
Abstract
This study seeks to extend research evaluating tools to assess the disclosure of sexually abusive behavior. The subjects were 239 male youth (ages 10–20 years) who were court-ordered to participate in a community-based collaborative intervention for sexual offending that includes outpatient and probationary services. All youth participated in an interview to capture referral incident details about admission, responsibility, empathy, and remorse at intake, during intervention, and at discharge. Intake, treatment, discharge, and recidivism measures were also collected from multiple sources. Latent class analysis identified three classes based on the intake interview: Empathetic Admitters (22%), Unempathetic Admitters (38%), and Unempathetic Deniers (40%). Significant class differences were found on intake (e.g., use of physical force, caregiver denial of youth responsibility), treatment (e.g., any sanctions/violations), and discharge measures (e.g., successful treatment, probation officer ratings), but not in recidivism rates. The findings extend efforts to identify and target different disclosure patterns whose clinical monitoring may support a comprehensive intervention.
Introduction
Defining and Understanding Offense Denial Dimensions
Understanding the prevalence, patterns, impact, and management of individuals, including children and adolescents, who deny or minimize their role in sexually abusive behavior is important for practice and research (see Malin et al., 2014; Rasmussen, 2013; Ryan & Otonichar, 2016). There does not seem to be a single or an established definition of denial in the general sexual offense literature. Most conceptualizations emphasize the need to define denial using multiple dimensions (e.g., commitment, fantasy, planning, harm, blame; Happel & Auffrey, 1995; Salter, 1988) rather than simply whether one does or does not admit to committing the offense (Nunes et al., 2007; O’Donohue & Letourneau, 1993) . Indeed, a comprehensive review by Levenson (2011) outlines several aspects of denial that have been used to define it beyond the simple refutation or minimization of the facts (e.g., victim impact, assignment of blame, severity, use of force, or threats not to tell). One perspective emphasized the importance of taking responsibility for offending behavior and the disclosure of events which match the official/victim’s account of the offense (Ware & Mann, 2012). Others have taken similar approaches to define denial based on varying degrees of disclosure in relation to the offense (e.g., its commission, seriousness, chronicity, and impact; externalizing blame) and one’s need for treatment (Jung & Daniels, 2012; Rich, 2018). Thus, by denial most formulations suggest that a person minimizes several details described in a victim statement (e.g., omitting key details, denying a sexual motive, claiming contact was consensual, minimizing impact, blaming the victim), besides actual denial of any involvement in an incident (commitment).
In contrast to adults, there is limited empirical information on the prevalence and correlates of denial, and its relationship to recidivism in adolescents. One small study found that 70.3% of 63 adolescent males made a full disclosure at intake and the quality of the level of attachment to their caregivers was found to mediate the relationship between their level of childhood poly-victimization and extent of disclosure of illegal sexual behavior during psychotherapy (Harrelson et al., 2017). Some family correlates include telling lies, having family myths, and engaging in taboo behavior (Baker et al., 2003). In terms of recidivism, an early meta-analysis reported an inclusive relationship between denial and recidivism in adolescent samples (Lund, 2000) and another no differences in sexual recidivism rates for juveniles who engaged in sexual abuse than for other juvenile offenders (Mulder et al., 2019).
Regardless of how denial relates to clinical correlates and recidivism, it is important for clinical management to understand the meaning of disclosure (vs. denial) as an indicator of treatment amenability, a key treatment target, and/or a predictor of low recidivism (Barbaree & Cortoni, 1993; Winn, 1996). Practitioners recommend that key elements of disclosure be addressed during CBT or other interventions, such as providing details of the incident, taking responsibility, or showing victim empathy (Levenson, 2011). Indeed, males who have engaged in sexually abusive behavior have acknowledged the importance of targeting accepting responsibility, victim empathy, and relapse prevention (understanding motives, triggers) during group therapy (Levenson et al., 2009). Some have suggested that denial is a defense mechanism to help one cope with the thought of having engaged in sexually abusive behavior (Reicher, 2013) or the distressing emotions related to it (e.g., shame, guilt, threat to self-esteem, fear of consequences), so it may help to manage symptoms (Vanhoeck & Daele, 2011). Thus, denial may capture more subtle psychological influences than simply reflecting extreme distortions (“I didn’t do it.”), as well as the possibility that a juvenile may not have committed the sexually abusive behavior or may need more time to discuss it before disclosure.
Standardized Assessment of Offense Details
Assessing these and other elements or dimensions of denial requires sensitive and careful strategies to initially solicit and then discuss adolescents’ perspectives regarding a referral incident. Although many programs and research studies use an interview at intake, only a few descriptions of their questions and use in case conceptualization and treatment were available in the literature when we initiated our work on this topic more than 20 years ago (Becker, 1998; Brown & Kolko, 1998; Chaffin, 1999; Freeman-Longo, 1985). Given certain limitations in the literature at that time (e.g., inconsistent operationalization of denial, exclusion of categorical deniers from some analyses, lack of longitudinal outcomes for deniers on treatment response and recidivism), we sought to develop an assessment to ascertain various incident details that could be used to capture disclosure or denial. The tool provides probe questions to guide the interview and clear rating criteria. We sought to incorporate many of the key elements of denial noted earlier in a brief interview designed to capture a youth’s perspectives on these details over time to support therapeutic conversations about the incident and to guide research examining the role of this information on the course and outcome of treatment.
Since our early work, other tools have been developed. For example, the Comprehensive Inventory of Denial – Sex Offender Version (CID-SO) is composed of four sets of items that include denial of the offense, victim blame, limited guilt, and minimization of harm that have been studied mostly in adults (Jung & Daniels, 2012). For adolescents, the Juvenile Sex Offender Assessment Protocol II (J-SOAP-II; Prentky & Righthand, 2003) includes a dynamic intervention subscale that includes some similar items (e.g., accept responsibility, empathy, remorse/guilt). Both tools have some supportive psychometrics, but evaluation of outcomes is either unknown for the CID-SO (e.g., treatment status, recidivism) or has shown some inconsistencies for the J-SOAP-II (e.g., recidivism; see Schwartz-Mette et al., 2020). Given assessment and psychometric challenges and the need to further explore the construct of denial, this study seeks to extend research that evaluates the use of brief tools to assess reports of one’s involvement in and reactions to an incident of sexually abusive behavior. Specifically, we describe the clinical use of a semi-structured interview protocol to capture this information upon intake, during intervention, and at discharge.
The Potential for Latent Class Analysis
One challenge to drawing inferences about denial with adolescents who engage in sexually abusive behavior is the inter-individual heterogeneity of denial – both the nature and degree of denial varies substantially across individuals. When heterogeneity like this is present, traditional assumptions of between-person homogeneity and generalizability are largely inappropriate and may lead to not only imprecise estimates of group-level effects (Fisher et al., 2018) but also inaccurate inferences about within-person variation in between-person effects (Hamaker, 2012). Person-centered and person-specific approaches are valuable for understanding heterogeneity directly, through developing inferences about people using information leveraged across many variables (i.e., a “person-centered” approach) instead of inferences about variable(s) using information across individuals assumed to be homogeneous (i.e., a “variable-centered” approach). Yet, variable-centered approaches dominate the clinical science literature, including investigations of how degrees of admission/denial (e.g., complete refutation, minimization, full disclosure) may vary along with factors like demographics (e.g., IQ, age), behavioral base rates (e.g., taboo behavior within the family), and accurately forecast long-term outcomes (e.g., varying rates of recidivism, clinical symptoms, and treatment response). As this work signals variability in the way that denial operates across adolescents who engage in sexually abusive behavior, assumptions of homogeneity in prevailing variable-centered lines of research are likely to benefit from person-centered ones that characterize heterogeneity. Specifically, a person-centered approach is needed to determine how clustered patterns of responding across items in each person (i.e., response patterns across items querying level of admission, assumption of responsibility, victim blame and empathy may differentiate subtypes of individuals) that vary between-person can differentiate variation in risk factors and inform implementation science research on what is needed for who and at what time.
Limitations of the variable-centered approach could be addressed with novel application of person-centered approaches, like latent class analysis (LCA), that have specific benefits for detecting subtypes of individuals using complex, multivariate patterns (Schreiber, 2017). Mathematically, LCA estimation identifies between-person consistency in within-person reports across items/variables to draw inferences about subtypes of individuals rather than any specific variable. Application of LCA to the study of denial in adolescents who have engaged in sexually abusive behavior would be paramount for (1) classifying subtypes of youths who exhibit distinct patterns of denial and (2) testing whether some subtypes also exhibit distinct patterns of recidivism, clinical symptoms, and treatment response. LCA has been fruitfully applied across a few studies in this population to characterize subtypes of youth based on characteristics of their victims, the nature of their behavior, and the motivating intent along with the behavioral antecedents of the abuse (Brown, 2019; McCuish et al., 2015). Characterizing subgroups of those who engage in sexually abusive behaviors using person-centered analyses may be an important first step in advancing person-centered treatment via implementation research comparing approaches for personalizing treatment across heterogeneous subgroups.
One recent example of the value of subgrouping in terms of disclosure comes from a recent study by Frost et al. (2019) who used cluster analysis to identify different patterns of change over time using an innovative measure of engagement in group-based CBT for adults. Based on Disclosure Management Style (DMS), the measure captures how group members respond to the expectation to disclose key details about the sexually abusive behavior along two dimensions: openness (vs. being closed/reluctant) and self-directedness (vs. other-directed), which yields four disclosure orientations (i.e., Exploratory, Oppositional, Placatory, Evasive). The Exploratory orientation reflects the desired orientation as it is based on active collaboration and responsiveness to feedback. Clinicians rated each participant on these two dimensions at four timepoints during the 33-week group: baseline (week 4), offense behavior characterization (week 11), victim empathy (week 17), and post group re-assessment (weeks 30–36). Initial results of the measure support its basic psychometrics and a cluster analysis of the ratings obtained near intake and discharge yielded a solution reflecting three styles: 1) neutral to openness, 2) evasive to exploratory, and 3) placatory to oppositional. The measure helps to capture the heterogeneity found in their trajectories of change related to group engagement and to monitor treatment responsivity. It is worth noting that changes during treatment in openness and self-directedness were unrelated to one another and to sexual interests or to recidivism.
Study Aims
We examine three aims related to the use and preliminary evaluation of a semi-structured clinical interview to assess key elements of a youth’s perspective on an incident involving sexually abusive behavior. First, we identify the baseline rates of disclosure and descriptions of their incident details in a sample of youth referred for treatment of sexually abusive behavior. Second, we use a person-centered approach to evaluate patterns of inter-individual variation in disclosure (i.e., class membership using LCA) based on the pattern of responses to an interview at intake about the incident of sexually abusive behavior. Third, we examine the relationship between class membership and key baseline, treatment, discharge, and recidivism measures, including variables found to predict recidivism in the literature.
Methods
Program Participants
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. The participants included 239 male youths adjudicated or placed on a consent decree for a sexually abusive behavior and ordered by a Family Court judge to participate in an outpatient treatment program while being maintained in the community. This program is offered by the Services for Adolescent and Family Enrichment program (SAFE) at UPMC Western Psychiatric Hospital in collaboration with the Special Services Unit (SSU) of the Juvenile Probation Department affiliated with the Allegheny County Juvenile Court (hereafter the SAFE/SSU Program; Kolko et al., 2004). The sample was ascertained from April of 1998 (program inception) through February of 2013. The participants were all males (two females were excluded) with an average age of 15.9 (SD = 2.0; range 10.9–20.7); 29 youths (12%) were age 18 to 20 at intake but had committed the referral behavior prior to their 18th birthdays. Half of youths identified as non-Hispanic White (119/238 = 50.0%), with almost all the rest identifying as non-Hispanic Black (108/238 = 45.4%). Very few youths identified as Hispanic (4/238 = 1.7%). Few participants had a prior nonsexual (23/228 = 10.1%) or sexual (2/228 = 0.9%) adjudication. The sample includes cases who provided informed consent forms that were approved by the University of Pittsburgh Institutional Review Board.
Data on the nature of the youths’ sexually abusive behavior was based on initial case referral records submitted by the SSU probation office and included case background, a juvenile petition form (listing charges), juvenile post-hearing information, the police investigation, and the victim’s statement. Youths had an average of 1.2 victims each (range: 1–8) and a mode of one (190/229 = 83.0%); five cases that committed offenses involving child pornography could not be coded for the number of “contact” victims or any of the other variables describing victim characteristics. Victims’ ages ranged from 2 to 60 years; the median (based on youngest age victim in cases with multiple victims) was 9.0 years of age (IQR = 7.0). Most youths had only female victims (171/234 = 73.1%), with almost a quarter offending against only males (55/234 = 23.5%), and only 3.4% (8/234) offending against both females and males. Few youths offended against a stranger (9/234 = 3.8%), one quarter (61/234 = 26.1%) offended against a biological relative, and the remainder offended only against acquaintances or nonbiological relatives. Slightly more than one-half of the participants (123/233 = 52.8%) were given at least one mental health diagnosis upon intake, which were mostly attention deficit hyperactivity disorder (79/233 = 33.9%), oppositional defiant disorder (27/233 = 11.6%), and conduct disorder (21/233 = 9.0%). Overall, 40.3% (94/233) of youths had a disruptive behavior disorder. Other diagnoses were less common (7.3% had an anxiety disorder, 2.1% an affective disorder, and 1.7% a substance use disorder).
Program Orientation and Assessment Procedures
Judges mandated all youths to either institutional or community placement based on commonly used triage/risk assessment findings and dispositional policies (Righthand & Welch, 2001). Those youths who were not mandated to institutional placement were court-ordered to the outpatient SAFE/SSU program as a condition of their community probation or consent decree to address their abusive sexual behavior. Each youth and at least one caregiver were scheduled to participate in intake and discharge assessments as part of routine treatment. During the intake process, the two participants were invited to participate in a voluntary research protocol approved by the University of Pittsburgh Institutional Review Board. The completion of caregiver consent and youth assent (or only youth consent if age 18 or higher) forms was required for the use of all assessment data for research purposes. Participants received $20 each for completing each assessment.
Recidivism data were collected from official juvenile court records and from public adult court records (depending on age) at approximately one year, two years, and three years after discharge from the program. Participants in the program completed a wide range of measures (see Kolko et al., 2004), but only those used in this study are reviewed here. The sample sizes for some measures were lower because they were added later to the battery.
Sexual Offense Disclosure Assessment (SODA)
As part of the intake assessment, both the youth and caregiver were interviewed separately on items designed to ascertain key details about the adolescent’s involvement in and response to the referral incident that are often addressed during treatment. The items in the SODA were developed in 1999 to be consistent with early interview and treatment guidelines for use with adolescents who engage in sexually abusive behavior (Becker, 1998; Brown & Kolko, 1998; Chaffin, 1999; Freeman-Longo, 1985), and were similar to those in later assessment tools (e.g., Jung & Daniels, 2012; Prentky & Righthand, 2003). During the youth interview, the assessment clinician carefully discussed the referral incident in relation to the information available in the referral packet. After completing the interview, the assessment clinician rated all SODA items. Although refinements were made to some of the wording and definitions of the item anchors over a more than 15-year period, the program manager reviewed the assessment materials and ratings to provide a second set of eyes for reviewing and confirming the original ratings. As part of the program’s efforts to monitor treatment response, the youth’s treatment clinician conducted follow-up interviews on the SODA between six weeks and three months later (“earlier in treatment”) to allow for time to teach key CBT skills and then at six months (“later in treatment”). A fourth interview was conducted at discharge with someone other than the treatment clinician. The SODA questions were designed to learn more from the client about what happened during the incident and how that information related to the youth’s behavior and intent over the course of the incident.
After the SODA interview, the assessor completed a 6-item Disclosure Impressions form. The assessor compared the responses obtained during the interview with the details on parallel items that were included in the victim(s) report of the sexually abusive behavior and other background information from the court intake referral record. All but one item was rated on a 4-point scale, although the exact response options varied for each item. The six items are: (1) Level of admission and involvement in the sexually abusive behavior (denial of any involvement, admits but with minimal details based on reported incident, admits to most details of incident, fully admits to details of incident), (2) Extent of responsibility accepted by the client (none, minimal, half, mostly, full), (3) How much the victim wanted this to happen (not at all, maybe, a little, a lot), (4) Extent of empathy for the victim shown by the client (none, some, considerable, complete), (5) Remorse/guilt shown for the sexually abusive behavior (none, some, considerable, complete), and (6) Clinician belief in culpability (did not commit, slight chance, probably, very sure). “How much the victim wanted this to happen” was coded as missing for cases (22/239 = 9.2%) who denied any involvement in the referral incident. For purposes of the LCA analysis (which utilizes dichotomous items, see below), all six Disclosure Impressions items were dichotomized into less disclosure (the first two listed responses) versus more disclosure (all other responses). This split served to best balance numbers across the two resulting groups. After examining the distributions of these dichotomous items, “Clinician belief in culpability” was excluded due to minimal variability (97% more disclosure).
Because of the minor changes in language and rating process in the initial SODA and the impracticality of replicating the second set of eyes in recent years, it was not possible to calculate interrater reliability between the original interviewer and a second independent clinician rater. So, we collected ratings for the “Level of admission and involvement in the sexually abusive behavior” item from two program clinicians who had no formal contact with the youth to calculate interrater agreement. The two clinicians reviewed the same court intake referral record and the written summaries of the youth’s responses to the assessor’s interview questions as were used to generate the original SODA ratings but not the original SODA ratings themselves. Interrater reliability comparing the two independent clinicians’ ratings for 20 randomly selected cases was high (kappa = 0.83).
The caregiver was also asked at intake about the child’s involvement in the referral incident. The clinician then rated the caregiver’s level of admission on a 3-point ordinal scale (1 = Caregiver admits/agrees child was involved in the sexual incident, 2 = Caregiver is “not sure” if child was involved in the sexual incident and/or believes child was involved but not in the way it was described in the offense report/court hearing, 3 = Caregiver denies the offense/disagrees; child was not involved in the sexual incident). Some cases (29/237 = 12.2%) lack this caregiver admission/denial data because no caregiver was involved in the baseline assessment.
Demographic Information
Information from the intake assessment included the youth’s age in years and items on racial and ethnic background dichotomized as a single variable (1 = minority status; 0 = not). Caregiver education (1 = less than 7th grade; 8 = graduate/professional training) was dichotomized due to distributional issues (1 = more than high school; 0 = high school or less), as was caregiver marital status (1 = married; 0 = single, divorced, separated, or widow/widower). We coded whether the family received any form of social assistance (medical, welfare, other types of social assistance) into a dichotomy (1 = yes; 0 = no).
Victim/Incident Characteristics and Prior Adjudications
Details of the referral incident were obtained from the court documents received with the referral packet. Several details were recorded by research staff about the victim(s), the nature of the sexually abusive behavior itself, victim gender, age of the youngest victim, presence of a biological relationship between the victim and the adolescent who engaged in abusive behavior, whether the sexually abusive behavior was repeated, the method used to secure victim cooperation (none, verbal only, physical [which may or may not have included verbal as well], other – e.g., pulled victim’s pants down/off), and whether there was any penetration or intercourse during the sexually abusive behavior. For the five cases referred for child pornography exposure, several variables were coded as non-applicable (e.g., victim age, method for gaining cooperation). Five cases with missing data for the age of the youngest victim were coded instead from the SODA interview (r = 0.91) for age of youngest victim between the two measures. For each dichotomous variable, we coded 1 = presence versus 0 = absence.
The court documents from the referral packet included information about any prior court involvement and prior adjudications. All prior adjudications were coded into sexual and nonsexual types. For predictive analyses, the prior sexual adjudications data are not used due to a very low frequency (<1%). The number of prior nonsexual adjudications (e.g., simple assault, trespass, burglary) ranged from zero to eight in our sample and was dichotomized (1 = any, 0 = none) due to a skewed distribution.
Diagnoses, Externalizing Problems, and Internalizing Problems
Diagnostic and other clinical history information were obtained at intake and at discharge based on the Schedule for Affective Disorders and Schizophrenia for School Aged Children – Present and Lifetime Version for DSM-IV (K-SADS-PL; Kaufman et al., 1996), a semi-structured interview designed to assist in the assessment of current and past episodes of major mental health disorders in school-aged children. Clinicians made diagnoses based on information from both the youth and the caregiver, as well as any available collateral information. To assess Multiaxial Diagnosis/Axis IV (“Psychosocial and Environmental Problems”), we coded (1 = present, 0 = absent) separately the two categories of “problems related to the social environment” (e.g., ADHD symptoms impair interactions with peers and family) and “educational problems” (e.g., ODD behavior affects school learning due to defiance and suspensions) from clinician entries. Other axis IV categories were too infrequent to use in analyses. The clinical supervisor reviewed all K-SADS-PL summaries to confirm any diagnoses based on a review of all information in the packet and the final psychiatric evaluation document. For discrepancies, the consulting psychiatrist reviewed the materials – including diagnoses and symptoms – to derive a final diagnosis. The K-SADS-PL has been demonstrated to have concurrent validity and excellent interrater and test-retest reliability (Kaufman et al., 1997).
The caregiver completed the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001) until it was replaced with the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997). Both scales capture the child’s behavioral and emotional problems and competencies, have excellent psychometrics including sensitivity and specificity in identifying disruptive behavior disorder (Achenbach, 2005; Warnick et al., 2008), and are highly correlated (r = 0.84; Goodman & Scott, 1999). To include all available caregiver reported data on this construct, we used whichever scale was available between the CBCL total externalization T-score (n = 134) and the SDQ externalizing problems score (n = 76). To ensure both scales were on the same metric, the SDQ externalizing problems score was re-scaled to the same T-score metric as the CBCL total externalization T-score.
The Antisocial Process Screening Device (APSD; Frick & Hare, 2001) assessed psychopathy-related features in children (6–13 years) using caregiver ratings of 20 items (0 = not at all true; 2 = definitely true; Frick et al., 2000). The three scale factors (callous/unemotional traits, impulsivity, narcissism) have acceptable psychometric properties, including test-retest reliability, internal consistency, and concurrent and predictive validity (e.g., Frick et al., 2000; Poythress et al., 2006). The APSD was designed for youths aged six to 13, but prior research has demonstrated acceptability up to age 21 (e.g., Bijttebier & Decoene, 2009; Kruh et al., 2005; Muñoz & Frick, 2007; Sadeh et al., 2009). The internal consistencies for these subscales in our sample were acceptable (α’s: callous/unemotional traits = 0.60, impulsivity = 0.68, narcissism = 0.79).
Trauma History and Related Symptoms
In the K-SADS-PL interview section on Post Traumatic Stress Disorder (PTSD), the clinician provided separate present (1) versus absent (0) ratings for a variety of traumatic experiences (e.g., physical abuse, sexual abuse, witnessing domestic violence). Each type of trauma was rated as present if either the caregiver or the youth reported it. Additionally, emotional abuse was assessed separately by both child-report and caregiver-report. Each reporter was asked if the youth had been emotionally abused (“Do you believe you [your child] have[has] been emotionally abused? [criticized, ridiculed, put down]”) on a 5-point Likert scale (not likely, possibly, probably, very likely, definitely). Responses were then dichotomized due to skewed distribution (0 = not likely; 1 = all other responses).
The youth completed the 54-item Trauma Symptom Checklist for Children (TSCC; Briere, 1996) to evaluate general trauma-related symptoms or distress. Clinical items are rated on a 4-point Likert scale (never, sometimes, lots of times, almost all of the time). TSCC scores are normalized by age and gender and reported as T-scores (i.e., mean = 50, SD = 10). There are six clinical subscales (anger, anxiety, depression, dissociation, post-traumatic stress, sexual concerns). Two validity scales identify invalid profiles (under-response [T >= 70] and hyper-response [T >= 90]). Applying these validity scores, TSCC baseline data for 44 cases and discharge data for 39 cases (including 14 cases also flagged at baseline), were removed due to meeting the cutoff for under-response. Hyper-response cutoffs invalidated only a single case at baseline (also invalidated by under-response) and no cases at discharge. Alphas for the six clinical scales ranged from 0.73 to 0.83 (anger = 0.83, anxiety = 0.74, depression = 0.75, dissociation = 0.77, post-traumatic stress = 0.79, sexual concerns = 0.73).
Caregiving Practices
The caregiver also completed the Alabama Parenting Questionnaire (APQ; Shelton et al., 1996) to evaluate positive and negative dimensions of parenting practices. We used the scoring procedure based on the short-form of the APQ (APQ-SF) which includes three, 3-item factors (poor monitoring, inconsistent discipline, positive parenting). The internal consistencies of these three respective factors were acceptable (α = 0.72, 0.63, 0.82, respectively). The APQ-SF has good reliability, factor structure, and discriminant validity.
Adolescent Sexual Behavior
The youth and caregiver completed the Adolescent Sexual Behavior Inventory (ASBI; Friedrich et al., 2004) to capture inappropriate or concerning sexual behaviors, including aggressive or risk-taking behaviors. It includes 45 items using a 3-point scale (0 = not true, 1 = somewhat true, and 2 = very true) that yield five subscales (concerns about appearance, fear, divergent sexual interests, sexual knowledge/interest, sexual risk/misuse). The ASBI has been used in our program with this population (e.g., Kolko et al., 2004). The item language included in each scale varies slightly between the youth and caregiver reports. Four scales were dichotomized (1 = any, 0 = none) due to a preponderance of “0” scores. Sexual knowledge/interest was dichotomized using a median split (<= 5) so that all ASBI variables would be dichotomous.
Treatment Course/Status and Satisfaction
The clinician completed a Treatment Termination Form for each case at discharge. Treatment completion (1 = complete vs. 0 = not) reflected whether the juvenile completed the full set of treatment topics. Various reasons might relate to not completing treatment (e.g., case closure due to chronic no-shows, placement). Treatment success was rated as full success (considerable symptom improvement and/or treatment goals accomplished), partial success (symptoms partially or somewhat improved and/or some progress towards treatment goals), or no success (level/type of treatment not working, non-legal problem got worse/clinical deterioration, unresponsive). Individualized treatment goals were created in collaboration with the youth after assessment was completed and integrated both clinical (e.g., engagement in services, symptom reduction) and probationary targets (e.g., follow-through with prosocial activities, avoids risky community situations). The clinician recorded the number of days in treatment, and whether the youth had any placement (1 = yes, 0 = no), had any sanctions or probation violations based on SSU probation officer reports (1 = yes, 0 = no), or had any referral for additional services or resources by the clinician at discharge (1 = yes, 0 = no). The clinician also indicated whether any no-shows or noncompliance were documented among the reasons for discharge (1 = yes, 0 = no). The clinical supervisor reviewed all discharge paperwork, suggesting rating revisions in some cases.
The youth completed the 8-item Consumer Satisfaction Questionnaire (Larsen et al., 1979) at discharge. All items are rated on 4-point scales with the exact response options varying for each item. A total score (range: 8–32) is calculated as a sum of all eight items (α = 0.81).
Probation officers rated two items to capture the level of goal improvement in the youth’s achievement of community safety/appropriateness or the youth’s likelihood of recidivism, on a 5-point Likert scale (1 = not at all; 5 = very much) on a questionnaire completed for each youth upon discharge. These two items were summed to create a progress scale reflecting treatment gains that conveyed a reduction in community risk behaviors (range: 2–10; r = 0.73).
Recidivism
Recidivism data were available for all 239 youths. Recidivism data were collected from official juvenile court records and from public adult court records (depending on age) at one year, two years, and three years after discharge from the program. Recidivism at each timepoint was coded (1 = yes, 0 = no) separately for any sexual charge or adjudication and for any non-sexual charge or adjudication.
Data Analysis
Prior Reporting of Manuscript Data
Some of the variables we report on have been reported in a prior study (Fanniff & Kolko, 2012), but not for this specific sample classified on the basis of responses to the SODA interview. All analyses were prespecified based on team discussions of key aims, although some variables were recoded or deleted due to skewed distributions. Interrelationships among variables at baseline within a given domain were examined to ensure that variables were sufficiently independent of each other. Intercorrelations and kappas were used, where appropriate. Patterns of missing data were examined among baseline variables and among the variables assessed at both baseline and discharge (i.e., diagnostic and problematic behaviors variables). Variables to account for any significant differences in missing data would be included as covariates in subsequent analyses if needed.
Latent class analysis (LCA) was applied using the poLCA package in R (Linzer & Lewis, 2011; R Core Team, 2020) and class comparisons were conducted using the best-practice for enumeration based on prior simulation work (Nylund-Gibson & Choi, 2018). Classes were estimated based on five of the six previously described disclosure impression items rated by the clinician (i.e., level of admission/involvement in the referral incident, extent of responsibility accepted, degree to which victims wanted the incident to happen, is blamed for incident, degree of victim empathy, degree of remorse/guilt). Models were estimated for one through 10 classes and the best fitting model was selected based on patterns across a set of common fit indices, including information criteria, likelihood ratio tests, and other probabilistic indicators (Masyn, 2013; Nylund-Gibson & Choi, 2018).
Conditional item probability plots were utilized to interpret and characterize variability across classes in constituent items (i.e., the five Disclosure Impressions items) Plots based on these classes then examined variation in demographic information, referral incident characteristics and prior adjudications, baseline psychiatric diagnoses and problematic behaviors, parameters of subsequent treatment, and criminal recidivism for three years following discharge. Class differentiation across each domain was estimated via χ2 tests and one-way ANOVAs, where appropriate. Class membership was also used to predict changes in psychiatric diagnoses and problematic behaviors that were collected at both baseline and discharge. These comparisons were estimated using ANCOVAs and logistic regressions (using dummy codes to represent each of the three classes), where appropriate. In both approaches, the discharge variable was predicted by class membership over and above the effect of the baseline variable. Additionally, χ2 tests were applied to evaluate class differences in the constituent disclosure impression items (i.e., utilized in the LCA) at the conclusion of treatment across simple categories of change trajectories for each item (i.e., “improved”, “plateaued”, and “regressed” relative to their pre-treatment assessment). Binary, Bonferroni-corrected, post-hoc comparisons among the three classes were done for any significant omnibus tests.
Results
Missing Data Analyses
In terms of missing data analyses at baseline, 80.8% (193/239) of the sample had no more than one missing measure (out of nine). At post-assessment, 52.7% (126/239) had no more than three missing measures (out of nine). Testing for missingness characteristics across variables (e.g., as a predictor in focal tests) revealed no significant influence on inferences drawn. Specifically, there were few if any significant differences between the amount of missing data (tabulated either at baseline only or across pre- and post-assessment) and our classes or our outcomes. Additionally, the inclusion of missing data covariates in subsequent analyses did not meaningfully affect the results. Consequently, only the more parsimonious models without the missing data covariates are reported.
Inter-relationships Among Variables
Interrelations among the five dichotomously-coded Disclosure Impression items (kappa) ranged from a low of −0.36 to a high of 0.69 with all others in the −0.20 to 0.36 range, suggesting generally minimal overlap. The highest absolute kappa (0.69) was found between item 4 (Extent of empathy for victims shown by client) and item 5 (Remorse/guilt shown for sexually abusive behavior). Interrelations among referral incident and referral history variables also were explored (kappa range: −0.38 to 0.31), which revealed minimal overlap among these nine variables.
Interrelations among course of treatment and post reports revealed kappas in the range of −0.35 to 0.75 and intercorrelations in the range of 0.11 to 0.87. Any placement and any sanction or violation of probation had a kappa of 0.75. Looking more closely at this relationship, all youth who were placed (29.7%, 70/236) also received a sanction or violation of probation during treatment. But there were a substantial number of cases (16.9%, 28/236) who received a sanction or violation of probation and were not placed. Consequently, both variables were retained to examine them separately. Treatment completion and Treatment success (full, partial, none) were also highly related (r = 0.87). Specifically, 100% of “full” success cases completed treatment versus 80% of “partial” and 0% of “none”. We retained both variables.
Identification of Best Fitting Class Solution and Class Descriptions
Model Fit Indices for Latent Class Enumeration.
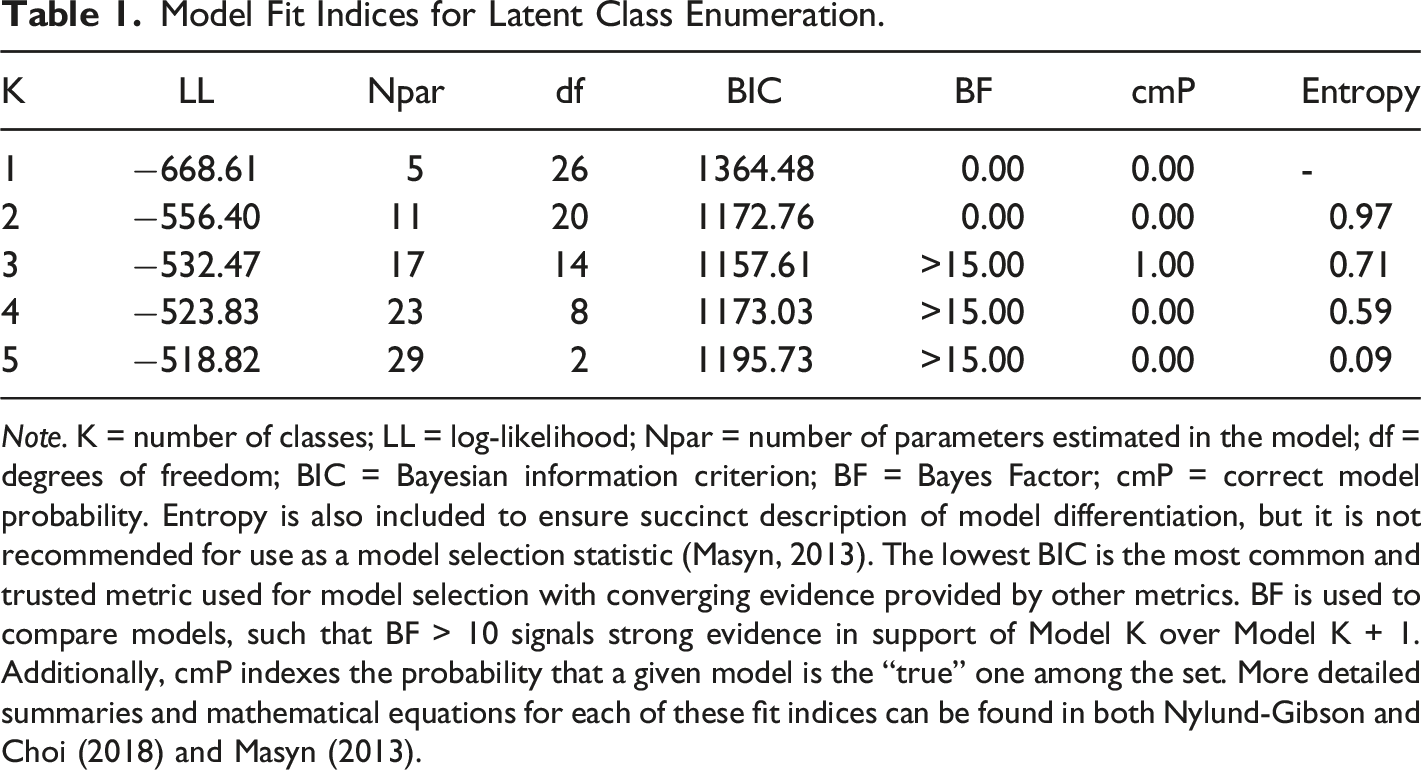
Note. K = number of classes; LL = log-likelihood; Npar = number of parameters estimated in the model; df = degrees of freedom; BIC = Bayesian information criterion; BF = Bayes Factor; cmP = correct model probability. Entropy is also included to ensure succinct description of model differentiation, but it is not recommended for use as a model selection statistic (Masyn, 2013). The lowest BIC is the most common and trusted metric used for model selection with converging evidence provided by other metrics. BF is used to compare models, such that BF > 10 signals strong evidence in support of Model K over Model K + 1. Additionally, cmP indexes the probability that a given model is the “true” one among the set. More detailed summaries and mathematical equations for each of these fit indices can be found in both Nylund-Gibson and Choi (2018) and Masyn (2013).
Converging evidence across all seven fit criteria suggested a three-class solution best captures patterns present in the data (see Table 1). Specifically, four out of the seven fit criteria utilized indicate best fit for the three-class model relative to others: the three-class solution has the lowest BIC and CAIC (Masyn, 2013), surpasses the “strong” support threshold for the Bayes Factor (Wagenmakers, 2007; Wasserman, 1997), and was identified as the model with the greatest probability of being “correct” among all models estimated (Masyn, 2013). While not all fit indices supported the three-class model, such discrepancy is not uncommon and is often supplemented with closer qualitative inspection (Masyn, 2013; Muthén, 2003; Ram & Grimm, 2009) to verify that classes are stable (e.g., absence of “rare” or unequal classes; Depaoli, 2013; Morgan, 2015; Tofighi & Enders, 2007; Tueller & Lubke, 2010) and well differentiated (e.g., clear substantive variation). In the case of the three-class solution, inspection of the item response probabilities (see Figure 1) highlights the distinct and ecologically meaningful attributes of each group, described in further detail below. Conditional item probability plot for the three class solutions. Note. Conditional item probabilities reflect the likelihood of endorsing the item among members of each class. For example, Unempathetic Deniers are associated with the highest probability of blaming the victim for the sexually abusive behavior relative to the other Classes while Empathetic Admitters is associated with the lowest probability (virtually 0) of blaming the victim relative to the other two Classes.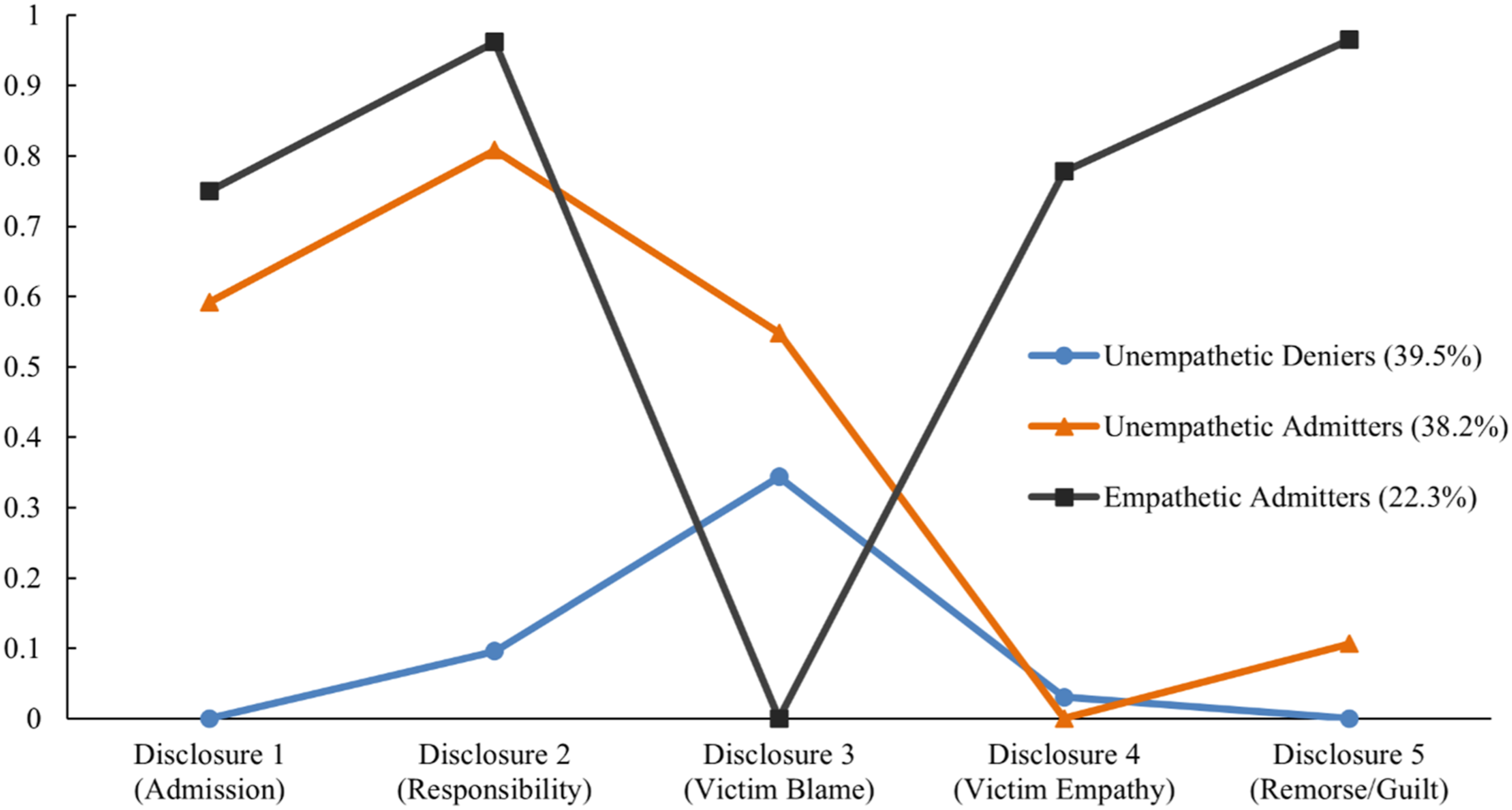
Class 1 (“Unempathetic Deniers”) accounted for the most cases (39.5%; 92/233). At intake, they exhibited the lowest rates of admission of involvement (0%), acceptance of responsibility (0%), and expression of remorse (0%). They also reported extremely limited rates of victim empathy (2.3%, 2/88). Their rates of victim blaming, while moderate, were higher (36.5%, 23/62) than the Empathetic Admitters, but lower than Unempathetic Admitters. Overall, many of these cases completely denied all aspects of the sexually abusive behavior at intake.
Class 2 (“Unempathetic Admitters”) accounted for 38.2% (89/233) of the sample at intake. Unlike Class 1, this class endorsed high rates of admission of involvement (61.8%, 55/89) and acceptance of responsibility (86.9%, 73/84). However, Class 2 exhibited the highest rates of victim blame (54.8%, 46/83). In addition, none of them reported empathy for the victim (0%) and few showed remorse for their behavior (6.8%, 6/88).
Class 3 (“Empathetic Admitters”) accounted for 22.3% (52/233) of the sample at intake. These individuals exhibited the highest rates of admission of involvement (36/52 = 69.2%), acceptance of responsibility (98.0%, 49/50), victim empathy (73.1%, 38/52), and expression of remorse (96.2%, 50/52). They also reported the lowest rate of blaming of the victim (0%).
Examining the Relationship Between Class and Youth Background Variables
Class Comparison on Demographic and Baseline Measures.
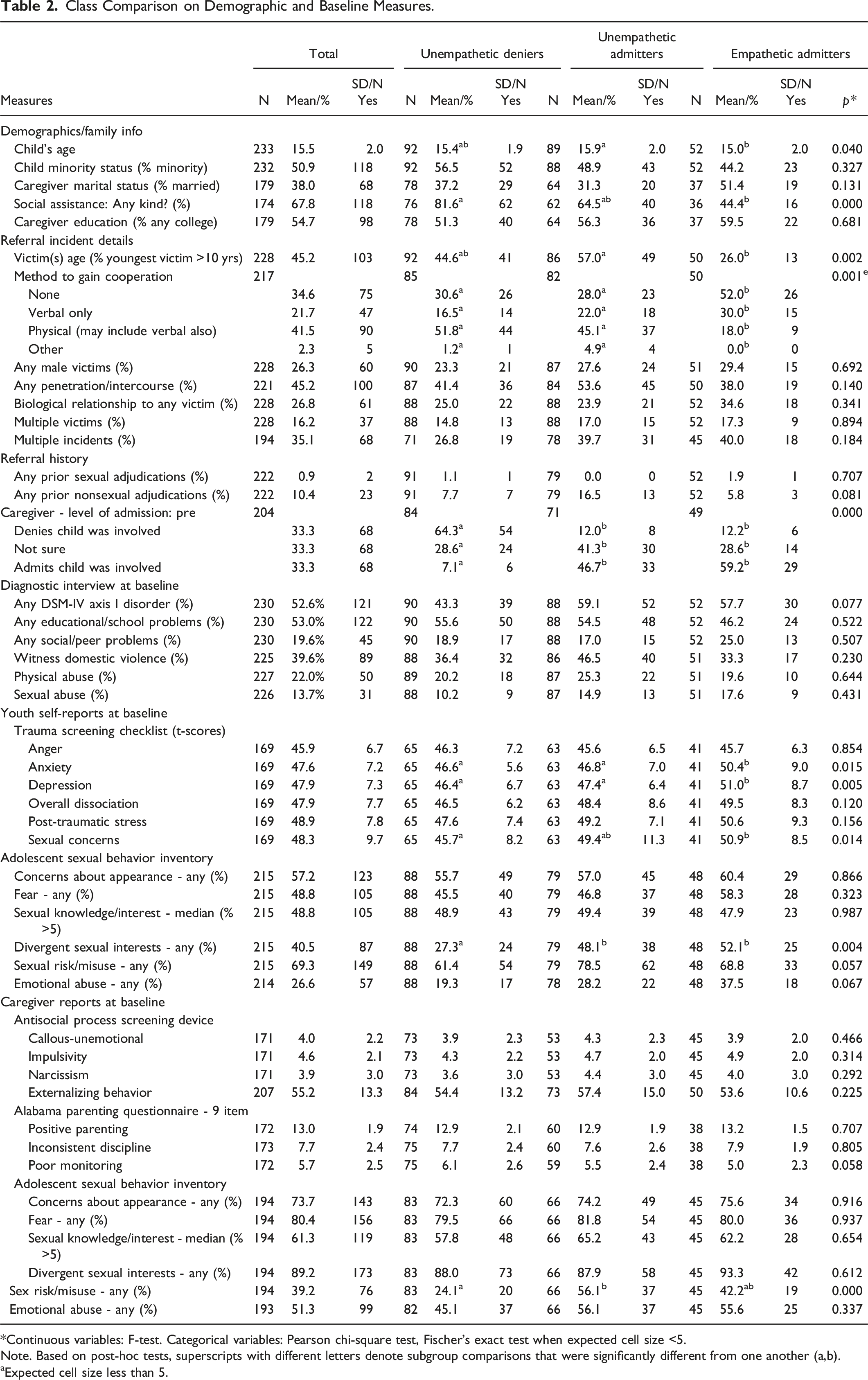
*Continuous variables: F-test. Categorical variables: Pearson chi-square test, Fischer’s exact test when expected cell size <5.
Note. Based on post-hoc tests, superscripts with different letters denote subgroup comparisons that were significantly different from one another (a,b).
Expected cell size less than 5.
Examining the Relationship between Classes and Pre-Post Changes in Disclosure Variables and Clinical Outcomes
Class Comparisons on Baseline and Discharge Offense Disclosure Variables.
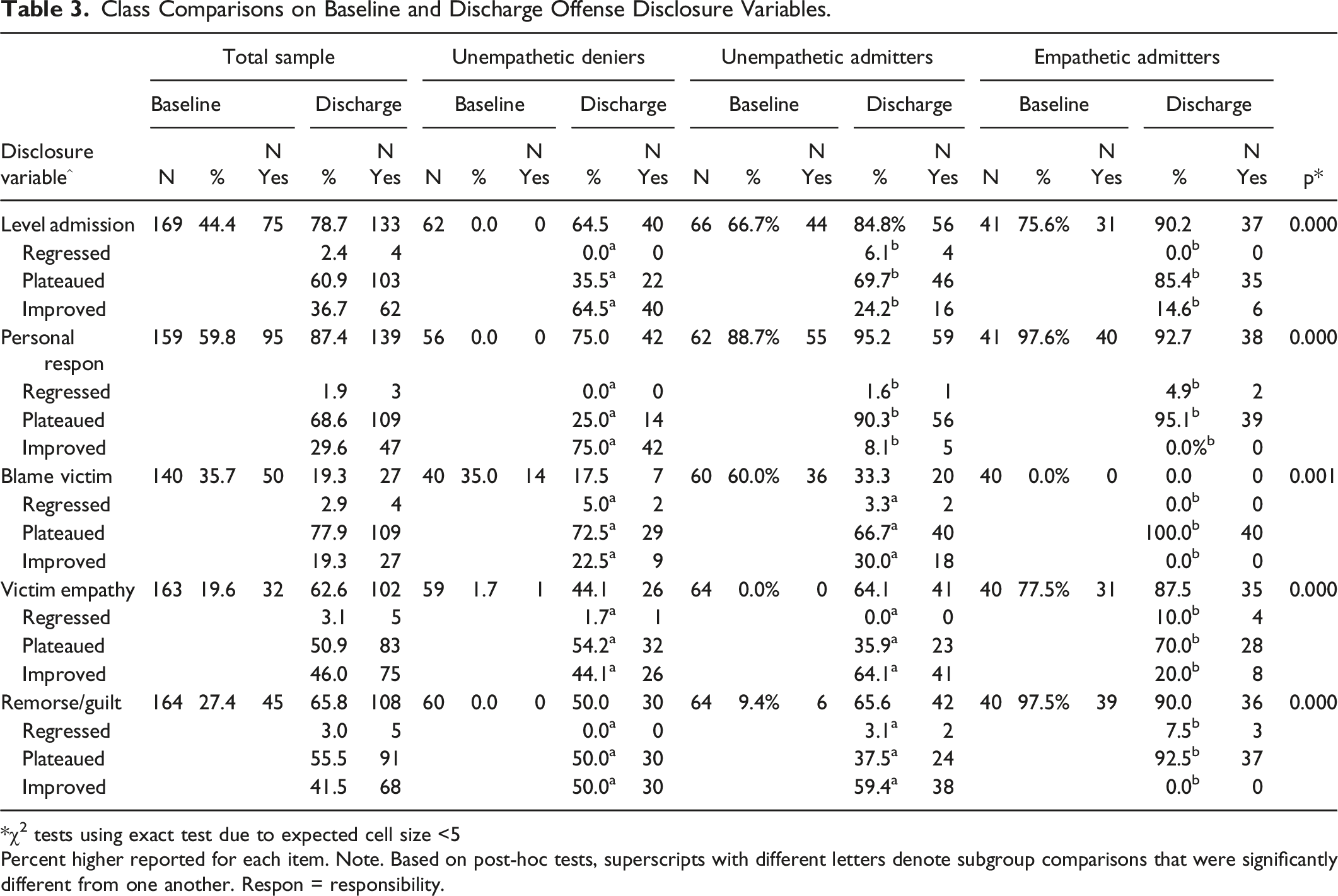
*χ2 tests using exact test due to expected cell size <5
Percent higher reported for each item. Note. Based on post-hoc tests, superscripts with different letters denote subgroup comparisons that were significantly different from one another. Respon = responsibility.
We also examined change in diagnoses and problematic behaviors by class membership on five caregiver-reports (K-SADS-PL, ASBI, APSD, CBCL/SDQP, APQ) and two youth reports (ASBI, TSCC). Direct group (class) contrasts were estimated using ANCOVAs and logistic regressions (using dummy codes to represent each of the three classes), where appropriate. Class membership did not significantly differentiate change in any outcome at discharge. A table of descriptives and test statistics is available from the first author.
Examining the Relationship between Class and Both Treatment Outcome and Recidivism
Class Comparisons on Treatment, Discharge, and Recidivism Measures.
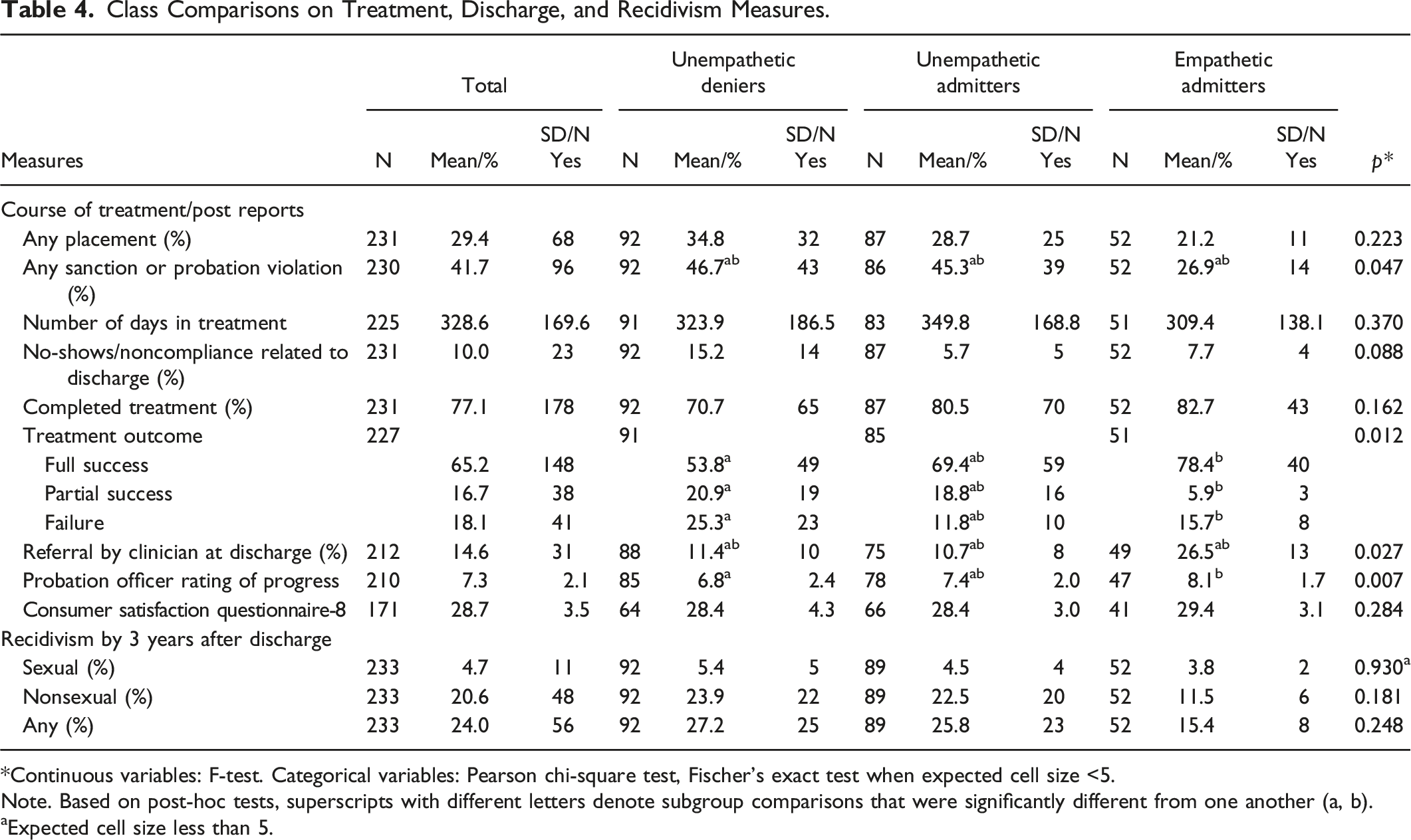
*Continuous variables: F-test. Categorical variables: Pearson chi-square test, Fischer’s exact test when expected cell size <5.
Note. Based on post-hoc tests, superscripts with different letters denote subgroup comparisons that were significantly different from one another (a, b).
Expected cell size less than 5.
Two other treatment measures had significant omnibus tests and Bonferroni-corrected post-hoc tests that narrowly failed to reach significance. The observed percentages for these two measures suggested that Empathetic Admitters may have had higher rates of discharge referral as well as lower rates of sanctions or probations violations than the other two Classes.
Finally, the rates of sexual and non-sexual recidivism were 5.4% and 23.9%, respectively. There were no significant differences across the three classes in either recidivism rate during the 3-year follow-up period, although the rate of non-sexual recidivism was only half as high in the Empathetic Admitters as compared to the other two Classes.
Discussion
Key Findings and Implications
Using a person-centered approach, we subtyped within-person, multivariate response patterns of disclosure (i.e., from full admission to denial) by youth regarding incidents of sexually abusive behavior after community-based outpatient clinical and probationary services have been mandated. In a semi-structured interview at intake, youth provided details of the incident relating to their perceived involvement, responsibility, victim blaming, empathy, and remorse. Three latent classes were identified for the set of responses to disclosure items: Unempathetic Deniers, Unempathetic Admitters, and Empathetic Admitters. The three classes varied significantly by measures at intake, treatment, and discharge, suggesting that the pattern of an individual youth’s responses may be a useful proxy for their initial severity, prognosis, and treatment needs. Class membership did not, however, differentiate rates of recidivism across youth. The findings are discussed in the context of relevant conceptual, therapeutic, and methodologic issues.
The three Classes identified at intake using latent class analysis reflected youth who did not admit to the offense or show victim empathy or remorse (Unempathetic Deniers. 39.5%), youth who admitted to their sexually abusive behavior but showed no victim empathy or remorse (Unempathetic Admitters, 38.2%), or youth who admitted and showed considerable empathy and remorse (Empathetic Admitters, 22.3%). Documentation of these subgroups extends other evidence for variation in the types and patterns of denial in youth who engage in sexually abusive behavior (Vanhoeck & Daele, 2011). Indeed, denial, minimization, and lack of victim empathy are fairly common in the general population of persons who engaged in sexually abusive behavior (Levenson, 2011). For example, Frost et al. (2019) noted that two of their three adult subgroups showed offense motivation trajectories that began with an evasive (17%) or placatory style (34%), whereas the third subgroup (52%) began with a more neutral style. Indeed, these varied levels of disclosure are consistent with the Classes identified in this study and the suggestion that denial is best captured by multiple dimensions (Levenson, 2011) or a spectrum (Reicher, 2013). Our results extend this variability to other disclosure parameters, such as victim empathy and remorse. The use of advanced analytic methods to identify clusters of youth is an important tool in the identification and interpretation of key subgroups, typologies, or trajectories based on varied sexually abusive behaviors (Barra et al., 2018; Cale et al., 2016; Kemper & Kistner, 2010; Lussier, 2017; Lussier et al., 2018). Methods that capture person-centered heterogeneity in profiles of sexually abusive behavior are critical for informing future implementation work designed to develop evidence-based methods for personalizing care.
Some baseline and treatment characteristics distinguished the three Classes. In particular, the Unempathetic Deniers had a higher rate of social assistance in the family (albeit not statistically higher than the other groups) than the Empathic Admitters, but all three classes were otherwise comparable in demographics. They were also more likely to use physical force with the victim during the referral incident than Empathetic Admitters. Their caregivers also showed the highest level of denial – over 64% – of the youth’s involvement in the incident. Although caregiver denial may potentially reflect one of the more salient influences on the youth’s level of denial, the reverse could also be true. The role of caregiver denial has rarely been examined but some research suggests that families of adolescents who engage in sexually abusive behaviors (vs. those who do not) have much higher rates of denial of the sexually abusive behavior (Baker et al., 2003) and may describe themselves as more healthy than they really are (Ware et al., 2015). Interestingly, this Class also reported far lower levels of sexual concerns and divergent sexual interest, and their caregivers reported less sexual risk.
The Unempathetic Deniers also varied in their disclosure reports over time and in relation to the other two groups. Given that their baseline levels of disclosure were so low, they showed the most improvement at discharge in admission details, responsibility, empathy, victim blame, and remorse. At the same time, their discharge levels did not reach the levels detected in the other two groups, especially the Empathetic Admitters who showed relatively high rates on these items at baseline and discharge. This pattern of change and discharge status in the Unempathetic Deniers is noteworthy given their year-long exposure to multiple intervention services (e.g., outside medication management). One potential contributor to this continuity in the Unempathetic Deniers is the heightened level of caregiver denial documented at discharge. Further, this Class received the highest level of probationary violations and sanctions during intervention, so it is not a surprise that they also received the lowest ratings of treatment success by their clinicians or improvement by their probation officers. These findings suggest the potential benefit of trying to help caregivers recognize the plausibility of a child’s or adolescent’s sexually abusive behavior and support community rule-following to enhance treatment participation and clinical effectiveness in this subgroup (see Worling & Langton, 2017).
Our overall rates of sexual and non-sexual recidivism (5.4%, 20.6%) are consistent with those found in meta-analyses documenting the benefits of treatment for youth who have engaged in sexually abusive behavior (Kim et al., 2016). Class was unrelated to sexual or non-sexual recidivism, although the Empathetic Admitters had non-sexual recidivism (e.g., assault) rates that were half as high as the other two Classes. Similar findings have been found among some adult studies of classes (Frost et al., 2019) or key clinical attributes (Leung et al., 2021). The fact that the sexual recidivism rates were generally low for all three Classes may contribute to this comparability (Reitzel & Carbonell, 2006). Other studies of adolescents with different types of sexually abusive behavior histories have found lower rates among those adolescents who have engaged in sexual (vs. non-sexual) offenses (Mulder et al., 2019). Our Classes were also comparable in certain sexual (e.g., referral incident or victim characteristics, reports of sexual concerns or knowledge) and non-sexual variables (e.g., age, ethnicity, trauma history, psychopathy, psychiatric disorder, parenting). Such findings extend research showing that subgroups of adolescents who engage in sexually abusive behavior share many clinical characteristics (see Fanniff & Kolko, 2012), which may be one reason why denial is often unrelated to recidivism (Hanson & Bussiere, 1998; Hanson & Morton-Bourgon, 2004; Righthand & Welch, 2001). Despite these shared characteristics, variation in baseline characteristics like disclosure may be a useful target for guiding implementation research designed to determine whether, how, when, and for whom specific care decisions are most effective for maximizing positive outcomes (e.g., reducing recidivism, improving mental health).
Limitations
The limitations of this research deserve mention. First, we had a modest sample size; especially when cases were divided into three Classes. We developed the Classes using baseline (vs. repeated) measures of disclosure, in part, to parallel the information that would be available for treatment planning upon referral. Further, we had some missing data for outcomes and ceiling effects that occasionally limited the change found for certain classes (most for Empathetic Admitters) so that the other Classes were playing “catch up” over time. While it is possible that characteristics associated with Class membership contribute to specific patterns of disclosure behavior, these also may vary without causal relationship to disclosure. Further research is needed to develop a sufficiently nuanced understanding of disclosure pattern variation and the extent to which that may have distinct antecedents and outcomes across individuals. Finally, we recognize that these results based on a community sample may not generalize to samples of adolescents mandated to placement.
Future Directions
Most recommendations from the field encourage an assessment of disclosure/denial for various reasons (see Dopp et al., 2015). These reasons include the benefits of understanding the client’s view of the sexual behaviors and responsibility, its relationship to the victim’s report, and the level of empathy and remorse displayed, to lower the risk of engaging in future sexually abusive behavior. At the same time, ATSA’s adolescent treatment workgroup guidelines do not formally expect providers to target and eliminate youth denial of sexually abusive behavior (Association for the Treatment of Sexual Abusers, 2017). This scenario seems to raise questions as to whether it is important to assess level of denial/admission and, if so, how often should it be done, how should the information be used during intervention, and what are the discharge and probationary implications of falling into any one of these subgroups.
One purpose of this study was to develop a referral incident disclosure tool to assess variations in key details related to admission/disclosure at intake and over time with each client. The SODA interview provides a standardized method to measure and characterize a continuum of disclosure (denial-admission) and may support ongoing clinical efforts to enhance greater disclosure and understanding of the context of abusive sexual behavior. The interview details can then be systematically compared to the victim’s report, incorporating the information over time to facilitate case formulation and disposition, to facilitate depiction of change. Additionally, patterns of responses for individual youth receiving care may be compared by clinicians to those response patterns characteristic of subgroups identified in this work to support linkage with these results. Of course, further refinement of the procedures for conducting the interview, evaluation of the psychometrics of the tool, and replication of the Classes and their relationship to similar outcomes are warranted. Whether and how group membership could be immediately useful for making specific clinical decisions with individual youth will require additional implementation trials comparing the effectiveness of procedures for personalizing care. Important questions to address in future implementation research would be (1) to what extent does longer-term behavior (e.g., recidivism) differ across subtype, marking a more persistent treatment need, (2) what is the optimal method for a clinician to use to identify probable group membership for a specific youth they are treating (e.g., what if youth report differing degrees of correspondence with what is prototypical for a given group), (3) how malleable is subtype (e.g., could a given youth of one subtype be supported to shift to another subtype to the benefit of other domains), and (4) to what extent would individual youths in different classes benefit from different treatment decisions.
The use of repeated measures of disclosure perceptions across intervention may inform providers about any needed tailoring of or modifications to the treatment plan/curriculum (see Fanniff et al., 2014). The SODA offers providers a structured approach to soliciting and then discussing key details related to a referral incident over time that may enhance treatment engagement and response. This review may also stimulate discussions of a youth’s exposure to ongoing risky situations or risky behaviors (e.g., rule-breaking/delinquent behavior, exposure to young child) that might alter a treatment regimen (Righthand & Hart, 2020). We hope that this tool may assist program evaluators or researchers to experimentally test different strategies designed to either modify youth’s level of disclosure, responsibility, and empathy, or to determine which clinical decisions may be most helpful in optimizing outcomes for particular youth (i.e., considering subtype) with differing disclosure patterns all in the service of enhancing treatment engagement and impact.
Footnotes
Acknowledgments
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results. We acknowledge the clinical assistance of the staff of the SAFE Program and the Probation Officers from the Northern Probation Office. The SAFE Program and this research are funded by the Allegheny County Juvenile Court. The Allegheny County Juvenile Court was not involved in the research or preparation of this manuscript. The authors do not have financial interests to report with regard to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Allegheny County Juvenile Court.