rewarding, respectful, warm, and empathic manner that was matched to each individual’s unique personal characteristics and learning capacity. These three RNR principles were later shown to be equally relevant to sex offender treatment (Hanson, Bourgon, Helmus, & Hodgson, 2009).
In addition to these observations, Andrews, Zinger, et al. (1990) noted that treatment appeared to be most effective when it was modeled on a CBT approach. However, there is substantial diversity in CBT programs for sex offense clients. For example, while Schmucker and Lösel (2015) noted that among psychological approaches, the ones that were shown to be most effective were described as CBT, they also observed considerable diversity in the elements of these programs making it difficult to clearly define such an approach. Similar diversity among so-called CBT approaches is evident in the details of the treatments entering the Safer Society’s surveys of North American sex offender programs (see, for example, McGrath, Cumming, Burchard, Zeoli, & Ellerby, 2010) and in two books describing CBT approaches with correctional clients (W. L. Marshall, Fernandez, Hudson, & Ward, 1998; Tafrate & Mitchell, 2014). The Safer Society’s surveys also reveal widespread inconsistencies in adherence to the RNR principles. We cannot, therefore, make inferences about a program’s content simply on the basis of its description as CBT/RNR, although it remains true that when properly implemented this model rests on sound empirical bases.
In addition to the general acceptance of the CBT/RNR approach, there has been a recent move to fashion treatment for men who have sexually offended after the strength-based approach (SBA) derived from the positive psychology movement (Linley & Joseph, 2004; Snyder & Lopez, 2005). SBA programs for sex offense clients have implemented the suggestions of Seligman (1998) that treatment should build strengths to compensate for the deficits evident in clients with all manner of psychological disorders. Reviews of these attempts to implement SBAs with these men did not identify any evaluations testifying to their benefits (W. L. Marshall, Marshall, & Olver, 2017). This, however, is partly to be expected since, for the most part, these are recent innovations.
There are four features that appear to distinguish SBAs from non-SBA approaches (W. L. Marshall & Marshall, in press). First, treatment should be offered to prospective clients as a way to build strengths that will offset their current deficits and provide them with a better more fulfilling prosocial life. In the case of clients who have sexually offended this would also include an indication that this approach to treatment should reduce the risk of reoffending. Second, treatment should initially assist clients in identifying their current strengths (e.g., a competent and reliable worker, a good friend, family supports, skills involved in leisure pursuits). Next, treatment targets (including criminogenic factors) should be addressed by providing skills (cognitive and behavioral) that are aimed at offsetting these deficits. Finally, during the latter stages of treatment, clients should be assisted in identifying strategies for the continued development of the skills acquired in treatment, which are to be implemented once the offender has been released from prison or discharged from a community program. It is, therefore, possible to explicitly incorporate the elements of an SBA while retaining the CBT/RNR features; the latter of which acknowledges strengths, but could do more to elucidate them. This is what constitutes the current version of Rockwood’s program (W. L. Marshall, Marshall, Serran, & O’Brien, 2011), although the earlier version evaluated here was not as comprehensively derived from an SBA model and is thus described as having strength-based elements.
Method
Aim
The primary intention of the present study was to determine the relative effectiveness of two prison-based sex offender treatment programs: CSC’s Standard sex offender treatment program (SOTP) operated in several federal prisons across Canada and Rockwood’s program conducted in a single federal Canadian prison. We also added a comparison with a group of untreated men convicted for sex offenses again collected from federal prisons across the country. Per Simmons, Nelson, and Simonsohn’s (2012) 21-word solution, “We report how we determined our sample size, all data exclusions (if any), all manipulations, and all measures in the study” (para. 6).
Readers need to know that two of the authors of this report (L.E.M. and W.L.M.) were among the therapists who delivered Rockwood’s program and that W.L.M. was the Director and, therefore, primarily responsible for the design and conduct of the program. Obviously, both these authors anticipated a positive outcome for Rockwood. To partly protect the study from such potential influences, two research assistants (RAs), with no knowledge of sex offender treatment or of Rockwood’s implementation or outcome expectations/hopes, were hired to extract long-term recidivism data from CPIC records. These two RAs conducted their searches 6 months apart without any knowledge of each other’s findings. The results identified by these two RAs were identical and served as the index of effectiveness for Rockwood’s program. Although this will perhaps not allay all fears of contamination, we hope it does serve to reduce these concerns.
The Programs
As noted, the two treatment programs compared in the present evaluation are SOTP, which is described in detail in a CSC (1996) document and an early version of Rockwood’s program (approximately described in W. L. Marshall, Anderson, & Fernandez, 1999). During the period of implementation evaluated in this report (1991-2001), SOTP remained stable while Rockwood continued to evolve based on clinical experience and emerging evidence. Therapists implementing SOTP were provided with a manual and were supervised by a senior clinician. Rockwood’s therapists were guided by both weekly supervisory sessions and by early versions of an evolving manual that in its most recent form is available at www.rockwoodpsyc.com .
Each program adopted a version of the CBT/RNR model according to the best evidence available at the time except that during the period of the operation under evaluation, evidence was not available indicating the required criminogenic factors. The targets of the two programs were those factors that had been shown to differentiate men who had committed sex offenses from other men; some of these targets were later shown to be criminogenic while others were not. Both programs attempted to follow current research and addressed almost the same issues: eliminating deviant sexual interests, overcoming cognitive distortions, raising victim awareness, instilling empathy for victims, increasing social and intimacy competence, education on the elements that maximize sexual satisfaction in intimate adult relationships, and the development of post-release plans. On this latter issue, the strategies differed. SOTP’s approach was aimed at developing relapse prevention plans according to accepted practices of the time, while Rockwood’s program emphasized post-release plans that were aimed at the continued enhancement and extension of the strengths acquired during treatment.
SOTP operated within a variety of federal prisons that varied in the level of security. High-risk clients received treatment in mostly maximum-security prisons, medium-risk clients were treated in medium security institutions, and low-risk offenders entered treatment in either so-called “soft” medium or minimum security prisons.
Bath Institution, when Rockwood’s program was initially implemented (1991), operated as minimum security (i.e., no peripheral fence), but within 4 years, its status was elevated to medium after a peripheral double razor-wired fence was erected. Immediately following this change, the population at Bath grew rapidly from 100 to more than 400 with men sentenced for sex offenses being approximately 40% of the total population. Not surprisingly, the level of risk among this group also increased. Furthermore, in the mid-1990s, Bath’s companion prison (Warkworth Institution), which housed medium- to high-risk sex offense clients, became unable to treat more than a limited number. As a result, many of these individuals were transferred to Bath for treatment, which additionally altered the distribution of risk levels in Rockwood’s program making the participants more similar to those in SOTP programs.
Potential Differences Between the Two Treatment Programs
There were several differences that may have influenced outcome. For instance, the data on SOTP, as mentioned, were drawn from differing prisons of differing security status, while all data on Rockwood were derived from the same prison. Also, throughout the 1990s, support for Rockwood’s program from the administration, case management, and prison officers at Bath was strong. It was clear that this support encouraged the dedication of the participants in Rockwood’s program. How true this was of the various prisons from which SOTP data were drawn is unclear. Perhaps, however, the most important differences likely to have influenced outcome concern the strength-based elements of Rockwood’s approach and the reliance by Rockwood on an open-ended group approach. SOTP implemented a closed group model and had no explicit strength-based elements.
As indicated in the introduction, during the period of Rockwood’s early operation, SBAs to treatment had not been articulated. However, many aspects of Rockwood’s approach anticipated the advent of SBAs. For example, treatment was offered as a way to not only reduce the likelihood of reoffending but also provide the strengths needed to have a better more fulfilling future. The early stages of treatment focused on the enhancement of a sense of self-efficacy by identifying the clients’ current strengths and by increasing self-esteem and training in coping skills. Criminogenic targets were conceptualized in terms of the absence of strengths rather than as deficits, and procedures were employed that aimed at increasing the skills necessary to overcome these deficits. Toward the end of treatment, participants were assisted in developing future plans aimed at the further enhancement of strengths such as education and work skills upgrading, the development and expansion of leisure pursuits, and involvement in social activities. Very limited relapse prevention plans were articulated as these were seen as contrary to the otherwise emphasis on strengths.
The deployment of an open group format in sex offender treatment has received limited attention. Ware, Mann, and Wakeling (2009) identified what they saw as the advantages of this approach but did not provide evidence on its value. L. E. Marshall, Marshall, Serran, and O’Brien (2008) demonstrated in a controlled study that an open approach generated higher levels of group cohesion than did a closed group format. This is important as Beech and Hamilton-Giachritsis (2005) have demonstrated that greater levels of cohesion lead to greater changes in the targets of treatment.
Open-ended group treatment, as implemented by Rockwood, involved the entry of a new participant when another client had completed all aspects of the program. Each client progressed through the same sequence of issues, and all members of the group were required to participate in all discussions including those focused on topics they may have already have dealt with. This meant that as each client progressed through the topics, he was in a position to offer advice or challenge other clients from a progressively more sophisticated point of view. Thus, by the time a client had completed the program, he would have repeatedly addressed each treatment target. These are conditions that are known to both strengthen and entrench learning and to provide long-term retention (O’Donohue, 1998; Spiegler & Guevremont, 1998).
Perhaps there were other aspects on which the two programs may have differed but these two seem to us the most likely to generate differential outcomes. The dose of treatment was similar across the two programs as was the average amount of time clients spent in each program. The minimum time each client spent in treatment at Rockwood was 4 months while the maximum was 8 months. This was approximately the same as the average time across CSC’s three-tiered programs (W. L. Marshall & Yates, 2005).
Two final factors that might have differentiated the two programs concern the rate of acceptance of the offer of treatment and the subsequent rate of withdrawals (dropouts) from the programs. These indices of the utility of sex offender treatment have been given far less attention than they should have because the meaning we can attach to treatment outcome is clearly compromised when refusal rates and dropout rates are high. A low number (3.8%) of those offered a place in Rockwood’s program refused to participate and of those who entered treatment, all but 4.2% completed all requirements. These rates are substantially better than has been reported in the literature to date (Browne, Foreman, & Middleton, 1998; Mann, Webster, Wakeling, & Keylock, 2013) and are lower than other CSC programs including Clearwater (12.8%; Olver & Wong, 2011), Warkworth (12.7%; Seto & Barbaree, 1999), and Kingston RTC (36.1%; Dickie, 2003). A report by Seager, Jellicoe, and Dhaliwal (2004) on these issues within a CSC sex offender program further indicated that 13% of those clients offered a place in treatment turned down the offer. Importantly, these refusers had subsequent reoffense rates (8 / 19 or 42%) that were far higher than those who completed treatment (3 / 81 or 4%). Clearly, these are important issues regarding the value of a treatment program. The present study employs an intent-to-treat design, incorporating all cases referred to Rockwood for services, both completers and noncompleters.
Participants
As noted earlier, all participants were federally incarcerated Canadian male sex offenders meaning they were all serving sentences of 2 or more years. The treated participants were derived from the Rockwood Sex Offenders’ program and from various SOTP programs operated by CSC. A group of untreated men federally sentenced for sex offenses was extracted from CSC archives.
A sample of 579 treated clients was extracted from Rockwood’s files and represented all sex offender referrals treated from the program’s commencement in early 1991 until the end of 2001, although, in some instances, the men remained in custody for some years still after participation in the program prior to community release. We chose this period because it allowed a long-term outcome although the program continued until early 2013 when the contract was canceled.
An original CSC sample (N = 2,401) appeared in two studies (Nicholaichuk, Olver, Gu, & Wong, 2014; Olver et al., 2013) and was gathered from institutions across the country. The original project was commissioned by CSC in 2004 and was a large-scale sex offender outcome study in which three consecutive cohorts who had reached warrant expiry in the fiscal years between 1997-1998, 1998-1999, and 1999-2000 were followed up in the community. Most of the men were offered treatment opportunities that some offenders declined. From this large sample, Olver et al. extracted samples (treated and untreated) that were used for comparative purposes in both the Olver et al. report and in the present study. No new data were collected on this sample for the purposes of the current evaluation. These groups were then followed up for an average of 11.7 years after release into the community.
The treated group (SOTP, n = 625) had been provided with CSC’s formal program as described previously and contrasted with the Rockwood Program. The program assignment field in the Offender Management System (OMS; CSC’s national electronic offender database) identified cases as having completed sex offender treatment or not having completed sex offender treatment, for the SOTP and untreated groups, respectively. This information was available from this OMS field for only about one third of the original sample of 2,401 men, hence, the current smaller numbers for the SOTP and untreated groups. For the SOTP group, program intensity was not available, thus further underscoring the importance of imposing some control for sexual violence risk. Given that high-intensity programs at the time were most frequently offered in designated regional treatment centers, it is anticipated that most of the SOTP participants completed a moderate intensity program (4-5 months, 10 hr per week).
As noted, the untreated clients (n = 107) were similarly identified as having not completed sex offender treatment; however, the reason for the untreated status was not provided. The untreated group was a mix of (a) treatment refusers, (b) men in a prison where treatment was not available, (c) men whose sentence was too short for them to complete a program by the time they were allocated to a prison, and (d) men whose sentence had expired before they could enter treatment. Of note, many of the men in the untreated group successfully completed other CSC services such as anger management and cognitive skills, and there was no significant association between having completed sex offender treatment or not and having completed either of these two programs (Olver et al., 2013).
Brief Actuarial Risk Scale (BARS)
The BARS was developed by Olver et al. (2013) to create a static scale to control for baseline risk status when comparing treated and untreated groups of men convicted for sex offenses, given that no sexual violence risk tool had yet been developed at the time of the program in the 1990s that would have been otherwise routinely administered. The scale consists of six binary items: any prior sex offense conviction (i.e., occurring prior to the index sex offense), any male sex offense victim, any unrelated sex offense victim, never married/single (according to demographic record), age below 35 years at time of most recent release, and four or more prior sentences for any offense. The item coding rules were informed by, but are not identical to, the STATIC-99R (see Harris, Phenix, Hanson, & Thornton, 2003; Helmus, Thornton, Hanson, & Babchishin, 2012). Only information from official criminal charges and convictions was utilized to score the BARS items. Possible scores range from 0 to 6 and are grouped into three risk categories: low (0-1), medium (2-3), and high (4-6). Olver et al. demonstrated that the BARS scores had good predictive accuracy for both sexual (area under the curve [AUC] = .71; 95% confidence interval [CI] = [.66, .76]) and violent (AUC = .69; 95% CI = [.65, .73]) recidivism. This is comparable in magnitude to other sex offender actuarial risk measures (Hanson & Morton-Bourgon, 2009). All participants in the present study were scored on the BARS. In the present study, the same sentencing date information was not available when coding the BARS for the Rockwood sample. As such, a modified five-item version of the BARS (BARS-Modified or BARS-M) was used with the sentencing dates item removed and the prior sexual offense item weighted by two points, given that it was the strongest predictor across samples to provide a better control of risk. The heavier weighting of sexual offense history is consistent with other actuarial sexual violence risk assessment tools (e.g., Harris et al., 2003; Helmus et al., 2012).
Procedure
Risk and treatment variables
Olver et al. (2013) and Nicholaichuk et al. (2014) provide details of the data collection procedures relevant to risk and reoffending for the SOTP and no-treatment groups. Briefly, all the relevant data for these two groups were collected in 2004 across the three fiscal years referenced previously (1997-2000). Only men who had completed the SOTP were entered into that group. A detailed coding protocol was developed at the Regional Psychiatric Centre (RPC) in Saskatoon, Canada, to rate criminal history, treatment participation, offender and victim demographics, and sentencing information. To code the study variables, two trained RAs independently accessed and coded the data from OMS from relevant fields, as well as from CPIC, which lists all charges and convictions for all offenders whether or not they received a prison sentence. The data were then entered into an electronic spreadsheet. The original BARS was scored on the SOTP and no-treatment samples through electronically recoding the variables into binary format as per the scoring rules outlined previously, and then summed to generate a scale total.
Two further independent RAs were hired by Rockwood to independently complete matching data for the Rockwood clients. However, in the latter cases, the BARS-M was scored by the senior author of this current article. BARS-M scores for each group are shown in Table 1 along with age at release and years of follow-up.
Group Comparisons on BARS-M Scores and Other Relevant Risk Variables.
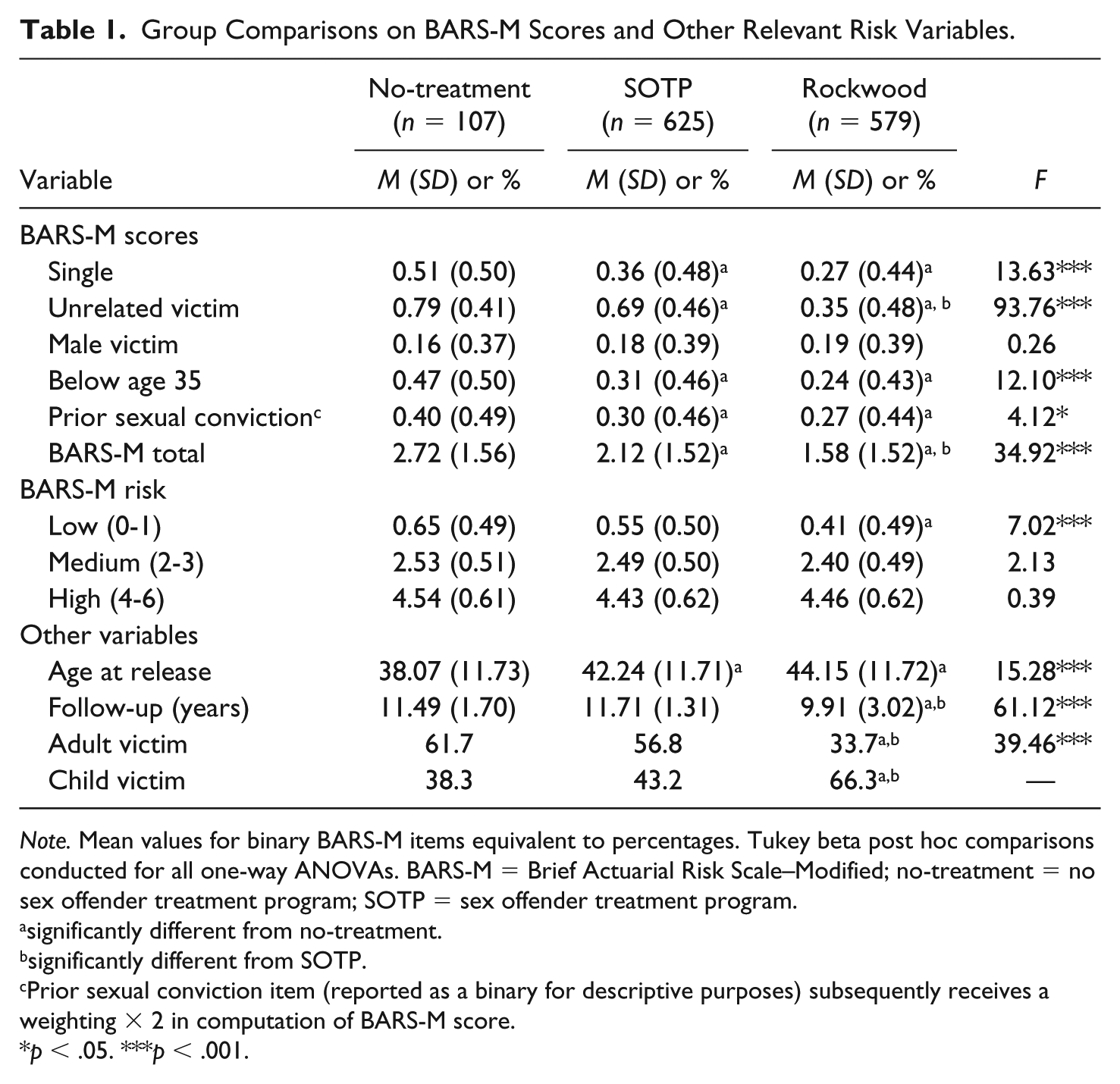
Note. Mean values for binary BARS-M items equivalent to percentages. Tukey beta post hoc comparisons conducted for all one-way ANOVAs. BARS-M = Brief Actuarial Risk Scale–Modified; no-treatment = no sex offender treatment program; SOTP = sex offender treatment program.
significantly different from no-treatment.
significantly different from SOTP.
Prior sexual conviction item (reported as a binary for descriptive purposes) subsequently receives a weighting × 2 in computation of BARS-M score.
p < .05. ***p < .001.
Recidivism data
These data for each group were coded from CPIC records by the respective Rockwood RAs and by a further independent RA at the RPC, who was blind to treatment status. For the SOTP and no-treatment groups, the relevant information was collected in 2009, whereas for the Rockwood clients, the data were extracted in 2012. The primary outcome criteria of interest were sexual and violent recidivism. Sexual recidivism was defined as any new criminal code conviction for an offense that was sexual in nature (e.g., sexual assault, sexual interference). For offenses that were adjudicated as nonsexual violent in nature, when it could be determined that the offense was sexually motivated (e.g., a sexual homicide adjudicated as murder), such offenses were coded as sexual offenses. Typically, this could only be done for new convictions resulting in a federal sentence as OMS documents, such as the criminal profile report (which provides a synopsis of the details of the criminal offenses for a given case), would be available on file. Violent recidivism was operationalized as any new conviction for offenses that involved actual, attempted, or threatened physical harm, including sexual offenses. For each group, and for each offense type, recidivism variables were coded by the RAs as either 0 or 1 (i.e., yes or no). Post-release sentencing dates served as the time marker for survival analyses. Time spent on remand (where applicable) for any new charges (including, but not limited to, the new sexual and violent offenses) was taken into consideration to adjust the time at risk for survival analyses.
Collaborative Outcome Data Committee (CODC) rating
The study authors and one of the anonymous reviewers rated the 21 criteria (CODC, 2007) on the present study to examine methodological strengths and weaknesses and potential for various forms of bias. (All three anonymous reviewers were highly familiar with the CODC criteria and offered comments on the study’s standing with respect to some of the criteria.) Given that three conditions are being compared, three separate sets of CODC ratings would be required to be completed. Given that the no-treatment group composition presents the plausible possibility for a priori group differences from the two treatment conditions (i.e., greater proportion of dropouts and treatment refusers, who tend to be higher risk), under the CODC guidelines, this comparison would likely be scored as REJECT. Thus, CODC ratings are presented in full for the Rockwood-SOTP comparison only in the appendix. Per the CODC criteria, this would be classified as “other concurrent comparisons design” as this entails a comparison between two different treatment programs in which the stream of referrals did not purposively target one program or the other. The Rockwood-SOTP comparison was assigned a global rating by the study authors of GOOD: “High confidence that the study has no more than a small amount of bias (intermediate rating). Reasonable efforts have been made to address threats to validity, but much remains unknown” (p. 86). Calibration of the overall rating was informed by the CODC ratings of other similar studies (Hanson et al., 2009) and the ratings provided by anonymous reviewers on earlier versions of the current article. We provide a synopsis of relevant strengths and limitations per the CODC criteria in the “Discussion” section.
Planned Analyses
The overarching intent of the analyses was to systematically examine treatment outcome for the Rockwood program relative to the SOTP and no-treatment groups, while controlling for risk levels and length of follow-up. Although the Rockwood-SOTP comparisons are the most rigorous basis for comparison, examination relative to a no-treatment condition was still viewed as informative, the concerns regarding potential threats to validity notwithstanding. In addition, the SOTP and no-treatment comparisons from Olver et al. (2013) are reported for comparative purposes with the Rockwood sample. Five sets of analyses were executed.
First, we conducted group comparisons on the BARS-M item scores and total scores, as well as on additional variables of interest, for descriptive purposes and to identify group differences on variables that might impact outcome.
Second, we examined the predictive accuracy of the BARS-M scores for sexual and violent recidivism using a fixed 8-year follow-up given that this was the maximum period that could be used while retaining most (over 95%) of the earlier samples. Nearly two thirds (65%) of the Rockwood sample had been at risk for 8 years and this was the mean of that group’s follow-up. These analyses were meant to establish that the BARS-M scores could serve as an appropriate control for baseline risk when making comparisons among the three conditions. Predictive accuracy was examined through AUC analyses in which values of .56, .64, and .71 correspond to low, medium, and large effect sizes, respectively (Rice & Harris, 2005).
Third, we conducted group comparisons among the three conditions, examining rates of sexual and violent recidivism at 8-year fixed, as well as overall unfixed, follow-ups. Given the influence of extreme base rates on effect size magnitude for some metrics, such as correlation (see Babchishin & Helmus, 2016, for a review), odds ratios (ORs) were computed as a preferred measure of effect size to examine group differences within low-, medium-, and high-risk bands on the BARS as follows: (nrecidTreat / nnonrecidTreat )/(nrecidControl / nnonrecidControl ) . Group differences, irrespective of risk level, were also examined for comparison purposes. OR values below 1.0 represent the odds of decreased recidivism in the intervention condition relative to the comparison condition, while values above 1.0 would indicate the odds of increased recidivism, and values of 1.0 indicate no difference between the conditions. These analyses were meant to demonstrate the extent to which participation in the Rockwood program, in contrast to participation in SOTP, and compared with no-treatment, was associated with reductions in sexual and violent recidivism within each risk category.
Fourth, we conducted Cox regression survival analyses using indicator contrasts to compare rates of sexual and violent recidivism between the three groups while controlling for age at release, sex offender type, and BARS-M score (minus the age at release item) and individual differences in follow-up time. These analyses are most sensitive given that they employ a continuous measure of risk while controlling for follow-up time. In these analyses, the Rockwood group was used as the reference category and compared with SOTP and no-treatment groups, on each recidivism outcome, followed by the BARS-M score (minus age), age at release, and sexual offense victim profile to control for risk. Finally, we conducted logistic regression analyses using fixed 8-year follow-ups to examine group differences controlling for these same covariates. This was done to generate an OR after controlling for risk and follow-up time, which could be used as an overall summary metric for the impact of the Rockwood Program relative to SOTP in reducing sexual and violent recidivism.
Results
Group Comparisons
Descriptive statistics for the three groups are presented in Table 1. The no-treatment men tended to be a somewhat higher risk group on average, having higher values on four of the five BARS-M items as well as a higher total score compared with the two treatment groups. The no-treatment group was also younger than the other groups and had significantly longer follow-ups than the Rockwood participants. Importantly, when BARS-M was stratified into low-, medium-, and high-risk bands, there were no significant differences between the three groups, with the exception of the low-risk men from Rockwood who had lower overall BARS scores than the two comparison groups; the initial difference between the Rockwood and SOTP groups in BARS-M score was small-moderate in magnitude (d = .355). The Rockwood sample had a significantly larger number of men who had only child victims, while the SOTP and no-treatment groups had significantly greater proportions of men with adult victims. Of note, across all samples, men with adult victims, compared with those who had abused children exclusively, had significantly higher rates of sexual recidivism overall (12.8% vs. 7.5%, respectively) and at 8-year fixed follow-up (12.9% vs. 6.0%, respectively), as well as violent recidivism overall (34.1% vs. 15.1%, respectively) and at 8-year fixed follow-up (33.3% vs. 13.6%, respectively).
Table 2 reports the predictive accuracy statistics (AUC values) for BARS-M total scores in terms of the prediction of sexual and violent recidivism employing a fixed 8-year follow-up and also without limiting the follow-up. The BARS-M scores significantly predicted all recidivism outcomes within each of the three groups. Broadly, the BARS-M showed moderate predictive accuracy for violent recidivism and low-moderate to high predictive accuracy for sexual recidivism. In the Rockwood treatment sample, BARS-M scores tended to show higher predictive accuracy that was closer in magnitude to the other two groups when fixed follow-ups were employed.
Predictive Accuracy of the BARS-M for Sexual and Violent Recidivism Among Treatment Groups and Overall.

Note. BARS-M = Brief Actuarial Risk Scale–Modified; no-treatment = no sex offender treatment program; SOTP = sex offender treatment program; AUC = area under the curve; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Treatment Outcome Analyses
Risk-stratified group comparisons
The first set of treatment outcome analyses examined rates of sexual and violent recidivism employing both 8-year fixed and overall unfixed follow-ups among the three treatment conditions stratified by BARS-M risk band (Table 3). The Rockwood program had lower rates of sexual and violent recidivism than did either the no-treatment or the SOTP group at both moderate and high levels of risk but not for the low-risk category. In terms of sexual reoffending, there were no differences across the three low-risk groups. The same was true for violent reoffending except that low-risk Rockwood clients fared better than the no-treatment offenders. The SOTP group had significantly lower 8-year sexual reoffense rates than did the no-treatment group when the analyses focused on the high-risk cases. As anticipated, all group comparisons on rates of sexual recidivism but one (p = .054) attained significance when the risk bands were collapsed into a single total category.
Rockwood, SOTP, and No-Treatment Group Comparisons on Sexual and Violent Recidivism Outcomes Over 8-Years Fixed and Overall Follow-Ups.

Note. Significant test statistics and effect sizes in bold font. SOTP = sex offender treatment program; no-treatment = no sex offender treatment program; OR = odds ratio; CI = confidence interval.
p = .054. *p < .05. **p < .01. ***p < .001.
Examination of OR values for 8-year and overall follow-ups, respectively, revealed that relative to the no-treatment group, participants in Rockwood’s program showed a 76% to 81% decrease in the odds of sexual recidivism among high-risk cases and 65% to 75% decrease for the medium-risk band. Differences also emerged in comparison between Rockwood participants and those in the SOTP group. Specifically, the Rockwood program had lower rates of sexual reoffending among both moderate-risk (OR = .28-.35) and high-risk (OR = .34-.61) participants, although the difference was not significant for high-risk men at the 8-year fixed follow-up. In terms of violent reoffending, both moderate- and high-risk men from the Rockwood program had significantly lower rates than did the SOTP group. Finally, as might be expected from the known rates of reoffending among low-risk sex offenders, there were no differences in outcome for these clients across the three groups except for significantly lower rates of violent recidivism between Rockwood men and those in the no-treatment group. All comparisons on rates of violent recidivism attained significance when the risk bands were collapsed.
Cox regression survival analyses
These analyses were most sensitive in that they examined rates of sexual and violent recidivism over time between the three groups, while controlling for continuous BARS-M scores (minus age), age at release, and sex offense victim profile (any adult victim vs. exclusively child victim). As is shown in Table 4, indicator contrasts demonstrated that men completing the Rockwood program had significantly lower rates of sexual and violent reoffending after controlling for the three sets of covariates. The BARS-M scores and age at release also incrementally predicted each outcome, indicating that additional risk variance predicted observed differences in rates of sexual and violent reoffending after controlling for group membership; sex offense victim profile did not uniquely predict sexual recidivism outcome when controlling for treatment status or other risk-relevant covariates. Scrutiny of the hazard ratios (eB) demonstrate that after controlling for risk-relevant covariates, there is a more than twofold increase in the hazard of sexual (eB = 2.43) or violent (eB = 2.70) recidivism for men in the no-treatment condition relative to those completing the Rockwood program. Moreover, a near twofold increase in the hazard of sexual (eB = 1.74) and violent (eB = 1.73) recidivism was observed for men attending the SOTP program relative to those completing treatment with Rockwood after controlling for risk-relevant covariates.
Cox and Logistic Regression Analyses: Examination of Rates of Sexual and Violent Recidivism for Rockwood Program Versus SOTP Versus No-Treatment Controlling for Risk-Relevant Covariates and Time at Risk.

Note. Group ns for Cox regression survival analysis model: Rockwood = 576, SOTP = 625, no-treatment = 107; logistic regression model: Rockwood = 376, SOTP = 616, no-treatment = 104. SOTP = sex offender treatment program; no-treatment = no sex offender treatment program; CI = confidence interval; BARS-M = Brief Actuarial Risk Scale–Modified. Significant p-values in bold font.
Logistic regression analyses
The same covariates employed in the Cox regression were used to conduct logistic regression analyses to examine group differences in 8-year rates of sexual and violent recidivism. As seen in Table 4, SOTP demonstrated a twofold increase in the odds of either recidivism outcome relative to Rockwood and the no-treatment condition, a threefold increase. The generation of ORs is practical in this regard and would represent a summary effect size for the purpose of the CODC ratings comparing SOTP with Rockwood after controlling for risk-relevant covariates. In this case, taking the inverse of the OR (i.e., 1/OR) reports the findings in terms of reductions in recidivism associated with the Rockwood Program relative to SOTP and would generate ORs = .493 (95% CI = [.27, .89]) and .483 (95% CI = [.33, .71]) for 8-year sexual and violent recidivism, respectively. Per Hanson et al. (2009), “When an odds ratio was coded that controlled for other variables, the odds ratio and the unadjusted recidivism rate for the comparison group were used to calculate the adjusted recidivism rate for the treatment group” (p. 873). In this case, 66 / 550 (OR for SOTP) × .493 (adjusted treatment effect OR) = .0592, the adjusted OR for Rockwood for 8-year sexual recidivism. The Rockwood OR frequencies can be generated, and hence, rates of recidivism computed from the sample n (376 for the logistic regression in Table 4) and the OR value: nnonrecid = 376 / (1 + .0592) = 354.98 or 355; nrecid = 376 − 355 = 21. This amounts to a 21/376 = 5.6% adjusted 8-year sexual recidivism rate for Rockwood relative to the unadjusted 8-year rate of 10.7% for SOTP. For violent recidivism, 163 / 453 × .483 = .174, which using the formulae above translates to a 14.8% adjusted 8-year rate of general violent recidivism for Rockwood relative to the unadjusted 8-year rate of 26.5% for SOTP.
Discussion
Brief Summary of Results
When we controlled for risk through stratified group comparisons, the Rockwood clients displayed significantly lower sexual and violent reoffense rates than did the no-treatment group over the 8-year as well as overall follow-up periods. These differences were most marked among the medium- and high-risk subgroups. Reoffense rates among Rockwood’s moderate-risk clients were also lower overall than the corresponding rates in the SOTP group. The SOTP clients also showed lower rates of reoffending than did men in the no-treatment group with these results being most evident in the highest risk groups. It appears, therefore, that both a standardized program implemented across various prisons and a specialized program operating in a single prison can both be effective in reducing the risk posed by sex offenders once they are released to the community. If these results are accepted, then they may be seen to partly offset the reservations expressed by Schmucker and Lösel (2015) concerning the effectiveness of prison-based programs, although further meta-analytic inquiry would be warranted.
Strengths and Limitations
There are several strengths and limitations to the present study that merit discussion. In the Hanson et al.’s (2009) treatment outcome meta-analysis, only two of the five studies coded as GOOD according to the CODC criteria were RCTs (Borduin, Schaeffer, & Heiblum, 2009; Marques, Wiederanders, Day, Nelson, & van Ommeren, 2005). Hanson, Broom, and Stephenson’s (2004) examination of CSC’s sex offender community treatment services (n = 403) relative to an untreated CSC sex offender comparison group (n = 321) released prior to the availability of such services served as a model methodologically for the present study. Hanson et al.’s (2004) was classified as an “other concurrent comparison group” and one of the few other studies rated as GOOD in Hanson et al. (2009). An eight-item static scale that predicted sexual recidivism (AUC = .63) was constructed to control for group differences, which were examined controlling for risk via Cox regression survival analysis and through employing fixed 7-year follow-ups. Although the treatment condition scored significantly higher than the control on the static scale (d = .206), there were no significant group differences on any recidivism outcomes. Hanson et al. (2009) further coded the community program as having not adhered to any RNR principles, and thus this would seem to be a GOOD evaluation of what would otherwise appear to have been a weak treatment service.
In terms of the present study, per the CODC criteria, the Rockwood and SOTP represent established sex offender programs, with manuals, articulated treatment goals, delivered by trained licensed mental health professionals, in turn supervised by a psychologist or other licensed professional. The SOTP served as a conservative comparison for Rockwood given that it only contained treatment completers, while Rockwood nonetheless had low rates of attrition and utilized an intent-to-treat design to examine recidivism outcomes. Treatment and recidivism variables were coded by independent raters, who were blind to either one or the other. Large treatment conditions (n > 300) were compared, utilizing high-quality uniform outcome data with 8-year fixed follow-ups or statistical methods to adjust for follow-up (e.g., survival analysis). A brief static actuarial risk scale was further developed, per Hanson et al. (2004), and rated to control for differences in baseline risk between the groups. Importantly, the SOTP group was higher risk on the BARS-M and had a higher proportion of men with adult victims, who were also higher risk than men with child victims, compared with the Rockwood Program. Risk-stratified comparisons were used to examine group differences controlling for BARS-M score, as was Cox regression survival analysis with the additional risk-relevant covariates of age at release and sex offense victim profile included in the final model.
There are important limitations, however. In particular, a measure of dynamic risk-relevant long-term vulnerabilities was not available, and thus, it is possible that other unmeasured risk factors could have contributed to observed group differences in rates of sexual and violent recidivism. That said, it is important to bear in mind that none of the GOOD studies included in Hanson et al. (2009) controlled for dynamic risk, and only two out of the five with this classification (Hanson et al., 2004; Marques et al., 2005) even included a static actuarial measure (developed within the study) to control for risk. A further potential limitation is that Indigenous ancestry was not available for the entire sample, thus restricting the possibility of examining treatment effects as a function of culture/ancestry. Nor was it possible to discern differential effects arising from the different treatment locations within the SOTP sample. Unfortunately, we did not have interrater reliability data for the coding of case file information, which tends to be less straightforward than coding recidivism data from CPIC, and thus, we cannot be certain whether some variables were coded less reliably than others and whether this may have impacted study findings. Some readers may disagree with our judgment here and view the study as closer to a “WEAK” design. Even so, we believe it is possible to draw conclusions, if somewhat tentatively, from such a design. We note the difficulties of evaluating the majority of programs that were, and still are, operating without the luxury of funding or support to be able to implement a rigorous prospective design. Indeed, the most important limitation to the present report concerns our inability to be able to implement an RCT designed study. Thus, in addition to the various factors mentioned in the “Method” section that either differentiated the two treatment programs, or on which the programs were matched, there may have been different features of the clients in each group that were not apparent but which would have been controlled for in a randomized design.
Implications
In so far as we can make inferences based on the present results, the findings offer encouragement to those implementing, or proposing the implementation of, sex offender treatment within prison settings. Convicted sex offenders housed in prisons are typically among the most at risk to reoffend and cause harm to innocent victims. Thus, any signs of encouragement to those providing treatment in these settings is to be welcomed.
Rockwood’s approach to the offer of treatment was to emphasize the benefits for building a better life. This feature was combined with the early focus in treatment on identifying and building on clients’ strengths. These two features are components of the definition of an SBA (W. L. Marshall & Marshall, in press). Given that this combination resulted in both low refusal rates and high completion rates, it may be that a singular advantage of SBAs is to maximize entry and commitment to treatment, without which outcome evaluations would be pointless. It is worth further noting that other critical therapist and nonspecific therapeutic elements, such as therapist warmth, empathy, and responsiveness, the importance of which has been documented extensively in the literature (W. L. Marshall et al., 2003) could have contributed to low attrition rates and positive outcomes.
We look forward to seeing more evaluations of prison-based sex offender programs, particularly those studies that are able to conduct an RCT while maintaining high standards of treatment implementation. We also hope that the now extensive evidence supporting the application of a well-defined CBT/RNR model will result in a more widespread careful adherence to these principles among sex offender treatment programs.
Footnotes
Appendix
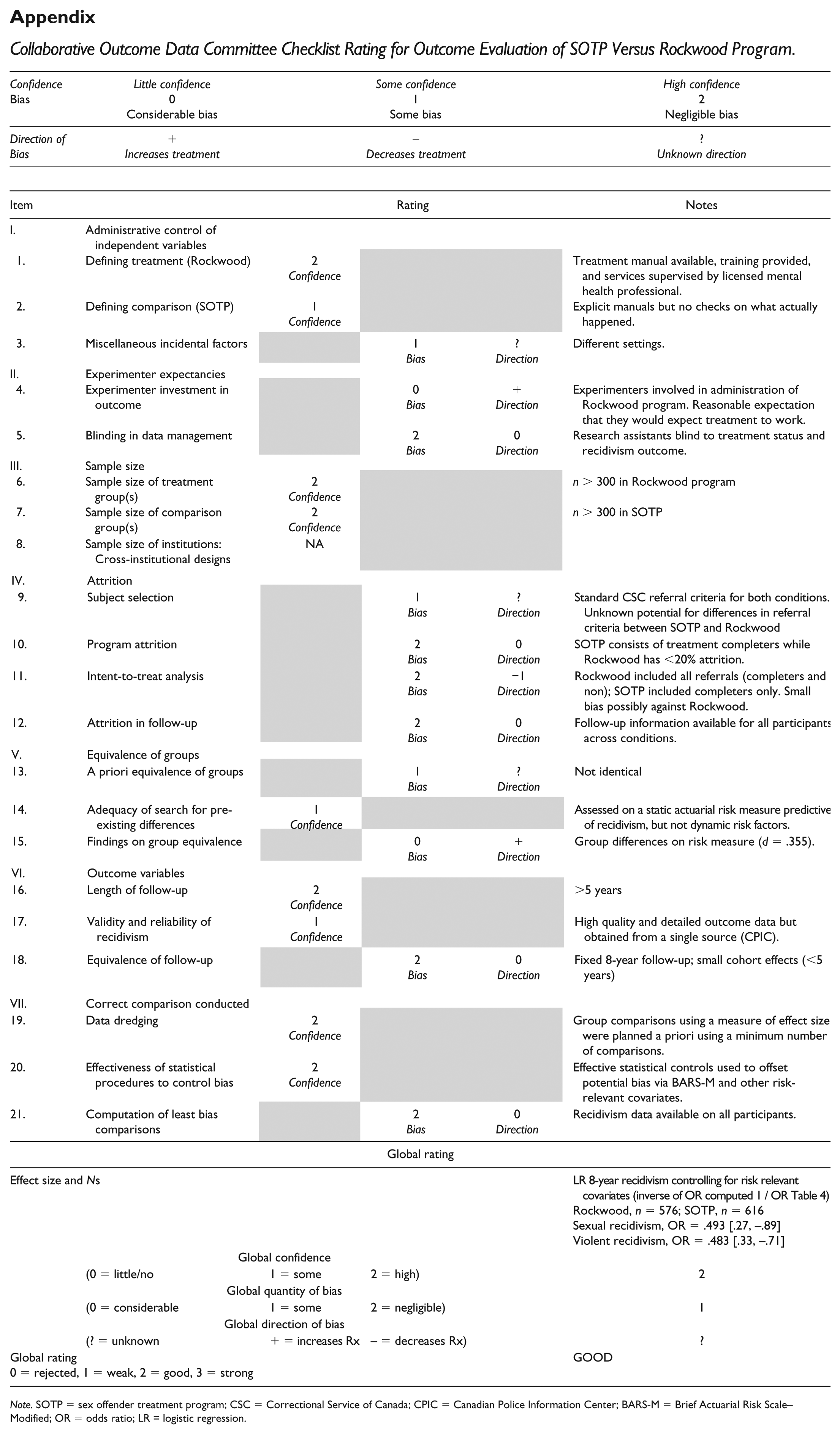
| Confidence |
Little confidence |
Some confidence |
High confidence |
||
|---|---|---|---|---|---|
| Direction of Bias | + |
– |
? |
||
| Item | Rating | Notes | |||
| I. | Administrative control of independent variables | ||||
| 1. | Defining treatment (Rockwood) | 2 |
Treatment manual available, training provided, and services supervised by licensed mental health professional. | ||
| 2. | Defining comparison (SOTP) | 1 |
Explicit manuals but no checks on what actually happened. | ||
| 3. | Miscellaneous incidental factors | 1 |
? |
Different settings. | |
| II. | Experimenter expectancies | ||||
| 4. | Experimenter investment in outcome | 0 |
+ |
Experimenters involved in administration of Rockwood program. Reasonable expectation that they would expect treatment to work. | |
| 5. | Blinding in data management | 2 |
0 |
Research assistants blind to treatment status and recidivism outcome. | |
| III. | Sample size | ||||
| 6. | Sample size of treatment group(s) | 2 |
n > 300 in Rockwood program | ||
| 7. | Sample size of comparison group(s) | 2 |
n > 300 in SOTP | ||
| 8. | Sample size of institutions: Cross-institutional designs | NA | |||
| Item | Rating | Notes | |||
| IV. | Attrition | ||||
| 9. | Subject selection | 1 |
? |
Standard CSC referral criteria for both conditions. Unknown potential for differences in referral criteria between SOTP and Rockwood | |
| 10. | Program attrition | 2 |
0 |
SOTP consists of treatment completers while Rockwood has <20% attrition. | |
| 11. | Intent-to-treat analysis | 2 |
−1 |
Rockwood included all referrals (completers and non); SOTP included completers only. Small bias possibly against Rockwood. | |
| 12. | Attrition in follow-up | 2 |
0 |
Follow-up information available for all participants across conditions. | |
| V. | Equivalence of groups | ||||
| 13. | A priori equivalence of groups | 1 |
? |
Not identical | |
| 14. | Adequacy of search for pre-existing differences | 1 |
Assessed on a static actuarial risk measure predictive of recidivism, but not dynamic risk factors. | ||
| 15. | Findings on group equivalence | 0 |
+ |
Group differences on risk measure (d = .355). | |
| VI. | Outcome variables | ||||
| 16. | Length of follow-up | 2 |
>5 years | ||
| 17. | Validity and reliability of recidivism | 1 |
High quality and detailed outcome data but obtained from a single source (CPIC). | ||
| 18. | Equivalence of follow-up | 2 |
0 |
Fixed 8-year follow-up; small cohort effects (<5 years) | |
| Item | Rating | Notes | |||
| VII. | Correct comparison conducted | ||||
| 19. | Data dredging | 2 |
Group comparisons using a measure of effect size were planned a priori using a minimum number of comparisons. | ||
| 20. | Effectiveness of statistical procedures to control bias | 2 |
Effective statistical controls used to offset potential bias via BARS-M and other risk-relevant covariates. | ||
| 21. | Computation of least bias comparisons | 2 |
0 |
Recidivism data available on all participants. | |
| Global rating | |||||
| Effect size and Ns | LR 8-year recidivism controlling for risk relevant covariates (inverse of OR computed 1 / OR Table 4) |
||||
| Global confidence | |||||
| (0 = little/no | 1 = some | 2 = high) | 2 | ||
| Global quantity of bias | |||||
| (0 = considerable | 1 = some | 2 = negligible) | 1 | ||
| Global direction of bias | |||||
| (? = unknown | + = increases Rx | – = decreases Rx) | ? | ||
| Global rating |
GOOD | ||||
Note. SOTP = sex offender treatment program; CSC = Correctional Service of Canada; CPIC = Canadian Police Information Center; BARS-M = Brief Actuarial Risk Scale–Modified; OR = odds ratio; LR = logistic regression.
Authors’ Note
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results. The authors acknowledge the therapists during the 1991-2001 period who contributed to the Rockwood Program through running treatment groups, who in addition to William L. Marshall and Liam E. Marshall, included Dana Anderson, Franca Cortoni, Yolanda Fernandez, and Geris Serran. The authors also thank Richard Coupland, Laura Garratt, and Brenda Maire through the Regional Psychiatric Centre, and Stephanie Humphries and Allana Lukacz through the Rockwood Program, for their assistance with data collection. The views, opinions, and conclusions are those of the authors and do not necessarily represent those of the University of Saskatchewan, Correctional Service of Canada, or Waypoint Centre for Mental Health.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: William L. Marshall and Liam E. Marshall were developers of, and service providers for, the Rockwood Program.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.