
Abstract
Since its earliest description by Still back in 1902, ADHD was considered a childhood-specific disorder, thought to disappear or diminish toward adolescence (Hill & Schoener, 1996). However, ADHD is now recognized as a disorder that persists into adolescence and further into adulthood in 40% to 70% of all cases (August, Braswell, & Thuras, 1998; Mannuzza et al., 1991; Weiss, Hechtman, Milroy, & Perlman, 1985; Weiss, Hechtman, Perlman, Hopkins, & Wener, 1979), affecting personal, social, academic, and professional development. In fact, ADHD-prevalence studies indicate that about 4% of the adult population suffers from this disorder (Faraone, Sergeant, Gillberg, & Biederman, 2003; Heiligenstein, Conyers, Berns, & Miller, 1998; K. Murphy & Barkley, 1996).
Although the expression of ADHD in adults resembles the set of symptoms identified earlier in childhood, clinical signs are influenced by the changes that occur as patients grow older. In accordance, several studies have shown that toward adolescence and adulthood, hyperactivity and impulsivity symptoms tend to diminish, whereas symptoms of inattention persist (Hart, Lahey, Loeber, Applegate, & Frick, 1995; Millstein, Wilens, Biederman, & Spencer, 1997).
Besides the impaired performance on tests of attention (Biederman, Mick, & Faraone, 2000) and inhibition (Barkley, 1997), executive functions seem to be the most severely impaired cognitive domain in adult ADHD patients, affecting planning, self-monitoring, working memory, flexibility, and set shifting, among others. The dysexecutive profile of ADHD patients is qualitatively, though not always quantitatively, similar to the pattern observed in adults with frontal lobe damage (Johnson et al., 2001; Shue & Douglas, 1992)
Although the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 2000) proposes three possible types of ADHD—predominantly inattentive type, predominantly hyperactive-impulsive type, and a combined type—recent studies have found little to no differences between ADHD adult subtypes in terms of their performance on neuropsychological tests (Schweitzer, Hanford, & Medoff, 2006; L. Tucha et al., 2008; O. Tucha, Mecklinger, et al., 2006; O. Tucha, Walitza, et al., 2006). Adult patients who fulfill DSM-IV criteria for ADHD but perform normally on neuropsychological tests are not unusual in clinical practice. For example, it is not uncommon for some successful professionals to consult at a memory clinic reporting difficulties in “memory,” especially with increase of daily life stress and more responsibilities or just because her or his kid was diagnosed with ADHD and, although she or he compensated it for many years, the symptoms are similar to those of the kid. Many such patients fulfill criteria for ADHD, though they were not diagnosed during their childhood, and perform within normal on neuropsychological assessment. Moreover, although executive functions seem to be primarily impaired in ADHD, real-life difficulties experienced by patients may go undetected using standard executive tests. This may be due to the fact that in classical tests of executive function, the examiner provides the structure, organization, guidance, plan, and monitoring necessary for optimal performance, soon becoming the patient’s own executive system (Gioia & Isquith, 2004) and thus lowering the sensitivity of these tests to detect executive dysfunction (Gregory et al., 2002). To overcome this, our group has recently demonstrated (Torralva, Roca, Gleichgerrcht, Bekinschtein, & Manes, 2009) the usefulness of incorporating executive tests that are more “ecological” in nature, for they resemble real-life demands more closely, in evaluating executive functioning in patients with frontal deficits.
With this growing need for tests that resemble real-life scenarios’ cognitive demands, the present study examined the neuropsychological performance of ADHD patients and healthy controls on both a standard neuropsychological battery, and ecological and highly demanding executive tasks. Patients were classified as showing either a high- or a low-functioning profile based on their standard neuropsychological examination.
Method
Participants
ADHD patients were evaluated during admission interviews to the specialized clinic of adult ADHD at the Institute of Cognitive Neurology (INECO, Buenos Aires, Argentina) where they underwent a detailed examination that include neuropsychatric assessment, neurological examination, and neuropsychological evaluation. Questionnaires were incorporated in the regular neuropsychiatric examination. Relatives or significant others were usually integrated in the assessment interviews, during which they completed the informant-based version of questionnaires. ADHD diagnosis based on the DSM-IV criteria was made by two experts (AL and FM). While DSM-IV criteria are oriented toward diagnosis in children, they provide a standard frame to include patients as previously done by other studies in ADHD adults (e.g., Torrente et al., 2010). All participants were assessed before initiating treatment with specific drugs for ADHD. Patients (N = 117) fulfilled DSM-IV criteria for ADHD and were examined to rule out other possible comorbid psychiatric or neurological disorders (exclusion criteria). Healthy control (n = 21) were recruited from a larger pool of volunteers who had neither a history of abuse of recreational drugs nor a family history of neurodegenerative or psychiatric disorders. All participants gave their informed consent prior to inclusion in the study.
Materials and Procedure
The study was approved by the ethics committee at the Institute of Cognitive Neurology in accordance with international principles for human medical research. Patients initially completed a series of psychiatric and behavioral questionnaires to establish a profile of clinical symptoms—including the Barkley Scale (Barkley, 1997) for inattention and hyperactive profiles, and the Beck Depression Inventory II (Beck, Steer, Ball, & Ranieri, 1996)—to control for mood disturbances. The neuropsychological examination included a standard battery and a series of experimental tests included in this study to detect executive dysfunctions in a more ecological or highly cognitive demanding way. Patients were assessed in two different sessions on two different days to avoid the influence of cognitive fatigue on task performance.
Standard neuropsychological battery
Participants completed a thorough neuropsychological battery assessing (a) estimated premorbid IQ with the Word Accentuation Test–Buenos Aires (WAT-BA; Burin, Jorge, Arizaga, & Paulsen, 2000); (b) general cognitive status with the Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975) and the Addenbrooke’s Cognitive Examination (ACE; Mathuranath, Nestor, Berrios, Rakowicz, & Hodges, 2000); (c) verbal memory through the Rey Auditory Verbal Learning Test (RAVLT; Rey, 1941), the logical memory subtest of the Wechsler Memory Scale–Revised (WMS-R; Wechsler, 1997), and nonverbal memory with the Rey Complex Figure Test (Rey, 1941); (d) attention with the forward digits span task of the WMS-R (Wechsler, 1997) and the Trail-Making Test Part A (TMT-A; Partington & Leiter, 1949); (e) language with the abbreviated version of the Boston Naming Test (Kaplan, Goodglass, & Weintraub, 1983) for naming, the Token Test (Spreen & Benton, 1977) for comprehension, and the semantic fluency task (Lezak, Howieson, & Loring, 2004) for fluency; and (f) executive function using the backward digits span test (Wechsler, 1997), Part B of the Trail-Making Test (TMT-B; Partington & Leiter, 1949), the letters and numbers ordering test (Wechsler, 1981), the phonological fluency task (Lezak et al., 2004), and the modified version of the Wisconsin Card Sorting Test (WCST; Nelson, 1976).
Experimental executive tasks
The experimental tasks used in this study included the following: the hotel task (adaptation from Manly, Hawkins, Evans, Woldt, & Robertson, 2002) as well as the inhibitory control (Go-No Go) and the working-memory subtests of the Test of Attentional Performance (TAP; Zimmermann & Fimm, 1994). The latter is a computerized battery of tests aimed at detecting attention and working-memory deficits using highly demanding tasks. Scoring of both TAP subtests included the percentage of correct responses as well as commission (incorrect responses) and omission (ignored responses) errors. The hotel task has been recently described for the first time as an assessment tool, rather than as a sole rehabilitation tool (Manly et al., 2002) by our group (Torralva et al., 2009). The task comprises recreating the scenario of a job interview at a hotel. The examiner instructs the participant as follows:
In this task, you are asked to imagine that you are working in a hotel. Your manager is keen for you to try each of these five everyday activities during the next 15 min so that you can get a “feel” for the tasks—and make an informed estimate of how long each task would take to complete. Your main goal is to attempt to do each of these five tasks over the next 15 min. There are five main tasks to do. Each of the tasks may take longer than 15 min to complete on its own, so there is no way that you will be able to complete all of them. The most important thing is to try and do a little of each task—spending as much time on each as possible within the total time available.
The stimuli needed for each task are distributed on a table. A written summary of the task is placed on top of the stimuli to reduce working-memory loading. Tasks included arranging individual bills by guest name, grouping coins according to their country of origin, looking up commercial telephone numbers in the local yellow pages, sorting conference name tags alphabetically, and proofreading a hotel leaflet for typos. Scoring of the hotel task included the number of main tasks attempted (out of five), the number of tasks correctly executed (out of five), and deviation from optimal time allocation (in seconds).
Statistical Analysis
Participants in the ADHD group were classified as showing either a high-functioning (Hi-ADHD) or a low-functioning (Lo-ADHD) neuropsychological profile. Patients were examined individually and categorized according to a strict set of criteria. Initially, patients whose performance on any of the standardized tests included in the neuropsychological battery—the logical memory WMS-R (immediate and delayed scores), the RAVLT (immediate, delayed, distractor list, and recognition scores), the Rey figure (immediate and delayed scores), the semantic and phonological fluency tasks, or the TMT-A and TMT-B—was 1.5 or more standard deviation units below the normalized scores were immediately assigned to the Lo-ADHD group. From the remaining ADHD patients, the following conditions were used as inclusion criteria for the Lo-ADHD group: (a) Boston Naming Test score of 17 (out of 20) points or lower, (b) Token Test score of 29 (out of 32) points or lower, (c) five or fewer digits achieved on the forward digit span task, (d) four or fewer digits achieved on the backward digit span task, and (e) four or fewer categories achieved on the WCST.
Neuropsychological performance was compared between Hi-ADHD, Lo-ADHD, and control groups using one-way ANOVA followed by Tukey’s honestly significant difference post hoc comparisons test when appropriate. When analyzing categorical variables (e.g., gender, Figure Rey recognition), the Freeman–Halton extension of the Fisher exact probability test for 2 × 3 contingency tables was used.
Results
Classification of ADHD Patients
Under the previously described criteria, 34 (29.1%) patients were categorized as Hi-ADHD and 83 (70.9%) patients were categorized as Lo-ADHD, setting a Lo- to Hi-ADHD ratio of 2.44.
Neuropsychological Profile
Table 1 summarizes general demographic information and neuropsychological test results for all three groups. Patients were successfully matched for age, F(2, 135) = 0.85, p = .43, and gender, χ2 = 2.1, df = 2, p = .35. While years of education significantly differed between the groups, F(2, 135) = 7.82, p < .05, particularly between controls and Lo-ADHD (p < .001) and Hi-ADHD (p < .01), premorbid intellectual performance was similar, F(2, 135) = 0.87, p = .45.
Demographic Information and Neuropsychological Background Tests for Hi-ADHD, Lo-ADHD, and Control Groups
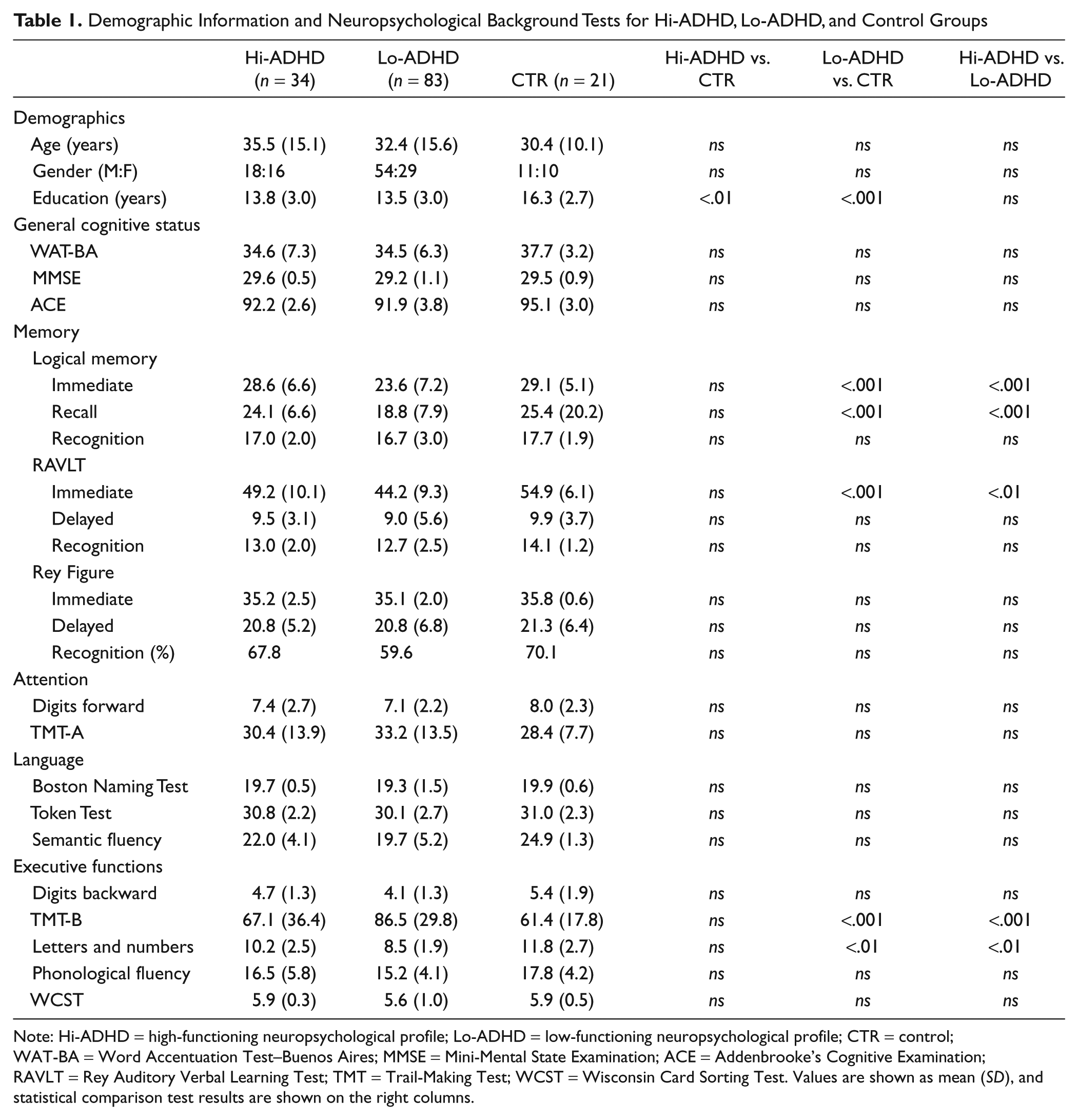
Note: Hi-ADHD = high-functioning neuropsychological profile; Lo-ADHD = low-functioning neuropsychological profile; CTR = control; WAT-BA = Word Accentuation Test–Buenos Aires; MMSE = Mini-Mental State Examination; ACE = Addenbrooke’s Cognitive Examination; RAVLT = Rey Auditory Verbal Learning Test; TMT = Trail-Making Test; WCST = Wisconsin Card Sorting Test. Values are shown as mean (SD), and statistical comparison test results are shown on the right columns.
The groups performed similarly on general cognitive status screening tests. On memory tasks, a significant difference was observed for the immediate, F(2, 135) = 9.42, p < .001, and recall, F(2, 135) = 8.57, p < .01, scores of the WMS-R logical memory test and the immediate score of the RAVLT, F(2, 135) = 10.6, p < .001. Post hoc comparisons showed a similar pattern for all variables: the Lo-ADHD group patients differed significantly from both Hi-ADHD and control participants, while these two groups showed a similar performance (corresponding p values shown on Table 1). Performance on classical executive tests were significantly different on the TMT-B, F(2, 135) = 9.74, p < .001, and the letters and numbers test, F(2, 135) = 7.45, p < .05. Again, the Lo-ADHD group differed significantly from the control and Hi-ADHD groups, while the latter did not show significant differences between themselves (corresponding p values shown on Table 1). No other significant differences were found between the groups on other standard neuropsychological battery tests.
Experimental Tasks Performance
Time deviation on the hotel task was similar across the groups, F(2, 135) = 0.81, p = .45, but the number of tasks attempted, F(2, 135) = 5.36, p < .01, and the number of tasks completed correctly, F(2, 135) = 7.01, p = .001, were significantly different across the groups. More specifically, control participants attempted a significantly higher number of tasks than did Hi-ADHD (p < .01) and Lo-ADHD (p < .01) participants. The control group also correctly executed a significantly higher number of tasks than did Hi-ADHD (p = .001) and Lo-ADHD (p < .001) groups. Hi- and Lo-ADHD participants did not differ significantly on any of the hotel task scores (Figure 1).

Mean (+ SEM) number of tasks attempted and performed correctly as well as time deviation on the hotel task
Performance on the inhibitory control subtest of the TAP did not differ significantly between the groups for the number of correct responses, F(2, 135) = 1.21, p = .33; omitted trials, F(2, 135) = 0.65, p = .52; or commission errors, F(2, 135) = 0.76, p = .47. On the working-memory test, however, the groups differed significantly on the three same variables—correct responses: F(2, 135) = 5.9, p < .01; omission errors: F(2, 135) = 3.38, p = .037; and commission errors: F(2, 135) = 3.9, p = .022. Post hoc comparisons showed that the control group differed significantly from both Hi-ADHD and Lo-ADHD (p < .01 for all cases) groups, whereas the patient subgroups did not differ between themselves (Figure 2).
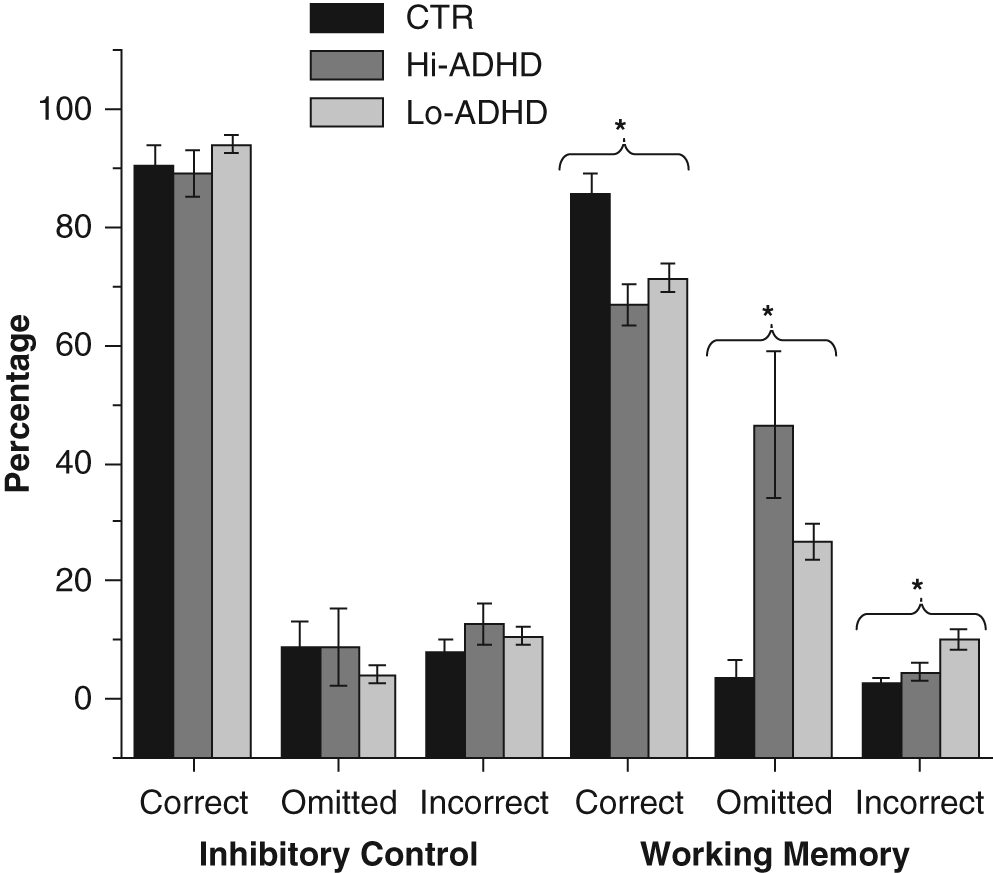
Mean (± SEM) percentage of correct, omitted, and incorrect responses on the inhibitory control and working memory computerized subtests of the Test of Attentional Performance battery
Discussion
The present study demonstrated that adult ADHD patients who showed within-normal performance on standard neuropsychological assessment that include classical executive tasks performed similarly to individuals with frontal lobe damage in ecological and highly demanding executive tasks. We divided ADHD patients based on their cognitive performance as presenting either a Hi-ADHD or Lo-ADHD. To our knowledge, this strategy has not been used in ADHD research before. Measures of the standard neuropsychological battery differed significantly between Lo-ADHD participants and healthy controls but not between the latter and Hi-ADHD patients. However, when ADHD patients were compared with healthy controls on ecological or highly demanding executive tasks, significant differences were consistently found, irrespective of whether they had shown within-normal (Hi-ADHD) or decreased (Lo-ADHD) neuropsychological functioning.
The neuropsychological profile of Lo-ADHD was characteristic, with significant differences found in comparison with controls on the immediate and recall scores of the logical memory, the immediate score of the RAVLT, and two classical executive tasks (TMT-B and letters and numbers). In fact, the immediate scores of both verbal memory tasks could be reinterpreted as measures of attention in memory acquisition, suggesting affection of memory, attention, and executive function. These findings are similar to those of previous studies in adult ADHD patients reporting performance deficits on certain measures of logical memory and RAVLT (Oncü & Olmez, 2004; Pollak, Kahana-Vax, & Hoofien, 2008) as well as executive dysfunction as measured by classical tests (Rodriguez-Jiménez et al., 2006; Schweitzer et al., 2006; Shallice et al., 2002). Interestingly, the same variables differed significantly between both ADHD groups, supporting the idea of a high-functioning group that performs at control level.
The rationale behind the inclusion of the experimental tasks chosen for this study was twofold. On one hand, the design of ecological tasks that mimic real-life scenarios has been of increasing interest in the field of neuropsychology over the past decades (Gioia & Isquith, 2004; Manly et al., 2002; Shallice & Burgess, 1991; Torralva et al., 2009). Such tasks are thought to minimize the executive aid of the examiner during cognitive assessment, which could potentially compensate the patient’s own dysexecutive functioning and overrate scoring on classical tests. Moreover, by resembling everyday scenarios, subtle dysexecutive signs become more apparent. The hotel task included in our battery was introduced originally by Manly et al. (2002) for the rehabilitation of patients with traumatic brain injury who seemed to experience difficulties in everyday functioning. Recently, our group (Torralva et al., 2009) demonstrated the usefulness of this task, among other tasks of ecological validity, for the detection of executive deficits in patients with frontal deficits that scored above the cutoff score of a general cognitive screening test. Similarly, ADHD patients in the present study who showed within-normal performance on every variable of the standard neuropsychological battery (Hi-ADHD) showed significant differences from controls on the experimental task aimed at evaluating real-life executive functioning. This is an important issue because other recent studies (Saboya, Coutinho, Segenreich, Ayrão, & Mattos, 2009) also failed to show executive deficits in a group of adult ADHD denoting low sensitivity of the standard executive tests to discriminate between controls and ADHD patients.
On the other hand, the inclusion of computerized tests that measured inhibitory control and working memory was thought of as a way to assess two aspects of executive functioning using highly demanding cognitive tasks. Again, patients in the Hi-ADHD group were outperformed by controls on the working memory computerized task. Previous studies have also found working memory deficits in ADHD patients on other computerized tasks (Assef, Capovilla, & Capovilla, 2007; Messina, Tiedemann, de Andrade, & Prini, 2006). Moreover, some studies have shown that training working memory with computerized software stimulation programs improves executive performance (Klingberg et al., 2005; Klingberg, Forssberg, & Westerberg, 2002). Although lack of inhibitory control is a main deficit reported in children with ADHD (for review, see Kenemans et al., 2005), the lack of significant differences between the groups on the computerized inhibitory control task found in the present study is consistent with previous studies using digitalized assessment tools to assess adults with ADHD on this domain. For instance, Nigg, Butler, Huang-Pollock, and Henderson (2002) showed that while adult ADHD patients showed persistent motor inhibition deficits, as measured by an antissacade task, performance on a negative priming task was normal. Findings in this regard, however, are both scarce and contradictory, as some other authors have actually reported motor inhibition (Armstrong & Munoz, 2003) and cognitive inhibition (Biederman et al., 2000; P. Murphy, 2002) deficits in adult ADHD patients. The differences between results most probably stem from inconsistent approaches in methodology (e.g., time frames for priming tasks, varying algorithms in stop-signal tasks, etc.).
Limitations
There are a number of shortcomings to the present study that must be acknowledged. First, it could be argued that the differences found in education levels between ADHD groups and healthy controls pose a limitation to the generalizability of our results. However, it must be taken into account that premorbid IQ, as measured by the WAT-BA, did not differ significantly between the groups, making differences in performance across cognitive domains less critically dependent on any potential differences in intellectual functioning. Moreover, one must consider that by comparing ADHD patients’ performance with a control group of such high education levels (M = 16.3, SD = 2.7), the lack of significant differences between Hi-ADHD patients and controls is actually indicative of genuine high-functioning ADHD patients, as it may be associated with high-functioning profiles in real life (e.g., completing a degree, being able to hold a career over time, etc.). Future studies will have to address this issue further to determine the way in which everyday life success in ADHD patients is reflected through neuropsychological performance, especially on these more ecological and highly demanding cognitive tasks. Future studies should also tackle the other major limitation to our study which is the relatively low number of control subjects. It will be important to identify subgroups within larger control populations to allow for comparisons based not only on categorical variables such as diagnosis (i.e., ADHD vs. control) but also based on neuropsychological performance (e.g., spared vs. impaired executive profile besides diagnosis), or the presence or absence of specific ADHD symptoms in patients and controls even when not fulfilling DSM-IV criteria for ADHD.
Conclusion
The findings of the present study have several important clinical implications. First, showing a group of adult ADHD patients as being “high functioning” based on normal performance on all variables of a standard neuropsychological battery is a novel concept that is worthy of further exploration. Second, our results highlight the importance of introducing novel tasks that mimic real-life scenarios and tasks that are designed to be highly challenging as a way to detect subtle, yet impairing, executive deficits that occur in everyday settings. This is especially important, as it also provides an objective tool for specialists to design specific treatment methods for helping patients achieve better functioning levels in their everyday life. Third, the findings of our study open a new line of research aimed at furthering our understanding of symptoms and clinical features of ADHD patients in adulthood. Future studies should attempt to understand how executive deficits may be apparently compensated as patients grow older and yet be impairing enough to not allow for proper functioning. More studies are also needed to address the question on what behavioral aspects of ADHD patients (e.g., impulsivity, apathy, etc.) may explain the difference between high- and low-functioning individuals with this disorder.
In conclusion, we have shown a group of adult patients diagnosed with ADHD who, while performing normally on all tasks of a comprehensive standard cognitive battery, show executive deficits when assessed with real-life and highly demanding tasks that have been previously shown to be sensitive to frontal lobe dysfunction. Ecological and highly demanding executive tasks may eventually be developed into a diagnostically useful clinical tests in adult ADHD that perform normally in the standard neuropsychological evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Financial Disclosure/Funding
The author(s) received no financial support for the research and/or authorship of this article.