
Abstract
This study aimed at assessing the extent to which factors associated with male child sexual offending may also be applicable to women with a self-identified sexual interest in children. Participants (n = 42) took part in an anonymous online survey covering questions about general characteristics, general sexuality, sexual interest in children, and previously-perpetrated contact child sexual abuse. Group comparisons between women who reported committing contact child sexual abuse compared to those who had not were conducted in terms of sample characteristics. Furthermore, the two groups were compared regarding the factors of high sexual activity, use of child abuse material, indication of ICD-11 pedophilic disorder diagnosis, exclusivity of sexual interest in children, emotional congruence with children, and childhood maltreatment. Our results revealed that high sexual activity, indication of ICD-11 pedophilic disorder diagnosis, exclusivity of sexual interest in children, and emotional congruence with children were associated with previous contact child sexual abuse perpetration. We recommend further research on potential risk factors relating to child sexual abuse on the part of women.
Introduction
Sexual violence against children is a worldwide problem. The consequences of abuse can be devastating for the healthy development of the child, resulting in a higher risk of psychopathological conditions such as depression, suicidality, anxiety, eating and personality disorders, as well as substance abuse (Anderson et al., 2000; Bensley et al., 1999; Bulik et al., 2001; Lee et al., 2008; Molnar et al., 2001). Whereas pedophilia and sexual offending among men have received broad attention in the last few decades, the corresponding phenomena among women have hardly been considered in research until relatively recently. The ultimate taboo status (Hayes & Baker, 2014; Tozdan et al., 2020) and “culture of denial” (Denov, 2004b) surrounding women who are sexually offensive, contribute to this empirical and societal lack of attention. This is regrettable as there are suppositions that female-perpetrated sexual abuse can be even more traumatic and damaging for the individuals affected (Denov, 2004a; Goldhill, 2013). Consequently, an understanding of its associated factors is crucial.
Definition of Sexual Interest in Children
The International Classification of Diseases for Mortality and Morbidity Statistics, 11th revision (ICD-11; World Health Organization, 2020) defines the symptoms of a pedophilic disorder as a sexual interest in prepubescent children (usually 10/11 years or younger), together with persistent sexual thoughts, fantasies, urgent needs, or behaviors for at least 6 months. Furthermore, individuals must have acted on these thoughts, fantasies or urges, or their pedophilic interest must result in distress or interpersonal problems. A sexual interest in pubescent children aged 11–13/14 years is called “hebephilia” but is not a diagnosis found in diagnostic manuals (American Psychiatric Association, 2022). In the present study, the term “sexual interest in children” is defined as sexual interest of adult persons in children up to 13 years which might include both pedophilic and hebephilic sexual interest but does not necessarily imply that diagnostic criteria are met.
Definition of (Female) Child Sexual Abuse
At the present time, numerous different definitions of child sexual abuse exist (Murray et al., 2014). According to the World Health Organization, 2006), involving a child in sexual acts that the child does not fully understand, cannot give informed consent to, or is developmentally unprepared to give such consent to, constitutes child sexual abuse. By this description, it does not only consist of physical acts, but can also comprise non-contact abuse such as display and exploitation (e.g., in child abuse material). In the present study, self-reported child sexual abuse perpetration refers to contact sexual acts. These are defined as vaginal, oral and anal sex, and all other sexual acts in which the genitals and/or the breast are touched to arouse oneself or the other person sexually.
Sexual Interest in Children Versus Child Sexual Abuse
It is noticeable that society sees a strong link between pedophilia and child sexual abuse (e.g., Cantor & McPhail, 2016; Feelgood & Hoyer, 2008). However, they are not synonymous (e.g., Jahnke, 2018). There is evidence that men who engage in child sexual abuse do not always have an underlying pedophilic interest (Gerwinn et al., 2018; Seto, 2008). Likewise, research indicates that people with a sexual interest in children do not inevitably offend against them (e.g., Bailey et al., 2016; Cantor & McPhail, 2016). Nevertheless, sexual interest in children seems to represent a risk factor for child sexual offenses, with a prevalence of approximately 50% in individuals who are sentenced for sexual crimes against children (Seto, 2008; Whitaker et al., 2008).
Prevalence Estimates of Sexual Interest in Children Among Women
Early work on the extent to which women have a sexual interest in children is based on clinical and correctional samples. Only recently, increased attention has been paid to non-clinical populations. Here, a large discrepancy with regard to prevalence estimates from different sources can be observed, ranging from 0 to 17.5% (for a systematic review see Savoie et al., 2021). Prevalence estimates for sexual interest in children among men from the general population vary between 3 to 23.1% (e.g., Ahlers et al., 2011; Seto, 2008; Ó Ciardha et al., 2022). Reasons for the differing estimates might be the presentation of varying items as indicators for pedophilia (masturbation fantasies, content of pornography, etc.) or the fact that surveys vary regarding the age at which individuals are defined as children (Tozdan et al., 2020).
Prevalence Estimates of Female Child Sexual Abuse Perpetration
To estimate the prevalence of child sexual abuse, research uses official statistics (e.g., from police or judicial authorities) or reports from those affected by the abuse. Tozdan et al. (2019) give an overview from different studies of the prevalence estimates of child sexual abuse committed by women, ranging from approximately 1–20%. Since about 2% of all officially-reported sexual crimes seem to be committed by women (Cortoni et al., 2017), it is well-established scientific knowledge that sexual offending is much more common among men. Regardless, the data on female child sexual abuse perpetration clearly demonstrates the relevance of research in this area, as it is not necessarily rare. In both groups, prevalence estimates vary greatly for methodological reasons and due to the use of different samples. They may also be a consequence of the different definitions of sexual abuse used in research (Saradjian, 2010).
Factors Associated with Male Child Sexual Offending
Certain parallels can be observed between men and women who sexually abuse children. Various studies indicate that both groups are mostly Caucasian (Allen, 1991; Lewis & Stanley, 2000; Sandler & Freeman, 2007) and tend to have experienced verbal, physical, or sexual abuse themselves in the past (e.g., Berner et al., 2009; Lewis & Stanley, 2000; Giguere & Bumby, 2007; Johansson-Love & Fremouw, 2006). Furthermore, they both show increased rates of mood, anxiety, personality, and substance abuse disorders (Christopher et al., 2007; Faller, 1996; Green & Kaplan, 1994; Strickland, 2008; Tardif et al., 2005; Miccio-Fonseca, 2000; Ahlmeyer et al., 2003). In addition, in most cases the men and women involved seem to be related or known to the children they abuse (Comartin et al., 2018; Johansson-Love & Fremouw, 2009; Vandiver & Kercher, 2004). Given the similarities, it might be the case that other factors associated with sexual abuse may occur in both groups. Therefore, it is reasonable to take a closer look at the considerable theory and research on factors related to child sexual abuse on the part of men. Here, sexual preoccupation seems to be associated with child sexual offending. For example, in an adolescent sample, Miner et al. (2010) found that sexual abuse of children is related to high levels of sex drive and sexual preoccupation. Depending on the study, there are different definitions and measurements of sexual preoccupation, often including the frequency of orgasms, sexual intercourse, or masturbation. Since pornography consumption may be understood as a behavioral pattern potentially related to hypersexuality (Klein et al., 2015), it is worth mentioning here as well. There are findings that sexual deviant pornography content (e.g., child abuse material, depictions of violence) is related to child sexual abuse perpetration (e.g., Bourke & Hernandez, 2009). Consuming child abuse material appears to be a valid indicator of sexual interest in children (Seto et al., 2006), which leads to the next factor worthy of consideration. There is evidence that deviant sexual interests (e.g., sexual interest in children) are a risk factor for child sexual abuse perpetration (Whitaker et al., 2008). Current research and clinical practice further indicate the importance of looking more closely at the degree of the underlying pedophilic interest. Exclusive pedophilia refers to being exclusively sexually attracted to children. In contrast, individuals with a non-exclusive sexual interest in children are attracted to adults as well as to children (Hall & Hall, 2007). Bailey et al. (2016) examined correlates of committing child sexual abuse in a sample of men with a sexual interest in children. In their sample, greater attraction to children relative to adults was predictive of sexually offending with regard to children. Furthermore, emotional congruence with children is considered an empirically-supported factor associated with child sexual offending (e.g., Hermann et al., 2017; McPhail et al., 2013). The definition of this construct includes an overly emotional and cognitive attachment to children (Fernandez et al., 2014). The findings of a meta-analysis by McPhail et al. (2013) demonstrated that increased scores on a scale that assessed emotional congruence with children were associated with sexual offending against unrelated children. Lower scores were associated with sexual offending against related children. Finally, childhood maltreatment seems to be a potential contributing factor in sexual abusing behaviors among both men and women (Gannon et al., 2008; Jespersen et al., 2009; Levenson et al., 2015; Reavis et al., 2013; Turner et al., 2008; Wijkman et al., 2014). Supporting the “sexually abused–sexual abuser hypothesis” (e.g., Seto et al., 2010), Jespersen et al. (2009) indicated a link between experiencing sexual abuse during childhood and committing sexual offenses later in life.
The Present Study
Research about women who sexually abuse children is growing slowly but steadily. Nevertheless, especially in non-clinical and non-forensic samples, there is still a noticeable gap in information on what is known about factors associated with child sexual abuse perpetration. As there is evidence that individuals with sexual interest in children are at a higher risk of abusing children (Seto, 2008; Whitaker et al., 2008), assessing a sample of women with a self-referred sexual interest in children seems to be particularly interesting in this context. The purpose of this study was to examine whether certain factors are associated with self-reported contact child sexual offending in this sample. The variables of interest were chosen based on factors associated with child sexual abuse on the part of men. They include high sexual activity, use of child abuse material, indication of ICD-11 pedophilic disorder diagnosis, exclusivity of sexual interest in children, emotional congruence with children, and childhood maltreatment. Data from an anonymous online survey directed towards women with a self-referred sexual interest in children was analyzed (Tozdan et al., 2021). The study covered questions about general characteristics, general sexuality, the participants’ sexual interest in children, and previously-committed contact child sexual abuse.
Methods
Procedure
Data was collected through an online survey from July to December 2020. Initially, the survey was created participatively by consulting a woman with a self-identified sexual interest in children. The woman reviewed a first draft of the survey. Her critical comments and change requests regarding content and language were taken into account in subsequent revisions. The subjects could participate via two study links generated with Qualtrics (www.qualtrics.de) and LimeSurvey (www.limesurvey.org) software. Links to the study were disseminated through websites that address people with a sexual interest in children 1 , the Homepage of the research project, the Instagram account of the University Hospital Hamburg-Eppendorf, emails to the German chamber of psychotherapy, and various other general websites. 2 We further sent the links to staff members of the prevention outpatient treatment center 3 of the Institute for Sex Research, Sexual Medicine, and Forensic Psychiatry at the University Hospital Hamburg-Eppendorf as well as to the counseling center “Wendepunkt e.V.” for minors and young adults with sexually-conspicuous behavior in Hamburg. The links were non-personalized and the therapists were not involved in the study processes. Where appropriate, therapists pointed out that there is an online study that is directed to women with sexual interest in children. Study participation was voluntary and did not affect treatment.
At the beginning of the survey, participants were informed that the study was directed to women who are at least 18 years of age and have a sexual interest in children under the age of 14 years. Subsequently, information about the study’s goal, procedures, associated benefits and risks, financing, compensation, cancellation rights, and notice on data protection was provided. To participate, signing a digital consent form was mandatory. The ethics committee of the Local Psychological Ethics Committee of the University Medical-Centre Hamburg approved the study (reference number: LPEK-0110).
Sample
The survey included participants meeting the following criteria: being female-assigned at birth or identifying with the female gender, being at least 18 years of age, and having a self-identified sexual interest in children under the age of 14 years. A total of 105 people opened the survey via one of the two study links. Of these, 59 did not complete the questionnaire, two indicated being male-assigned at birth and identifying with the male gender, and two stated that they were under 18 years of age. Individuals who identified exclusively with the male gender were excluded from the study. Four participants (9.5% of the total sample) were not female-assigned at birth but identified with the female gender. Even though it might be assumed that these participants might not be comparable to the others because biology has a profound influence on sexual interest, analysis showed no differences in the main results when including solely participants assigned female at birth (n = 38). Therefore, the final sample for the data analyses comprised 42 participants. At the time of the data collection, the participants’ age ranged from 19 to 67 years. The assessed sample characteristics included the participants’ age, education level, sexual attraction, relationship status, partner’s age at data collection, whether they had ever sought help due to their sexual interest in children, and the number of previously-diagnosed mental disorders. They were further asked to specify their previous psychological diagnoses. The reported diagnoses included depression (19%), anxiety disorders (7.1%), posttraumatic stress disorder (9.5%), personality disorders (9.5%), obsessive-compulsive disorder (2.4%), dissociative disorder (2.4%), stimulus filter disorder/autism (2.4%), eating disorder (2.4%), adjustment disorder (2.4%), Munchhausen by proxy syndrome incl. Munchhausen by adult proxy syndrome 4 (2.4%), and substance abuse (2.4%).
Measures
To obtain replicable results, we describe the surveyed measures in detail below.
High Sexual Activity
In the current study, high sexual activity is measured by the frequency of masturbation. Information on participants’ masturbation was ascertained by the following questions. First, participants were asked “Have you ever masturbated in your life?”. Afterwards they were asked “How often have you masturbated in the last 12 months?” and chose one of the four provided response categories: (1) “Never”, (2) “Once or several times during the year”, (3) “Once or several times a month”, (4) “Several times a week”. Due to the small sample size and low numbers of cases in the categories, the categories (1), (2), and (3) were summarized into “low frequency of masturbation” as an indicator for low sexual activity. The category (4) represents “high frequency of masturbation” as an indicator for high sexual activity.
Use of Child Abuse Material
Use of child abuse material was measured via items about the content of the pornography consumed. Exposure to pornography was assessed with the same questions as used for masturbation. In addition, participants were presented with the multiple-choice question “Which kind of pornography do you watch?” providing different response categories such as (1) “Adult actors (18 years or older)”, (2) “Adolescent actors (about 13 years)”, (3) “Child actors (about 12 years or younger)”, and others (i.e., gay couples, violence/rape, BDSM, fetishes). It was possible to select more than one response category here. Participants who chose one or both of the pornography categories (2) “Adolescent actors (about 13 years)” and (3) “Child actors (about 12 years or younger)” were deemed to be using child abuse material. In order to lower the participants’ barriers to report the consumption of such abuse material, the term “actor” was used instead of “victim”. Nevertheless, we consider the former term inappropriate with regard to the abusive contents of such material.
Indication of ICD-11 Pedophilic Disorder Diagnosis
To measure “Sexual Interest in Children” participants were presented with the multiple choice question “Which of the following age groups relates to your sexual interest?” giving the response categories (1) “Male infants and/or small children (at the age of four or younger)”, (2) “Female infants and/or small children (at the age of four or younger)”, (3) “Boys before puberty (between 5 and 10 years old, i.e., no pubic hair yet and children’s genitals)”, (4) “Girls before puberty (between 5 and 10 years old, i.e., no pubic hair yet and children’s genitals)”, (5) “Boys in puberty (between 11 and 13 years old, i.e., beginning growth of pubic hair and maturing genitals)”, and (6) “Girls in puberty (between 11 and 13 years old, i.e., beginning growth of pubic hair and maturing genitals)”. Participants could select multiple response categories. If they selected one or more of the categories (1) to (4) they were asked “Are you ever (i.e., now or in the past) repeatedly sexually aroused (accompanied by lasting sexual thoughts, fantasies, urgent needs or behaviors) by children before puberty over a longer time period (e.g., several months) to an intensive (i.e., strong) degree? “This first yes/no question corresponds with the first part of the guidelines of the ICD-11 pedophilic disorder diagnosis (World Health Organization, 2020). If participants indicated “Yes”, they were presented with a second and third yes/no questions: “Have you acted in accordance with these thoughts, fantasies, or urgent needs? (For example, did you masturbate to these fantasies?)” and “Are (or were) you adversely affected by the thoughts, fantasies, or urgent needs? (Did you suffer as a result of your fantasies, for example?)”. This second and third question constitute the second part of the guidelines of the ICD-11 pedophilic disorder diagnosis (World Health Organization, 2020). Answering the first question and one or both of the other two questions in the affirmative was considered to be an indication for a possible ICD-11 diagnosis of pedophilic disorder. It should be noted that the questions are at best vague indicators for a pedophilic disorder and do not necessarily result in diagnoses. That is why we use the term “indication of pedophilic disorder diagnosis”.
Exclusivity of Sexual Interest in Children
Participants were asked to complete the introductory statement “My sexual interest is...” providing the response categories (1) “... Exclusively in children” (2) “... Mainly in children but also in adults.” (3) “... Equally in children and adults.” (4) “... Mainly in adults but also in children.” Due to the low numbers of cases, we summarized the categories (1) and (2) into “exclusively or mainly in children and adolescents” for purpose of the present study.
Emotional Congruence with Children
We provided the German version of the “Child Identification Scale – Revised”, CIS-R (Wilson, 1999). This scale measures emotional congruence with children and attachment to childhood. A higher score indicates a stronger identification with children with regard to cognitive and emotional connectedness. The questionnaire consists of 20 items and has a maximum score of 80. Reliability was excellent in this sample (Cronbach’s ⍺ = .93). To the best of our knowledge, the scale had never been normed on females before the present study. Items are, for example, “I enjoy myself most when I attometer playing with children.” and “I enjoy discovering new things with children.“. The items form the three subscales “special relationship with children”, “immaturity”, and “special closeness to children”.
Childhood Maltreatment
Participants were asked to fill in the German version of the “Adverse Childhood Experiences Questionnaire” (ACE-D; Schafer et al., 2014). This was taken as an indicator for childhood maltreatment. It captured participants’ adverse childhood experiences before the age of 18 (emotional, physical, and sexual abuse; emotional and physical neglect; household dysfunction). Higher scores indicate more severe adverse experiences during childhood. The questionnaire has a total score of 10. It demonstrated marginal internal consistency in this sample (Cronbach’s ⍺ = .62). Items are, for example, “Did a parent or other adult in the household often or very often … Swear at you, insult you, put you down, or humiliate you? Or act in a way that made you afraid that you might be physically hurt?” and “Did an adult or person at least 5 years older than you ever … Touch or fondle you or have you touch their body in a sexual way? Or attempt or actually have oral, anal, or vaginal intercourse with you?”
Self-Reported Child Sexual Abuse Perpetration
The survey included the question “Have you had sexual acts with one or more of the following age groups since you were 18 years old?” The response categories were (1) “infants/toddlers” (0–4 years old), (2) “prepubescents” (5–10 years old), (3) “pubescents” (11–13 years old) and (4) “no sexual interactions with anyone from these age groups”. Participants could select multiple response categories. Sexual acts were defined as vaginal, oral and anal sex, and all other sexual acts in which the genitals and/or the breast are touched in order to arouse oneself or the other person sexually. The categories (1), (2), and (3) were summarized to create the variable “self-reported contact child sexual abuse perpetration”.
We are aware that the mentioning of age ranges focusses on chronological age as opposed to developmental stage. Discordances may exist here. Nevertheless, we decided to provide the age information as a general guide in this study to avoid misunderstandings on the part of the participants.
Data Analyses and Presentation
All tests were performed using IBM SPSS Statistics, version 27 (International Business Machines Corp, 2020). The authors take responsibility for the integrity of the data and the accuracy of the data analyses. We did not correct for multiple testing as this is the first exploratory examination of factors associated with child sexual abuse perpetration in such a sample to the best of our knowledge (Wason et al., 2014). Hence, statistical significance was set to p < .05 for all analyses. We conducted group comparisons between women who reported committing contact child sexual abuse and women who did not report previous child perpetration regarding sample characteristics. Subsequently, we compared the two groups of women with respect to several factors associated with child sexual offending identified in men. We tested for normal distribution of the continuous variables using the Shapiro-Wilk test (p > .05). Levene’s test (p > .05) was used to verify the assumption of variance homogeneity. Differences in continuous variables were analyzed using t-tests (effect size: Cohens d; Cohen, 1988) and Mann-Whitney U tests (effect size: r; Cohen, 1988) as a non-parametric alternative, whereas the comparisons of the remaining categorical variables were calculated with χ2 (effect size: ϕ-coefficient; Wearden, 2010). If more than 20% of expected cell frequencies were below five, Fisher’s exact test was conducted (Fisher, 1992). We did not find fundamental differences between participants who were female-assigned at birth and those who were male/other-assigned at birth which was also shown for the overall sample by Tozdan et al. (2021). Therefore, we did not make specific distinctions in the data between these groups.
Results
Sample characteristics for the total sample as well as for the subsamples and results of group comparison analyses.
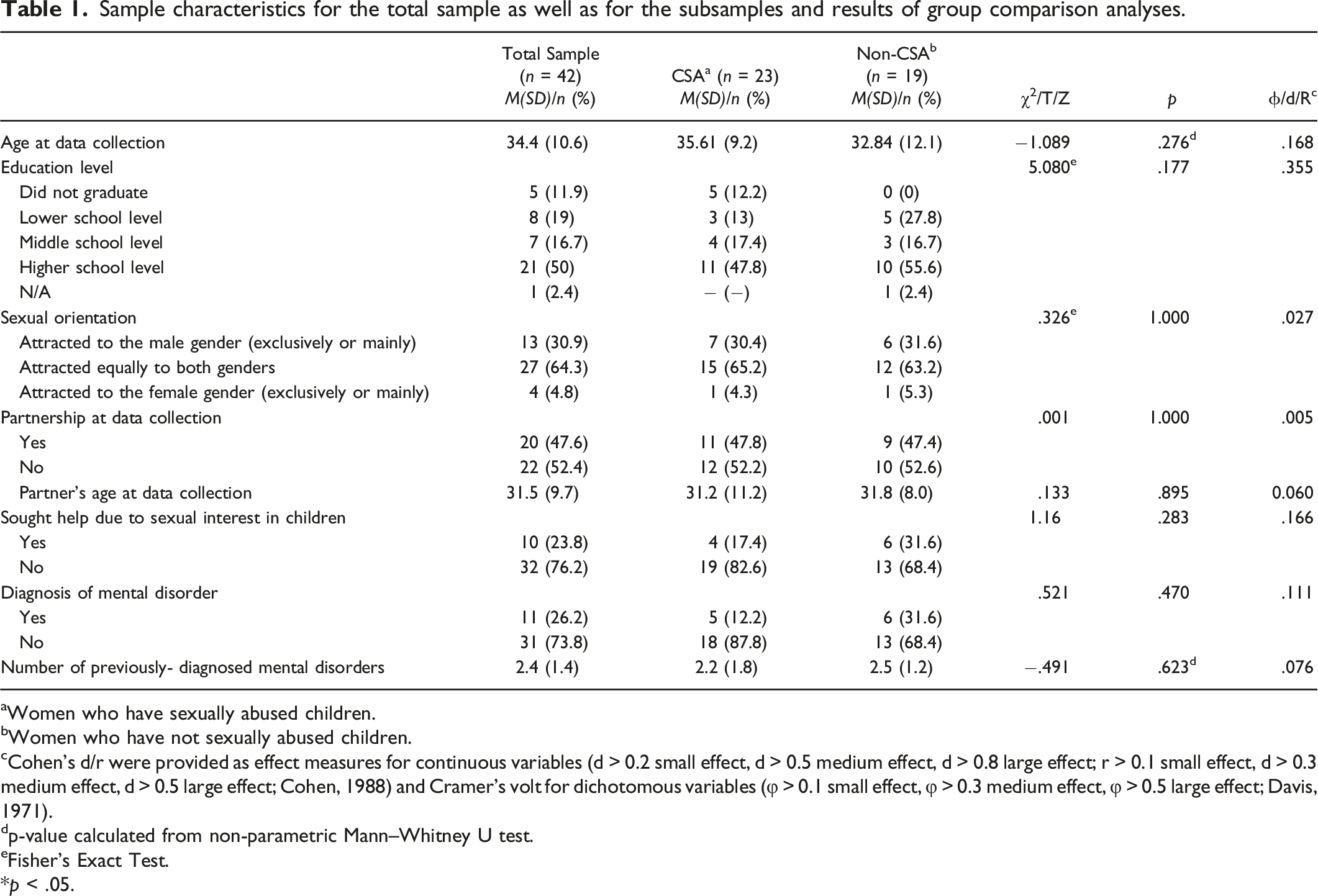
aWomen who have sexually abused children.
bWomen who have not sexually abused children.
cCohen’s d/r were provided as effect measures for continuous variables (d > 0.2 small effect, d > 0.5 medium effect, d > 0.8 large effect; r > 0.1 small effect, d > 0.3 medium effect, d > 0.5 large effect; Cohen, 1988) and Cramer’s volt for dichotomous variables (φ > 0.1 small effect, φ > 0.3 medium effect, φ > 0.5 large effect; Davis, 1971).
dp-value calculated from non-parametric Mann–Whitney U test.
eFisher’s Exact Test.
*p < .05.
Variables of interest for the total sample as well as for the two subsamples and results of group comparison analyses.
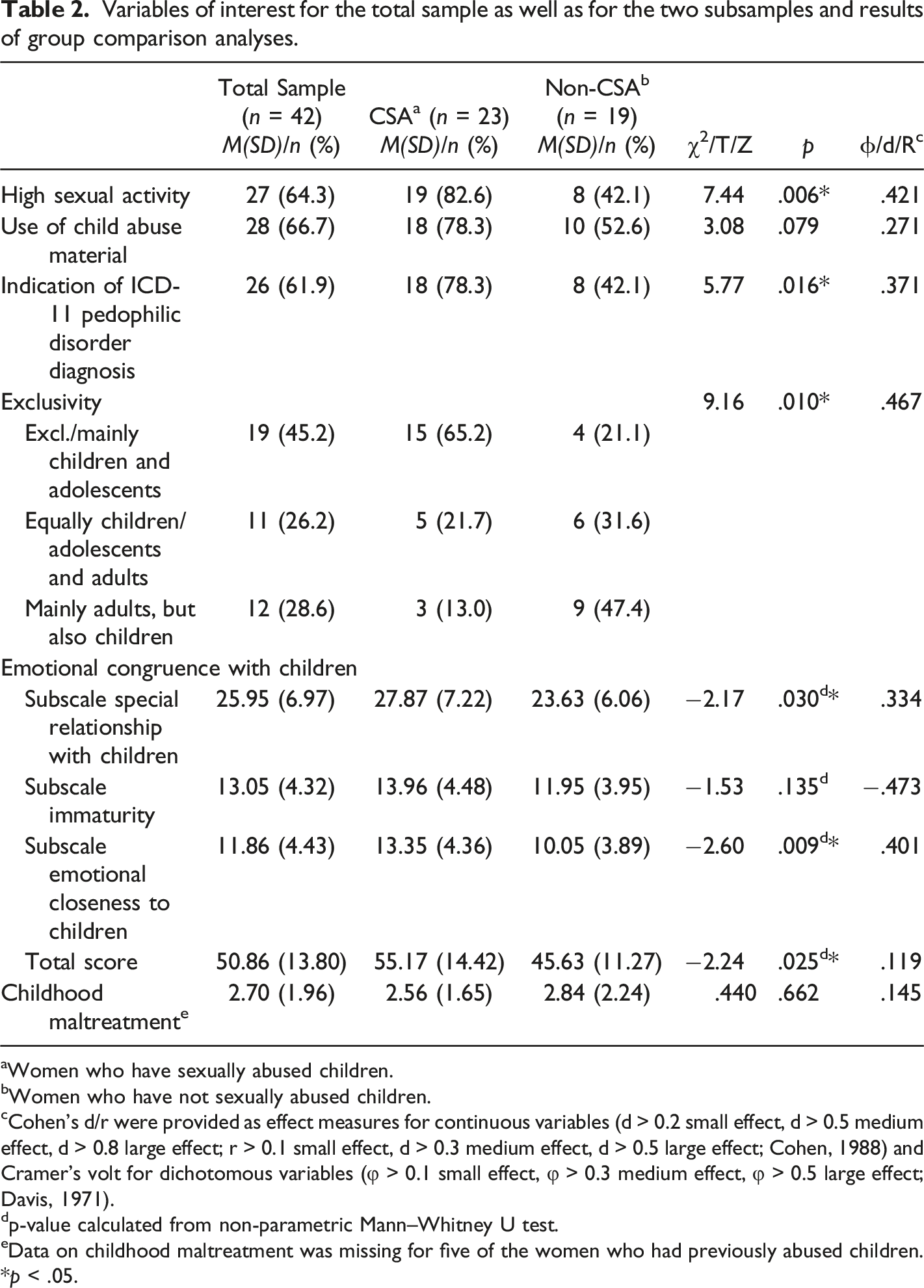
aWomen who have sexually abused children.
Women who have not sexually abused children.
Cohen’s d/r were provided as effect measures for continuous variables (d > 0.2 small effect, d > 0.5 medium effect, d > 0.8 large effect; r > 0.1 small effect, d > 0.3 medium effect, d > 0.5 large effect; Cohen, 1988) and Cramer’s volt for dichotomous variables (φ > 0.1 small effect, φ > 0.3 medium effect, φ > 0.5 large effect; Davis, 1971).
p-value calculated from non-parametric Mann–Whitney U test.
Data on childhood maltreatment was missing for five of the women who had previously abused children.
*p < .05.
For high sexual activity and indication of ICD-11 pedophilic disorder diagnosis, no expected cell frequencies were below five. Both factors were significantly associated with previously-committed contact child sexual abuse. For exclusivity, one expected cell frequency (16.7%) was below five. Exclusivity was found to be significantly-associated with self-reported contact child sexual perpetration in this sample. We found a statistically significant difference in the total scores of the emotional congruence with children scale between the CSA group and the non-CSA group. Furthermore, the two groups of women differed significantly regarding the subscales special relationship with children and emotional closeness to children, with higher scores in the CSA group. The subscale immaturity did not significantly differ between the two groups of women. Concerning use of child abuse material and childhood maltreatment, no significant differences occurred between the CSA group and the non-CSA group.
Discussion
Using a sample of women with self-referred sexual interest in children, this study examined factors related to the women having previously committed a contact sexual offense against a child. Of this sample, more than half reported some sort of previously perpetrated contact sexual abuse of children. Compared to the women without a history of sexual perpetrating, those who previously abused a child did not vary significantly in terms of age, education, sexual orientation, relationship status, partner’s age, and number of previously-diagnosed mental disorders. We found a high level of sexual activity, indication of ICD-11 pedophilic disorder diagnosis, exclusivity of sexual interest in children, and emotional congruence with children to be associated with self-reported contact child sexual abuse perpetration, which is in line with previous findings with regard to male samples. To the best of our knowledge, this is the first study assessing the associations of contact child sexual offending in such sample. Despite the small sample size, the trends observed are a powerful insight into female child sexual abuse perpetration and provide research impulses for future work. Due to the exploratory approach of the present study, we decided to report the results without correcting for multiple testing beforehand. However, when applying different correction methods, some effects remain significant (high sexual activity, exclusivity of sexual interest in children, and emotional congruence with children when using the False Discovery Rate (FDR) based on the approach of Beier et al. (2015); and exclusivity when the Bonferroni correction (Bland & Altman, 1995) was performed). This shows that the trends remain visible even when more conservative methods are applied.
High Sexual Activity
In the present study, high sexual activity was significantly associated with having previously committed a contact sexual offense against a child. This is consistent with findings on the influence of hypersexuality or sexual preoccupation on child sexual abuse perpetration in male studies (e.g., Miner et al., 2010). Nevertheless, high sexual activity indicated via the response category “masturbating several times a week” does not directly correspond to the aforementioned hypersexuality or sexual preoccupation from male research. Furthermore, there are different ways to measure hypersexuality/sexual preoccupation (Klein et al., 2015).
Use of Child Abuse Material
The consumption of child abuse material was not related to self-reported contact child sexual offending in our sample. This result is not in line with male research, where there is evidence of a link between using child abuse material and committing contact sexual offenses (Seto et al., 2011). It also contradicts the suggestion by some researchers that the use of child abuse images acts as part of a behavioral pathway that can lead to contact offending (Buschman et al., 2010; Sullivan, 2002). However, regardless of the lack of significance in the present study, our findings of n = 28 women who use child abuse material (representing 66.7% of the sample) clearly confirm that female consumers exist. Most research on this topic only deals with men (e.g., Ly et al., 2018). Future studies on CSEM should not only address men but also explicitly reach out for women who use CSEM as well.
Indication of ICD-11 Pedophilic Disorder Diagnosis
Our results show that participants who could possibly meet the criteria for the pedophilic disorder diagnosis (according to their answers to the corresponding questions) were significantly more likely to report some sort of contact child sexual abuse committed in the past. It is interesting that in our survey, which was clearly addressed to women with a self-identified sexual interest in children under the age of 14 years, not all participants (n = 26) showed an indication of a pedophilic disorder. This can be explained by the fact that the diagnosis only refers to a sexual interest in prepubescent children (i.e., 10/11 years or younger). In the present study, we have also included women who have a sexual interest in pubescent children, which is not covered by the diagnosis. Interestingly, none of the women participating in our study reported a pedophilic disorder diagnosis when they were asked to specify previously-diagnosed psychological disorders. However, we see the indication of a possible diagnosis in 62% of the women in our sample. This raises the question of why they have not received such a diagnosis by clinicians in the past. Most participants in the present sample who likely met pedophilia criteria reported that they never had sought professional help due to their sexual interest in children (Table 1) - likely because of the stigma associated with sexual interest in children. Thus, most participants had not self-referred for pedophilia assessment and diagnosis. In addition, it might be that most participants had not been criminally charged for sexual contact with children, which might result in clinical or forensic evaluation. However, some participants who likely met pedophilia criteria stated that they had sought professional help due to their sexual interest in children. One potential explanation for why they have not received the diagnosis of pedophilia could be that the aforementioned social taboo surrounding female child sexual abuse (Hayes & Baker, 2014; Tozdan et al., 2020) is also relevant when it comes to diagnosing sexual interest in children among women (Tozdan et al., 2021). Consequently, it might be that even professionals are biased in terms of their assessment of women with a sexual interest in children (Tozdan et al., 2021).
Exclusivity of Sexual Interest in Children
Being exclusively attracted to children was also associated with reporting previously-committed contact child sexual abuse in our sample, which is in line with findings with regard to pedophilic men (Bailey et al., 2016). According to these researchers, it is possible that individuals with a stronger degree of exclusive pedophilia are less likely to find sexual activities with adults or pornography with adult actors and actresses rewarding. Thus, there is potentially no way to satisfy their needs at least partially. Therefore, the risk of committing child sexual offenses might increase. In our sample, most participants indicated that they are also sexually interested in adults. This is consistent with the finding that a significant proportion of the total sample (45%) reported being in a relationship with an adult partner. Research on non-forensic male samples with a sexual interest in children found similar results (Tozdan & Briken, 2015; 2019). According to Tozdan et al. (2021), the fact that sexual interest in children is non-exclusive in many individuals represents a great opportunity for them. Focusing on sexuality with adults might lead to a sufficient level of sexual satisfaction, which can play an important role in the prevention of child sexual abuse.
Emotional Congruence with Children
Our results show that feeling emotionally and cognitively connected to children to a higher degree is related to previously-committed child sexual abuse. This is consistent with research on factors associated with child sexual offenses among men (e.g., Hermann et al., 2017; McPhail et al., 2013). Cognitions that can be related to emotional congruence with children are, inter alia, perceptions about intimate relationships with children that are mutual and reciprocal (Beier et al., 2015; Beier et al., 2015). Thus, it is possible that such underlying beliefs may lead to committing child abuse in our female sample as well. However, having abusive relationships with children could also feed these feelings of connection.
Childhood Maltreatment
Contrary to our expectations based on findings in men (e.g., Jespersen et al., 2009; Reavis et al., 2013), in this sample, victimization involving childhood maltreatment did not show an association with self-reported contact child sexual abuse perpetration. One reason for this result could be the missing data for the Adverse Childhood Questionnaire (ACE-D; Schafer et al., 2014) for five women of the group that had perpetrated contact child sexual abuse previously. Participants possibly did not answer the questions on childhood maltreatment due to their positioning at the very last part of the questionnaire (see also Limitations section).
Limitations
The present study has some limitations. First of all, there is the small number of participants, which is due to the studied population. Links to the study were spread in different ways, yet it is challenging to find women with a self-referred sexual interest in children who are willing to participate in research addressed to that topic. Nevertheless, to generalize beyond our sample, the present results should be replicated with larger samples.
Anonymity in such a survey is indispensable due to some of the question we have investigated, as it seems crucial for participants’ comfort in providing information on personal and sensitive subjects (Joinson, 2001). This clearly represents one of the numerous advantages of web-based studies (Gosling et al., 2004; Ray et al., 2010), especially when considering the stigma surrounding sexual interest in children (Grady et al., 2019; Jahnke et al., 2015). However, there are some disadvantages that come with anonymous studies. There is no guarantee that subjects do in fact meet the given inclusion criteria, participate only once, or answer the questions seriously and without exaggerating or minimizing information.
Furthermore, due to the legal situation which classifies child abuse as a punishable crime, it is possible that participants did not report previous perpetration honestly for fear of being prosecuted. In this context, it should also be noted that the child abuse we have studied is based on retrospective reports. In the professional world, voices are skeptical about retrospective surveys, as they can entail various data biases (e.g., Hardt & Rutter, 2004).
Moreover, as the survey is entirely based on self-reported answers, and no social desirability scale was applied, the participants self-descriptions might be biased. The women who participated have classified themselves as having a sexual interest in children. Nevertheless, it may be that, in a professional evaluation, no such sexual interest would be attributed to them. The number of women in our sample who do not meet the diagnostic criteria for the disorder may indicate this. Therefore, it is not possible to generalize the findings to individuals with a professionally-confirmed sexual interest in children.
The entire questionnaire comprised over 60 questions, with the ACE-D being the very last part, resulting in a potentially lower motivation to finally complete it. As data on the ACE-D was therefore missing for five women of the group with self-reported child sexual abuse, our findings regarding the impact of childhood maltreatment on committing contact child sexual abuse are only meaningful to a limited extent. This possibly explains the differences to equivalent male and female samples, where childhood maltreatment seems to be a common factor associated with CSA.
For our analyses, we had to merge the categories of some variables as well as dichotomize certain measures due to the low numbers of cases (see section Measures). Thus, another methodological approach could lead to different results, which should be kept in mind when interpreting the findings of this study. Moreover, we chose our independent variables based on studies with samples constituted of men who were often incarcerated or convicted for their sexual crimes. Factors associated with contact sexual offending against children in our non-clinical, non-forensic female sample could be different from those identified in, firstly, men and, secondly, forensic samples.
Moreover, pornography depicting adolescents who are not around 13 but might not appear to be adults (i.e., 14–17 years) are missing. We did not include the age range 14–17 years in the pornography categories as the study was directed to women with a sexual interest in children aged 13 or younger. We accordingly developed the categories among all questions in the study. However, it seems relevant if someone watches pornographic material involving adolescents aged 14–17 years. Therefore, this category should be included in further studies.
Furthermore, the measure for sexual activity is limited as it does not directly correspond to the aforementioned hypersexuality or sexual compulsivity from male research. An instrument assessing hypersexuality would have been more reasonable for the present study. However, such instrument was not included. Therefore, masturbation frequency appeared to be the best measure for sexual activity available.
Finally, the definition of sexual interest in children that we used appears to be one-dimensional. Nevertheless, our aim was to assess sexual interest in prepubescent and/or pubescent children among adult women in the broadest possible way. This is because we assume that women who do not meet the diagnosis criteria for a pedophilic disorder, but have a sexual interest in pubescent children, might nonetheless be at risk when it comes to offending against children. We further need to mention that the way we assessed diagnosis criteria for a pedophilic disorder might have overestimated the number of women who have an indication for the diagnosis. Participants agreed with the question on acting on their sexual interest when masturbating to fantasies about children. We cannot conclude a pedophilic disorder from that information because we do not know who had only masturbated to fantasies about children and who had acted on their interest by having sexual contact with children or by consuming child abuse material. However, at least 18 participants might have agreed to the question because they have had sexual contact with children as they reported CSA on a later question in the study (see Table 2). Since use of child abuse material is relevant to the second part of the guidelines of the ICD-11 pedophilic disorder diagnosis (World Health Organization, 2020), a total of 20 participants stated that they had acted on their interest and reported the use of child abuse material. This subgroup includes the 18 participants mentioned above. Thus, two additional participants might qualify for the diagnosis of pedophilic disorder by using child abuse material. This also suggests that eight participants agreed to the question on acting on their sexual interest in children because they only masturbated to corresponding fantasies.
Future Directions
Further research should assess larger samples of women who are at risk of sexually-offending children. As there are several forms of child abuse behaviors, it would be interesting to consider this in future research involving more participants. To gain further insight and overcome the previously-mentioned limitations linked to self-reporting and anonymity, it would be interesting to conduct studies not based solely on online questionnaires. For example, in order to be sure that participants are formally diagnosed with pedophilia, one could use data from diagnostic interviews. The inclusion of different sources of information in addition to self-reporting could be useful. However, considering the challenges of accessing non-clinical, non-forensic women with a sexual interest in children in general, this may be difficult to implement. In future questionnaires, in addressing the topic of female child sexual abuse perpetration, it might be reasonable to apply social desirability scales, as there is evidence for their benefits in the self-reporting of various behaviors (e.g., Perinelli & Gremigni, 2016). Considering the broad range of potentially-relevant associated factors, it might be valuable to focus on others than the ones we did for this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is part of a project that was funded by the Independent Inquiry into Child Sexual Abuse (“Unabhängige Kommission zur Aufarbeitung sexuellen Kindesmissbrauchs”) in Germany.