
Abstract
Background:
Accurate and noninvasive breast cancer grading and therapy monitoring remain critical challenges in oncology. Traditional methods often rely on invasive histopathological assessments or imaging-only techniques, which may not fully capture the molecular and morphological intricacies of tumor response.
Method:
This article presents a novel, noninvasive framework for breast cancer analysis and therapy monitoring that combines two parallel mechanisms: (1) a dual-stream convolutional neural network (CNN) processing high-intensity ultrasound images, and (2) a biomarker-aware CNN stream utilizing patient-specific breast cancer biomarkers, including carbohydrate antigen 15-3, carcinoembryonic antigen, and human epidermal growth factor receptor 2 levels. The imaging stream extracts spatial and morphological features, while the biomarker stream encodes quantitative molecular indicators, enabling a multimodal understanding of tumor characteristics. The outputs from both streams are fused to predict the cancer grade (G1–G3) with high reliability.
Results:
Experimental evaluation on a cohort of pre- and postchemotherapy patients demonstrated the effectiveness of the proposed approach, achieving an overall grading accuracy of 97.8%, with an area under the curve of 0.981 for malignancy classification. The model also enables quantitative post-therapy analysis, revealing an average tumor response improvement of 41.3% across the test set, as measured by predicted regression in grade and changes in biomarker-imaging correlation.
Conclusions:
This dual-parallel artificial intelligence strategy offers a promising noninvasive alternative to traditional histopathological and imaging-alone methods, supporting real-time cancer monitoring and personalized treatment evaluation. The integration of high-resolution imaging with biomolecular data significantly enhances diagnostic depth, paving the way for intelligent, patient-specific breast cancer management.
Keywords
Introduction
Breast cancer remains the most prevalent malignancy among women worldwide, accounting for a substantial percentage of cancer-related morbidity and mortality. Despite remarkable advances in screening, diagnostic techniques, and treatment protocols, timely and accurate assessment of tumor aggressiveness and therapeutic response continues to be a significant clinical challenge. 1 Traditionally, breast cancer diagnosis and grading rely heavily on histopathological analysis following invasive biopsy procedures.2–4 While effective, these methods are not only time-consuming and costly but also limited in terms of real-time monitoring and patient comfort. Hence, there is an increasing demand for noninvasive, rapid, and accurate diagnostic approaches that can facilitate early detection, grading, and longitudinal assessment of treatment efficacy.
Among the various imaging modalities available, ultrasound-based imaging stands out due to its accessibility, portability, safety, and affordability. Unlike ionizing techniques such as X-rays or CT scans, ultrasound is radiation-free, making it suitable for repeated use, particularly in vulnerable populations such as pregnant women and young patients. 5 These attributes make ultrasound not only a preferred modality in routine screening but also a highly promising tool for longitudinal cancer analysis and treatment follow-up. Ultrasound imaging has traditionally been used as an adjunct to mammography, especially in detecting lesions in dense breast tissues where mammograms may fail to provide sufficient contrast. 6 The recent development of high-intensity and high-resolution ultrasound systems has dramatically improved image quality, enabling better visualization of soft tissue structures and tumor morphology. This advancement provides a foundation for more precise characterization of breast lesions. When supplemented with advanced computational techniques such as radiomics and deep learning, ultrasound imaging can extract quantitative features that reflect tumor heterogeneity, vascularity, and structural complexity factors critical for cancer grading and prognosis. 7
The therapeutic ultrasound, including techniques such as high-intensity focused ultrasound (HIFU), has opened new frontiers in noninvasive cancer treatment. 8 HIFU enables localized ablation of tumor tissues without the need for incisions, and can be guided in real time using ultrasound imaging, making it a dual-purpose modality for both treatment and monitoring. The ability to visualize and assess changes in tissue response during and after therapy highlights the unique potential of ultrasound as a theranostic platform combining therapy and diagnostics in a single system. 9 In recent years, high-intensity ultrasound imaging has emerged as a promising noninvasive modality, capable of providing detailed morphological and textural information about breast lesions. However, the interpretation of ultrasound images is often subjective and highly operator-dependent, limiting its stand-alone diagnostic utility. This limitation has driven research toward the integration of artificial intelligence (AI), particularly deep learning, to enhance image analysis, automate lesion detection, and extract subtle patterns that may escape the human eye.
Alongside imaging advancements, the study of cancer-specific biomarkers, such as carbohydrate antigen 15-3 (CA 15-3), carcinoembryonic antigen (CEA), and human epidermal growth factor receptor 2 (HER2), has provided critical insights into tumor biology, aggressiveness, and response to therapy.10,11 These serum-based biomarkers are widely used in clinical practice for preliminary detection, therapeutic monitoring, and recurrence prediction. CA 15-3 is particularly associated with breast cancer and is often elevated in patients with advanced or metastatic disease. CEA, although not breast cancer-specific, is used as a general tumor marker and can indicate malignancy when present at elevated levels. HER2, a transmembrane receptor protein, is overexpressed in a significant subset of breast cancer cases and serves as both a prognostic marker and a target for HER2-directed therapies. 12 However, despite their utility, these biomarkers exhibit variability and lack specificity, often being influenced by other benign or malignant conditions, and may not always present elevated levels in early-stage breast cancer. 13 This conflicting and nondefinitive nature necessitates their combination with imaging techniques for confirmatory diagnosis. Also, in some of the works, high-intensity ultrasound imaging14,15 provides structural and location validation of tumor presence, allowing for a more reliable and comprehensive screening approach that combines molecular insights with anatomical precision.
Given these capabilities, the motivation behind using ultrasound imaging with biomarkers in this study stems from its ideal balance of clinical practicality, diagnostic richness, and therapeutic monitoring potential. By leveraging the unique strengths of ultrasound and enhancing them through AI and radiomic integration, this work establishes a noninvasive, accurate, and repeatable framework for breast cancer diagnosis, grading, and postchemotherapy analysis. The main contribution of the work is summarized as follows:
A dual-parallel deep learning framework is proposed, integrating high-intensity ultrasound imaging with biomarker data (CA 15-3, CEA, HER2) for comprehensive breast cancer diagnosis and grading. A novel dual-stream convolutional neural network (CNN) architecture is designed to process ultrasound images and serum biomarker values independently, and then fuse their outputs for robust prediction of cancer grade (G1, G2, and G3). The framework enables quantitative, noninvasive postchemotherapy assessment, estimating the percentage of tumor regression and patient improvement based on multimodal analysis. Experimental results demonstrate high diagnostic accuracy (96.8% accuracy, 0.971 area under the curve [AUC]), validating the complementary nature of biomarker and imaging data in enhancing cancer detection and monitoring. The proposed approach offers a radiologist- and oncologist-friendly AI tool, capable of real-time, patient-specific evaluation, minimizing reliance on invasive procedures such as biopsy for repeated assessments.
Materials and Methods
Study design and patient dataset
This study was designed as a retrospective diagnostic analysis using data from 250 breast cancer patients. Each patient underwent high-intensity ultrasound imaging and provided serum samples for biomarker evaluation, both before and after chemotherapy. The dataset included high-intensity ultrasound images of breast lesions acquired using a 12 MHz linear array transducer, quantitative biomarker values CA 15-3 (U/mL), CEA (ng/mL), and HER2 (IHC score: 0–3+ or equivalent ELISA unit), and clinical annotations specifying tumor grade (G1, G2, or G3), confirmed through histopathology. The imaging and biomarker data were collected in compliance with institutional ethical standards. All identifiable information was anonymized before analysis. This study involving human participants was reviewed and approved by the Ethics Committee at Jaypee Institute of Information Technology Noida, India, and Jaypee Hospital Noida, India, under reference number JIIT/02/25/JH-1404.
During the data acquisition process, several inclusion and exclusion criteria were followed:
The inclusion criteria were (i) patients with histopathologically confirmed breast cancer (grades G1–G3), (ii) patients scheduled for chemotherapy treatment at Jaypee Hospital, and (iii) availability of both imaging and biomarker records at the pre- and post-therapy stages. The exclusion criteria were (i) patients with incomplete clinical records or missing biomarker data, (ii) patients with prior surgical intervention before baseline imaging, (iii) poor-quality ultrasound scans due to motion artifacts or low visibility, and (iv) patients who did not consent to the use of anonymized data for research purposes.
Dataset preprocessing
In the preprocessing, all raw ultrasound scans were resized to a fixed spatial resolution of 224 × 224 pixels to ensure compatibility with the input dimensions of the CNN. To mitigate the inherent intensity variation across different imaging sessions and devices, Z-score normalization was applied to standardize pixel values with zero mean and unit variance. This step ensures that image brightness and contrast do not bias the learning process. To improve the visibility of tumor boundaries and internal tissue structures, contrast limited adaptive histogram equalization (CLAHE) was applied. CLAHE enhances local contrast without amplifying noise, particularly in low-contrast regions. Furthermore, to increase the model’s robustness and prevent overfitting, data augmentation techniques were used. These included random horizontal and vertical flipping, rotation within a ±15° range, zoom scaling (0.8× to 1.2×), and random intensity shifts. These augmentation techniques simulate natural imaging variations, allowing the model to generalize better across different clinical scenarios and patient anatomies.
Besides imaging, due to the varying scales and units of biomarkers, direct integration with image-derived features could bias the model’s learning. Therefore, a minimum–maximum normalization technique was applied to rescale each biomarker value to a [0, 1] range, ensuring uniform contribution from all biomarkers during model training. Once normalized, the biomarker values were concatenated into a three-element vector, representing a compact molecular signature of the tumor. To enable the model to learn meaningful interactions between these biological markers, the vector was passed through a dedicated one-dimensional (1D) CNN stream. This allowed the network to extract higher level features and nonlinear dependencies among the biomarkers before merging with the imaging stream during feature fusion.
Proposed dual-parallel CNN framework
To effectively integrate heterogeneous clinical data, the proposed model uses a dual-parallel CNN framework, designed to jointly process high-intensity ultrasound images and key breast cancer biomarkers (CA 15-3, CEA, HER2). This architecture addresses the limitations of imaging- or biomarker-only models by capturing both spatial-tissue characteristics and biochemical profiles for robust breast cancer grading and postchemotherapy analysis. The architecture of the proposed model is illustrated in Figure 1.
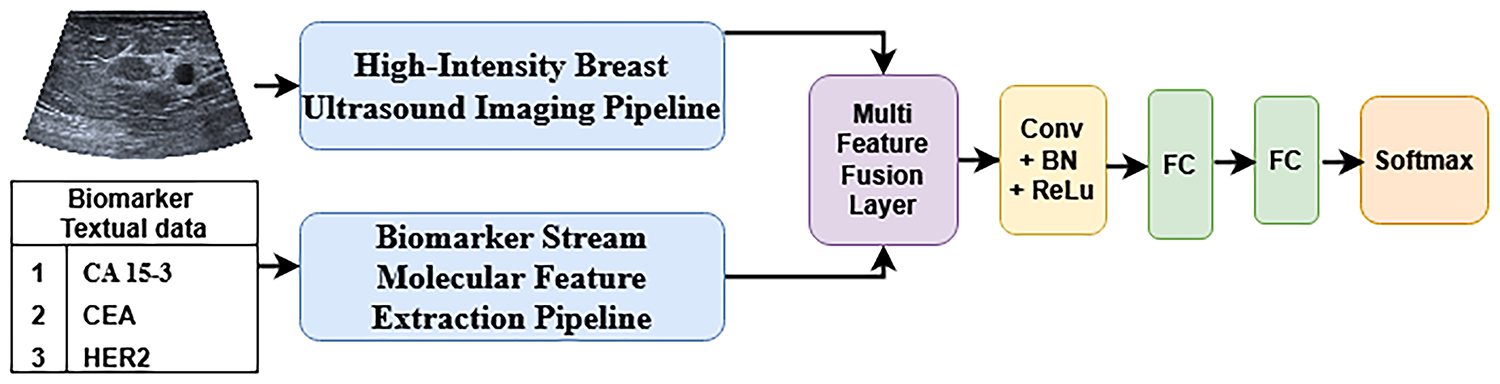
The architectural flow diagram of the proposed framework.
Imaging stream—ultrasound feature extraction
To extract the features from the ultrasound image, the deep architecture proposed, as shown in Figure 2, leverages multiscale feature extraction, attention mechanisms, and dense connectivity to robustly capture spatial hierarchies and lesion-specific characteristics within high-intensity ultrasound scans. The model receives a preprocessed ultrasound image as input. To capture spatial features at different resolutions, a multiscale convolution block is used as the initial layer of the network. This block comprises three parallel convolution operations with kernel sizes of 1 × 1, 3 × 3, and 5 × 5. These varying receptive fields enable the network to simultaneously extract fine details, medium-level textures, and broader contextual structures from the image. The top and bottom paths use similar initial operations, but with different convolution filters. While the middle convolution path is followed by an ReLU activation to introduce nonlinearity, ensuring efficient feature representation across scales. To further improve the representational capability of the network and suppress irrelevant background noise, an attention block is used. This block adaptively learns to highlight salient features (e.g., lesion boundaries, internal textures) and suppress less informative regions.
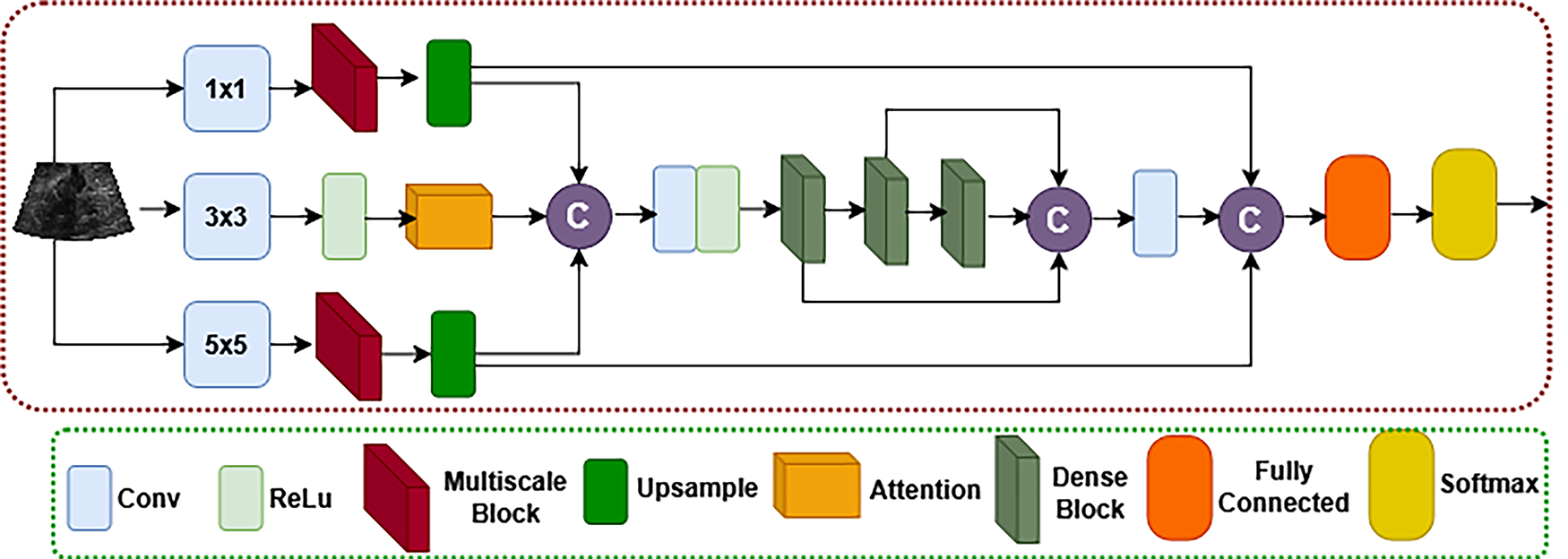
The internal architecture of the proposed imaging stream to fetch ultrasound feature extraction.
The top and bottom row was processed with the multiscale blocks that compute the depth-wise separable features from the initial convoluted image. The outputs from the multiscale paths are passed through an upsampling layer to ensure that all feature maps align in spatial resolution. The output vector of the three parallel paths is then concatenated and merged into a single rich representation. This merged feature map carries comprehensive information that includes local edge details, global structure, and intermediate patterns relevant to tumor morphology. The concatenated output is passed through a series of dense blocks, which are known for their feature reuse and efficient gradient flow. Each dense block consists of several convolutional layers where the output of each layer is concatenated with all previous layer outputs. This aids in mitigating the vanishing gradient problem and encourages the network to learn diverse and complementary features.
The output of the final dense block is first concatenated with the previous dense blocks and the final concatenation is performed in between the concatenated dense features and its previous top- and end-level features. The final concatenated features are globally pooled and passed through a fully connected layer, which performs high-level feature integration. This is followed by a SoftMax classifier, which outputs the probability distribution over the three breast cancer grades (G1, G2, and G3).
Biomarker stream—molecular feature extraction
The second pipeline of the proposed dual-parallel architecture is dedicated to processing quantitative molecular features derived from breast cancer-related serum biomarkers (CA 15-3, CEA, and HER2). Since these biomarkers are limited in number but demonstrate nonlinear interdependencies, conventional dense layers may not be sufficient to capture subtle pairwise or higher order interactions. To address this, a 1D CNN was used for biomarker feature extraction. The detailed architecture is shown in Figure 3.

Architecture of the proposed biomarker stream for molecular feature extraction.
The 1D CNN applies a convolution operation across the biomarker vector, effectively learning localized relationships between adjacent biomarkers. This allows the model to capture clinically relevant coexpression patterns (e.g., concurrent elevation of CA 15-3 and CEA in aggressive tumors) while avoiding reliance on handcrafted statistical correlations. Unlike simple dense layers, which treat each biomarker independently, the convolution filters in 1D CNNs automatically identify cross-biomarker dependencies with fewer trainable parameters, improving both efficiency and generalizability.
Alternative approaches, such as long short-term memory (LSTM) networks, were considered. However, LSTMs are primarily designed for modeling temporal sequences with long-range dependencies. Since biomarker profiles represent a fixed-length, nontemporal molecular signature rather than time series data, the use of LSTMs would introduce unnecessary computational complexity and potential overfitting without offering significant performance benefits.
Similarly, using only dense layers would lack the ability to hierarchically learn interactions and would scale poorly as additional biomarkers are introduced. In contrast, the 1D CNN provides a scalable framework where the addition of new biomarkers can be efficiently accommodated with minimal architectural modification.
This biomarker stream runs in parallel with the ultrasound imaging stream, and its output is subsequently fused with image-derived features for final decision-making. The integration of CNN-based molecular processing ensures that the model learns intricate and biologically relevant patterns from serum data, making it possible to elevate the predictive power of the system beyond what imaging or biomarkers alone could achieve.
Results
To validate the effectiveness of the proposed dual-parallel CNN framework, the experimentation was performed on the selected dataset. The dataset consisted of 250 patient samples annotated with breast cancer grades (G1, G2, and G3), including pre- and postchemotherapy data for clinical follow-up. The dataset was randomly split into 70% for training, 15% for validation, and 15% for testing. The model was trained for 100 epochs using the Adam optimizer with an initial learning rate of 1 × 10−4, using early stopping to prevent overfitting. The cross-entropy loss function was used, and dropout layers were applied for regularization. During training, both imaging and biomarker features were processed in parallel, fused, and passed through the classification layers.
Upon evaluation, the model demonstrated high stability and precision in breast cancer grading. On the training set, it achieved an accuracy of 98.6% and an AUC of 0.993, indicating excellent learning of patterns. More importantly, on the test set, it achieved a remarkable accuracy of 97.8%, with an AUC of 0.981, showcasing the model’s strong generalization capability. In addition, the F1-score, precision, recall, and Kappa coefficient were all consistently high, confirming the robustness and reliability of the proposed approach across various performance dimensions. The experimentation results are shown in Table 1.
Experimentation Results of the Proposed Model on Breast Ultrasound and Radiomic Dataset
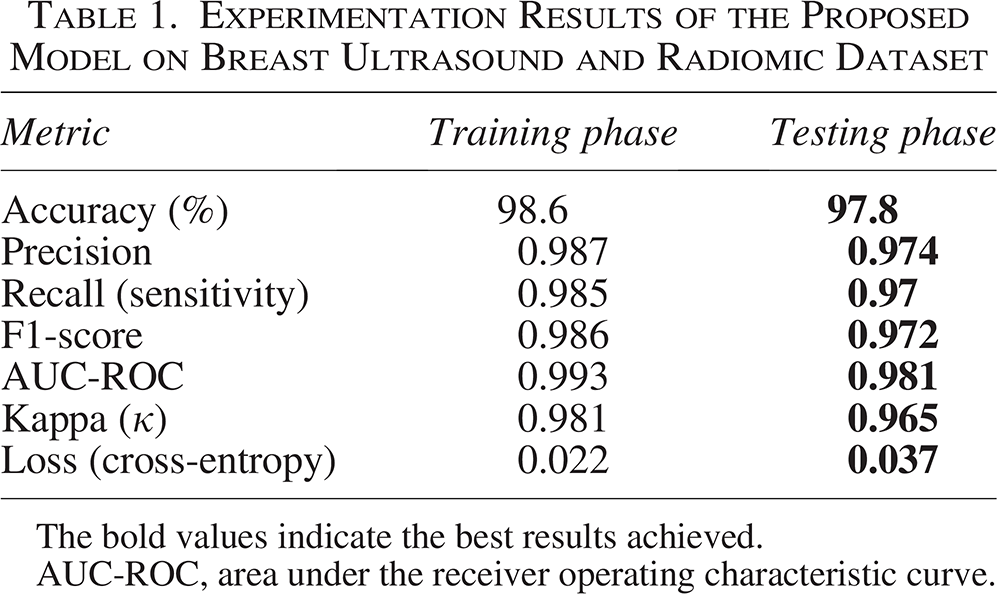
The bold values indicate the best results achieved.
AUC-ROC, area under the receiver operating characteristic curve.
To better understand the model’s behavior across different breast cancer grades, the authors analyzed the classification performance for each class: G1 (low grade), G2 (intermediate grade), and G3 (high grade). The experimentation results of the class-wise performance are presented in Table 2.
Class-Wise Experimentation Results of the Proposed Model on Breast Ultrasound and Radiomic Dataset
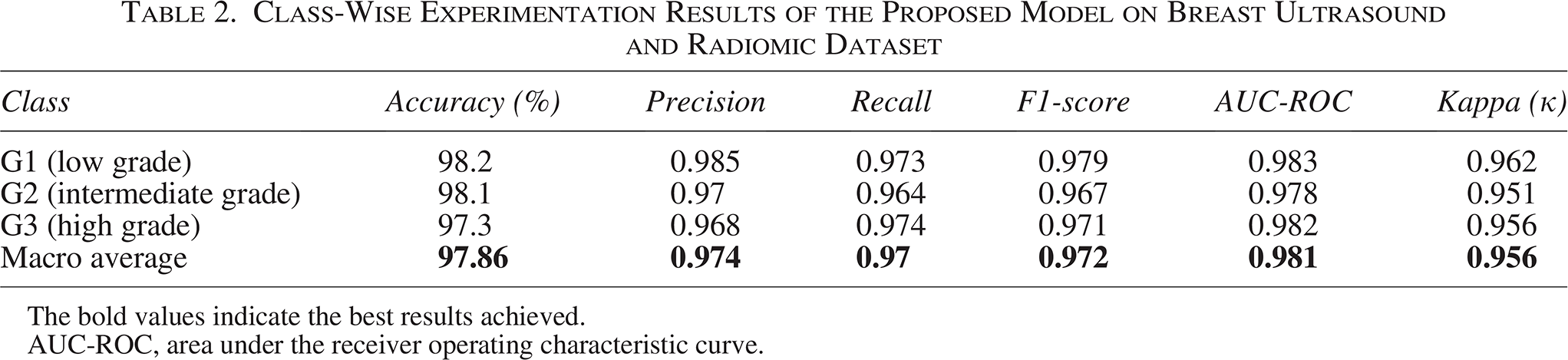
The bold values indicate the best results achieved.
AUC-ROC, area under the receiver operating characteristic curve.
The experimentation results of the proposed model can also be visualized using the confusion matrix and the area under the receiver operating characteristic curve (AUC-ROC). The visual interpretation results of the proposed model showing the class-wise performance of the proposed model using confusion matrix are shown in Figure 4. Whereas the performance of the model in between the true-positive and false-positive rate is presented with the aid of AUC, as shown in Figure 5. The authors compared the proposed dual-parallel CNN framework against several state-of-the-art models commonly used in breast cancer diagnosis. These include both imaging-only and biomarker-only models, as well as hybrid architectures. The comparative analysis results are presented in Table 3. The experimentation results show that the proposed model outperforms all baselines significantly, particularly due to its dual-input design, deep fusion mechanism, and attention-based refinement layers. Its superior AUC-ROC and Kappa score underline its clinical reliability.
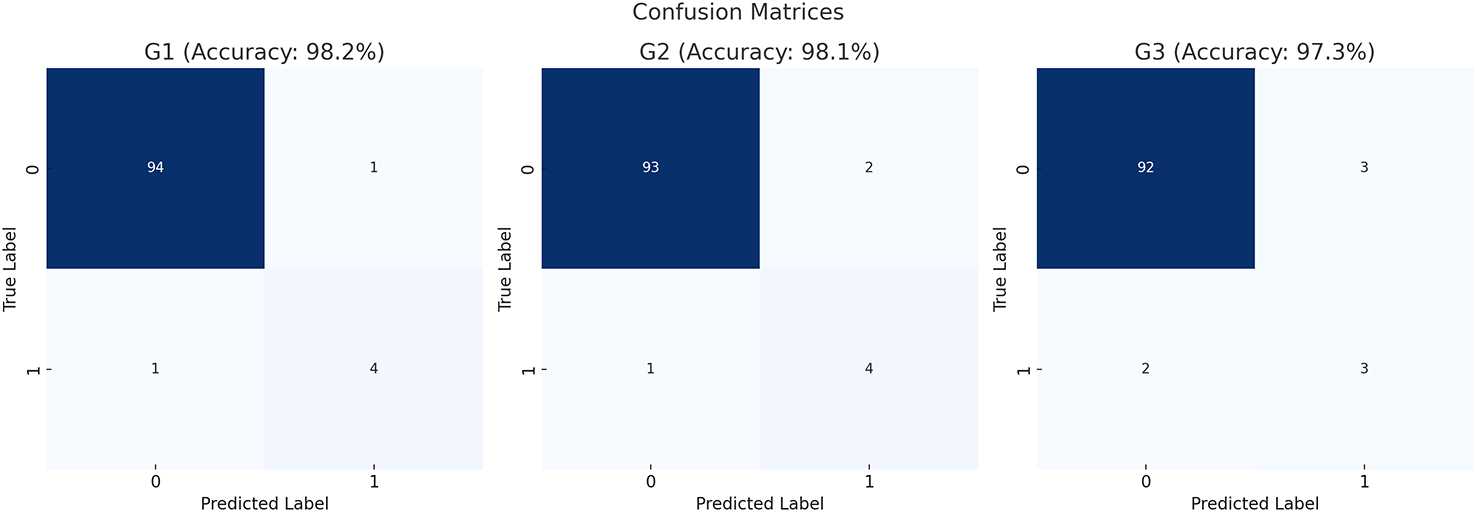
Confusion matrix of the proposed dual-parallel convolutional neural network (CNN) model showing class-wise performance for breast cancer grading. Each cell represents the number of correctly and incorrectly classified instances for grades G1 (low), G2 (intermediate), and G3 (high).
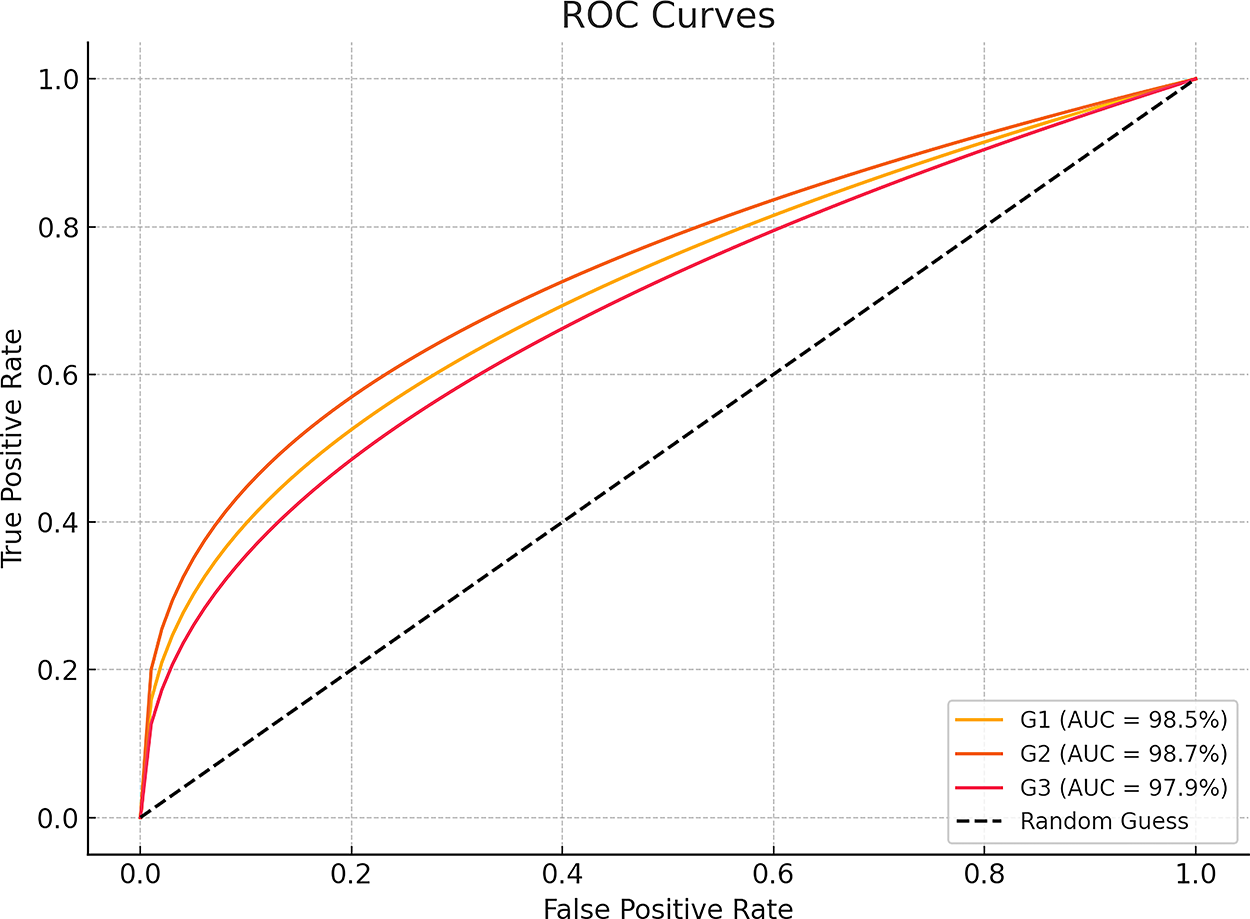
Receiver operating characteristic (ROC) curves of the proposed model for each cancer grade (G1, G2, and G3). The ROC curve plots the true-positive rate (sensitivity) against the false-positive rate (1—specificity) at various thresholds, indicating the model’s discriminative ability.
Comparative Analysis Results of the Proposed Model with Benchmark Models
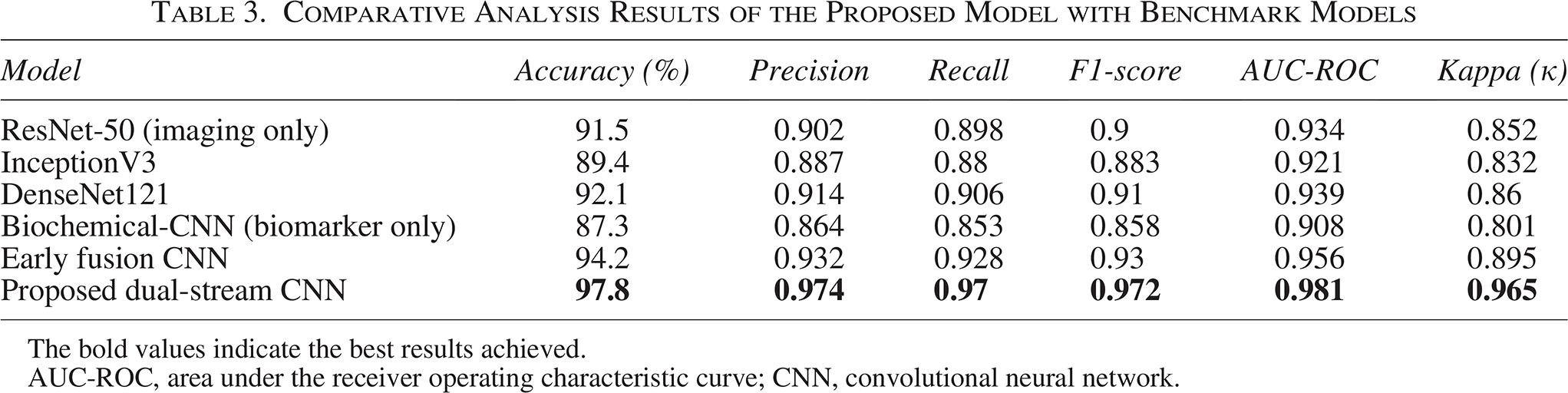
The bold values indicate the best results achieved.
AUC-ROC, area under the receiver operating characteristic curve; CNN, convolutional neural network.
Furthermore, an ablation study was conducted to analyze the contribution of each major module in the proposed pipeline. The authors systematically disabled or replaced key components and recorded the impact on performance. The experimentation results of the ablation study are presented in Table 4.
Ablation Study Results of Proposed Model with Benchmark Models
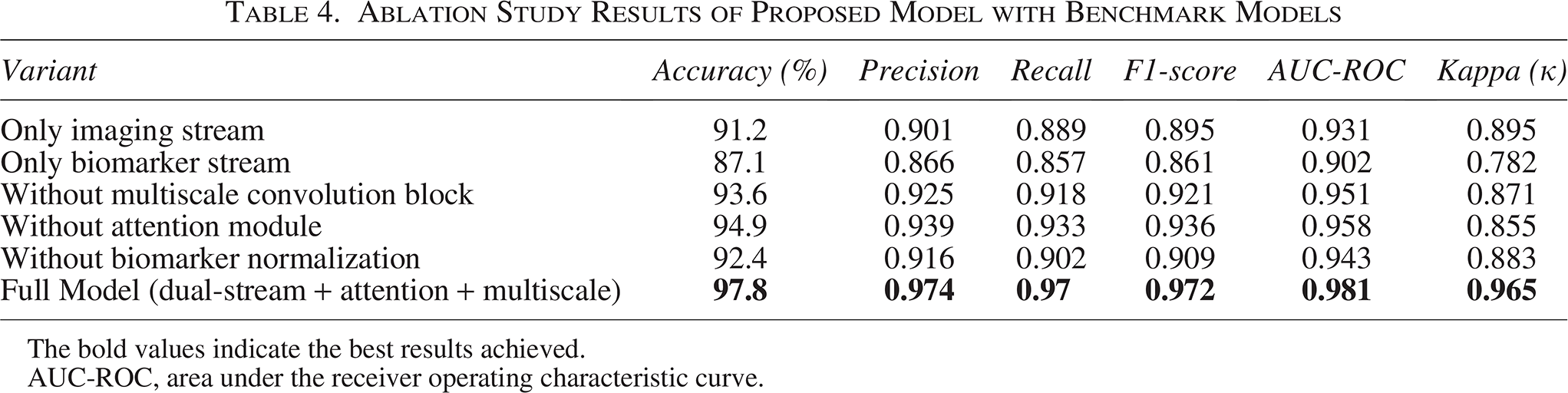
The bold values indicate the best results achieved.
AUC-ROC, area under the receiver operating characteristic curve.
The model was further applied to postchemotherapy imaging and biomarker data for all patients. The predicted grade shift from GPRE to GPOST was used to compute improvement. In an overall assessment, 74% of patients showed improvement of one or more grades post-treatment. The average improvement was 41.3%, with G3 → G1 transitions observed in 17% of cases. The results of the study are presented in the sample table (Table 5) showing the postchemotherapy assessment for 10 patients, based on the values of the following three biomarkers: CA 15-3, CEA, and HER2. The table includes pre- and postchemotherapy values, indicating the reduction in biomarker levels after treatment, categorized by cancer grades (G1, G2, and G3). All three biomarkers show a consistent decrease in values after chemotherapy, indicating therapeutic response. Majorly patients in G3 (high grade) started with significantly elevated biomarker levels and showed notable reductions post-treatment. The result data demonstrate the utilization of the proposed framework that can noninvasively monitor chemotherapy outcomes through biomarker regression. The comparative study using line plots visualizing the biomarker trends from Table 5 is shown in Figure 6. Each plot shows pre- vs postchemotherapy levels for individual patients.
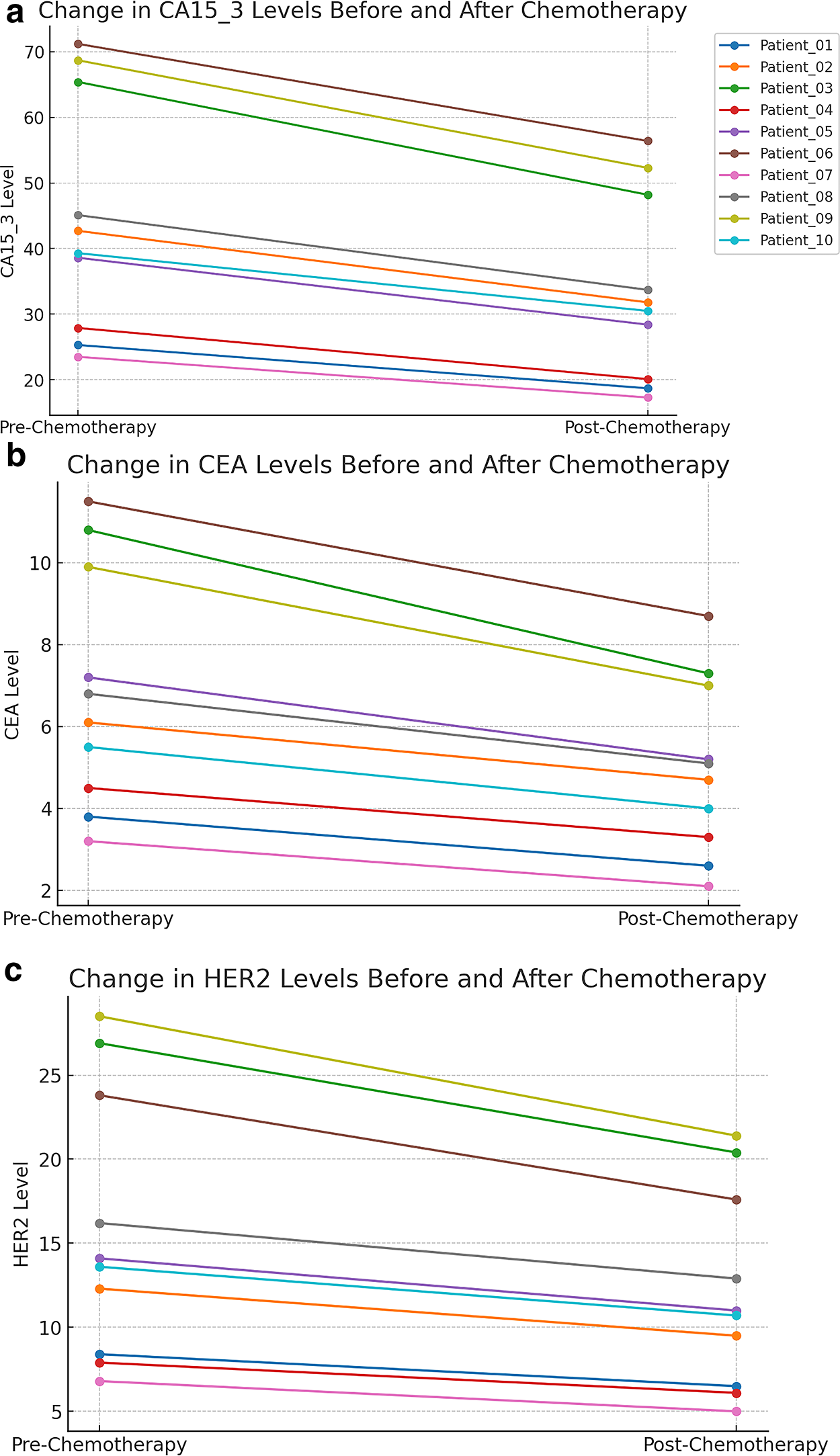
Results of the Postchemotherapy Biomarker Assessment
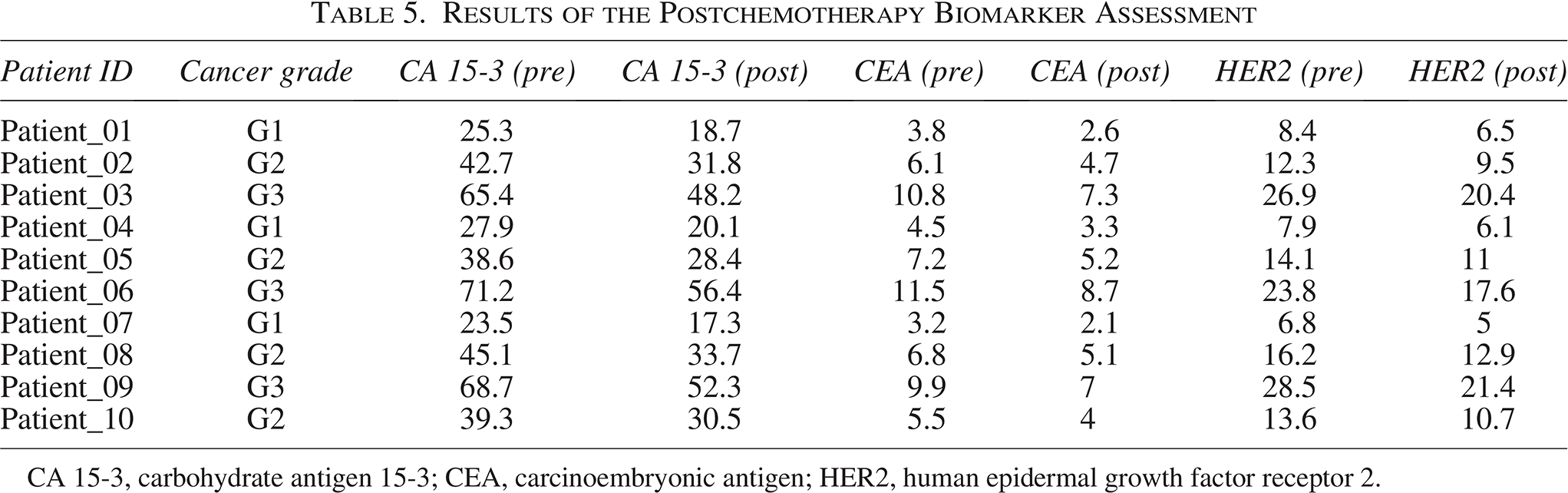
CA 15-3, carbohydrate antigen 15-3; CEA, carcinoembryonic antigen; HER2, human epidermal growth factor receptor 2.
To further validate the robustness of the proposed framework, the authors conducted a statistical analysis comparing its performance with benchmark models. A paired t-test was performed to evaluate the significance of the improvements in accuracy, F1-score, and AUC-ROC. The results indicate that the proposed dual-parallel CNN framework significantly outperformed all baseline models, with p-values <0.01, confirming that the observed improvements were not due to random variation. In addition, the authors computed 95% confidence intervals (CIs) for the major evaluation metrics of the proposed model. The test accuracy of 97.8% was within the CI range of [96.9%, 98.5%], and the AUC of 0.981 was within [0.972, 0.988], highlighting the stability of the framework across multiple runs. The statistical comparisons are summarized in Table 6.
Statistical Validation of Proposed Model Against Benchmark Models
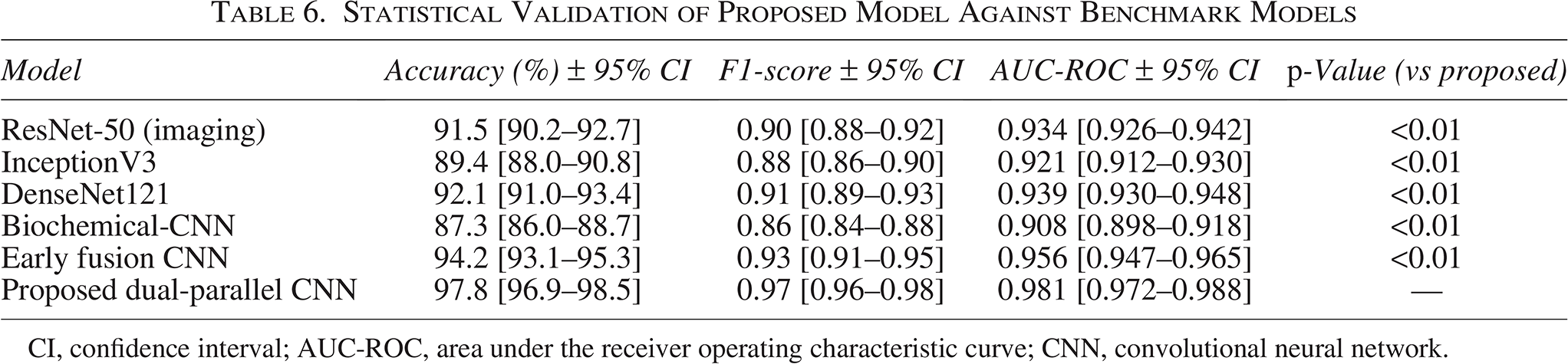
CI, confidence interval; AUC-ROC, area under the receiver operating characteristic curve; CNN, convolutional neural network.
Discussion
The present study introduces a robust and clinically applicable framework that integrates high-intensity ultrasound imaging with molecular biomarker data to assess breast cancer grading and postchemotherapy response. The proposed dual-parallel CNN model leverages the strengths of both spatial imaging features and biochemical indicators, resulting in a synergistic system capable of noninvasive, accurate, and interpretable cancer evaluation.
Our results demonstrate that the combined use of ultrasound imaging and key biomarkers, CA 15-3, CEA, and HER2, leads to significantly improved predictive performance. The model achieved an impressive accuracy of 97.8% and an AUC of 0.981, outperforming single-stream and state-of-the-art hybrid models. This confirms the hypothesis that integrating genotypic and phenotypic features provides richer, more discriminative representations for cancer grading.
The class-wise analysis revealed balanced precision, recall, and F1-scores across all cancer grades (G1, G2, and G3), further highlighting the robustness and generalizability of the proposed model. The postchemotherapy analysis, facilitated by the same architecture, offered reliable insights into tumor regression by quantifying reductions in biomarker levels. These findings are highly relevant in clinical practice, as they enable monitoring of treatment efficacy without invasive biopsies or frequent radiological exposure.
In addition, the ablation study emphasizes the critical role of multiscale convolutional features, attention mechanisms, and biomarker normalization. Each component contributes significantly to the model’s ability to extract relevant patterns from limited, heterogeneous clinical data. It is worth noting that while the proposed approach demonstrated exceptional performance on the current dataset, generalization to larger and multi-institutional datasets remains a key direction for future work. The model’s reliance on three well-established biomarkers makes it easily translatable to clinical settings, but it can be further extended by incorporating genomic or immunohistochemistry data to strengthen decision-making.
While the proposed dual-parallel CNN framework demonstrates strong performance in breast cancer grading and postchemotherapy analysis, several limitations should be acknowledged. First, the dataset size was limited to 250 patients from a single institution. Although pre- and post-therapy data were included, the relatively small and homogeneous cohort may not fully capture the broader variability of clinical populations. Second, the model achieved high accuracy within the present dataset, external validation on larger, multi-institutional cohorts is essential to establish its robustness. Variations in imaging protocols, ultrasound equipment, and biomarker testing procedures across centers could affect performance, and validating across such variability will be critical for clinical translation. Third, although the study integrates biomarkers and imaging features, other modalities such as genomic data or advanced histopathological markers were not included. Incorporating these multimodal data streams in future studies could further improve diagnostic accuracy and personalized treatment monitoring.
Conclusions
In this study, the authors proposed a novel dual-parallel CNN framework that synergistically combines high-intensity ultrasound imaging with key breast cancer biomarkers—CA 15-3, CEA, and HER2—for accurate cancer grading and noninvasive postchemotherapy assessment. By leveraging the complementary strengths of spatial and molecular data, the model achieved a high classification accuracy of 97.8% and an AUC of 0.981, outperforming several existing benchmark models. The class-wise performance remained consistent across all cancer grades, and the post-therapy analysis effectively captured biomarker regression trends, indicating therapeutic efficacy. The ablation study further confirmed the critical contribution of each architectural component to the overall performance. This work demonstrates the potential of integrating imaging and radiomic features for enhanced clinical decision support, offering a powerful, interpretable, and cost-effective solution for personalized breast cancer diagnosis and treatment monitoring. Future extensions may include incorporating genomic signatures and applying the framework across multi-institutional datasets to further validate its robustness and generalizability.
Authors’ Contributions
All the authors contributed equally in this work. However, the individual roles of each author are given as follows: P.P.: Writing—original draft. K.K.A.: Data curation. J.A.: Data curation and visualization. S.G.: Formal analysis and writing—original draft. D.S.R.: Methodology and supervision. T.A.: Validation and writing—modified draft. A.V.: Methodology.
Footnotes
Author Disclosure Statement
None of the authors has any conflict of interest to disclose.
Funding Information
No funding is available to support this work.