
Abstract
Purpose:
Rho-associated kinase (ROCK) regulates fibrosis and angiogenesis. This study evaluated the effects of the topical ROCK inhibitor HA1077 (fasudil) to attenuate corneal fibrosis and corneal neovascularization (CNV) in vivo.
Methods:
Primary human corneal stromal fibroblasts (hCSF) and New Zealand White rabbits (n = 12) were used. Corneal fibrosis and CNV in vivo were provoked by alkali injury. Immediately post-injury, eyes received topical balanced salt solution (BSS) or HA1077 (3 nM twice/day for 3 days). Clinical slit-lamp biomicroscopy and stereomicroscopy gauged corneal haze/fibrosis (Fante’s score) and CNV (morphometric score) in live rabbits. Post-euthanasia, H&E, immunofluorescence, and terminal deoxynucleotidyl transferase-mediated dUTP nick end labeling (TUNEL) assays analyzed α-smooth muscle actin (α-SMA), filamentous actin (F-actin), endoglin, CD11b, and apoptotic cells.
Results:
HA1077 treatment to hCSF did not alter viability, morphology, and proliferation ability at 3 nM or lower doses. Topical HA1077 (3 nM) treatment significantly reduced corneal haze/fibrosis (P < 0.0001) and CNV (P < 0.0001) in vivo at days 7 and 14 compared with the corresponding controls. Histological H&E analysis revealed retrieval of overall corneal health with a remarkable decrease in fibrotic (myofibroblasts), angiogenic (neovessels), and immune cell infiltration in rabbit corneas treated with HA1077 than the control corneas. HA1077 therapy significantly reduced α-SMA+, F-actin+, and endoglin+ cells, markers of fibrosis and CNV. Intraocular pressure (IOP) remained within the normal physiological range of eyes with HA1077. TUNEL assay revealed the tolerability of the examined HA1077 regimen in vivo.
Conclusions:
The tested HA1077 dosage regimen is effective and tolerable to rabbit eyes in abrogating corneal fibrosis and CNV triggered by alkali injury in vivo without major adverse effects. ROCK inhibition represents a promising therapeutic strategy for vascularized and fibrotic corneal wounds but warrants additional dose–response in vivo studies.
Introduction
The factors contributing to the loss of vision resulting from a robust corneal wound healing response after severe corneal injury include the formation of vasculature in the normally avascular cornea and the concurrent establishment of corneal scars. 1 Reestablishing a transparent and avascular cornea is critical for maintaining normal vision following severe corneal injuries. Corneal neovascularization (CNV) and corneal fibrosis are frequent sequelae of a robust corneal wound healing response that accompanies a corneal insult resulting from trauma (chemical, desiccation, laceration, and penetration, including surgical intervention)2–4 or infection (bacterial, fungal, and viral).5–7 Visual acuity is actively threatened when the disrupted balance between pro- and antiangiogenic and fibrotic factors fails to reestablish homeostasis at the conclusion of active wound healing, leading to the persistence of microvasculature and myofibroblasts at the site of previous injury.8,9 Chemical injuries to the cornea are frequently observed and often severe occupational hazards, particularly in industrial and military working environments. 10 Chemical injuries to the cornea, especially those involving basic compounds such as sodium hydroxide (NaOH), routinely lead to a significant degree of sight-threatening CNV and corneal fibrosis.11,12
CNV threatens vision following corneal insult and is estimated to affect >4% of the U.S. population, with approximately 1.4 million new cases annually; approximately 12% of affected individuals experience measurable visual deficits.13–15
Currently, the clinical treatment of corneal pathology involving fibrosis and CNV is challenging and often yields suboptimal results, as contemporary pharmacologic and surgical therapeutic options are generally associated with significant deleterious effects, low efficacy, and the potential for failure.16,17 In the event of total failure, a corneal transplant is needed, but this restorative option may be limited due to the lack of suitable transplant quality donor corneal tissues and immunological rejection. 18 Corticosteroids are frequently employed in CNV treatment but are associated with severe complications, including cataract formation, the initiation of glaucoma, and ocular infection. 19 Clinical trials have been conducted to evaluate the safety and efficacy of exogenous anti-vascular endothelium-derived growth factor (VEGF) antibodies and alternative antiangiogenic proteins in mitigating CNV with limited success. The currently available CNV treatment options are hampered by inefficiency, a limited duration of relief, the potential for serious complications, and low clinical efficacy. 20 Although targeted gene therapies for the treatment of CNV are in development, pharmacologic treatments remain the mainstay in the treatment of CNV until their approval and dissemination.
New pharmacologic agents that engage distinct cellular pathways are attractive for modulating post-traumatic corneal angiogenic and fibrotic responses. The Rho-associated kinase (ROCK) family (ROCK1/ROCK2) comprises serine/threonine kinases activated by Rho GTPases (notably RhoA) that control actin stress fiber formation and actomyosin contractility, thereby influencing adhesion, migration, proliferation, survival, and apoptosis. 21 Through the phosphorylation of downstream targets, ROCK facilitates cytoskeletal organization, cell contractility, focal adhesion assembly, and stress fiber formation. 22 In the cornea, ROCK activity has been implicated in epithelial differentiation and cell cycle progression, intercellular adhesion, and stromal phenotype transitions,23–25 while Rho signaling is integral to epithelial migration, proliferation, and focal adhesion dynamics during wound healing. 26 Given its roles in fibrosis and CNV across tissues, ROCK is a promising target for therapeutic inhibition. 27
Clinically, two ROCK inhibitors are approved outside the United States, fasudil (HA1077) for cerebral vasospasm and ripasudil for glaucoma/ocular hypertension. 28 Fasudil is a small-molecule, ATP-competitive inhibitor that targets the kinase domain of ROCK27 and exhibits antifibrotic activity across hepatic, 29 pulmonary, 30 renal, 31 peritoneal, 32 cardiac, 33 and ocular 34 models in vitro and in vivo. In ophthalmology, ROCK inhibition has been leveraged primarily in glaucoma and ocular surface/retinal indications, 35 where it enhances trabecular outflow to lower intraocular pressure, improves ocular perfusion, supports retinal ganglion cell survival and axonal regeneration, and facilitates epithelial/endothelial wound healing. 36 ROCK inhibitors also demonstrate antiangiogenic effects in endothelial systems and experimental CNV37,38 and suppress Transforming Growth Factor Beta 1 EDTA – Ethylenediaminetetraacetic Acid (TGF-β1)-induced α-smooth muscle actin (α-SMA) expression, linking ROCK blockade to antifibrotic actions at the stromal-cell level.39,40 Additional preclinical work in rabbit and nonhuman primate corneas supports the roles of Rho/ROCK in epithelial and endothelial repair.41,42
Despite this rationale, the therapeutic potential of fasudil for corneal fibrosis accompanied by CNV has not been systematically tested in vivo. Here, we evaluate the effect of topical fasudil (HA1077) in a rabbit alkali injury model that produces both stromal fibrosis and CNV to provide an assessment of a single-agent approach.
Methods
Primary human corneal fibroblast cultures
Primary human corneal stromal fibroblast (hCSF) cultures were generated from donated human corneas obtained from a regional eye bank (Saving Sight, Kansas City, MO, USA). The corneas were washed twice with serum-free minimum essential medium (MEM) (Thermo Fischer Scientific, Grand Island, NY, USA). The corneal epithelium and endothelium were dissected free of the stroma with a surgical blade, and the remaining stromal sections were subdivided for explant culture. The stromal sections were placed convexly down onto a sterile 10-cm2 tissue culture dish and maintained in a humidified 5% CO2 incubator at 37°C. The cultures were incubated in MEM supplemented with essential amino acids, sodium pyruvate, MEM vitamins, penicillin/streptomycin, and 10% fetal bovine serum (MEM plus media) for approximately 21 days, and the medium was fully replaced every other day. hCSF were collected via trypsinization. In brief, 2 mL of 0.25% trypsin-EDTA was added to the plate, and the plate was kept in a CO2 incubator for 4–5 min. Then, the plate was observed under a microscope to observe the dissociation of the cells, and two volumes of MEM plus media were immediately added for neutralization. The cell suspension was centrifuged at approximately 110 × g for 5 min (equivalent to 1,000 rpm with a rotor radius of 10 cm), and cells were seeded at a density of 7.5 × 104 cells/well in six-well plates and allowed to reach 60%–70% confluence before experimental use. hCSF cultures of passage numbers 3–4 were used in this study. HA1077 (Cat# 0541) was procured from Tocris (Bio-Techne Corporation, Minneapolis, MN, USA) with purity ≥98% and used in this study.
Cytotoxicity studies
Cellular viability was evaluated via a trypan blue exclusion assay (Sigma-Aldrich, St. Louis, MO, USA). Primary human corneal fibroblasts (hCSF) were treated with HA1077 at the final concentrations of 0, 0.1, 0.5, 1, 2, 3, 4, or 5 nM. After 48 h, the cells were trypsinized and suspended in 0.4% trypan blue solution (Invitrogen, Carlsbad, CA, USA), and both nonviable (blue) and viable (unstained) cells were counted. Cellular viability (percentage) was calculated as the proportion of viable cells relative to the total cell count via an automated cell counter (Countess, Invitrogen).
Morphological changes in hCSF following HA1077 treatment were recorded via phase contrast microscopy (Leica, DMIL, Bannockburn, IL, USA). hCSF cultures treated with various concentrations of HA1077 (0–5 nM) for 48 h were examined, and representative images were captured via a digital imaging system (Leica DFC290, Bannockburn) fitted with a microscope.
The effect of HA1077 on hCSF apoptosis was examined via a terminal deoxynucleotidyl transferase-mediated dUTP nick end labeling (TUNEL) assay. hCSF cultures were treated with or without HA1077 (3 nM) for 48 h, washed with phosphate-buffered saline (PBS), and fixed with fresh 4% paraformaldehyde at room temperature for 20 min. The TUNEL assay was performed via a commercial ApopTag apoptosis detection kit according to the manufacturer’s instructions (S7165, ApopTag Red In Situ Apoptosis Detection Kit, Millipore Sigma, Burlington, MA, USA). In brief, the fixed cells were permeabilized with ethanol:acetic acid (2:1 ratio; at −20°C) and treated with TdT enzyme (37°C for 1 h), stop wash buffer (room temperature for 10 min), and anti-digoxigenin rhodamine conjugate (room temperature for 30 min), with assay kit reagents. Cells were mounted with Vectashield 520 containing 4′,6-diamidino-2-phenylindole (DAPI; Vector Laboratories, Burlingame, CA, USA) for the visualization of nuclei and photographed with a digital camera (SpotCam RT KE, Diagnostic Instruments, Inc., Sterling Heights, MI, USA).
In vivo rabbit model of corneal fibrosis and neovascularization
Twelve adult female New Zealand White rabbits weighing 1.8–2.2 kg (Charles River Laboratories, Wilmington, MA, USA) were used in this study. All animal work proposed for this study was approved by the Institutional Animal Care and Use Committees of the University of Missouri-Columbia and Harry S. Truman Memorial Veterans’ Hospital. All animals were treated in accordance with the Association for Research in Vision and Ophthalmology Statement for the Use of Animals in Ophthalmic and Vision Research. A well-established corneal alkali injury rabbit model of corneal fibrosis and CNV was utilized. 43 The rabbits were anesthetized via intramuscular injection of ketamine (35–50 mg/kg) or xylazine (5–10 mg/kg). Two drops of 0.5% proparacaine hydrochloride were instilled into the eye several minutes prior to alkali injury to provide topical anesthesia. A wire eyelid speculum was used to permit the full visualization of the corneal surface. A 7-mm filter paper disc soaked in 1 N NaOH was applied to the central cornea for 1 min and then removed, after which the cornea was washed with balanced salt solution (BSS) for 30 s. This optimized protocol results in severe scarring and CNV in rabbits in vivo. 44
Preparation of ROCK inhibitor (HA1077) and treatment regimen
The HPLC-grade ROCK inhibitor (purity ≥98%) was procured from Tocris (Cat# 0541; Bio-Techne Corporation, Pittsburgh, PA, USA). Prior to corneal wounding, the animals were randomly divided into two groups: Group 1 (6 rabbits) served as a control, and following corneal wounding of the left eye, they received 50 µL of BSS topically twice daily for 3 days. Group 2 (6 rabbits) served as the treatment cohort and received 50 µL of HA1077 (3 nM) topically twice daily for 3 days following corneal wounding. The HA1077 dose was selected based on preliminary dose–response studies, and this dose does not show any significant cellular toxicity. Contralateral untreated eyes served as negative controls.
Corneal haze (fibrosis) and CNV were monitored for 14 days post-injury.
Clinical evaluation: Serial slit-lamp microscopy, stereomicroscopy, and tonometry
Anesthetized rabbits were clinically evaluated via slit-lamp biomicroscopy, and a Fante’s scoring system was used to grade the degree of the corneal haze present. The grades assigned were as follows: grade 0, totally clear, no haze seen by any method of slit-lamp examination; grade 0.5, trace corneal haze, seen only by indirect broad tangential illumination; grade 1, haze of minimal density, seen with difficulty by direct and diffuse illumination; grade 2, mild haze, easily visible with direct focal slit illumination; grade 3, moderately dense opacity that partially obscures the iris details; and grade 4, severely dense opacity that completely obscures the details of intraocular structures. 45
Morphometric quantification of CNV was performed from slit-lamp images by masked graders (M.K.F., L.M.M., S.G.) via Adobe Photoshop CS2 (Adobe Systems, San Jose, CA, USA) and NIH ImageJ 1.38X (NIH, Bethesda, MD, USA). The corneal region was highlighted at the limbus, vascularized areas were isolated by color thresholding with manual correction, and measurements were exported from ImageJ.
CNV was quantified using a composite scoring system proportional to both the vascularized area and centripetal extension. Scores were normalized to a 0–4 scale, as described in the published literature. 46 A score of 0 indicated no detectable vessels. A score of 1 corresponded to new vessels restricted to the peripheral cornea and extending no more than 1 mm from the limbus. A score of 2 denoted vessels extending 1–2 mm from the limbus, but not yet reaching the central cornea. A score of 3 reflected more extensive vascularization with vessels extending beyond 2 mm and approaching the central cornea, although not involving the visual axis. A score of 4 indicated pan-corneal vascularization with vessel ingrowth reaching the visual axis. This rubric was applied by masked graders (M.K.F., L.M.M., S.G.) to ensure the consistent and unbiased quantification of CNV.
Corneal fibrosis and CNV were assessed using a Leica MZ16 FA stereomicroscope (Leica Microsystems, Wetzlar, Germany) equipped with a SpotCamRT KE digital camera system (Diagnostic Instruments, Inc.). Imaging was performed under 10× magnification with consistent illumination and exposure settings across all groups. Clinical evaluations were conducted at standardized time points on days 0 (immediately after injury), 3, 7, and 14 post-injury across all experimental groups to assess corneal fibrosis and CNV. All corneas were digitally documented at each time point. Intraocular pressure (IOP) for each eye was obtained at the same time points with an applanation tonometer (Tono-Pen AVIA, Reichert Technologies, Depew, NY, USA). Rabbits were gently restrained without sedation. Three consecutive readings were taken from each eye, and the average value was recorded for analysis.
Euthanasia and tissue collection
Euthanasia of the rabbits was performed via intravenous administration of pentobarbital (250 mg/kg), and the animals were placed under general anesthesia (ketamine + xylazine). Death was confirmed through cardiac auscultation, and a secondary physical means of euthanasia, bilateral pneumothrorax, was employed to ensure death. These methods of euthanasia are consistent with the standards of the American Veterinary Medical Association Guidelines for the Euthanasia of Animals: 2020 Edition. 47
Animals were euthanized at 14 days post-alkali injury for tissue collection. This time point was chosen to capture the subacute wound-healing phase when corneal fibrosis and CNV are established and quantifiable, consistent with previous reports of alkali burn-induced corneal injury models.48,49
The corneas were removed with forceps and sharp Westcott scissors, embedded in liquid optimal cutting temperature compound in a 24 × 24 × 5-mm mold, and snap frozen. Frozen tissue blocks were maintained at −80°C for future use. Tissue sections were cut into 7-μm-thick sections with a cryostat, placed on 25 × 75 × 1-mm microscope slides, and stored at −80°C until staining.
Immunofluorescence and TUNEL apoptosis assay
Corneal sections (7 μm) were prepared with a cryostat and were used for the immunofluorescence study. For α-SMA staining, a mouse monoclonal antibody (1:200 dilution, M0851; Dako, Carpinteria, CA, USA), for filamentous actin (F-actin) staining, Alexa 594-conjugated phallotoxin (A12381; Invitrogen, Molecular Probes, Life Technologies Corp., Eugene, OR, USA), and for endoglin (1:100 dilution, SC 18838; SantaCruz Biotechnology, Inc., Dallas, TX, USA). In brief, the cryosection slides were placed at room temperature for 5 min, washed twice with 1× PBS, followed by blocking with 2% serum (30 min at room temperature) and then with respective primary antibodies (90 min at room temperature). After primary antibody staining, the sections were exposed to Alexa Fluor-tagged IgG secondary antibody (1:500 dilution, Invitrogen Molecular Probes, Life Technologies Corp.) for 1 h in the dark, followed by subsequent three times washing with 1× PBS. Tissues were mounted with Vectashield 520 containing DAPI (Vector Laboratories) for the visualization of nuclei. Irrelevant isotype-matched primary antibody, secondary antibody alone, and tissue sections from naïve eyes were used as negative controls. Stained cells were visualized under a Leica fluorescence microscope (Leica) and photographed with a digital camera (SpotCam RT KE, Diagnostic Instruments, Inc.). For quantification and statistical analyses, six corneas were used to quantify α-SMA+ and F-actin+ cells in the tissues from each group. The α-SMA+ and F-actin+ cells in six randomly selected, nonoverlapping, full-thickness central corneal columns extending from the anterior stromal surface to the posterior stromal surface were counted at 400× magnification of the microscope field.
A TUNEL assay was performed on acetone-fixed corneal sections for apoptotic cells staining according to the manufacturer’s instructions (S7165, ApopTag Red In Situ Apoptosis Detection Kit, Millipore). In brief, the corneal tissue sections were permeabilized with ethanol:acetic acid (2:1 ratio; at −20°C) and treated with TdT enzyme (37°C for 1 h), stop wash buffer (room temperature for 10 min), and anti-digoxigenin rhodamine conjugate (room temperature for 30 min), with assay kit reagents. Tissues were mounted with Vectashield 520 containing DAPI (Vector Laboratories) for the visualization of nuclei and photographed with a digital camera (SpotCam RT KE, Diagnostic Instruments, Inc.).
Statistical analysis
The results are expressed as means ± standard errors. For clinical and molecular data statistical assessment, one-way analysis of variance (one-way ANOVA), followed by post hoc Bonferroni or Dunnett post hoc multiple comparison test, was used to compare the effect of HA1077 in naïve and alkali injury groups. A P value of <0.05 was considered significant.
Results
HA1077 treatment is well-tolerated by human corneal fibroblasts
The tolerability of the HA1077 concentration to corneal stromal cells was evaluated via an in vitro assay. Figure 1 shows the concentration-dependent effects of HA1077 on the cellular viability of hCSF. No significant loss of cellular viability was observed at concentrations up to 3 nM HA1077 (P = 0.41 at 3 nM), whereas higher concentrations (4 and 5 nM) showed significantly reduced viability compared with control (P < 0.05 or P < 0.01). To further assess the cytotoxicity of HA1077 to hCSF, we used phase-contrast microscopy. Treatment with 3 nM HA1077 did not alter hCSF morphology at 48 h (Fig. 2A,B). In contrast, cultures treated with ≥4 nM HA1077 presented distinct morphological changes, including reduced density and loss of typical spindle-shaped appearance at the tested time points (Supplementary Fig. S1). The TUNEL apoptosis assay confirmed that 3 nM HA1077 was non-toxic to hCSFs, as there was no detectable difference in the number of TUNEL-positive cells between HA1077-treated and untreated control hCSFs (Fig. 2C,D).
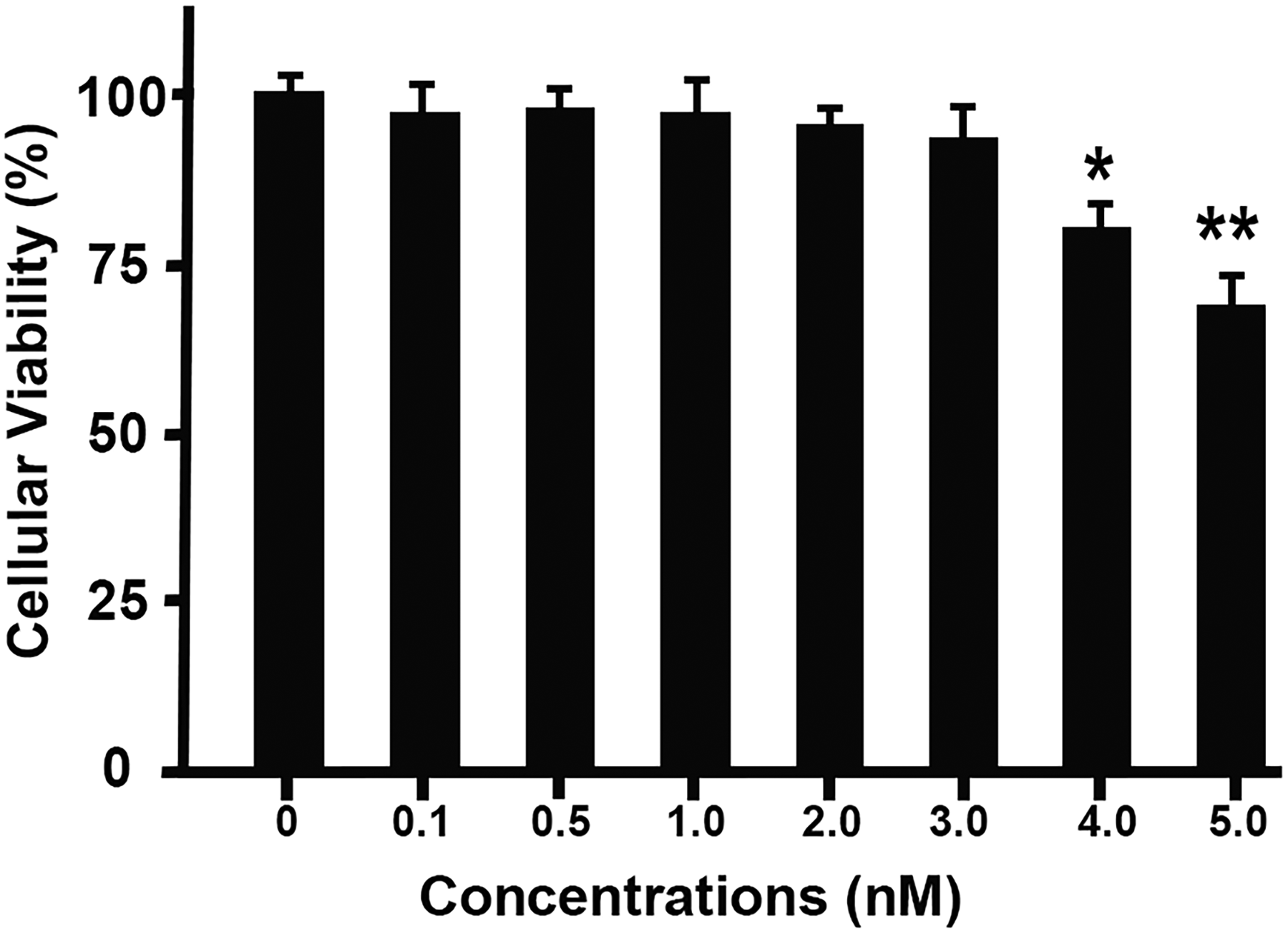
Concentration-dependent effect of HA1077 on human corneal fibroblast viability. Primary human corneal fibroblasts were treated for 48 h with HA1077 at concentrations ranging from 0 to 5 nM, and cell viability was assessed via a trypan blue assay. Viability was unaffected at concentrations ≤3 nM, whereas significant reductions were observed at 4 nM (*P < 0.05) and 5 nM (**P < 0.01) compared with untreated controls. The data represent the means ± Standard Error of the Means (SEMs) from three independent experiments.
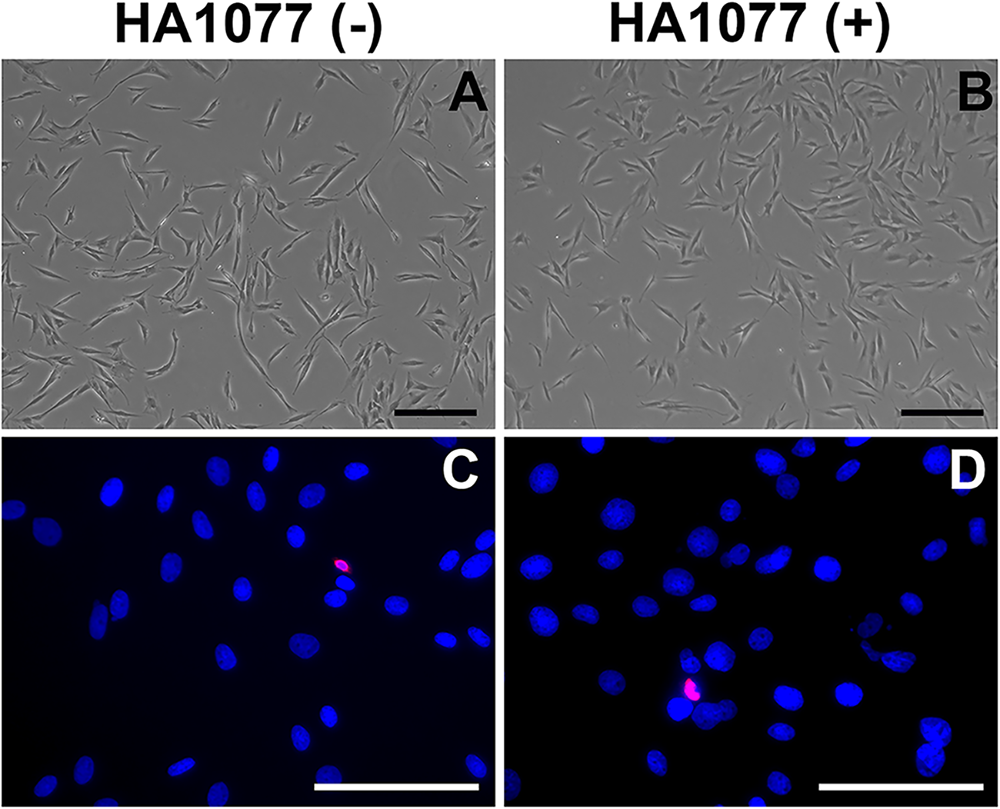
Effect of HA1077 (3 nM) on human corneal fibroblast morphology and apoptosis in vitro. Phase-contrast microscopy revealed no change in hCSF morphology after 48 h of HA1077 treatment
HA1077 treatment attenuates corneal fibrosis and CNV after alkali injury in rabbit corneas
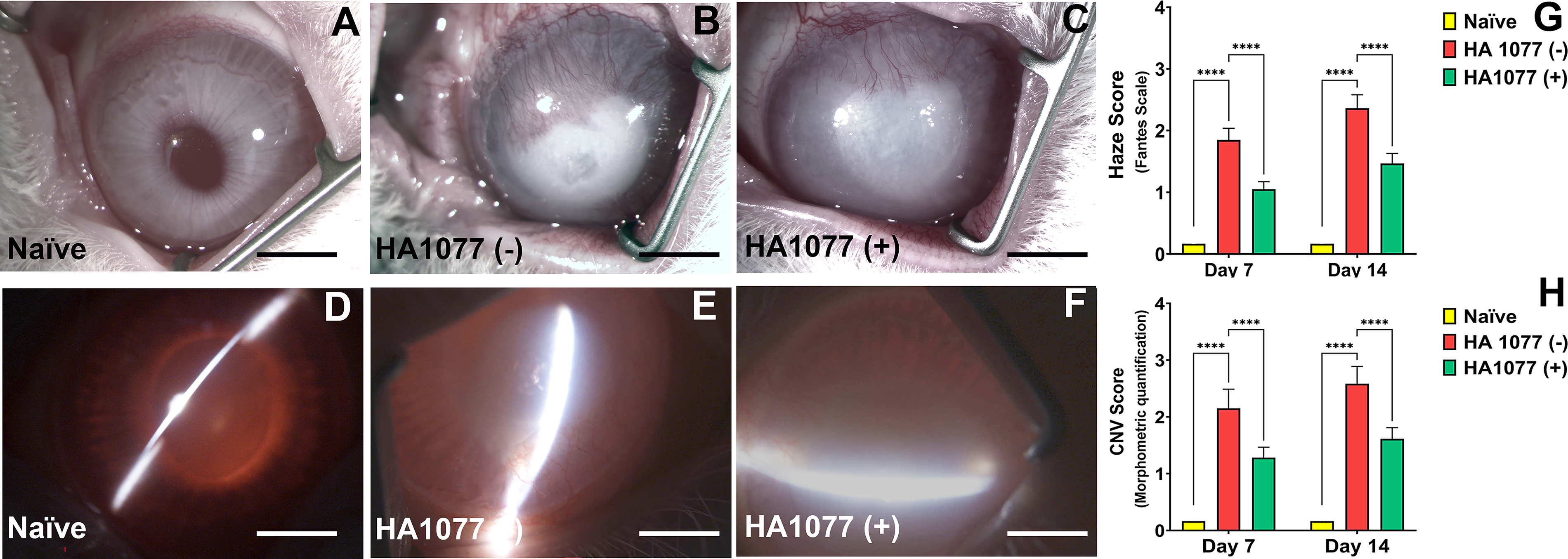
Naïve control corneas (no alkali injury, no treatment) exhibited normal transparency and morphology (Fig. 3A,D). In contrast, BSS-treated alkali-injured corneas developed marked haze and dense neovascularization (Fig. 3B,E). Compared with BSS-treated eyes, HA1077-treated corneas presented visibly reduced fibrotic and angiogenic responses on day 7 (Supplementary Fig. S2) and day 14 (Fig. 3C,F). Quantitative analysis revealed that HA1077 significantly reduced fibrosis scores at both days 7 and 14 (Fante’s score: day 7, 1.0 ± 0.2 vs 2.0 ± 0.3; day 14, 1.4 ± 0.2 vs 2.6 ± 0.3; P < 0.0001) (Fig. 3G). Similarly, CNV scores were significantly lower in HA1077-treated corneas than in BSS-treated controls at both time points (morphometric quantification score: day 7, 1.2 ± 0.2 vs 2.3 ± 0.3; day 14, 1.5 ± 0.2 vs 2.7 ± 0.3; P < 0.0001) (Fig. 3H).
Effect of HA1077 treatment on corneal haze (fibrosis) and neovascularization after alkali injury.
Periodic clinical eye examinations confirmed that the repeated topical application of HA1077 did not cause adverse effects on corneal anatomy or physiology. Across all observation points (days 1, 3, 7, and 14), there was no evidence of worsening ocular inflammation, conjunctival hyperemia, corneal or conjunctival edema, ocular discharge, or infection attributable to HA1077 treatment. The findings demonstrated that topical HA1077 significantly attenuated fibrosis and CNV after alkali injury in the rabbit cornea without apparent ocular toxicity.
HA1077 treatment does not alter normal IOP following corneal alkali injury
IOP was monitored in naïve, BSS-treated, and HA1077-treated rabbit eyes at 0, 3, 7, and 14 days post-alkali injury (Supplementary Fig. S3). Across all the groups, IOP remained within the normal physiological range for the rabbits, and no noticeable differences were detected.
Effect of HA1077 on corneal tissue architecture post-alkali injury
Histological evaluation was performed to assess cell/tissue organization in rabbit corneas at 14 days in all groups (Fig. 4). H&E-stained corneal sections from BSS-treated alkali-injured eyes showed more inflammatory cells and damaged epithelium compared with HA1077-treated corneas (Fig. 4B vs C). Naïve corneas had normal epithelium and stromal tissue organization (Fig. 4A). These data indicated that HA1077 treatment limits corneal damage post-alkali injury.
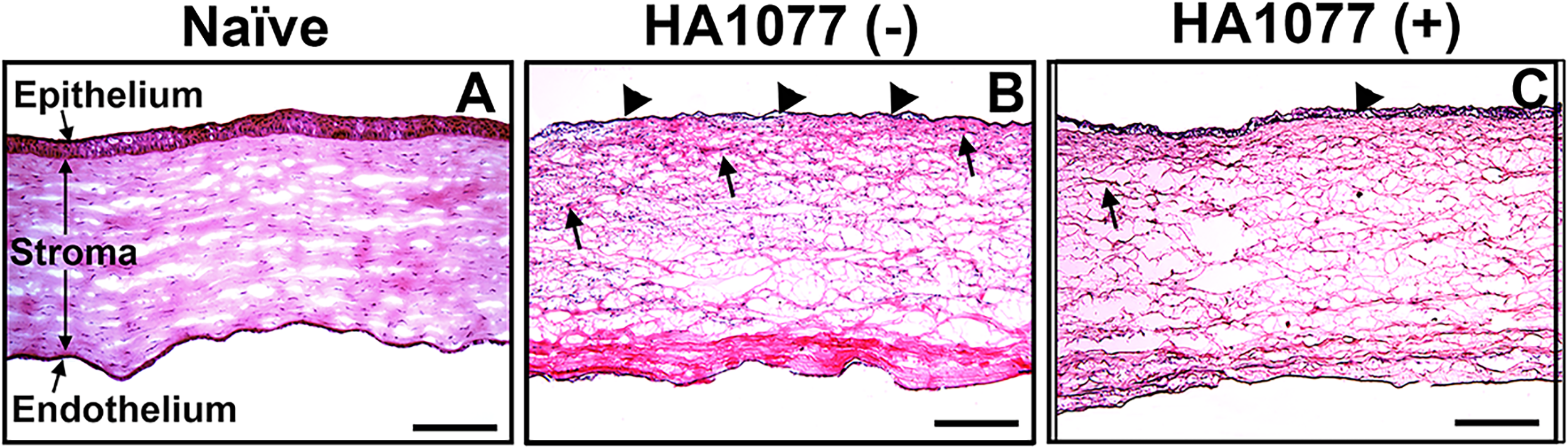
H&E staining of naïve
HA1077 treatment markedly attenuates myofibroblast accumulation and vessel formation following corneal alkali injury
In BSS-treated alkali-injured corneas, abundant α-SMA+ cells (green) and F-actin+ cells (red) were present throughout the anterior stroma beneath the epithelium (Fig. 5B,E), with a dense myofibroblast presence. In contrast, HA1077-treated alkali-injured corneas showed markedly reduced α-SMA+ and F-actin+ cells (Fig. 5C,F). Naïve corneas had no α-SMA- or F-actin-positive staining (Fig. 5A,D).
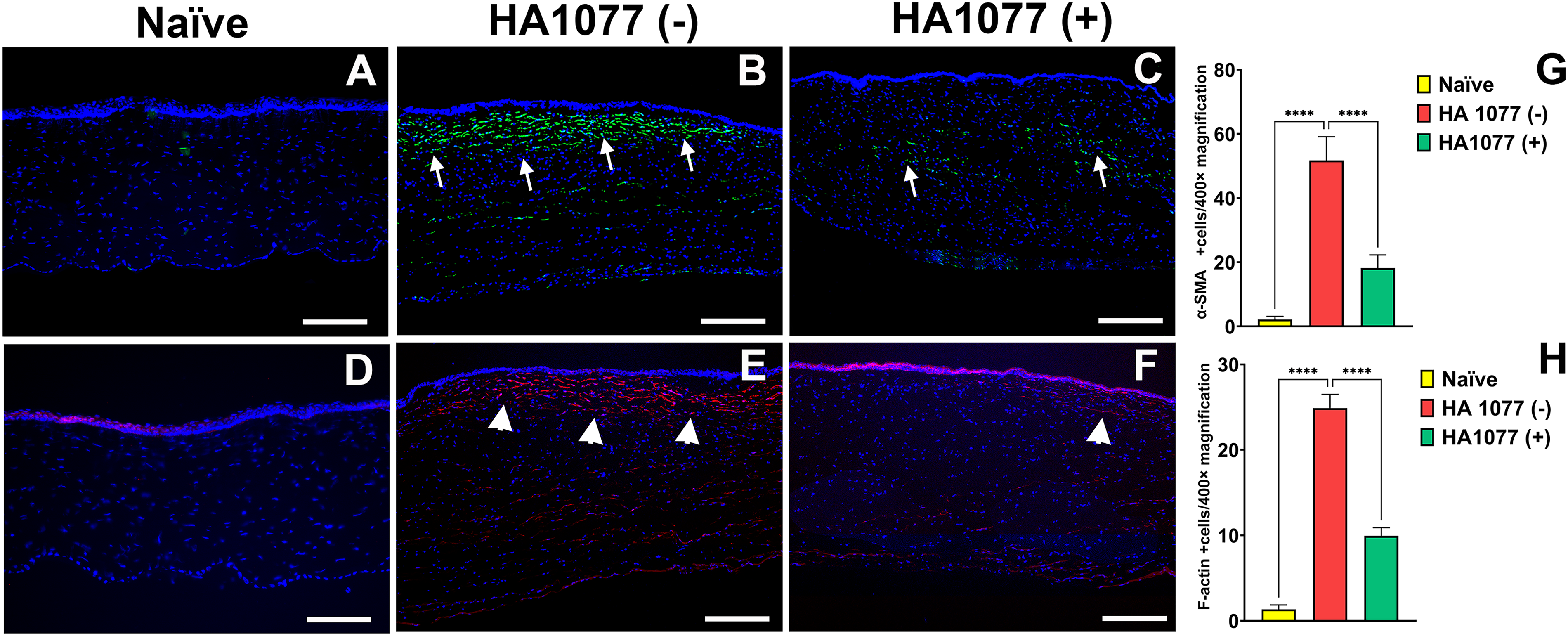
Immunofluorescence detection of α-SMA and F-actin in rabbit corneas 14 days after alkali injury.
The extent of CNV in rabbit eyes was assessed by immunofluorescence staining for endoglin, a marker of vascular endothelial cells. BSS-treated alkali-injured corneas presented abundant endoglin-positive endothelial cells (red) throughout the stroma (Fig. 6B), while HA1077-treated corneas had markedly reduced endoglin-positive cells in the stroma (Fig. 6C). Naïve corneas had no endoglin-positive cells (Fig. 6A). This analysis indicated that topical HA1077 suppresses CNV.
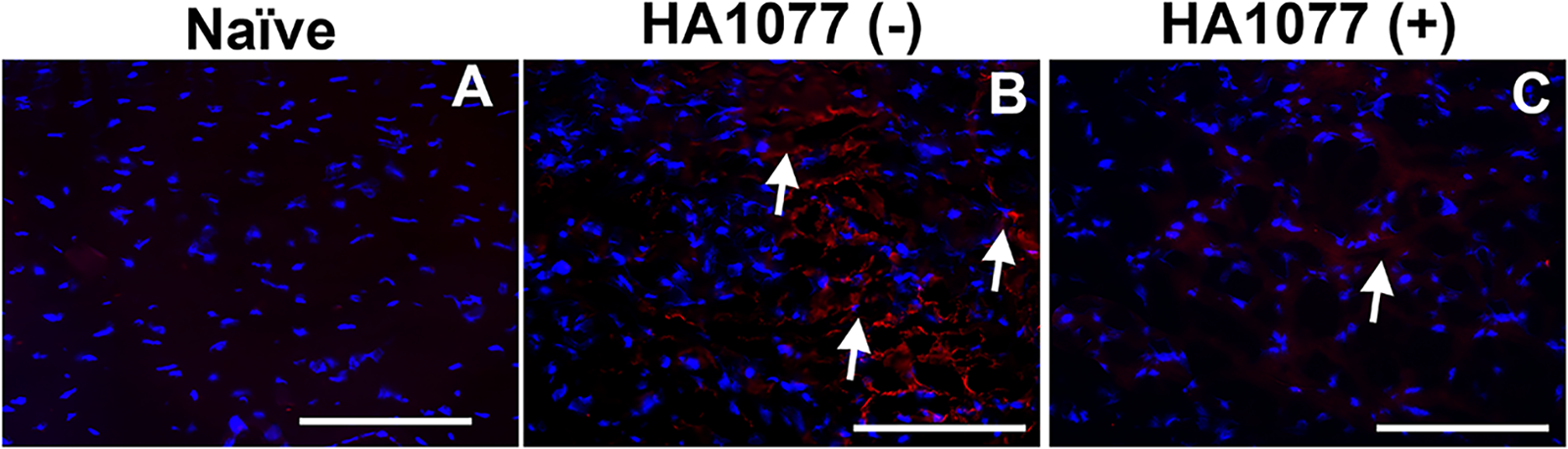
Immunofluorescence detection of endoglin in rabbit corneas 14 days after alkali injury. Representative images of naïve
Effect of topical HA1077 treatment on corneal epithelial and stromal apoptosis in vivo
The TUNEL assay was used to evaluate the effects of topical HA1077 on cornea (Fig. 7). Both HA1077- and BSS-treated alkali-injured corneas presented similar numbers of TUNEL-positive cells in the stroma, indicating that HA1077 is safe to corneas. Naïve corneas displayed minimal/no TUNEL staining in the stroma. These findings demonstrated that HA1077 is safe to corneal epithelial and stromal cells in vivo.
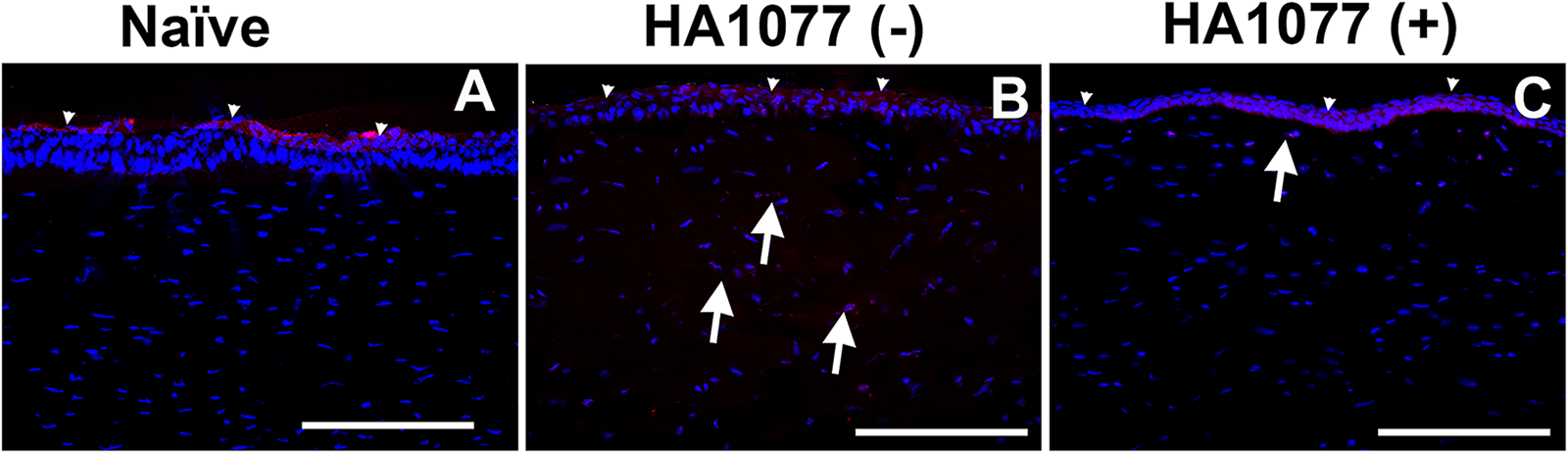
In vivo effects of HA1077 treatment on corneal epithelial and stromal apoptosis after alkali injury. TUNEL assays were performed 14 days post-injury in naïve
Discussion
Corneal fibrosis and CNV are major vision-threatening sequelae of chemical injury. In this rabbit model, brief topical treatment with the ROCK inhibitor HA1077 (fasudil; 3 nM, twice daily for 3 days) significantly reduced both stromal haze and CNV at days 7 and 14 after chemical injury, as per subjective clinical and histological evaluations (Figs. 3–6, Supplementary Fig. S2). Safety assessments indicated that topical 3 nM HA1077 did not cause epithelial or stromal cell damage or change IOP (Supplementary Fig. S3), or cytotoxicity to hCSF or rabbit corneas (Figs. 1, 2, and 7).
Rho kinase regulates cytoskeletal dynamics, myofibroblast activation, and apoptosis.50,51 Prior studies in nonocular systems have shown that ROCK signaling controls α-SMA upregulation and actin stress fiber formation, and that ROCK inhibition reduces TGF-β1-induced myofibroblast differentiation and extracellular matrix deposition.52–54 In line with these observations, HA1077 treatment in the current study was associated with a reduction in α-SMA- and F-actin-positive cells after injury, indicating the suppression of myofibroblast accumulation, a principal driver of corneal light scatter and stromal scarring.
Angiogenesis in the injured cornea is likewise coupled to RhoA/ROCK activity downstream of VEGF. Pharmacologic ROCK inhibition has been shown to blunt endothelial migration, tube formation, and survival in vitro and in vivo.55–57 Our endoglin staining aligns with these mechanisms; BSS-treated corneas displayed dense stromal endoglin positivity, whereas HA1077 markedly reduced signals across the stroma, which reflects the lower morphometric CNV scores.
Inflammation amplifies both fibrosis and neovascularization.58,59 The reduction in stromal leukocyte influx with HA1077 suggests that ROCK inhibition may also temper injury-evoked inflammatory recruitment and/or preserve tissue architecture, thereby indirectly limiting profibrotic and proangiogenic signaling. These findings support a mechanistic framework in which HA1077 attenuates both fibrosis and CNV after ocular injury by targeting RhoA/ROCK signaling. Ocular trauma activates keratocytes and fibroblasts and initiates their differentiation to myofibroblast via TGF-β/Smad signaling and angiogenesis via VEGF signaling, both of which require RhoA/ROCK activation.56,60 By inhibiting ROCK, HA1077 interrupts these two signaling cascades, thereby reducing myofibroblast formation and pathological vascular ingrowth. This dual antifibrotic and antiangiogenic activity addresses two major pathological drivers of vision loss, which makes ROCK inhibition a promising therapeutic approach for severe corneal wounds.
From a translational standpoint, ROCK inhibition has attributes that make it attractive as a frontline or adjunct therapy. In minor injuries (e.g., superficial abrasions or elective surface procedures), short-course topical HA1077 could help prevent scar formation and angiogenesis, with a favorable safety profile. In moderate-to-severe injuries, HA1077 is well-positioned for combination therapy, complementing interventions that modulate TGF-β signaling at multiple levels: extracellular (e.g., decorin), intracellular/transcriptional (e.g., Bone Morphogenetic Protein 7, Soluble Transforming Growth Factor Beta Receptor II), and epigenetic (e.g., Histone Deacetylaseinhibitors such as Trichostatin A or Suberoylanilide Hydroxamic Acid).61–64 Compared with single-agent approaches, such multimodal strategies are likely to provide deeper and more sustainable resolution.
Although the present study focused on corneal fibrosis and CNV, the effect of HA1077 on epithelial wound closure was not systematically assessed. This represents a limitation of the study, and future work incorporating fluorescein eye staining and in vivo confocal corneal imaging will be needed to determine if HA1077 influences corneal epithelial healing. Another limitation of the study includes one HA1077 dose (3 nM) and two time points (days 7 and 14). Additional in vivo studies are warranted with multiple doses of HA1077 and longer time points. Longer-term studies will be necessary to fully characterize the time course of corneal fibrosis and to assess the therapeutic potential of HA1077. Future studies incorporating topical steroids as a benchmark will be important to contextualize the therapeutic potential of ROCK inhibition relative to the current clinical practice. This study presents the proof-of-concept for HA1077 that the topical ROCK inhibitor HA1077 is a viable option for the clinical management of corneal fibrosis and CNV resulting from corneal insult. Further in vitro and in vivo investigations with ROCK inhibitors are warranted.
Authors’ Contributions
R.R.M.: Conceptualization. M.K.F., S.G., P.R.S., and L.M.M.: Data curation. M.K.F., S.G., and R.K.: Formal analysis. R.R.M.: Funding acquisitions. M.K.F., S.G., P.R.S., and L.M.M.: Investigations. R.R.M.: Supervision. S.G., P.R.S., and J.L.: Visualization. M.K.F., S.G., and R.K.: Writing—original draft. R.K., S.G., and R.R.M.: Writing—review and editing.
The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the NEI/NIH 1R01EY030774 and the Merit 1I01BX000357 and RCS IK6BX005646 awards from the NIH, U.S. Department of Veterans Affairs, Washington DC, USA, and Ruth M. Kraeuchi Endowed Chair Ophthalmology Fund, University of Missouri, Columbia, Missouri, USA. Thanks are also due to the Arora Family Foundation, Cleveland, Ohio, USA, for a gift to the cornea research program.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.