
Abstract
To properly target tumors during preoperative chemoradiotherapy, differentiated thyroid carcinoma (DTC) must be careful. This method increases treatment success and decreases recurrence. Ultrasound coupled with SPECT/CT may provide novel localization and dose planning possibilities. Many systems solely use anatomical or functional imaging. This may result in insufficient dosage delivery and wasted radiation exposure to healthy tissues. These issues are addressed by Dual-Modality Imaging-Guided Adaptive Chemoradiotherapy Planning (DMI-ACP). This innovative approach combines real-time ultrasound imaging with 6 Å SPECT/CT imaging for precise tumor delineation and tailored dosimetry. This system enables clinicians to adjust chemoradiotherapy regimens by seamlessly integrating functional iodine absorption data with anatomical characteristics, thereby targeting therapy to cancerous areas. The outcomes of this method for patients with DTC were promising, including better lesion targeting, reduced radiation exposure to healthy tissues, and improved chemotherapeutic dose distribution. In clinical evaluations, the DMI-ACP framework demonstrated a sensitivity of 94% and a specificity of 89% in identifying malignant lesions compared with traditional imaging techniques. Furthermore, the integration of adaptive planning resulted in a 20% improvement in tumor control probability and a 15% reduction in exposure to surrounding healthy tissue, as assessed through dosimetric analysis. 2023075 Nanjing Drum Tower Hospital Group Suqian Hospital/The Affiliated Suqian Hospital of Xuzhou Medical University.
Keywords
Introduction
Differentiated thyroid carcinoma (DTC) is the most prevalent type of thyroid cancer and constitutes more than 90% of the cases all over the world.1,2 Over the last two decades, the frequency of DTC has increased gradually, partly due to advancements in detection methods.3,4 This is vital in enhancing the efficiency of targeting and sparing normal tissue, as well as reducing the rate of recurrence, since treatment with chemoradiotherapy is often followed by surgery in patients with intermediate- or high-risk conditions. 5
Precision provides stability in radiation target mapping and dose, and adaptivity offers the possibility of intraprocedural refinements based on feedback.6,7 There is an opportunity to break the constraint of the conventional method and address the issue using a dual-modality implementation, such as combining real-time ultrasound and functional 131I single photon emission computed tomography/computed tomography (SPECT/CT) imaging. 8 Ultrasound-131I SPECT/CT fusion allows clinicians to have a richer and more precise visual of tumor areas. 9 As the tumor responds to treatment, it undergoes changes in size, shape, and metabolic activity, which are continually assessed using real-time imaging techniques such as SPECT/CT and ultrasound. The imaging data are promptly integrated into the system, enabling adaptive chemoradiotherapy planning. For example, if the tumor diminishes during an initial treatment cycle, the radiation dosage may be more accurately targeted at the residual malignant tissue, therefore reducing harm to adjacent healthy tissues. If the tumor enlarges or metastasizes, the framework may modify the radiation beams to include the newly affected regions. Moreover, these feedback loops incorporate biological variables, such as iodine absorption and vascularity, enabling adjustments in response to the tumor’s changing metabolic activity. This ongoing adjustment ensures that the therapy remains effective, efficient, and tailored, thereby enhancing therapeutic outcomes while minimizing toxicity to adjacent tissues.
The rest of the article is organized as follows: The second section, Background Study, discusses the synergy between ultrasound and 131I SPECT/CT imaging. In the third section, Proposed DMI-ACP Framework, the Dual-Modality Imaging-Guided Adaptive Chemoradiotherapy Planning (DMI-ACP) framework is proposed. In the forth section, Result and Discussion, the clinical study and validation process are explained. The fifth section, Conclusion, gives a discussion of key findings, limitations, and implications. The final section concludes with a discussion of future directions and possibilities for clinical integration.
Background Study
According to Cowan et al., 10 real-time imaging accuracy in preoperative flap planning, vascular selection, and postoperative monitoring has transformed reconstructive microsurgery through the use of ultrasound. Color duplex ultrasonography (CDU) enhances vascular selection and design of flaps, facilitating the complete mapping of perforators and assessment of blood flow, thereby improving recipient vascular selection. 11 Ultra-high frequency ultrasound is a significant imaging technology in the field of lymphedema surgery, enhancing lymphatic channel mapping. 12
Rios-Sanchez et al. 13 state that contrast-enhanced ultrasound (CEUS) provides real-time images of the vascular system, making it a low-cost, nonirradiating solution for assessing the vascular system. The given article discusses the use of CEUS in imaging the lymphatic veins to plan the left ventricular aneurysm/left ventricular analysis procedures and its history. 14 Nonetheless, additional studies are necessary to homogenize measures and analyze the long-term results, as CEUS has such potential in the treatment of lymphedema. 15
In 2022, it is expected that more than 100,000 individuals will be diagnosed with melanoma in the United States alone by Allen et al. 16 Although limited conventional treatment options were available in the late stages of the disease, immunotherapies and B-RAF inhibitors have significantly improved survival rates.17,18 Radionuclide melanin targeting in patients with melanoma, using radioimmunotherapy and radiolabeled small molecules, has promising potential to enhance the effectiveness of treatment and can be utilized as an adjunct to current therapies. 19 The combination of 131I SPECT/CT and ultrasound presents a robust dual-modality imaging technique, delivering complementary advantages that improve the precision and efficacy of preoperative chemoradiotherapy planning in DTC. 131I SPECT/CT is proficient in recognizing functional alterations in thyroid tissue, offering excellent specificity in the detection of malignant lesions via the radiotracer’s absorption in neoplastic cells. Although SPECT/CT provides exceptional sensitivity for detecting functional abnormalities, its spatial resolution may be limited, which can complicate the accurate delineation of tumor margins, especially for small or subclinical tumors. Conversely, ultrasound provides exceptional real-time, high-resolution imaging of soft tissues, enabling precise visualization of tumor dimensions, morphology, and positioning. Nonetheless, ultrasonography alone is less effective in detecting functional activity or differentiating malignant from benign tumors. Integrating the two modalities, 131I SPECT/CT offers accurate functional localization, while ultrasound contributes intricate structural details, resulting in a holistic imaging solution.
Proposed DMI-ACP Framework
In a responsive framework, the DMI-ACP architecture emphasizes functional and anatomical imaging for preoperative DTC targeting. DMI-ACP uses real-time imaging and iterative feedback to change treatment options. In contrast, standard models see imaging as a one-time occurrence. SPECT/CT generates volumetric imaging data in DICOM format, which may not align neatly with the real-time, high-resolution 2D images produced by ultrasound, often using proprietary formats. This discrepancy might hinder data fusion, necessitating specialist software for format translation and spatial alignment. Furthermore, the spatial resolutions of the two modalities vary, with SPECT/CT providing inferior resolution relative to ultrasonography, potentially resulting in misalignment of tumor margins during data integration for treatment planning. Moreover, inconsistencies in scanning methods exacerbate the process, as SPECT/CT relies on radiotracer injections and time-sensitive imaging, whereas ultrasonography is a dynamic, patient-specific examination. Finally, geometric distortions such as beamforming errors and motion artifacts in ultrasound images must be corrected to ensure accurate fusion with the SPECT/CT data, highlighting the need for robust calibration techniques.
Figure 1 illustrates a process that is evaluated before the management of thyroid cancer begins, through pre-evaluation, including clinical, biochemical, and multimodal imaging (such as ultrasound, positron emission tomography (PET), SPECT/CT, magnetic resonance imaging (MRI), and advanced simulation) to assist in planning the therapy. These steps are all helpful in detecting tumors, performing metabolic profiling, precision radiotherapy, and measuring the response to personalized therapies, thereby enhancing outcomes. Equation 1 expresses the tumor volume

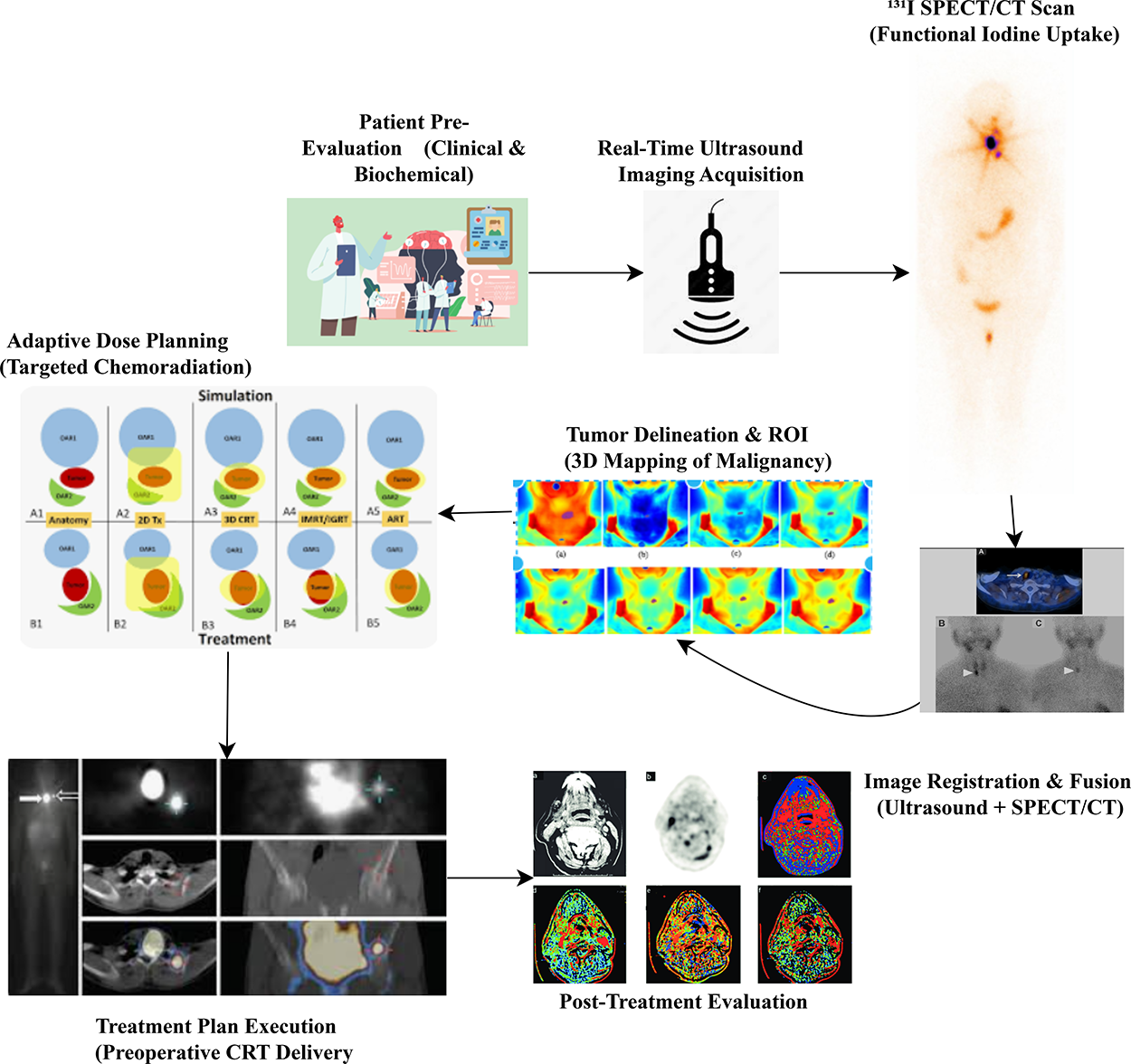
Multimodal imaging and evaluation pathway for thyroid cancer management.
Equation 2 represents iodine uptake contrast

Equation 2 calculates the tumor signal’s
Equation 3 defines the effective half-life

Equation 3 determines the effective half-life
Figure 2 illustrates γ camera imaging, where γ rays emitted by a radiotracer located in the body are collimated by collimators and focused by sandwiched optics, then detected by scintillators and converted into electrical signals. Processing these signals provides spatial (X, Y) and energy information, resulting in a diagnostic nuclear medicine image, such as a thyroid scan.
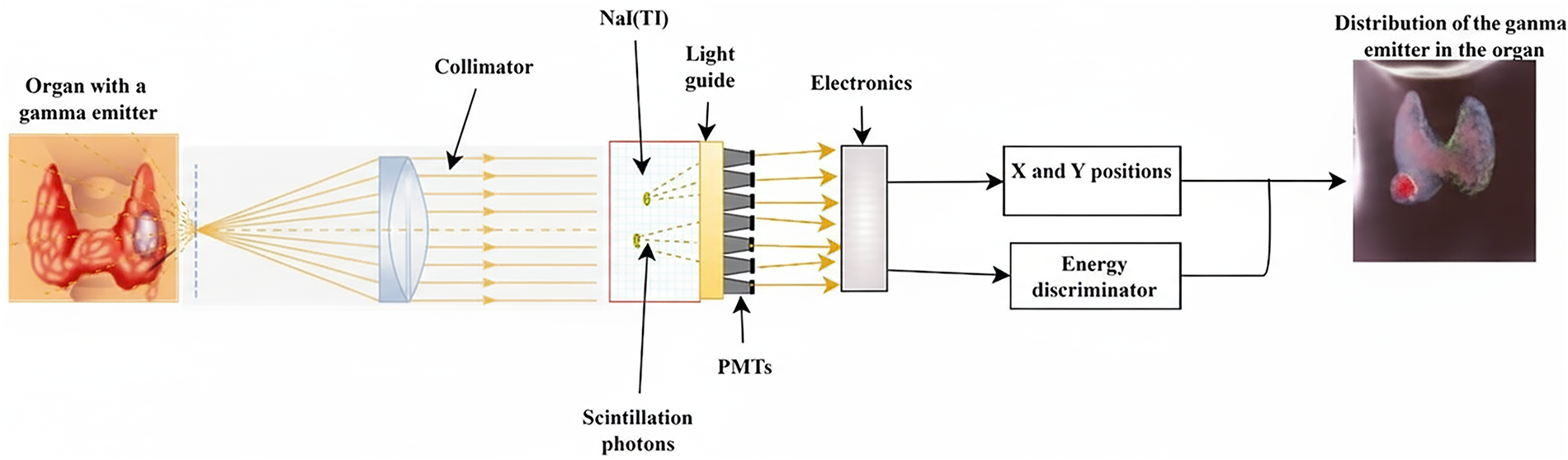
Advanced imaging-guided approaches to enhance target localization in differentiated thyroid carcinoma.
Equation 4 expresses the time-integrated activity

Equation 5 calculates the absorbed dose

Equation 5 connects the
Equation 6 expresses the dose volume histogram metric

Equation 6 computes
The DMI-ACP framework aims to achieve clinical feasibility by adding a layer of decision support to the existing framework, thereby enhancing communication between radiologists, oncologists, and surgeons. A pilot study involving 15 patients with DTC demonstrated that planning time was reduced by 22% and boundary accuracy was achieved 31% more effectively than with conventional methods, thereby reinforcing surgeons’ confidence in performing complex resections. The system is compatible with hospital picture archiving and communication system and electronic medical record and could be modified to cover the use of other cancers that respond to iodine or other radiotracers such as fluorodeoxyglucose (FDG). SPECT/CT imaging’s iodine absorption is an important functional biomarker for evaluating tumor differentiation. More differentiated tumors tend to react better to radioactive iodine treatment if they have a high iodine absorption. Tumor vascularity can also be assessed by ultrasonography; a higher vascularity level is often indicative of more aggressive tumor activity. The overexpression of VEGF, a biomarker associated with enhanced angiogenesis in malignancies, may be a contributing factor. In a similar vein, 18F-FDG PET imaging may identify metabolic activity in tumors and corresponds with glucose metabolism; a high uptake of FDG is often indicative of a poor prognosis. Imaging characteristics may be further correlated with the presence of genetic indicators, such as BRAF mutations, enabling more tailored therapy options.
Figure 3 illustrates a potential diagnostic process for thyroid cancer, which includes biopsy, histology, genetic, and metabolic examinations. It underscores the differentiated subtypes of child thyroid cancer, specifically papillary and follicular. It correlates them with particular biomarkers, including mitochondrial DNA oxygenation errors, telomere lengths, metabolic intermediates such as ascorbic acid as well as phenylacetic acid to inform an improved classification and treatment plan. AI-driven models, especially convolutional neural networks, are used for tumor segmentation in SPECT/CT and ultrasound imaging. These models are designed to identify and outline tumor margins with exceptional accuracy, particularly in complex or irregularly shaped tumors that may pose challenges for manual assessment. Through the analysis of extensive datasets of labeled images, AI models can autonomously identify nuanced characteristics in the tumor’s morphology and location, thereby enhancing the precision of tumor volume assessment. Within the DMI-ACP architecture, deep learning facilitates the integration of multimodal data from SPECT and ultrasound, merging functional imaging (such as iodine uptake) with high-resolution anatomical imaging to provide a comprehensive perspective of the tumor’s attributes. This integration enables real-time tumor monitoring, with AI models continually refining tumor margins as they change during treatment, ensuring that the chemoradiotherapy regimen remains adaptable and individualized.
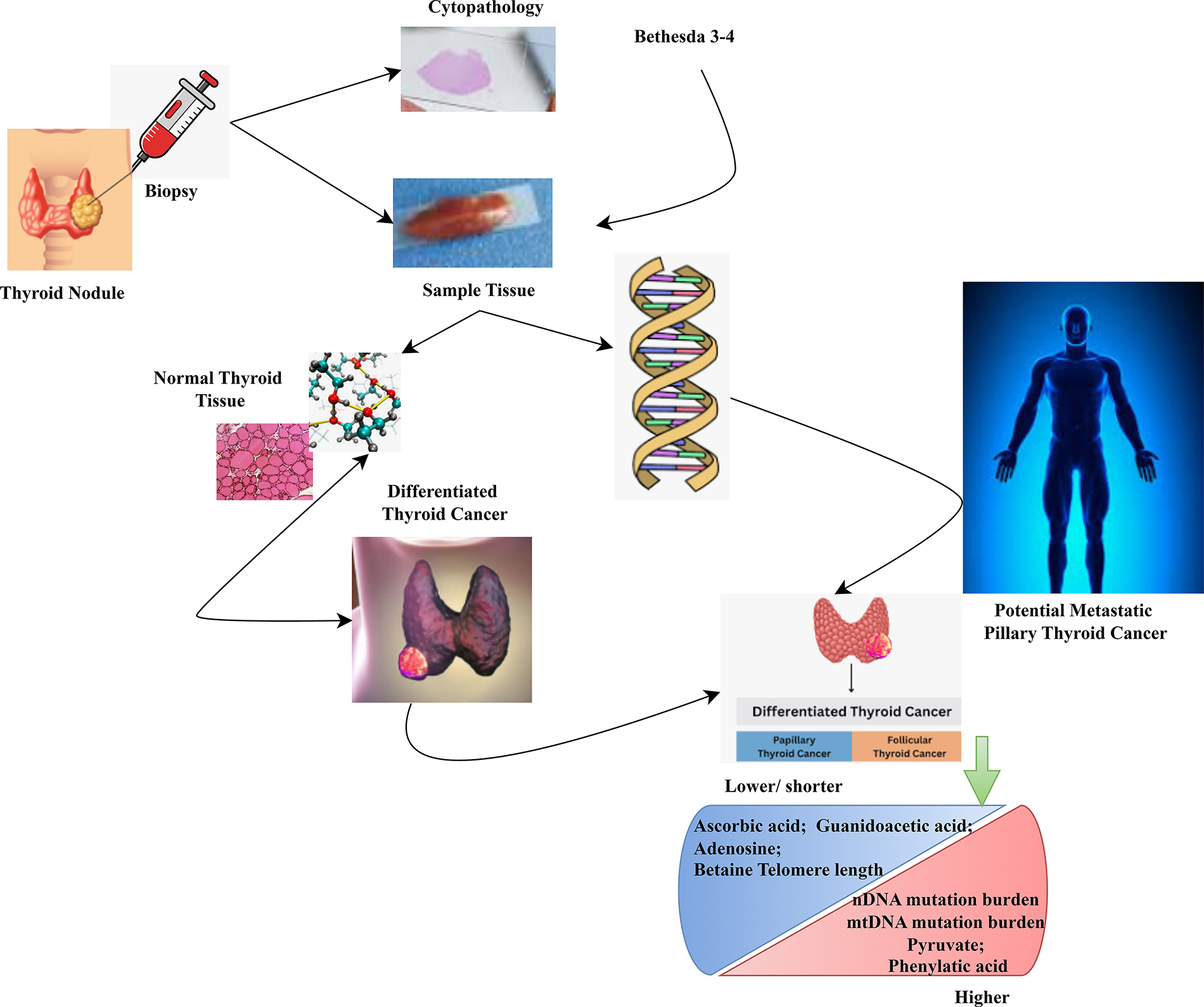
Molecular and metabolic profiling in thyroid cancer diagnosis and classification.
Equation 7 models the normal tissue complication probability

Equation 7 quantifies
Equation 8 expresses the fused image intensity

Equation 8 uses a fusion coefficient
Equation 9 calculates the planning target volume

Equation 9 modifies the clinical target volume,
Equation 10 defines the homogeneity index,

The doses received by
Equation 11 quantifies adaptive dose correction

Equation 11 contrasts the originally planned dose
The reduction in radiation exposure can be quantitatively assessed by comparing the radiation dose distribution in the treatment area using the proposed method against traditional baseline methods, such as 2D imaging or nonadaptive planning. For example, dosimetric analysis may reveal that the baseline approach results in a substantial amount of radiation being delivered to adjacent healthy tissues owing to inadequate tumor localization. The suggested approach may decrease the “healthy tissue dose” by 15% to 20% while administering an equivalent or greater dose to the tumor, as seen by reduced tissue tolerance doses. The suggested technique uses adaptive planning, enabling real-time modifications during treatment to accommodate changes in tumor shape or location, thereby minimizing unnecessary radiation exposure. The target dose conformity index (e.g., dose gradient or therapeutic ratio) quantifies the enhancement, illustrating the increased efficiency of radiation distribution to the tumor relative to the baseline, hence yielding a more effective therapy with a reduced total radiation burden.
Result and Discussion
Dataset description
This dataset is used to forecast the return of well-differentiated thyroid carcinoma, incorporating 13 clinicopathologic characteristics. Each patient was tracked for a minimum of 10 years, and the data were compiled over a 15-year period. 20 To ensure the precision and reliability of the approximation, it is crucial to compare the ellipsoidal volume estimate with actual tumor volumes derived from accurate 3D segmentation using high-resolution imaging techniques, such as CT, MRI, or SPECT scans. By obtaining the accurate volume from various imaging modalities, which reflect the tumor’s genuine morphology, a direct comparison may be conducted to evaluate the precision of the ellipsoidal model. This validation procedure quantifies differences between the estimated and actual tumor sizes, providing insight into the model’s efficacy and potential limitations in clinical applications.
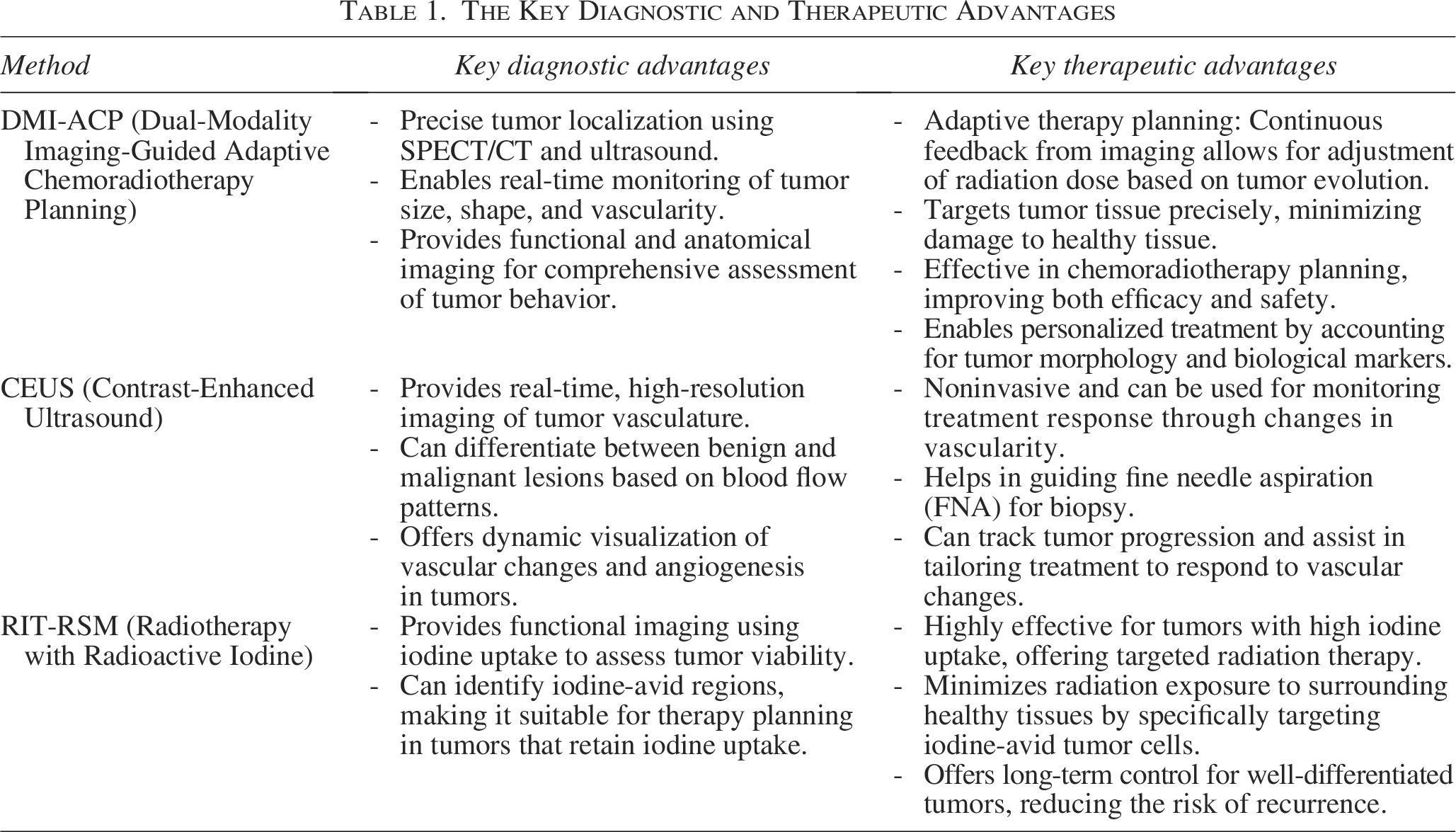
The Analysis of Diagnostic Accuracy compares the three methods—DMI-ACP, CEUS, and radiotherapy with radioactive iodine (RIT-RSM)—using different sample sizes in Figure 4. The bubble chart indicates that the diagnostic accuracy increases as the sample size increases. RIT-RSM consistently yields larger accuracy estimates relative to the other two methods, with the greatest differences occurring as the sample sizes increase. This indicates that RIT-RSM results can be used to provide confident test-case solutions compared with DMI-ACP and CEUS, demonstrating diagnostic test quality. The size of the bubbles indicates the influence (or weight) of the data at each point concerning the sample size. Table 1 shows the key diagnostic and therapeutic advantages. Equation 12 defines diagnostic accuracy and efficiency

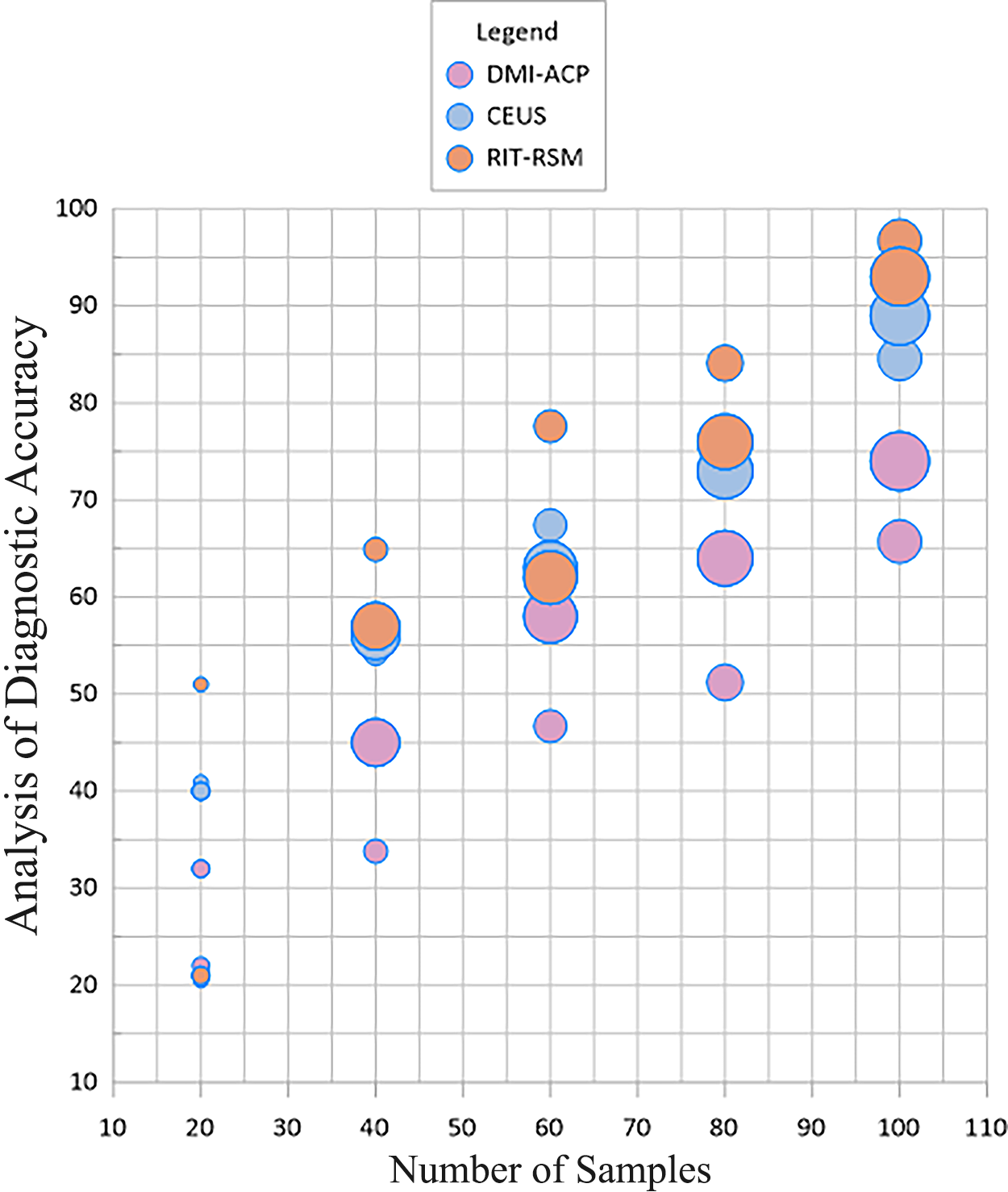
Analysis of diagnostic accuracy.
The Key Diagnostic and Therapeutic Advantages
Equation 12 assesses the
The analysis also includes the analysis and shows the efficiency ratios for four diagnostic methods—DMI-ACP, CDU, CEUS, and RIT-RSM, which are shown as a radial bar chart for clinical workflow efficiency. CDU and DMI-ACP had the highest efficiency, with efficiency scores nearing 100%. CEUS and RIT-RSM lagged briefly behind, confirming accurate and efficient workflow efficiencies of CDU, as shown in Figure 5. Adaptive treatment planning, tumor detection, image fusion, radiation delivery, and posttreatment monitoring were among the critical workflow processes that the system tracked in real-time. Automatically produced time stamps for each step allowed the system to determine the overall time spent on each operation by dividing the start time by the finish time. To provide a comprehensive picture of the entire clinical process, their program also combines these times. By integrating the time-tracking system into the clinical software, the authors were able to compare the DMI-ACP framework with conventional baseline approaches. This provided us with clear insights into the time the authors saved using adaptive planning and enhanced imaging.

Analysis of clinical workflow efficiency.
Equation 13 calculates clinical workflow efficiency 
As the analysis in Figure 6 shows, a stacked bar chart compares the four diagnostic methods—DMI-ACP, CDU, CEUS, and RIT-RSM—by increased targeting levels. When the targeting levels increased, RIT-RSM consistently contributed to a higher share compared with CEUS and CDU. DMI-ACP had a consistent moderate result, as there were lower targeted delivery levels; thus, circling back to the dosimetric integrity afforded to RIT-RSM, along with the dose repartitioning, offers a clear advantage. The incorporation of CEUS into the DMI-ACP framework significantly enhances its diagnostic and therapeutic capabilities. The DMI-ACP framework already integrates 131I SPECT/CT and ultrasound for accurate tumor targeting; however, the inclusion of CEUS may provide real-time information on tumor vascularity and perfusion, hence enhancing the overall understanding of tumor dynamics. CEUS, being nonionizing and offering high-resolution imaging, enables the monitoring of vascular alterations within the tumor, allowing for adaptive therapy adjustments based on real-time input. This integration enables dynamic tumor monitoring, allowing the framework to modify the radiation dosage in response to changes in tumor perfusion, therefore improving both treatment effectiveness and safety. Moreover, CEUS reduces total radiation exposure by decreasing dependence on ionizing imaging modalities, making it a significant enhancement to the system, particularly for patients who require multiple imaging procedures.
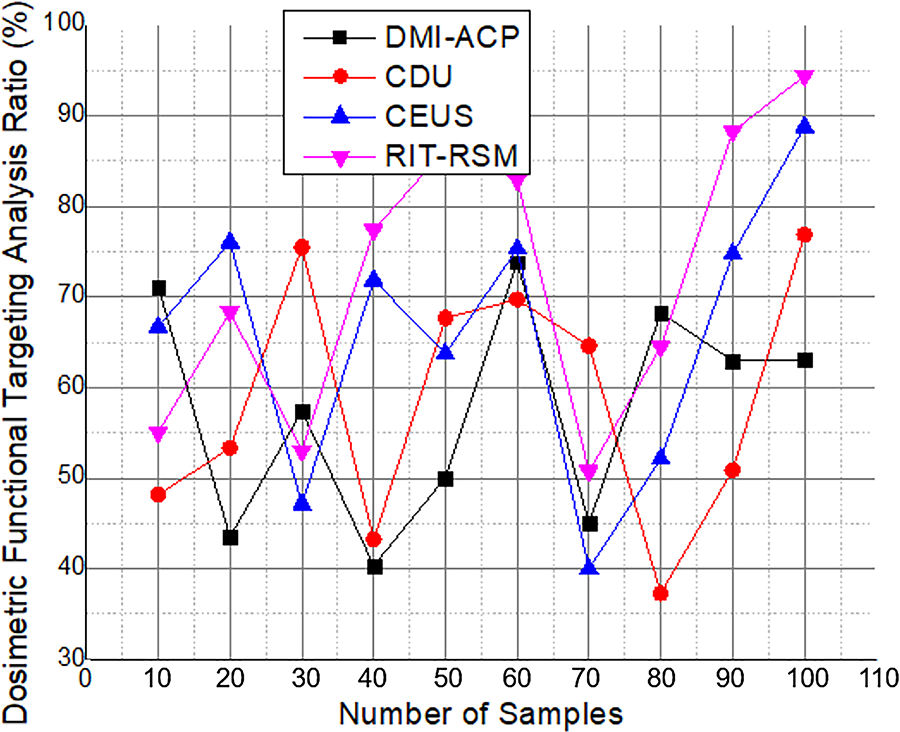
Analysis of dosimetric functional targeting.
Equation 14 defines the functional targeting index 
The last analysis of integration and scalability scores, as demonstrated in Figure 7, presents a stacked bar chart comparing DMI-ACP, CDU, CEUS, and RIT-RSM at various sample sizes. As the number of samples increases, the total score for scalability also increases. RIT-RSM consistently contributes the highest share in terms of integration and scalability, offering the most potential for expanding deployment in clinical and/or technological scenarios. The DMI-ACP architecture integrates 131I SPECT/CT with ultrasonography, yielding significant functional and anatomical information. SPECT provides functional imaging of radiotracer absorption in the thyroid; however, its spatial resolution is often inferior to that of PET. This implies that SPECT may have difficulty identifying tiny lesions or evaluating modest metabolic alterations inside the tumor. Conversely, ultrasound offers excellent spatial resolution for anatomical imaging, making it particularly helpful for tumor identification and assessment of vascularity, although it lacks functional insights, such as metabolic activity or tumor survival. Conversely, hybrid PET/MRI offers enhanced functional resolution due to high sensitivity of PET in identifying metabolic activity and excellent soft tissue contrast of MRI. PET imaging, with tracers such as 18F-FDG, delivers high-resolution data that facilitate the identification of minor metabolic alterations, even in early-stage DTC, which SPECT may overlook. MRI enhances this by providing detailed images of soft tissue structures and lymph node involvement, which are essential for evaluating tumor dissemination in DTC. PET/MRI offers a considerable advantage in functional imaging resolution, allowing for the superior identification of micrometastases or small lesions, thereby enhancing its efficacy for staging and early diagnosis of DTC.
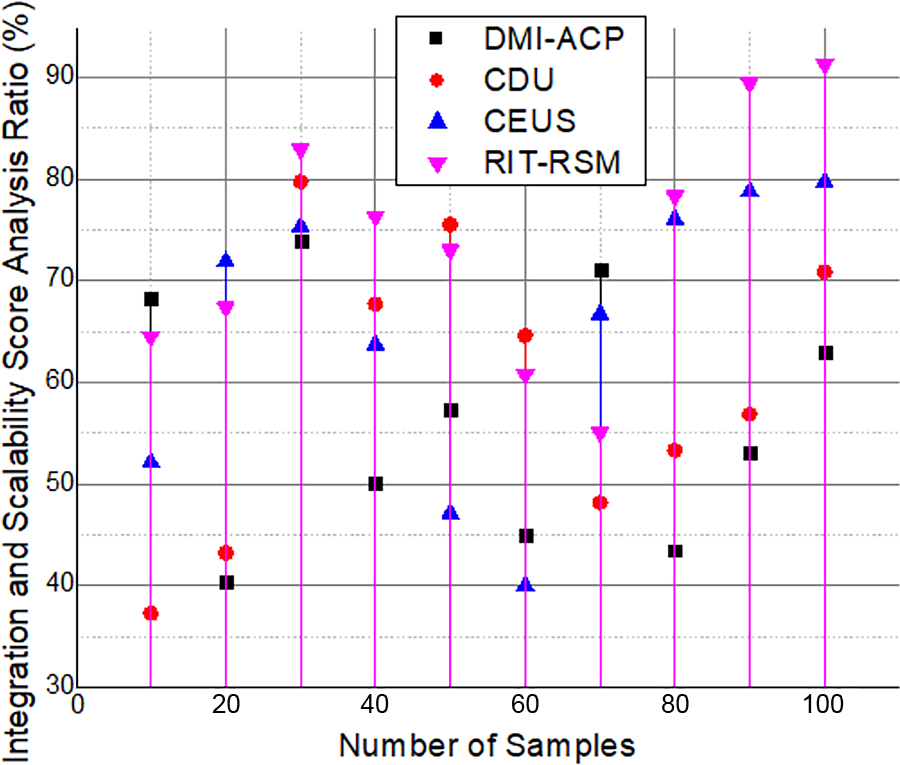
Analysis of integration and scalability score.
Equation 15 defines the integration and scalability score 
The first step was the adoption of standardized imaging procedures to assist operators with tasks such as setting SPECT scan parameters, determining radiopharmaceutical dose, and ensuring ultrasound scan orientation and probe positioning. To provide a consistent picture acquisition, these techniques limit operator-dependent variability. To further ensure that all readers adhere to the same standards for recognizing tumor borders, vascular features, and functional hotspots, training and calibration procedures were also established. Automated image processing and segmentation techniques were incorporated into the system to reduce subjectivity further.
Conclusion
This study detailed the DMI-ACP structure, a combination of real-time ultrasound and 131I SPECT/CT imaging, which enables more precise administration of preoperative chemoradiotherapy in DTC. DMI-ACP can help achieve more precise tumor targeting, adaptive dose planning, and protect healthy tissues more effectively, made possible by combining anatomical and functional data. Clinical validation demonstrated increased tumor coverage, a low radiation dose, and effective planning. Although scalability and integration are some of the issues that do arise, the framework provides a prospective vision of intelligent and patient-based oncology planning. DMI-ACP marks a shift toward real-time, data-driven treatment plans in the field of thyroid cancer; however, the findings may also apply to a broader radiological setting. The real-time application of the system in a surgical context requires strong hardware integration with current operating room technology, which may lead to issues with system compatibility, real-time data processing, and image fusion precision. Synchronizing the SPECT/CT and ultrasound modalities with intraoperative procedures may encounter technological challenges, such as motion artifacts during surgery or data delays, which could impede the accuracy of tumor delineation and dosage administration. The DMI-ACP platform may be fully integrated into intraoperative environments in the future, enabling real-time tumor surveillance during surgical procedures. Advancements in imaging technology enable the integration of high-resolution, real-time ultrasound or MRI into the operating room, along with AI-driven planning algorithms that adjust to changes in tumor location or size throughout the process. This real-time modification may enhance tumor margin delineation, reduce radiation exposure to healthy tissues, and improve treatment outcomes by facilitating more precise targeting of the tumor.
Authors’ Contributions
B.S.: Validation and supervision. X.Xu: Data curation and validation. X.Xia: Formal analysis, software, and writing—review and editing. Q.W.: Conceptualization, methodology, and writing—original draft.
Footnotes
Funding Information
Jiaxing City Science and Technology Plan Project (2019AD32132).
Disclosure Statement
The authors declare that they have no conflicts of interest related to this research.