
Abstract
A person convicted of sex offences (PCSO) is confronted with several challenges upon re-entry to the community, often facing difficulties accessing housing and employment, and experiencing stigmatisation, hostility and harassment from community members. Given the importance of community support for successful reintegration, we examined differences in public (N = 117) attitudes toward a PCSO against a child (PCSO-C) with mental illness or intellectual disability compared to a neurotypical PCSO-C in an online survey. At present, differences in attitudes towards these groups has not been explored. Results indicated the PCSO-Cs with intellectual disability or mental illness were seen to pose less risk of sexual reoffending and prompted higher levels of reintegration comfort than the neurotypical PCSO-C. Participants’ prior personal exposure to mental illness or intellectual disability was unrelated to attitudes, but those who believed that PCSOs in general have a low capacity for change attributed greater risk of sexual reoffending, greater risk of future harm to children, higher levels of blame and lower reintegration comfort, regardless of MI and ID information. Female participants also perceived greater risk of future harm to adults, and older participants estimated higher risk of sexual reoffending than younger participants. Findings have implications for community acceptance of PCSO-Cs and jury decision-making processes and highlight the importance of public education regarding neurodiverse PCSO-Cs and PCSO capacity for change to encourage knowledge-based judgements.
A person convicted of sex offences (PCSO) is confronted with several challenges upon re-entry to the community following release from prison. They often have difficulties in securing stable housing and employment as a result of their conviction (Clark, 2007; Levenson & Cotter, 2005), and can face stigmatisation, threats and harassment and physical assault by community members due to their ‘sex offender’ label (Tewksbury, 2005; Tewksbury & Lees, 2006). Successful community reintegration is heavily influenced by the level of social support demonstrated in community within which they are placed upon release (Burchfield & Mingus, 2014). Similarly, a lack of prosocial support is a key predictor of sexual recidivism (Bahr et al., 2010; Hochstetler et al., 2010). Importantly, public opinions and attitudes are often taken into account in the formation of government legislation that guides the reintegration of people convicted of sexual offences into the community, such as ‘sex offender registration’ and notification requirements, which can have additional implications for successful re-entry (Levenson, D’Amora, & Hern, 2007; Mercado et al., 2008).
Background
Attitudes towards people who have been convicted of sex offences are generally found to be more negative than those toward other types of offenders (Gakhal & Brown, 2011), with individuals who have committed a sexual offence against a child (PCSO-C) being further discriminated against (Sanghara & Wilson, 2006). Those attitudes held by the general public can impact on the nature of related sex-offence legislation (Schiavone & Jeglic, 2009). While social policies such as ‘sex offender registration’, community notification and residency restrictions are primarily designed and put in place to protect the community from risk (Lees & Tewksbury, 2006; Petrunik, 2003), there is little evidence that these policies have been effective in reducing sexual violence (Levenson, Brannon, et al., 2007). This may serve to further fuel the inaccurate elevated perceptions of risk and limited reform potential that the general population hold regarding those convicted of sex offences. The portrayal in the media is also thought to contribute to and exacerbate erroneous representations of these individuals, often depicting them as chronic predators and social outcasts (Levenson, D’Amora, & Hern, 2007; Malinen et al., 2014). Media coverage labels these individuals as ‘monsters’ and ‘perverts’ (Cucolo & Perlin, 2013); such language is dehumanising and individuals who have committed a sex offence are seen to be undeserving of moral or legal rights (Spencer, 2009). Three particular stereotypes directed towards PCSOs are suggested to facilitate these negative public perceptions: (1) that their victims are most often strangers; (2) that their offences are driven by immorality, sexual deviance and selfishness; and (3) that those who have committed a sex offence are unreformable (Quinn et al., 2004; Sample & Bray, 2003; Spencer, 2009). These stereotypes strengthen the endorsement of a ‘get tough’ punishment approach to sex-offence specific treatment over and above rehabilitation and reintegration efforts (Pickett et al., 2013).
Research demonstrates public discomfort with the idea of living near an individual who has been released following a sex offence conviction (Willis et al., 2013), eliciting fear and discomfort (Kernsmith et al., 2009). Effective treatment and reintegration of people who have committed a sex offence are heavily impacted by the way in which they are perceived and treated by both mental health professionals and neighbours within the community (Marshall et al., 2003); individuals incarcerated for a sex offence report higher re-entry concerns related to housing and employment than those convicted of other offences (Baker et al., 2021). Upon release, they report experiencing harassment from neighbours, problems in securing employment and difficulties in protecting family members from being targeted as a result of their relationship with the individual (Levenson & Cotter, 2005; Tewksbury, 2005; Tewksbury & Lees, 2006). This emphasises the importance of general public attitudes towards this group in facilitating successful reform, and so an increased understanding of the factors associated with these attitudes is crucial.
One such factor that may influence public attitudes towards someone convicted of a sex offence is the presence of a condition that may be perceived to somewhat explain the offence behaviour, such as intellectual disability or mental illness. If people believe that an offence was committed by someone with full capacity for understanding, decision making, and behavioural control, it is possible that their estimation of factors like risk and blame will be elevated in comparison to a convicted individual who is not seen as meeting these criteria. However, there is limited empirical evidence as to the impact of these factors on public opinion, especially where mental illness is concerned.
Public Attitudes Towards Individuals with Intellectual Disability and Mental Illness
It is well-documented that the general public’s attitudes towards an individual can vary based on whether they are given a label of ‘intellectually disabled’ or ‘mentally ill’. For example, social distance is a measure used when investigating public attitudes toward individuals with an intellectual disability that reflects the willingness to recognise, be associated, or live with a certain group or individual (Harth, 1971). A study carried out by Scior et al. (2013) found that the general public demonstrate reduced social distance toward individuals who have a label of intellectual disability, suggesting that providing such a label may reduce misattribution of stigmatised beliefs. Additionally, those with education or previous experience of intellectual disabilities are seen to hold more positive attitudes in terms of social distance and comfort (Morin et al., 2013; Ouellette-Kuntz et al., 2010). This may suggest that recognition of intellectual disability and education are vital parts in the formation of attitudes towards individuals with such a diagnosis.
On the other hand, individuals with mental illness are often automatically attributed with dangerous behaviours, despite evidence that people with a mental disorder are unlikely to be any more dangerous than neurotypical individuals (Pescosolido et al., 2019). This contrasts with literature that demonstrates that the public perceive individuals with mental illness as more violent and dangerous (Jorm & Reavley, 2014; Stuart, 2003; Varshney et al., 2016). This has largely been ascribed to sensationalised media coverage depicting those with mental illness as more inherently violent and less predictable than those without mental illness (Ciydem et al., 2020). For instance, Battaglia et al. (2022) examined the general public’s perceptions following exposure to online media posts reporting real incidents of individuals with schizophrenia committing criminal offences. They found that participants reported increased intended social-distancing and perceptions of dangerousness towards the perpetrators in the incidents, and this increase was magnified when no clinically relevant contextual information was provided in the post itself (i.e., regarding the treatment of schizophrenia, access to appropriate healthcare, clinician opinions and research on mental illness and crime). As a result of media depictions of mental illness and individual attitudes, prejudiced beliefs toward mental illness can lead to support for coerced treatment, seeing such measures taken against individuals with schizophrenia in particular as warranted given their diagnosis (Pescosolido et al., 2019). Similar to intellectual disability, reduced social distance has also been associated with awareness and knowledge about mental illness. This may suggest that prejudiced beliefs about individuals with mental illness could be linked to lack of education (Henderson et al., 2020). However, considerably less research has examined differential general public attitudes towards a person convicted of a sex offence presented as having an intellectual disability or mental illness.
Attitudes towards PCSOs with Intellectual Disability
Individuals diagnosed with an intellectual disability are at an increased risk of contact with the criminal justice system and exhibit heightened rates of reoffending and recidivism compared to those without an intellectual disability diagnosis (Camilleri & Quinsey, 2011; Lindsay et al., 2011). While the overall offending rate of those with intellectual disability is lower than the general population (Day, 1994), the prevalence of sex offences in offending individuals with intellectual disability is suggested to be up to six times higher, suggesting overrepresentation of this offence category within this group (Day, 1994; Hawk et al., 1993). However, this is likely attributed to a plethora of factors that put those with an intellectual disability at an increased risk of offending, being apprehended and being convicted. For example, impulsivity is inherent in many intellectual disabilities, and impairment in decision-making and planning abilities can lead to easier detection by authorities (Hickson & Khema, 2013). Once apprehended, these individuals are also more likely to comply with or try to please authority figures (Kebbell & Hatton, 1999), and can have difficulty comprehending their rights, legal proceedings, or the consequences of what they divulge during an interrogative interview (Cederborg et al., 2009; Kebbell et al., 2004). More recently, researchers have begun to explore whether attitudes towards people convicted of a sex offence vary based on the presence of an intellectual disability diagnosis. Steans and Duff (2018) found that both forensic staff and the general public attributed lower levels of blame to a convicted individual with an intellectual disability compared to one without. It is suggested that those who believe criminal acts are the result of external circumstances and constraints are likely to be less punitive (Maruna & King, 2009). This may explain why the general public might attribute reduced levels of blame to a person convicted of sex offences who also holds an intellectual disability diagnosis.
Similarly, the general public have also been seen to hold more positive attitudes towards community reintegration of people who have committed a general (non-sexual) offence with intellectual disability than those without a diagnosis (Worthington & Rossetti, 2020). This may suggest that the presence of an intellectual disability may reduce anxiety and discomfort around community placement of a person convicted of a sex offence. However, where an element of conscious cognitive planning of the offence is evident, general public reintegration comfort has been seen to significantly reduce (Steans & Duff, 2018). This emphasises the importance of the interplay between perceived blame (i.e., accountability based on cognitive impairment) and willingness to accept an individual being reintegrated into one’s community. It is therefore important that the extent to which an offence is planned is controlled for when examining differences in the attribution of blame and reintegration comfort of a person with an intellectual disability who has been convicted of a sex offence.
Despite reduced estimates of blame and increased reintegration comfort for those with an intellectual disability diagnosis (where the crime is deemed to be unplanned), the general public have been found to perceive a higher risk of physical harm to those working to support those with an intellectual disability (Steans & Duff, 2018). Additionally, Westphal (2020) found that participants from the general population estimated equal levels of risk for those convicted of sex offences with and without an intellectual disability. This may be a product of the presumed uncontrollability of sexual behaviours in some intellectual disabilities, which even forensic care staff report as being a core element or characteristic of the individual’s personality, rather than something that can be consciously controlled (MacKinlay & Langdon, 2009). This highlights that the presence of such a condition could influence separate elements of general population attitudes (risk, blame, reintegration comfort) in differential ways. It can be argued that the extenuating circumstances imposed by intellectual disability may be similar to those inflicted by certain mental illnesses (Raffard et al., 2009). However, to date, this has received little attention.
Attitudes towards PCSOs with Mental Illness
Studies conducted in Europe, the United States and Australia estimate that PCSOs are up to 6 times more likely to have previously been hospitalised for a psychiatric condition than the general population, with a 4.8 times higher likelihood of schizophrenia and a 3.4 times higher likelihood of a bipolar affective disorder diagnosis (Brennan et al., 2000; Fazel et al., 2007; Mullen et al., 2000; Pinta, 2001). Compared to the wider prison population, there is a significantly higher incidence of major mood disorders and psychosis-related disorders within this group; though it should be noted that symptoms are largely more severe in those placed in psychiatric residential settings or who have additional paraphilia diagnoses (Stinson & Becker, 2011). The pervasive link between offensive sexual behaviours and major disorders such as schizophrenia is a complex one. There is debate in the literature as to whether psychosis symptoms are related directly or indirectly (or both) to sex offence behaviour. For example, Fazel et al. (2007) note that the risk factors for sexual offending in those with schizophrenia are not necessarily different to those without a diagnosis (e.g., cognitive distortions, sexually deviant fantasies, social skill deficits). However, they acknowledge that episodes of psychosis may induce disinhibition that may interact with these more chronic risk factors and result in offence behaviour.
People convicted of sex offences who are diagnosed with major mental illness (e.g., schizophrenia; Craissati & Hodes, 1992) are thought to experience heightened stigmatisation, as they represent two widely marginalised social groups (Guidry & Saleh, 2004). As discussed earlier, the presentation of those with disorders involving elements of psychosis (e.g., schizophrenia) in the media is often highly negative, resulting in public perception of these individuals as potentially more likely to engage in offensive or violent behaviours (Battaglia et al., 2022; Ciydem et al., 2020). While one study did find that mock jurors considered schizophrenia to be a mitigating factor in sentencing decisions, with participants less likely to assign a death sentence in cases where the defendant had this diagnosis (Barnett et al., 2004), there is no research evidence to indicate whether the wider opinions of the general public regarding those who have been convicted of sex offences are influenced by the presence of major mental illness (e.g., schizophrenia).
The Current Study
This research addresses this gap in the literature by investigating potential differences between public attitudes toward individuals with intellectual disability (ID) or mental illness (MI) who have committed a planned sex offence against a child (PCSO-C) compared to a neurotypical PCSO-C. In the context of this study, the term “neurotypical” reflects an individual who does not display any symptoms of intellectual disability or mental illness. We explored differences across five factors: (1) perceived likelihood of reoffending, perceived risk of future harm posed to (2) children and (3) adults, (4) attributed blame for the offence, and (5) comfort at reintegration of the individual into their own community. Further, we examined the impact of participant’s prior exposure to mental illness and intellectual disability and their general attitudes towards PCSOs on their attitudes towards each individual. This allowed for a fine-grained, multivariate investigation as to the general public’s potentially varying attitudes towards PCSO-Cs diagnosed with an intellectual disability or mental illness in comparison to an individual who has committed such an offence without any indication of MI or ID symptomology. If these attitudes can be understood, progress can be made in terms of clarifying the public’s understanding of the impact of ID and MI on criminal culpability and potential for successful reintegration. Based on the literature outlined above, it was predicted that: (1) Ratings of blame would be lower for the PCSO-C with ID or MI than the neurotypical PCSO-C. (2) Ratings of risk of harm and reoffending would be higher for the PCSO-C with ID or MI than for the neurotypical PCSO-C.
Hypotheses 1 and 2 were based on the prior literature that indicates that those with an ID or MI may be perceived to be limited in terms of cognitive capacity and/or behavioural control, which may lead the public to attribute their behaviour to elements of their condition, but also to deem them substantially more dangerous in terms of risk (e.g., Barnett et al., 2004; Maruna & King, 2009; Worthington & Rossetti, 2020). (3) Scores on reintegration comfort would be higher for the PCSO-Cs with ID than the MI and neurotypical PCSO-Cs.
Hypothesis 3 was based on evidence that indicates that the general population are less threatened by the social closeness of those with ID, while those with MI are often misattributed ‘dangerousness’ stereotypes (e.g., Connolly et al., 2013; Morin et al., 2013; Ouellette‐Kuntz et al., 2010; Pescosolido et al., 2019).
Method
Participants
According to an a-priori power analysis (G*Power 3.1), a total sample of 85 participants was required to achieve 95% power in detecting a medium effect size, with an analysis from within the F-test family (based on α = .05). In order to allow for the possible removal of outliers or missing data, a final sample of 117 participants was recruited (male = 35, female = 82) with an age range of 17–59 (M = 27.3, SD = 11.5). Our sample was composed of 113 participants based in the United Kingdom (72 in Scotland, 17 in England, 1 in Wales, and 1 in Northern Ireland; 22 unknown), 3 based in Spain, and 1 based in Turkey.
In terms of having personal experience/diagnosis of mental illness, 59 participants responded “yes” and 58 “no”. In terms of having a known associate with experience/diagnosis of mental illness, 97 responded “yes”, whereas only 20 responded “no”. In terms of having personal experience/diagnosis of intellectual disability, only 11 participants responded “yes” and 106 “no”. In terms of having a known associate with experience/diagnosis of intellectual disability, 55 responded “yes”, whereas 62 responded “no”. To maintain a sense of balance for between-groups comparisons, personal experience of MI was taken forward rather than known associate, whereas association with an ID individual was taken forward, rather than personal.
Participants were recruited through the use of social media (primarily Facebook and Twitter), with the research team and host institution advertising the study to wide networks on both personal and professional profiles, asking participants to further share with their own networks following participation to facilitate diverse recruitment. The only inclusion criteria was that the individuals were over the age of 16 (the local age of legal adulthood) and no compensation was provided to participants. The participant advertisement provided the institutional ethical approval code and read “We are looking at the general public’s (aged 16 and over) attitudes towards people who have committed a sexual offence. If you feel this is something that would upset or trigger you, please do not take part. You can find out more information and access the survey here: [survey link] We aim to recruit as many people as possible so please re-share with friends and family. If you have any questions, please email me us at [researcher email address]”.
Materials
A short demographic questionnaire (age and gender identification) was completed before the following questionnaires.
General Attitudes Towards those who have Committed a Sex Offence
The Community Attitudes Towards Sex Offenders Scale is an 18-item questionnaire (Church, Wakeman, Miller, Clements, & Sun, 2007) which aims to evaluate the participants general attitudes towards PCSO. There are four sub-scales, relating to: social isolation (i.e., the perception that people convicted of sex offences are isolated from society and struggle to form relationships), capacity to change, severity/dangerousness, and deviancy. Participant responses are placed a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), with high scores indicating more negative attitudes towards individuals who have committed a sex offence. Analysis of the current data set revealed that the social isolation subscale had good reliability (α = .718), as did the capacity for change subscale (α = .865). However, the severity subscale (α = .526) and the deviance subscale (α = .134) did not demonstrate appropriate reliability. As such, only the social isolation and capacity for change sub-scale data will be included in subsequent analyses.
CSO Vignettes
The vignettes created for this study were based on the vignette used by Steans and Duff (2018). Permission was received from the authors to use the initial vignette depicting a PCSO-C with an intellectual disability. Further, two additional vignettes were created by the researchers to reflect a PCSO-C with a mental illness and a neurotypical PCSO-C. Hogue and Peebles (1997) identified that when offenders were presented as acting with intent, they received a harsher sentence, were attributed more blame and responsibility and were seen as more deserving of punishment. For this reason, all three vignettes controlled for the possibly confounding impact of perceived impulsivity of the offence (Steans & Duff, 2018) by indicating the offence was planned. The vignettes are as follows:
PCSO-C with an Intellectual Disability
‘Jason has a learning disability and is detained within a secure facility. As a child Jason struggled to progress at school and was sent to a school designed for children with special needs. As an adult Jason requires support to complete day to day tasks. He lacks independence because of an inability to take care of himself. Jason sometimes struggles to communicate with other people. He feels what he says often isn’t understood and he regularly does not understand what is being said to him. Jason’s learning disability is classed as moderate and he has an I.Q. score of 50. Jason is also a sexual offender and is detained due to a sexual assault against a child. Jason planned his offence over a number of months, in order to gain access to his victim.’
PCSO-C with Mental Illness
‘Mark has a mental illness and detained in a secure facility. Growing up, Mark struggled with his sense of reality and hallucinations and was sent to a hospital for inpatient care. As an adult, Mark struggles on a day-to-day basis with a variety of issues. He finds it difficult to make friends, has severe issues of telling between reality and hallucination, has cognitive issues and an odd manner of thinking and speaking. Mark is also a sexual offender and is detained due to a sexual assault against a child. Mark planned his offence over a number of months, in order to gain access to his victim.’
Neurotypical PCSO-C
‘Ben is a typical individual who had a nice childhood and did his best at school. He didn’t have an issue making friends and considered himself to have a good life. As an adult, Ben had a good job and worked hard. Ben is also a sexual offender and is detained due to a sexual assault against a child. Ben planned his offence over a number of months, in order to gain access to his victim.’
After reading each of the vignettes in a randomised order, participants responded to the same six questions using a 5-point Likert scale. These questions reflect the participants’ attitudes on risk of harm, risk of reoffending, blame attribution and comfort at community reintegration. The questions were: 1. How likely do you think it is that X will commit another sexual offence in the future? (1 = very unlikely, 5 = very likely); 2. How likely do you think it is that X will commit another offence in the future? (not a sexual offence) (1 = very unlikely, 5 = very likely); 3. How much of a sexual risk does X pose towards adults? (1 = very low risk, 5 = very high risk); 4. How much of a sexual risk does X pose towards children? (1 = very low risk, 5 = very high risk); 5. If X was moved into your community, how comfortable would you be with that decision? (1 = very uncomfortable, 5 = very comfortable); 6. X is to blame for sexually assaulting the child (1 = not to blame at all, 5 = entirely to blame).
Mental Illness/Intellectual Disability Exposure
To control for prior exposure to mental illness and intellectual disability, four questions were included. These questions asked if participants had a personal experience or diagnosis of intellectual disability or mental illness and if they knew anyone with a diagnosis of intellectual disability or mental illness. The responses were either ‘yes’ or ‘no’. During analysis, MI and ID exposure variables were created to reflect whether participants indicated ‘yes’ to either of the questions.
Procedure
Following ethical approval from the host university’s Institutional Ethical Review Board, the survey was created using QuestionPro and shared on social media, using a combination of opportunity and snowball sampling. Upon following the URL provided, participants were presented with an information sheet providing details as to what would be required during the study, highlighting the sensitive nature of the content to ensure an informed decision could be made. After reading this, participants completed a digital consent form requiring them to indicate agreement with several statements before being permitted to proceed. After providing consent, participants responded to the demographic questions, followed by the CATSO. Participants then read each of the three vignettes in a randomised order, answering the six questions outlined above after each one. After the vignettes, participants responded to the mental illness/intellectual disability exposure items before being debriefed online. The debrief provided support contact details if the participants felt in any way distressed following participation and provided details of how to remove their data should they wish to do so up to 4 weeks after completion.
Analytical strategy
Prior to inferential analysis, raw data was checked for completeness. Data visualisations were performed (histograms, Q-Q plots) to explore assumptions of linearity and normality, and boxplots were used to determine the position of any outlying data. No transformations were required.
It is common to use general linear model-type analyses to interpret this type of data, despite outcomes being measured by ordinal response categories. Individual scale points might appear equally-spaced but there is no evidence that each participant makes the same judgements as to what constitutes a response at each scale point, nor that every participant’s evaluation of adjacent points is equal (Taylor et al., 2021). Minimally, the relationship between participant responses and underlying latent dimension(s) are underspecified (Taylor et al., 2021). Our analytical approach – Cumulative Link Mixed Models (CLMM) – maps ordinal outcomes against ordered regions of a latent distribution (Bürkner & Vuorre, 2019; McCullagh, 1980). There is clear evidence of the problems in using general linear modelling/ANOVA to evaluate ordinal data sets (Taylor et al., 2021), and the need for CLMM approaches has been successfully argued by, for example, Liddell and Kruschke (2018).
We used the ‘ordinal’ package (Christensen, 2019) in R (R Development Core Team, 2016; http://www.r-project.org) to generate CLMMs. Optimal random effect structures were identified using forward model selection (see Barr et al., 2013; Matuschek et al., 2017). Fixed effects were tested using likelihood-ratio tests comparing full and reduced models (based on the principles of analysis of variance). Post-hoc tests were conducted using the ‘emmeans’ package (v1.4.8, 26/06/20; Lenth et al., 2020); significance thresholds were adjusted using the Bonferroni method. All models included random intercepts by-participants.
Results
Descriptive Statistics.

Note. Values are rounded to two decimal places; standard deviations are shown in brackets; 95% Confidence Intervals (CIs).
Sexual Reoffending
Summary of Cumulative Link Mixed Effects Models – Sexual Reoffending.

Note. * = p is significant at the .05 level.
Follow-up comparisons revealed that there was no significant difference in perceived risk of sexual reoffending between the PCSO-C with ID and with MI (z = −0.83; p > .999), and no difference between the PCSO-C with MI and PCSO-C neurotypical (z = −1.67; p = .288). However, there was a significant difference between perceptions of risk of future sexual reoffending between PCSO-C with ID and PCSO-C neurotypical (z = −2.43; p = .046), with the PCSO-C neurotypical perceived as being at greater risk of such reoffending.
The fixed effect of participants’ Age on perceptions of Sexual Reoffending was also significant. Typically, as participant ages increased so did perceptions of risk (rs = .159, p = .003).
The fixed effect of participants’ CATSO Capacity for Change ratings on perceptions of Sexual Reoffending was also significant. Participants with more negative perceptions of PCSO-Cs were more likely to perceive a greater risk of future sexual reoffending (rs = .146, p = .006).
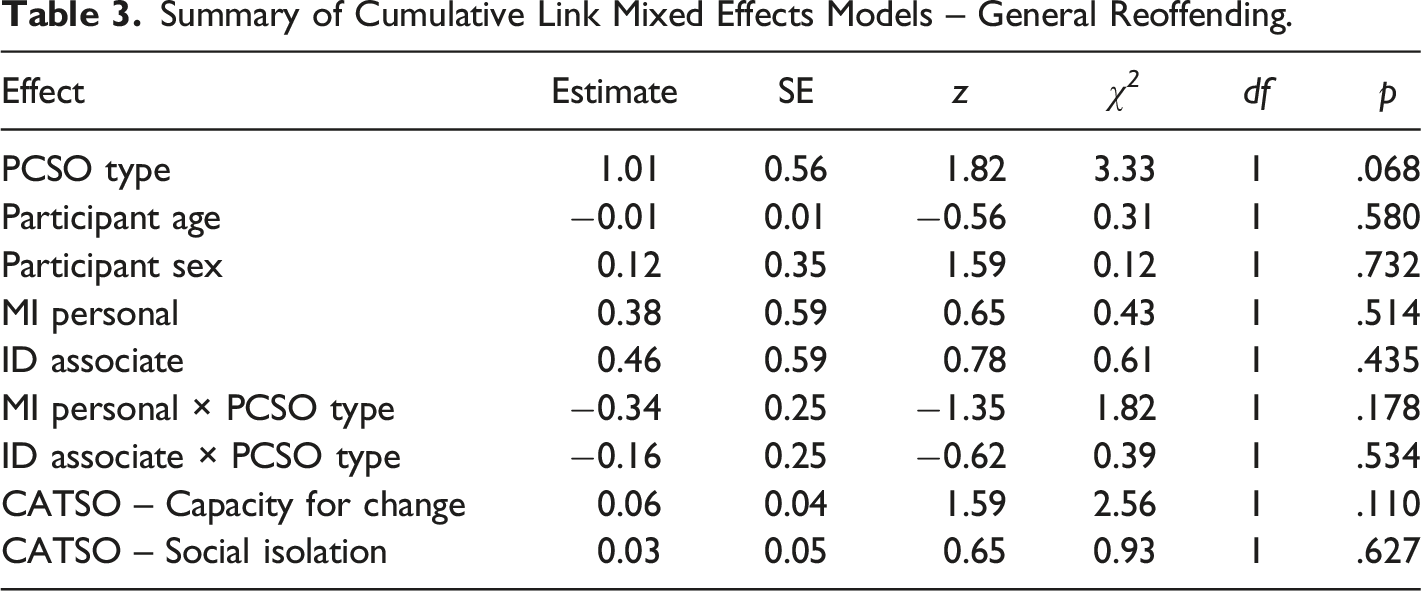
General Reoffending
Summary of Cumulative Link Mixed Effects Models – General Reoffending.
Sexual Risk to Adults
Summary of Cumulative Link Mixed Effects Models – Sexual Risk to Adults.
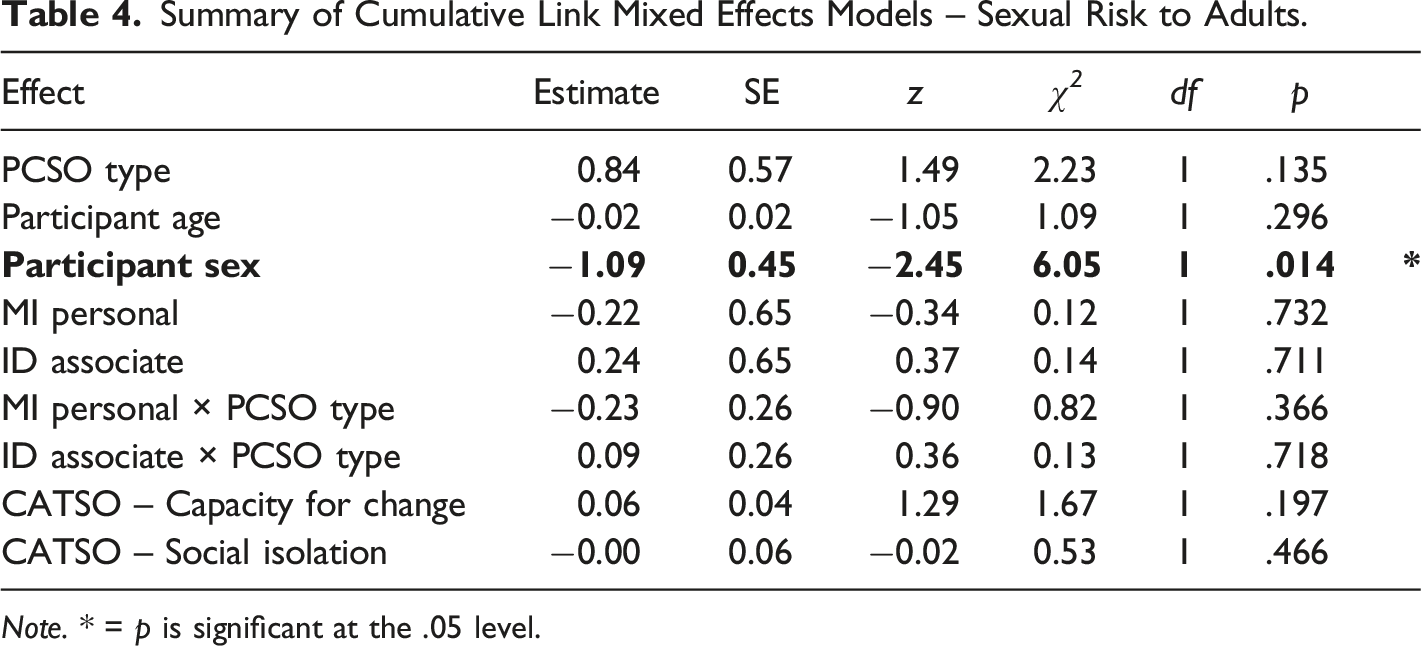
Note. * = p is significant at the .05 level.
Follow up comparisons revealed that female participants perceived PCSO-Cs as posing a greater risk of future sexual harm to adults (z = 2.52, p = .012).
Sexual Risk to Children
Summary of Cumulative Link Mixed Effects Models – Sexual Risk to Children.
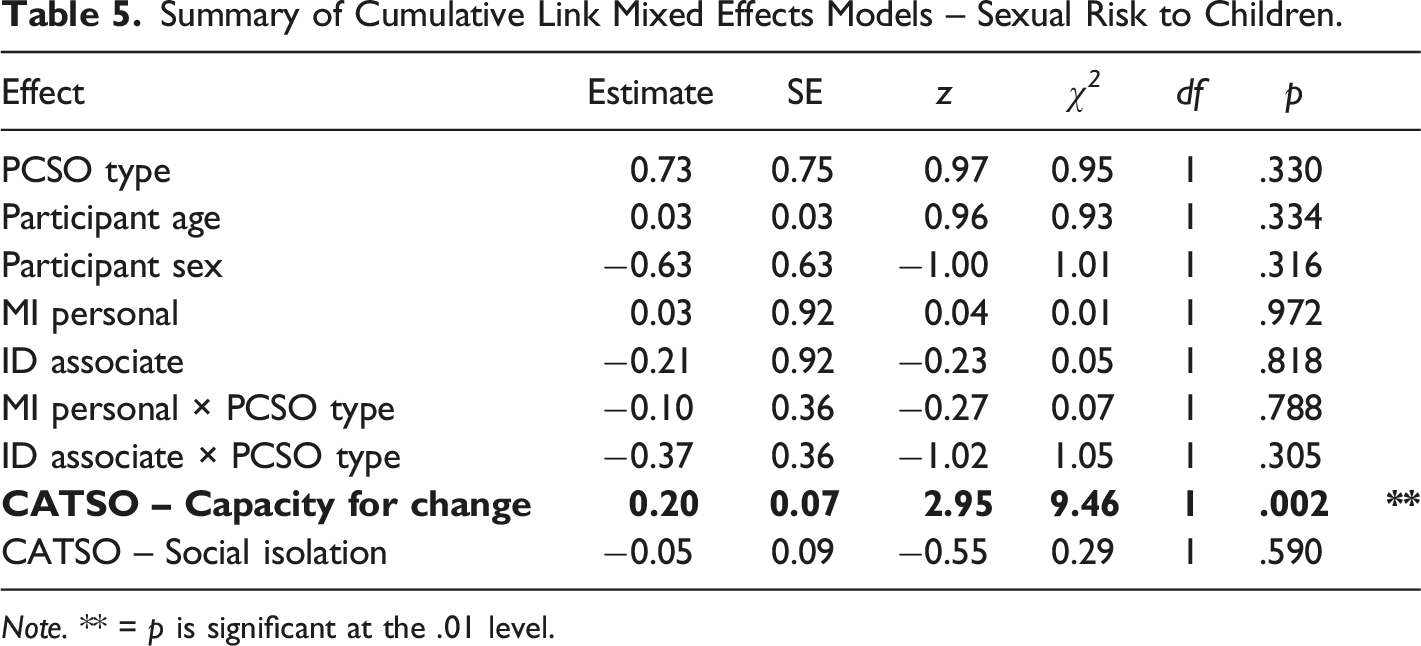
Note. ** = p is significant at the .01 level.
Follow up comparisons revealed that participants with more negative perceptions of PCSO-Cs were more likely to perceive a greater sexual risk to children (rs = .197, p < .001).
Comfort
Summary of Cumulative Link Mixed Effects Models – Reintegration Comfort.
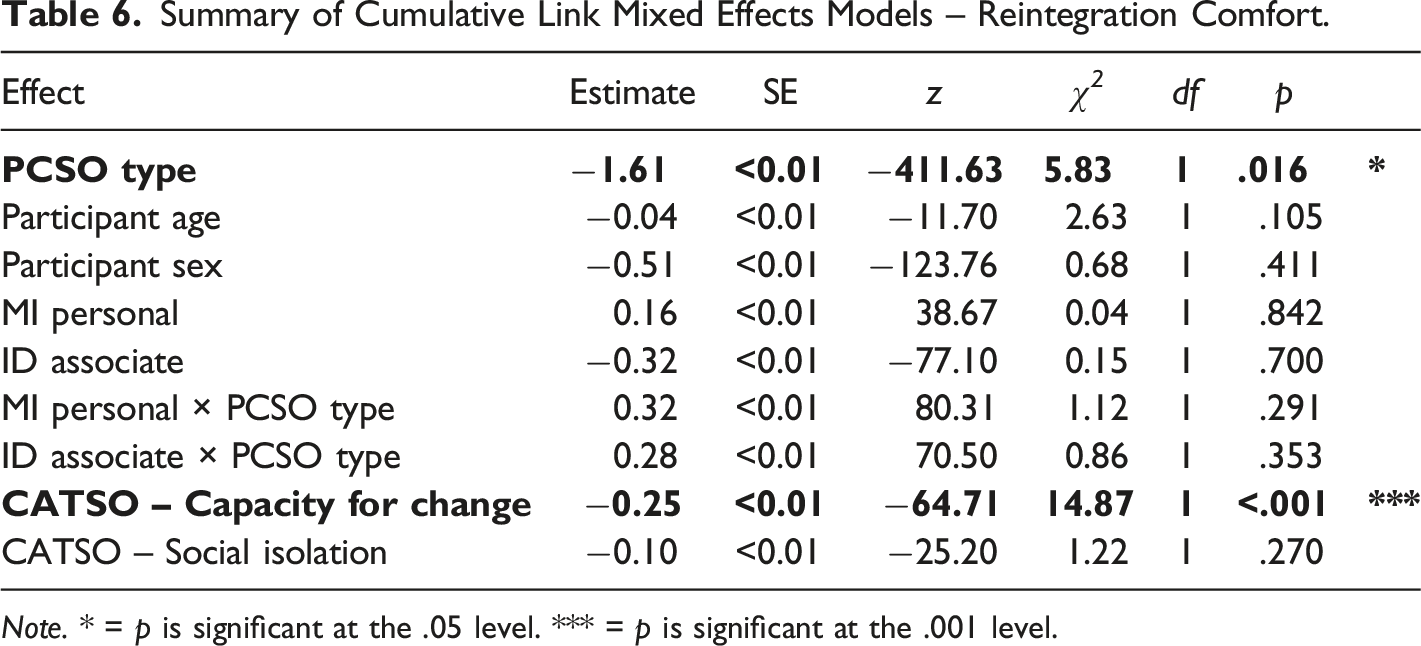
Note. * = p is significant at the .05 level. *** = p is significant at the .001 level.
Follow-up comparisons revealed that there was no significant difference in perceived Comfort between the PCSO-C with ID and with MI (z = 1.36; p = .521). However, there was a significant difference between reported comfort between PCSO-C with ID and PCSO-C neurotypical (z = 4.46; p < .001), with participants reporting less comfort with neurotypical PCSO-Cs than those with ID. Furthermore, there was a significant difference between the reported comfort associated with PCSO-C with MI and PCSO-C neurotypical (z = 3.24; p = .004), again with less comfort associated with the PCSO-C neurotypical than with MI.
The fixed effect of Capacity for Change was also significant. It was found that those with more negative attitudes towards PCSO-Cs were less-comfortable with reintegration (rs = −.318, p < .001).
Blame
Summary of Cumulative Link Mixed Effects Models – Blame.

Note. *** = p is significant at the .001 level.
It was found that those with more negative attitudes towards PCSO-Cs were more likely to blame them for their offences (rs = .242, p < .001).
Discussion
This study investigated differences in public attitudes towards a person who has committed a sexual offence against a child with an intellectual disability or mental illness compared to a neurotypical individual, accounting for the participant’s own prior exposure to both predictors and pre-existing attitudes towards people who have committed sex offences (capacity for change and social isolation). Specifically, differences were explored in terms of perceived likelihood of reoffending, perceived risk of harm posed to both children and adults, blame attributed for the offence, and comfort at reintegration of the individual into their own community.
Differences in Attitudes Based on Mental Illness or Intellectual Disability
Firstly, we predicted that ratings of blame would be lower for the individual with mental illness or intellectual disability than the neurotypical individual (hypothesis 1), while ratings of risk of harm and risk of reoffending would be higher (hypothesis 2). Contrary to our expectations, there was no difference in attributions of blame or risk of future harm between any of the three PCSO-C types. This suggests that, regardless of whether a person convicted of a child sex offence is presented as having symptoms associated with intellectual disability or mental illness (or neither), all are perceived to have a comparable risk of sexual harm to both children and adults following release, which aligns with previous findings (Steans & Duff, 2018). However, Steans and Duff found that the those convicted of child sex offences with an intellectual disability were attributed less blame than one without, which contradicts our current findings. This may reflect the fact that their analysis did not consider the impact of MI/ID status on attitudes whilst controlling for perceptions of capacity for change, which was found to be an independent predictor of blame attribution in the current study.
However, the individuals with mental illness or intellectual disability were seen to pose less of a risk of sexual reoffending than their neurotypical counterpart; thus, we cannot support hypothesis 2. We predicted that reintegration comfort would be higher for the individual with an intellectual disability than with mental illness and the neurotypical individual (hypothesis 3); this was partially supported. While there was a significant difference between reintegration comfort for the individuals with an intellectual disability or mental illness versus the neurotypical individual, there was no differences between the mental illness and intellectual disability conditions themselves. In contrast to literature indicating that the general public perceive those particularly with mental illness as more violent and dangerous (Jorm & Reavley, 2014; Stuart, 2003; Varshney et al., 2016), this suggests that those with mental illness or intellectual disability may actually be perceived to pose less danger to the community than an individual without. It is possible that the indication of mental illness or intellectual disability as a potential underlying causal or contributory factor for the offence behaviour may be more comforting to the general public than the presentation of no identifiable aggravating factors that can be used to explain or excuse the onset of their offence behaviour. It is also possible that reintegration comfort is higher for these individuals, and expectation of sexual reoffence is lower, under an assumption that they will receive more therapeutic support, be more heavily monitored, and receive ongoing treatment for their conditions following release from prison, though this notion requires further investigation.
No significant differences were found in general public attitudes towards the individuals convicted of child sex offences with intellectual disability or mental illness, suggesting that both were considered to be less likely to sexually reoffend than the neurotypical individual, and both were subject to higher levels of comfort at the placement within the community upon release. The current study also sheds novel light on the similarity in public perceptions of those convicted of child sex offences with a mental illness and intellectual disability, which was previously unexplored in the literature, indicating that attitudes may be less punitive towards both groups than towards an individual with neither diagnosis. This aligns with and extends prior findings that the public hold more positive attitudes towards community reintegration of people with intellectual disability who have committed a general (non-sexual) offence than those without a diagnosis (Worthington & Rossetti, 2020). However, interestingly, it has been argued that evidence of conscious cognitive planning of the offence significantly reduces differences between individuals with or without an intellectual disability (Steans & Duff, 2018). Given that our findings indicate increased reintegration comfort for those with intellectual disability or mental illness despite the indication that the offence was planned, it is possible that both diagnoses may still impact on the general public’s willingness to accept someone convicted of a child sex offence into their community over-and-above the planned nature of the offence. However, future experimental work comparing planned and non-planned offences in those with intellectual disability or mental illness is needed to clarify this.
Pre-Existing Attitudes Towards a People Who Have Committed of Sex Offences
Regardless of intellectual disability or mental illness information, participant’s general attitudes towards individuals who have committed a sex offence with regards to capacity for change presented as a strongly significant predictor of sexual reoffending, risk of future sexual harm to children, attribution of blame, and reintegration comfort. Those who reported believing that these individuals have a reduced capacity for change perceived a higher risk of sexual reoffending and future sexual risk to children across all three diagnosis types, attributed a higher level of blame for the offence, and indicated they would be less comfortable with placement of all three individuals within their community. Similarly, prior literature indicates that those with higher pre-existing negative attitudes demonstrate elevated anger and hostility at the notion of these individuals being placed within their community, and an expectation that fellow community members mirror this perspective (Klein et al., 2020). This adds important insight into prior findings, which indicate that mental illness and intellectual disability diagnoses do impact on mock-jurors sentencing decisions due to their potential mitigating effect (Barnett et al., 2004; Mossière & Maeder, 2016), highlighting the importance of considering pre-existing attitudes and understanding of propensity for change in this offence group when examining these decision-making processes.
Impact of Exposure to Mental Illness and Intellectual Disability
Prior exposure to intellectual disability or mental illness did not significantly contribute to attitudes towards the each of the profiles presented. Given that attitudes towards intellectual disability and mental illness have been found to change following increased awareness and understanding of these conditions (Rillotta & Nettelbeck, 2007; Wallach, 2004), we expected that this kind of exposure might make individuals less likely to apply wider violence or deviance stereotypes to a person convicted of a child sex offence with an intellectual disability or mental illness. However, this was not the case within our sample. This contradicts prior research that indicates that those who do not have a relative with schizophrenia (the mental illness depicted in the mental illness vignette) perceive schizophrenic patients to be more dangerous than the average person, while relatives of patients believe this group to pose little risk of harm compared to neurotypical individuals (Grausgruber et al., 2007). Those with familial exposure to this disorder have also been found to demonstrate less stigma and higher tolerance levels to those with a diagnoses (Smith et al., 2011). Furthermore, research also suggests a relationship between familiarity of schizophrenia and perceived dangerousness (Angermeyer et al., 2004). The results highlighted that if an individual is familiar with schizophrenia and the symptoms, they are less likely to perceive individuals with a schizophrenia symptoms to be dangerous. While these findings highlight the importance of exposure to mental illness and intellectual disability in promoting less negative attitudes and reducing stigma against these two marginalised groups, our findings indicate that in the context of a person convicted of a sex offence against a child, prior exposure to mental illness or intellectual disability may be less influential. It is possible that the nature of the crime depicted in the vignettes (i.e., child sexual assault) reflects a level of severity that over-rides any additional empathy or understanding that exposure may arguably bring. Given the nature of the crime, it may be that those who do have experience with intellectual disability or mental illness fail to see similarities between themselves or those close to them and the offender depicted in the vignette, despite shared symptomology.
Age and Gender
Female participants perceived a greater risk of future sexual harm to adults across all three individuals than male participants. This is consistent with previous research as it was found that female participants consider sexual abuse to be more serious when the offender is characterised as male (Banton & West, 2020). This is further supported by the findings of Koon-Magnin (2015) who found that female participants were significantly more likely than male participants to report feeling fear if someone who has committed a sex offence was to move into their neighbourhood. The finding that female participants perceived higher risk is consistent with the findings of Caputo & Brodsky (2004) that women expressed more fear of crime in general, and specifically sexual assault, and could be related to the fact that women are known to be at higher risk to experience sexual abuse (WHO, 2021).
Participant age was also seen to negatively impact on attitudes regarding likelihood to sexually reoffend, regardless of mental illness and intellectual disability information. This contradicts prior research (e.g., Craig, 2005; Kjelsberg & Loos, 2008) that suggests that increased potential for exposure to someone convicted of a sex offence for older individuals may have contributed to reduced negative attitudes towards them. While there is a lack of research regarding how an individual’s age impacts their attitude toward people with mental illness or intellectual disability convicted of sexual offences, previous research suggests that education can be an important factor in reducing negative attitudes about mental illness. Meta-analyses have shown that education can be successful in challenging adults’ attitudes toward mental illness (Corrigan et al., 2012) however, the sample was not inclusive of studies examining attitudes toward convicted individuals with mental illness.
Limitations and Future Directions
There are several limitations that must be noted. Firstly, the usual caveats associated with snowball sampling should be considered. Given that the initial advertisements for participation were shared mainly through researcher and university social media platforms, this may have resulted in a higher likelihood of participants who have an interest or experience in higher education, which may not be representative of the general population. However, previous studies exploring public attitudes towards those convicted of sex offences have used a similar sampling approach (Shelton & Winder, 2013; Steans & Duff, 2018). Furthermore, the vignettes used in this study present a sexual offence committed against a child victim. As child sex offences are considered to be more severe (Ferguson & Ireland, 2006) and those who have offended against a child are deemed to be more dangerous, immoral and incapable of change than those with adult victims (Rogers et al., 2011; Weekes et al., 1995), it is possible that this may have clouded more-discrete differences based on the mental illness or intellectual disability factors being explored, with the victim type overriding the application of any exceptions based on the reported symptoms. However, the present study did identify differences in risk of harm to children and adults, blame attribution and reintegration comfort based on intellectual disability and mental illness symptomology. Future research should further explore the extent of differences in a series of sexual offence and non-sexual offence categories to determine where mental illness and intellectual disability influence is taken into account by the general public when estimating risk of harm, reoffending likelihood, liability and acceptance of these individuals back into the community.
Furthermore, the vignettes in this study were presented following completion of the CATSO scale, in which the use of problematic “sex offender” terminology may have caused a “priming” effect with the propensity to detrimentally impact participant attitudes towards the individuals depicted in the vignettes (Harris & Socia, 2016). As such, in future replications or extensions of this work, it is suggested that the CATSO be completed following the experimental element of the study. As indicated earlier, the vignette created to depict a person convicted of a child sex offence with mental illness specifically presented symptoms associated with schizophrenia. This decision was made based on the higher prevalence of this disorder in the those convicted of sex offences relative to other psychiatric disorders (Fazel et al., 2007). However, it is very possible that this disorder may be unique in eliciting responses that may not be comparable to other types of mental illness. This is also a possible explanation as to why exposure to mental illness in the current study did not impact on perceptions of the individual with mental illness; given the low prevalence of schizophrenia in the general population compared with other mental illnesses (e.g., bipolar disorder; GBD, 2017), it is possible that comparison to one’s own experience of mental illness was limited. With this in mind, it is important that this study is replicated with other types of psychiatric diagnoses to determine whether responses were made based on mental illness generally, or the specific mental illness depicted in this study. It may also prove fruitful to further examine participants’ beliefs based on exposure to different types of psychological disorders (e.g., mood disorders, anxiety disorders, psychotic disorders, trauma and stress-related disorders, and personality disorders).
It should also be noted that while the present study accounted for prior exposure to mental illness and intellectual disability, it did not account for participant exposure to sexual offences. In fact, the participant information sheet highlighted that the study would include a vignettes of people convicted of child sex offences, which may have dissuaded those with sexual assault experiences from participating. Given that females are more likely to be sexually victimised than males (WHO, 2021), this may explain some of the gender differences identified with regards to estimations of risk of harm and sexual reoffending. Future research should make efforts to control for participant exposure (either personally or as a third-party) to sexual offences.
While the current study used a within-subjects approach to minimise confounding individual differences, there is also a need for future, more ecologically valid, experimental research to examine more implicit differences in attitudes towards those convicted of a sex offence who present with mental illness and intellectual disability symptomology. Such research would benefit from the inclusion of a planned/impulsivity factor to better understand any potential interaction between mental illness/intellectual disability and perceived impulsivity in predicting general public attitudes.
Conclusions
This research indicates that the general public demonstrate less concern about a person convicted of a child sex offence being released into their community if that individual has an intellectual disability or mental illness, and that they perceive these individuals to be less likely to commit further sexual offences in the future than someone convicted of the same offence who presents as neurotypical. Extending prior research, our findings provide novel insight; the lower levels of risk of sexual reoffending attributed by the general public to those with intellectual disability also extend to those with mental illness. While it has previously been found that the general public overestimate the risk, dangerousness, and likelihood of violence in those who have committed an offence with a mental illness (Angermeyer & Dietrich, 2006; Stier & Hinshaw, 2007), these results suggest that they are in fact perceived to pose less risk of future sexually abusive, harmful or offensive behaviour and incite less concern about community reintegration than one without mental illness. Upon release from prison, those with serious mental illness or intellectual disability are considerably more likely to experience residential instability and homelessness (Mallik-Kane & Visher, 2008; Visher et al., 2010). In order to alleviate these risks, community-based supportive housing can be especially beneficial to ensure the individual has a stable residence, whilst also receiving support to address their ongoing treatment needs and reduce the likelihood of recidivism. Although our findings suggest that the general public may feel more comfortable with the individuals presented in the vignettes as having a mental illness or intellectual disability being reintegrated into the community, these attitudes can be heavily influenced by social distance. For example, the greatest opposition to the placement of community housing most commonly lies with those closest to the location itself, known as the ‘Not in My Back Yard’ effect (NIMBY; Dum et al., 2017). This means there is often conflict between beliefs that those who have committed an offence deserve to be placed in community-based facilities to support rehabilitation, and one’s willingness to have that facility in their own neighbourhood. Further research is needed to determine whether this social distance factor influences the public’s level of reintegration comfort for those with a mental illness or intellectual disability.
Those who believed that people convicted of sex offences, as a demographic, have a reduced capacity for response to intervention or rehabilitation were also less discriminating in terms of risk, blame, and comfort at community reintegration based on the presence of either mental illness or intellectual disability symptoms. Importantly, our findings suggest that exposure to intellectual disability and/or mental illness may not necessarily have the propensity to reduce the perceived level of more generalised risk to the public associated with a person convicted of a sex offence who also has an intellectual disability or mental illness over-and-above an individual’s belief that capacity for change is limited in anyone convicted of such offences.
These findings have implications for the rehabilitation of those convicted of sex offences who present with these conditions, as successful reform is heavily influenced by the attitudes and reactions of the community within which they are placed upon release (Burchfield & Mingus, 2014). Our results suggest that through increasing exposure and understanding about capacity for change in people convicted of a sex offence, the negative attitudes and stigma associated with this marginalised group, and understanding regarding the impact of certain conditions on offence behaviour could be reduced. It is important that future research aims to determine whether interventions targeted at increasing understanding of these conditions, and of the effectiveness of sex offence-focused intervention efforts, can in fact change attitudes towards those convicted of sex offences. Finally, it should be noted that research indicates that those with intellectual disability and mental illness do present a significantly higher likelihood of recidivism than those without (Camilleri & Quinsey, 2011; Looman & Abracen, 2013), suggesting that the risk associated with these individuals in reality may be higher than a convicted individual without such diagnoses. Therefore, care must be taken to ensure that these more positive (or less negative) attitudes towards someone convicted of a child sex offence with a mental illness or intellectual disability do not lead to an underestimation of risk by members of the general public. Such an outcome might increase vulnerability to victimisation through a belief that precautions they might put in place whilst in contact with a neurotypical individual are not necessary where that individual presents with mental illness or an intellectual disability.
Footnotes
Acknowledgments
The authors take responsibility for the integrity of the data, the accuracy of the data analyses, and have made every effort to avoid inflating statistically significant results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.