
Abstract
Background:
Radiopharmaceuticals are being used more frequently to treat neuroendocrine tumors and advanced prostate cancer; however, their clinical application is associated with adverse drug reactions (ADRs) that may affect patient safety. Real-world data from spontaneous reporting systems such as the World Health Organization’s (WHO’s)-VigiAccess can aid in assessing safety after the drugs have been marketed.
Materials and Methods:
A retrospective descriptive analysis was conducted using ADR reports from the WHO-VigiAccess database up to November 2024. Reports related to lutetium (177Lu) dotatate (Lutathera®), lutetium (177Lu) vipivotide tetraxetan (Pluvicto®), and radium (223Ra) dichloride (Xofigo®) were extracted and analyzed with respect to patient demographics, geographic distribution, and ADRs classified by MedDRA System Organ Class and Preferred Terms. Descriptive statistics were used to compare safety profiles.
Results:
A total of 17,743 ADR reports were analyzed. Lutathera was predominantly associated with gastrointestinal disorders and skin or subcutaneous tissue reactions. In contrast, Pluvicto demonstrated a higher frequency of general systemic disorders and a disproportionately higher number of fatal outcomes, a finding consistent with its indication for the treatment of advanced prostate cancer. Xofigo was primarily linked to hematological and musculoskeletal toxicities. In addition to 169 ADRs that were common to all three agents, distinct drug-specific reaction patterns were also observed.
Conclusions:
WHO-VigiAccess data reveal clearly differentiated ADR profiles among Lutathera, Pluvicto, and Xofigo. These results highlight the necessity for individualized risk assessment, careful monitoring, and further prospective investigations to optimize the safe clinical application of radiopharmaceuticals.
Introduction
Neuroendocrine tumors (NETs) represent a heterogeneous group of malignant neoplasms that arise from neuroendocrine cells, which possess both neurological and endocrine functions and are capable of synthesizing and secreting hormones and other biologically active substances. NETs can occur in various anatomical locations throughout the body, including the gastrointestinal tract, pancreas, etc. 1 Prostate cancer is a malignant neoplasm originating from the epithelial cells of the prostate; however, in a minority of cases, it may also originate from neuroendocrine cells, particularly in advanced stages, where it is associated with a more aggressive biological phenotype.2,3 Despite significant advancement in diagnostic techniques and therapeutic strategies for both tumor types, the management of these malignancies in advanced or metastatic stages remains substantially challenging. Consequently, there remains an urgent imperative for the development of innovative therapeutic approaches aimed at improving patient prognosis.
Radiopharmaceuticals have emerged as a promising class of therapeutic agents for the treatment of various malignancies, including NETs and prostate cancer. These agents combine the targeting specificity of molecular imaging compounds with the cytotoxic effects of ionizing radiation, thereby enabling precise delivery of radiation to tumor cells while minimizing exposure to surrounding healthy tissue. 4 Despite their therapeutic potential, the clinical use of these radiopharmaceuticals is not without risk. Adverse drug reactions (ADRs) may occur, and a comprehensive understanding of their characteristics is essential for optimizing patient safety and treatment outcomes. For example, as documented in the literature, common ADRs associated with lutetium (177Lu) dotatate (Lutathera®), lutetium (177Lu) vipivotide tetraxetan (Pluvicto®), and radium (223Ra) dichloride (Xofigo®) include myelosuppression (e.g., leukopenia, anemia, and thrombocytopenia), nausea and vomiting, renal dysfunction, oral ulceration, and xerostomia.5–7 Nonetheless, with regular monitoring and the implementation of appropriate precautionary measures, the therapeutic benefits of these agents can be maximized while minimizing the incidence and severity of adverse effects.
Spontaneous reporting systems, despite inherent limitations, remain a critical tool for obtaining real-world data on the safety profiles of drugs and vaccines, enabling comparisons across different treatment regimens, and facilitating in-depth exploration of the underlying mechanisms of ADRs. Since their introduction in the 1960s, spontaneous reporting systems have served as a foundational component of post-marketing drug surveillance, with the primary objective of identifying previously undetected ADRs at the earliest possible stage. 8 In addition, spontaneous reports can provide valuable insights into novel associations between established drugs and known adverse reactions. 9 The World Health Organization’s (WHO’s)-VigiAccess database provides a valuable resource for accessing global data on drug-related ADRs, including those associated with radiopharmaceuticals. Systematic analysis of VigiAccess data enables a deeper and more comprehensive characterization and understanding of the safety profiles of Lutathera, Pluvicto, and Xofigo, facilitating identification of both shared and drug-specific ADRs patterns, and thereby informing evidence-based clinical decision-making.
Lutathera, Pluvicto, and Xofigo are three such radiopharmaceuticals, each developed to target specific receptors or biological pathways implicated in tumor progression. Lutathera is a radiopharmaceutical conjugated from the radionuclide 177Lu to the somatostatin analogue peptide 1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid-Tyr³-Octreotate (DOTA-Tyr³-Octreotate) (DOTA-TATE), which is mainly used for the treatment of refractory NETs, especially advanced gastrointestinal or pancreatic-derived tumors expressing growth inhibitory receptors (somatostatin receptors [SSTRs]). Pluvicto is an innovative nuclear drug of prostate-specific membrane antigen (PSMA)-617, a ligand of the radionuclide 177Lu combined with PSMA, which can specifically bind to PSMA for the targeted treatment of advanced PSMA-positive metastatic castration-resistant prostate cancer (mCRPC). Xofigo injures adjacent tumor cells by releasing high-energy α particles, which are osteotropic and are mostly used for the treatment of mCRPC with symptomatic bone metastases and no known visceral metastatic disease.
The present study describes and compares the ADR profiles of three commonly used radiopharmaceuticals—Lutathera, Pluvicto, and Xofigo—by interrogating the WHO-VigiAccess database. This comparative analysis provides clinicians with evidence-based guidance for safer and more effective therapeutic decision-making in the management of NETs and prostate cancer. Ultimately, this analysis will contribute to a broader understanding of the risk-benefit profiles associated with radiopharmaceutical therapy in routine clinical practice.
Materials and Methods
Drug profiles
Table 1 shows general information about the radiopharmaceuticals.
General Information for the Three Radiopharmaceuticals
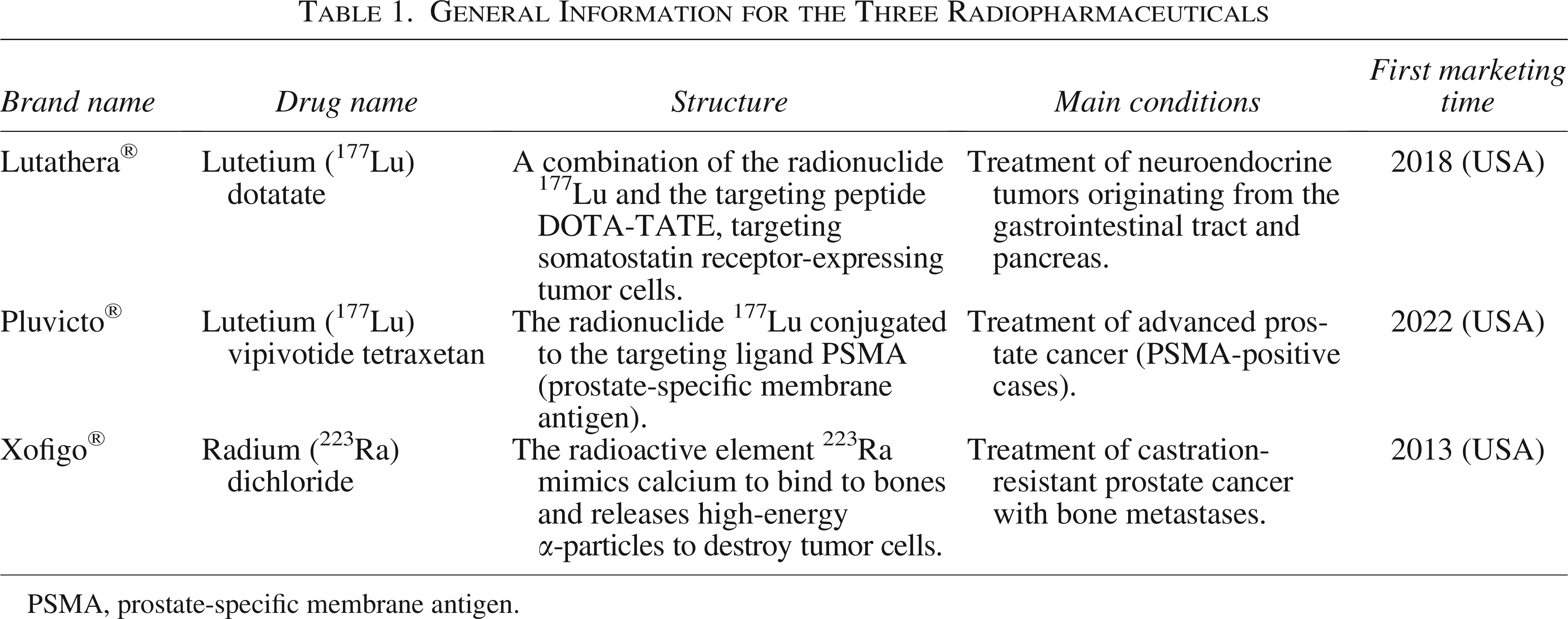
PSMA, prostate-specific membrane antigen.
Lutathera is a targeted radiopharmaceutical indicated for the treatment of advanced or metastatic NETs of gastrointestinal and pancreatic origin, in particular tumors expressing the growth-inhibitory receptor (SSTRs). This agent consists of the radionuclide 177Lu conjugated to the somatostatin analog peptide DOTA-TATE, which binds with high affinity to SSTRs overexpressed on the surface of tumor cells. Following receptor-mediated internalization, it subsequently delivers cytotoxic beta-radiation locally, thereby inducing tumor cell death while minimizing exposure to surrounding healthy tissue.10,11 Lutathera is approved for adult patients with unresectable or metastatic gastroenteropancreatic NETs.
Pluvicto, also known as 177Lu-PSMA-617, is an innovative radioligand-based therapeutic drug for the treatment of patients with advanced PSMA-positive mCRPC. Pluvicto combines the radionuclide 177Lu conjugated to the PSMA-targeted ligand PSMA-617, which binds with high specificity to PSMA, a transmembrane protein substantially overexpressed on prostate cancer cells. Upon binding, Pluvicto delivers targeted beta-radiation directly to the cancer cells, resulting in DNA damage and cell death, while sparing nonmalignant tissue.12,13
Xofigo is a targeted alpha-emitting radiopharmaceutical indicated for the treatment of patients with mCRPC with symptomatic bone metastases and no known visceral metastatic disease. As a calcium mimetic, Ra-223 selectively binds to areas of increased bone turnover, such as those associated with osteoblastic bone metastases. The high-energy alpha particles emitted by Ra-223 induce predominantly double-strand DNA breaks in adjacent tumor cells, resulting in potent cytotoxic effects. Due to the short path length of alpha radiation (less than 100 micrometers), damage to surrounding healthy tissue, particularly bone marrow, is substantially limited.14,15 In addition to delaying disease progression, Xofigo has been shown to reduce the incidence of symptomatic skeletal events (e.g., bone pain and pathological fractures) and improve quality of life in the indicated patient population.
Data sources
ADRs data for the three radiopharmaceuticals of interest were extracted from the WHO-VigiAccess database on November 5 2024. VigiAccess is a publicly accessible online platform (https://www.vigiaccess.org) maintained by the Uppsala Monitoring Center on behalf of the WHO. The platform collects and aggregates global data by WHO-VigiAccess, individual case safety reports (ICRS) contained within VigiBase, age, gender, year, and region, to access these drug safety records using the free Program for International Drug Monitoring (PIDM) database portal, WHO-VigiAccess, a publicly available resource providing statistical presentations of the VigiBase database. Since its establishment in 1968, VigiBase has documented reports submitted by the national pharmacovigilance centers participating in the WHO-PIDM of PIDM. ICRS reports are typically submitted by other countries, mainly by health care professionals, patients, and pharmaceutical manufacturers, to their respective national regulatory authorities, where they undergo preliminary review and assessment prior to being uploaded to VigiBase in aggregate format. 16
Report definitions are based on the Preferred Terminology (PT) and System Organ Classification (SOC) of the International Medical Dictionary for Regulatory Activities (MedDRA). To characterize the toxicity profile, data are obtained by drug classification with 27 categories, and each specific adverse event is identified by the recorded MedDRA SOC and PT levels. MedDRA’s sources of reporting terminology are from various dictionaries, including the WHO Adverse Reaction Terminology. 17 For the purposes of this study, drug-specific search strategies were constructed using generic drug names to identify all reports associated with Lutathera, Pluvicto, and Xofigo. Individual SOC and PT categories were then extracted to characterize search formulas and screen for relevant active ingredients to obtain target data. 18
Statistical analysis
This study employed a retrospective, descriptive design to characterize and compare the ADR profiles of the three selected radiopharmaceuticals. Data processing and descriptive analyses were performed using Microsoft Excel. The ADR reporting rate for each drug was calculated as the number of reports listing that ADR symptoms divided by the total number of reports for the drug. Common ADRs were defined as the top 20 symptoms with the reporting rate for each agent. Descriptive statistics, including frequencies and percentages, were used to summarize, calculate, and analyze the distribution of ADRs across SOC categories and to facilitate cross-drug comparisons.
Results
ADR reporting characteristics of the three radiopharmaceuticals
According to the WHO-VigiAccess database, the first reports of ADRs for Lutathera, Pluvicto, and Xofigo were received in 2014, 2017, and 2010, respectively. As of 2024, the WHO has received a total of 5,058 ADRs for Lutathera, 7,728 for Pluvicto, and 4,957 for Xofigo, cumulatively representing 17,743 individual case safety reports. Within these reports, the specific number of adverse event symptoms recorded was 10,086 for Lutathera, 11,532 for Pluvicto and 11,378 for Xofigo.
In the three radiopharmaceuticals, there were a total of 9804 reports of unspecified gender, excluding these unspecified gender reports, the number of male patients suffering from ADRs (n = 6, 891) was significantly greater than that of female patients (n = 1, 051). This disparity was especially pronounced for Pluvicto and Xofigo, where reports involving female patients were exceedingly rare. This gender difference is due to the fact that these drugs are mostly used for the treatment of prostate cancer. Excluding reports of unknown age, Lutathera demonstrated the highest proportion of reports in the 45–64 age group (9%), while Pluvicto and Xofigo had the highest reporting rates in the > 75 years age group (4% and 23%, respectively). Geographically, the vast majority of ADR reports originated from the Americas and Europe, while reports from Africa were rare or absent. The details are shown in Table 2.
Characteristics of ADR Reports in the Three Radiopharmaceuticals
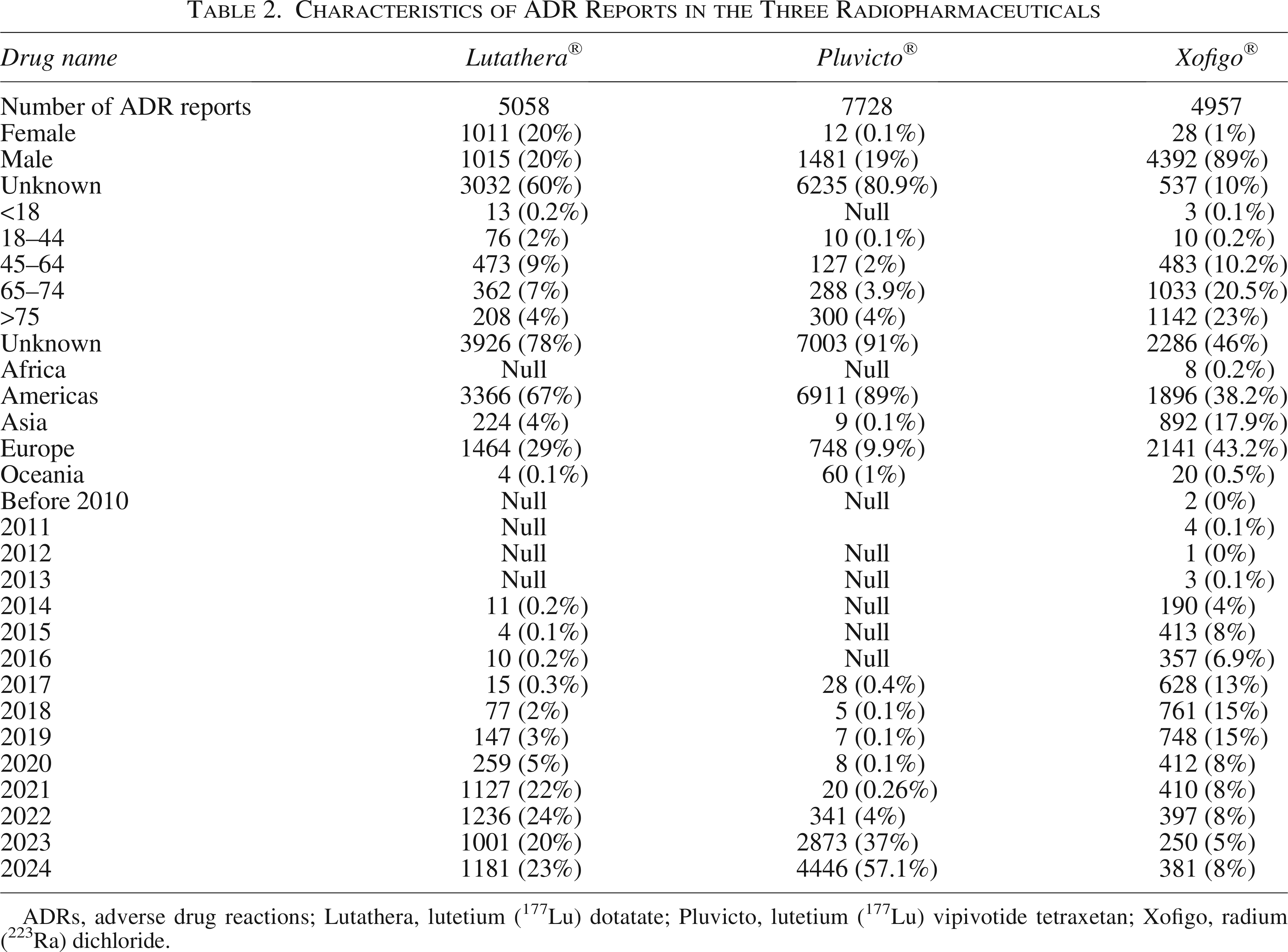
ADRs, adverse drug reactions; Lutathera, lutetium (177Lu) dotatate; Pluvicto, lutetium (177Lu) vipivotide tetraxetan; Xofigo, radium (223Ra) dichloride.
Distribution of the 20 SOCs in the three radiopharmaceuticals
Figure 1 and Supplementary Table S1 show the reporting rates of 20 SOCs for the three radiopharmaceuticals. The ADR reporting rates of gastrointestinal disorders, blood and lymphatic system disorders, benign neoplasms, malignant and unspecified (including cysts and polyps) were high (>10%) in all three radiopharmaceuticals and can be considered as common.
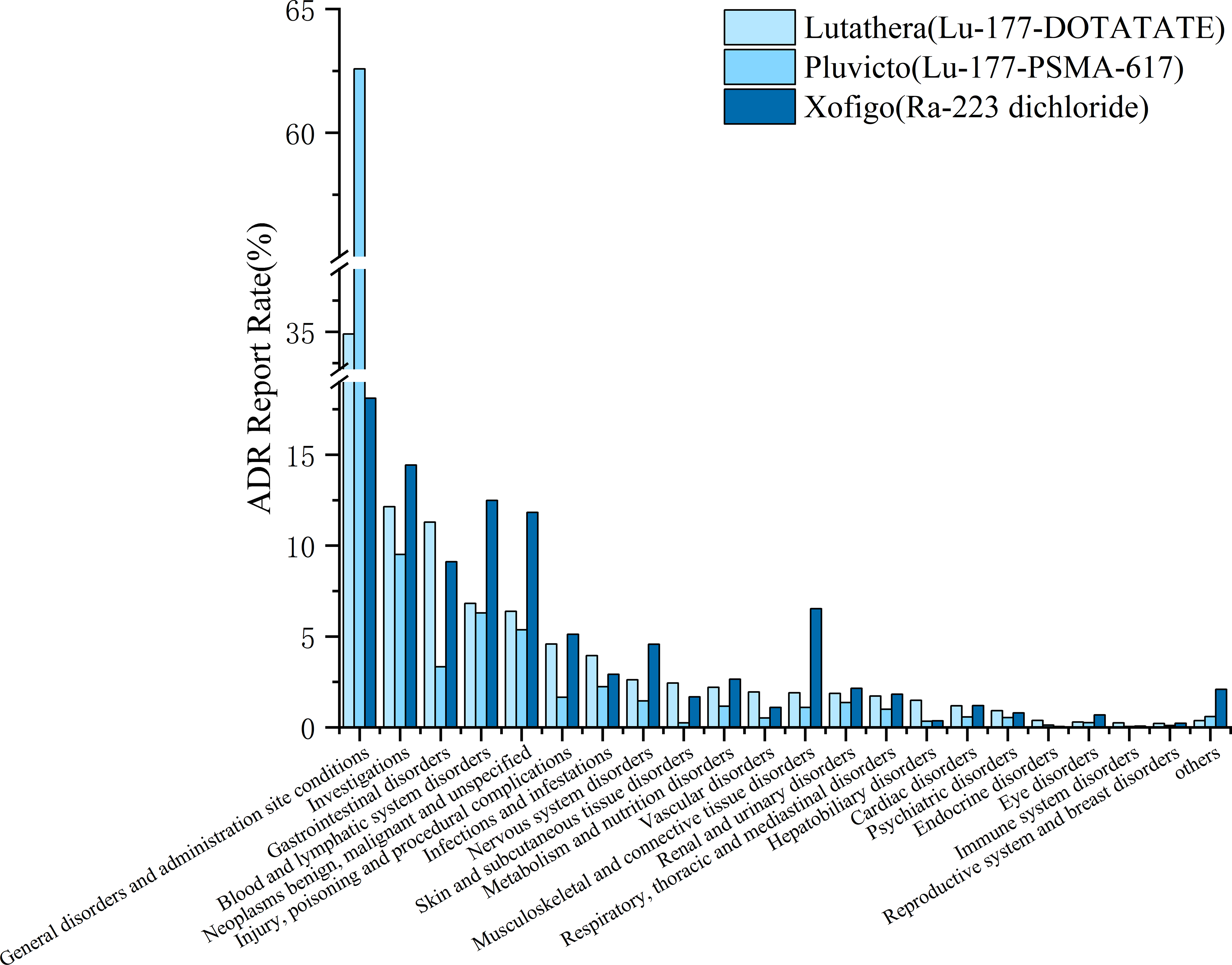
Reporting rate of ADRs for 27 SOCs in the three radiopharmaceuticals. ADRs, adverse drug reactions; SOCs, System Organ Classifications.
At the same time, the distinct inter-drug differences were observed across SOC categories. Lutathera demonstrated a significantly higher ADR reporting rate than the remaining two radiopharmaceuticals in gastrointestinal disorders, skin and subcutaneous tissue disorders, blood and lymphatic system disorders, benign neoplasms, malignant disorders, and other disorders. Benign neoplasms, malignant, and unspecified (including cysts and polyps) had significantly lower ADR reporting rates than the other two agents. Pluvicto was associated with significantly lower ADR reporting rates relative to Lutathera and Xofigo, including poisoning and procedural complications, skin and subcutaneous tissue disorders. In contrast, Xofigo demonstrated in Musculoskeletal and connective tissue disorders compared with Lutathera and Pluvicto; however, the ADR reporting rate of Xofigo in infestations and infections was significantly lower than that of the other two radiopharmaceuticals.
The top five frequently reported adverse event types across the three radiopharmaceuticals were General disorders and administration site conditions (n = 12, 783 cases), investigations (n = 3, 992 cases), blood and lymphatic system disorders (n = 2, 832 cases), benign neoplasms, malignant and unspecified (including cysts and polyps) (n = 2, 605 cases), and Gastrointestinal disorders (n = 2, 558 cases).
The most common ADRs in the three radiopharmaceuticals
Table 3 lists the 20 most frequently occurring ADRs for the three radiopharmaceuticals, categorized according to MedDRA PTs within each SOC. Among these, the five most common ADRs reported for Lutathera were ill-defined disorder, general physical health deterioration, death, nausea, and thrombocytopenia. For Pluvicto, the top five ADRs were ill-defined disorder, general physical health deterioration, death, anemia, and malignant neoplasm progression. In the case of Xofigo, the most frequently reported ADRs were anemia, prostate-specific antigen increase, thrombocytopenia, hemoglobin decrease, and nausea. It is noteworthy that the overall ADR reporting rate for Xofigo was lower than observed for Lutathera and Pluvicto.
The Report Rate of Top 20 ADRs in the Three Radiopharmaceuticals (%)
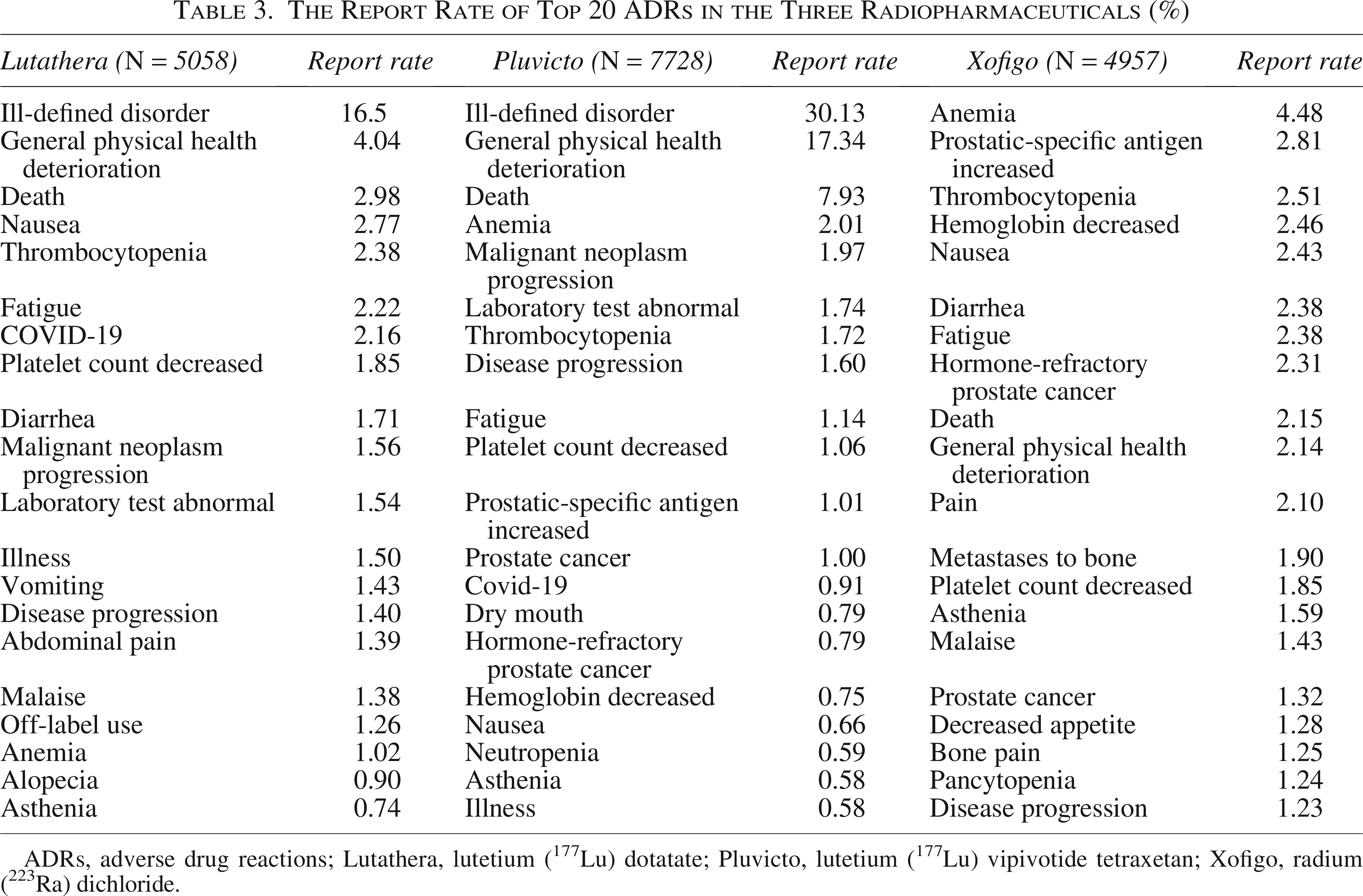
ADRs, adverse drug reactions; Lutathera, lutetium (177Lu) dotatate; Pluvicto, lutetium (177Lu) vipivotide tetraxetan; Xofigo, radium (223Ra) dichloride.
Similarities and differences between common ADRs in three radiopharmaceuticals
Figure 2 and Supplementary Table S2 illustrate the commonality of the most frequently ADRs for Lutathera, Pluvicto, and Xofigo. By comparing the top 20 ADRs for each agent in the SOC, a total of 169 common ADRs were identified, that is, ADRs reported for all three radiopharmaceuticals. The three SOCs with the highest number of ADRs were renal and urinary disorders, general disorders and administration site conditions, and blood and lymphatic system disorders.
ADRs in different systems among the three radiopharmaceuticals. ADRs, adverse drug reactions.
Different ADRs among three radiopharmaceuticals
It presents the differences between the three radiopharmaceutical ADRs in Table 4. Lutathera has a wide range of unique ADRs covering a variety of systems including hematological, cardiac, endocrine, and gastrointestinal, such as bone marrow infiltration, carcinoid heart disease, and carcinoid syndrome. Laboratory investigations also revealed changes in several biomarkers such as weight gain and a decrease in blood creatinine. Pluvicto is associated with fewer distinctive adverse reactions, predominantly affecting the eye (xerophthalmia), the gastrointestinal tract (stomatitis, xerostomia), and manifesting as prostate-specific antigen abnormalities upon examination. Xofigo is associated with a higher incidence of unique ADRs including ventricular tachycardia among cardiac disorders, glaucoma in conditions, as well as a diverse range of infections and injury-related responses. Notably, significant alterations are observed in test markers, such as an elevated level of C-reactive protein and increased blood pressure.
Different ADRs Among Three Radiopharmaceuticals
ADRs, adverse drug reactions; Lutathera, lutetium (177Lu) dotatate; Pluvicto, lutetium (177Lu) vipivotide tetraxetan; Xofigo, radium (223Ra) dichloride.
Discussion
Due to the inherent limitations of clinical trials, such as stringent inclusion criteria, small sample sizes, and relatively short follow-up periods, the spontaneous reporting system (SRS), which is an indispensable tool, has been widely used in pharmacovigilance to assess the safety of suspected adverse events. These systems are essential for the early identification of signals. 19 Currently, the majority of drug safety signals detection studies leverage data from three major international databases: WHO-VigiBase, the U.S. FDA and Drug Administration Adverse Event Reporting System, and the European Medicines Agency’s EudraVigilance Data Analysis System; 20 however, the WHO-VigiBase has a more comprehensive range of information and a larger sample size. These databases collectively provide an invaluable data resource for global drug safety monitoring, facilitating the early detection of potential drug safety problems, as well as their assessment and analysis.
With the launch of the publicly accessible WHO-VigiAccess platform in 2015, the WHO sought to make information from its global individual case safety ADR database, as VigiBase, available to the general public. Data mining has uncovered several known clinical associations and previously undetected adverse drug events within the WHO-VigiAccess database. While the database supports searches by a drug’s proprietary or brand name, it identifies the active ingredient contained within and presents the results of its adverse drug reaction (ADR) reports based on that active ingredient. This functionality offers researchers, clinicians, and healthcare professionals a valuable resource for obtaining detailed, real-world information on drug safety. Our findings reveal characteristic differences in the ADR profiles of three radiopharmaceuticals—Lutathera, Pluvicto, and Xofigo. These observed disparities are likely attributable to differences in the drugs’ respective molecular structures, mechanisms of action, and target receptor specificities.
Regarding the gender distribution of reported ADRs, Lutathera demonstrated approximately equal reporting rates between men and women patients, whereas Pluvicto and Xofigo exhibited a markedly higher proportion of reports among male patients, a finding consistent with that Pluvicto and Xofigo, their primary indications for the treatment of prostate cancer and bone metastases in the prostate. PSMA, the molecular target of Pluvicto, is a transmembrane glycoprotein expressed in a variety of solid tumors beyond prostate cancer, including certain cancers specific to women. For example, PSMA expression has been documented in the tumor-associated neovasculature of breast, kidney, and lung cancers, rather than on the tumor cells themselves.21–23 Thus, while PSMA is well established as a diagnostic and therapeutic target for prostate cancer, it may also represent a potential therapeutic target for other malignancies. This suggests that female patients may potentially receive Pluvicto for non-prostate cancer indications. Similarly, although Xofigo is primarily indicated for prostate cancer with bone metastases, its therapeutic application is not inherently limited to male-specific cancers. In fact, Xofigo has also been investigated for the treatment of other malignancies, including certain female-specific cancers.24,25 For example, one study showed that 223Ra may be able to be combined with other agents to treat breast cancer bone metastases. 26
With respect to organ-specific toxicity profiles, Lutathera was associated with significantly more commonly reported in the SOC for gastrointestinal disorders (11.29%) and skin and subcutaneous tissue disorders (2.44%) this finding may be attributable to its targeting of SSTRs, which are known to influence gastrointestinal motility and cutaneous metabolism,27,28 The frequent reporting of “ill-specified disorder” (16.5%) and “general physical health deterioration” (4.04%) for Lutathera likely reflects systemic radiation distribution and multiorgan involvement associated with peptide receptor radionuclide therapy.
The prominence of Pluvicto with the high reporting rate of “systemic disorders and administration site conditions” (62.58%) and “malignant neoplasm progression” (1.97%) may be related to its property of targeting PSMA. Despite the high precision, patients with advanced prostate cancer may be confounded by the underlying advanced disease state of patients with metastatic castration-resistant prostate cancer, potentially obscuring drug-specific toxicity signals. 5 Of particular concern is the substantially elevated reporting rate of death for Pluvicto (7.93%), which is alarming and may be related to the advanced clinical status of the treated patients, cumulative drug-overlay toxicity, or alterations in the tumor immune microenvironment. Conversely, Pluvicto exhibited a low dermal toxicity (0.25%) which reflects the precision of PSMA targeting, while, the high incidence of Xofigo in the musculoskeletal (6.53%) and hematological (12.48%) systems is related to its alpha-radiation targeting of bone metastases, which may be associated with adverse effects through myelosuppression and disruption of the bone microenvironment, “anemia”, and “death”. The high incidence of “anemia” (4.48%) and “thrombocytopenia” (2.51%), is associated with direct damage to bone marrow hematopoietic stem cells by α-particles, while “bone pain” (1.25%) may stem from an imbalance in bone reconstruction following radionuclide therapy. 29
A fundamental distinction among three radiopharmaceuticals lies in the physical characteristics of the emitted particles and their radiobiological consequences. Lutathera and Pluvicto are β-particle emitters based on 177Lu, whereas Xofigo contains Radium-223, an α-particle nuclide. The longer tissue penetration range and lower linear energy transfer (LET) of β-particles enable a cross-fire effect that helps cover heterogeneous receptor expression within tumor tissue, although this can also increase exposure of surrounding normal tissues to irradiation.30–32
In contrast, α-particles have a very short path length (typically < 100 μm) and high LET, leading to dense ionization tracks and complex double-strand DNA breaks, which contribute to high relative biological effectiveness and potent cytotoxicity even at low particle counts.32,33 Recent radiobiological studies emphasize that the concentrated energy deposition of α-particles can overcome radioresistance mechanisms more effectively than low-LET ray. 33 Because Radium-223 deposits preferentially at sites of increased bone turnover, adjacent hematopoietic niches may receive significant localized irradiation, consistent with the concentrated hematological toxicities observed in clinical practice.33,34 Together, these differences highlight an intrinsic trade-off in radiotherapeutic design: β-emitting agents provide broader spatial coverage that may be suitable for systemic disease but with diffuse toxicity, whereas α-emitting agents deliver highly localized, high-potency cytotoxic effects with a risk of compartment-specific marrow toxicity. Integrating contemporary radiobiological insights from both α- and β-emitter therapies enables a mechanistic interpretation of observed adverse reaction patterns beyond descriptive comparison.
Radiopharmaceuticals differ not only in radiation type but also fundamentally in their targeting strategies, which substantially influence biodistribution, therapeutic scope, and toxicity profiles. Peptide receptor–targeted therapies, such as 177Lu-DOTATATE for neuroendocrine tumors and Pluvicto for metastatic castration-resistant prostate cancer (mCRPC), rely on selective binding to tumor-associated surface receptors. This strategy enables systemic delivery of radiation to receptor-expressing lesions throughout the body and has demonstrated significant clinical benefit in advanced disease. However, because these receptors are not entirely tumor-exclusive, physiological expression in normal tissues—such as renal tubular cells, salivary glands, and bone marrow—may lead to off-target radiation exposure. Consequently, the most frequently reported adverse events include hematological suppression, xerostomia, nausea, and fatigue, although severe organ toxicity remains relatively uncommon with appropriate patient selection and renal protection protocols.11,35
In contrast, metabolic bone-seeking radiopharmaceuticals such as 223Ra dichloride do not depend on receptor expression but instead exploit physiological bone remodeling processes. As a calcium mimetic, 223Ra selectively localizes to areas of increased osteoblastic activity characteristic of bone metastases, where it emits high-LET α-particles within a very short path length. This results in highly localized cytotoxicity within the bone microenvironment and has been shown to improve overall survival and reduce skeletal-related events in patients with mCRPC and predominant bone involvement. Nevertheless, because accumulation is confined to regions of active bone turnover, 223Ra has limited activity against visceral or soft-tissue metastases. Its toxicity profile is therefore primarily hematological, reflecting irradiation of adjacent bone marrow niches rather than receptor-mediated off-target organ exposure. 5
Taken together, peptide receptor targeting provides broader systemic applicability for receptor-positive disease but carries potential off-target effects related to physiological receptor distribution, whereas metabolic bone-seeking therapy offers highly localized skeletal targeting with limited extraosseous efficacy. These mechanistic distinctions may partly explain the divergent adverse reaction patterns observed in spontaneous pharmacovigilance databases and should be considered when interpreting comparative safety signals. In addition, exploring combination treatment strategies, such as the use of bone marrow protectors and some anti-inflammatory agents, such as curcumin, may help to enhance the safety of radiopharmaceuticals.36,37 From a clinical perspective, these differentiated safety patterns imply that radiopharmaceutical selection should be individualized not only based on receptor expression or disease distribution, but also on baseline organ reserve and comorbidity profile. Patients with limited marrow reserve or extensive prior chemotherapy exposure may require careful hematological monitoring when treated with α-emitting agents, such as Xofigo. Conversely, for patients with diffuse receptor-positive disease and preserved organ function, β-emitting peptide-based therapies may offer broader systemic tumor coverage with relatively diffuse but manageable toxicity.
Importantly, spontaneous reporting databases cannot establish causality or incidence rates. However, they can highlight real-world toxicity clustering that complements controlled-trial evidence. Integrating pharmacovigilance data with randomized clinical trial outcomes may therefore provide a more complete understanding of therapeutic positioning in advanced malignancy. Although this study provides important insights into the safety profile of the three radiopharmaceuticals investigated, several limitations should be acknowledged. First, those data were derived from an SRS, which is subject to inherent shortcomings that may lead to reporting bias, such as underreporting, overreliance on serious event reporting, and differences in reporting practices and regulatory standards in different regions. 38 Second, the retrospective nature of this analysis cannot clarify the establishment of a causal relationship between agents and their reactions, only suggesting potential safety signals that need to be validated by further experimental or prospective cohort studies. In addition, the absence of detailed baseline patient characteristics (such as comorbidities, coadministration) and treatment details (e.g., dosage, regimen) in the individual case reports may confound the attribution analysis of observed ADRs to specific drugs. For example, the high mortality rate associated with Pluvicto may be partly attributable to the poor prognosis inherent to the advanced-stage patient population for whom this therapy is indicated, rather than representing direct drug toxicity alone. Finally, the inherent breadth of the SOC classification may obscure the finer, organ-specific toxicity profile. For example, “systemic disorders” covers a heterogeneous range of symptoms and needs for comprehensive analysis, deeply at the specific PT terminology, to achieve a more granular understanding of agents’ safety. 39 To comprehensively evaluate the risk-benefit profile of radiopharmaceuticals, future endeavors should encompass multi-center cohort studies, in-depth exploration of molecular mechanisms, and the implementation of standardized data collection methodologies.
Conclusion
This study systematically analyzed the ADR profiles of three radiopharmaceuticals—Lutathera, Pluvicto, and Xofigo—based on the WHO-VigiAccess database. The results revealed that there were significant differences in the ADR profiles among the three agents: Lutathera was characterized by prominent gastrointestinal and dermatological toxicity; Pluvicto exhibited a predominance of general systemic disorders and a notably higher mortality reporting rate, while Xofigo was associated predominantly with hematological and bone-related toxicities. These differences may be closely related to the drug’s mechanism of action (e.g., receptor targeting specificity and radiation type) and the clinical characteristics of the treated population (e.g., patients with advanced prostate cancer). In addition, the observed gender and age distribution characteristics further corroborate the association between drug indications and patient demographics. Notwithstanding the inherent limitations of the spontaneous reporting system, such as underreporting, reporting bias, and limited capacity for causal inference, this study provides valuable insights to inform the optimization of the three clinical radiopharmaceuticals, such as the implementation of preventive management strategies for high-risk ADRs and individualized dose adjustments, particularly for elderly patients. In the future, it is necessary to combine multicenter prospective studies, molecular imaging techniques, and dynamic monitoring of biomarkers to explore the mechanisms of radiopharmaceutical-induced toxicities in depth. Additionally, the development of combination treatment strategies may offer further opportunities to enhance therapeutic safety while maintaining efficacy. Overall, radiopharmaceuticals demonstrate remarkable potential for precision cancer therapy; however, achieving an optimal risk-benefit balance will require continued long-term follow-up and multidimensional evaluation in real-world clinical settings.
Authors’ Contributions
Y.J. wrote and submitted the article. Y.J., K.G., and K.C. collected and analyzed data, drew figure and wrote manuscript. Y.J. and X.Wang were responsible for the critical revision of the article. X.Wan and S.Q. provided ideas, participated in the coordination of the study, and reviewed the article. All the authors reviewed and edited the article before submission.
Footnotes
Acknowledgments
The authors acknowledge the editors and reviewers for their helpful comments on this article. Thanks to the Figdraw platform for drawing all the graphics in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Disclosure Statement
All authors declare no competing interests.
Funding Information
This work was funded by the National Natural Science Foundation of China (82103774), Wenzhou Major Science and Technology Innovation Research Program (ZY2022003), and Scientific Research Project of Wenzhou Medical University (wyx2024101039). The authors appreciate the open project of South Zhejiang Institute of Radiation Medicine and Nuclear Technology (ZFY2023-003).
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.