
Abstract
Aging has long been implicated in the onset and progression of major retinal diseases, including age-related macular degeneration (AMD), diabetic retinopathy (DR), and retinal vein occlusion (RVO). Glaucoma is likewise increasingly recognized as an age-related disorder. Across these conditions, converging patterns of neurodegeneration and microvascular injury contribute to age-associated ocular decline. Structural and neuronal degeneration of the retina, including loss of retinal ganglion cell axons, along with impaired microvascular circulation and chronic inflammation, contribute to the pathogenesis of glaucoma, AMD, DR, and RVO. Geroprotectors, a class of longevity-promoting pharmacologic agents investigated for systemic benefits in cardiovascular and neurological aging, have therefore drawn growing ophthalmic interest for their potential relevance to ocular health and the management of age-associated eye diseases. These agents are now frequently encountered as concomitant medications in ophthalmic practice, yet their ocular effects remain incompletely characterized, variably reported, and in some cases controversial. Glucagon-like peptide-1 (GLP-1) receptor agonists, widely used for glycemic control and increasingly for weight management, have been associated with reduced risk of age-related glaucoma but also with unconfirmed reports of severe nonarteritic anterior ischemic optic neuropathy. Similar uncertainties surround other geroprotective, metabolic, and weight-modifying therapies, creating challenges for clinicians attempting to incorporate evolving pharmacologic evidence without compromising patient safety. This review synthesizes reported therapeutic and adverse ocular outcomes across geroprotective agents to support clinical awareness, identify knowledge gaps, and guide future investigation. The agents reviewed include GLP-1 receptor agonists, metformin, sodium-glucose cotransporter-2 inhibitors, statins, cannabinoids, calcium channel blockers, spermidine, taurine, nicotinamide adenine dinucleotide precursors, rapamycin, and mifepristone.
Keywords
Introduction
Retinal degenerative diseases, including glaucoma, age-related macular degeneration (AMD), diabetic retinopathy (DR), and retinal vein occlusion (RVO), are major causes of progressive and irreversible vision loss worldwide.1,2 The prevalence of glaucoma and AMD rises substantially after age 60, reflecting the influence of aging biology and the growing burden of metabolic disease.1,3 Glaucoma comprises a spectrum of disorders characterized by optic nerve damage and progressive retinal ganglion cell (RGC) degeneration. Although elevated intraocular pressure (IOP) remains a central pathogenic factor, multiple age-related mechanisms are increasingly implicated in disease onset and progression. These mechanisms impair trabecular meshwork function, disrupt retinal perfusion, and promote RGC loss. 4
Similar neurovascular and metabolic degenerative processes have long been documented in other age-associated retinal diseases. AMD is a chronic degenerative disorder of the macula marked by progressive dysfunction of photoreceptors and the retinal pigment epithelium, leading to central vision loss. DR, although driven primarily by long-standing diabetes, worsens with aging due to cumulative microvascular injury, impaired vascular repair capacity, and increased susceptibility of the aging retina to metabolic stress. RVO is an occlusive vasculopathy whose incidence rises with age, reflecting age-related vascular stiffening, endothelial dysfunction, and heightened vulnerability to thrombotic events. 5 Across these conditions, well-established age-related biological processes, including microvascular ischemia, oxidative stress, mitochondrial dysfunction, and chronic neuroinflammation, contribute to disease onset and/or progression, underscoring the shared susceptibility of ocular tissues to systemic aging.6,7
The increasingly recognized association between aging-related neurovascular degeneration and ocular decline has two major implications. First, despite advances in medical, laser, and surgical therapies, the impact of glaucoma, AMD, DR, and RVO is expected to intensify as the global population continues to age,1,5 underscoring the need for novel adjunctive neuroprotective strategies. Second, an emerging class of pharmacologic agents—referred to as geroprotective agents—that target fundamental aging mechanisms, including cellular senescence, metabolic dysregulation, and impaired stress-response signaling implicated in susceptibility to glaucomatous and retinal neurovascular degeneration, have gained interest for their potential relevance to the management of age-related ocular diseases. Academic investigations have explored their roles in mitigating ocular aging through neurovascular protection, immune modulation, and reduction of allostatic load.6–10
Geroprotective agents, however, are not formally defined by the scientific community and are not recognized as an official therapeutic class by regulatory bodies. The term is used informally in academic research to describe compounds investigated for their potential to slow biological aging, extend lifespan, or delay age-associated diseases. Although hundreds of substances have been cataloged, the most prominent candidates—widely recognized in academic research—are medications already approved for other chronic conditions, such as type 2 diabetes mellitus (T2DM), dyslipidemia, heart failure, organ transplantation, or weight management. Agents including metformin, glucagon-like peptide-1 receptor agonists (GLP-1 RAs), and sodium-glucose cotransporter-2 inhibitors (SGLT-2 inhibitors) exert systemic protective effects that overlap with biological pathways implicated in glaucomatous optic neuropathy and retinal neurovascular degeneration observed in AMD, DR, and RVO.6–10 Their ophthalmic implications, however, remain incompletely defined, with evidence encompassing both potential protective effects10–17 and neutral18–23 or adverse association.24–30 The complexity of modern polypharmacy further complicates clinical decision-making. As weight-control and longevity-promoting drugs such as GLP-1 gain rapid adoption, ophthalmologists may increasingly encounter patients using agents with uncertain ocular safety profiles.
This review synthesizes current evidence on the therapeutic and adverse ocular effects of geroprotective agents, including GLP-1 receptor agonists, metformin, SGLT-2 inhibitors, statins, cannabinoids, calcium channel blockers (CCBs), spermidine, taurine, nicotinamide adenine dinucleotide (NAD+) precursors, rapamycin, and mifepristone, to inform future research and clinical practice in age-related ocular diseases.
Relevant literature was identified through comprehensive searches of MEDLINE (PubMed), Scopus, and the Cochrane Library, supplemented by targeted searches in Google Scholar to capture emerging or highly cited studies. Peer-reviewed studies were selected based on their relevance to aging biology, antiaging pharmacology, geroscience, and age-related ocular disorders.
Overview of Evidence
Geroprotective agents and their systemic roles
Geroprotective compounds investigated for systemic cytoprotection and longevity are summarized in Table 1. With the exception of spermidine, taurine, and NAD+, classified by the US Food and Drug Administration (FDA) as Generally Recognized as Safe, the remaining agents are active ingredients in at least one FDA-approved indication, most commonly T2DM or weight management. 31 No medications are currently approved by the FDA for lifespan-extending indications. Across these agents, underlying protection against cardiovascular, renal, and neurodegenerative decline is linked to cytoprotective pathways, including activation of AMP-activated protein kinase (AMPK), inhibition of mechanistic target of rapamycin (mTOR), enhancement of DNA repair, and attenuation of oxidative stress and inflammation.10,32–34
Geroprotective Agents and Their Systemic Roles
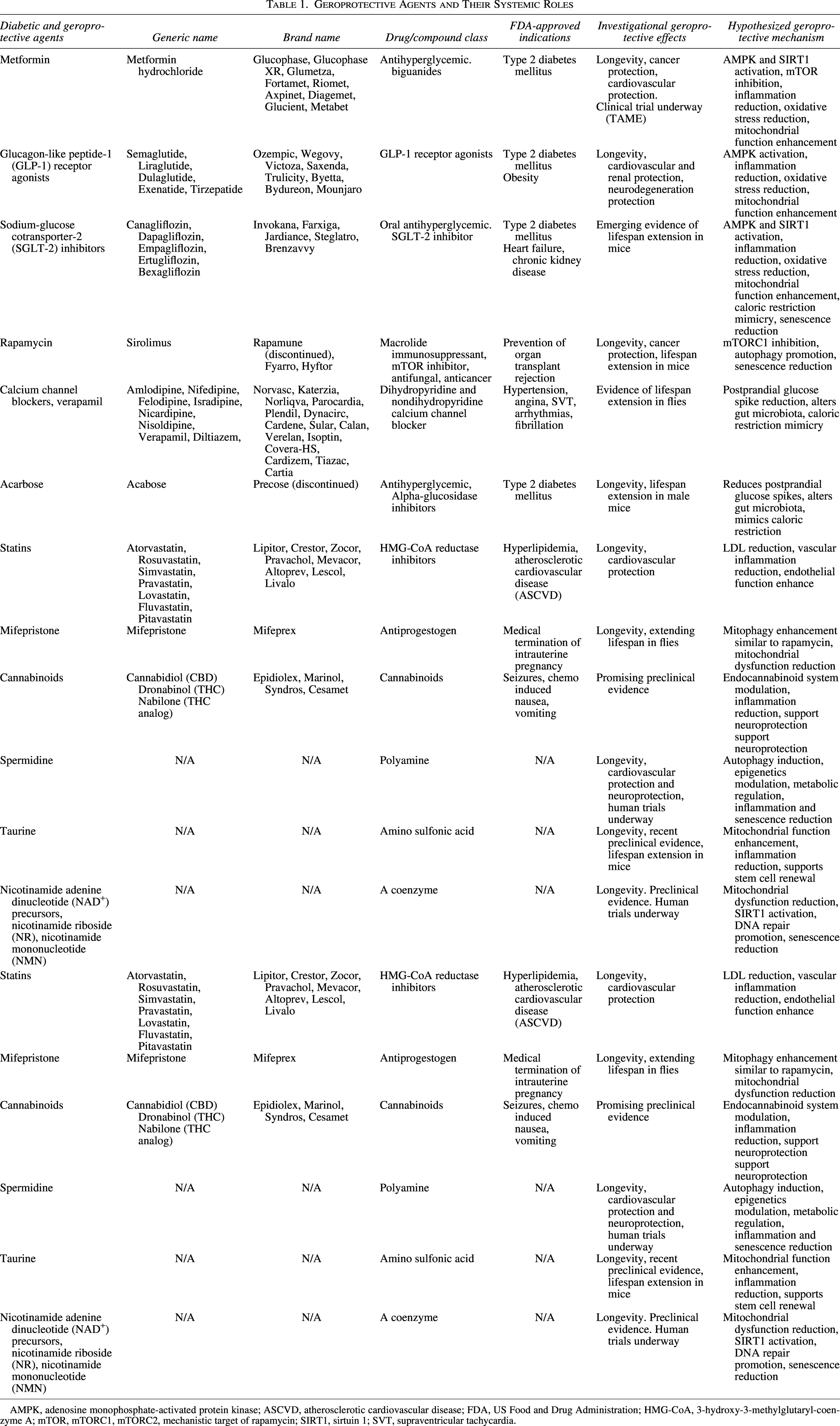
AMPK, adenosine monophosphate-activated protein kinase; ASCVD, atherosclerotic cardiovascular disease; FDA, US Food and Drug Administration; HMG-CoA, 3-hydroxy-3-methylglutaryl-coenzyme A; mTOR, mTORC1, mTORC2, mechanistic target of rapamycin; SIRT1, sirtuin 1; SVT, supraventricular tachycardia.
Monotherapy and combination regimens using geroprotective agents
Table 2 outlines antihyperglycemic and weight-management therapies commonly encountered as concomitant medications in ophthalmic practice. Metformin hydrochloride remains the foundational first-line therapy for T2DM, whereas second-line agents such as GLP-1 receptor agonists, SGLT-2 inhibitors, and dipeptidyl peptidase-4 (DPP-4) inhibitors are added when glycemic control is inadequate.31,34 Notably, in 2022, both GLP-1 RAs and SGLT-2i were incorporated into first-line recommendations for patients with cardiorenal comorbidities. 31 Several fixed-dose combinations incorporating metformin, GLP-1 RA, or SGLT-2i are commonly used, tailored to patient comorbidities and therapeutic goals.34,35
Common Monotherapy and Combination Regimens Involving Geroprotective Agents
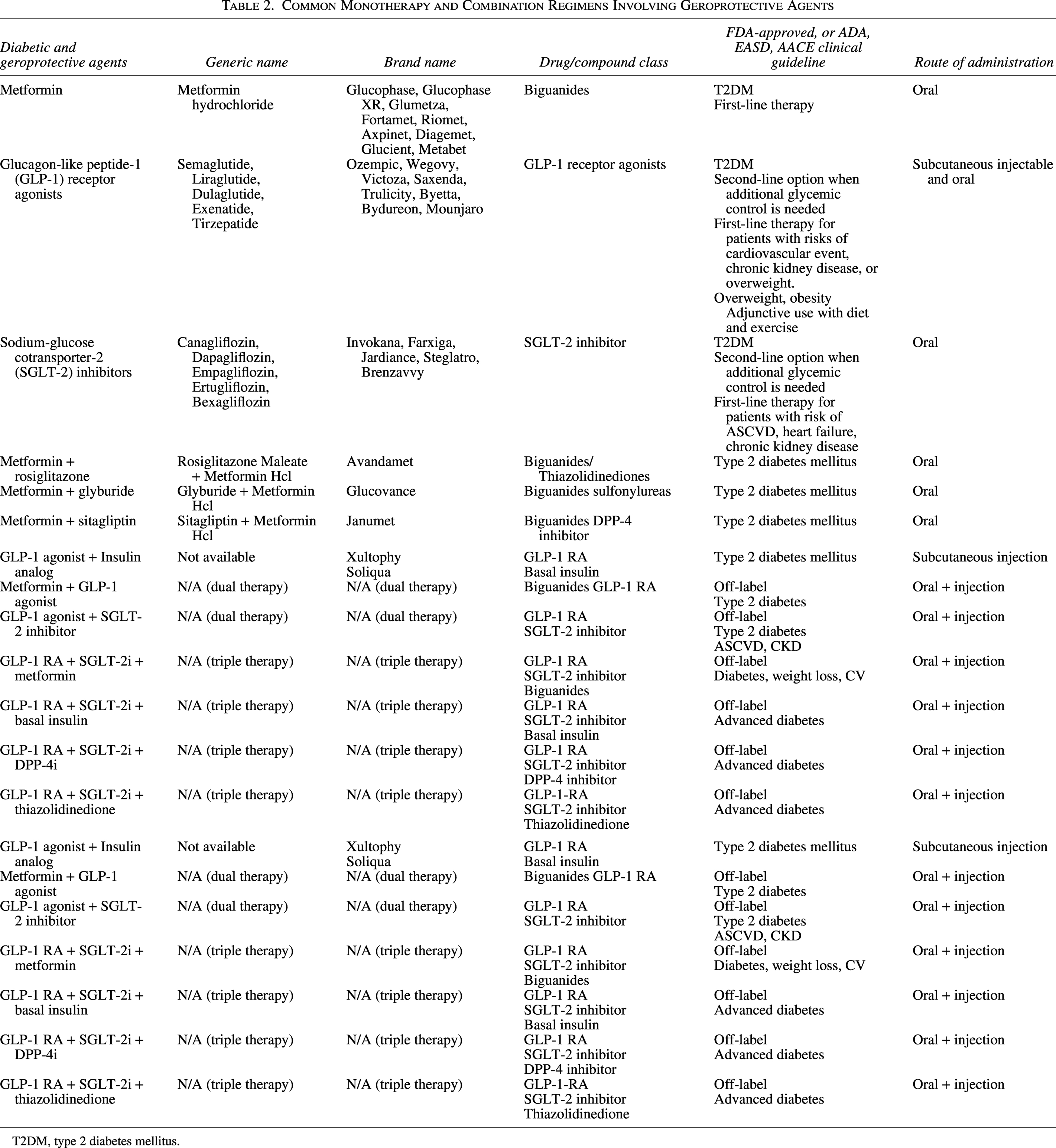
T2DM, type 2 diabetes mellitus.
Ocular associations reported with geroprotective agents
Table 3 synthesizes reported therapeutic and adverse ocular associations across geroprotective agents. Most available evidence derives from retrospective analyses, small observational cohorts, cross-sectional studies, or post hoc evaluations. Few longitudinal, multicenter randomized trials with ophthalmic endpoints have been completed, and available evidence remains limited and, at times, conflicting. Some of the most frequently reported associations are summarized in this section, with an agent-specific synthesis presented in the sections that follow.
Reported Ocular Associations of Geroprotective Agents
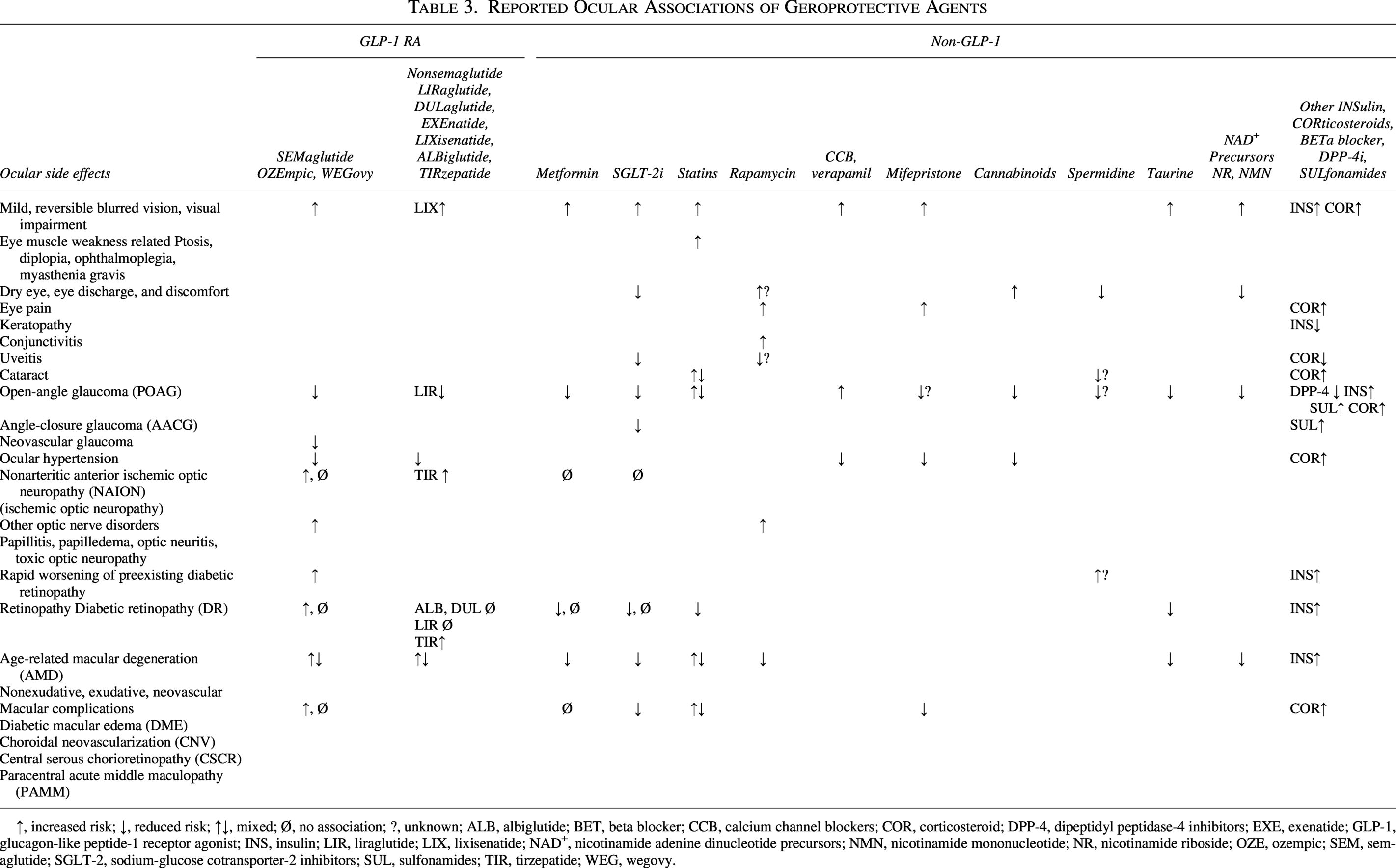
↑, increased risk; ↓, reduced risk; ↑↓, mixed; Ø, no association; ?, unknown; ALB, albiglutide; BET, beta blocker; CCB, calcium channel blockers; COR, corticosteroid; DPP-4, dipeptidyl peptidase-4 inhibitors; EXE, exenatide; GLP-1, glucagon-like peptide-1 receptor agonist; INS, insulin; LIR, liraglutide; LIX, lixisenatide; NAD+, nicotinamide adenine dinucleotide precursors; NMN, nicotinamide mononucleotide; NR, nicotinamide riboside; OZE, ozempic; SEM, semaglutide; SGLT-2, sodium-glucose cotransporter-2 inhibitors; SUL, sulfonamides; TIR, tirzepatide; WEG, wegovy.
Across the literature, several agents, including GLP-1 RAs, metformin, SGLT-2, taurine, NAD+, and cannabinoids, have been associated with reduced risk of open-angle glaucoma (POAG) or lower IOP,11–13,18,36–43 whereas CCBs are linked to potential risk.44,45 SGLT-2i are also associated with reduced risk of ACG, 13 whereas semaglutide with lower risk of neovascular glaucoma in some cohorts. 25 Unconfirmed IOP-lowering effects have been described with GLP-1 receptor antagonists, CCBs, mifepristone, and cannabinoids.42–46 Statins, metformin, SGLT-2i, rapamycin, and NAD+ precursors have been found to be protective for uveitis, DR, RVOs, and nonexudative and exudative AMD disease.14,22,47–50 The evidence implicating statins in glaucoma remains inconclusive.14,15,19,20 Adverse effects, such as nonarteritic anterior ischemic optic neuropathy (NAION), have been controversially linked to GLP-1 RAs,24,26 and isolated reports describe the role of semaglutide in the worsening of chorioretinal diseases, including DR, diabetic macular edema, choroidal neovascularization, central serous chorioretinopathy, and paracentral acute middle maculopathy.25,27–30 No significant ocular harm signals have been reported for metformin or SGLT-2i.
Pharmacotherapeutic Interventions Targeting Longevity and Ocular Health
Contemporary geroscience has identified a network of agents and conserved molecular pathways that regulate aging and influence susceptibility to age-related diseases. Figure 1 illustrates the cytoprotective cascade induced by geroprotective agents, outlining the activated molecular pathways, the resulting biological effects, and the downstream clinical outcomes. 51
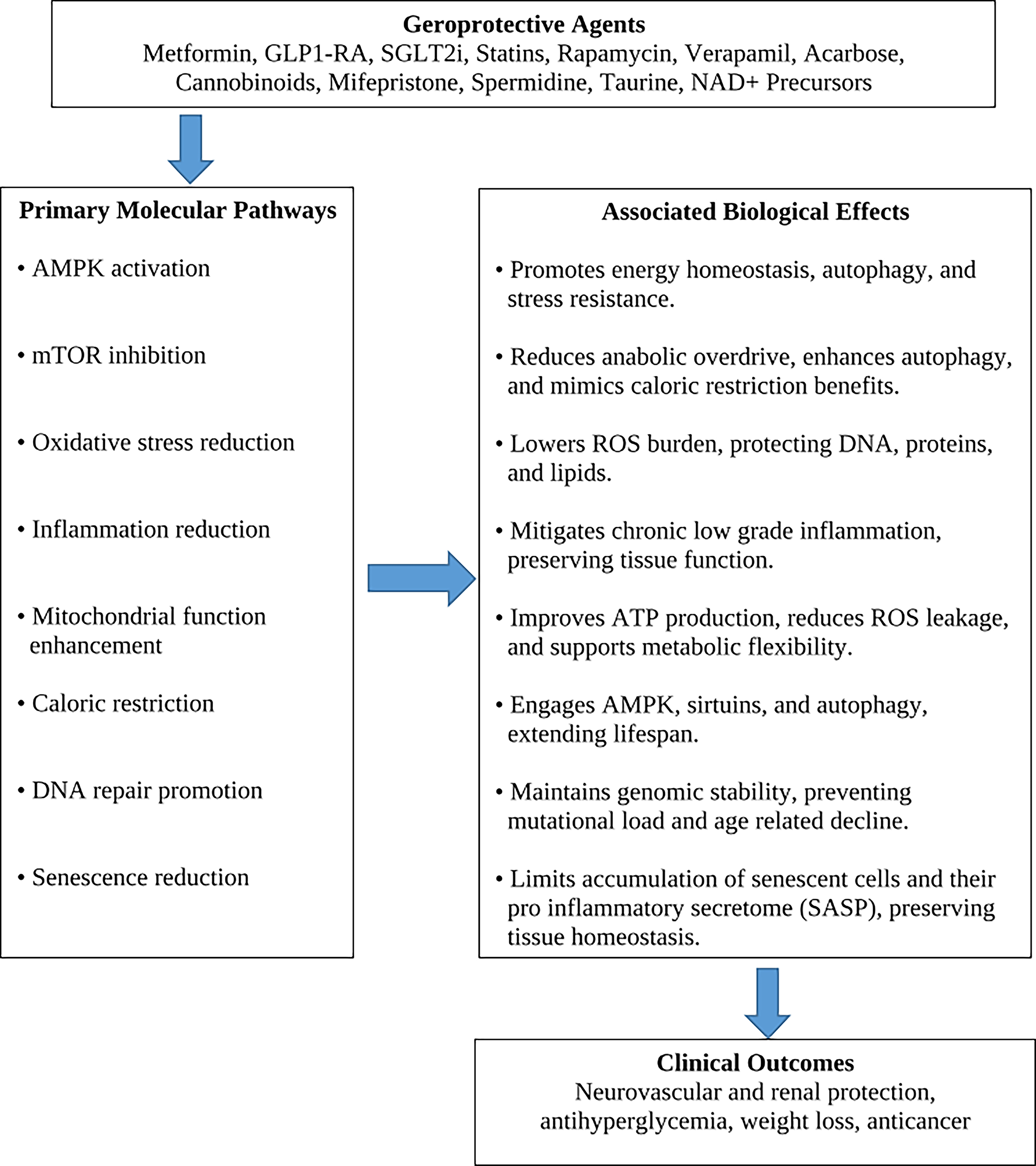
Cascade of geroprotective molecular pathways, biological effects, and clinical outcomes.
Several hallmark mechanisms influence aging. Hyperactivation of mTOR and inflammatory signaling cascades accelerates aging, whereas AMPK and sirtuin-1 (SIRT1)-mediated stress responses and DNA repair enhance cellular resilience.51–53 These mechanistic insights have catalyzed translational pharmacology strategies aimed at modulating aging pathways, delaying the onset of age-related diseases, and enhancing functional longevity. Pharmacologic activation of AMPK and SIRT1 as well as inhibition of mTOR are key actions of GLP-1 RAs, metformin, and SGLT-2i (Table 1).54–56 Robust evidence that GLP-1 RAs and SGLT-2i reduce major adverse cardiovascular events (MACE), heart failure, stroke, and lowering risks of Alzheimer’s and Parkinson’s diseases has supported expanded indications for T2DM with comorbidities.57–60 These tailored and fixed-dose combination therapies are increasingly used, reflecting a shift toward multidisciplinary management of hyperglycemia, cardiovascular disease, and neurodegenerative comorbidities (Table 2).6,7,34,35 Their implications for ocular comorbidities, however, remain understudied and insufficiently documented.
Indications for semaglutide and liraglutide were subsequently expanded to include chronic weight management as adjuncts to a reduced-calorie diet and increased physical activity. No pharmacologic monotherapy for overweight or obesity has been approved by the FDA. Owing to the growing societal emphasis on weight control and public demand for easy and rapid weight-loss pharmacologic interventions, Ozempic and Wegovy (Novo Nordisk) have emerged as widely recognized household brands—often driven by marketing that omits conditional recommendations and potential adverse effects, including ocular complications. 61
Recognition of glaucoma, DR, and macular disease as neuro-microvascular disorders that worsen with age, together with identification of GLP-1 receptor expression on RGCs, has prompted investigation into the potential protective role of GLP-1 receptor agonists against ocular decline.62,63 Other geroprotective agents have also been explored in a growing body of clinical and translational research for their potential to protect against ocular pathology.14,16,17,22,25,38–45,50,64 Nevertheless, despite promising preclinical findings, clinical evidence has not been substantiated. The ocular safety profiles of widely used metformin, GLP-1 receptor agonists, SGLT-2 inhibitors, and statins remain poorly defined and unresolved, with many associations derived from retrospective cohorts or secondary analyses. The current literature highlights both potential therapeutic effects and adverse events associated with each agent (Table 3), underscoring the need for monitoring pharmacovigilance signals of these evolving therapies and future prospective clinical trials with predesignated primary ophthalmic measures.
Ocular Pharmacodynamics of Geroprotective Agents
GLP-1 receptor agonists
GLP-1 receptor agonists have attracted substantial interest for their potential ocular effects, supported by a growing body of mechanistic, clinical, and translational research. Molecular and preclinical studies consistently demonstrate anti-inflammatory, vasoprotective, and neuroprotective actions in ocular tissues.65,66 Semaglutide can activate AMPK in retinal tissues, enhance aqueous humor outflow, and attenuate oxidative and inflammatory injury, thereby providing a biologically plausible foundation for the hypothesis that GLP-1 RAs may mitigate RGC loss and glaucomatous.63,66,67
Substantial clinical evidence has increasingly supported a protective association between GLP-1 receptor agonists and glaucoma risk.11,36,62,68,69 Significantly lower glaucoma incidence among GLP-1 users was first reported in 2022. 11 Subsequent real-world evidence demonstrated reduced incidence of open-angle glaucoma and neovascular glaucoma in both diabetic and nondiabetic populations, independent of glycemic status.25,36,68,70 Meta-analyses similarly supported a pooled reductions in glaucoma risk,71,72 whereas comparison analyses reported greater glaucoma risk reduction compared with metformin, but less compared with SGLT-2i.13,69 Modest IOP reductions have also been described in retrospective analyses, aligning with preclinical observations of improved ocular perfusion and reduced neuroinflammation. 46
Conversely, concerns have emerged regarding a range of ocular adverse events associated with GLP-1 exposure.24–30 A fourfold increased risk of NAION among semaglutide users was first reported in 2024. 24 Subsequent evidence linking semaglutide and other GLP-1 RAs to NAION remains equivocal and has generated considerable debate.25,26,73–75 Elevated risks of other optic neuropathies, including optic neuritis, papillitis, and papilledema, are associated with semaglutide exposure, though causality remains uncertain.27,28,76
Regulatory agencies have responded cautiously, albeit with notable variation across jurisdictions. The European Medicines Agency (EMA) added NAION as a very rare adverse event for semaglutide products and recommends discontinuation upon diagnosis, 77 while the American Academy of Ophthalmology (AAO) and the North American Neuro-Ophthalmology Society (NANOS) emphasize individualized risk–benefit assessment and advise continued monitoring without routine cessation.78,79 Given the widespread use of combination antihyperglycemic and weight-loss therapies, ophthalmologists must remain current with evolving pharmacovigilance data and clinical recommendations.
Associations between GLP-1 receptor agonists and DR also remain unsettled. Early worsening of preexisting DR was first noted in 2016, particularly in the context of rapid glycemic improvement 80 —a known class effect first described in the landmark Diabetes Control and Complications Trial. 81 Subsequent controlled trials and real-world analyses, however, yielded mixed findings, with some confirming the signal and others attributing it to baseline severity or glycemic velocity.25,29,82,83 Nevertheless, the FDA added DR warnings to semaglutide labeling, and the EMA recommended close ophthalmic monitoring. The FOCUS trial, a large prospective study currently underway, is expected to provide definitive evidence regarding this risk.
Pharmacovigilance databases have reported a broad spectrum of ocular events with semaglutide, including ischemic optic neuropathy, maculopathy, optic neuritis, and papilledema, compared with metformin, SGLT-2, or DPP-4.27,28 Additional controversial reports describing associations with AMD, diabetic macular edema, choroidal neovascularization, central serous chorioretinopathy, and paracentral acute middle maculopathy further underscore the limited understanding of GLP-1–related ocular pharmacodynamics.21,66,75,76,84 Large-scale and long-term clinical trials with predesignated primary ophthalmic endpoints are needed to determine causal relationships.
Metformin
Metformin remains the foundational first-line therapy for type 2 diabetes and has long been studied for its potential geroprotective and ocular benefits. Although glycemic control is an important confounder in evaluating ocular outcomes among individuals with type 2 diabetes, mechanistic studies demonstrate that metformin exerts independent protective effects, including AMPK activation, improved mitochondrial resilience, and modulation of cellular stress responses.64,85 These pathways provide a plausible rationale for its associations with reduced ocular decline.
Epidemiological studies consistently report lower incidence of primary open-angle glaucoma among metformin users, independent of glycemic status.12,18 Retinal protective associations have also been described in multiple retrospective and pooled analyses, showing reduced risk of nonproliferative retinopathy and diabetic macular edema.16,86–89 Additional vascular benefits are suggested by reduced incidence of retinal ischemia and RVO. 50 Emerging evidence also points to potential relevance in AMD,47,90 but this could not be confirmed in a subsequent controlled trial. 91
Importantly, aside from the transient retinopathy worsening during rapid glycemic improvement, metformin has not been implicated in NAION, toxic optic neuropathies, or other serious ocular adverse events. Although not FDA-approved for weight management, metformin is frequently prescribed off-label for modest weight reduction in prediabetes or insulin resistance, further expanding its relevance to populations at risk for ocular disease.
Sodium-glucose cotransporter 2 inhibitors
SGLT-2 inhibitors exert broad systemic effects that extend beyond glycemic control, including improvements in vascular function, reductions in oxidative stress, and modulation of inflammatory pathways, which may help explain their observed cardiorenal and retinal benefits.10,92–94
Clinical evidence consistently associates SGLT-2 inhibitors with reduced risks of primary open-angle glaucoma and angle-closure glaucoma,13,37 while genetic profiling supports a plausible causal relationship. 95
Recent real-world data demonstrate reduced progression to proliferative retinopathy and new-onset diabetic macular edema, 17 as well as lower incidence of AMD and uveitis.96,97 In comparative analyses, SGLT-2 inhibitors generally demonstrate a more favorable ocular profile than other glucose-lowering therapies, with no significant ophthalmic adverse events directly attributed to this class to date.37,96
Although SGLT-2 inhibitors have been shown to produce modest weight loss in patients with type 2 diabetes,98,99 they are not FDA-approved for weight management, and off-label use for this purpose remains less common than with GLP-1 RAs or metformin.
Statins
Statins remain foundational therapies for hyperlipidemia and atherosclerotic cardiovascular disease. 100 Emerging ophthalmic evidence, however, remains mixed, with studies reporting both protective and adverse associations, depending on the condition and statin intensity. Statins have been linked to slower DR progression, reduced choroidal neovascularization in nonexudative AMD, as well as protection against noninfectious uveitis, owing to their anti-inflammatory and immunomodulatory properties.14,15,101,102 Conversely, increased risks of glaucoma19,20 and cataract22,103 formation have been reported, with some inconsistent signals that appear to be context-dependent.104,105
Taken together, current evidence suggests that statins exert protective or neutral effects on DR and AMD, while may be associated with context-dependent risks of cataract and glaucoma. Prospective ophthalmic trials and mechanistic investigations are needed to clarify the ocular safety profile in defined patient subgroups and delineate the biological pathways underlying potential visual benefits.
Cannabinoids
Cannabinoids—particularly Δ9-tetrahydrocannabinol (THC) and cannabidiol—exert complex and sometimes conflicting effects on ocular physiology. THC has been shown to transiently reduce IOP by decreasing aqueous humor production, but the effect is short-lived, typically lasting only a few hours.42,43,106 Preclinical exploration of the endocannabinoid system as a therapeutic target for glaucoma has yielded inconclusive results.107–111 Reported ocular adverse effects include conjunctival hyperemia, dry eye symptoms, likely related to reduced tear production and vasodilation,107,108 and potential alterations in retinal signaling and visual processing.109,110 More significant systemic effects, including impaired cognition and motor function, further limit the therapeutic utility of systemic cannabis. Currently, professional societies, including the American Academy of Ophthalmology and the American Glaucoma Society, do not recommend cannabis as a treatment for glaucoma. Emerging interest has focused on topical cannabinoid formulations, which may offer localized IOP reduction with reduced systemic exposure, though clinical evidence remains preliminary.112,113
Calcium channel blockers
Systemic CCBs have been associated in some large datasets with higher odds of glaucoma and thinner macular structural parameters, often without corresponding increases in IOP.44,45 These findings raise the possibility of vascular or neurodegenerative effects rather than pressure-mediated mechanisms. However, real-world cohorts and long-term incidence analyses do not observe consistent or significant increases in glaucoma risk.23,114 Overall, systemic CCBs may carry a small structural risk signal, whereas locally delivered CCBs have demonstrated promising neuroprotective and IOP-lowering properties, which could be leveraged therapeutically with careful patient selection and monitoring.115,116
Spermidine
Current evidence suggests that spermidine supports RGC survival and optic nerve resilience through antioxidant and neuroprotective mechanisms.117,118 Metabolomic studies consistently report reduced polyamine levels, including spermidine, in glaucoma and exfoliation syndrome, suggesting a potential deficiency state.118,119 Despite compelling mechanistic rationale, no clinical studies have yet demonstrated ocular benefits or harms attributable to spermidine supplementation.
Taurine
Emerging evidence over the past decade has demonstrated a central role for taurine in retinal physiology. Taurine is one of the most abundant amino acids in the healthy retina. Experimental depletion accelerates RGC loss and photoreceptor degeneration,120,121 whereas supplementation confers robust neuroprotective effects across multiple models of retinal injury.122,123 Animal models of glaucoma, DR, AMD, and inherited retinal degenerations consistently confirm structural and functional neuroprotection mediated by taurine.124–126 These findings position taurine as a compelling therapeutic candidate for glaucoma and other retinal neurodegenerative disorders.38,39 Nonetheless, existing evidence remains limited to small pilot studies, and definitive clinical trials are needed to establish optimal dosing and long-term safety of taurine as an adjunctive therapy.
Nicotinamide adenine dinucleotide precursors
Growing evidence implicates age-related NAD+ depletion in RGC vulnerability. NAD+ decline emerges early in glaucoma pathophysiology and is tightly linked to mitochondrial dysfunction, metabolic insufficiency, dendritic atrophy, and ultimately RGC loss.40,127,128 Upregulation of CD38, a major NAD-consuming enzyme, has been recently identified as a contributor to NAD+ loss in early age-related glaucoma, offering fresh insight into glaucoma pathophysiology and providing a mechanistic rationale for NAD+ augmentation strategies. 129 Replenishing NAD+ through precursor supplementation has been shown to protect RGCs, preserve mitochondrial function, and support healthy aqueous outflow.40,130 Translational uncertainties remain regarding long-term dosing, durability of effect, and systemic safety. 41 Controlled clinical trials are needed to determine if NAD+ restoration can meaningfully alter retinal decline.
Rapamycin
Rapamycin is an mTOR inhibitor with established systemic geroprotective properties. Ophthalmic investigations in preclinical models of corticosteroid-induced glaucoma demonstrate reduced trabecular meshwork fibrosis and improved IOP.131,132 Rapalogs such as zotarolimus also decrease postoperative scarring and help preserve bleb function following glaucoma filtering surgery.133,134 Despite these mechanistic insights, clinical evidence remains absent, and the translational relevance of these findings has yet to be established.
Mifepristone
Glucocorticoid exposure has been shown to induce trabecular meshwork extracellular matrix remodeling and fibrosis, increasing outflow resistance and the risk of ocular hypertension.135–137 On this basis, glucocorticoid receptor antagonists such as mifepristone have been hypothesized to modulate aqueous outflow and trabecular meshwork homeostasis. However, no clinical studies to date have demonstrated a direct therapeutic benefit in glaucoma or ocular hypertension. Further investigation is required to determine whether these theoretical mechanistic pathways translate into measurable ocular outcomes.
Conclusion
The rapid adoption of GLP-1 RAs illustrates how public interest in longevity and weight regulation may accelerate the development and uptake of emerging health-promoting pharmacologic agents. Although these therapies aim at systemic benefits, they may also confer ocular therapeutic potential or carry unanticipated ocular risks that are not fully characterized during early clinical development. As additional geroprotective agents enter clinical use, ophthalmologists should monitor the clinical integration and pharmacovigilance signals of these evolving therapies and incorporate ophthalmic assessment into patient care. Prospective studies and interdisciplinary collaboration are essential to clarify the ocular safety profiles of future longevity-promoting agents and to inform evidence-based guidance for their safe clinical integration.
Authors’ Contributions
A.S.K.: Conceived study, designed review protocol, supervised, and approved. A.Y.Z.: Conducted search, screened studies, and revised article. A.N.: Conducted search, screened studies, synthesized, drafted, and revised article.
Footnotes
Ethical Considerations
As this review synthesizes data from previously published studies and does not involve human participants, ethics approval was not applicable.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors did not receive any funding for this study.