
Abstract
Keywords
Introduction
Attention, memory, and motivation are critical for learning. The inattention, problems with following instructions, poor planning/executive dysfunction, and other symptoms that characterize ADHD thus increase the risk for learning disorders (LDs) in children with this syndrome (Barkley, 1997; Bental & Tirosh, 2007; Miranda-Casas, Melia-de Alba, Marco-Taverner, Rosello, & Mulas, 2006; Pineda et al., 1998). The comorbidity of ADHD and LD varies from 25% to 40% in selected groups (Willcutt & Pennington, 2000). The pathogenesis causing ADHD probably affects frontostriatal circuits and central dopaminergic and noradrenergic pathways (Martin-González et al., 2008).
A genetic polymorphism of ADHD is not yet defined (De Luca, Muglia, Jain, & Kennedy, 2004).
According to the Diagnostic and Statistical Manual (American Psychiatric Association, 2000), LDs are characterized by childhood academic difficulties, particularly in the development of reading, writing, and mathematical skills. LD subtypes overlap in some individuals, whereas others experience isolated deficits that have minimal effect on their work or social activities. Boys are more likely than girls to be affected by LDs (by a ratio of 3:1 to 5:1). These may occur in combination with attention and behavioral problems, with effects extending into adult life, to the detriment of school, work, recreation, daily habits, and social interactions (Kronenberger & Dunn, 2003). LDs are complex disorders of multiple causality, which apparently include a genetic component (McCann et al., 2008). Maternal hypothyroidism (Vermiglio et al., 2004), toxic exposure during pregnancy, complications of gestation or delivery, and neonatal distress (prematurity, low birth weight, jaundice, and perinatal hypoxia) (Colletti, 1979; Rodrigues, Mello, & Fonseca, 2006) are additional risk factors for LD. Some authors report disturbances in brain circuits involving neurotransmitters, implying potential opportunities for pharmacological treatment (Grizenko, Bhat, Schwartz, Ter-Stepanian, & Joober, 2006; Liu et al., 2008).
Learning requires the capacity to assimilate information, store it in both short- and long-term memory, and apply the newly acquired knowledge to particular problems. Therefore, tests for LD quantify among other variables such as language, visual–perceptive, motor coordination, visual–motor, visual–spatial problem solving, and social interaction skills.
ADHD frequently jeopardizes cognitive, school, and social performance, especially as academic and social demands increase (Zametkin & Ernst, 1999). It affects approximately 5.3% of children and 4.4% of adults, depending on the population, and disproportionately occurs in men (the male:female ratio ranges from 2:1 to 9:1 (Cardo & Servera-Barcelo, 2005; Cornejo et al., 2005; Montiel-Nava et al., 2002; Polanczyk & Jensen, 2008). ADHD may result from abnormal central nervous system development due to biological or environmental factors. It often coexists with other conditions (Banerjee, Middleton, & Faraone, 2007; Ellison-Wright, Ellison-Wright, & Bullmore, 2008; Strang-Karlsson et al., 2008), including LD, behavior disorders, anxiety, depression, bipolar disorder, Gilles de la Tourette syndrome, and oppositional defiant disorder (Rappley, 2005).
There is a dearth of comparable data on ADHD and LD in Latin America, an enormous region that is geographically, linguistically, and culturally different from the populations from which the preceding generalizations derive. The objective of the present study was to analyze the potential co-occurrence of ADHD and LD in a sample of primary schoolchildren from several socioeconomic strata and districts of Bogotá, Colombia, who were evaluated by the authors in 2004-2005.
Method
The data presented here derive from a cross-sectional study of a nonrandom sample of 5- to 12-year-old children, from different socioeconomic backgrounds in private and public primary schools in Bogotá, Colombia (circa 7 million inhabitants), which was designed to detect and quantify the prevalence of childhood neurological pathologies (including ADHD and LD) (Velez van Meerbeke, Talero-Gutierrez, & Gonzalez-Reyes, 2007; Velez van Meerbeke, Talero-Gutierrez, Gonzalez-Reyes, & Ibañez, 2008). The study was approved by the Universidad del Rosario Ethics Committee and parents provided informed consent. It represents a convenience sample of schools serving mainly low to medium income families.
The parents of the 10,259 children registered in these schools responded to a questionnaire inquiring about known or possible neurological and developmental disorders (especially ADHD and LD) in their families (including the children under evaluation as well as demographic, social, and economic variables). Teachers acquainted with the children participated in a complementary survey to identify those with possible or known disorders, including low academic performance and behavioral or attention disturbances.
In this way, we identified and selected from the total population those children exhibiting any type of learning difficulty in reading, mathematics, or writing, or general underperformance in comparison with their age and grade, as well as children characterized by either parents or teachers as presenting any of the typical symptoms of attention impairment (restlessness, difficulty following instructions, inattention, lack of concentration, and low academic performance), who comprised the target sample for this study (N = 1,026). Those with neurological disorders such as a cognitive disability (i.e., mental retardation, cerebral palsy, or severe sensory handicaps such as blindness and deafness) were excluded from the analysis.
During the second stage of the study, these children were individually assessed at their schools with the DSM-IV checklist approved for Colombia (Pineda, Henao, et al., 1999; Pineda, Ardila, et al., 1999) (see appendix) and a medical history taken, including a clinical neurological examination. Parents and teachers using this checklist scored their perceptions of the children’s average observed behavior over the past 6 months. This is a screening instrument for childhood ADHD and is well correlated with other more specific and objective tests (Pineda et al., 2005). McBurnett, et al. (1999) studied the reliability of this instrument, evaluating the answers provided by parents and teachers and found a Cronbach’s alpha value of .80 for both inattention and hyperactivity.
Children scoring 6 or higher for the symptoms evaluated in each of the modules of the checklist for inattention or hyperactivity-impulsivity were identified operationally as potential ADHD. They were further classified into three subtypes: (a) predominantly inattentive type (ADHD-A) if they scored ≥6/9 on the inattention list, (b) predominantly hyperactive-impulsive type (ADHD-H) if they scored ≥6/9 on the hyperactivity-impulsivity list, and (c) combined disorder (ADHD-C) if they scored high on both.
In addition, children with poor academic performance took standard tests (in Spanish) to detect possible LDs. These were administered to same-grade or same-age groups by a speech therapist and an occupational therapist trained in the application of these instruments and supervised by one of the authors (CT, AV). General and Differential Aptitudes Battery (BADyG) is a test adjusted to age or grade that has been developed to evaluate different cognitive skills (Yuste Herranz, 1998). The following subtests that allow evaluation of general development of cognitive/language skills and learning abilities were applied: basic general information, verbal reasoning, verbal concepts, visual–auditory memory, and the semantic component of verbal intelligence and motor perceptual skills related to the basic learning process.
The Beery-Buktenica Developmental Test of Visual Motor Integration (VMI), which measures motor coordination, visual perception, and constructional abilities, was also used (Beery, 1997).
The present analysis is based on the 834 children who were completely assessed and were considered at risk of having ADHD and/or LD (Figure 1). The tests are graduated by levels according to age and difficulty, with percentiles established to help interpret the results. As there was a large spread of age in each grade, we decided not to group according to age or gender and present instead a global evaluation of the results.
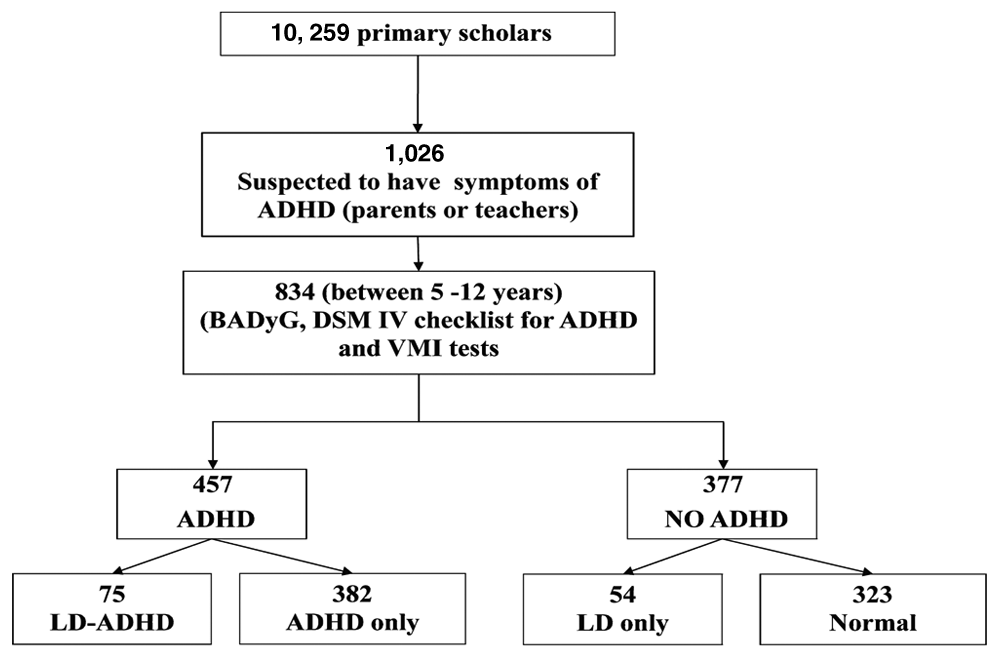
Study flowchart (“ADHD” indicates high DSM-IV ADHD checklist results and “LD” indicates low scores on the BADyG and VMI tests)
Children were grouped into four categories based on the test results: (a) normal, (b) at risk for LD only (LD) (BADyG results below 15th percentile and the VMI written tests results below 15th percentile), (c) high scoring on ADHD checklist only (ADHD) (DSM-IV checklist of ≥6/9 in inattention or hyperactive-impulsive scores), and (d) students both at risk for LD and high-scoring on the ADHD checklist (LD-ADHD).
For analyses of the associations, we used the χ2 test without Pearson’s correction (expected values more than 10), the χ2 test with Yates’s correction for continuity (expected values between 5 and 10) or Fisher’s exact test (expected values lower than 5). The magnitude of the association was also studied with disparity ratios (odds ratio [OR]) with 95% confidence intervals (CI). We used 5% significance for statistical tests; only significant relationships are reported. Stratified analyses were used to evaluate the relationship of different variables. Pearson’s regression coefficient was used for determining correlations among numerical variables. LD-associated variables were evaluated using stepwise logistic regression analysis. Variables included in the model had associated probability of less than 10%.
Results
The 834 sample children ranged in age from 5 to 12 (mean = 8.09 years) and in grade level from preschool through 5th grade (Figure 2). There were more boys than girls (N = 509, 61%).

Age distribution according to school grade in sample children
According to the criteria defined earlier, 457 had ADHD (attention deficit [AD] = 203, combined deficit [CD] = 195, and hyperactive-impulsive deficit [HD] = 69). Of these, 392 had only ADHD and 75 had both ADHD + LD. There were 54 children with LD but without ADHD (Figure 1).
There were 308 boys (67%) with ADHD; a ratio of 2:1 over girls (p = .00). There were also more boys with HD (3.9:1 boys:girls; N = 55/14; p = .00) and with CD (4:1; N = 148/37; p = .00). No significant gender differences in AD (105/98), in LD (N = 67/62), or in ADHD + LD (N = 43/32) were found.
A total of 456 children scored poorly on the VMI. More boys than girls were in this group (N = 284/172; ratio = 1.7:1; p = .00).
Other significant associations or differences were found in the following variables:
AD with LD (p = .02; OR = 1.85; 95% CI [1.21, 2.83]). There is a significant gender difference, with boys more frequently affected than girls (p = .024; OR = 1.95; 95% CI [1.06, 3.56]).
HD was inversely correlated with LD (p = .005; OR = 0.23; 95% CI [0.06, 0.77]); this relationship occurs significantly more in boys than in girls (p = .024; OR = 1.95; 95% CI [1.06, 3.56]).
ADHD was significantly related to poor VMI test scores (p = .024; OR = 1.37; 95% CI [1.03, 1.82]) and girls presented significantly poorer scores (p = .05; OR = 1.88; 95% CI [1.18, 3.0]). ADHD + LD was also significantly related to poor VMI scores (p = .03; OR = 1.73; 95% CI [1.02, 2.94]).
There was a significant relationship between the analog relations part of BADyG and AD (p = .01). HD was not significantly related to scores on the other components of the tests. It is noteworthy, though, that 96.4% of the HD children had high performance on the visual–auditory memory test (p = .001).
Logistic regression analysis revealed the following high-risk factors in this group associated with the presentation of LD symptoms: presenting symptoms of AD, being an 8+ year old boy, and scoring poorly on the VMI test (Table 1). Grade level was not included in this analysis due to colinearity (88% Pearson’s correlation).
Logistic Regression Analysis for LD
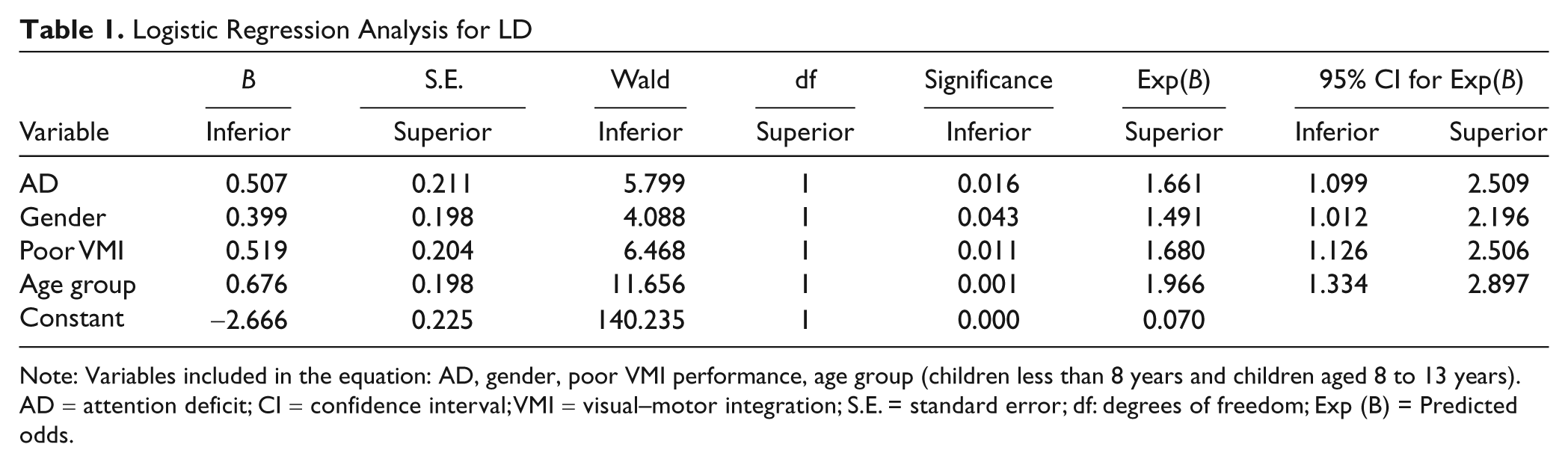
Note: Variables included in the equation: AD, gender, poor VMI performance, age group (children less than 8 years and children aged 8 to 13 years). AD = attention deficit; CI = confidence interval; VMI = visual–motor integration; S.E. = standard error; df: degrees of freedom; Exp (B) = Predicted odds.
Discussion
ADHD and LD are the most frequently reported neurological conditions in schools (Mayes & Calhoun, 2007). Prevalence of ADHD varies from 1% to 22%, taking into account differences in age, geographical region, social characteristics, and study design (Benjasuwantep, Ruangdaraganon, & Visudhiphan, 2002; Pineda et al., 2001; Skounti, Philalithis, & Galanakis, 2007; Wolraich et al., 2003). Definitive quantitative data for LD are lacking, especially in developing countries such as Colombia, but the prevalence of LD is similar to that of ADHD; it is a common reason for clinical consultations. The 1997-1998 U.S. National Health Survey reported 3% prevalence for ADHD, 4% for LD, and 4% for the association of both (Pastor & Reuben, 2002). In Colombia, a cross-sectional study for characterizing neuropediatric pathology occurrence reports 5.7% prevalence of symptoms of ADHD and 5.4% for low scores on learning tests (Velez van Meerbeke et al., 2008). In the present study, 8% of the total population of the sampled schools presented symptoms of a combined condition including ADHD and LD. A relationship between the two disorders has been previously reported (Cantwell, 1996; McGillivray & Baker, 2009; Zametkin & Ernst, 1999).
Learning problems are one of the most important comorbidities of ADHD (Seidman et al., 2006). Children with ADHD may have lower intellectual ability than paired age and grade controls, and this typically has a negative effect on school, social, or work performance (Frazier, Demaree, & Youngstrom, 2004; Wahlstedt, Thorell, & Bohlin, 2008). However, not all ADHD children manifest LD. The ADHD-A subtype is usually associated with academic underperformance (Elia, Ambrosini, & Rapoport, 1999; Willcutt & Pennington, 2000), whereas children with ADHD-H are more likely to develop behavior disorders or problems that undermine their academic performance even though they do not have cognitive deficits. ADHD-C children usually have average academic and social performance. Our findings from a Colombian population show a relationship between poor academic achievement and the AD component but not the hyperactive-impulsive component.
Linguistic skills, including verbal reasoning, visual and auditory memory, and VMI, are essential for the successful acquisition of reading and writing proficiencies in children. Impairment of these skills secondary to development disorders or environmental factors is reflected in impaired academic performance. Learning difficulties in children with attention disorders, but without inherent problems in these linguistic or perceptual skills, may be indirect consequences of their inattention rather than difficulties related to the underlying processes related to learning acquisition.
Low VMI performance in children with ADHD symptoms only or with both ADHD + LD symptoms is consistent with the hypothesis of Korkman and Pesonen (1994) that VMI difficulty in the absence of perceptual deficiencies could be evidence of a motor coordination deficiency associated with an overall tendency of development disorders.
The high visual–auditory memory test scores observed in the children with only ADHD-H provides a clue as to why some of them are able to get good academic grades. Their impairment appears to be an executive dysfunction that does not interfere with perceptual and memory skills. Martin-González et al. (2008), in a study of auditory–verbal and visual–perceptual memory in patients with ADHD-C, did not find differences in performance with a normal control group.
The sampling methodology used in this study was nonrandom and thus caution is appropriate in extrapolating results to the general population; nevertheless, both private and public schools from different socioeconomic strata were included and the sample size was large enough to be generally representative of Colombian schoolchildren from Bogotá. Although the tests applied provided information about various skills (linguistic, perceptual, and visual–motor), as well as attention and memory components, they were administered to groups. Individual, more thorough tests could be helpful for obtaining a more precise evaluation of each child and for providing additional insight into the relationships among ADHD, learning difficulties, and behavioral problems.
The value of these findings lies in the additional quantitative evidence they provide for a relationship between ADHD and LD, particularly regarding detailed aspects such as verbal reasoning, visual–auditory memory, and VMI in a previously unstudied population. They make clear the importance of identifying the dysfunctional components of ADHD subtypes in designing successful treatment strategies and in reducing academic and social costs.
Footnotes
Appendix
ADHD Checklist Based on DSM-IV
| Inattention 1. Does not pay attention to details and makes careless errors doing tasks 2. Has difficulties paying attention to tasks and games 3. Appears not to listen to what he or she is told 4. Does not follow instructions or does not finish tasks in school or chores at home in spite of understanding them 5. Has difficulties in organizing activities 6. Avoids doing tasks or things that require effort 7. Loses his or her school supplies or the things necessary for carrying out his or her activities 8. Easily distracted by irrelevant stimuli 9.Forgetful of daily activities Hyperactivity-impulsivity 10. Restless, moving hands and feet when seated 11. Gets up in class or in other situations when he or she should remain seated 12. Runs around and climbs in inappropriate situations 13. Experiences difficulties in relaxing or playing games that require being still 14. Always moving, as if there’s an internal motor always running 15.Talks too much 16. Answers or acts without having processed the questions 17. Experiences difficulties waiting in lines or waiting for a turn when playing games 18.Interrupts others’ conversations or games Total score: ______________ |
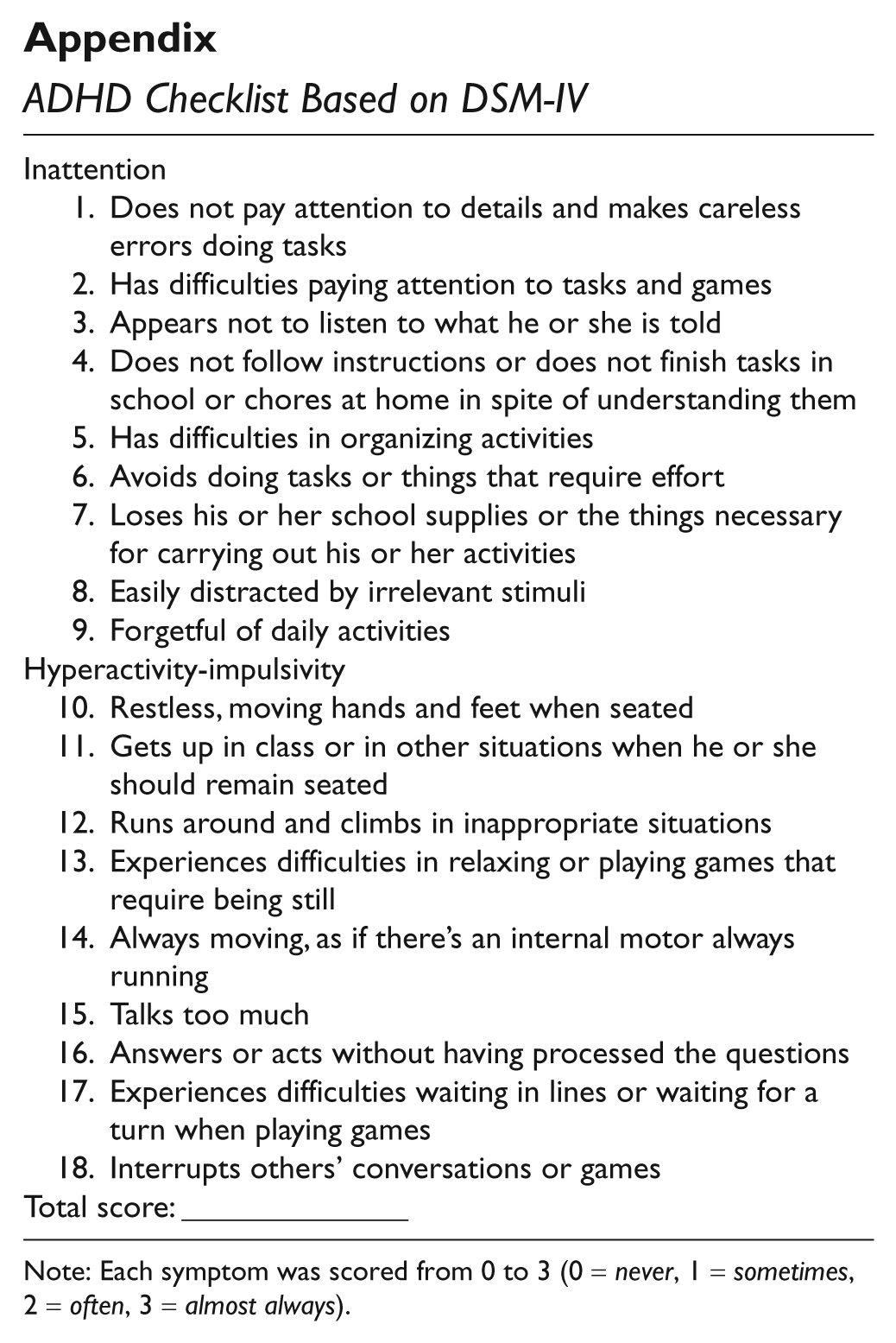
Note: Each symptom was scored from 0 to 3 (0 = never, 1 = sometimes, 2 = often, 3 = almost always).
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.