
Abstract
Objective:
To assess the impact of attention deficit on learning problems in a sample of schoolchildren in the city of Salvador, Bahia, Brazil.
Method:
All students enrolled in selected elementary schools were included in this study, making a total of 774 children. Each child was assessed by his or her teacher using a standardized scale. The Attention Deficit Hyperactivity Disorder Scale–Teacher’s Version (Benczic, 2000) was used to evaluate ADHD symptoms and learning problems.
Results:
A very strong association was found between attention deficit and learning problems (prevalence ratio [PR] = 31.7; 95% confidence interval = [16.1, 62.3]).
Conclusion:
Results suggest either that attention deficit leads to learning problems or that attention deficit and learning problems are comorbid conditions, in which case learning problems may also contribute to secondary symptoms in ADHD.
ADHD is the most common neuropsychiatric syndrome in childhood and is characterized principally by a persistent pattern of attention deficit or hyperactivity, more frequent and severe than what would be expected for a child at the equivalent developmental level (American Academy of Pediatrics [AAP], 2000). ADHD is characterized by three groups of symptoms, the predominance of which defines the subtype of the disease: predominantly inattentive, predominantly hyperactive–impulsive, or combined. ADHD is estimated to affect 5.5% to 8.5% of schoolchildren, the mean prevalence from the various studies carried out to date being 6.9% (AAP, 2000). A study carried out in Brazil, which was conducted with the same sample population as the current study, estimated that 6.7% of schoolchildren had a high probability of having ADHD, predominantly inattentive being the most prevalent subtype in 4%, hyperactive-impulsive in 1.7%, and a combination of both in 1% of the sample (Pondé & Freire, 2007).
Children with ADHD may have difficulties at school, relationship problems, and low self-esteem (Allmond, Tanner, & Goffman, 1999). Follow-up studies have shown that scholastic difficulties are continuous from childhood through adolescence (Hechtman, Weiss, Finklestein, Werner, & Benn, 1976), and academic performance and educational achievements were poorer in ADHD children compared with controls (Barkley, Fischer, Smallish, & Fletcher, 2006; Mannuzza, Klein, Bessler, Malloy, & Hynes, 1997; Mannuzza, Klein, & Moulton, 2002; Weiss, Hechtman, Milroy, & Perlman, 1985). It has been speculated that children with ADHD may have learning difficulties and children with learning disorders may be inattentive (Mayes, Calhoun, & Crowell, 2000). Learning disorders, which also result in difficulties at school, consist of results below those expected for the child’s age, IQ, and school level in standard tests for reading, mathematics, and writing. The prevalence of learning disorders varies from 2% to 10% (American Psychiatric Association [APA], 2000); however, the prevalence of learning disorders in ADHD children varies from 20% to 80% (Brook & Boaz, 2005).
To acquire a better understanding of which groups of ADHD symptoms are more strongly associated with learning disorders, this study addresses correlations between the symptoms of ADHD and those found in children with learning problems in a sample of schoolchildren in Salvador, Bahia, Brazil.
Methods
A study was carried out in a sample population taken from a total of 237,057 primary school students enrolled for the 2004 school year in the city of Salvador, Bahia, Brazil. Of these, 35,537 were enrolled in private schools, whereas 201,520 were enrolled in public schools. Assuming an ADHD prevalence of 8.5%, a confidence interval (CI) of 95%, and a presumed error of 3%, the sample size was calculated at 660 children. Schools were randomly selected from a list supplied by the State Education Department of all the schools in the city of Salvador, Bahia, Brazil. Two private schools with a total of 418 eligible students and three public schools with a total of 356 eligible students were included in the sample. In these selected schools, all students enrolled in the first to fourth grades of primary school were included in the study, making a total of 774 children, a larger sample than that required according to the calculated sample size. Meetings were held with teachers and directors of the selected institutions, at which time information was supplied with respect to the study, and the staff that voluntarily agreed to participate signed informed consent forms. All teachers from the selected schools voluntarily agreed to participate in the study.
The Attention Deficit Hyperactivity Disorder Scale–Teacher’s Version (ADHDS-TV; Benczic, 2000) was used to evaluate ADHD symptoms and learning problems. This scale is designed to evaluate the behavioral symptoms of ADHD within a school environment in which the teacher is the source of information. The instrument is composed of 49 items subdivided into four factors that evaluate ADHD within the school environment: Factor 1—attention deficit (16 items); Factor 2—hyperactivity–impulsiveness (12 items); Factor 3—learning problems (14 items); and Factor 4—antisocial behavior (7 items). A sample question for each scale is included in the appendix. The scale is a 6-point, Likert-type scale, designed for the teacher to select one of the following options: DC (disagree completely), D (disagree), DP (disagree in part), AP (agree in part), A (agree), and AC (agree completely). Each answer is awarded a score ranging from 1 to 6. After obtaining a score for each item, these scores are added together to provide a total score for each factor. The results are then transformed into percentiles using correlation tables contained in the instruction manual of the scale. Percentiles ≤25 suggest that the child has fewer problems with respect to that factor than the majority of children, and he or she is classified as below expectation. Percentiles between 26 and 75 suggest that the student is within the mean, that is, within expectation. Percentiles between 76 and 94 suggest that the child has more problems than the majority, and he or she is classified as above expectation. Percentiles >95 indicate that the child is in the range with the highest probability of having the disorder and is classified as highly probable. This instrument was chosen because it had already been validated in Brazil, it emphasizes the importance of information provided by teachers, and it allows the recording of behavior that may have been omitted if techniques involving direct observation of the child had been used. Furthermore, in addition to permitting identification of children with a high probability of having ADHD, this method identifies the group of most prevalent symptoms: impulsiveness, hyperactivity, attention deficit, learning problems, and antisocial behavior. It takes approximately 10 to 15 min for the teacher to complete a form for a child.
All the students in the selected schools were evaluated by their respective teachers. After the completed questionnaires had been returned, forms with any missing data or discrepancies in answers were sent back to the respective teachers for correction. The information was stored in a database using the SPSS statistical software package, version 9.0 for Windows. Analysis of the demographic variables and those concerning ADHD was carried out using the same program.
Results
In the period between May and August of 2004, a total of 774 children were evaluated, 356 of whom were enrolled in the public school system and 418 in the private system. With respect to gender, 430 children (44.4%) were girls, whereas 344 (55.6%) were boys. Age ranged from 6 to 17 years, with a mean age (± SD) of 8.9 ± 1.6 years. For children who scored above the 95th percentile in each subscale, the probability of them having the disorder was considered high. In fact, 3.7% of the children scored above the 95th percentile for learning problems, 4.9% for attention deficit, 2.6% for hyperactivity–impulsivity, and 3.2% for antisocial behavior. Overall, 23.5% of the children were above expectation in terms of learning problems, 52.1% were within expectation, and 20.7% were below expectation. With respect to attention deficit, 16.8% were above expectation, 56.1% were within expectation, and 21.7% were below expectation (Table 1).
Sample Population According to Attention Deficit and Learning Problems

Note: n = number of participants.
As shown in Table 2, there were no statistically significant differences between the group of children with learning problems (high probability) and the group that did not have learning problems in terms of age, gender, or type of school (public or private). The proportions of children with a high probability of attention deficit, hyperactivity–impulsivity, and antisocial behavior, however, were significantly higher among those with learning problems compared with those without learning problems.
Characteristics of the Sample Population According to the Presence of Learning Problems
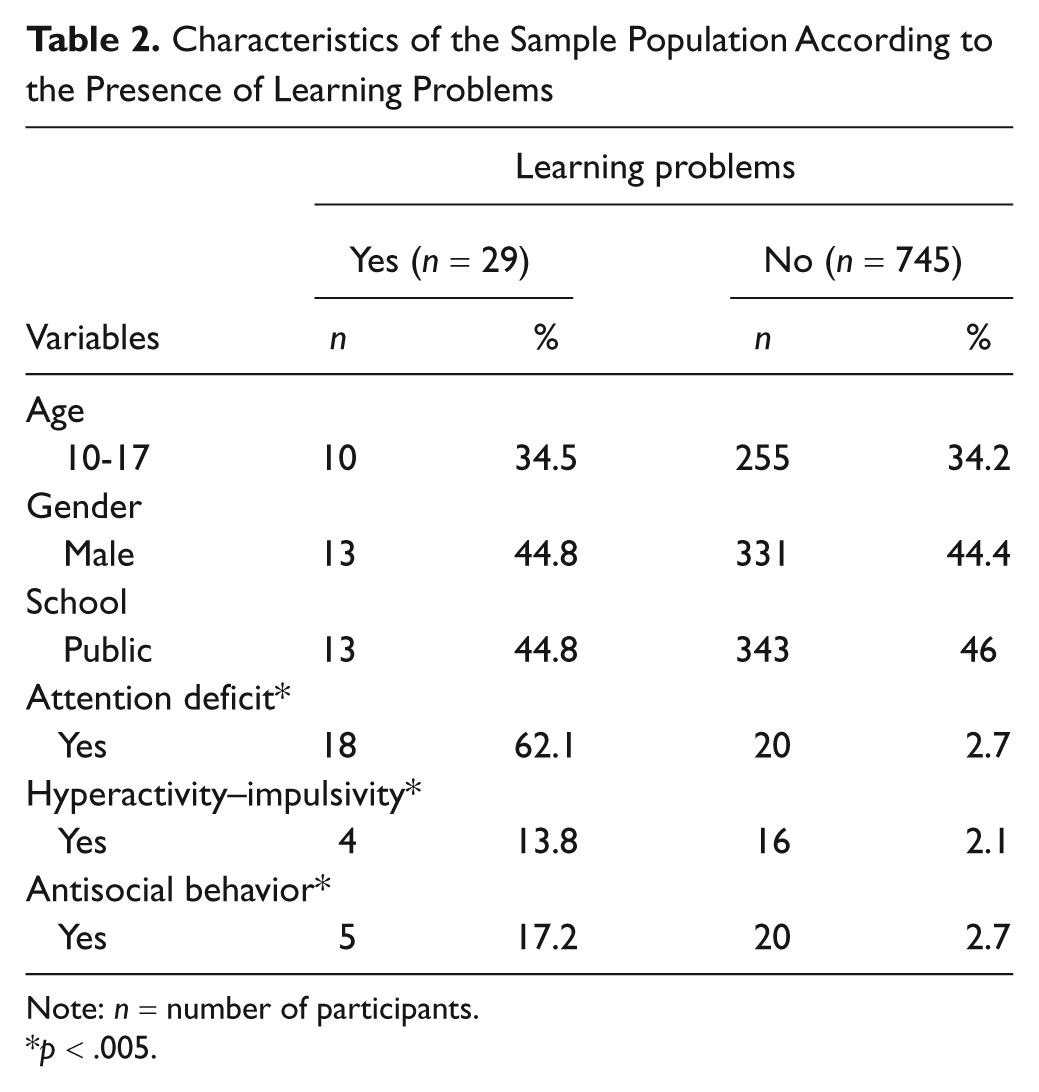
Note: n = number of participants.
p < .005.
The row association was positive between hyperactivity–impulsivity and learning problems (prevalence ratio [ PR] = 6; 95% CI = [2.3, 15.7]) and between antisocial behavior and learning problems (PR = 6.2; 95% CI = [2.6, 15]). There was also a very strong association between attention deficit and learning problems (PR = 31.7; 95% CI = [16.1, 62.3]). Stratified analysis was performed for the association between attention deficit and learning problems. Table 3 shows that gender was an effect modifier, the association being stronger for boys than for girls. Type of school, hyperactivity–impulsivity, and antisocial behavior were considered borderline effect modifiers. The association between attention deficit and learning problems was stronger in the case of children in public schools. With respect to comorbid symptoms of hyperactivity–impulsivity and antisocial behavior, the association between attention deficit and learning problems was stronger in the strata of children who did not have hyperactivity–impulsivity and in the strata in which antisocial behavior was absent. Stratified analysis, therefore, showed that the association between attention deficit and learning problems was statistically significant only in the case of children in whom hyperactivity–impulsivity and antisocial behavior were not present (Table 3). Analysis of confounding factors shows that age, type of school, hyperactivity–impulsivity, or antisocial behavior could not be considered as confounding factors.
Stratified Analysis for Association Between Learning Problems and Attention Deficit

Note: n = number of participants; PR = prevalence ratio; 95% CI = 95% confidence interval.
Effect modifier.
Borderline effect modifier.
Table 4 shows that even if all the independent variables had a significant effect on learning problems, attention deficit had a greater effect on the dependent variable (B = .881). Learning problems as a function of attention deficit proved to be the best regression model. All variables were tested for colinearity, and none was found. Attention deficit was considered responsible for 71% of the variance in learning problems (Table 5). Another model was tested in which the four variables suspected as being effect modifiers or borderline effect modifiers (gender, school, hyperactivity–impulsivity, and antisocial behavior) were controlled. The difference with respect to explanations of variance between the two models was 4.9%, which was negligible.
Regression Analysis of Learning Problems (n = 774)

Note: Attention deficit, hyperactivity–impulsivity, and antisocial behavior are considered continuous variables.
Regression Models for Association Between Attention Deficit and Learning Problems, Controlled for Interactions Between the Candidate Variables (n = 774)

Discussion
The prevalence of learning problems in the schoolchildren assessed in this study was 3.7%, a finding that is similar to data published in the literature on learning disorders in which figures range from 2% to 10% (APA, 2000). The prevalence of learning problems was significantly higher (62.1%) in children with attention deficit compared with those without attention deficit (37.9%; p < .005). Of the children with attention deficit, 62.1% had learning problems, whereas only 2.7% of those who did not have attention deficit had learning problems (p < .005). Mayes, Calhoun, and Crowell (2000) estimated that the prevalence of learning disorder was 68.9% in children with ADHD and 39.4% in children without the disorder.
The row association between attention deficit and learning problems shows a very strong association (PR = 31.7; 95% CI = [16.1, 62.3]). Stratified analysis of the association between attention deficit and learning problems shows that the comorbid presence of hyperactivity–impulsivity or antisocial behavior reduced the risk of learning problems in this sample. Multivariate analysis confirmed the strong association found in the bivariate analysis: 71% of the variance in learning problems could be explained by the presence of attention deficit, whereas other variables (hyperactivity–impulsivity, antisocial behavior, type of school, and gender) appeared to add only 4.9% of variance to the equation. Many follow-up studies have suggested that problems at school represent a very important aspect of ADHD (Barkley et al., 2006; Barkley et al., 2006; Mannuzza et al., 1997, 2002; Weiss et al., 1985). Pastura, Mattos, and Araújo (2009) suggested that the predominantly inattentive subtype of ADHD is the type most strongly related to poor school results. Children who met the modified criteria for the predominantly inattentive subtype of ADHD had lower reading, spelling, and mathematics scores over time compared with children who met the modified criteria for the other subtypes of ADHD (Massetti et al., 2008). The strong association between attention deficit and learning problems in the present study suggests either that attention deficit results in learning difficulties or that attention deficit and learning problems are comorbid conditions in which case learning problems may also contribute to secondary symptoms of attention deficit.
This study is very important because it clarifies that, according to the teacher’s evaluation, the symptoms of attention deficit are much more closely related to learning problems than symptoms of hyperactivity. Symptoms of attention deficit, however, are often underestimated by teachers because they tend to be less disruptive than symptoms of hyperactivity. In this sense, children who are identified by teachers as having symptoms of attention deficit should be provided with extra learning support from the school to enable them to cope better with possible learning difficulties.
It is important to mention some limitations of this study. This is a cross-sectional study that does not permit inferences with respect to the direction of the risk. In addition, the children were not evaluated by direct observation but by questionnaires filled out by their teachers. These findings may not, therefore, represent the real disorder but rather the teachers’ perceptions of the children’s difficulties. In our view, however, even if the evaluation tool used does not permit a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; APA, 1994) diagnosis to be reached, it represents an excellent proxy of children’s function as long as they have only one teacher who has been in contact with them for at least 6 months.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a grant from the Bahia State Foundation for the Support of Research (FAPESB).