
Abstract
Objective:
To compare the clinical efficacy of the curved vertebroplasty system combined with targeted radionuclide therapy (radium-223/strontium-89) versus conventional percutaneous vertebroplasty (PVP) combined with radionuclide therapy in the treatment of malignant tumor-related pathological vertebral fractures, and to evaluate differences between the two surgical approaches in postfracture pain relief, vertebral morphological reconstruction, spinal functional recovery, and quality-of-life improvement.
Methods:
A retrospective analysis was performed on 125 patients with pathologically confirmed malignant tumor bone metastasis-related pathological vertebral fractures treated between January 2022 and December 2024. All patients received targeted radionuclide therapy, and vertebroplasty was performed 14–21 d after the last radionuclide dose. Patients were divided into the curved vertebroplasty combined with radionuclide therapy group (study group, n = 63) and the conventional PVP combined with radionuclide therapy group (control group, n = 62). The primary outcome was the Visual Analogue Scale (VAS) pain score. Secondary outcomes included the postfracture vertebral height recovery rate, the Oswestry Disability Index (ODI), the Roland–Morris Disability Questionnaire (RMDQ), bone cement distribution, vertebral kyphotic angle, and SF-36 quality-of-life score. Patients were followed for 6 months, and radionuclide therapy-related adverse events were monitored.
Results:
Baseline characteristics were comparable between the two groups (p > 0.05). At 3 and 6 months after pathological fracture surgery, VAS scores were significantly lower in the study group than in the control group (1.6 ± 0.8 vs. 2.5 ± 1.0; 1.4 ± 0.7 vs. 2.4 ± 0.9; both p < 0.01). At all postoperative time points, the study group demonstrated significantly superior vertebral height recovery rates, ODI, and RMDQ improvement (all ps < 0.017), as well as a better kyphotic angle correction (p < 0.017). The anterior–middle column bone cement fill rate was significantly higher in the study group (88.4% ± 9.1% vs. 74.6% ± 13.2%, p < 0.001), with no intraspinal cement leakage. All eight SF-36 domain scores were significantly higher in the study group at 6 months (all ps < 0.001). Hematological toxicity rates did not differ significantly between groups (14.3% vs. 12.9%, p = 0.819).
Conclusions:
In the surgical management of malignant tumor-related pathological vertebral fractures, the curved vertebroplasty system combined with targeted radionuclide therapy demonstrates significantly superior postfracture pain control, vertebral morphological reconstruction, spinal functional recovery, and quality-of-life improvement compared with conventional PVP combined with radionuclide therapy, without increasing radionuclide-related toxicity. The precise anterior–middle column cement filling achieved by the curved system, combined with the systemic antitumor effect of radionuclide therapy, establishes a synergistic precision treatment model of local surgical reconstruction plus systemic radionuclide therapy for tumor-related pathological vertebral fractures.
Keywords
Introduction
Bone metastasis is the most common cause of pathological vertebral fractures in cancer patients, occurring in up to 30%−70% of patients with skeletal metastases, most frequently in lung, breast, and prostate cancers, as well as multiple myeloma. 1 Tumor cell infiltration of the vertebral body causes progressive destruction of the trabecular architecture and thinning of the cortical bone, leading to pathological fractures that may occur with minimal or even no trauma. 2 Unlike osteoporotic vertebral fractures, tumor-related pathological fractures are characterized by poor healing potential, severe pain, high risk of neurological compromise, and the additional complexity of concurrent systemic oncological treatment. 3
Targeted radionuclide therapy represents one of the most important advances in the management of bone metastases in recent years. Radium-223 (223Ra), the first approved α-particle radionuclide, selectively accumulates at bone metastasis sites and delivers high linear energy transfer radiation that induces double-strand DNA breaks in tumor cells while causing minimal injury to the surrounding marrow. 4 Strontium-89 (89Sr) is a β-emitting radionuclide that accumulates at osteoblastically active lytic and mixed bone metastases, exerting a sustained local radiotherapeutic effect and providing well-validated pain control across multiple tumor histologies. 5 However, radionuclides exert systemic antitumor effects that require several weeks to manifest clinical benefit; for pathological fractures with established cortical collapse, radionuclide therapy alone cannot promptly restore vertebral mechanical stability, and local surgical intervention remains essential. 6
Surgical management of tumor-related pathological vertebral fractures presents unique challenges: Extensive lytic destruction creates large anterior–middle column defects that are difficult to fill uniformly with bone cement; many patients are under active cancer treatment with varying degrees of bone marrow suppression, making the surgical window critical to select carefully; and tumor involvement may compromise the posterior vertebral wall, increasing the risk of cement extravasation. 7 Percutaneous vertebroplasty (PVP), owing to its minimal invasiveness and rapid analgesic effect, has become the primary minimally invasive approach for pathological vertebral fractures. However, the fixed working-channel angle of the conventional straight-needle system limits its ability to adequately cover the anterior–middle column in lytic defects, compromising local biomechanical reconstruction. 8 Tumor bone metastases preferentially destroy the anterior and middle vertebral columns through lytic resorption, creating large, irregular defect cavities that the fixed straight-needle trajectory cannot adequately reach; the curved system’s adjustable working channel allows targeted cement delivery into these anterior-column defects, providing a mechanistic basis for its superior performance in metastatic pathological fractures.
The curved vertebroplasty system, equipped with an adjustable-angle (0°–30°) working channel, can achieve multidirectional precise cement injection under C-arm fluoroscopic guidance, theoretically offering substantially improved anterior–middle column fill rates in lytic pathological fractures. 9 Combining the local mechanical reconstruction advantage of curved vertebroplasty with the systemic targeted antitumor effect of radionuclide therapy holds promise for establishing a synergistic precision treatment model of local surgical reconstruction plus systemic radionuclide therapy for tumor-related pathological vertebral fractures. 10
To date, no comparative study has systematically evaluated the curved vertebroplasty system against conventional PVP in the specific context of tumor-related pathological vertebral fractures treated concomitantly with radionuclide therapy. The present retrospective cohort study analyzed 125 patients to compare the two approaches with respect to postfracture pain relief, vertebral morphological reconstruction, spinal function, quality of life, and radionuclide therapy safety, to provide evidence-based guidance for treatment selection in this challenging patient population.
Materials and Methods
Study design
This was a retrospective cohort study. Clinical data were collected from patients with tumor-related pathological vertebral fractures treated in the Department of Orthopedics in collaboration with the Department of Nuclear Medicine between January 2022 and December 2024. The study was approved by the institutional review board (approval number: LFYYLL-2021-10), and all patients provided written informed consent for surgery and radionuclide therapy.
Participants
Inclusion criteria
(1) Pathologically confirmed or radiologically and clinically diagnosed malignant tumor bone metastasis-related pathological fracture of the thoracolumbar spine (T10–L5); (2) age 18–80 years, ECOG performance status 0–3; (3) vertebral compression degree ≤60%, with radiologically intact or <30% disrupted posterior wall, and no cord compression; (4) currently receiving or planned to receive targeted radionuclide therapy (radium-223 or strontium-89); (5) ASA classification grades I–III, able to tolerate vertebroplasty; and (6) complete clinical data with follow-up ≥6 months.
Exclusion criteria
(1) Burst fracture with spinal canal compromise >1/3; (2) preexisting lower extremity neurological deficits; (3) infectious spondylitis or tuberculosis-related vertebral destruction; (4) severe cardiopulmonary dysfunction precluding surgery; (5) severe coagulopathy international normalized ratio (INR) >2.0 or anticoagulant use within 2 weeks preoperatively; (6) allergy to contrast agent or bone cement; (7) estimated survival <3 months; (8) concurrent other spinal surgeries; and (9) incomplete clinical records.
Grouping
Patients were allocated to two groups based on the surgical approach: The curved vertebroplasty combined with the radionuclide therapy group (study group, n = 63), in which pathological fractures were addressed with the curved vertebroplasty system while concurrently receiving radionuclide therapy; and the conventional PVP combined with the radionuclide therapy group (control group, n = 62), in which fractures were managed with conventional straight-needle PVP while concurrently receiving radionuclide therapy. Both groups received standardized radionuclide treatment regimens as per the Department of Nuclear Medicine protocols. To minimize operator-related variability, all vertebroplasty procedures in both groups were performed by the same two senior spine surgeons, each with more than 5 years of dedicated experience in PVP.
Treatment protocols
Targeted radionuclide therapy: Following diagnosis of pathological vertebral fracture, all patients were evaluated by the nuclear medicine team. Radium-223 was administered at 55 kBq/kg intravenously every 4 weeks for six cycles, primarily for prostate cancer and selected breast cancer bone metastases; strontium-89 was administered at 148 MBq intravenously every 3 months, primarily for other solid tumor bone metastases. Selection between agents was based on tumor histology, bone scan characteristics (blastic/lytic/mixed), and bone marrow reserve. Specifically, radium-223 was preferred for prostate cancer owing to its established overall survival benefit in osteoblastic disease, and for selected breast cancer patients with predominantly blastic skeletal involvement; strontium-89 was used for other solid tumor histologies with lytic or mixed metastatic patterns, given its well-validated analgesic efficacy across multiple histologies. Agent selection was made jointly by the nuclear medicine and oncology teams at a multidisciplinary tumor board.
Surgical timing for pathological fracture: Vertebroplasty was performed 14–21 d after the last radionuclide dose, corresponding to the postnadir bone marrow recovery phase. Preoperative hematological criteria included white blood cell count >3.0 × 109/L and platelet count >80 × 109/L. For patients with severe postfracture pain or high vertebral instability risk, surgery was performed earlier with enhanced supportive care. Hematological monitoring: Complete blood counts were obtained at baseline, on the day of surgery, and at weeks 1, 2, and 4 postoperatively, then monthly thereafter. Radionuclide therapy was delayed when the white blood cell count fell below 3.0 × 109/L or the platelet count went below 80 × 109/L, with resumption contingent on recovery above these thresholds on two consecutive weekly assessments.
Curved vertebroplasty (study group): Patients were positioned prone. C-arm biplane fluoroscopy was used to localize the target vertebra and delineate the extent of lytic destruction and residual cortical margins. Under sterile preparation and local anesthesia (1% lidocaine to periosteum), a working channel (outer diameter 4.0 mm, 0°–30° adjustable) was advanced via a unilateral or bilateral transpedicular approach under alternating anteroposterior and lateral fluoroscopic guidance, with the channel tip directed to the anterior–middle column lytic zone. Based on CT-assessed lytic defect distribution, the channel angle was adjusted to achieve multidirectional polymethylmethacrylate (PMMA) cement injection (4–5 mL), with emphasis on complete anterior–middle column fill. Real-time fluoroscopic monitoring was maintained throughout; injection was immediately halted upon any sign of posterior wall leakage. After cement polymerization, the instruments were withdrawn, local compression hemostasis was applied, and a sterile dressing was placed.
Conventional PVP (control group): Patient positioning and anesthesia were identical to those of the study group. A straight-needle vertebroplasty system (working cannula outer diameter 4.0 mm) was advanced via a unilateral or bilateral transpedicular approach. The cannula tip was placed at the anterior–middle third of the vertebral body under C-arm guidance. PMMA cement (4–5 mL) was injected slowly under continuous fluoroscopic monitoring; the injection was halted immediately upon any leakage sign. After cement solidification, the needle was withdrawn, and local compression hemostasis was applied.
Postoperative management: All patients underwent CT of the lumbar spine within 24 h of surgery to assess cement distribution and leakage. Supervised bed exercises were initiated on postoperative day 2, and patients were mobilized with a brace support on days 3–5 based on pain and stability assessment. Radionuclide therapy was resumed as per the original schedule after surgery, and concurrent systemic oncological treatment (chemotherapy, targeted therapy, endocrine therapy, immunotherapy) was continued throughout.
Outcome measures
General data
Baseline variables collected included age, sex, body–mass index, primary tumor type, number and type (lytic/mixed/blastic) of bone metastases, pathological fracture level, fracture-to-surgery interval, radionuclide regimen and number of cycles administered, interval from last radionuclide dose to surgery, ECOG performance status, hemoglobin level, and bone mineral density T-score.
Primary outcome
Pain relief: Assessed using the Visual Analogue Scale (VAS, 0–10 points; 0 = no pain, 10 = worst imaginable pain) at preoperative day 1 (time of pathological fracture diagnosis), and at postoperative day 1, week 1, and at months 1, 3, and 6.
Secondary outcomes
(1) Vertebral height recovery rate: Measured from lateral radiographs of the thoracolumbar spine. Recovery rate (%) = (postoperative vertebral height—preoperative fracture height)/(expected normal height—preoperative fracture height) × 100%, assessed at postoperative day 1 and at months 1, 3, and 6. (2) Functional disability: The Oswestry Disability Index (ODI) assessed at preoperative day 1 and at postoperative months 1, 3, and 6. (3) Bone cement distribution: CT performed within 24 h postoperatively to assess cement fill volume, distribution uniformity, anterior–middle column coverage, and leakage (paravertebral/intraspinal). (4) Spinal function: Roland–Morris Disability Questionnaire (RMDQ, 0–24 points) assessed at preoperative day 1 and at postoperative months 1, 3, and 6. (5) Vertebral kyphotic angle: Measured from lateral radiographs at preoperative day 1, postoperative day 1, and months 3 and 6. (6) Quality of life: SF-36 (eight domains, each 0–100 points) assessed at preoperative day 1 and postoperative month 6. (7) Radionuclide therapy safety: Hematological toxicity (CTCAE v5.0 grade ≥2), radionuclide dose delay rate due to hematotoxicity, postoperative radionuclide therapy continuation rate, and 6-month bone scan lesion response rate were recorded. Imaging assessment: Cement distribution on postoperative CT, vertebral height recovery, and kyphotic angle were assessed by two radiologists blinded to group allocation; group assignment labels were removed from all imaging files before review, and discrepancies were resolved by consensus with a third independent reviewer.
Statistical analysis
All analyses were performed using SPSS 26.0. Normality was tested with the Shapiro–Wilk test. Normally distributed continuous variables are presented as mean ± SD; non-normally distributed variables as median (interquartile range); categorical variables as n (%). Between-group comparisons of normally distributed continuous variables used the independent-samples t-test; non-normal distributions used the Mann–Whitney U test; categorical variables used the χ2 test or Fisher’s exact test where the expected cell count was <5. Repeated-measures data (VAS, vertebral height recovery, ODI, RMDQ, kyphotic angle, SF-36) were analyzed with the repeated-measures analysis of variance; multiple comparisons were corrected using the Bonferroni method. A p-value of <0.05 was considered statistically significant. Post hoc power analysis confirmed that the achieved sample of 125 patients provides greater than 90% power for the primary VAS outcome (observed group difference 1.0 point, SD approximately 0.9, two-sided α 0.05). Interobserver reliability for vertebral height recovery rate and kyphotic angle was assessed using the intraclass correlation coefficient (ICC); ICC values of 0.91 (95% confidence interval [CI] 0.87–0.94) and 0.89 (95% CI 0.84–0.93), respectively, indicated excellent agreement between the two blinded reviewers.
Results
Baseline characteristics
A total of 125 patients with tumor-related pathological vertebral fractures were enrolled: 63 in the study group and 62 in the control group. The most common primary tumors were lung cancer (33.3% vs. 30.6%), breast cancer (25.4% vs. 27.4%), and prostate cancer (19.0% vs. 17.7%). Lytic and mixed metastases predominated in both groups. The fracture-to-surgery interval (12.4 ± 4.8 vs. 12.9 ± 5.1 d) and the interval from last radionuclide dose to surgery (18.4 ± 5.2 vs. 18.9 ± 5.6 d) were comparable, confirming consistent application of the surgical timing strategy. All baseline characteristics are summarized in Table 1; no statistically significant differences were observed (all ps > 0.05).
Baseline Characteristics of the Two Groups
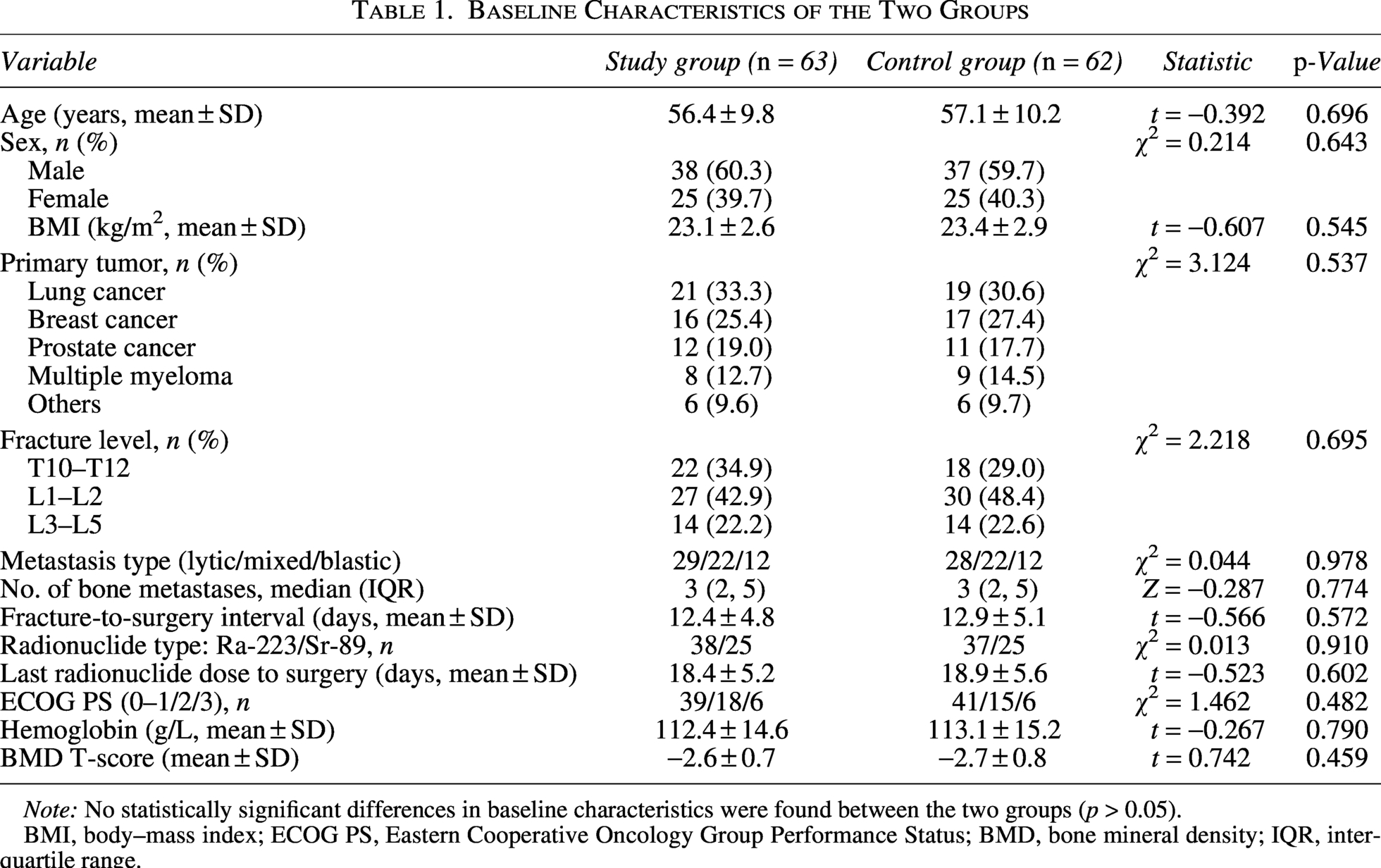
Note: No statistically significant differences in baseline characteristics were found between the two groups (p > 0.05).
BMI, body–mass index; ECOG PS, Eastern Cooperative Oncology Group Performance Status; BMD, bone mineral density; IQR, interquartile range.
Primary outcome
VAS pain score
At the time of pathological fracture diagnosis, both groups exhibited severe pain (VAS 7.9 ± 0.9 vs. 8.0 ± 0.8, p = 0.463), consistent with the pain burden of tumor-related pathological fractures. VAS scores declined significantly in both groups at all postoperative time points compared with baseline (p < 0.001). Bonferroni-corrected pairwise comparisons demonstrated that the study group had significantly lower VAS scores at 3 (1.6 ± 0.8 vs. 2.5 ± 1.0, p = 0.003) and 6 months (1.4 ± 0.7 vs. 2.4 ± 0.9, p = 0.001) postsurgery (Table 2).
Visual Analogue Scale Pain Scores over Time (Mean ± SD, Points)
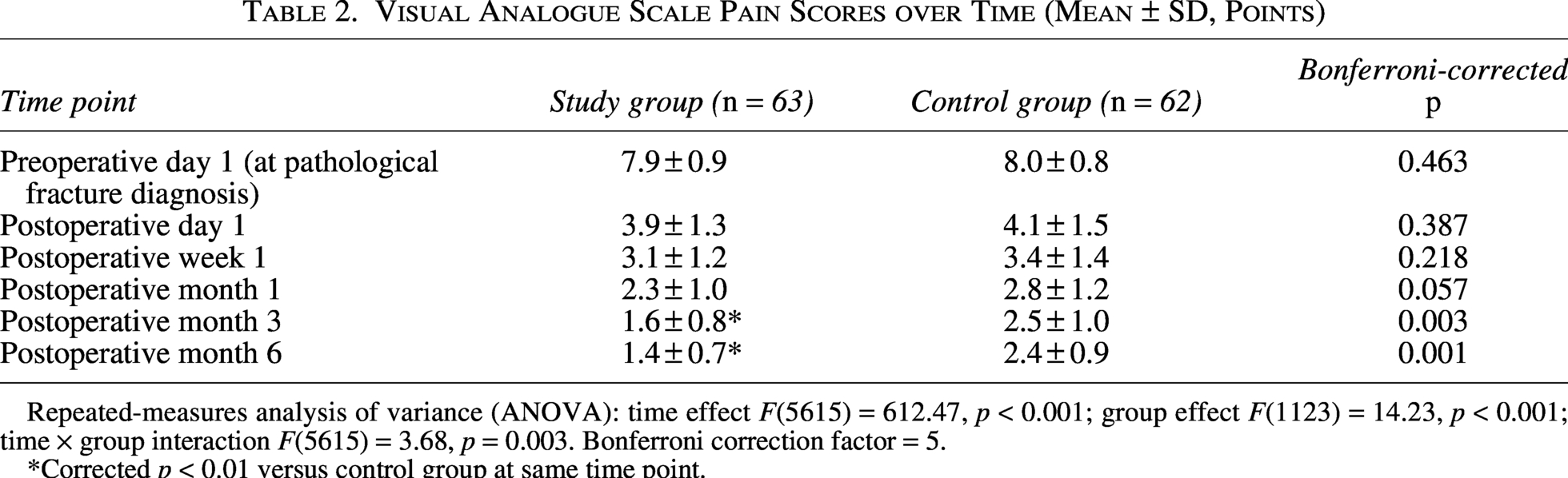
Repeated-measures analysis of variance (ANOVA): time effect F(5615) = 612.47, p < 0.001; group effect F(1123) = 14.23, p < 0.001; time × group interaction F(5615) = 3.68, p = 0.003. Bonferroni correction factor = 5.
*Corrected p < 0.01 versus control group at same time point.
Secondary outcomes
Vertebral height recovery rate
At all postoperative time points, the study group demonstrated significantly higher vertebral height recovery rates than the control group (all corrected ps < 0.017; Table 3). On postoperative day 1, the study group achieved a recovery rate of 66.8% ± 13.1% versus 55.4% ± 15.2% in the control group, and this advantage was maintained at the 6-month follow-up (59.3% ± 11.4% vs. 48.7% ± 12.9%), reflecting more durable vertebral structural restoration enabled by superior anterior–middle column cement filling.
Vertebral Height Recovery Rate After Pathological Fracture Surgery (Mean ± SD, %)
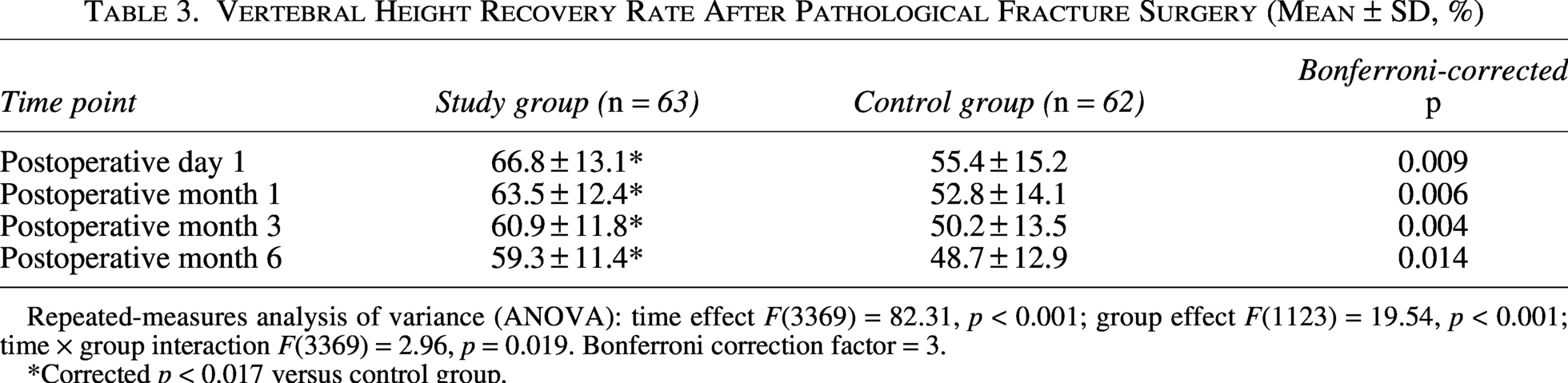
Repeated-measures analysis of variance (ANOVA): time effect F(3369) = 82.31, p < 0.001; group effect F(1123) = 19.54, p < 0.001; time × group interaction F(3369) = 2.96, p = 0.019. Bonferroni correction factor = 3.
*Corrected p < 0.017 versus control group.
ODI functional disability index
ODI scores declined significantly in both groups from baseline at all postoperative time points (p < 0.001). The study group had significantly lower ODI scores at postoperative months 1, 3, and 6 (all corrected ps < 0.017), indicating a more rapid and sustained functional recovery (Table 4).
Oswestry Disability Index Scores over Time (Mean ± SD, %)
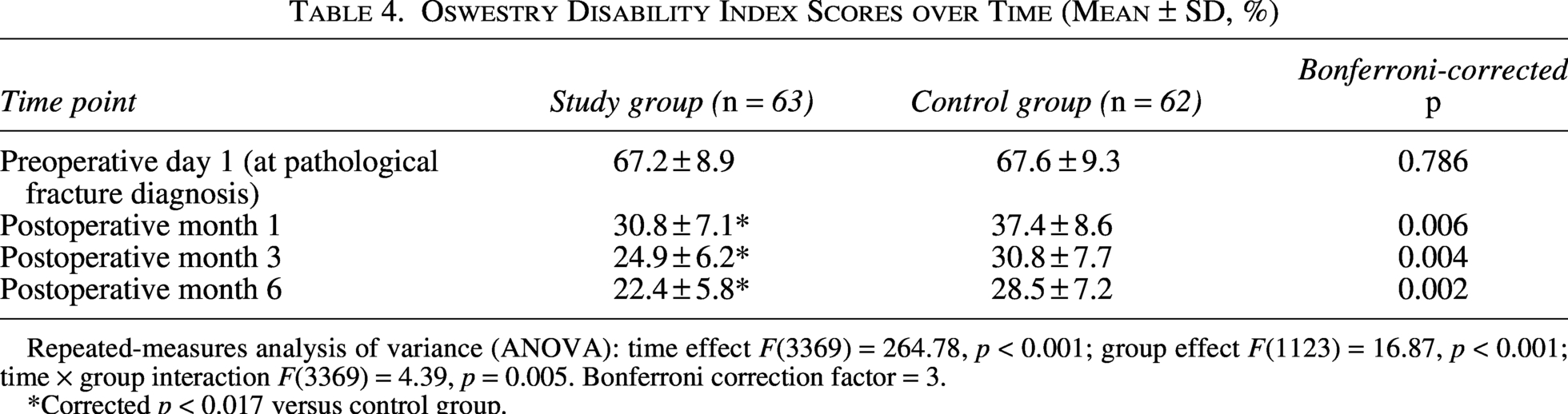
Repeated-measures analysis of variance (ANOVA): time effect F(3369) = 264.78, p < 0.001; group effect F(1123) = 16.87, p < 0.001; time × group interaction F(3369) = 4.39, p = 0.005. Bonferroni correction factor = 3.
*Corrected p < 0.017 versus control group.
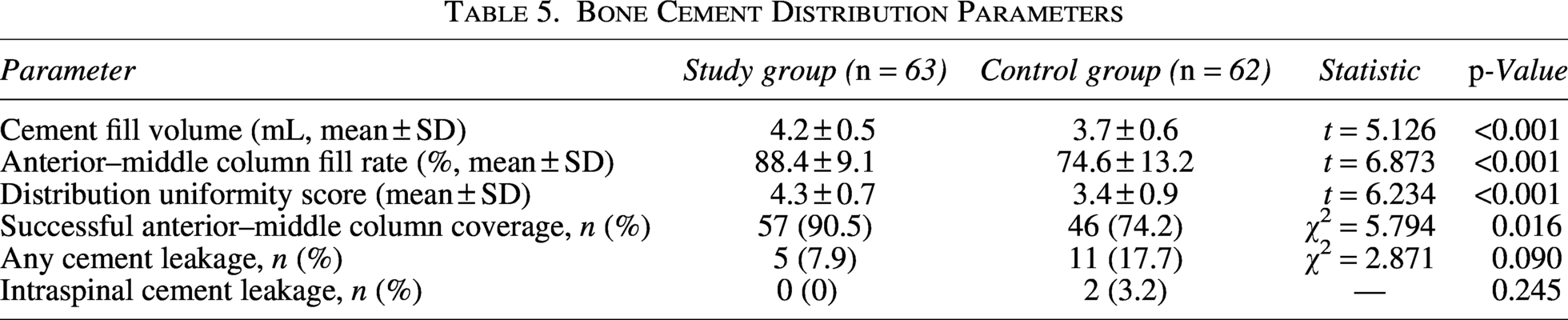
Bone cement distribution
Postoperative CT assessment of bone cement distribution is summarized in Table 5. The study group was significantly superior to the control group in cement fill volume (4.2 ± 0.5 vs. 3.7 ± 0.6 mL, p < 0.001), anterior–middle column fill rate (88.4% ± 9.1% vs. 74.6% ± 13.2%, p < 0.001), distribution uniformity score (p < 0.001), and rate of successful anterior–middle column coverage (90.5% vs. 74.2%, p = 0.016). Overall cement leakage trended lower in the study group (7.9% vs. 17.7%, p = 0.090). Importantly, two cases of intraspinal cement leakage occurred in the control group (3.2%) compared with none in the study group (0%).
Bone Cement Distribution Parameters
RMDQ spinal function score
RMDQ scores were significantly lower in the study group at all postoperative time points (all corrected ps < 0.017), indicating more substantial and sustained improvement in spine-related functional disability following pathological fracture surgery (Table 6).
Roland–Morris Disability Questionnaire Scores over Time (Mean ± SD, Points)
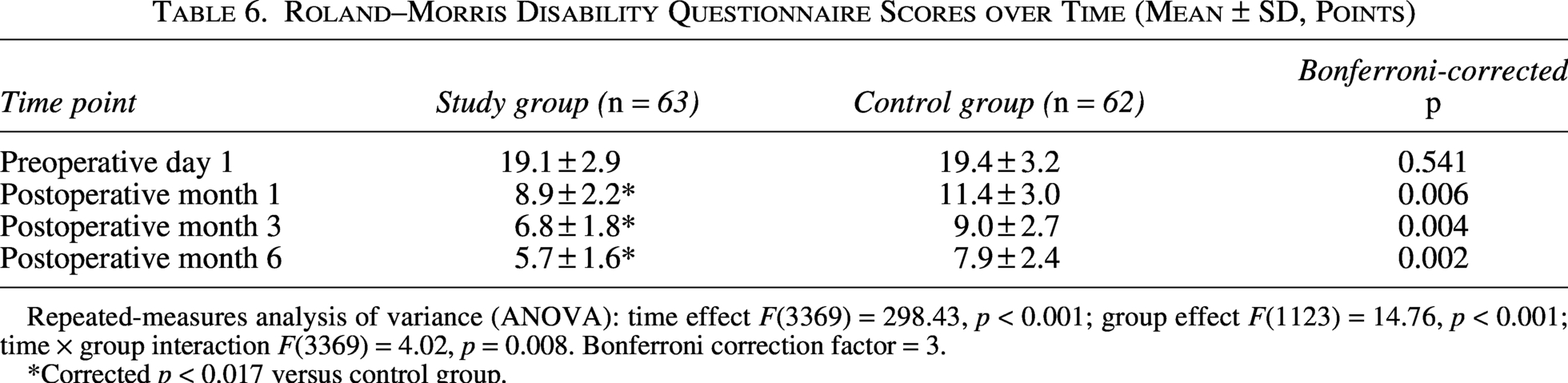
Repeated-measures analysis of variance (ANOVA): time effect F(3369) = 298.43, p < 0.001; group effect F(1123) = 14.76, p < 0.001; time × group interaction F(3369) = 4.02, p = 0.008. Bonferroni correction factor = 3.
*Corrected p < 0.017 versus control group.
Vertebral kyphotic angle
The study group demonstrated a significantly greater kyphotic angle correction at all postoperative time points (all corrected ps < 0.017), with superior immediate correction on postoperative day 1 (11.6 ± 3.3 vs. 14.1 ± 4.0°, p = 0.002) and better maintenance at 6 months (13.1 ± 3.5 vs. 15.9 ± 4.3°, p = 0.002), reflecting more effective restoration of vertebral morphology following tumor-related pathological fracture (Table 7).
Vertebral Kyphotic Angle Changes (Mean ± SD, Degrees)
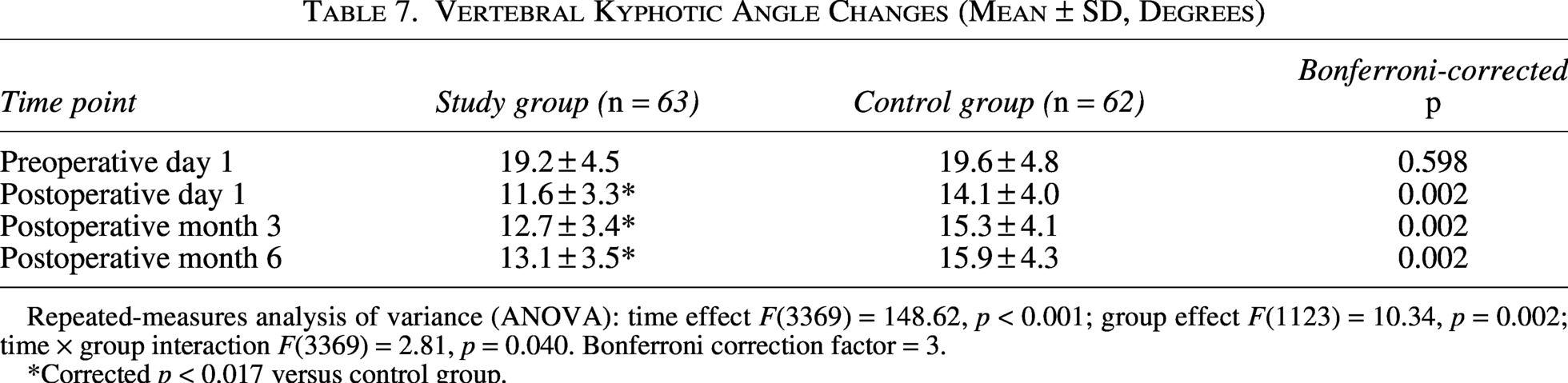
Repeated-measures analysis of variance (ANOVA): time effect F(3369) = 148.62, p < 0.001; group effect F(1123) = 10.34, p = 0.002; time × group interaction F(3369) = 2.81, p = 0.040. Bonferroni correction factor = 3.
*Corrected p < 0.017 versus control group.
SF-36 quality of life
Preoperatively, both groups exhibited markedly reduced SF-36 scores across all domains, with no significant between-group differences, reflecting the profound physical and psychosocial burden of tumor-related pathological fractures. At 6 months postsurgery, all eight SF-36 domains were significantly higher in the study group compared with the control group (all ps < 0.001; Table 8), demonstrating the comprehensive quality-of-life benefits of the curved vertebroplasty plus radionuclide approach.
SF-36 Quality-of-Life Scores (Mean ± SD, Points)
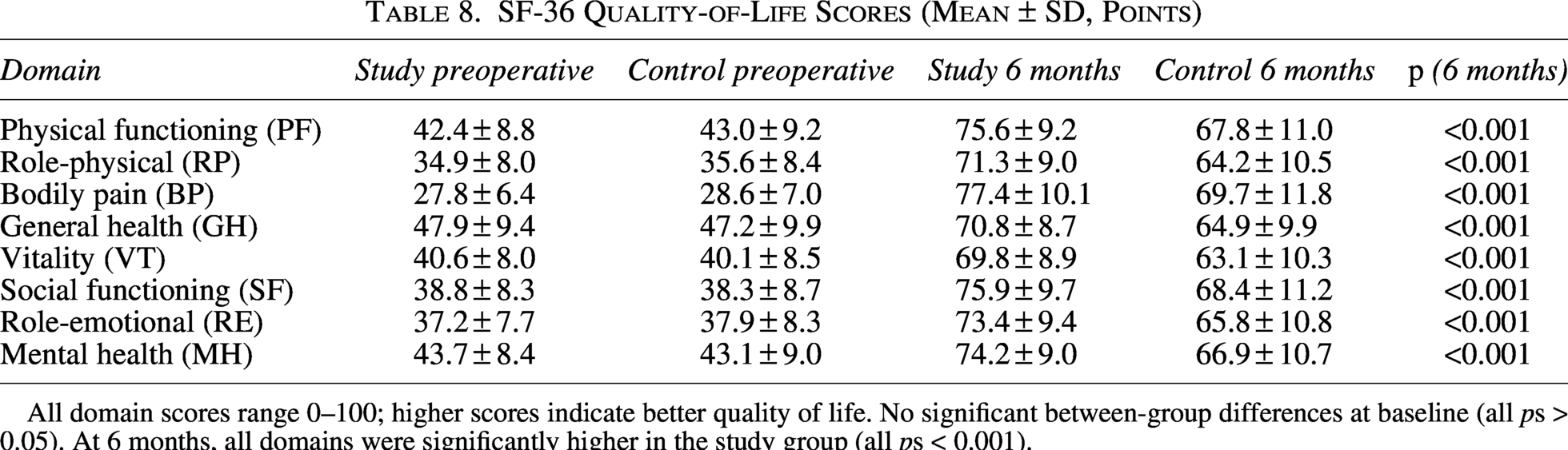
All domain scores range 0–100; higher scores indicate better quality of life. No significant between-group differences at baseline (all ps > 0.05). At 6 months, all domains were significantly higher in the study group (all ps < 0.001).
Radionuclide therapy safety
Radionuclide therapy-related safety parameters are presented in Table 9. No statistically significant between-group differences were observed in grade ≥2 hematological toxicity (14.3% vs. 12.9%, p = 0.819), radionuclide dose delay due to hematotoxicity (9.5% vs. 8.1%, p = 0.780), or postoperative radionuclide therapy continuation rate (85.7% vs. 83.9%, p = 0.779), confirming that curved vertebroplasty surgery did not adversely affect the safety or continuity of radionuclide therapy.
Radionuclide Therapy-Related Safety Parameters
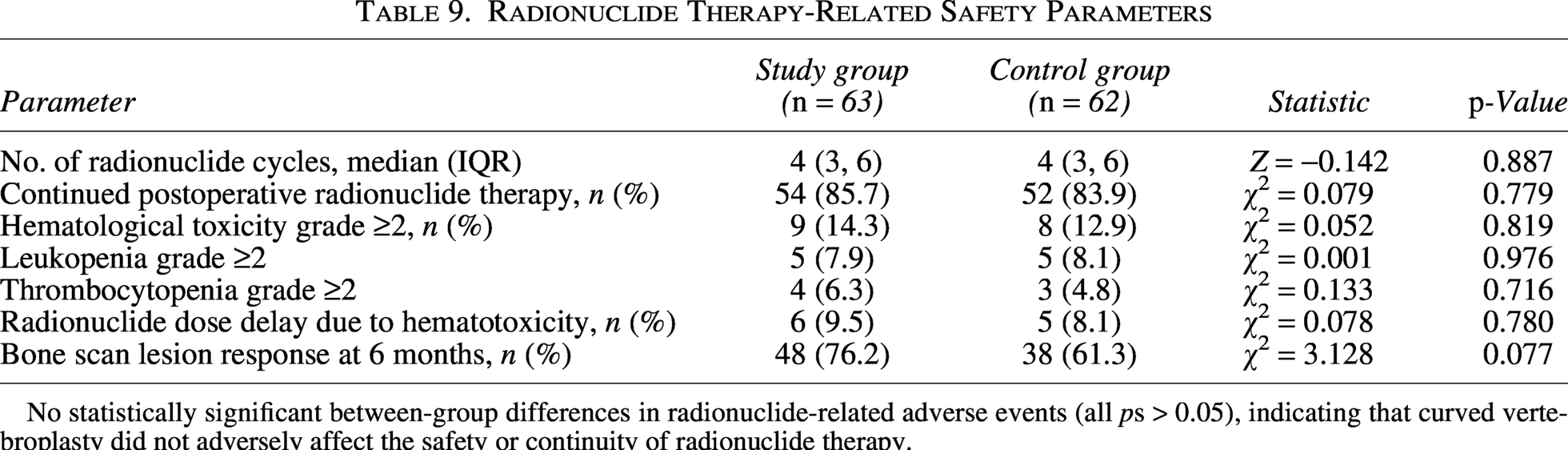
No statistically significant between-group differences in radionuclide-related adverse events (all ps > 0.05), indicating that curved vertebroplasty did not adversely affect the safety or continuity of radionuclide therapy.
Discussion
This study focused on the clinically challenging scenario of malignant tumor-related pathological vertebral fractures managed with combined surgical and systemic radionuclide therapy. The results demonstrate that, within a standardized radionuclide treatment framework, the curved vertebroplasty system achieves significantly superior mid-to-long-term pain control, vertebral morphological reconstruction, and functional recovery after pathological fracture surgery compared with conventional PVP, without compromising the safety of radionuclide therapy. These findings validate the feasibility and safety of a synergistic local surgical plus systemic radionuclide treatment strategy.
The pain mechanisms underlying tumor-related pathological vertebral fractures are considerably more complex than those of osteoporotic fractures, involving periosteal stretch, sensory nerve invasion by tumor, prostaglandin- and cytokine-mediated central sensitization, and biomechanical spinal instability. 11 Radionuclide therapy suppresses bone metastasis activity systemically, addressing the biological root cause, but typically requires 4–6 weeks before clinically meaningful pain reduction is achieved. Vertebroplasty immediately restores vertebral load-bearing stability and interrupts the mechanical nociception arising from pathological fracture micromotion, creating a temporally complementary analgesic mechanism. 12 The observation in the present study that between-group pain differences emerged principally at the 3- and 6-month time points, rather than in the early postoperative phase, suggests that the curved system’s advantage lies specifically in its capacity to maintain long-term vertebral structural stability through superior anterior–middle column coverage, rather than in immediate cement-mediated analgesic effects.
Vertebral height recovery after pathological fracture surgery is a critical measure of surgical quality. The extensive lytic destruction of the anterior–middle load-bearing column characteristic of tumor bone metastases poses a fundamental limitation for conventional straight-needle PVP, which concentrates cement near the needle trajectory and struggles to uniformly cover the full extent of lytic defects. 13 In the present study, the anterior–middle column fill rate reached 88.4% in the study group versus 74.6% in the control group (p < 0.001), directly accounting for the consistently higher vertebral height recovery rates at all time points. By restoring the axial load-bearing capacity of the lytic zone, the curved system provides structural support for the tumor-eroded vertebral body that straight-needle PVP cannot reliably achieve. 14
In comparison with other minimally invasive techniques, balloon kyphoplasty creates a cavity before cement injection and achieves reliable kyphosis correction in osteoporotic fractures; however, balloon expansion is often inadequate within the dense fibrous stroma of lytic metastatic lesions, and the technique does not permit directional targeting of specific column defects. Radiofrequency ablation-assisted vertebroplasty partially devitalizes tumor tissue before augmentation, potentially improving local tumor control, but adds procedural complexity and hardware cost. The curved vertebroplasty system offers targeted anterior-column cement delivery without the need for balloon inflation or ablation, representing a pragmatic and reproducible approach for metastatic pathological fractures that warrants direct comparative investigation in future studies.
A defining feature of this study is the establishment of a safe surgical timing protocol within the radionuclide treatment framework: Surgery was performed 14–21 d after the last radionuclide dose, corresponding to the postnadir marrow recovery window. Data from Table 9 confirm that this approach preserved the safety and continuity of radionuclide therapy, with no significant between-group differences in hematological toxicity or dose delay rates. This finding is clinically important: It demonstrates that, with appropriately timed surgical planning, minimally invasive vertebroplasty can be seamlessly integrated into an ongoing radionuclide treatment course without interrupting systemic antitumor therapy. 15
With respect to cement leakage safety, two cases of intraspinal cement extravasation occurred in the control group (3.2%) versus none in the study group. Although the overall leakage rate difference did not reach statistical significance, likely due to limited sample size, the absence of intraspinal leakage in the curved group suggests that achieving well-distributed anterior–middle column filling may reduce the hydrostatic pressure gradient driving cement toward the posterior vertebral wall and epidural space, a mechanism worthy of further investigation in larger series. 16
The comprehensive SF-36 analysis revealed that tumor-related pathological fractures inflict profound impairment across all health dimensions before treatment. The study group’s superiority across all eight SF-36 domains at 6 months, encompassing not only physical functioning and bodily pain but also mental health, role-emotional, and social functioning dimensions, reflects the holistic benefit of more effective pain control and functional recovery conferred by the curved vertebroplasty plus radionuclide strategy. The observed between-group differences in all the eight SF-36 domains exceeded the published minimal clinically important difference thresholds, confirming that the quality-of-life benefits are clinically meaningful rather than merely statistically significant. 17
Several limitations of this study warrant acknowledgment. The retrospective design is susceptible to selection bias; the sample size is relatively small and follow-up was limited to 6 months, precluding assessment of tumor progression effects on long-term vertebral stability; cost-effectiveness was not evaluated; and the potential differential impact of various primary tumor histologies and metastasis subtypes on surgical outcomes requires dedicated subgroup analyses in future studies In addition, the absence of randomization means that unmeasured confounders cannot be excluded despite baseline comparability, and the single-center design limits generalizability across institutions with differing surgical volumes and nuclear medicine protocols. Regarding diagnostic confirmation, 71.2% of fractures were histologically confirmed while the remaining 28.8% were diagnosed on the basis of convergent imaging findings in the context of known systemic malignancy; this distinction is acknowledged as a potential source of diagnostic heterogeneity. A formal cost-utility analysis incorporating quality-adjusted life years is planned as part of the prospective multicenter extension study. 18 Prospective multicenter randomized controlled trials incorporating tumor-specific outcomes such as overall survival and skeletal-related events are needed to provide higher level evidence. Future research should also explore the integration of SPECT/CT image-guided navigation for preoperative planning of curved needle trajectories targeting specific lytic zones, and the applicability of this combined strategy with emerging radiopharmaceuticals such as 177Lu-PSMA and 177Lu-DOTATATE.19,20
Conclusion
In the treatment of malignant tumor-related pathological vertebral fractures, the curved vertebroplasty system combined with targeted radionuclide therapy is significantly superior to conventional PVP combined with radionuclide therapy in postfracture pain control, vertebral morphological reconstruction, spinal functional recovery, and quality-of-life improvement, without increasing radionuclide-related adverse events or disrupting the safety and continuity of radionuclide treatment. The precise anterior–middle column bone cement filling achieved by the curved system, combined with the systemic targeted antitumor effect of radionuclide therapy, establishes a synergistic precision treatment model of local surgical reconstruction plus systemic radionuclide therapy, providing important clinical evidence for the minimally invasive comprehensive management of tumor-related pathological vertebral fractures.
Authors’ Contributions
H.Z. and L.S. conducted the primary research, including patient enrollment, surgical procedures (curved vertebroplasty and conventional PVP), data collection, and drafted the article. Z.Z., as the corresponding author, designed the study, supervised the entire research process, performed the statistical analysis, and takes full academic responsibility for the integrity of the data and the accuracy of the data analysis. All authors have read and approved the final article.
Ethics Statement
This study was approved by the institutional review board of Beijing Long Fu Hospital (approval number: LFYYLL-2021-10). The research was carried out in compliance with the Declaration of Helsinki and relevant Chinese ethical regulations for clinical research.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.