
Abstract
The rising prevalence of metabolic dysfunction-associated steatotic liver disease (MASLD) poses a critical public health challenge, yet current diagnostic and therapeutic approaches remain limited. Interleukin-11 (IL-11) is a pro-inflammatory cytokine expressed by various cell types in the liver. Although preclinical studies have revealed the pro-fibrotic role of IL-11 in mouse models, the clinical relevance between serum IL-11 and human MASLD remains unclear. This cross-sectional study enrolled 375 patients with MASLD from the outpatient department to explore the relationship between the serum level of IL-11 and the indicators of MASLD in adults with MASLD. Demographic characteristics, clinical parameters, laboratory biomarkers, FibroScan results, and serum IL-11 concentrations were prospectively collected in patients with MASLD for further analysis. As a result, the liver stiffness measurement values were significantly elevated in patients with detectable serum IL-11 compared to the IL-11-undetectable group, while the controlled attenuation parameter values between the groups showed no significant difference. It was also illustrated by logistic regression models that serum IL-11 is an independent predictor of advanced hepatic fibrosis. Our findings provide the references for further developing IL-11 as a potential evaluative biomarker and therapeutic target of MASLD.
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD) impacts approximately 25% of the global adult population (Chan et al., 2022). MASLD, named by the international Delphi consensus, encompasses the full disease spectrum of traditional nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH), emphasizing its metabolic etiology while avoiding the use of potentially stigmatizing terminology (Rinella et al., 2023). Notably, this reclassification shifts from exclusionary criteria to an affirmative diagnosis centered on metabolic dysfunction, which requires at least 1 of the 5 specified cardiometabolic risk factors (Cusi et al., 2025). Additionally, a separate category, metabolic and alcohol-related/associated liver disease, has been introduced for patients with concurrent alcohol use and metabolic dysfunction, who were previously difficult to classify (Targher et al., 2025).
During MASLD, hepatic lesions and metabolic disorders exhibit a bidirectional causal relationship, jointly driving the onset and progression of cardiovascular disease (CVD), chronic kidney disease, and various carcinomas, which exert a significant health and economic burden on societies worldwide (Eslam et al., 2020). However, the diagnostic biomarkers as well as the effective therapeutic strategies of MASLD remain limited (Méndez-Sánchez et al., 2022).
Growing evidence supports that the cytokines drive key pathological processes in MASLD, including hepatic inflammation, steatosis, and fibrogenesis, by mediating cross talk between hepatocytes, immune cells, and hepatic stellate cells (HSCs) (Stefan et al., 2023). Interleukin-11 (IL-11) is a member of the IL-6 family of pro-inflammatory cytokines (Yang and Yin, 1992). Its receptor, IL-11 receptor alpha, forms a heterodimer with the common β-subunit gp130 to activate JAK-STAT3 signaling (Widjaja et al., 2022). This complex demonstrates prominent expression in polarized epithelial cells (eg, hepatocytes, alveolar epithelial cells, and renal tubular epithelial cells) and mesenchymal cells (eg, fibroblasts, smooth muscle cells, adipocytes, and HSCs), enabling IL-11 to regulate diverse biological activities. For example, IL-11 promotes the translation of pro-fibrotic protein via an autocrine loop in fibroblasts, while IL-11 increases the expression of lipolytic genes and decreases adiposity in adipocytes (Dong et al., 2022; Schafer et al., 2017). Up to now, both recombinant human IL-11 (Neumega) and anti-IL-11 monoclonal antibodies (9MW3811) have been developed into drugs to treat thrombocytopenia and advanced malignancies, respectively (Al-Samkari and Soff, 2021; Zhang et al., 2025).
Notably, although other pro-inflammatory cytokines such as IL-6 and TNF-α are well-characterized in MASLD, the role of serum level of IL-11 in the progresssion of MASLD, especially in patients, remains underexplored, which restricts the potential application of IL-11 as a diagnostic biomarker or therapeutic target of MASLD. For a long time, IL-11 was identified as a hepatoprotective cytokine with therapeutic potential in multiple types of hepatic injuries (Bozza et al., 1999; Trepicchio et al., 2001; Yu et al., 2016). But recent studies revealed upregulated hepatic protein expression of IL-11 in patients with liver injury as well as patients with MASLD (Tsuchiya et al., 2024; Widjaja et al., 2019). Moreover, the inhibition of IL-11 attenuated hepatic fibrosis, hepatic steatosis, and hyperglycemia in the diet-induced mouse model of MASLD (Cook and Schafer, 2020). Also, IL-11 elevates in the liver of aged mice, and the deletion of IL-11 improves the life span, the insulin sensitivity, and the liver function of aged mice (Widjaja et al., 2024). In all, the exact function of IL-11 in the progress of MASLD, especially in patients with MASLD, requires further exploration.
In this study, we revealed that IL-11 is an independent risk factor of liver stiffness measurement (LSM, a hepatic fibrosis indicator) in patients with MASLD, while the correlation between IL-11 and controlled attenuation parameter (CAP, a hepatic steatosis indicator) is not significant. These findings are consistent with the mechanisms previously identified in animal studies and further provide clinical evidence supporting the relevance of IL-11 in the pathophysiology of human MASLD.
Materials and Methods
Subjects
Three hundred seventy-five patients with MASLD meeting the 2023 Asia-Pacific Association for the Study of the Liver diagnostic criteria of MASLD were enrolled from the Department of Endocrinology of the Affiliated Hospital of Nanjing University of Chinese Medicine (Eslam et al., 2025). The exclusion criteria for this study are as follows: (1) Individuals with MASLD and increased alcohol intake (alcohol consumption >30 g/day for men and >20 g/day for women); (2) individuals with viral hepatitis, drug-induced liver injury, or other liver damage caused by nonmetabolic risk factors; and (3) individuals with severe CVD and cerebrovascular disease [including uncontrolled hypertension, ie, systolic blood pressure (SBP) >170 mm Hg or diastolic blood pressure (DBP) >100 mm Hg], renal system diseases, hematopoietic system diseases, mental disorders, autoimmune diseases, and active cancer.
This research study received the approval from the Affiliated Hospital of Nanjing University of Traditional Chinese Medicine Medical Ethics Committee. All participants provided written informed consent before biospecimen collection.
Clinical data collection
General information (sex, age, height, and weight); laboratory indices, including aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), total bilirubin (TBIL), total bile acid (TBA), triglyceride (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (FBG), glycosylated hemoglobin (HbA1c), fasting insulin (FINS), C-reactive protein (CRP), and IL-6; body fat mass (BFM), waist-to-hip ratio (WHR), visceral fat area (VFA) detected by InBody; and controlled attenuation parameter (CAP) and LSM detected by transient elastography were collected from the patients.
This study utilized LSM obtained through transient elastography (FibroScan) to quantify the degree of hepatic fibrosis. Although liver biopsy remains the gold standard for fibrosis staging, it is an invasive procedure and unsuitable for large-scale clinical cohort screening. FibroScan is a widely validated noninvasive alternative, which has demonstrated diagnostic efficacy confirmed in previous studies (Mózes et al., 2022).
Serum IL-11 measurement
The venous blood of all subjects was collected in the fasting state in the morning, and the serum IL-11 concentrations were quantitatively analyzed using a commercially available Human IL-11 Enzyme-Linked Immunosorbent Assay Kit (RayBiotech, Lot numbers: 0916240146, 1118240146). According to the manufacturer’s instructions, the limit of detection for this kit is 3 pg/mL. Given that a substantial proportion of participants had a serum IL-11 concentration lower than the blank control level (50.0% in the control group and 45.6% in the MASLD group), which lead to a severely skewed distribution of IL-11 as a continuous variable, we recorded IL-11 concentrations above the blank control as the detectable group and the remaining subjects as the undetectable group for subsequent analyses.
Statistical analysis
Statistical analysis was conducted using SPSS 26.0, GraphPad Prism 9.0, and Origin. All data were reported as mean ± standard deviation, median with interquartile range (IQR), or percentage, as appropriate. The chi-square (χ2) test was used to compare categorical data. The Student’s t-test and analysis of variance test were employed for the comparisons of normally distributed continuous variables. The Mann–Whitney U test and Kruskal–Wallis test were employed for asymmetrically distributed continuous variables. The relationships between clinical indicators were assessed using Spearman correlation. The ordinal logistic regression and multiple linear regression were used to examine the association between potential predictors and hepatic fibrosis. The likelihood ratio test (LRT) is used to compare the goodness-of-fit of two models. A P value of <0.05 was considered statistically significant.
Results
The baseline characteristics of the study population
The baseline characteristics of the study population are summarized in Table 1. A total of 375 participants were included, with a balanced sex distribution (50.7% male and 49.3% female). The median body mass index (BMI) was 32.7 (IQR: 30.6–35.7) kg/m2, indicating a predominantly obese cohort. The median WHR was 0.99 (IQR: 0.95–1.03), and the mean CAP was 326.65 ± 33.61 dB/m, suggesting a high burden of hepatic steatosis. Regarding cardiometabolic risk factors, the mean SBP was 136.90 ± 15.63 mm Hg, with DBP at 86.02 ± 12.44 mm Hg. Lipid profiling revealed slightly elevated TG levels (median: 1.77 mmol/L, IQR: 1.25–2.46) along with reduced HDL-C (median: 1.15 mmol/L, IQR: 1.02–1.30). Glycemic parameters demonstrated that the median FBG was 5.36 mmol/L (IQR: 5.05–5.73), and the median HbA1c level was 5.70% (IQR: 5.50–6.00).
Baseline Characteristics of Study Population
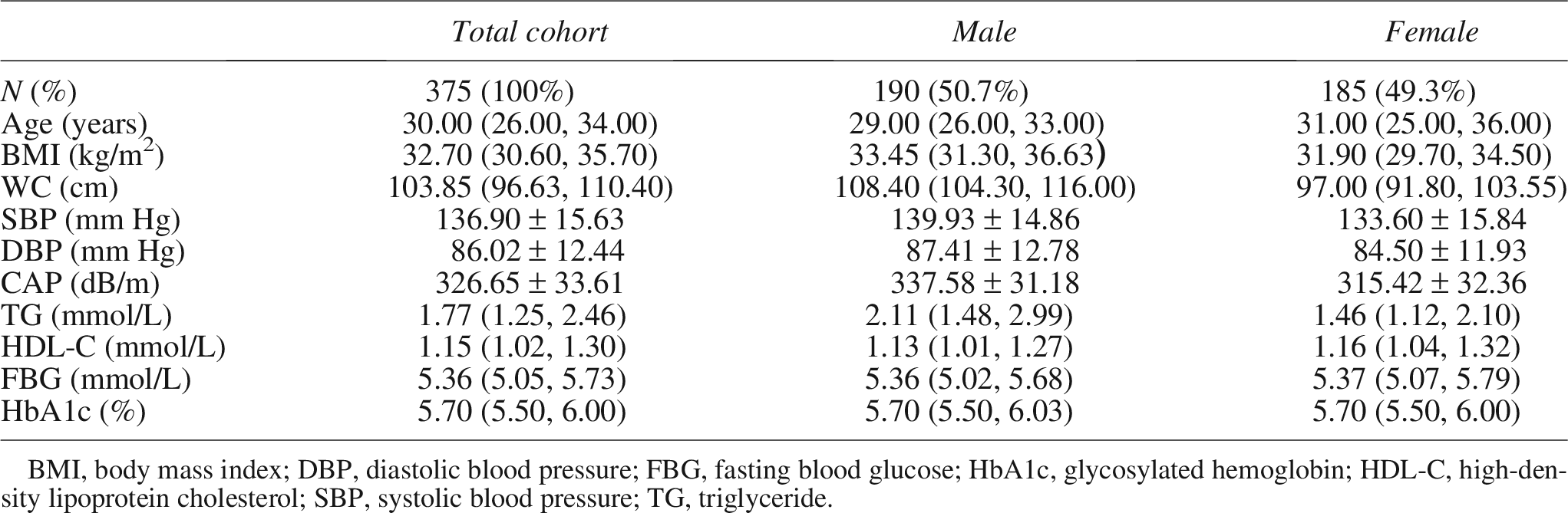
BMI, body mass index; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglyceride.
The LSM value is higher in the IL-11-detectable patients than in the IL-11-undetectable patients
To elucidate the clinical relevance of serum IL-11 in MASLD, we stratified the patients with MASLD (n = 375) into the IL-11 detectable (serum IL-11 of >0 pg/mL, n = 204) and the IL-11 undetectable (serum IL-11 = 0 pg/mL, n = 171) groups. By comparing the data between the IL-11 detectable and undetectable groups, it was showed that the LSM value of patients in the IL-11 detectable group (7.00 kPa) was significantly higher than that of the IL-11 undetectable group (6.80 kPa) (P < 0.05, Fig. 1), while no significant differences were observed in the body weight, BMI, liver function indicators (ALT, AST, ALP, GGT, TBIL, and TBA), glucose-lipid metabolism indicators (LDL-C, HDL-C, TG, TC, FINS, FBG, and HbA1c), inflammatory markers (CRP and IL-6), and the hepatic steatosis indicator (CAP) value (P > 0.05, Table 2).
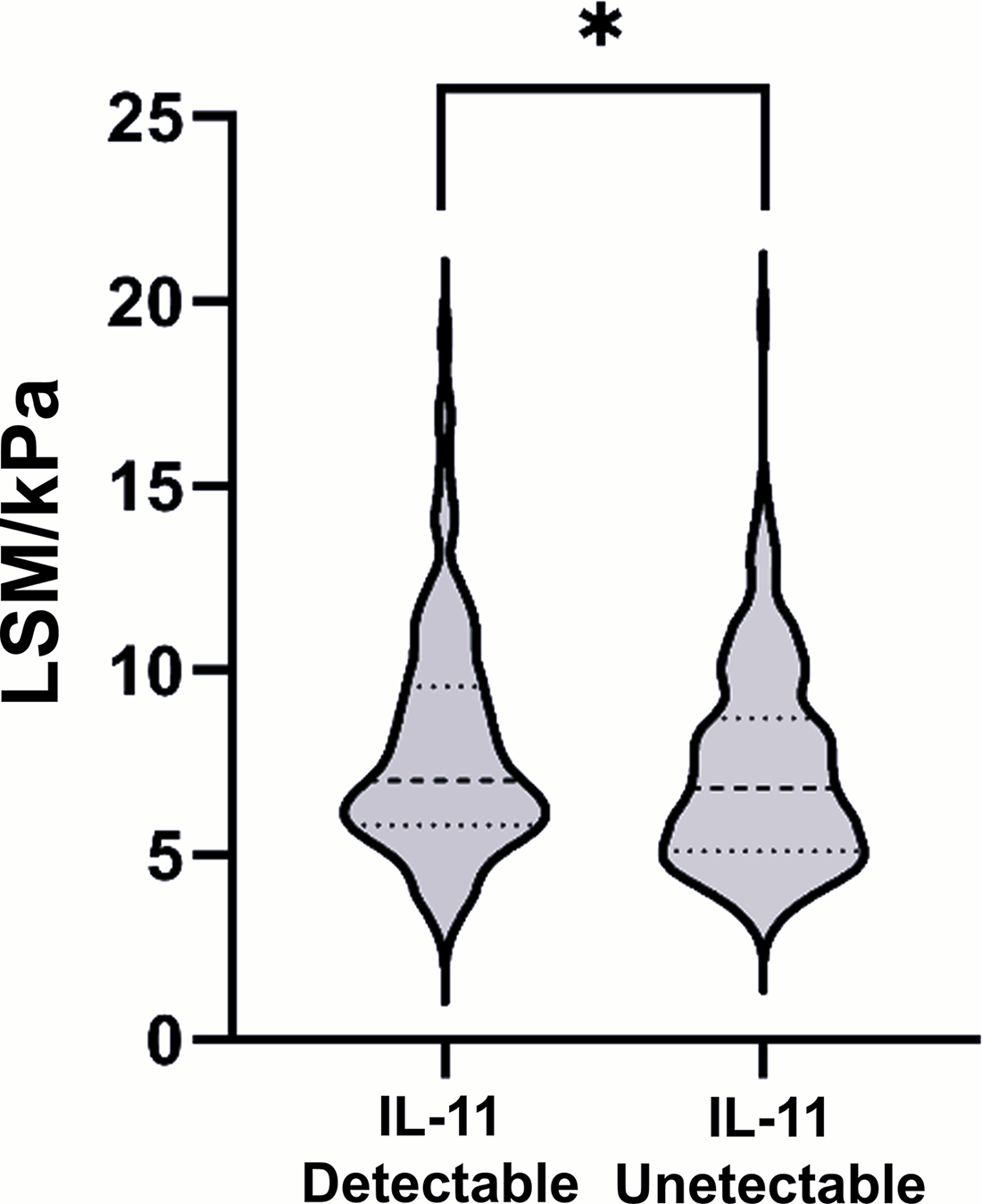
Levels of LSM in patients between the detectable and undetectable groups. Significance, *P < 0.05 versus corresponding group (Mann–Whitney U test). LSM, liver stiffness measurement.
Clinical Data Between Interleukin-11-Detectable and Interleukin-11-Undetectable Groups
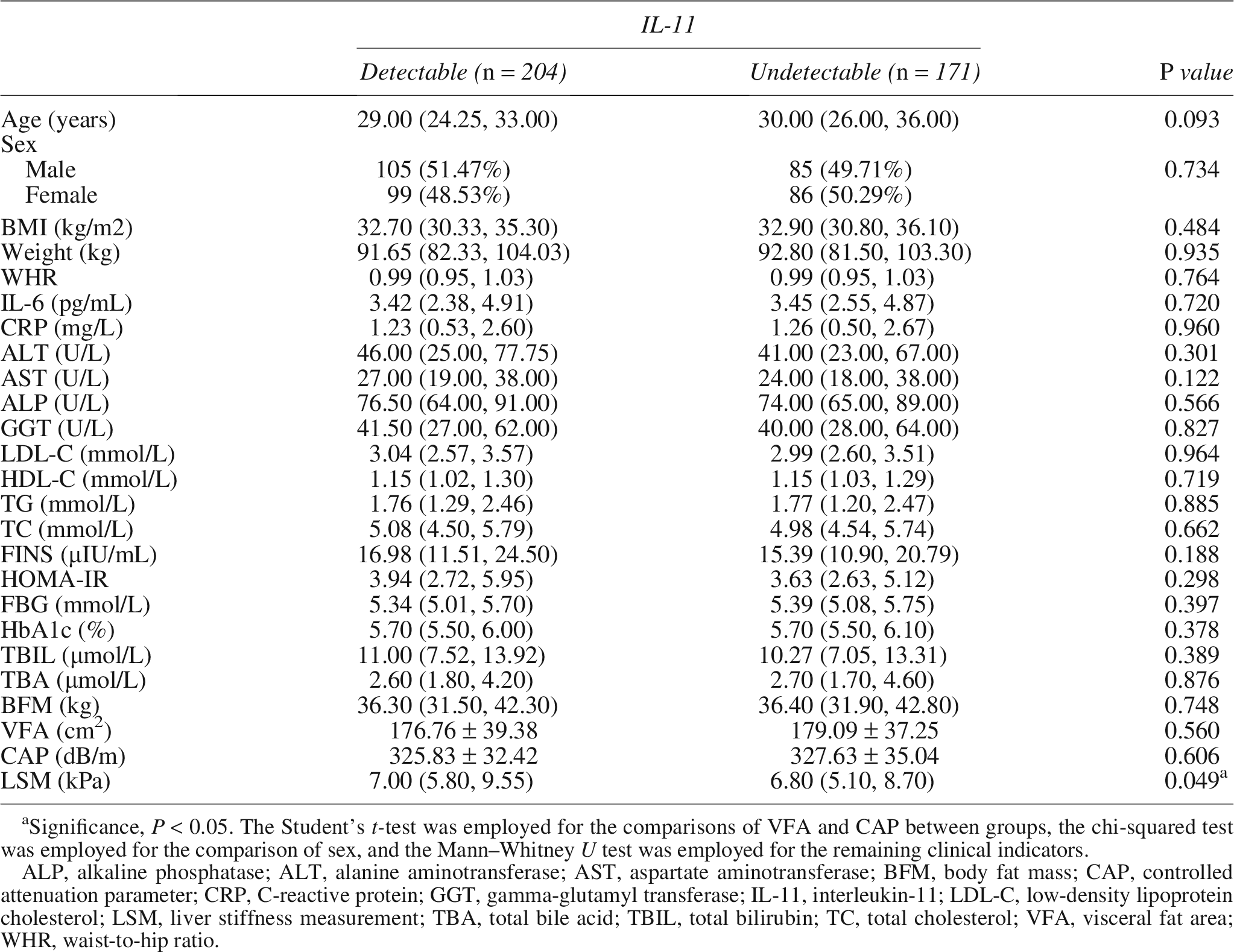
Significance, P < 0.05. The Student’s t-test was employed for the comparisons of VFA and CAP between groups, the chi-squared test was employed for the comparison of sex, and the Mann–Whitney U test was employed for the remaining clinical indicators.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BFM, body fat mass; CAP, controlled attenuation parameter; CRP, C-reactive protein; GGT, gamma-glutamyl transferase; IL-11, interleukin-11; LDL-C, low-density lipoprotein cholesterol; LSM, liver stiffness measurement; TBA, total bile acid; TBIL, total bilirubin; TC, total cholesterol; VFA, visceral fat area; WHR, waist-to-hip ratio.
The LSM is correlated with the serum IL-11 in patients with MASLD
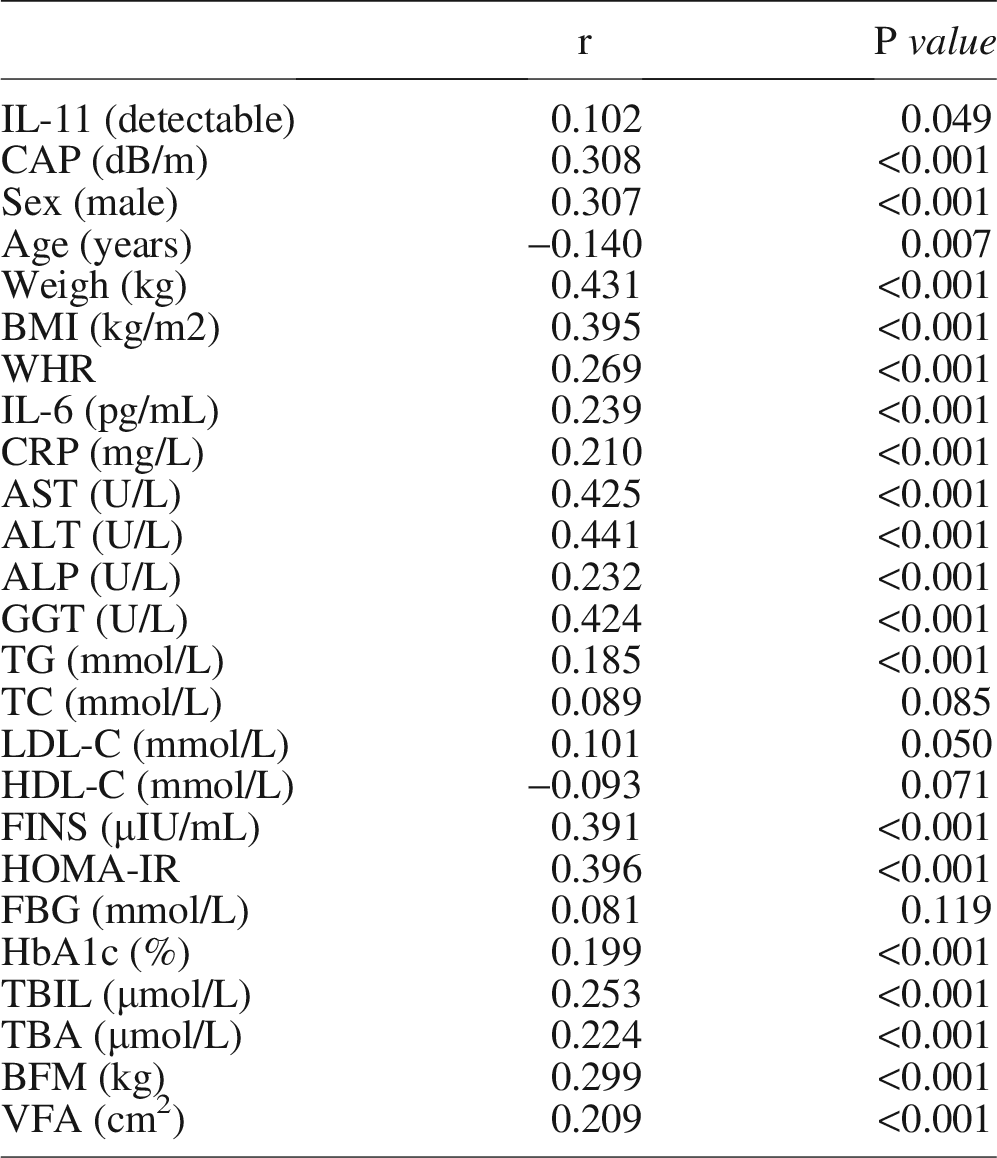
To further investigate the correlation between the LSM and the serum IL-11 in patients with MASLD, we did a Spearman correlation analysis. As shown in Table 3 and Supplementary Figure S2, the LSM was positively correlated with serum IL-11, CAP, sex (male), weight, BMI, WHR, IL-6, CRP, AST, ALT, ALP, GGT, TG, FINS, HOMA-IR, HbA1c, TBIL, TBA, BFM, and VFA (r > 0, P < 0.05), while inversely correlated with age (r < 0, P < 0.01). The positive correlation between the serum IL-11 and the LSM remained in the IL-11-detectable group of patients with MASLD (P < 0.05), as shown in Supplementary Table S1 and Supplementary Figure S1.
The Correlation of the Liver Stiffness Measurement with Other Clinical Indicators in Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease
Serum IL-11 levels in patients with MASLD differ between LSM quartiles
Table 4 demonstrates the clinical profile stratification based on LSM quartiles. Interquartile comparisons revealed a significant stepwise increase in IL-11 across LSM strata (P < 0.05). Notably, the serum IL-11-detectable rate in Q3 was lower than that in Q2. In addition, there are age disparities across groups (P < 0.05), with a distinct graded elevation in BMI, body weight, WHR, and male predominance paralleling LSM progression (P < 0.01). Systemic inflammation markers (IL-6 and CRP) were elevated across LSM strata (P < 0.05). Hepatic injury markers displayed pronounced augmentation: ALT, AST, ALP, and GGT exhibited exponential elevation with LSM advancement (P < 0.01), while TBIL and TBA demonstrated progressive accumulation from Q1 to Q4 (P < 0.01). Glycolipid metabolism showed different alterations: TG, FINS, HOMA-IR, and HbA1c followed LSM-dependent upward trajectories (P < 0.05), whereas LDL-C, HDL-C, TC, and FBG remained invariant across quartiles (P > 0.05). Among the body fat distribution indexes, BFM, VFA and CAP demonstrated significant LSM-correlated increase (P < 0.01).
Clinical Indicators Between Liver Stiffness Measurement Quartiles of Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease
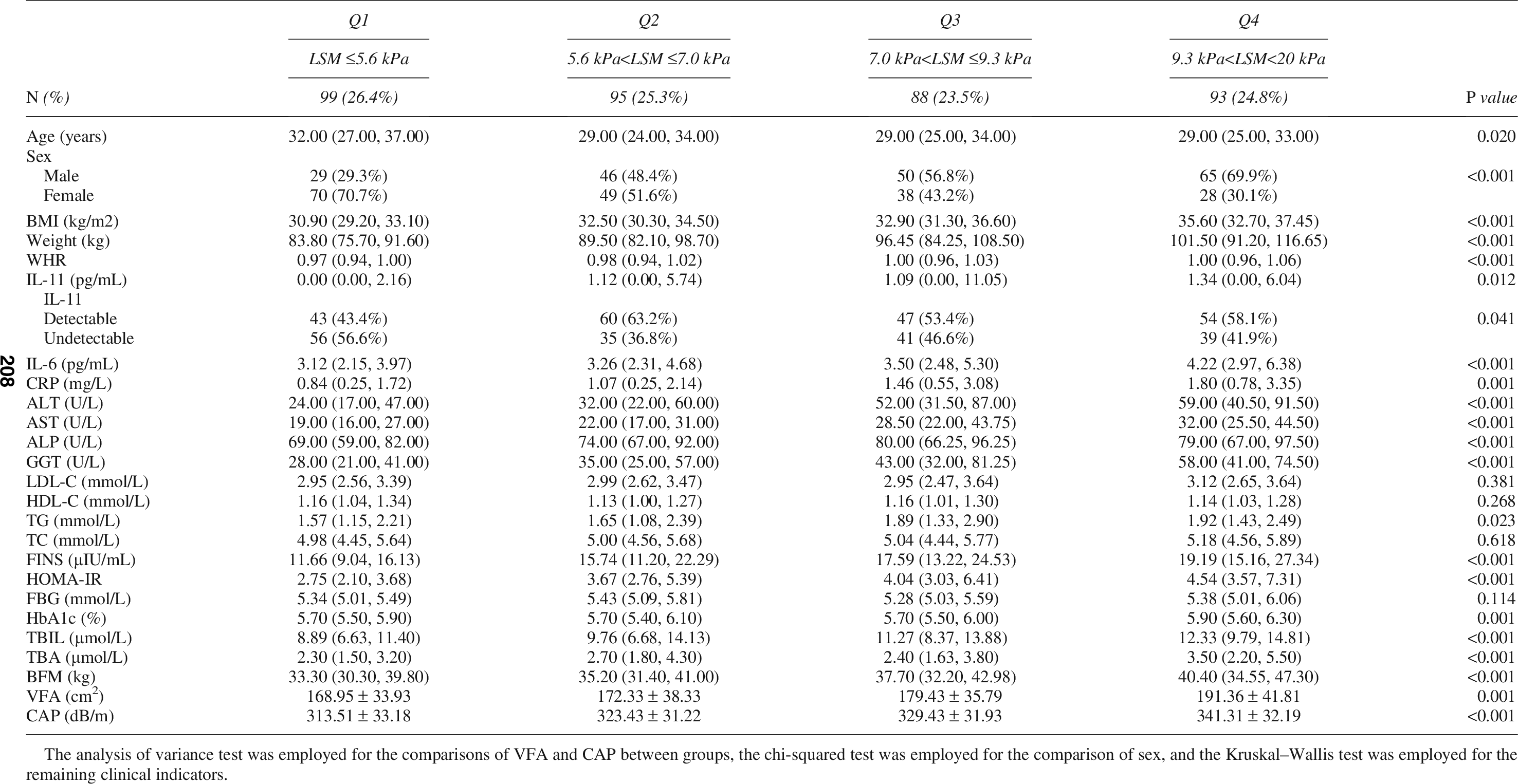
The analysis of variance test was employed for the comparisons of VFA and CAP between groups, the chi-squared test was employed for the comparison of sex, and the Kruskal–Wallis test was employed for the remaining clinical indicators.
Elevated serum IL-11 level is an independent risk factor of hepatic fibrosis progression in patients with MASLD
To elucidate the association between the serum IL-11 level and the severity of hepatic fibrosis in patients with MASLD, we constructed an ordinal logistic regression model using LSM quartiles as the ordinal dependent variable. The model incorporated key clinical and metabolic parameters, including age, BMI, sex, serum IL-11 (stratified as a categorical variable), TG, HbA1c, CAP, CRP, and ALT. After adjusting for potential confounders, BMI (P < 0.01), male sex (P < 0.01), elevated serum IL-11 (P = 0.041), HbA1c (P < 0.01), and ALT (P < 0.01) emerged as independent predictors of advanced hepatic fibrosis, while age, TG, CAP, and CRP did not exhibit significant associations (Table 5 and Fig. 2). These findings suggest a robust relationship between IL-11 elevation and fibrosis progression.

Serum IL-11 level is an independent risk factor for hepatic fibrosis in MASLD patients. Significance, *P < 0.05, **P < 0.01. IL-11, interleukin-11; MASLD, metabolic dysfunction-associated steatotic liver disease.
Risk Factors of Hepatic Fibrosis in Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease (Ordinal Logistic Regression)
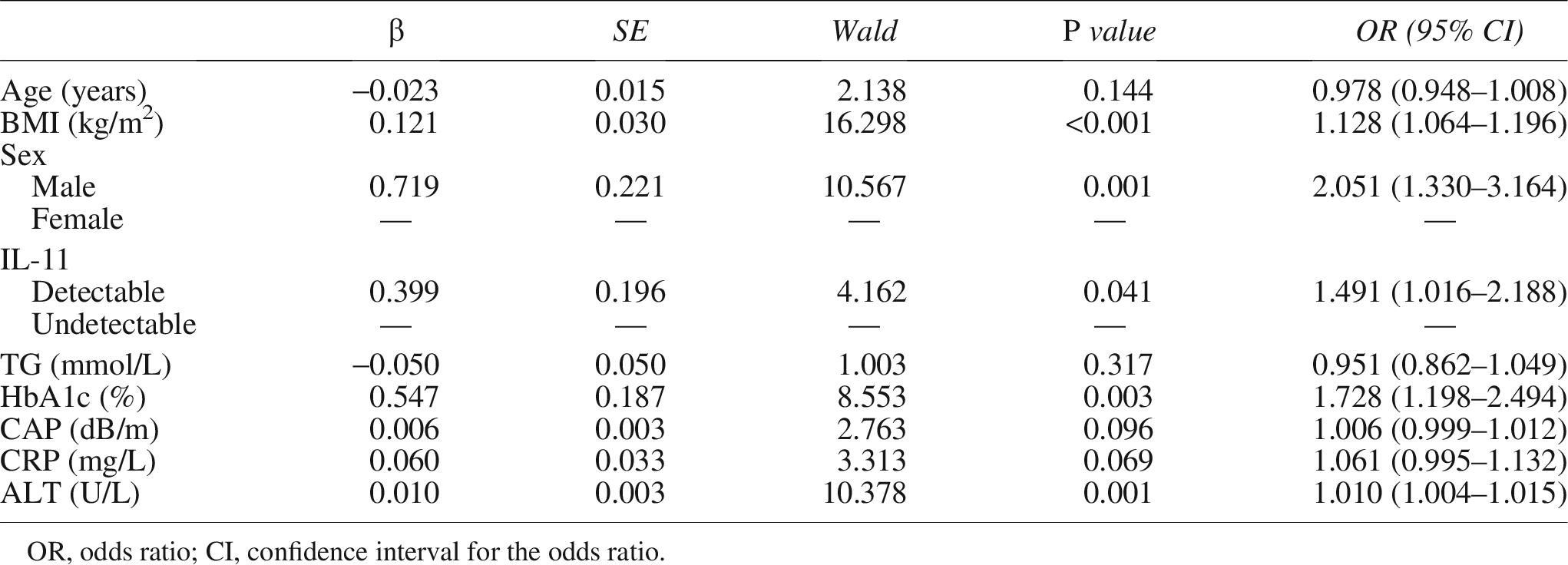
OR, odds ratio; CI, confidence interval for the odds ratio.
To evaluate the incremental predictive value of IL-11, we established two ordinal logistic regression models. Model 1 incorporated conventional risk factors: age, sex, BMI, TG, HbA1c, CRP, ALT, and CAP. Model 2 was further adjusted for IL-11 in addition to all variables in Model 1. The goodness-of-fit between the two models was compared using the LRT, with the results showing: χ2(1) = 4.15, P = 0.042, indicating that the addition of IL-11 to Model 1 significantly improved the model’s predictive ability for hepatic fibrosis (Supplementary Table S2).
Discussion
This study revealed that the serum level of IL-11 is an independent risk factor for the severity of hepatic fibrosis in patients with MASLD, an association that persisted even after the adjustment for multiple metabolic factors, including CAP, CRP, and ALT. These findings extend the conclusions regarding the pro-fibrotic mechanism of IL-11 from preclinical studies (Widjaja et al., 2019) to human diseases. Despite the substantial heterogeneity observed in patients with MASLD compared to animal models, IL-11 has been identified as an independent predictor of hepatic fibrosis even within this complex context, further reinforcing confidence in its potential as a therapeutic target.
Hepatic fibrosis serves as a critical determinant of disease progression and prognostic outcomes in patients with MASLD, with advanced fibrotic stages significantly elevating risks of cirrhotic and hepatocellular carcinoma development while substantially reducing life expectancy (Grady et al., 2026). Despite the substantial global health burden and socioeconomic impact of MASLD, therapeutic options remain markedly limited (Munk Lauridsen et al., 2025). A critical need persists for targeted antifibrotic therapies that directly interrupt HSC activation and extracellular matrix deposition.
Multiple mechanisms may underlie the fibrosis-promoting effect of IL-11 (Tsuchida and Friedman, 2017). On the one hand, upregulated transforming growth factor-B1 stimulates HSCs to secrete IL-11, and IL-11 promotes the trans-differentiation of HSCs into myofibroblasts in an autocrine manner (Widjaja et al., 2019). On the other hand, hepatocytes secrete IL-11 in response to lipid loading and thus stimulate HSCs and cause fibrosis in a paracrine way (Dong et al., 2021). Further experiments confirmed that IL-11 enhances HSCs activation/proliferation and induces human hepatocyte apoptosis via the JNK/ERK pathways (Jiang et al., 2023). Consistent with our results, prior investigations have established IL-11 as a critical mediator of myofibroblast differentiation in cardiovascular and pulmonary tissues, where it drives fibrotic remodeling in response to injury (Ng et al., 2019; Schafer et al., 2017). However, its pathophysiological role in MASLD remains understudied. Our findings demonstrate a positive association between serum IL-11 level and LSM in patients with MASLD, consistent with its pro-fibrotic activity. The pathogenesis of MASLD is highly complex. As indicated by the correlation analysis, LSM is associated with multiple factors including sex, BMI, CRP, and IL-11. Although the correlation coefficient between serum IL-11 and LSM in our study (r = 0.102) was lower than that of liver injury markers such as ALT, the two factors play distinct roles in disease development. ALT primarily reflects the degree of hepatocyte injury, whereas IL-11, as a cytokine, is more likely to act as a driving mediator in the initiation and progression of hepatic fibrosis. Its circulating levels may not fully capture its paracrine/autocrine activity within local liver tissue, which could partially explain the relatively weak correlation observed. Meanwhile, our study further confirmed the clinical relevance of IL-11 through rigorous model comparisons. Although its individual effect size (OR = 1.491) was relatively smaller than certain conventional factors (eg, sex), the LRT demonstrated that adding IL-11 to the model resulted in a statistically significant incremental improvement (P = 0.042). The finding implies that incorporating IL-11 when assessing a patient’s fibrosis risk can provide unique information beyond existing clinical indicators, thereby potentially optimizing risk stratification.
Furthermore, the ordinal logistic regression analysis identified elevated serum IL-11 as an independent risk factor for hepatic fibrosis in patients with MASLD, yet no statistically significant differences in CAP values were observed between IL-11-detectable and IL-11-undetectable groups, and Spearman correlation analysis failed to demonstrate any direct association between IL-11 and hepatic steatosis or lipid concentrations. Moreover, IL-11 showed no significant correlation with conventional markers of liver injury and inflammation, and this lack of association remained consistent both in the entire MASLD cohort and within the IL-11-detectable subgroup. These findings may be caused by the fact that most of the patients recruited in this study only had mild-to-moderate fibrosis. It was reported in animal models that IL-11 is the leading cause of hepatic fibrosis rather than steatosis (Skuratovskaia et al., 2021). Therefore, the phenomenon observed in this study that serum IL-11 correlated with LSM but not with hepatic injury markers in this study may be because the hepatic injury or the inflammation in the patients with MASLD recruited is more likely to be caused by hepatic steatosis but not fibrosis. However, it is worth noting that IL-11 is a dominant regulator of adipocyte differentiation as well as a promoter of lipolysis in adipocytes (Dong et al., 2022). Thus, there remains the possibility that IL-11 may affect the hepatic steatosis via influencing the whole-body lipid homeostasis.
There are several limitations in this study. First, though pathological diagnosis is the gold standard for the diagnosis of hepatic fibrosis, the samples of liver biopsy are hard to access. Alternatively, we employed LSM from FibroScan as the primary index for assessing hepatic fibrosis. Although this method is a well-acknowledged, noninvasive technique for evaluating hepatic fibrosis, its precision is inferior to that of liver biopsy. Second, owing to the relatively limited sample size and the inherent constraints of the real-world disease spectrum in our cohort, this study was unable to encompass the full range of MASLD subtypes. Future studies with larger, multicenter cohorts are warranted to validate our findings across different subtypes and to better characterize the heterogeneous nature of this disease. Moreover, due to the gradual progression of hepatic fibrosis in MASLD, most of the subjects recruited in this study featured only mild-to-moderate hepatic fibrosis. This limited our ability to extrapolate the study conclusions to patients with advanced cirrhosis. From another perspective, identifying patients at high risk of progression at the early, reversible stages of fibrosis represents a core challenge in the clinical management of MASLD. Our study found that even in such a cohort dominated by early to mid-stage disease, IL-11 still demonstrated an independent association with the degree of fibrosis and provided incremental predictive value. This suggests that IL-11 may act as a driving factor in the early phases of hepatic fibrosis, indicating its potential utility for early risk stratification. Thus, efforts are warranted to further clarify the role of IL-11 in a larger sample, in which liver biopsy may be employed. It must be emphasized that this study cannot establish causal relationships. Although our data suggest that IL-11 is a potential evaluative biomarker and therapeutic target, this hypothesis requires validation in future investigations.
Authors’ Contributions
Y.X.: Writing—original draft, formal analysis, methodology, software, and visualization. H.F.: Validation, investigation, and methodology. H.W. and L.S.: Investigation and methodology. Z.W.: Investigation, methodology, and funding acquisition. J.Z., Z.Z., Y.C., Y.X., and X.Y.: Validation and methodology. W.S.: Methodology, project administration, funding acquisition, writing—review and editing, and supervision. R.Z.: Conceptualization, writing—review and editing, resources, and supervision.
Footnotes
Acknowledgments
The authors would like to extend their sincere gratitude to all participants in the study for their invaluable cooperation and unwavering support.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research was funded by the National Natural Science Foundation of China Grant Awards (82474139) and the Postgraduate Research & Practice Innovation Program of Jiangsu Province (SJCX24_0982).
Data Availability
The supplementary figures and tables supporting the findings of this study are available upon the inquiries directed to the corresponding author.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.