
Abstract
This study seeks to add to the existing knowledge and available literature on schema therapy elements in forensic inpatient samples. Early maladaptive schemas and emotional states were assessed in Dutch individuals with sexual convictions and compared to individuals with nonsexual violent convictions. Self-ratings of the Young Schema Questionnaire and the Schema Mode Inventory of 95 patients with either convictions for child sexual abuse (N = 30), sexual violence against adults (N = 34), and nonsexual violent convictions (N = 31) were examined using one-way multivariate ANOVAs. Regardless of victim type, forensic patients convicted for sexual offending, and patients with convictions for nonsexual violent offending, seem to make equal use of specific maladaptive cognitive schemas and schema modes during mandated inpatient care. Other studies have shown that people with sexual offense histories are typically characterized by insecure attachment, overvigilance towards women, or a child-like self-concept. Our study indicates that forensic patient in Dutch mandated care may be qualitatively different from typical patients with sexual offense histories and that Dutch patients with violent or sexual offense histories are more similar than they are dissimilar.
Keywords
Relationships Between Early Cognitive Schemas and Emotional States in Individuals with Sexual Convictions
Multiple studies have shown that emotional problems and cognitive distortions are linked to sexual violence (Byrne et al., 2016; Gunst et al., 2019; Ó Ciardha & Ward, 2013). For example, individuals with histories of sexual offending typically report frequent and intense negative emotional experiences (e.g., loneliness) and experience difficulties in regulating emotions (Gillespie & Beech, 2016; Ward & Beech, 2016). These difficulties are less prominent in individuals with no (sexual) offending histories (Garofalo et al., 2019; Gillespie et al., 2018). For example, in a study a by Garofalo et al. (2019), individuals with sexual offence histories reported greater levels of general sadness and lower levels of general excitement compared to individuals with nonsexual violent offences or individuals with no offence histories.
Emotional experiences may be partly triggered by problems in social relationships and cognitive distortions, which lead to misreading social observations and increased negative emotions (Barnett, 2011; Martin & Tardif, 2015). Cognitive distortions refer to propositions, views or ideas that people accept as true. Ó Ciardha and Ward (2013, p. 5) define distortions in relation to sexual violence as “beliefs or attitudes that violate commonly accepted norms and reality that are associated with the onset/maintenance of sexual violence.” For example, some perpetrators of sexual violence believe that children are sexual beings while others have a sense of sexual entitlement towards women (Bouffard & Goodson, 2017; D’Urso et al., 2019). Cognitive distortions and emotional regulation problems are important objectives to address in psychological treatment for sexual violence (Carter & Mann, 2016; Gillespie et al., 2012), such as cognitive (behavior) therapy (Beck et al., 2004), emotion focused therapy (Greenberg, 2002) and schema therapy (Young et al., 2007).
Schema therapy’s (Young et al., 2003) framework of early maladaptive schemas (EMSs) offers an approach to understanding cognitive distortions in perpetrators of sexual violence. EMSs refer to a core set of underlying schemas or structures that we have about ourselves, other people and the world, which may result from interactions of child temperament, insufficient parental sensitivity for the child’s basic emotional needs, and adverse childhood experiences. The framework of EMS expands on Beck model of cognitive schemas (Beck et al., 2004) by describing five organizing domains: (1) the disconnection domain that involves schemas related to violations of basic universal needs for security, safety, acceptance and respect; (2) the impaired autonomy and performance domain that refers to schemas related to the basic universal need for autonomy and competence which leads to expectations about oneself and others; (3) the impaired limits domain involves schemas related to deficiencies in internal limits and responsibility to others; (4) the other-directedness domain refers to excessive focus on the desires, feelings and responses to others at the expense of one’s own needs; and (5) the overvigilance domain that refers to excessive emphasis on suppressing one’s feelings, impulses and choices (Young et al., 2003). Each domain encompasses a thematically related cluster of EMSs that guide interpersonal (violent) behavior. For example, within a student sample (N = 166, all male), having committed any form of sexually aggressive behavior was linked to significantly higher levels of EMSs referring to disconnection, impaired autonomy and performance, and overvigilance (Sigre-Leirós et al., 2011). These underlying EMS may give rise to implicit theories about victims, and broader categories of individuals (i.e., children, women; Ward, 2000). EMSs are triggered by emotional and stressful events. Subsequently, EMS guide cognitive processing of life events and interpersonal interactions. It is assumed that the thoughts and interpretations produced in any offence chain are situation specific products of underlying schemas (Mann & Beech, 2003; Young et al., 2003). These schemas may interact with other factors such as sexual deviance and emotional states.
According to the schema therapy framework, individuals with histories of violent offending can also exhibit frequent and rapid fluctuations in emotional states, or remain rigidly stuck in a particular emotional state, lacking the flexibility to respond adaptively to situations. These states are referred to as schema modes and are defined as the current emotional state that a person is in (Young et al., 2003). They are divided across five organizational domains: (1) child modes refer to feeling, thinking and acting in a “child-like” manner; (2) avoidant coping modes involve attempts to protect oneself from pain by means of avoiding; (3) parent modes relate to self-directed criticism or demands that reflect internalized parent behavior and emotional stance; (4) overcompensatory modes refer to extreme attempts to overcompensate painful feelings; and (5) the healthy domain refers to expression of healthy, balanced self-reflection, and feelings of joy (Young et al., 2003). Each domain encompasses a thematically related cluster of schema modes. Schema modes may play a role in criminal behavior, including sexual violence. Keulen-de Vos and colleagues (2016) showed that, in a sample of 95 offenders including 27 people convicted for sexual crimes, criminal behavior was often preceded by schema modes that refer to feelings of vulnerability, abandonment and loneliness (i.e., child modes), and states of intoxication (i.e., avoidant modes) whereas criminal behavior itself is characterized by emotional states of anger, and the use of overcompensatory strategies involving threats, intimidation, and aggression (i.e., overcompensatory coping modes).
Studies on EMSs and schema modes in adults convicted for sexual violence against children or adults are relatively limited. Carvahlo and Nobre (2014) showed that individuals convicted for child sexual abuse (N = 33) presented significantly more schemas from the domains of disconnection, impaired autonomy and performance, other-directedness, and overvigilance than non-offenders (N = 30), whereas participants convicted for sexual offending against adults (N = 32) scored higher on the impaired autonomy domain than non-offenders. Further, Chakhssi and colleagues (2013) showed that EMSs related to disconnection and other-directedness were more prevalent in males convicted for child sexual abuse (N = 23) compared to males convicted for nonsexual violence (N = 24). There were no significant differences between participants convicted for sexual offending against children and adults (Chakhssi et al., 2013).
The Present Study
Early maladaptive schemas and schema modes among individuals with sexual offence histories have predominantly been examined in prison samples (e.g., Carvahlo & Nobre, 2014; Sigre-Leirós et al., 2011) or non-clinical groups. To our knowledge, only one study tested offending groups who were residing in mandated clinical care (Chakhssi et al., 2013). Our study adds to this gap within the literature. The main purpose of this explorational study was to examine EMS and schema modes in individuals convicted for either sexual violence against adults or children, compared to individuals convicted for nonsexual violence. As the literature on EMS and schema modes in forensic inpatient samples is scarce, we were not set out to confirm previous empirical findings. Therefore, our hypotheses were exploratory.
Exploratory hypotheses on early maladaptive schemas
We hypothesized that individuals convicted for sexual violence against adults were more likely to endorse the EMS domain related to overvigilance and the domain related to impaired autonomy compared to individuals convicted for sexual violence against children or nonsexual violence. Characteristic of the schemas in the overvigilance domain is the emphasis on internalized strict rules and the minimization of feelings and emotional expression. People who develop these schemas were typically brought up in demanding, strict, punitive, or perfectionistic families (Young et al., 2003). The impaired autonomy domain relates with a lack of sense of self and self-agency. The development of the schemas in these EMS domains typically happens when one grows up in a family where the parents were overprotective, too involved in the child’s life, or careless about the child’s development (Young et al., 2003). For example, Reavis et al. (2013) compared perpetrators of sexual offending against adults, child sexual abuse, domestic violence, and stalking offences and reported that the first group have the highest prevalence of household substance abuse, parental divorce, criminal behavior in household, and household mental illness. These findings indirectly support the view that people who have sexually offended against adults are more likely to report schemas relating to impaired autonomy. Schemas related to power, controlling, and overvigilance (e.g., suspicion of or hostility toward women) in perpetrators of rape have been reported by Milner and Webster (2005) and Polaschek and Gannon (2004). For example, Polaschek and Gannon (2004) showed that “dangerous world/women are dangerous” is an empirically supported implicit theory in men convicted for rape. They have belief systems through which they perceive the world as an inherently dangerous place in which other people tend to behave in an abusive and rejecting way. Based on these findings, we argue that people who have sexually offended against adults are more likely to report schemas relating to overvigilance.
We hypothesized that individuals convicted for child sexual abuse were more likely to endorse schemas related to disconnection because a secure attachment style is less common in these individuals compared to individuals with convictions for sexual violence against women or nonsexual convictions (Chawke et al., 2021; Garofalo & Bogaerts, 2019). For example, Marsa et al. (2004) reported that 93% of their sample of men convicted for child sexual offences (N = 29) had an insecure attachment style. Compared with three control groups (i.e., community controls, violent offences, nonviolent offences), men convicted for child sexual offences reported significantly more sense of loneliness (Marsa et al., 2004). The EMS domain of disconnection is closely related to the concept of insecure attachment, mostly because people who have these kind of schemas lack the inability to form secure bonds with others (Young et al., 2003).
Exploratory hypotheses on schema modes
We hypothesized that individuals with sexual offence histories against children were more likely to experience child modes and avoidant modes. According to schema therapy, child modes refer to feeling, thinking and acting in a child-like manner. The name of the domain refers to childhood basic emotional needs (i.e., secure attachment) that have been neglected, overindulged or frustrated (Young et al., 2003). Patients with violent and sexual offence histories are both likely to experience adverse childhood experiences and inadequate parental boundaries (e.g., insufficient gratification) during childhood (Levenson et al., 2016; Reavis et al., 2013). However, people with sex offence histories have higher rates of childhood sexual abuse than people with nonsexual violent offence histories (Jespersen et al., 2009), and those with a sexual abuse history are more likely to have younger victims and pedophilic interests (Nunes et al., 2013). Furthermore, emotional congruence with children (ECWC) is a key factor in understanding the etiology of sexual offending against children (McPhail et al., 2013; Seto, 2018). ECWC encompasses identifying with children and having a child-like concept and is associated with childhood sexual victimization (Blank et al., 2018; McPhail et al., 2018). In conjunction with what is known about adverse childhood experiences and ECWC, it can be argued that people with sexual offense histories against children are more likely to endorse child modes. According to schema therapy, people typically use strategies to protect oneself from emotional pain by means of avoiding. Therefore, we also hypothesized that patients with sexual offence histories against children score higher on avoidant coping modes.
We expected stronger endorsement of overcompensatory emotional states in individuals with sexual offence histories against women than in individuals with convictions for child sexual abuse or nonsexual violence. Although numerous factors predict sexual aggression, several theories imply that self-aggrandizement is an important dispositional risk factor (Malamuth, 2003). For example, people who have a high sense of grandiosity may be particularly oriented towards sexual relationships and may respond more aggressively to interpersonal rejections in the sexual domain (Widman & McNulty, 2010). However, only a handful of studies have directly examined whether men high on self-aggrandizement are more likely to perpetrate sexual aggression. Prior research did find that hostility towards women, (sexual) entitlement, seeing women as sexual objects, and a need for control is common in men convicted for sexual violence against women (Milner & Webster, 2005; Polaschek & Gannon, 2004; Sigre-Leirós et al., 2016). These factors are closely related to overcompensatory schema modes such as self-aggrandizement (i.e., sense of grandiosity), instrumental violence, and need for control, therefore we anticipated stronger endorsement of overcompensatory emotional states in individuals with sexual offence histories against women.
Method
Setting and Participants
This cross-sectional study was conducted at two high security hospitals in the Netherlands. By Dutch criminal law, individuals convicted for a violent crime can be admitted involuntarily to forensic care if their offence carries a punishment of at least 4 years of imprisonment, and if their accountability is judged to be diminished because of (a) mental disorder(s). This is referred to as the “TBS order” which translates to treatment on behalf of the state which is comparable to court-ordered institutionalization of a person suffering from mental illness because the person is dangerous to himself or others (e.g., civil commitment in North America) although “tbs” populations typically have larger relapse percentages and relapse faster upon (conditional) release. The hospitals offer a multimodal treatment and care program to patients with offence histories aimed at reducing (the impact of) their mental disorders, increasing the quality of life, and reducing the risk of future violence.
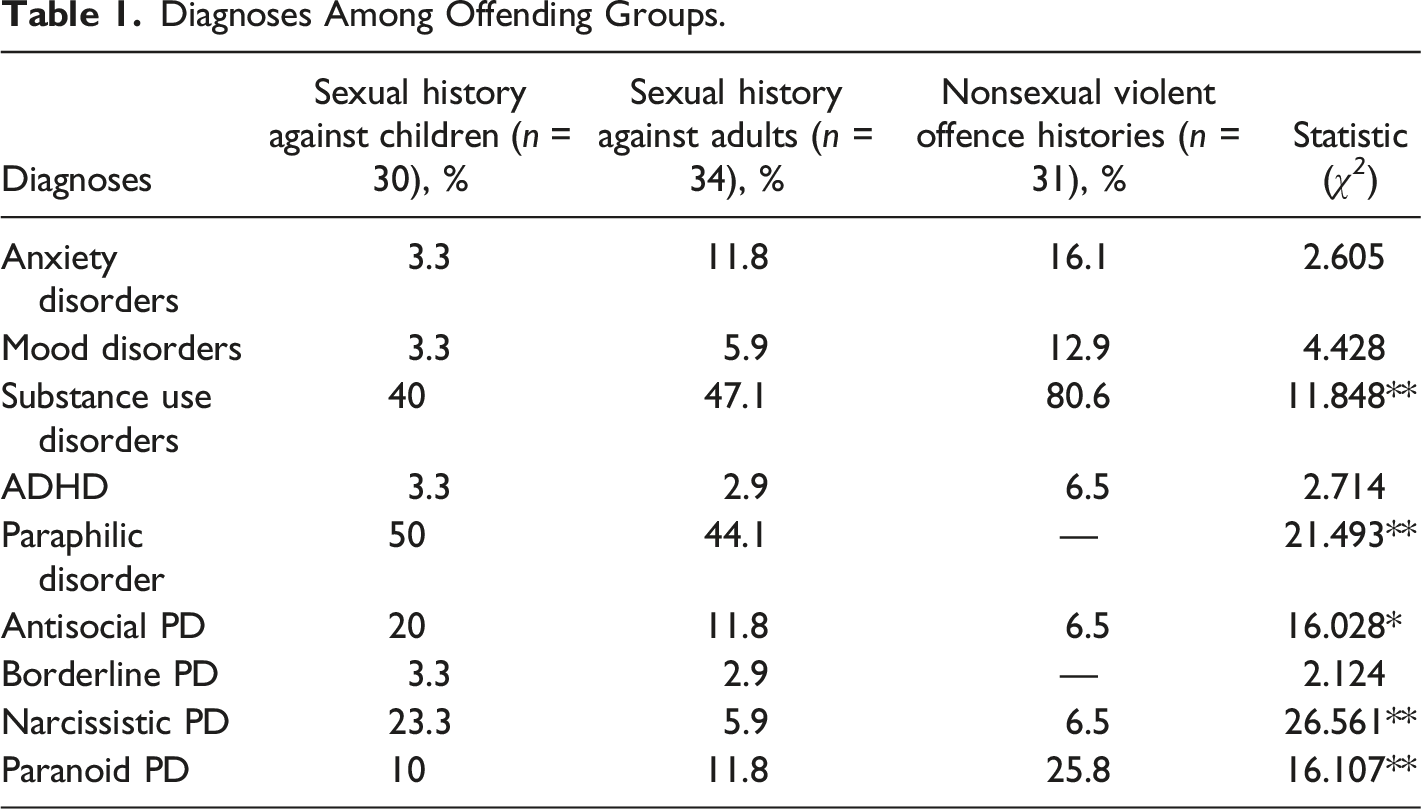
Our sample consisted of three groups: (1) patients with a sexual index 1 offence against adults and no prior sexual offence histories against children; (2) patients with a sexual index offence against children (<14 years old 2 ); and (3) patients with a nonsexual violent index offence (e.g., murder, assault). Groups were homogenous, meaning that we did not include participants with both sexual offences against children and adults, nor did any of the participants with violent nonsexual offences have any prior convictions for sexual violence. There were no restrictions with regard to gender or age. Participants who were admitted to one of the two hospitals were asked to participate (i.e., convenience sample). Patients who met DSM-5 criteria for autism spectrum disorders and/or intellectual disabilities (full scale IQ <70) were excluded as poor meta-cognition and emotional awareness is a common area of difficulty in individuals with these disorders (Nader-Grosbois, 2014; Huggins et al., 2020). An a-priori power analysis (G*Power 3.1.9.7; Faul et al., 2007) indicated a required sample of 66 participants for each analysis to detect large effects with 80% power using one-way analysis of variance (ANOVA) with a two-tailed alpha set at .05. Our total sample (N = 95) consisted of 30 participants convicted for a sexual index offence against children, 34 participants convicted for a sexual index offence against adults and 31 participants convicted for a nonsexual violent index offence.
Diagnoses Among Offending Groups.
Materials
Detailed information on DSM-5 diagnoses, demographic and criminal information was extracted from the patients’ file charts. Diagnoses are based on clinical and/or semi-structured interview diagnoses made by psychiatrists and clinical psychologists.
Early maladaptive schemas
We assessed early maladaptive schemas with the Young Schema Questionnaire-short version (YSQ-S3; Young, 2005) which consists of 90 items that are scored on a six point scale (1 = absolutely not applicable to me, 6 = entirely applicable to me). Schemas are divided into five overall domains. The overall score on each domain is obtained by calculating the mean of the items in that domain. Higher domain scores indicate more intense levels of a particular EMS domain. There are no YSQ-norms established yet for different samples (e.g., community, prison, mandated care). The YSQ-S3 shows good psychometric properties in forensic populations with adequate to high internal consistency and good discriminative power (Bernstein et al., 2021; Doyle et al., 2016). Cronbach’s alphas for the schema domains in our study ranged from .79 to .96.
Emotional states
We assessed emotional states with the Schema Mode Inventory – short version (SMI-R; Young et al., 2007) which contains 80 items that are divided into five domains and are rated on a 6-point frequency scale (1 = never; 6 = always). The overall score on each subscale or domain is obtained by calculating the mean of the items in that domain. Higher domain scores indicate more intense levels of a particular schema mode domain. There are no SMI-norms established yet for different samples (e.g., community, prison, mandated care). In a recent study, the SMI-R proved to be a reliable and valid instrument for assessing schema modes in forensic patients. For example, Keulen-de Vos and colleagues (2017) reported good to excellent internal consistencies with Cronbach’s alpha ranging from .69 to .96. The Cronbach’s alphas for the schema mode domains in our study ranged from .82 to .95.
Procedure
This study was approved by Maastricht University’s Medical Ethical Committee (METC 06-3–066) and carried out in accordance with the Declaration of Helsinki. The study was conducted by a research assistant and a master’s student from Tilburg University. Before approaching potential participants, permission was asked from the treatment coordinator. After permission, participants received oral information about the study and a letter describing the design and rationale for the study, including the nature of the task (i.e., filling out two questionnaires). Patients were given a 2-week decision window before giving their written informed consent to the study procedure including collection of specific file information.
Statistical Analyses
All analyses were conducted using the Statistical Package for the Social Sciences, version 27. The analyses were specified prior to data collection and no cases were excluded from the analyses. Group differences between psychopathy levels were assessed with a one-way ANOVA. Given the non-significant difference between groups, psychopathy was not added as a covariate. Differences between early maladaptive schemas and emotional states were examined using one-way multivariate ANOVAs, with the EMS and emotional state domains as dependent variables and group as independent variable. To adjust for multiple hypotheses testing, we Bonferroni corrected our alpha by dividing the alpha of .05 by the number of hypotheses (i.e., .05/2 = .025). When omnibus tests were significant, they were followed by Tukey post hoc analyses to investigate differences between groups. While Shapiro-Wilk tests suggested that the YSQ-S3 and SMI-R data was largely not normally distributed (p < .05), ANOVAs are commonly regarded as robust against the assumptions of normality (Blanca et al., 2017; Knief & Forsmeier, 2021), thus no non-parametric alternatives were conducted. Similarly, outliers were detected using multivariate analyses in 12 participants with regard to all assessed domains. 3 Since ANOVA is not routinely considered to be robust against outliers, analyses were run with and without outliers included and the results were compared. Unless otherwise noted, the outliers did not affect the overall results and were thus included in the analysis. In our sample, the eta squared effect sizes (η2) were interpreted as follows: η2 = 0.01 indicates a small effect; η2 = 0.06 indicates a medium effect; η2 = 0.14 indicates a large effect.
Results
Mean and Standard Deviations for the Schema and Mode Domains of the YSQ-S3 and SMI-R.
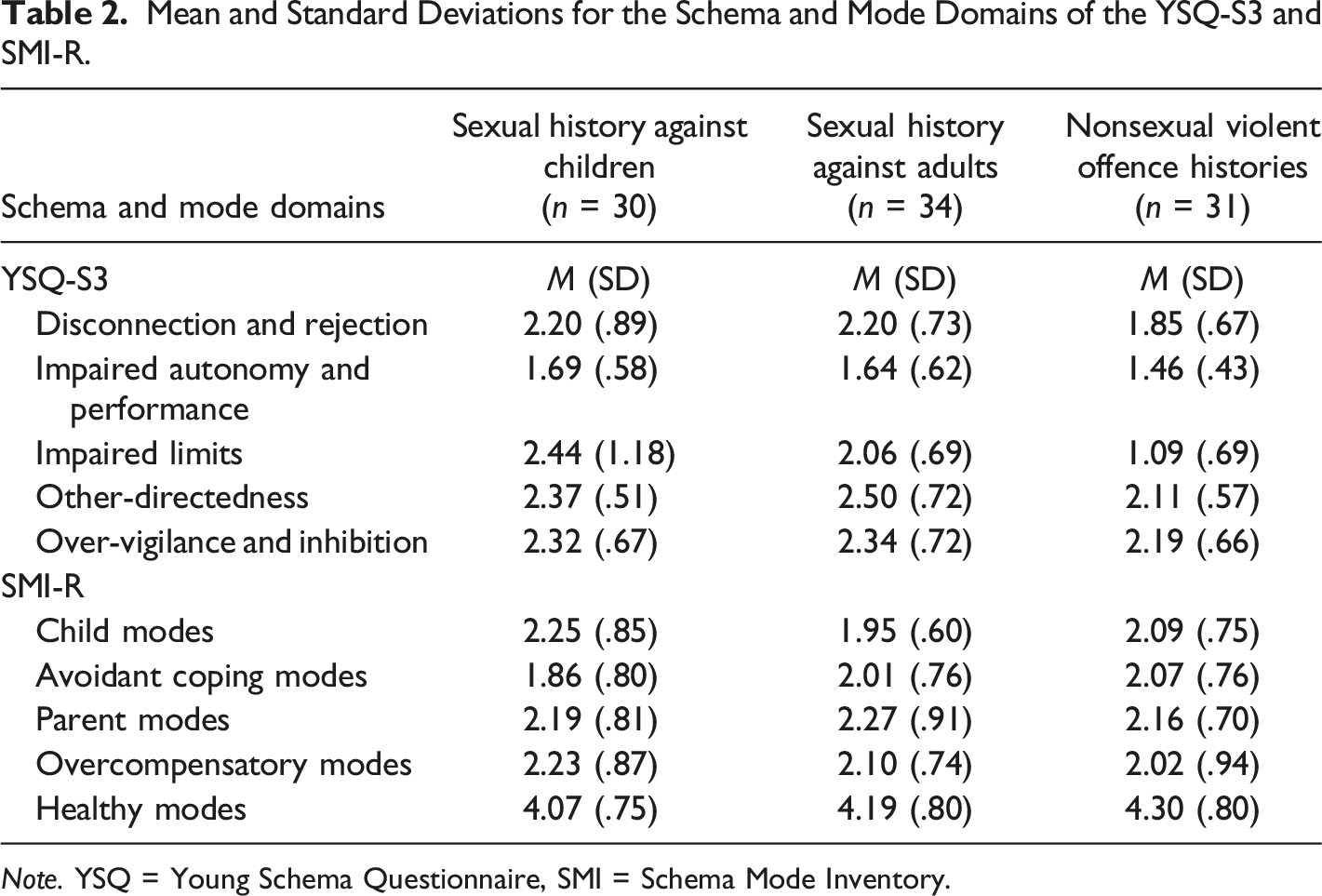
Note. YSQ = Young Schema Questionnaire, SMI = Schema Mode Inventory.
Group Differences in Early Maladaptive Schemas
With regards to hypothesis 1, no differences were found between individuals with nonsexual violent offence histories, sexual offence histories against children and sexual offence histories against adults. Thus, all three types of patients were equally likely to endorse maladaptive schema related to overvigilance (F (2, 90) = .747, p = .477, η2 = .016; 95% CI [.000–.084]) and impaired autonomy and performance (F (2, 92) = 1.96, p = .146, η2 = .042; 95% CI [.000–.133]). Unrelated to the present hypothesis, no differences between groups were found for impaired limits (F (2, 90) = 3.28, p = .042, η2 = .068; 95% CI [.000–.172]), other-directedness (F (2, 92) = 3.372, p = .039, η2 = .069; 95% CI [.000–.175]), and disconnection and rejection (F (2, 92) = 2.30, p = .106, η2 = .049; 95% CI [.000–.144]).
Group Differences in Emotional States
With regards to hypothesis 2, no differences were found between individuals with nonsexual violent offence histories, individuals with sexual offence histories against children or sexual offences against adults. Thus, all three groups were equally likely to endorse schema modes that refer to experiencing child modes (F (2, 94) = 1.273, p = .285, η2 = .027; 95% CI [.000–.105]) avoidance modes (F (2, 94) = .636, p = .532, η2 = .014; 95% CI [.000–.076]) and overcompensatory states (F (2, 94) = .643, p = .528, η2 = .014; 95% CI [.000–.077]). Unrelated to the hypothesis, no differences were found for endorsement relating to parent mode (F (2, 93) = .044, p = .957, η2 = .001; 95% CI [.000–.012]) and healthy modes (F (2, 94) = .692, p = .503, η2 = .015; 95% CI [.000–.079]). No changes to the overall findings were detected after removing outliers.
Discussion
The current study explored early maladaptive cognitive schemas and emotional states in patients convicted for sexual violence against adults and children, compared to patients convicted for nonsexual violence, and aimed to contribute to the existing knowledge and available literature on schema therapy elements in forensic inpatient samples. Our sample size per offence group was similar to previous research in prison samples (e.g. Carvahlo & Nobre, 2014; approx. N = 30 per offence group) and similar to Chakhssi et al. (2013; approx. N = 20 per offence group). In our study, the average EMS domain scores were relatively similar to Chakhssi et al. (2013), the only other study that was also conducted in mandated inpatient care.
Our study revealed no group differences with regard to early maladaptive schemas indicating overvigilance, impaired autonomy, and disconnection. A considerable proportion of individuals with sexual offence histories, or nonsexual violent offence histories for that matter, are exposed to childhood adversities such as abuse and neglect, and household violence (Levenson et al., 2016; Segeren et al., 2020). It might be that, in both offence groups, their detection of anger puts them in a similar hypervigilant state (Craig & Zettler, 2021). We hypothesized that people with sexual offence histories against children would endorse more schemas referring to disconnection compared to those who have sexually offended against adults. Our findings failed to support this hypothesis. The findings are, however, in line with research that shows that individuals with sexual offence histories generally have problematic social and relationship skills that interfere with their sense of belonging and connection (Martin & Tardiff, 2015; Weldon, 2016). Social and relational experience is greatly influenced by the quality of the attachment bond that is formed between a child and their parent/caregiver during childhood. Forensic patients with sexual offence histories (either against children of adults) have often experienced childhood relationships that transgressed healthy boundaries (Craissati, 2015; Drury et al., 2017), which may have impacted their sense of connection to others and sense of autonomy later in life. Also, because of the involuntary nature of the admission in secure hospitals, patients may perceive their treatment as coercive (Adshead & Davies, 2016). Patients across all offence groups may feel constraint of freedom and attacked in their feelings of autonomy.
We failed to find support for the hypothesized differentiation in emotional states between patients with sexual abuse histories against children and adults. There were no differences with regard to child, avoidant and overcompensatory schema modes. Child modes are parts of the self (or representations of the self) which came into being in childhood in response to received parenting and childhood experiences. This mode domain harbors the emotional pain (e.g., loneliness, shame), beliefs and behaviors belonging to childhood (Jacob & Arntz, 2013). The avoidant mode domain is characterized by interpersonal and situational avoidance whereas overcompensatory states refer to extreme attempts to compensate for painful feelings (i.e., child modes; Jacob & Arntz, 2013). Schema modes develop gradually during childhood or adolescence, and the coping modes (i.e., avoidant and overcompensatory modes) serve to safe-guard against harm and emotional pain (Young et al., 2003). The similarity in endorsement of these modes may be explained by the fact that our sample consist of a selective population. First, the prevalence of adverse childhood experiences may be high in both patients with sexual offence histories and patients with nonsexual violent offence histories. For example, Bruce & Laporte (2015) showed that when someone experienced trauma before the age of 15, the chance of becoming violent was 2.8 times higher compared to having no traumatic experiences. Levenson et al. (2016) showed that, compared to males in the general population, people with sexual offence histories were 13 times more likely to experience verbal violence, four times more likely to experience emotional neglect, three times more likely to experience sexual abuse during childhood and twice as likely to experience physical violence. In our sample, patients with nonsexual violent offence histories might be just as traumatized as those with sexual convictions. Second, recent research shows that patients with sexual offence histories against adults who receive treatment on behalf of the state (just like in our sample), could be less aggressive or hostile and more sexually motivated. For example, Schippers and Smid (2021) examined attitudes towards women in a sample of high risk patients convicted for rape (N = 42), patients with nonsexual violent convictions (N = 65) and community controls (N = 42) by means of self-report and implicit measures. Results showed that the patients with rape convictions score low on hostility towards women (Schippers & Smid, 2021). The study took place at a Dutch high secure hospital, just like our study. The patients who receive this treatment on behalf of the state might be qualitatively different from typical patients with sexual offence histories. Furthermore, research showed that forensic patients who have committed a sexual offence may cause fewer aggressive incidents compared to forensic patients who have committed a non-sex violent offence (Huitema et al., 2021), although the true prevalence of aggressive incidents in forensic psychiatric hospital may be difficult to establish.
Our study revealed no group differences with regard to early maladaptive schemas nor schema modes. Also, the mean scores on the YSQ and SMI were relatively low compared to most studies, whether in related population or not. Most studies report higher average scores on both instruments than that we report in our study. For example, in the study by Dunne et al (2018), prisoners reported high levels of early maladaptive schemas and schema modes (i.e., scores ranging from 2.7 to 3.8). In the previous sections, we discussed possible substantive arguments as to why there are no differences between the three groups. Those sections assumed that early maladaptive schemas and schema modes play a role in patients with (sexual) offense histories. However, an alternative explanation is that neither play a significant role in Dutch forensic patients who are admitted to treatment on behalf of the state.
Strengths and Limitations
This study has a number of strengths that support the generalizability of our results. First, our groups were homogenous which allow for a meaningful analysis of the subgroups. Another strength of our study design was the inclusion of a nonsexual violence control group to compare to two sexual offending group.
The findings of our study should be considered in the light of certain limitations. First, our study had a cross sectional design, therefore no inferences can be made about causal relationships. Another limitation was the reliance on a convenience sample and self-report measures to assess EMSs and emotional states which always carry the risk of social desirable responding; participants may under- or over-report their EMSs and emotional states (Keulen-de Vos et al., 2011). Future studies should examine the use of implicit measures to assess schemas, use other methods to assess emotional states (e.g., observations made by professionals), and assess EMS measures alongside measures that assess sex-offending specific implicit theories. Also, emotional states were defined as “schema modes” which refer to a combination of emotion, cognition and behavior; we did not study emotions in a pure sense. Future research should disentangle schema modes and measure affect and mood, physiological arousal and cognitive aspects separately. Finally, the sample sizes per group were relatively small which may reduce the generalizability of our findings. Future studies should clarify the relationship between EMSs, schema modes and risk factors for sexual offending, including sexual deviance, intimacy problems and impulsivity. Also, it would be interesting to examine whether EMSs and schema modes in individuals with sexual offence histories change over time during treatment. Our sample had been hospitalized for an average of 3.5 years and their EMS and modes upon admission are likely to have been impacted by their stay.
Conclusion
The present study adds to the emerging literature on understanding schema therapy elements in offending samples, specifically to understanding forensic patients with convictions for sexual violence. In our study forensic patients with sexual offence histories against children and adults seemed to make equal use of specific maladaptive cognitive schemas and schema modes while being admitted to mandated inpatient care. Furthermore, these patients were not markedly different from people with nonsexual violent convictions with regard to these schema therapy elements. Future studies is warranted to examine whether therapists should consider similar schema and mode domains when treating forensic patients with various offence histories.
Footnotes
Acknowledgments
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results. We thank the participants for taking part in this study and the board of directors of both high secure hospitals for their support.
Declaration of Conflicting Interests
We have no known conflict of interest to disclose and received no financial support for the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.