
Abstract
Background:
Type 5 insular and paralimbic gliomas are surgically challenging because resection is limited by perforator-rich vascular anatomy and eloquent subcortical pathways, often leaving clinically relevant residual disease. We evaluated a precision-oncology workflow integrating multimodal preoperative planning, transsylvian microneurosurgical resection, and postoperative radionuclide-oriented stratification.
Methods:
This retrospective study included 38 adults with type 5 insular and paralimbic gliomas treated through a transsylvian approach. Structural magnetic resonance imaging (MRI), T2/fluid-attenuated inversion recovery imaging, diffusion tensor tractography, and vascular mapping were integrated to define operative corridors and safety boundaries. Early postoperative MRI was used to assess extent of resection, neurologic outcome, and residual-disease category, which was then linked to standard follow-up, radionuclide-oriented reassessment, or targeted radionuclide therapy candidacy.
Results:
Gross total resection was achieved in 72% of patients, subtotal resection in 21%, and partial resection in 7%. No new neurologic deficit occurred in 80% of patients, transient deficits in 15%, and permanent deficits in 5%, yielding a neurologic preservation rate of 95%. Residual disease was categorized as no significant residual in 55%, surgically constrained residual in 30%, and biologically high-risk residual in 15%.
Conclusions:
This integrated workflow achieved high rates of maximal safe resection and neurologic preservation while providing a structured postoperative framework for biologically informed residual-disease assessment, radionuclide-oriented reassessment, and targeted radionuclide therapy candidate selection in surgically complex gliomas.
Keywords
Introduction
Type 5 insular gliomas with paralimbic extension are one of the most technically challenging objects in neuro-oncologic surgery due to the limited exposure and excision of the tumor by the opercular envelope, middle cerebral artery branches, and the lenticulostriate perforators as well as the proximity of the lesion to the internal capsule and eloquent subcortical association pathways. In the classical anatomical model, these tumors may reach outside of the insular compartment into the related paralimbic areas, raising the risk of vascularity, and the chances of clinically significant residual disease after maximal safe resection.1,2 Consequently, a delicate balance must be achieved between oncologic and neurologic sparing in surgical management.
Complete resection, when safe, is a paramount concept in the management of glioma, but structural magnetic resonance imaging (MRI) may underestimate infiltrative margins and not be fully discriminating of the position of the tract or vascular limitations within deep insular compartments.3,4 Modern insular glioma surgery is thus becoming more dependent on multimodal preoperative imaging that combines structural MRI and T2/fluid-attenuated inversion recovery (FLAIR) imaging assessing infiltrative extent and diffusion tensor imaging (DTI) tractography to map out the operative corridors and high-risk margins.5–7 This combined approach is especially relevant in the case of type 5 lesions, where the limit of medial resection is frequently not determined by the visibility of tumors but by the preservation of perforator-rich vascular and deep, functional anatomy. It has demonstrated that preservation of lenticulostriate arteries and careful dissection of the sylvian fissure are key predictors of postoperative neurologic outcome, particularly when the resection approaches the medial boundary.8,9
In this situation, the transsylvian microneurosurgical pathway offers a logical operative pathway to the selected type 5 insular and paralimbic glioma since it allows the visualization of M2 branches, perforators, and deep vascular interface as well as facilitating the controlled debulking of tumors.10,11 Surgical resection of the tumor with meticulous technique can result in residual tumor in surgically restricted areas near major vessels or eloquent subcortical pathways. This constraint underscores the necessity of a postoperative paradigm that goes beyond a two-pole dichotomy of gross total versus incomplete resection and integrates residual-disease stratification into the individualized management. 12 We tested an integrated workflow with multimodal preoperative planning and transsylvian microsurgery with boundaries and postoperative precision stratification of patients with type 5 insular and paralimbic gliomas (Fig. 1) in this work.
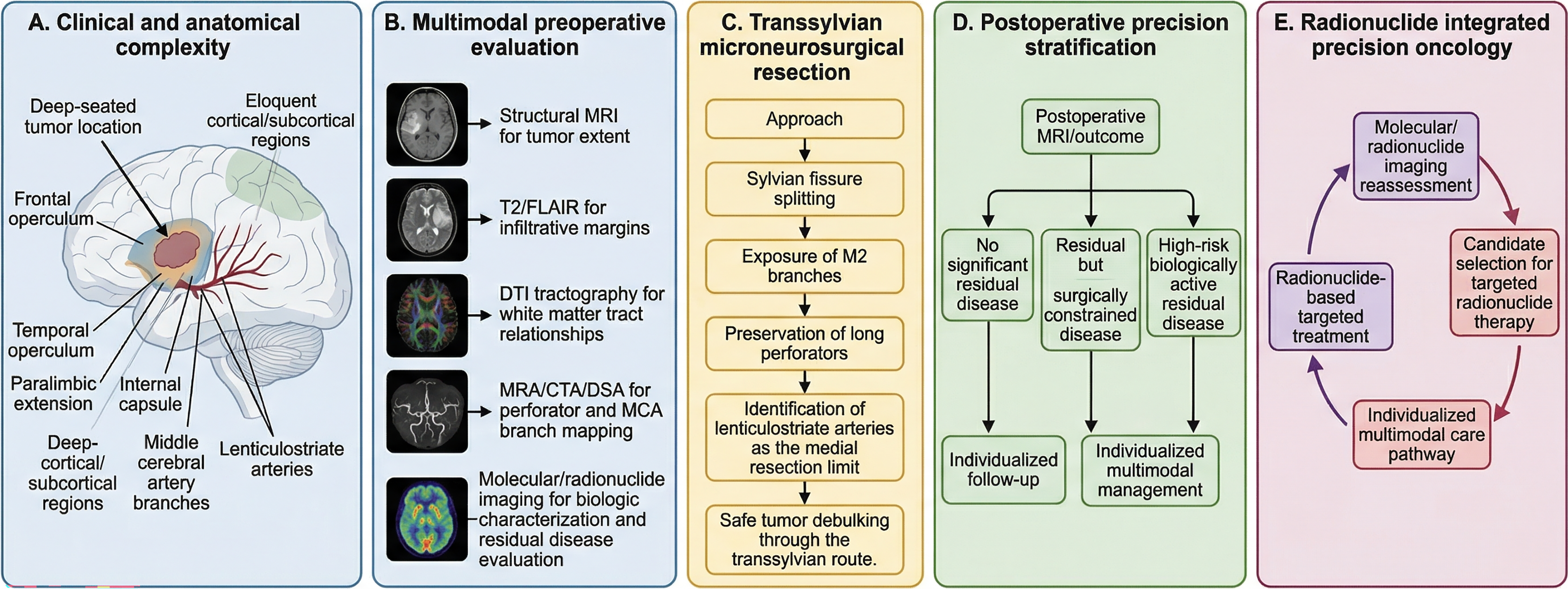
Precision-oncology workflow for radionuclide therapy integrated multimodal management of type 5 insular and paralimbic gliomas.
Materials and Methods
Ethics and oversight
This study was approved by the Ethics Committee of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou (No. [2021]714). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Study design, cohort, and eligibility
We retrospectively reviewed a consecutive cohort of 38 adult patients with surgically treated type 5 insular and paralimbic gliomas. This cohort should be interpreted as a selected surgical series of anatomically complex type 5 insular and paralimbic gliomas rather than as a representative sample of all insular gliomas or diffuse gliomas. Patients without transsylvian surgical treatment, without adequate multimodal preoperative imaging, or without early postoperative MRI were not included, which limits generalizability to broader disease presentations. Eligible patients met the following criteria: (1) radiographic and intraoperative findings consistent with a deep insular tumor with paralimbic extension; (2) microsurgical resection performed through a transsylvian corridor with the intent of maximal safe resection; and (3) availability of both preoperative multimodal imaging and early postoperative MRI for assessment of extent of resection and residual disease. All patients were managed within a unified precision-oncology framework linking preoperative planning, intraoperative boundary control, and postoperative stratified management.
Multimodal preoperative imaging and precision-planning map
Preoperative imaging included structural MRI to define tumor extent and T2/FLAIR sequences to characterize infiltrative margins and their relationships to deep structures (Fig. 2). FLAIR-defined infiltrative margins were used to expand the preoperative risk map beyond the contrast-enhancing or structurally visible tumor core, particularly near the internal capsule and deep subcortical interface. In final boundary selection, these margins supported planned debulking when they remained within the safe corridor, but they were converted into likely residual-risk zones when they approached lenticulostriate arteries, critical perforators, or preserved tract interfaces. DTI tractography was used to assess tumor relationships with major white matter pathways and to distinguish tract displacement or compression from regions in which preserved pathways could define functional resection boundaries. When DTI demonstrated tract displacement away from the sylvian operative corridor, the planned transsylvian route was maintained. When tract compression or preservation was located along the anticipated deep or posterior interface, the corridor trajectory and debulking direction were adjusted to avoid traction across the tract-risk zone, and the tract interface was treated as a functional stop boundary. Vascular mapping was performed using MRA, CTA, or DSA, according to clinical indication, to delineate M2 branching anatomy and the anticipated perforator-rich medial boundary, including the lenticulostriate artery territory. These datasets were integrated into a qualitative precision-planning map defining a safe operative corridor, a no-go vascular zone, a tract-risk zone, a likely residual-risk zone, and a biologically active target zone. For each patient, the planning map was constructed using a standardized sequence: first, structural MRI defined the tumor core and anatomical extent; second, T2/FLAIR imaging identified infiltrative margins; third, DTI tractography classified adjacent white matter pathways as displaced, compressed, or preserved; fourth, vascular imaging delineated M2 branches, perforators, and the lenticulostriate artery territory; and fifth, these layers were reviewed together to assign corridor, vascular-risk, tract-risk, likely residual-risk, and biologically active target zones. When imaging signals were discordant, planning decisions were resolved using a predefined safety-priority hierarchy. Vascular no-go anatomy, especially lenticulostriate arteries and critical M2/perforator relationships, was assigned the highest priority, followed by preserved or compressed eloquent white matter tracts on DTI tractography, FLAIR-defined infiltrative margins, and contrast-enhancing tumor burden. Therefore, MRI-defined tumor extent did not independently determine the resection boundary when it overlapped with vascular or tract-risk zones. Because deep insular and subcortical anatomy may be affected by edema, tract displacement, vessel compression, and image-registration uncertainty, all imaging-defined boundaries were treated as planning estimates rather than absolute intraoperative determinants. Final boundary selection was therefore confirmed against real-time microsurgical anatomy and functional safety considerations. This map was used to guide operative route selection and to anticipate areas in which residual tumor might be intentionally preserved because of vascular or functional constraints. When risk zones overlapped, the highest-risk category determined the operative decision. No-go vascular zones superseded tract-risk zones, tract-risk zones superseded FLAIR-defined infiltrative margins, and biologically active target zones were pursued only when they remained outside vascular or functional stop boundaries. Overlapping risk therefore favored preservation and planned residual classification rather than aggressive resection.
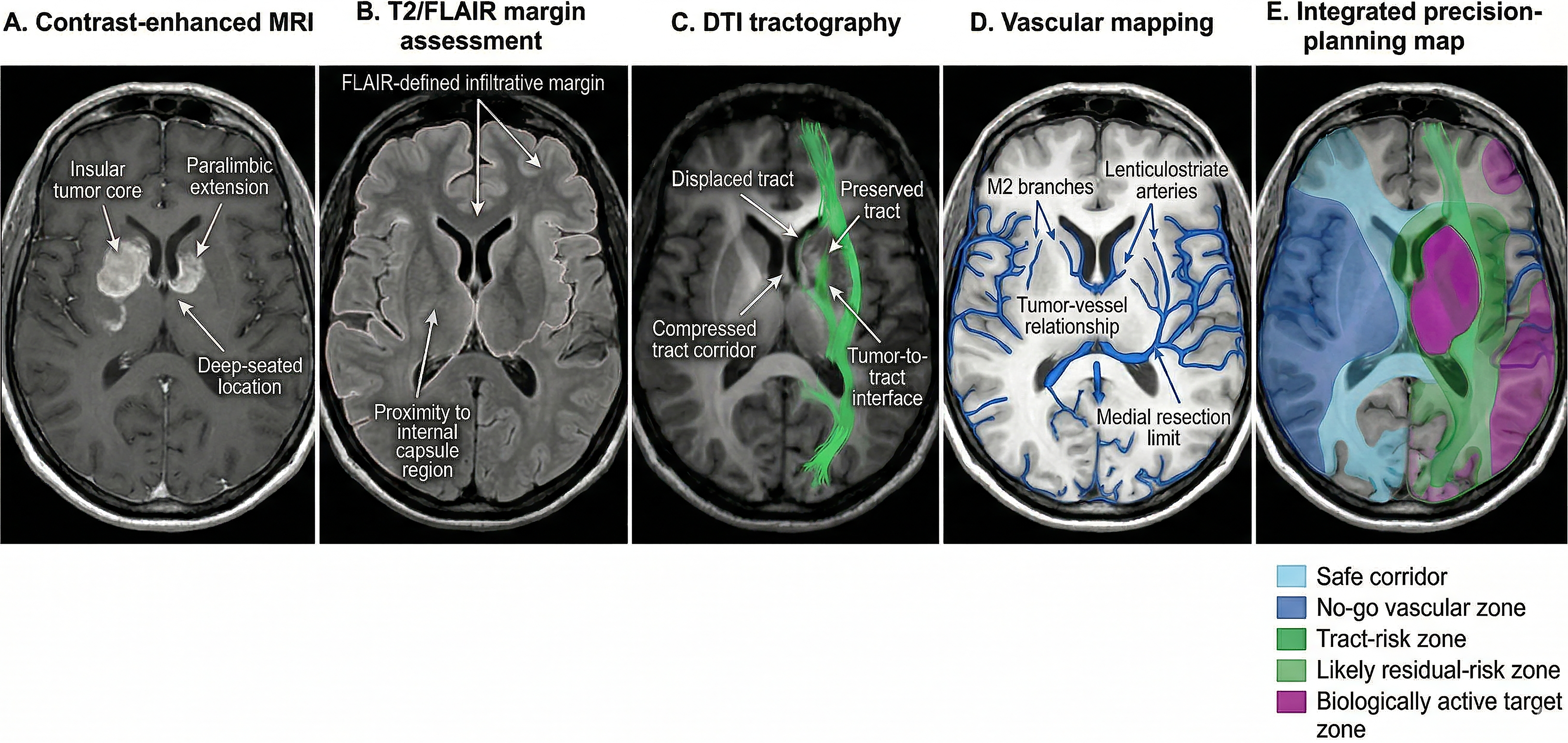
Representative multimodal preoperative imaging for precision planning in type 5 insular and paralimbic gliomas.
Operative strategy: transsylvian microneurosurgical resection
A standardized transsylvian microsurgical approach was used in all cases. After frontotemporal exposure, the sylvian fissure was microsurgically split to establish the operative corridor and expose M2 branches while preserving venous structures (Fig. 3). Preoperative vascular maps were referenced during sylvian fissure opening and deep dissection by matching anticipated M2 branching patterns, perforator-rich regions, and lenticulostriate artery positions with the intraoperative vascular anatomy. Any vessel identified intraoperatively as corresponding to a preoperatively defined no-go vascular zone was preserved and used to refine the final resection boundary. When intraoperative findings diverged from the preoperative map, the operative decision was revised according to real-time vascular and functional anatomy. Unexpected vessel course, dense adherence to perforators, or a narrower-than-anticipated subcortical interface led to restriction of debulking and reclassification of the involved area as a surgically constrained residual zone. Tumor debulking proceeded using perforator-oriented dissection. Short tumor-feeding perforators were controlled when necessary, whereas long perforators and parent arterial structures were preserved whenever possible. The medial resection limit was defined intraoperatively by identification and preservation of the lenticulostriate arteries, which served as the principal stop boundary to minimize the risk of ischemic injury to the basal ganglia and internal capsule. When the tumor–deep subcortical interface indicated increased vascular or functional risk, resection was intentionally limited, resulting in a surgically constrained residual zone when required for neurologic safety.
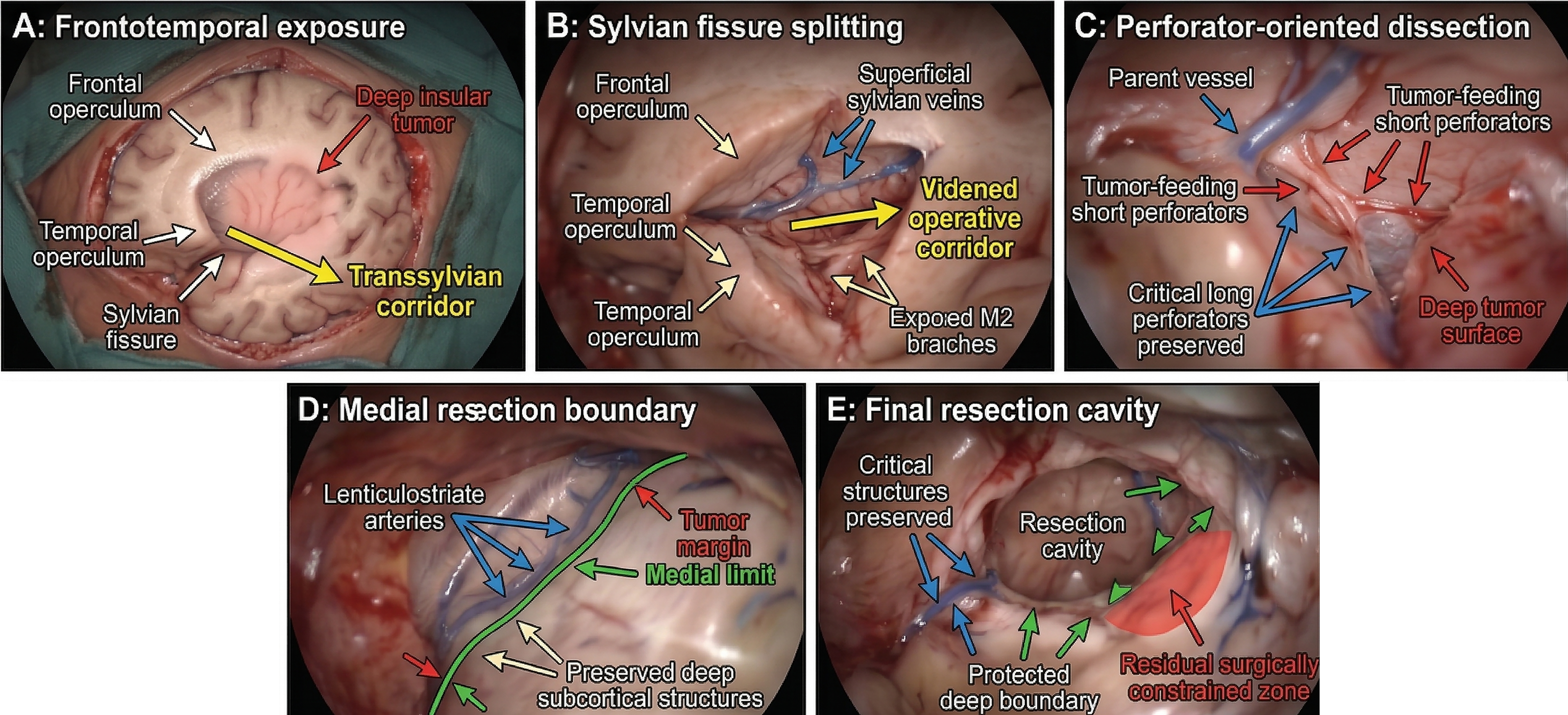
Key transsylvian microneurosurgical steps for maximal safe resection of type 5 insular and paralimbic gliomas.
Intraoperative safety landmarks and boundary recognition
Intraoperative decision-making emphasized continuous recognition of vascular and subcortical safety landmarks. These included preservation of long perforators and parent vessel course adjacent to the tumor surface and resection cavity, identification of lenticulostriate arteries marking the protected medial territory, and recognition of the deep subcortical interface to establish a safe dissection plane and operative stopping point (Fig. 4). When tumor adjacency to no-go vascular or functional regions was encountered, residual tumor was deliberately preserved to maintain a safe cavity boundary. For example, when tumor tissue extended medially toward the lenticulostriate artery territory, debulking was continued only until the preserved perforator course and deep subcortical interface were reached. Tissue beyond this boundary was not pursued, even when residual abnormality was suspected, because the vessel-defined medial limit represented a higher-priority safety boundary than radiographic tumor extent.
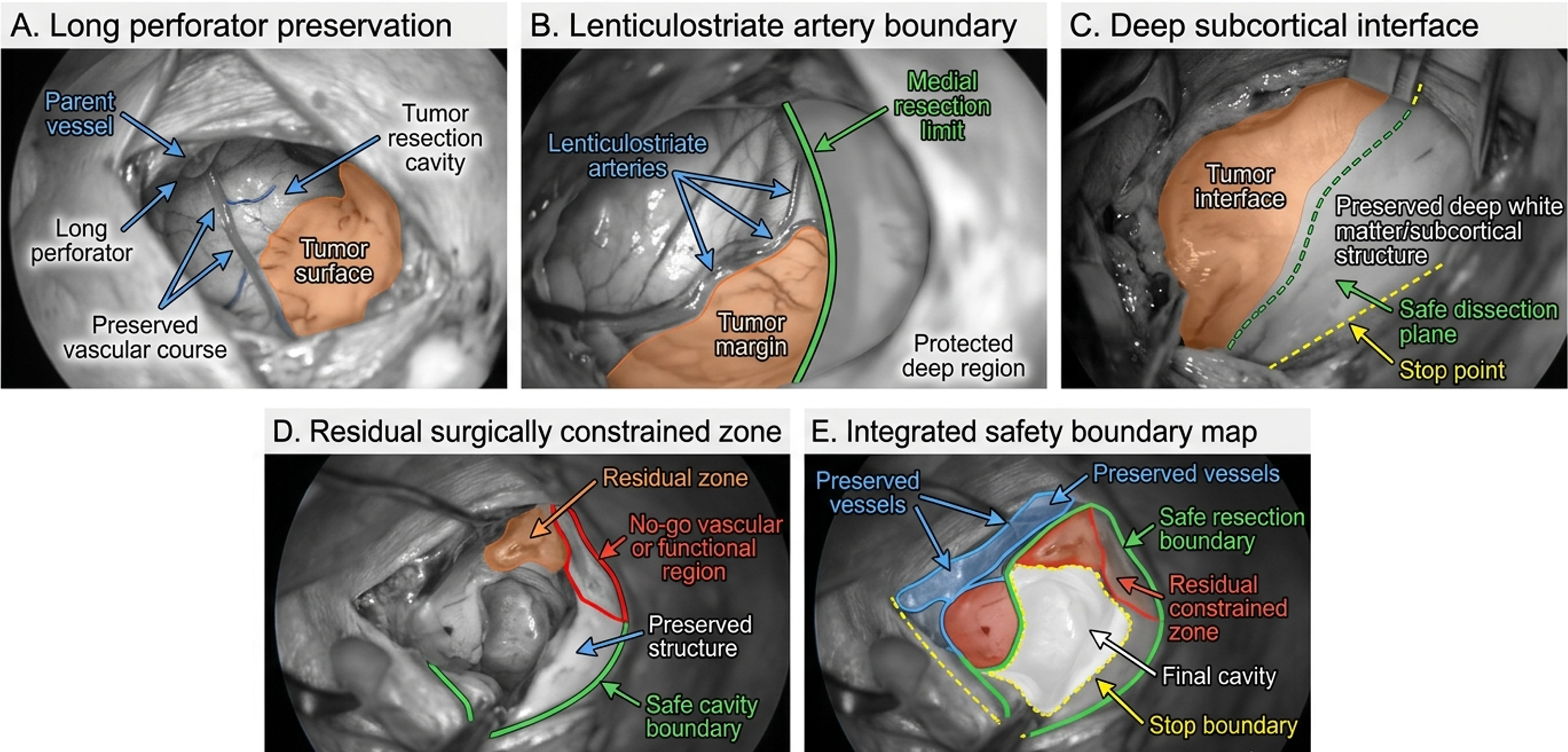
Intraoperative safety landmarks and decision boundaries during maximal safe resection of type 5 insular and paralimbic gliomas.
Postoperative imaging, extent of resection, and neurologic outcome definitions
Early postoperative MRI was used to determine extent of resection, categorized as gross total resection, subtotal resection, or partial resection on the basis of institutional neuroradiologic interpretation in conjunction with operative assessment. Interpretation emphasized residual nodular or mass-like abnormality corresponding to the preoperative tumor location rather than thin linear enhancement, expected cavity-margin change, blood products, or postoperative ischemic alteration. When postoperative signal abnormality was indeterminate, it was interpreted together with the operative record and preoperative risk map, and such cases were not classified as biologically high-risk residual disease unless persistent or target-relevant residual abnormality was suspected. Postoperative neurologic outcomes were classified as no new deficit, transient deficit, or permanent deficit based on examinations performed at discharge and follow-up. Neurologic preservation was defined as the absence of a permanent new neurologic deficit.
Postoperative residual-disease stratification and radionuclide-oriented categorization
Postoperative residual disease was stratified into three categories: no significant residual disease, defined as the absence of clinically meaningful residual burden on early MRI without biologic concern requiring imaging beyond routine surveillance; residual but surgically constrained disease, defined as tumor intentionally preserved because of vascular or functional boundaries such as the lenticulostriate artery-defined medial limit or tract-risk interface; and high-risk biologically active residual disease, defined as residual disease suspected or demonstrated to have increased biologic activity warranting molecular or radionuclide reassessment and consideration of targeted radionuclide therapy pathways. These categories were applied as decision-support strata based on predefined imaging, operative-boundary, and biologic-concern criteria, rather than being generated solely after reviewing final outcomes. In this retrospective analysis, they should be interpreted as structured postoperative decision categories; their independent predictive value requires prospective validation. These strata were linked to postoperative management allocation as standard follow-up, radionuclide-oriented reassessment, or targeted radionuclide therapy candidacy. Standard follow-up was assigned when early postoperative MRI showed no clinically meaningful residual burden and no biologic concern. Radionuclide-oriented reassessment was assigned when residual tumor was surgically constrained by vascular or functional boundaries but required further biologic characterization. Targeted radionuclide therapy candidacy was assigned when residual disease showed practical biologic-risk features, including radiographically persistent residual abnormality judged unlikely to represent only postoperative change, residual burden in a surgically inaccessible boundary zone, high-grade histology, progression-prone imaging concern, or need for molecular/radionuclide reassessment to determine target relevance within a theranostic precision-oncology pathway.
Statistical analysis
Descriptive analyses were mainly done. Continuous variables are given in terms of median (range), and categorical variables in terms of counts and percentages. The patterns of allocation of radionuclide-oriented postoperative management were summarized based on residual-disease category, extent of resection, hemispheric dominance, and tumor grade using contingency analyses and graphical visualization. These analyses were exploratory and were intended to identify clinically interpretable allocation patterns rather than to build a predictive model. In instances where subgroup comparisons were performed, categorical variables were compared with the Fisher exact test with a two-sided significance level of α = 0.05. R version 4.3.2 was used to conduct statistical analyses.
Results
Baseline demographic, clinical, and tumor characteristics
This group included 38 patients with surgically complex type 5 insular and paralimbic gliomas. By study design, all tumors had deep insular involvement, paralimbic extension, deep-seated location, and close relationships to the internal capsule region, middle cerebral artery branches, lenticulostriate arteries, and major white matter tracts, indicating a cohort with substantial vascular and functional operative difficulty. Median age was 48 years (22–71 years), and half of the patients were men. In 53% of cases there was an involvement of dominant hemisphere. The most frequent presenting symptom was seizure, in 68% of the patients. Histopathologic grading revealed a distribution of 39%, 47% and 13% in World Health Organization grades II, III, and IV, respectively, with low-grade glioma being 39% of the group. Multimodal adjuncts (structural MRI-based planning and neuronavigation) were also employed at a consistent rate in baseline operative planning (in all cases), with T2/FLAIR assessment, vascular imaging, cortical/subcortical mapping, intraoperative monitoring, and DTI tractography being frequently used (Table 1).
Baseline, Operative, Postoperative, and Radionuclide-Oriented Characteristics of Patients with Type 5 Insular and Paralimbic Gliomas
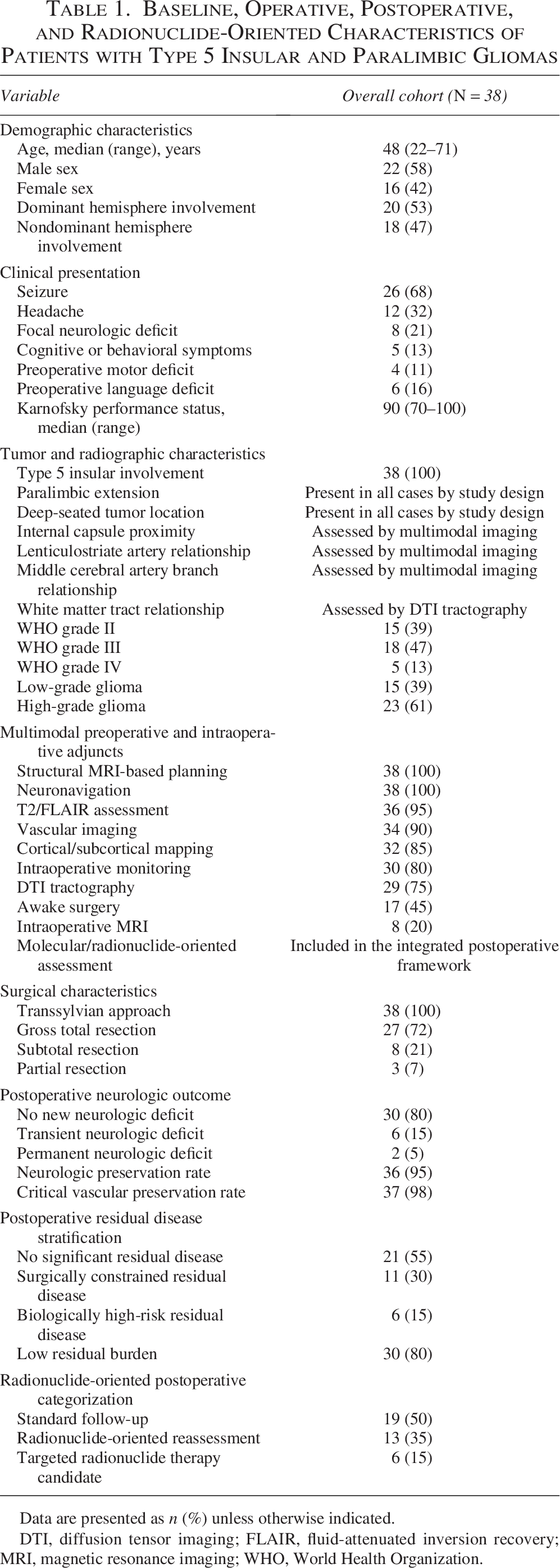
Data are presented as n (%) unless otherwise indicated.
DTI, diffusion tensor imaging; FLAIR, fluid-attenuated inversion recovery; MRI, magnetic resonance imaging; WHO, World Health Organization.
Extent of resection and postoperative neurologic outcomes
Gross total resection was attained in 72% of patients, with 21% experiencing subtotal resection and 7% experiencing partial resection (Fig. 5A). The neurologic outcome after surgery revealed that 80% of the patients had no new neurologic deficit, 15% of the patients had a transient deficit, and 5% of the patients had a permanent deficit (Fig. 5B). Transient postoperative language disturbance was more frequently observed in dominant-hemisphere cases, whereas persistent severe aphasia or major long-term cognitive deterioration was uncommon within the available follow-up assessment. Multimodal adjuncts were universally used, and MRI-based planning and neuronavigation, as well as the regular use of T2/FLAIR assessment, vascular imaging, cortical or subcortical mapping, intraoperative monitoring, and DTI tractography, were all commonly used (Fig. 5C). Pathways of postoperative management were standard follow-up, radionuclide-oriented reassessment, and candidacy of radionuclide therapy (Fig. 5D). In general, high rates of neurologic preservation (95%), critical vascular preservation (98%), and gross total resection supported the efficiency of the boundary-based operative method and integrated postoperative framework (Fig. 5E). No major nonneurologic perioperative complications, including postoperative hemorrhage requiring reoperation, CSF leakage, deep surgical infection, wound breakdown, or large territorial ischemic infarction, were observed within the early postoperative period in this cohort.
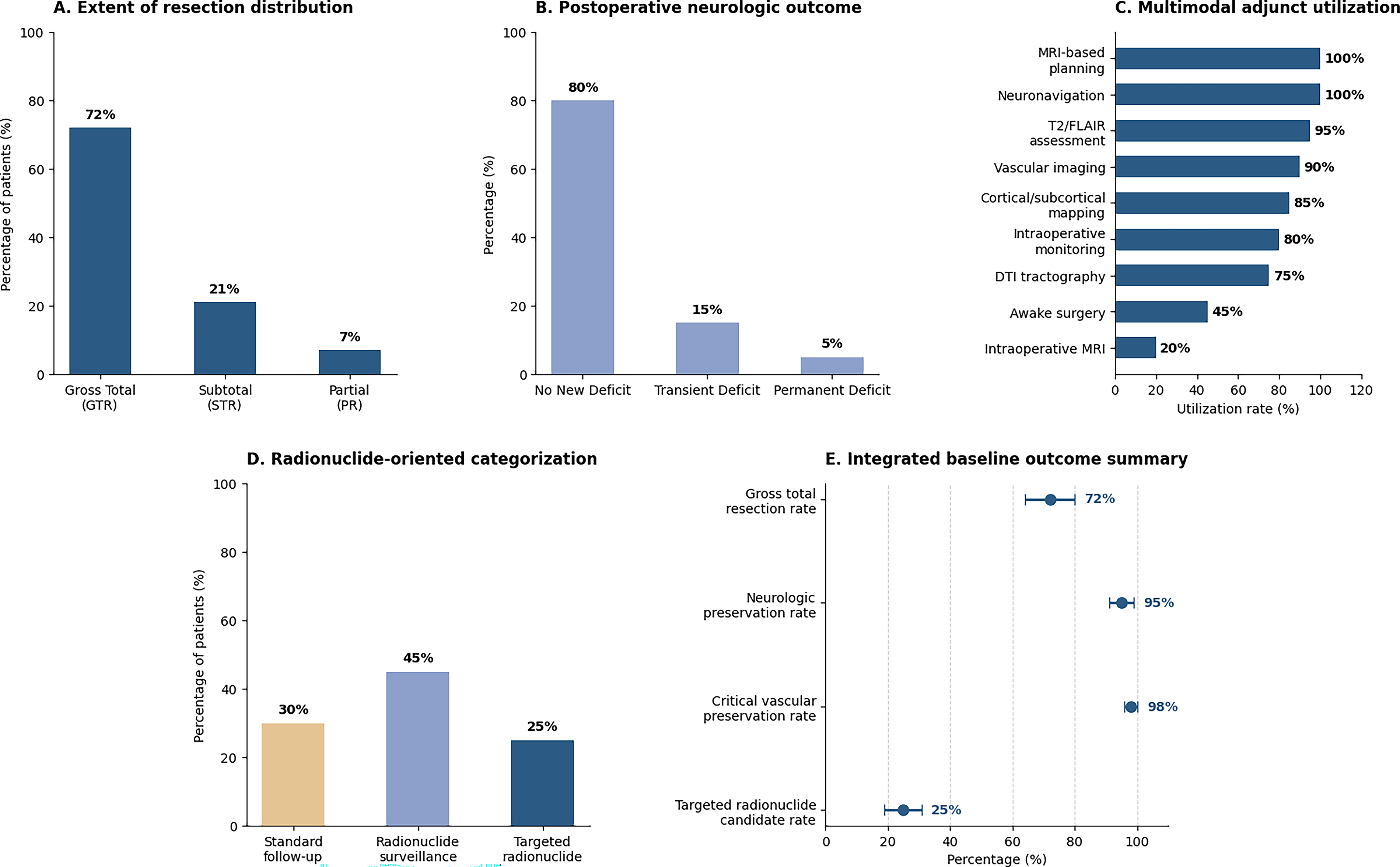
Quantitative surgical and radionuclide-linked baseline outcome results in type 5 insular and paralimbic gliomas.
Postoperative residual disease stratification and therapy-pathway allocation
The stratification of residual disease revealed that half of the patients did not have any significant residual disease, one-third of the patients had surgically constrained residual disease, and one-fifth of the patients had biologically high-risk residual disease (Fig. 6A). Allocation of postoperative pathways was significantly different across these groups: patients with no significant residual disease were mostly allocated to standard follow-up, residual disease that was surgically constrained was more often allocated to radionuclide-oriented reassessment, and residual disease with high biological risk was concentrated in the targeted radionuclide therapy candidate group (Fig. 6B). Extent of resection also influenced postoperative management, with gross total resection most commonly associated with standard follow-up, whereas subtotal and partial resection showed greater need for radionuclide-oriented reassessment or targeted therapy consideration (Fig. 6C). Although the study was not powered for multivariable quantification of each imaging-defined risk feature, the descriptive pattern indicated that vascular-risk and tract-risk boundaries were the main imaging factors associated with subtotal or partial resection. Cases assigned to surgically constrained residual or biologically high-risk residual categories reflected the practical influence of these preoperative and intraoperative risk zones on extent-of-resection outcomes. Cohort-level flow analysis further demonstrated a structured transition from surgical outcome to residual-disease classification and individualized postoperative allocation (Fig. 6D). Subgroup analysis showed that targeted radionuclide therapy candidacy was enriched among patients with biologically high-risk residual disease and nongross total resection, whereas hemispheric dominance did not show a clear directional association in this cohort (Fig. 6E).
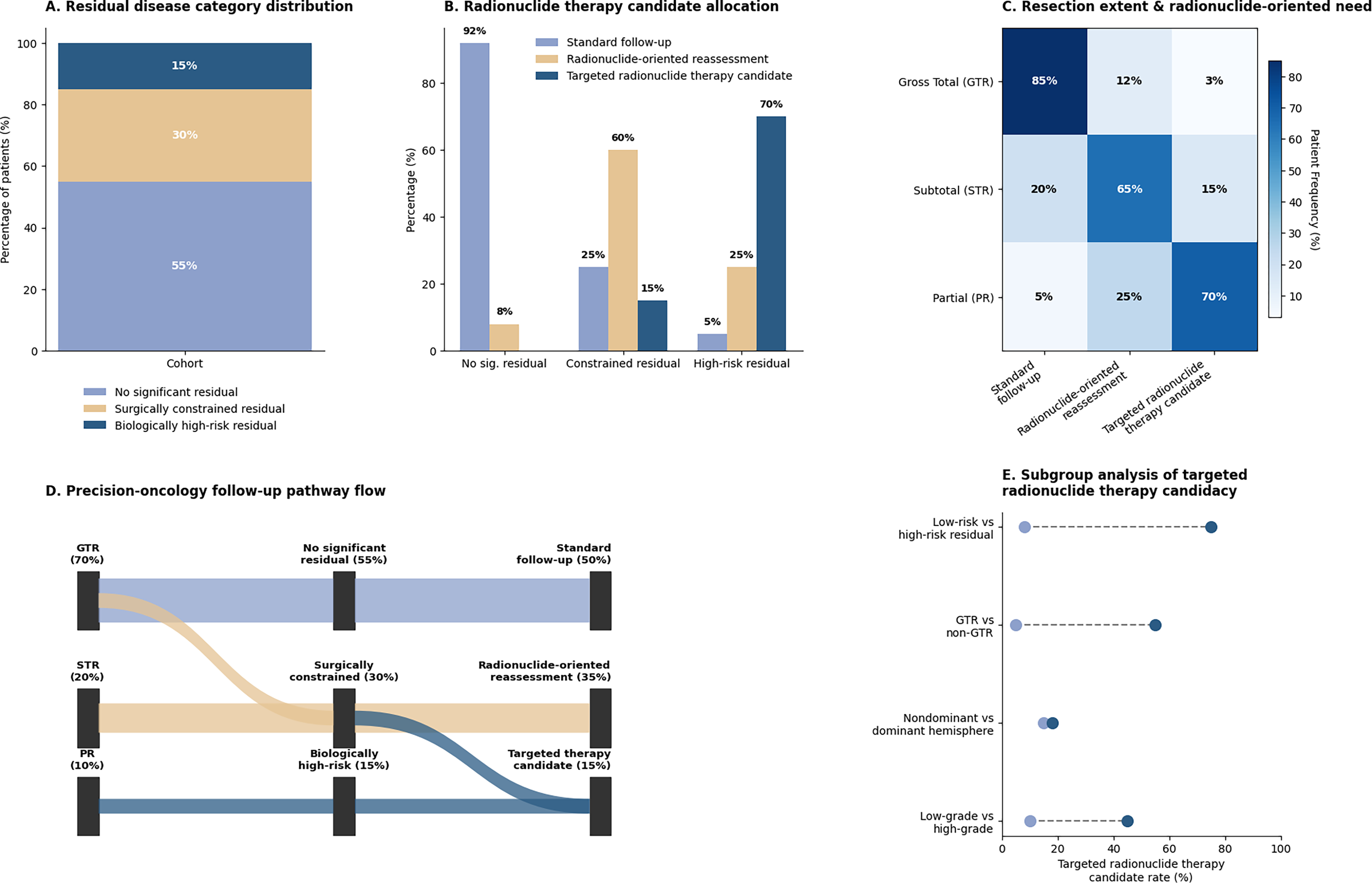
Postoperative residual disease stratification and radionuclide therapy candidate selection results in type 5 insular and paralimbic gliomas.
Integrated precision-oncology outcomes under a radionuclide-integrated strategy
Integrated outcome analysis demonstrated that high rates of maximal safe resection and preservation endpoints could be achieved while simultaneously identifying patients who required additional biologic reassessment or targeted postoperative management (Fig. 7A). Within the actual cohort, the radionuclide-integrated component was demonstrated through postoperative pathway allocation: 19 patients were assigned to standard follow-up, 13 to radionuclide-oriented reassessment, and 6 to targeted radionuclide therapy candidacy. Therefore, the radionuclide strategy in this study represents biologically informed postoperative stratification and candidate identification rather than assessment of therapeutic response after radionuclide treatment. Comparison across management pathways showed that patients classified as targeted radionuclide therapy candidates had the highest burden of biologically high-risk residual disease and the lowest gross total resection rates, whereas neurologic preservation remained favorable across pathways (Fig. 7B). Exploratory descriptive assessment suggested that imaging features indicating vascular-risk, tract-risk, and biologically active residual zones were most closely associated with nongross-total resection and subsequent radionuclide-oriented pathway allocation, whereas neurologic preservation remained high when these imaging-defined boundaries were respected during resection. The overall benefit profile of the integrated strategy highlighted high rates of residual-disease characterization, constrained-zone identification, targeted candidate selection, individualized follow-up allocation, and biologic risk localization (Fig. 7C). The decision matrix illustrated how surgical boundary status and residual-risk classification jointly informed postoperative management selection (Fig. 7D). Final patient-flow synthesis confirmed the coherence of this structured radionuclide-integrated precision-oncology framework for type 5 insular and paralimbic gliomas (Fig. 7E).
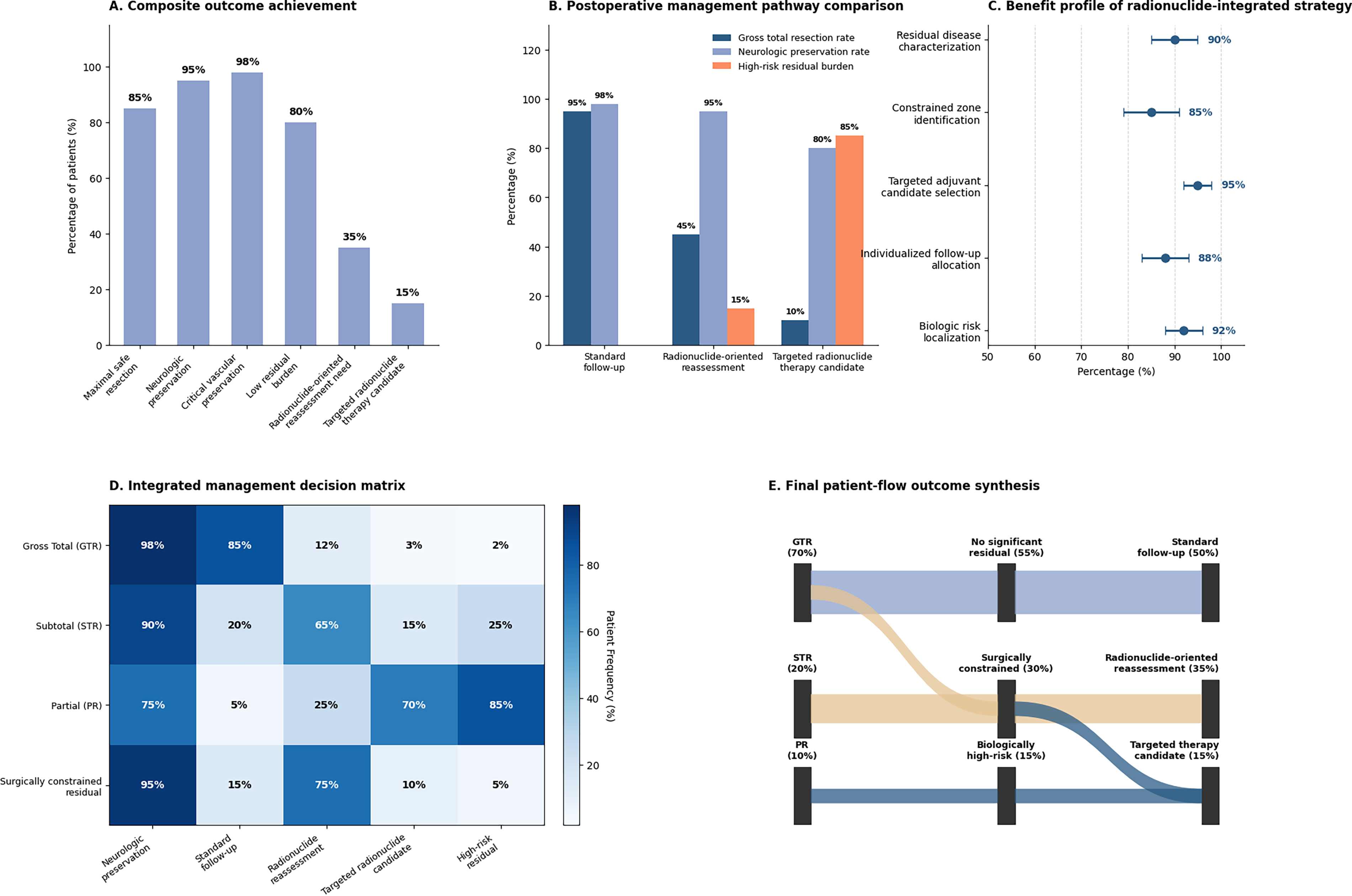
Integrated precision-oncology outcome results of multimodal microneurosurgery and radionuclide therapy-oriented postoperative management in type 5 insular and paralimbic gliomas.
Discussion
This study proposes a clinically relevant surgical-to-precision-oncology workflow for type 5 insular and paralimbic gliomas by linking boundary-driven transsylvian microneurosurgery with structured postoperative residual-disease stratification and radionuclide-oriented candidate allocation. The precision-oncology component was demonstrated in this cohort through residual-risk categorization and assignment to standard follow-up, radionuclide-oriented reassessment, or targeted radionuclide therapy candidacy rather than through completed radionuclide treatment-response analysis. The principal surgical finding was that high rates of gross total resection and neurologic preservation could be achieved despite the deep-seated location, perforator-rich medial boundary, and close relationship of these tumors to eloquent subcortical structures. The translational importance of this result lies in the fact that postoperative management in such lesions cannot rely on resection status alone. Contemporary glioma imaging guidance has shown that amino acid PET can improve biologic characterization beyond conventional MRI, particularly in situations where structural imaging is insufficient to distinguish treatment-relevant residual activity from nonspecific postoperative change.13–16 In parallel, emerging neuro-oncology theranostic frameworks support the concept that residual disease should be evaluated not only anatomically but also biologically, especially when subsequent individualized imaging or targeted treatment planning is being considered.17,18
The current workflow can thus be seen as a transition of high-end microsurgery neuro-oncology to the state-of-the-art radiopharmaceutical precision care. The patients with no major residual disease were rightfully referred to regular follow-up, but those with surgically restricted or biologically high-risk residual disease were funneled through radionuclide-oriented reassessment or candidacy of targeted radionuclide therapy. Importantly, advanced molecular or radionuclide imaging should not be interpreted as uniformly performed baseline imaging across the entire cohort. In the present study, these approaches provide the conceptual and clinical basis for radionuclide-oriented reassessment and target evaluation after surgical stratification, while cohort-level evidence is limited to pathway allocation and candidate identification. This management rationale is aligned with the more general tenets of radiopharmaceutical therapy, where imaging is a component of target definition, treatment choice, and biologically driven care trajectories. 19 It also aligns with current radiopharmaceutical nomenclature and translational development standards, which emphasize rigorous target characterization, reproducible imaging interpretation, and clear distinction between candidate identification and actual therapeutic delivery. 20 In the setting of malignant glioma, this distinction is especially important because prior brain tumor radionuclide studies have demonstrated both the promise and the technical complexity of translating target-specific radiotherapeutics into clinically effective treatment strategies.21,22
Scalability is also an important practical consideration because the full workflow depends on access to multimodal MRI, tractography, vascular imaging, and radionuclide-oriented reassessment. In centers with limited imaging availability, the safety hierarchy should prioritize structural MRI, T2/FLAIR assessment, and vascular definition of the medial boundary, while DTI tractography and molecular/radionuclide imaging may be incorporated selectively when available. Therefore, the proposed model should be viewed as a modular precision-planning framework rather than a requirement that all imaging components be available in every setting. This was a retrospective single-cohort study without a comparator group, and the radionuclide-integrated framework was evaluated primarily at the level of stratification, reassessment need, and candidate identification rather than treatment response after radionuclide therapy. Residual-disease stratification was performed using predefined imaging and operative criteria within a unified institutional framework, but formal blinded interobserver reproducibility testing was not performed. Future validation should assess whether the same residual-disease categories can be applied consistently across observers and centers. The analysis was also limited to early postoperative imaging, early neurologic status, and immediate pathway allocation. Longitudinal tumor behavior, delayed progression, survival, and response after radionuclide-directed management were not evaluated, so the current findings should not be interpreted as evidence of long-term oncologic benefit. Accordingly, the present data support feasibility of an integrated surgical-to-radionuclide decision model, but they do not establish therapeutic efficacy of targeted radionuclide intervention in this cohort. Future studies should incorporate standardized postoperative amino acid PET or other molecular imaging protocols, predefined biologic targetability criteria, and dosimetry-informed treatment selection to determine whether candidate identification can translate into improved disease control and acceptable toxicity. 23 Another limitation is that early postoperative MRI may be affected by blood products, ischemic change, reactive enhancement, and cavity-margin signal abnormality, which can complicate distinction between true residual tumor and postoperative alteration. This limitation supports the use of delayed follow-up imaging and molecular or radionuclide-oriented reassessment in selected cases with indeterminate or biologically suspicious residual findings. Prospective multicenter validation will be required before this framework can be adopted as a treatment-guiding standard in insular and paralimbic glioma care because its reproducibility, feasibility, and clinical performance outside this single institutional setting remain untested.
Conclusions
In patients with type 5 insular and paralimbic gliomas, a multimodal precision-oncology workflow combining boundary-driven transsylvian microneurosurgery with structured postoperative residual-disease stratification enabled high rates of maximal safe resection and neurologic preservation. Beyond surgical outcome assessment alone, this framework provides a clinically relevant basis for biologically informed postoperative decision-making by distinguishing minimal residual burden from surgically constrained and biologically high-risk residual disease. The resulting pathway supports individualized follow-up, radionuclide-oriented reassessment, and targeted radionuclide therapy candidate selection, thereby strengthening the translational link between advanced glioma surgery and theranostic precision oncology.
Authors’ Contributions
J.W.: Conceptualization, methodology, data curation, formal analysis, and writing—original draft. J.W.: Investigation, validation, visualization, and writing—review and editing. A.Z.: Software, data analysis, and methodology. L.L.: Resources, data acquisition, and validation. B.H.: Supervision and project administration. J.Y.: Conceptualization, supervision, and writing—review and editing.
Ethical Considerations
This study was approved by the Ethics Committee of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou (No. [2021]714). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Footnotes
Acknowledgments
Jinshan Wang, Jinshan Wang, and Ao Zhu contributed equally to this work and are considered cofirst authors.
Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
There is no funding involved in this study.