
Abstract
Purpose:
To compare the effects of topical bevacizumab and dasatinib on experimental corneal neovascularization and oxidative stress and to determine the effective dose of dasatinib.
Methods:
Forty-two healthy Wistar–Albino rats were randomly divided into six groups. The right corneas of all rats except group 1 were cauterized with silver nitrate. Group 2 received dimethyl sulfoxide, group 3 received topical bevacizumab (5 mg/mL, three times a day), and groups 4, 5, and 6 received dasatinib (2.5 mg/dL, 5 mg/dL, and 10 mg/dL, three times a day respectively), between days 1 and 7. The corneas were removed to determine the level of vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF) values for neovascularization and superoxide dismutase (SOD), malondialdehyde (MDA), and protein carbonyl (PC) levels for analyzing oxidative stress. Nonparametric variance analysis and post hoc Tamhane test was used for statistical analysis.
Results:
The VEGF level was statistically significantly lower in groups 3, 4, and 5 compared with group 2 (P < 0.05). The PDGF, SOD and MDA levels were compared; there was significant difference between all the groups compared with group 2. However, the MDA level for group 6, compared with other treatment groups, had a higher value (P < 0.05). The PC levels compared were statistically significantly lower in groups 3 and 4 compared with group 2 (P < 0.05).
Conclusions:
Dasatinib 2.5 mg/dL was as effective as bevacizumab and seems to be dose-dependent and higher doses than 2.5 mg/dL show higher oxidative stress and an increase in neovascularization.
Introduction
Neovascularization may occur in the cornea due to chemical burns, infection, trauma, contact lens use, immunological, and degenerative diseases. Many factors have been found to play a role in corneal neovascularization. Release of angiogenic growth factors in the cornea is induced by the appearance of inflammatory cytokines and hypoxia. Hypoxia and the above-mentioned reasons cause the release of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF) from corneal tissues. 1 VEGF is involved in many steps of angiogenesis such as proteolytic activity, migration, endothelial cell proliferation, and capillary tube formation. VEGF is secreted by epithelial cells, keratocytes, corneal endothelial, and vascular endothelial cells in the cornea. There are many studies showing that VEGF plays an important role in corneal neovascularization and its inhibition reduces for neovascularization.1–3
PDGF has an angiogenic effect in many organs and tissues. It has been reported that the angiogenic effect of this growth factor is proliferative, migratory, and differential, especially on endothelial precursor cells, bone marrow cells, and mature vascular cells. At the same time, it plays critical roles by acting on various cells during choroidal, retinal, and corneal angiogenesis. 4 Some of these factors are produced by the corneal epithelium, stroma, and endothelium.1,2,4,5 Tears and aqueous humor may also be sources for angiogenic factors. 6 Neovascularization resulting from these conditions may cause permanent vision loss.
Corneal diseases and drugs may cause oxidative stress in the eye. Superoxide dismutase (SOD), malondialdehyde (MDA), and protein carbonyl (PC) are oxidative stress biomarkers, which are used to determine the corneal oxidative stress levels.5–9
VEGF inhibitors such as bevacizumab have been used experimentally to prevent corneal neovascularization. However, an ideal method for effective dosage and desired level of recovery has still not been discovered.1,2
Dasatinib, a tyrosine kinase inhibitor, has been shown to inhibit PDGF and VEGF.10,11 Dasatinib is known to cause cellular damage by increasing oxidative stress with higher doses, as shown in other studies.12,13
According to our research, no study could be found in the literature regarding the use of dasatinib in the treatment of corneal neovascularization. In this study, it is planned to investigate the effect of dasatinib on the experimental corneal neovascularization model by defining the dose and evaluating its effect on VEGF and PDGF levels, which are the main mediators of neovascularization and evaluation of effects on oxidative stress by measuring SOD, MDA, and PC levels.
Methods
The study was conducted with the contribution of the Departments of Ophthalmology, Biochemistry, and Pathology and with the permission of the Fırat University Faculty of Medicine Ethics Committee (2020-12). The authors confirm adherence to the Association for Research in Vision and Opthalmology Statement for the Use of the Association for Research in Vision and Ophthalmology (ARVO). A total of 42 Wistar–Albino male rats with an average weight of 250–300 g were included in the study. A chemical burn was created with the help of silver nitrate but only in the right cornea so that the rats could continue their feeding.
Topical treatment was started 60 min after the burn procedure and continued for 7 days. The rats were divided into six randomized groups, with seven subjects in each group. Group 1 had no corneal burn and was untreated (the control group). A chemical corneal burn was produced in all the other groups. Group 2 was the sham group, where the corneal burn was not treated but given dimethyl sulfoxide, the solvent for dasatinib and bevacizumab; group 3 received bevacizumab 5 mg/mL three times a day; group 4 received 2.5 mg/dL dasatinib three times a day; group 5 received 5 mg/dL dasatinib three times a day; and group 6 received 10 mg/dL three times a day.
Corneal samples were homogenized in 0.01 M phosphate buffer (w:v; 1:19) solution at 16,000 rpm for 4 min under appropriate conditions. The homogenate prepared at 5,000g for 10 min. The supernatants were separated by centrifugation (at +4°C) and worked immediately. Corneal samples were divided into two for histopathologic and biochemical examination. The protein levels in the supernatants were determined by the Lowry method. 14
VEGF and PDGF levels of the supernatants were measured by enzyme-linked immunosorbent assay (ELISA) method.
Determination of VEGF levels
Tissue VEGF levels were measured using the Rat VEGF ELISA kit (Sunred Biotechnology Company, catalog no: 201-11-0660) in accordance with the manufacturer’s instructions. The kit is specifically validated for the quantitative analysis of VEGF in rat tissue samples.
Absorbances were read spectrophotometrically at 450 nm on an EPOCH 2 (BioTek Instrument, Inc, USA) microplate reader. Results were expressed as nanograms per milliliter. The measuring range of the kit was 11–3,000 ng/mL, and the sensitivity was 10,127 ng/mL. Intra-assay Coefficients of Variability (CV) was <9%; inter-assay CV was <11%.
Determination of PDGF levels
Tissue PDGF levels were measured using the Rat PDGF ELISA kit (Sunred Biotechnology Company, catalog no: 201-11-0692) according to the manufacturer’s protocol. This kit is validated for the quantitative detection of PDGF in rat tissue samples. Absorbances were read spectrophotometrically at 450 nm on an EPOCH 2 (BioTek Instrument, Inc, USA) microplate reader. Results were expressed as picograms per milliliter. The measuring range of the kit was 8–2,000 pg/mL, and the sensitivity was 8 pg/mL. Intra-assay CV was <10%; inter-assay CV was <12%.
Histopathological examination
Following euthanasia, the eye balls were enucleated and fixed in 10% buffered formalin solution and cut in dorsoventral position and routinely processed, embedded in paraffin, and sectioned in 5-μm thickness and stained by hematoxylin and eosin. The selected sections were also stained Masson’s trichrome.
Measurement of corneal thickness
The overall thickness of the cornea and the thickness of its epithelial layer were measured using the Olympus BX51 (Olympus Corp., Tokyo, Japan) digital light microscope in conjunction with the Image software. The measurements were performed at three distinct histological sites, including both the central cornea and the peripheral regions adjacent to the limbus.
Immunohistochemistry
Avidin–Biotin Complex method was used for immunohistochemistry. The eyes were sectioned in dorsoventral position at 5 µm, incubated in primary antibodies, including VEGF (Bioss, 1/100, bc-0279R) and PDGF (PDYN, 1/100, A5830), which are validated for rat samples. Then immunodetection was performed for 60 min at 37°C with biotinylated goat anti-polyvalent, followed by peroxidase-labeled streptavidin using a labeled streptavidin biotin kit with a 3-amino-9-ethylcarbazol (ThermoFisher Scientific, Rockford, IL, USA), as the chromogen substrate.
Oxidative stress measurements
Corneal tissues taken into tubes containing 0.4 mL 0.01 M phosphate buffer solution (PBS; pH 7.4) were at 4°C. It was homogenized for 3 min at 16,000 rpm. A clear supernatant was obtained by centrifugation by homogenates at 5000g for 15 min (+4°C). The samples were stored under appropriate storage conditions to perform the measurements for MDA, SOD, and PC. Protein levels in the supernatants were determined by the Lowry method. 14 The principle of this method is based on the fact that proteins form a blue color with the Folin–Phenol reagent in alkaline medium. MDA levels measured the technique described by Ohkawa et al. 15 Spectrophotometrically, using the thiobarbituric acid (TBA) reaction method was considered the principle of this method; in an acidic environment (pH: 3.5) and under aerobic conditions, the pink color formed by MDA, which is released as a result of lipid peroxidation, and TBA. It is based on the spectrophotometric measurement of the complex at a wavelength of 532 nm, and results were expressed as nanomoles per milligram of protein. SOD activity was determined using the method of Sun et al. 16 Enzymatic activity, evaluated by measuring the ability to inhibit the photoreduction of nitro blue tetrazolium (NBT). 505 nm of the red colored formazone chromogen formed as a result of reduction. SOD activity is measured as a result of reading the wavelength spectrophotometrically. The intensity of the red color is inversely proportional to the SOD activity. SOD activity per milligram of protein is expressed as a unit. The unit of SOD activity is defined as the amount of enzyme required to prevent a 50% reduction of NBT.
PC was evaluated with a colorimetric method using 17 ; 2,4-dinitrophenylhydrazine, prepared in supernatant hydrochloric acid (HCl) (2,4-Dinitrophenylhydrazine (DNPH); 10 mM), was added to the solution. The mixture was vortexed and at room temperature for 1 h incubated. Trichloroacetic acid (20%) was added to the mixture and centrifuged at 10,000g for 5 min.
The proteins were precipitated. Then, the pellets were mixed with ethanol–ethyl acetate (1:1 v/v) and three times washed. Finally, 6 M guanidine-HCL was used to dissolve the pellets of each sample. The carbonyl content was read at a wavelength of 360 nm (ϵ = 22,000/M/cm), and the results in nanomole were expressed as carbonyl per milligram protein.
The statistical analysis was conducted with the Statistics Package for the Social Sciences version 24 (SPSS for MacOS, IBM Corp., New York, USA) package program. Nonparametric variance analysis (Kruskal–Wallis) and post hoc Tamhane test were used for statistical analysis of the data. P-values <0.05 were considered statistically significant.
Results
The VEGF ELISA levels were significantly higher in the group 2 compared with those of group 1 (P = 0.007). The group 3 VEGF levels were significantly lower than in group 2 (P < 0.01). In groups 4 and 5, VEGF levels decreased and it was statistically significant, but in group 6 there was no statistically significant difference when compared with group 2 (P = 0.893). In group 6, VEGF level was 530.30 ± 228.10 ng/mL, and there was an increase compared with the control group, but there is no statistically significant difference compared with group 1 (P > 0.05).
When the PDGF ELISA levels were compared, there was significant difference between group 1 and 2 (P = 0.041). When group 2 and treatment groups were compared, there was a statistically significant difference between all treatment groups (P < 0.05). The VEGF and PDGF levels are shown in Table 1.
Corneal VEGF and PDGF ELISA Levels in Groups
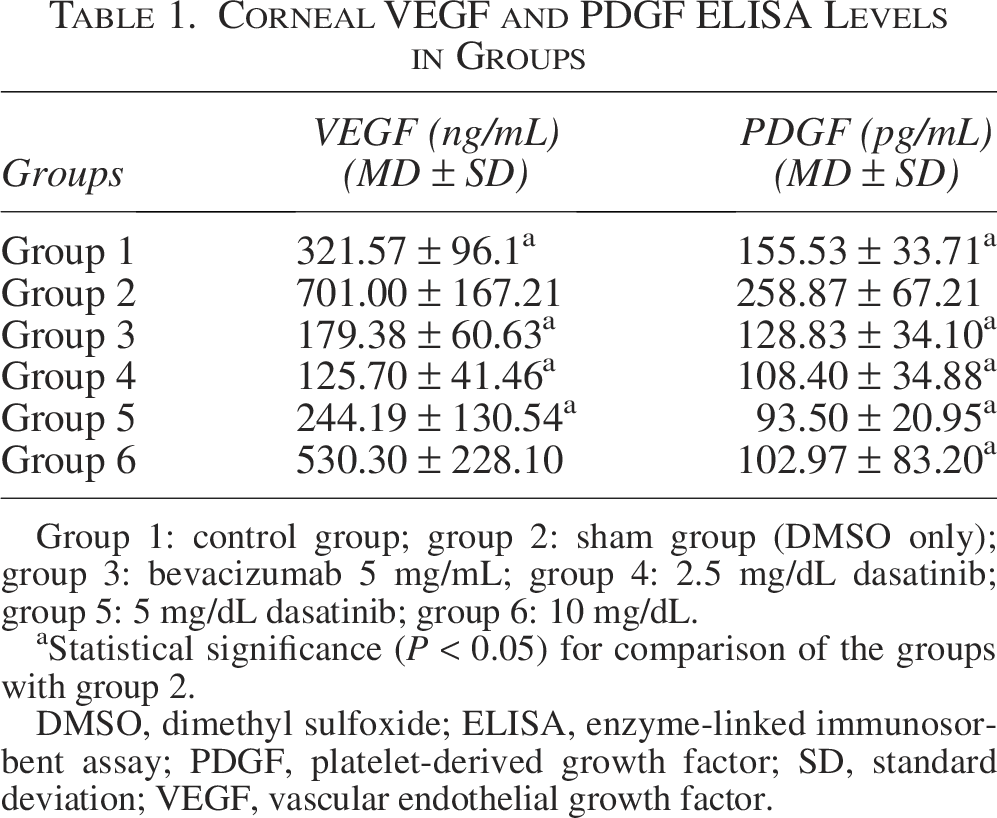
Group 1: control group; group 2: sham group (DMSO only); group 3: bevacizumab 5 mg/mL; group 4: 2.5 mg/dL dasatinib; group 5: 5 mg/dL dasatinib; group 6: 10 mg/dL.
Statistical significance (P < 0.05) for comparison of the groups with group 2.
DMSO, dimethyl sulfoxide; ELISA, enzyme-linked immunosorbent assay; PDGF, platelet-derived growth factor; SD, standard deviation; VEGF, vascular endothelial growth factor.
When the groups were compared for SOD levels, there was a statistically significant difference between group 1 and group 2 (P < 0.01). The SOD levels for group 3–6 were statistically significantly higher than the group 2 (P < 0.05). When MDA values were compared, there was a statistically significant difference between group 1 and group 2 (P < 0.05). For the treatment groups and group 2 also, lower MDA levels and a statistically significant difference were observed, but group 6 MDA levels were higher than groups 3, 4, and 5, and there was a statistically significant difference (P < 0.05). In terms of PC values, there was a statistically significant difference between group 1 and group 2 (P < 0.01). There was a statistically significant difference with group 2 between group 3 and 4 (P = 0.044 and P = 0.032, respectively). There was no statistically significant difference with group 2 between group 5 and 6 (P = 0.81 and P = 0.84, respectively). The SOD, MDA, and PC levels are shown in Table 2.
Corneal SOD, MDA, and PC Levels in Groups
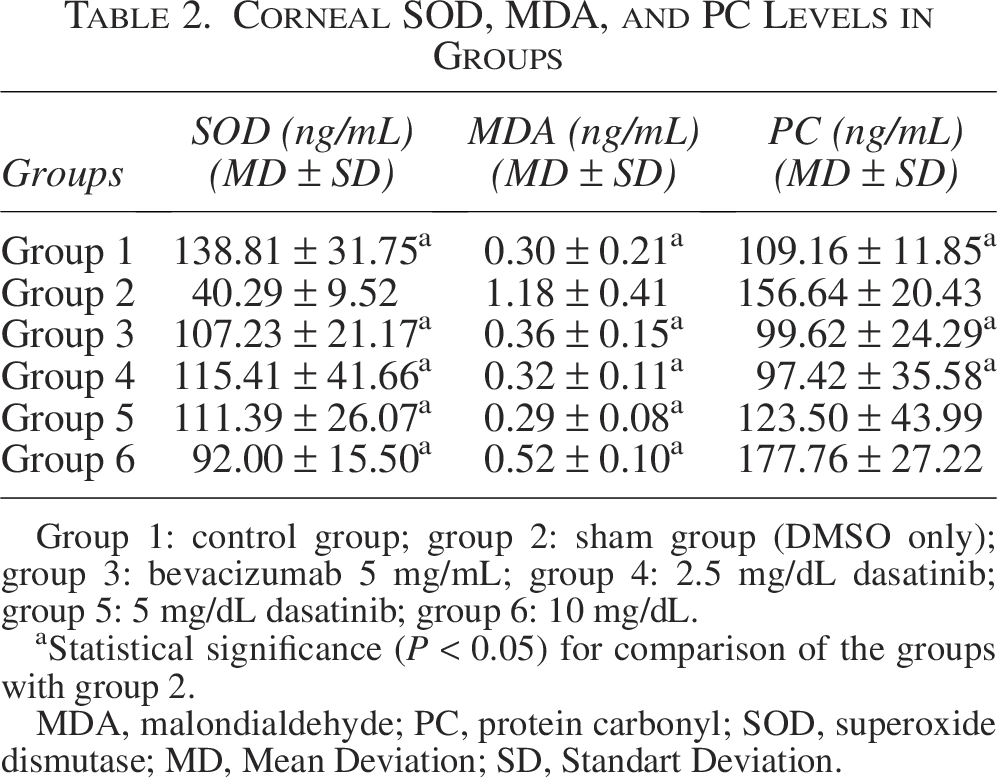
Group 1: control group; group 2: sham group (DMSO only); group 3: bevacizumab 5 mg/mL; group 4: 2.5 mg/dL dasatinib; group 5: 5 mg/dL dasatinib; group 6: 10 mg/dL.
Statistical significance (P < 0.05) for comparison of the groups with group 2.
MDA, malondialdehyde; PC, protein carbonyl; SOD, superoxide dismutase; MD, Mean Deviation; SD, Standart Deviation.
In the control group, corneal histology showed well-organized epithelium and basement membrane, stroma, Descemet’s membrane, and endothelium. There were no histological lesions in the corneas of group 1 (Fig. 1A). However, the corneas in group 2 showed the moderate to severe corneal neovascularization, hemorrhage, multifocal moderate polymorphonuclear cell, and macrophage infiltrations (Fig. 1B). These changes were absent or minimal in other treatment groups (Fig. 1C–F). However, the treatment groups showed the corneal stromal scar formation thinning of epithelial layer and minor epithelial erosions (Fig. 1D–F). Subepithelial scars consisted of fibroblasts or collagen fibers. All the histological lesions in groups are summarized in Table 3.
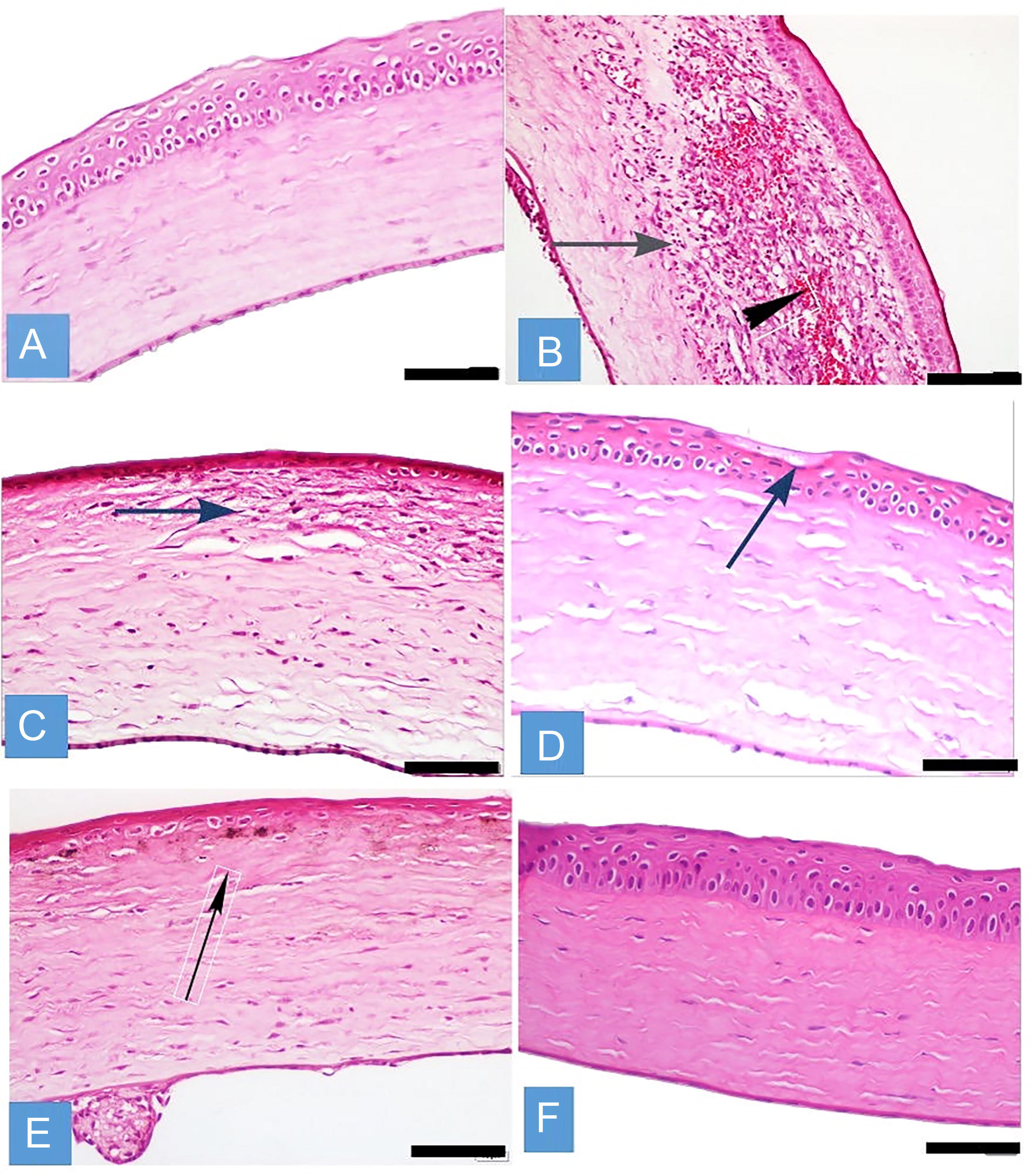
Comparison of histological changes in groups, H&E, ×40. Bars:40 µm.
Distribution of Histopathological Changes in Sham, Control, and Experimental Groups
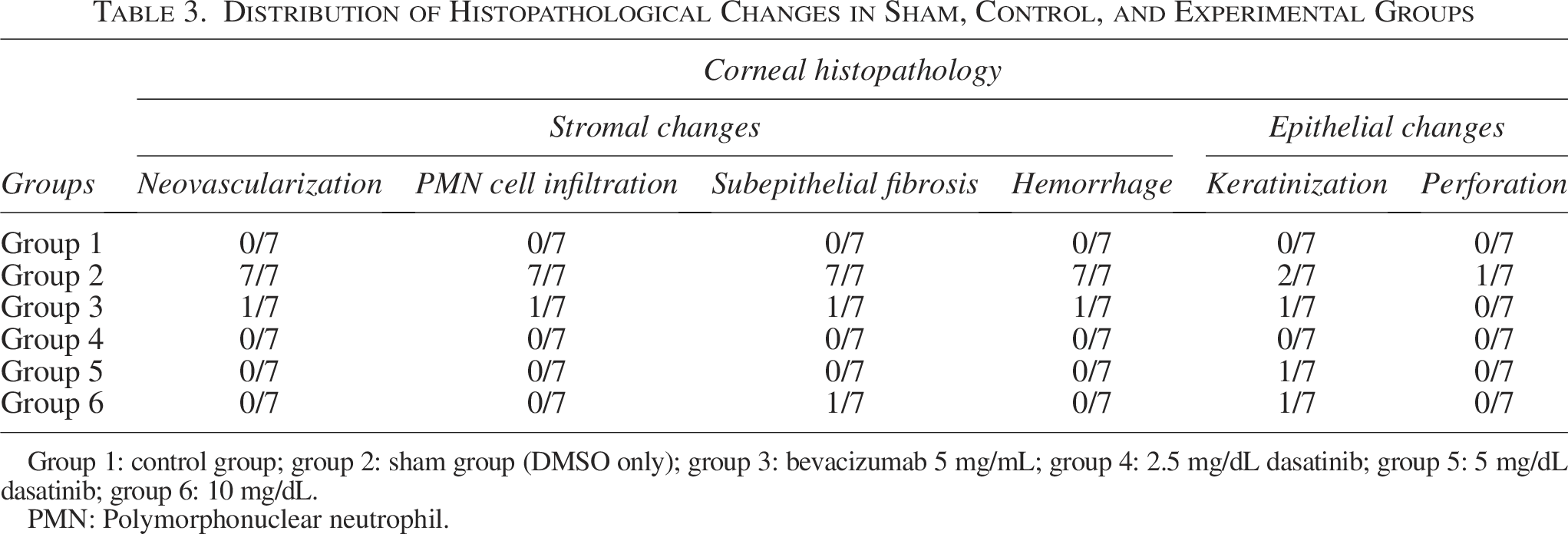
Group 1: control group; group 2: sham group (DMSO only); group 3: bevacizumab 5 mg/mL; group 4: 2.5 mg/dL dasatinib; group 5: 5 mg/dL dasatinib; group 6: 10 mg/dL.
PMN: Polymorphonuclear neutrophil.
The group 3, 5, and 6 treatments reduced inflammatory infiltrate and vascularization. Corneal thickness and central corneal epithelial thickness were altered in treatment groups as compared with group 2. When the other groups and group 2 were compared for corneal thickness measurement, all of the measurements were higher than the mean thickness of group 2, and groups 1, 3, 4, and 5 showed statistical significance (P < 0.05) when compared with group 2 (Table 4). In terms of epithelial thickness, there is a statistical difference (P < 0.05) between group 2 and groups 1, 4, and 6. However, there was no statistical difference between group 3 and 5 with group 2.
Central Corneal Epithelial and Corneal Thickness in Groups
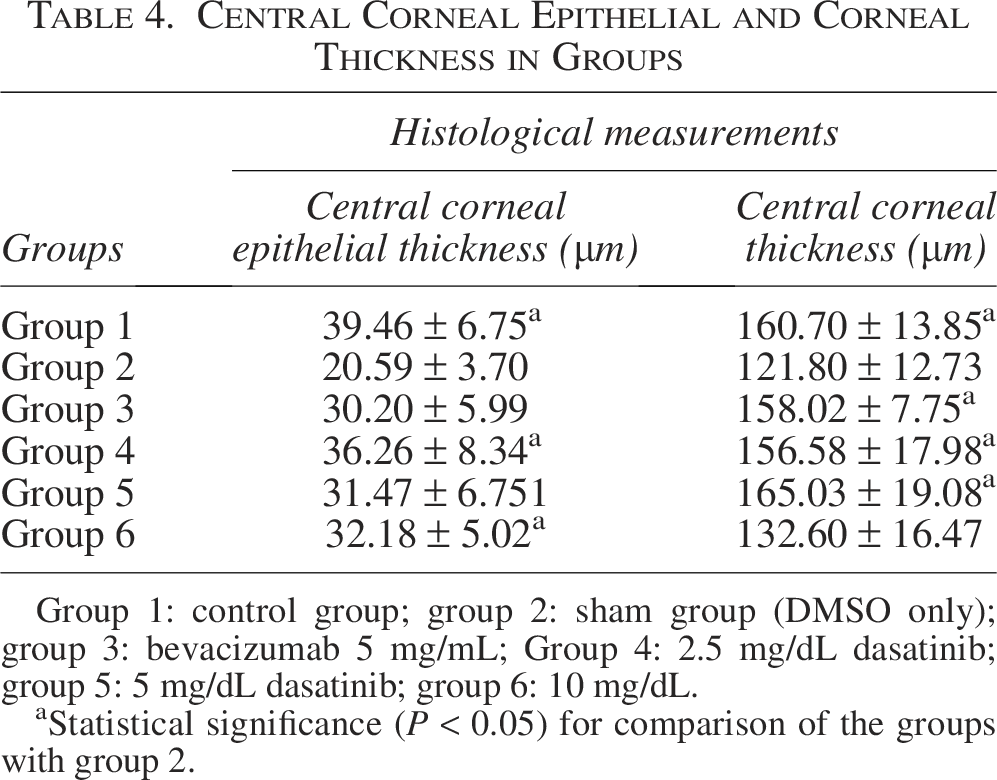
Group 1: control group; group 2: sham group (DMSO only); group 3: bevacizumab 5 mg/mL; Group 4: 2.5 mg/dL dasatinib; group 5: 5 mg/dL dasatinib; group 6: 10 mg/dL.
Statistical significance (P < 0.05) for comparison of the groups with group 2.
The positive immunoreaction of VEGF was characterized by red granules in cytoplasm of infiltrated polymorphonuclear cells, macrophages, neovascular endothelium, and limbal vasculature. Positive staining for VEGF was detected in groups 2 and 4 in corneal inflammatory infiltrate. In other treatment groups, no positive immunostaining was detected (Fig. 2).

Comparison of immunohistochemical analysis of the VEGF in corneas of all groups, ×40.
Positive expression of PDGF was seen in all the cases in sham group. In this group, widespread and severe expression of PDGF was detected by red granules in cytoplasm of fibroblasts, vascular endothelium, and keratocytes in subepithelial scar tissue (Fig. 3). However, in the treatment groups, focal and mild immunoreactivity was present in cases only having corneal fibrosis where subepithelial fibrosis was detected. In most of the treatment groups, there was no positive immunoreaction against PDGF.

Comparison of immunohistochemical analysis of the PDGF in corneas of all groups, ×40.
Discussion
In this study, we aimed to find the most effective dose by comparing the effects of dasatinib and bevacizumab on VEGF and PDGF, which are important angiogenesis markers, and MDA, SOD, and PC, which are oxidative stress markers, in experimental corneal neovascularization. When the results were compared, it was seen that dasatinib, especially the 2.5 mg/dL dose, had a similar effect to bevacizumab and had a statistically significant effect on angiogenesis and oxidative stress markers compared with the sham group. These effects were observed to decrease at higher dasatinib doses.
Dasatinib is a tyrosine kinase inhibitor used in the treatment of Philadelphia chromosome-positive chronic myeloid leukemia that inhibits VEGF and PDGF. Also, dasatinib suppresses the release of inflammatory cytokines from T cells and other inflammatory cells. 15 Li et al. observed angiogenesis inhibition in corneal neovascularization and Human umbilical vein endothelial cells (HUVEC) cells with nanostructured lipid carrier and stated that dasatinib dissolved in this carrier is promising for the treatment of corneal neovascularization. 18
VEGF and PDGF both play an important role in corneal neovascularization. Inhibition of these growth factors plays an important role in stopping and regressing neovascularization.1,3,4,19–23 In a study where the binding profile of bevacizumab to human, mouse, and rat VEGF was tested directly by ELISA, bevacizumab was shown to bind to mouse and rat VEGF-A at antibody concentrations above 10 μg/mL. 24 Although bevacizumab binding to rodent VEGF-A at low concentrations is limited, it may explain the antineovascular effects observed in rodent models. The majority of monoclonal antibodies in clinical use show limited cross-reactivity between species. 24 This allowed us to use the effect of the molecules in our study on VEGF and PDGF in an animal model. In light of this information, we determined the use of a dose above this concentration in our study. This study is unique in terms of investigating the effects of dasatinib on VEGF and PDGF in an experimental corneal neovascularization model and evaluating the effect on neovascularization immunohistochemically with oxidative stress.
In this experimental corneal neovascularization model, bevacizumab 5 mg/dL and dasatinib at doses of 2.5 and 5 mg/dL produced a statistically significant decrease in VEGF levels. Considering the PDGF levels, a significant decrease is observed in all treatment groups compared with group 2. Groups 3 and 4 showed ideal levels of neovascular inhibition and oxidative stress, but when these groups were compared in detail, we observed that 2.5 mg/dL dasatinib showed lower VEGF and PDGF levels, with similar changes in markers of oxidative stress. Similarly, in the study by Lei et al. on corneal neovascularization, dasatinib and erianin were coencapsulated in nanostructured lipid carriers and a significant decrease was found in neovascular parameters such as Tumor necrosis factor-α (TNF-α), VEGF-A, and Hypoxia-inducible factor-1α (HIF-1α). 25 As Lei et al. stated, our study shows that the application of dasatinib in corneal neovascularization holds promise in the future.
Bevacizumab is actively used in corneal neovascularization. According to studies, it has a low side effect profile and good effectiveness.21,26 However, new and more effective alternative treatments continue to be investigated. Therefore, in our study, we aimed to define the effective and safe dose of dasatinib for an alternative treatment option. VEGF, PDGF, Fibroblast growth factor (FGF), and Nitric oxide (NO) inhibitors, drugs affecting the Rho-associated coiled-coil kinase (Rho/ROCK), Wnt, and NOD1 pathways, and tyrosine kinase inhibitors to prevent corneal neovascularization are drugs working in this field. 27 Tyrosine kinase inhibitors that act on many pathways, such as dasatinib, are promising in the treatment of corneal neovascularization.10,11,28–31
Several studies have investigated the response of the cornea to oxidative damage. SOD is an enzymatic antioxidant with three isoforms in the cornea, which plays a role in the primary antioxidant defense of the cornea, and whose enzyme levels decrease when the oxidative stress level increases.6,32–34
MDA, which has cytotoxic effects, is formed as a result of lipid peroxidation of reactive oxygen radicals. High MDA levels are indirect indicators of decreased antioxidant capacity or increased oxidative stress. Since MDA is formed as a result of peroxidation of polyunsaturated fatty acid in the cell membrane, it can also indirectly show membrane damage.32,35
PC, which is formed due to oxidative stress causing protein oxidation, is the most widely used marker of protein oxidation and is used to evaluate oxidative stress. 36 The most important measurement advantage is that the damage occurs in the early period and is stable. 37 In many studies evaluating corneal neovascularization and oxidative stress, it has been shown that SOD values decrease and PC and MDA values increase.38,39
According to our study, when oxidative stress markers were evaluated, it was observed that SOD and MDA levels changed statistically significantly in all groups compared with group 2. However, SOD levels seem to decrease even more, especially with increasing dasatinib doses. Additionally, MDA levels due to oxidative stress increased as dasatinib dose increased in treatment groups, and group 6 shows a statistically significant increase compared with other treatment groups. When the PC levels were examined, there was a statistically significant difference in the subjects in groups 3 and 4 compared with group 2. However, when higher dasatinib doses were compared with the sham group, it was observed that there was no statistically significant difference in terms of PC levels and that PC levels increased in these groups and even increased to higher levels in the subjects who received 10 mg/dL dasatinib than the sham group.
While 5 mg/dL dasatinib significantly decreased VEGF and PDGF levels, it increased oxidative stress even though it was not statistically significant in SOD and MDA levels, and it increased oxidative stress on PC levels statistically. Although the 5 mg/dL dasatinib dose reduces neovascularization, it increases oxidative stress and probably the ideal treatment dose is below this level. The strongest decrease in PDGF levels is observed at the 10 mg/dL dasatinib dose; it is not an ideal dose due to the increase in VEGF levels and the severe oxidative stress seen in SOD, MDA, and PC levels. Moreover, this increased oxidative stress may have caused an increase in VEGF and may have contributed to neovascularization. Oxidative stress induced by dasatinib has been demonstrated at the cellular level in many studies.12,13,40 Therefore, in our study, we thought that cellular oxidative stress levels should be evaluated in determining the dose that can be used in the treatment of corneal neovascularization.
Since there was no corneal neovascularization topical dose study on dasatinib before, and there were no in vivo and in vitro toxic studies, we tried to find the most effective dose of dasatinib in our study. We found the most effective and safe dose to be 2.5 mg/dL dasatinib in this study, but further studies are needed to show whether it is effective at lower doses.
Our study had some limitations. First, the pharmacokinetics, pharmacodynamics, and side effects of the drug were not evaluated. Second, only short-term effects were evaluated; long-term effects were not evaluated. Third, the effects of the drug on other neovascularization pathway markers, other oxidative stress markers, and other administration methods were not considered. And finally, such as HUVEC, cell culture studies can be done to support our in vitro work.
In conclusion, bevacizumab 5 mg/mL and 2.5 mg/dL dasatinib are effective to reduce neovascularization on VEGF and PDGF levels in an experimental corneal neovascularization model. Also, this dose can be safe; hence, it did not observe an increase in oxidative stress biomarkers such as SOD, MDA, and PC. Dasatanib doses higher than 2.5 mg increase oxidative stress even though they reduce neovascularization and the higher doses may not be appropriate. Further studies are needed to evaluate the efficacy of dasatinib on corneal neovascularization.
Authors’ Contributions
Concept: H.Y., M.B., and M.C. Design: H.Y., M.B., M.E., and A.D. Practices: H.Y. and M.C. Data collection or processing: H.Y., M.C., M.E., and A.D. Biochemistry: N.I. Pathology: Y.E. and C.A.I. Analysis or interpretation: M.B., M.C., and A.D. Literature search: H.Y., M.B., M.E., and A.D. Writing: H.Y., M.B., and M.C. All authors have read and approved the final article.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
No specific funding was received for this study.
Ethical Approval
The present study was conducted with the approval of the Animal Research Ethics Committee of Firat University (ID: 2020-12).
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.