
Abstract
Symptoms of ADHD typically first appear in early childhood and are chronic for the majority of affected individuals (Barkley, 2006; Barkley, Murphy, & Fischer, 2008). Due to the chronicity of ADHD and frequent association of symptoms with academic impairment, research has focused on the challenges experienced by college students with this disorder. As college students are not required to disclose their ADHD diagnosis to institutions, the prevalence of ADHD among college students is difficult to ascertain, but various studies have found that between 2% and 8% of college students exhibit clinically significant levels of ADHD symptoms (e.g., DuPaul et al., 2001). In a recent survey of college freshmen, 6.4% of men and 3.8% of women (5% overall) reported having ADHD (Pryor, Hurtado, DeAngelo, Blake, & Tran, 2010). In fact, ADHD was the most prevalent disability of any kind reported by 1st-year students in this survey.
Studies have also examined the extent to which significant ADHD symptoms in college students are associated with deficits in various areas of functioning (for review, see DuPaul, Weyandt, O’Dell, & Varejao, 2009). By far, the most ubiquitous impairments are found for academic performance with studies indicating that college students with ADHD obtain lower grade point averages (Heiligenstein, Guenther, Levy, Savino, & Fulwiler, 1999) and are more likely to experience academic impairment than their non-ADHD peers (Lewandowski, Lovett, Codding, & Gordon, 2008). Preliminary findings suggest that academic deficits may be related to symptomatic inattention as well as executive functioning deficits, including inadequate academic coping strategies, poor organizational/study skills, and time management difficulties (Norwalk, Norvilitis, & MacLean, 2009; Reaser, Prevatt, Petscher, & Proctor, 2007). Some studies have found college students with ADHD to exhibit deficits in psychological (e.g., Rabiner, Anastopoulos, Costello, Hoyle, & Swartzwelder, 2008), emotional (e.g., Ramirez et al., 1997), and social (Kern, Rasmussen, Byrd, & Wittschen, 1999) functioning. Although college students with ADHD may be only mildly impaired relative to standardization samples, a recent study found large effect size differences in executive, academic, psychological, and social functioning in comparison with college students who do not have ADHD (Weyandt et al., 2011).
Psychotropic medications, particularly psychostimulants, are the primary treatment for managing ADHD in adults (Prince, Wilens, Spencer, & Biederman, 2006). Numerous controlled studies have found stimulants to reduce ADHD symptoms and, in some cases, enhance functioning in adults with ADHD (for review, see D. F. Connor, 2006). Recent investigations have focused on the prodrug stimulant lisdexamfetamine dimesylate (LDX), given that it was developed to provide longer duration of effect throughout the day; in addition, it may have a lower abuse potential than is found with dextroamphetamine (Najib, 2009). The results of open-label (Brown, Brams, Gao, Gasior, & Childress, 2010; Krishnan, Pennick, & Stark, 2008) and placebo-controlled (Adler et al., 2008; Wigal et al., 2010) studies have found that LDX usage is associated with reductions in ADHD symptoms among adults with ADHD as well as improved executive and overall functioning, including enhanced performance on structured academic tasks.
Although the prevalence of pharmacotherapy in the college ADHD population has not been studied extensively, available evidence suggests that the majority of college students with this disorder are prescribed stimulants to provide symptom relief (Advokat, Lane, & Luo, 2010). Uncontrolled and qualitative investigations suggest that stimulants may reduce symptoms, particularly inattention, in the college ADHD population (e.g., Heiligenstein, Johnston, & Nielsen, 1996). Alternatively, qualitative (Loe & Cuttino, 2008; Meaux, Hester, Smith, & Shoptaw, 2006) and survey (Advokat et al., 2010) data indicate that at least some college students treated with stimulants are ambivalent about their treatment, due to adverse side effects and/or perceived limited effects of pharmacotherapy. Further research has raised concerns over the possibility that college students with ADHD may give or sell stimulants to their peers who are seeking to use these drugs for recreational purposes (Rabiner et al., 2009; Upadhyaya et al., 2005; Weyandt et al., 2009).
We are unaware of any prior controlled investigation of any stimulant medication, including LDX, for the treatment of ADHD in a sample exclusively composed of college students. This is an important gap in the literature because results obtained with adults of varying ages operating in noneducational environments cannot be assumed to generalize to the functioning of young adults in college settings, who are expected to demonstrate successful functioning in a postsecondary educational environment. Furthermore, specific examination of stimulant medication in the college population is necessary given the high risk of alcohol and substance use in this age group (Smith, Molina, & Pelham, 2002) and the growing problem of medication diversion in the college population (Weyandt et al., 2009).
The purpose of this study was to investigate the acute effects of three dosages of LDX (30 mg, 50 mg, and 70 mg) relative to placebo and medication-free baseline conditions in a sample of college students with ADHD. This is the first study to investigate medication in this population using a double-blind, placebo-controlled, crossover design. Medication outcomes in two primary areas (ADHD symptoms and executive functioning) were examined, given prior evidence that these are the two areas most frequently impaired in this population. Treatment outcomes were also examined regarding psychological and social functioning. Potential impact on alcohol and drug use, as well as experience of adverse side effects, was evaluated. It was hypothesized that ADHD symptoms and related executive functioning would be significantly improved for all three active dosages relative to baseline and placebo. Furthermore, we explored whether LDX would enhance psychological and social functioning without increasing risk of adverse side effects, including greater use of alcohol or illicit substances. Finally, data were also collected on a non-ADHD control sample to examine whether LDX normalized functioning across these domains.
Materials and Method
Participants and Setting
Students with ADHD
Participants were recruited from student disabilities and health service offices at two universities in the Northeastern United States (one public and one private). Students already identified with ADHD who registered with the student disabilities office at either university were targeted for recruitment. In addition, students with ADHD who were not registered with student disabilities were recruited via undergraduate classes, campus flyers, and campus newspapers; to be eligible for the study, however, students needed to provide written documentation of their ADHD diagnosis.
ADHD diagnoses were confirmed by insuring that all students (a) met Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) criteria for one of three ADHD subtypes based on diagnostic interview with student or parent (Barkley & Murphy, 2006) and (b) scored at or above the 90th percentile on current symptom ratings based on self-report (C. K. Conners, Erhardt, & Sparrow, 1999) or had parent ratings of childhood symptoms that met Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) criteria (Barkley & Murphy, 2006). In addition, students were excluded from participation if any one of the following were present: (a) significant cardiac condition based on medical history and/or physical examination, (b) significant illicit substance abuse based on self-report and toxicology screen at intake, (c) pregnant based on self-report and blood screen, and/or (d) significant symptoms of major depressive disorder, bipolar disorder, or thought disorder based on initial diagnostic interview.
The 24 participants were between 18 and 23 years of age (M = 20.17, SD = 1.20) and were primarily male (62.5%), White non-Hispanic (91%), in their senior year of college (44%), and had fathers (65%) and mothers (62.5%) with bachelor’s or higher degrees. Of the 24 participants, 6 met criteria for ADHD Predominantly Inattentive type, 1 met criteria for ADHD Predominantly Hyperactive-Impulsive type, and 17 met criteria for ADHD Combined type based on self-report of symptoms (Barkley & Murphy, 2006). In addition, participants met criteria for oppositional defiant disorder (29%), specific phobia (12.5%), social phobia (8%), and generalized anxiety disorder (21%). Prior to the LDX trial, 15 participants were receiving central nervous system (CNS) stimulant medication (4 LDX, 4 methylphenidate, 6 mixed amphetamine salts, 1 dextroamphetamine) and 1 participant was receiving modafinil for ADHD.
Diagnostic interviews and weekly assessment sessions were conducted in laboratories at each university. Although rooms varied for different procedures, they were located in the same building and were similar in size across sessions and universities.
Control student sample
A sample of 26 students without ADHD was included so that possible LDX effects for students with ADHD could be compared with the functioning of typical college students (without medication). These were the same students who participated as nondisordered controls in the Weyandt et al. (2011) study. Control participants were included if they (a) did not meet DSM-IV-TR (APA, 2000) criteria for any of the three ADHD subtypes or any other disorder based on diagnostic interview with the student (Barkley & Murphy, 2006) and (b) scored below the 90th percentile on current ADHD symptom ratings based on self-report (Conners et al., 1999). Control students were between 18 and 22 years of age (M = 20.00, SD = 1.17) and were primarily male (54%), White non-Hispanic (81%), in their senior year of college (31%), and had fathers (62%) and mothers (66%) with bachelor’s or higher degrees (see Table 1). None of the control participants received psychotropic medication. Chi-square analyses revealed no significant differences between ADHD and control participants for gender, χ2(1, N = 50) = 0.384, p = .536; ethnicity, χ2(4, N = 48) = 4.724, p = .317; year in college, χ2(3, N = 49) = 2.224, p = .527; father’s education level, χ2(4, N = 49) = 2.669, p = .609; or mother’s education level, χ2(5, N = 50) = 3.695, p =.594. Comparison of group means revealed no significant differences for age, t(48) = 0.497, p = .621. Significant and large mean differences between groups were found for inattention and memory problems, t(48) = 18.836, p < .001, Cohen’s (1988) d = 5.33; hyperactivity and restlessness, t(48) = 8.817, p < .001, d = 2.50; ADHD total symptoms, t(48) = 14.517, p < .001, d = 4.11; and ADHD index, t(48) = 12.255, p < .001, d = 3.47, with ADHD participants having significantly higher reports of symptoms than did controls.
Participant Demographic Information
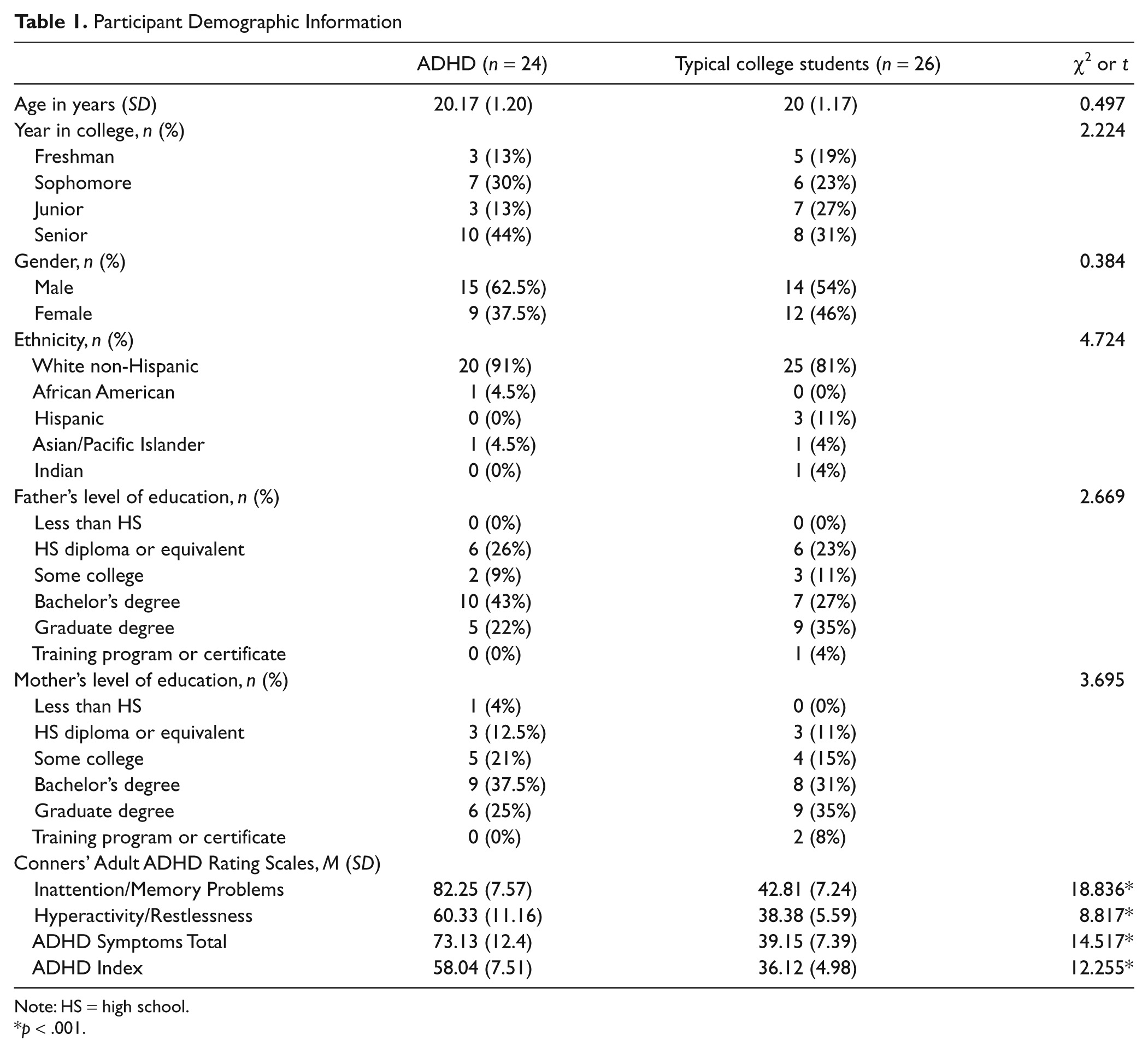
Note: HS = high school.
*p < .001.
Procedures
The student disabilities offices at each university were informed of the study prior to formal recruitment, and the directors were provided with flyers, frequently asked questions, and detailed information regarding the study that they could pass on to potential participants. Interested students were provided with the project coordinator’s contact information, and the student disabilities office director also received written or oral consent from students to have the project coordinator contact them directly.
This study was conducted in a manner consistent with the Declaration of Helsinki and Good Clinical Practice according to International Conference on Harmonisation guidelines. Each university’s institutional review board approved the study protocol. All students were at least 18 years old and provided written informed consent prior to participation. To ensure confidentiality, the signed consent form was filed in a folder separate from other materials, and participants were assigned identification numbers that appeared on their research materials.
Students then underwent a clinical evaluation to confirm their ADHD diagnosis, or in the case of control participants, to establish the absence of ADHD and other disorders, by meeting individually with the project coordinator (master’s- level psychologist) at their respective university to complete a structured diagnostic interview (Barkley & Murphy, 2006). The interview lasted approximately 1 hr and screened for ADHD symptoms based on DSM-IV-TR criteria (APA, 2000) as well as conduct and antisocial disorders, and mood disorders, including anxiety, depression, and bipolar disorder. Students were asked to report presence of ADHD symptoms during the past 6 months as well as when they were between the ages of 5 and 12 years old. In addition, participants completed an ADHD rating scale concerning their current functioning (Conners et al., 1999). For students with ADHD, a parent, or parents, was also contacted via telephone by the project coordinator and asked to complete the same diagnostic interview as well as provide current and retrospective symptom ratings of their child. Parent participation was optional and did not exclude students from participation.
In addition, students with ADHD underwent a toxicology (urinalysis) screen, and women underwent a pregnancy screen and were excluded if positive for either. If all inclusion and exclusion criteria were met, then students were determined to be eligible to participate. In all, 55 students with ADHD were initially referred and screened for participation eligibility, resulting in the eventual enrollment of 24 participants. A total of 31 students were excluded for not meeting participation eligibility criteria (n = 13), declining participation (n = 14), or for various other reasons (e.g., parents requested they not participate; n = 4). In addition, 2 students (one from each university) dropped out of the study after the first active medication phase due to adverse side effects. (See Figure 1 for complete information regarding participant attrition through the course of the study.) One of the two participants who discontinued the trial experienced heart palpitations after ingesting LDX 30 mg; the other participant also dropped out after ingesting LDX 30 mg and experiencing a variety of adverse side effects (e.g., irritable mood, increased anxiety, and social withdrawal). A total of 41 students were screened for participation as controls, with 15 of these students not meeting participation eligibility criteria.
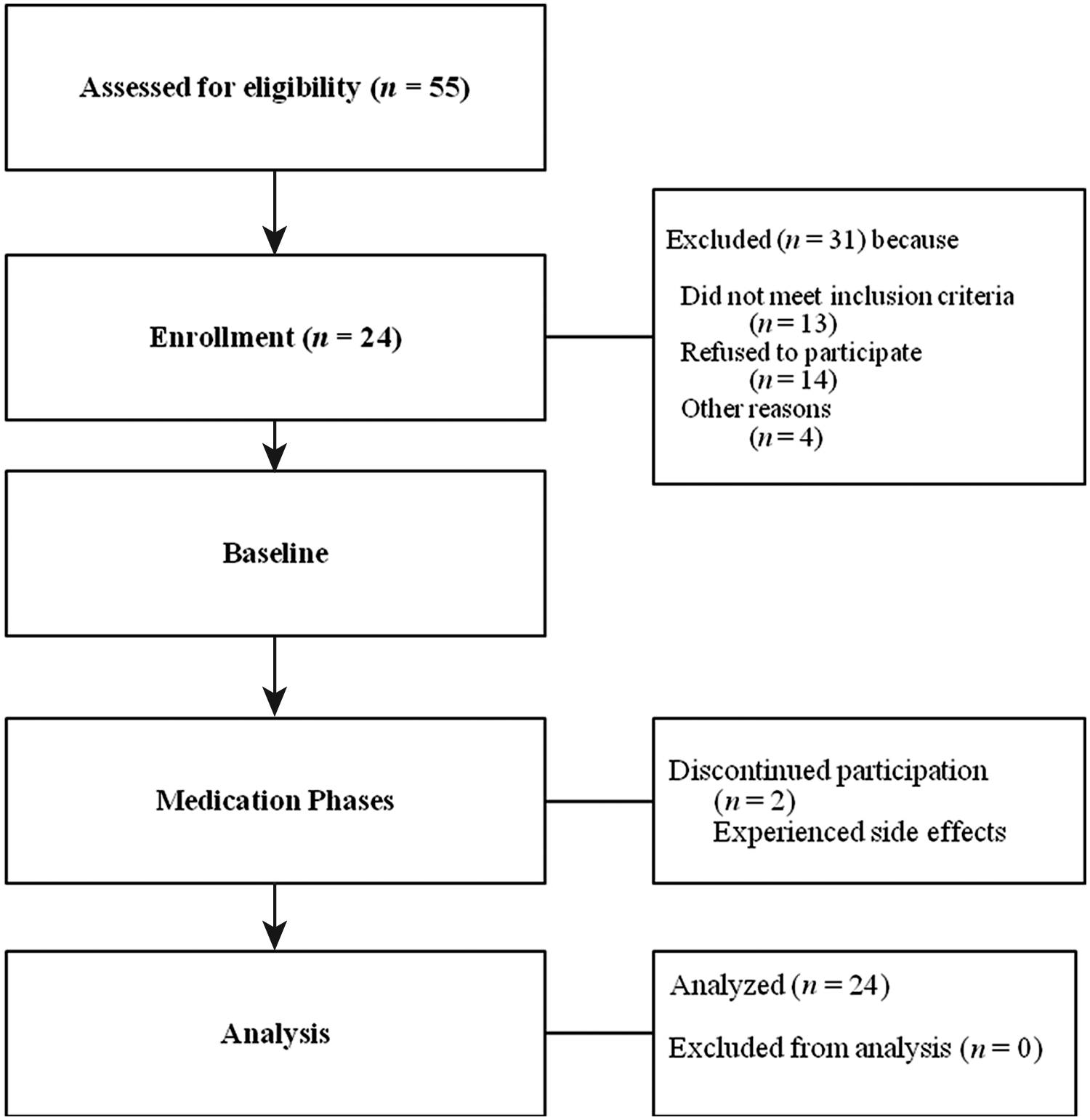
Attrition of participants with ADHD through each phase of the LDX trial
LDX (Vyvanse®, Shire US Inc.) effects were examined in the context of a double-blind, placebo-controlled design that included five phases: no-drug baseline, placebo, and three dosages (30, 50, and 70 mg per day) of active medication. Phase orders (following baseline) were assigned in a counterbalanced fashion across participants. To avoid starting any participant with the highest dosage, the 50-mg condition always preceded the 70-mg condition. Thus, there were six possible orders of dosage phases. Each phase was conducted for 1 week, and therefore, the total trial took place over 5 weeks and was able to be completed during a single semester. Participants ingested one pill per day on awakening. Control students only participated in the baseline phase and did not receive LDX.
Medication and placebo were packaged so that dosage was undetectable by sight or taste and used a numbered code that corresponded to the dosage. Participants received a 1-week supply of capsules at each visit (at the conclusion of each previous trial phase) and were instructed to return all unused capsules. Each supply included nine pills, and students were expected to return two at the end of each week. Participants returned the appropriate number of two pills for 87% of all dosage phases. Students were also asked to report whether they missed any dosage administration over the prior week (self-report of adherence). For 9% of the dosage phases, participants returned more than two pills due to reported adverse side effects, illness, or ending the trial a day early due to Thanksgiving break. Participants returned fewer than two pills for 4% of the dosage conditions and reported having lost pills or having to discard pills after difficulties swallowing. During their weekly visits with the health care provider for the study, students also reported any adverse side effects from the week’s dosage, and the health center physician measured their heart rate and blood pressure.
Participants, research assistants, and professors were blind to dosage condition. Only the principal investigators (PIs) and health center clinicians had access to the corresponding codes and dosages. Medical staff was instructed to keep this information confidential from participants unless there was a medical need that prohibited this from occurring (e.g., if the participant experienced a severe adverse reaction to the medication). Medications, information regarding dosage conditions, and all other research material were stored in a locked file cabinet in the offices of the co-PIs and medical staff. Following the completion of the study, the extra medications were destroyed in a manner consistent with Drug Enforcement Administration (DEA) regulations and health center policies.
At the end of each 1-week phase, students met individually with a research assistant (who was blind to dosage condition) to complete dependent measures. Participants were instructed to ingest LDX or placebo 2 to 4 hr prior to the weekly session so that assessment data were collected during the active phase of LDX (Wigal et al., 2010). During the session, the following measures were administered: Conners’ Adult ADHD Rating Scales (CAARS)–Short Form (C. K. Conners et al., 1999), Behavior Rating Inventory of Executive Functioning–Adult Version (BRIEF-A; Roth, Isquith, & Gioia, 2005), Expression and Emotion Scale (EESC) adapted from Perwien et al. (2008), Conners’ Continuous Performance Test (CPT-II; C. K. Conners, 2000), California Verbal Learning Test–Second Edition (CVLT-II; C. K. Delis, Kramer, Kaplan, & Ober, 2000), a self-report instrument of study habits and organizational skills (adapted from Glutting, Sheslow, & Adams, 2002), Symptom Checklist 90–Revised (SCL-90-R; Derogatis, 1986), Social Adjustment Scale–Self-Report (SAS-SR; Weissman, 1999), side effects self-report questionnaire (adapted from Barkley & Murphy, 2006), and a self-report questionnaire regarding use of alcohol and illicit substances (Janisus & Weyandt, 2009). Research assistants instructed participants to respond to each measure based on the current week’s dosage, ignoring any directions that prompted them to report within different time frames.
The individual measures were presented to the students in a randomized order each week, with the exception of the CVLT-II and the CPT-II. As the CVLT-II requires a 15 to 20 min break that should include nonverbal tasks, these measures were consistently presented in the following order: CVLT-II immediate recall and short-delay recall, CPT-II, and CVLT-II long-delay recall. Therefore, when the measures were randomized, the CVLT-II and CPT-II were considered to be one unit. Research assistants conducted direct observations of student attention and behavior during CPT-II testing. To increase the likelihood that students would complete weekly assessments, participants were given US$50 following each 1-week assessment phase. Those students who completed the entire protocol received an additional US$100 (i.e., total compensation of US$350).
Dependent Measures
CAARS
The CAARS (C. K. Conners et al., 1999) are comprised of three different versions, long, short, and screening, each of which can be completed by self- or observer report. For the purposes of this study, the screening form was used as part of participant inclusion criteria and the short version, self-report for 18- to 29-year-olds was used once each week to assess ADHD symptoms. Normative data from a nationally representative sample are available. Internal consistency coefficients for the short form, self report for 18- to 29-year-olds range from .77 to .86, indicating adequate reliability (C. K. Conners et al., 1999). T-scores for all subscales on the short version were used as dependent measures with higher scores representing greater ADHD symptomatology.
BRIEF-A
The BRIEF-A (Roth et al., 2005) is a standardized self-report measure that captures adults’ views of their own self-regulation in their everyday environment. T-scores on the nine clinical (Inhibit, Shift, Emotional Control, Self-Monitor, Initiate, Working Memory, Plan/Organize, Task Monitor, and Organization of Materials) and two composite scales (Behavior Regulation Index and Metacognition Index) served as dependent variables in this study. Higher scores indicate greater difficulties with executive functioning. Normative data for a nationally representative sample are available. The BRIEF-A has demonstrated good internal consistency with alpha coefficients ranging from .73 to .90 for the subscales and between .93 and .96 for the composite scales. Test–retest reliability was also adequate, with a range from .82 to .93 over a 4-week period. In addition, convergent and discriminant validity studies have been conducted for BRIEF-A clinical scales and indexes with other measures of executive function, anxiety, and mood for a variety of clinical and healthy adult samples (Roth et al., 2005).
CVLT-II
The CVLT-II (Delis et al., 2000) provides a short, individually administered assessment of strategies and processes involved in learning and remembering verbal information. The CVLT-II measures both recall and recognition of two lists of words over a number of immediate- and delayed-memory trials. Two unique forms of the CVLT-II were available for administration to participants to minimize practice effects. Students were randomly assigned to receive either the standard form or the alternate form during their first weekly session and completed alternating versions of the CVLT-II during subsequent sessions. The CVLT-II has been shown to have adequate internal consistency across age and gender, and factor analyses confirm subscale structure and content validity (Delis et al., 2000). Normative data from a nationally representative sample are available, and T-scores for all subscales were used as dependent measures. Higher scores indicate better verbal learning and memory.
CPT-II
The CPT-II (C. K. Conners, 2000) is a computer-based measure of sustained attention and behavioral inhibition. The test has been shown to be a useful attention and learning disorder measure as well as a particularly sensitive measure to drug treatment effects in children with ADHD (C. K. Conners, 2000). During the test administration, respondents are required to press the space bar on the keyboard or the left mouse button when any letter except “X” appears on the computer monitor. The interstimulus intervals (ISI) are 1, 2, and 4 s with a display time of 250 min. There are six blocks, with three subblocks, each containing 20 trials (i.e., letter presentations), with ISI varying between blocks. Split-half reliability between trials was shown to be adequate on indices used as dependent variables, including Hit Reaction Time (.95), Errors of Commission (.83), Errors of Omission (.94), Standard Error (.87), Variability (.66), d prime (i.e., detectability = .83), and Beta (i.e., response style = .73). Test–retest reliability was shown to be highly satisfactory for most measures. Perseverations were shown to be adequate (.43), Block Change (.08-.28) and ISI change (.05-.51) Response Time and Standard Error were shown to be unsatisfactory, and d prime (.76) and Beta (.62) were shown to be adequate (C. K. Conners, 2000). Norms are available for a nationally representative sample, and T-scores for all subscores were used as dependent variables.
Behavior observations during CPT-II
During each CPT-II administration, a research assistant observed the student for Off-Task Behavior (any continuous period of 3 s or longer where the student was not visually looking at the computer or monitor), Fidgeting (a repetitive, purposeless motion of the arms, hands, buttocks, or trunk that occurred at least four consecutive times), Task-Relevant Vocalizations, Task-Irrelevant Vocalizations, and Out-of-Seat Behavior (any time in which the student’s buttocks fully broke contact with the flat surface of their chair). A second research assistant observed 26% of participant sessions across dosage conditions for the purposes of assessing interobserver agreement, resulting in a mean overall agreement of 96.4% and a mean kappa of .48. Behavior observations were only conducted during CPT-II sessions for students with ADHD. Percentage intervals where each behavior category was observed were used as dependent measures.
SCL-90-R
The SCL-90-R (Derogatis, 1986) is a 90-item self-report questionnaire assessing psychopathological symptoms, including Somatization, Obsessive-Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. Symptom severity is rated on a 5-point Likert-type scale ranging from “not at all” to “extremely”, and outcomes are computed by summing the raw scores and converting them to T-scores (M = 50, SD = 10) with higher scores representing greater pathology. T-scores for all subscales as well as for three global indices (Global Severity Index [GSI], Positive Symptom Total [PST], and Positive Symptom Distress Index [PSDI]) served as dependent variables in this study. The SCL-90-R has been shown to have adequate internal consistency with a mean coefficient of .95 (Edwards, Yarvis, Mueller, Zingale, & Wagman, 1978), good test–retest reliability with coefficients ranging from .81 (Edwards et al., 1978) to .84 (Horowitz, Rosenberg, Baer, Ureno, & Villasenor, 1988), and moderate- to high-convergent validity correlations with the Minnesota Multiphasic Personality Inventory ranging from .40 to .75 (Derogatis, Rickels, & Rock, 1976). Normative data from a nationally representative sample are available.
SAS-SR
The SAS-SR (Weissman, 1999) is a 54-item scale assessing behaviors in six aspects of life, including work role (i.e., student), social and leisure activities, relationships with extended family, role as spouse, role as parent, and role within family. Each of these scores served as dependent variables. Each item is rated on a 5-point scale with high scores indicating more impairment. Outcomes are calculated by adding up raw scores and converting them to T-scores that were used as dependent measures in this study. Higher scores represent greater social adjustment difficulties. The SAS-SR has adequate internal consistency, with a mean coefficient of .74, and test–retest reliability, with a mean coefficient of .78 (Edwards et al., 1978). Normative data from a nationally representative sample are available.
EESC–College Student Version (EESC-C)
The EESC-C is a self-report rating scale of positive and negative emotional expression adapted from the informant-report rating scale developed by Perwien et al. (2008) to assess parent perception of emotional expression in children with ADHD who were being treated with atomoxetine. The rating scale contains 29 items, and validation studies show that it is a reliable and valid tool with three factors: Positive Emotional Expression, Flat Emotional Expression, and Emotional Lability. The EESC has adequate internal consistency, with a mean coefficient of .91, and adequate test–retest reliability, with a mean coefficient ranging from .65 to .69 (Kratochvil et al., 2007). The EESC-C updates the language of the 29 items to be appropriate for self-report with college-age individuals. Raw scores for the three factors mentioned previously served as dependent variables with higher scores representing greater difficulties with emotional expression. Normative data are not available for this measure.
Substance Use Frequency Scale
This is a 21-item self-report rating scale (Janisus & Weyandt, 2009) with which individuals rate the frequency of use of stimulant, depressant, analgesic, hallucinogenic, and an “other” class of drugs on a 5-point Likert-type scale with anchors at 1 (never), 2 (yearly), 3 (monthly), 4 (weekly), and 5 (daily). For each phase following baseline, participants reported information based on their weekly phase; thus, anchors 1, 4, and 5 were the only available rating options during placebo and dosage conditions. Raw scores for use of each substance as well as an overall substance use score were used as dependent variables. Normative data are not available for this measure.
Study and organizational skills ratings
This measure is a 14-item self-report rating scale adapted from Glutting et al. (2002). The rating scale requires individuals to rate the frequency of positive and negative behaviors related to study and organization skills as occurring never, sometimes, often, or very often. The total raw score was used to determine student level of study and organizational skills with higher scores representing better functioning. The study and organizational skills rating scale has adequate internal consistency (coefficient alpha = .90) and test–retest reliability (r = .91; Glutting et al., 2002).
Side Effects Self-Report Questionnaire
This 15-item self-report rating scale required individuals to rate the severity of known adverse side effects associated with stimulant medication. Adapted from material in Barkley and Murphy (2006), possible side effects were rated on an 8-point Likert-type scale from 0 (absent) to 7 (serious). Participants with ADHD completed the self-report rating for all phases except baseline. Total raw score (representing frequency and severity of adverse side effects) was used as a dependent variable.
Pulse and blood pressure
Health professionals recorded resting heart rate (i.e., pulse) in beats per minute and systolic/diastolic blood pressure for participants with ADHD once per week during placebo and LDX dosage conditions. Normal resting heart rate ranges from 60 to 100 beats per minute. Systolic less than 120 mmHg and diastolic less than 80 mmHg is considered normal blood pressure. Systolic readings of 140 mmHg and above or diastolic readings of 90 mmHg and above represent high blood pressure.
Statistical Analyses
It was hypothesized that LDX would lead to statistically significant improvements in symptomatic behavior and executive functioning for college students with ADHD relative to placebo conditions. A series of 2 (site) × 5 (dosage conditions) ANOVAs with repeated measures across dosage were used to assess medication effects on each dependent variable. Statistically significant (p < .05) main effects for dosage were followed by Tukey’s honestly significant difference test (HSD) comparison tests to identify specific between-dosage differences. Trend analyses were used to determine the shape (e.g., linear or quadratic) of the dose-response curves for each measure. It was also hypothesized that LDX would lead to moderate to large effect sizes for symptom change and small to moderate effect sizes for academic functioning, psychological functioning, and social relationships. Thus, effect sizes (partial η2) were calculated to determine the amount of variance in each dependent measure that is accounted for by LDX treatment. Following Cohen’s (1988) definitions, a partial η2 value of .01 was considered a small effect, .06 a medium effect, and .14 a large effect. Next, an additional exploratory analysis of adverse side effects with LDX treatment was conducted. A one-way ANOVA was used to assess medication effects on total self-reported side effects as well as systolic and diastolic blood pressure and pulse. A follow-up comparison test using Tukey’s HSD was conducted to determine specific between-dosage differences. Finally, the degree to which dosage effects resulted in reliable change for individual participants was determined using methods described by Jacobson and Truax (1991) for placebo and the three active LDX conditions using two primary measures: CAARS ADHD Index and BRIEF Metacognition Index. These two measures were selected because they represented general indicators of ADHD symptoms (CAARS) and planning/organizational skills critical for college success (BRIEF-A). The reliable change index (RCI) compares change in pre- and posttreatment scores to the standard error of the difference for the dependent measure (Jacobson & Truax, 1991). The latter represents the spread of the distribution of change scores that would be expected if no actual change has occurred. A RCI of 1.96 or larger indicates that a lack of actual change is unlikely (p < .05).
A series of independent sample t tests was used to compare ratings on the two primary outcome measures (CAARS ADHD Index and BRIEF-A Metacognition Index) for non-ADHD controls (n = 26) during no-medication baseline relative to participants with ADHD during placebo, 30-mg, 50-mg, and 70-mg LDX conditions.
Given that multiple outcome measures were investigated, the number of analyses conducted could have inflated experiment-wise Type I error rate. A multivariate approach was precluded due to the small sample size available for analysis. Given that this was an initial study of LDX effects with the college student population, we chose to protect against experiment-wise Type I error rate while also limiting Type II error by correcting alpha levels for each individual analysis to control for false discovery rate using procedures described by Benjamini and Hochberg (1995).
Results
Means and standard deviations for all dependent measures across dosage conditions are provided in Table 2. For the 2 (site) × 5 (dosage) ANOVAs, very few main effects for site or Site × Dosage interactions were statistically significant. For the dosage main effects, using an alpha level of .05, statistically significant differences were observed on 46 of 92 dependent measures (50%). However, the site and interaction effects each achieved significant effects not much greater than chance (15% and 6%, respectively). For the .01 alpha level, only 3% and 1% of the site and interaction effects were significant, respectively (compared with 27% for the dosage main effect). Thus, results are reported for main effects of dosage. Furthermore, we adjusted p values to control for the false discovery rate using procedures described by Benjamini and Hochberg (1995). Thus, an alpha value of .021 was used wherein significant dosage effects were found for 39 of 92 dependent measures.
Means and Standard Deviations for Measures Across Dosage Conditions

Note: BRIEF-A = Behavior Rating Inventory of Executive Function–Adult; SCL-90-R = Symptom Checklist-90–Revised; SAS-SR = Social Adjustment Scale–Self-Report; CVLT-II = California Verbal Learning Test–Second Edition; EESC-C = Expression and Emotion Scale–College Student Version; CPT-II = Conners’ Continuous Performance Test; ISI = interstimulus interval; CAARS = Conners’ Adult ADHD Rating Scale.
Effects on ADHD Symptoms
Statistically significant main effects for dosage were obtained for CAARS Inattention/Memory Problems, F(4, 84) = 8.88, p < .001, partial η2 = .30; CAARS Hyperactivity/Restlessness, F(4, 84) = 14.7, p < .001, partial η2 = .41; and CAARS ADHD Index, F(4, 84) = 10.9, p < .001, partial η2 = .34. Negative linear trends were significant for all four variables wherein CAARS scores decreased with increasing LDX dosage (see Figure 2). Cubic trends were significant for CAARS Hyperactivity/Restlessness and CAARS Problems with Self-Concept as these were characterized by decreasing trend to 30 mg, flat trend to 50 mg, and another decrease at 70 mg. Significant main effect for dosage was not found for CAARS Impulsivity/Emotional Lability subscale.
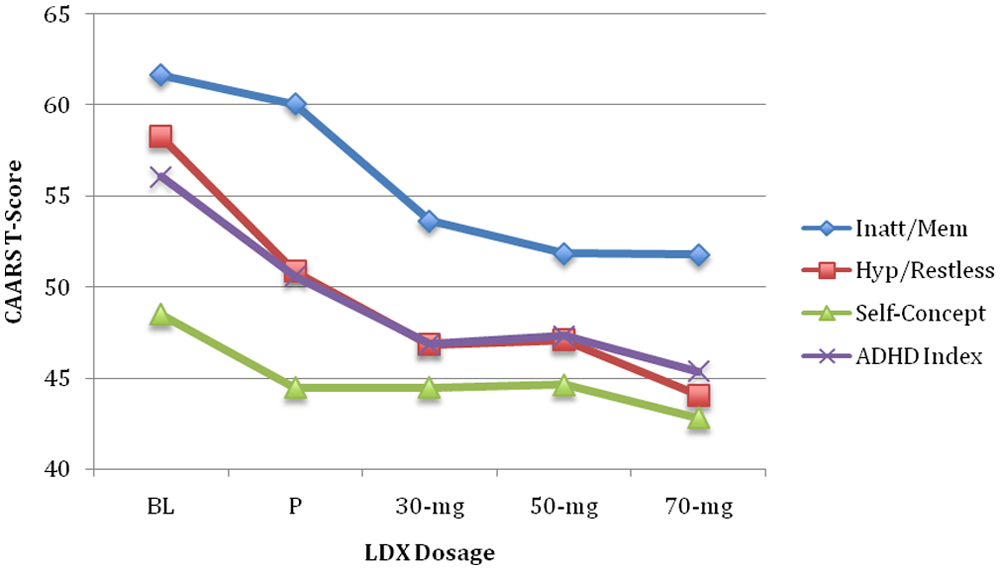
Self-report ratings of ADHD across dosage conditions
Tukey’s HSD post hoc comparison tests indicated that CAARS ratings for all three LDX dosages were significantly lower than baseline for Inattention/Memory Problems, Hyperactivity/Restlessness, and ADHD Index (p < .01). Inattention/Memory Problems were significantly lower for 30 mg (p < .05), 50 mg, and 70 mg (p < .01) relative to placebo. For Hyperactivity/Restlessness and ADHD Index, 70 mg was significantly lower than placebo (p < .05). Placebo ratings were lower than baseline CAARS scores for Hyperactivity/Restlessness (p < .01) and ADHD Index (p < .05).
CPT-II results revealed significant main effects for dosage for the following measures: Commission Errors, F(4, 80) = 4.84, p = .002, partial η2 = .20; Hit Reaction Time-Standard Error, F(4, 80) = 3.07, p = .02, partial η2 = .13; Variability of Standard Error, F(4, 80) = 3.56, p = .01, partial η2 = .15; and Hit Reaction Time-Block Change, F(4, 80) = 3.08, p = .02, partial η2 = .13. Significant linear trends (i.e., enhanced performance with increasing dosage) were found for all but one CPT-II score, Hit Reaction Time-Block Change, with the latter showing a significant quadratic trend (peak improvement at 30 mg with declining trend for subsequent dosages). A significant cubic effect was found for Variability of Standard Error with increasing variability from baseline to placebo, decreasing to 50 mg, and then a slight increase at 70 mg. Significant main effect for dosage was not found for remaining CPT-II scores, including Omissions, Hit Reaction Time, Response Style, Perseverations, Hit Reaction Time-ISI Change, and Hit Standard Error-ISI Change.
Tukey’s HSD results showed that Commission Errors were significantly higher in baseline relative to 50 and 70 mg (p < .01). Hit Reaction Time-Block Change was significantly greater for 30 mg than for baseline (p < .05). Hit Reaction Time-Standard Error and Variability of Standard Error were significantly greater for placebo than for 70 mg (p < .05), with placebo greater than 50 mg for the latter score (p < .05).
The only dosage main effect for direct observations of behavior during CPT-II was found for Percentage of Task-Related Vocalizations, F(4, 84) = 5.02, p = .001, partial η2 = .19. A significant quadratic trend was found wherein Task-Related Vocalizations decreased from baseline to 30 mg with an increase over the two higher dosages. Tukey’s HSD tests indicated that baseline was associated with a significantly higher percentage of Task-Related Vocalizations than 30 mg (p < .01) and 50 mg (p < .05). No dosage main effects were seen for Fidgeting Percentage, Off-Task Percentage, Task-Irrelevant Vocalization Percentage, Out-of-Seat Percentage, or Total Percentage.
Effects on Executive Functioning
Significant main effects for dosage were found for nearly all BRIEF-A subscales, including Inhibit, F(4, 84) = 8.14, p < .001, partial η2 = .28; Shift F(4, 84) = 3.06, p = .02, partial η2 = .13; Initiate, F(4, 84) = 4.05, p = .005, partial η2 = .16; Working Memory, F(4, 84) = 6.02, p < .001, partial η2 = .22; Plan/Organize, F(4, 84) = 7.02, p < .001, partial η2 = .25; Task Management, F(4, 84) = 5.74, p < .001, partial η2 = .22; Organization of Materials, F(4, 84) = 3.34, p = .01, partial η2 = .14, Behavioral Regulation Index, F(4, 84) = 3.54, p = .01, partial η2 = .14; Metacognition Index, F(4, 84) = 8.14, p < .001, partial η2 = .28; and the Global Executive Composite, F(4, 84) = 7.31, p < .001, partial η2 = .26. A significant negative linear trend (indicating improved scores with increasing dosage) was found for all of these scores (see Figure 3). Main effects for dosage were not significant for Emotional Control or Self-Monitor scores.
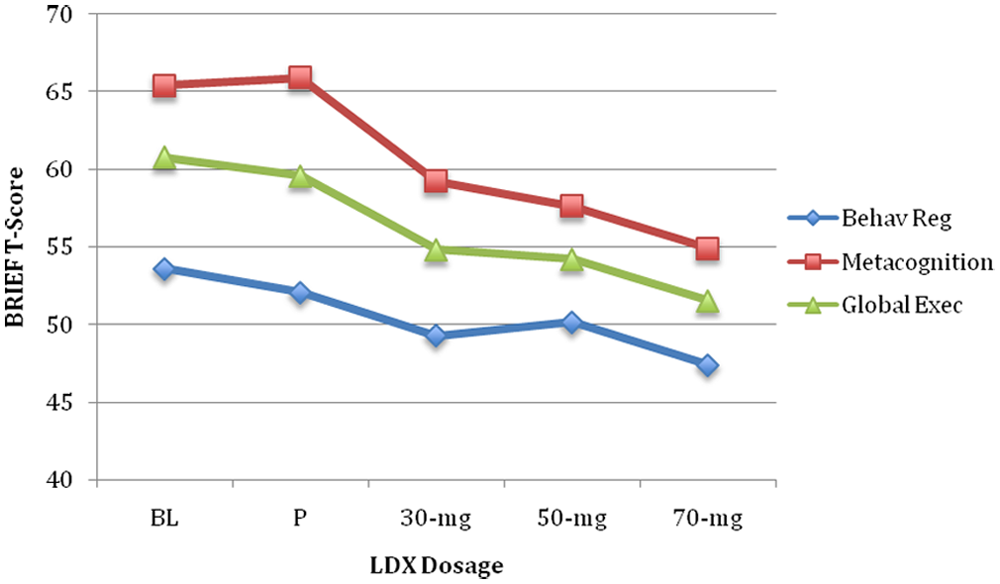
Self-report ratings of executive functioning across dosage conditions
Tukey’s HSD post hoc comparison tests indicated that baseline BRIEF-A scores were significantly greater than 30 mg, 50 mg, and 70 mg (p < .01) for Inhibit; greater than 50 mg (p < .05) and 70 mg (p < .01) for Working Memory; greater than 30 mg (p < .05) and 70 mg (p < .01) for Plan/Organize; greater than 70 mg (p < .05) for Task Management; greater than 50 mg and 70 mg (p < .05) for Organization of Materials; greater than 70 mg (p < .01) for Behavioral Regulation Index; greater than 50 mg (p < .05) and 70 mg (p < .01) for Metacognition Index; and greater than 30 mg (p < .05), 50 mg (p < .05), and 70 mg (p < .01) for General Executive Composite. Placebo BRIEF scores were significantly greater than 70 mg (p < .01) for Inhibit, Initiate, Plan/Organize, Task Management, Metacognition Index, and the Global Executive Composite. In addition, placebo scores were significantly greater than 70 mg (p < .05) for Working Memory, greater than 30 mg and 50 mg (p < .05) for Task Management, and greater than 50 mg (p < .01) for Metacognition Index.
A significant main effect for dosage was also obtained for total raw score on the Study and Organizational Skills Scale, F(4, 84) = 8.88, p < .001, partial η2 = .30. Dosage effects on this variable were characterized by a positive linear trend with improved scores associated with increasing dosage in a stepwise fashion. Tukey’s HSD tests revealed that baseline scores were significantly lower than 30 mg (p < .05), 50 mg (p < .01), and 70 mg (p < .01). Furthermore, placebo was significantly lower than 70 mg (p < .01).
Significant main effects for dosage were found for four CVLT-II scores, including Level of Recall SD Cued, F(4, 84) = 3.42, p = .01, partial η2 = .14; Semantic Clustering, F(4, 84) = 3.75, p = .007, partial η2 = .15; Subjective Clustering-Bidirectional, F(4, 84) = 5.51, p = .001, partial η2 = .21; and Repetition Errors, F(4, 84) = 3.23, p = .02, partial η2 = .13. Significant linear trends were obtained for these CVLT scores. A significant cubic trend was found for Subjective Clustering-Bidirectional showing an increase from baseline to placebo followed by a slight downward trend to 50 mg and then an increase at 70 mg. Significant main effects for dosage were not found for the remaining 22 CVLT-II scores.
Tukey’s HSD post hoc comparison tests indicated that 70 mg scores were significantly greater than baseline (p < .01) for Level of Recall SD Cued, Semantic Clustering, and Subjective Clustering-Bidirectional. Repetition Errors were significantly greater in baseline relative to 30 mg (p < .01). Semantic Clustering scores were greater in 50 mg than baseline (p < .05) and Subjective Clustering-Bidirectional scores were greater in placebo and 30 mg than baseline (p < .05).
Effects on Psychological Functioning
Significant main effects for dosage were obtained for most SCL-90-R scores, including Obsessive-Compulsive, F(4, 80) = 5.56, p = .001, partial η2 = .22; Interpersonal Sensitivity, F(4, 80) = 4.24, p = .004, partial η2 = .18; Depression, F(4, 80) = 6.61, p < .001, partial η2 = .25; Hostility, F(4, 80) = 3.0, p = .02, partial η2 = .13; Paranoid Ideation, F(4, 80) = 3.46, p = .01, partial η2 = .15; Psychoticism, F(4, 80) = 3.16, p = .02, partial η2 = .14; GSI, F(4, 80) = 4.95, p = .001, partial η2 = .20; and PST, F(4, 80) = 3.54, p = .01, partial η2 = .15. Significant linear and cubic trends were found wherein there was a general decrease in SCL-90-R scores (indicative of improvement) with increasing dosage; however, the pattern was for a decrease from baseline to placebo, flat trend to 50 mg, and then another decrease with 70 mg. Significant dosage effects were not found for Somatization, Anxiety, Phobic Anxiety, or Positive Symptom Distress.
Post hoc comparison tests indicated that SCL-90-R scores were significantly higher (p < .01) in baseline than 70 mg for Obsessive-Compulsive, Interpersonal Sensitivity, Depression, Hostility, Paranoid Ideation, GSI, and PST. Furthermore, baseline scores were greater than 70 mg for Psychoticism (p < .05), greater than 30 mg for Depression (p < .05), and greater than placebo for GSI (p < .05). Finally, placebo Depression score was greater than 70 mg (p < .05), whereas 50 mg was greater than 70 mg for GSI (p < .05).
No significant main effects were obtained for any of the three EESC-C scores indicating no dosage impact on affect or emotional expression.
Effects on Social Functioning
No significant main effects for dosage were obtained for SAS-SR total score or for any subscale scores.
Alcohol/Substance Use
Significant main effects for dosage were obtained for self-reported use of hallucinogens, F(4, 80) = 9.50, p < .001, partial η2 = .32, and total use of substances, F(4, 84) = 10.32, p < .001, partial η2 = .33. These effects were subject to linear and cubic trends. There appeared to be an overall decrease in use of substances across dosage conditions with a drop from baseline to placebo, flat trend to 50 mg, and then another decrease with 70 mg. Post hoc comparisons indicated that hallucinogen use and overall substance use was significantly greater at baseline than during all remaining conditions, including placebo (p < .01). No dosage effects were found for stimulants, depressants, or “other” substance use.
Possible Adverse Side Effects
There was no significant effect of dosage on self-report of total side effects, pulse rate, or systolic blood pressure. The most commonly reported adverse side effects were decreased appetite and trouble sleeping. Only 2 of the 24 participants (8.3%) dropped out due to side effects. A significant main effect for dosage was found for diastolic blood pressure, F(4, 80) = 2.65, p = .04, partial η2 = .12. This effect was linear, with increasing diastolic blood pressure associated with increasing dosage. Tukey’s HSD comparison tests indicated that 30 mg was associated with elevated diastolic blood pressure relative to baseline (p < .05). It should be noted that mean diastolic blood pressure readings were within normal limits (i.e., less than 80) across all phases (see Table 2).
Individual Response to LDX Versus Placebo
To gauge the degree to which individual students with ADHD responded to each LDX dosage and placebo, a RCI (Jacobson & Truax, 1991) was calculated for two primary outcome measures: CAARS ADHD Index and BRIEF Metacognition Index. These two measures were selected because they represented general indicators of ADHD symptoms (CAARS) and planning/organizational skills critical for college success (BRIEF-A). The RCI indicates the degree to which treatment-induced changes are beyond chance levels (i.e., statistically reliable). Jacobson and Truax (1991) asserted that when RCI ≥ 1.96, it is unlikely that a posttest score does not reflect real change. RCIs were calculated for placebo, 30-mg LDX, 50-mg LDX, and 70-mg LDX using baseline scores as a comparison (i.e., RCI represents degree of change from baseline score).
Mean RCIs for CAARS ADHD Index ranged from 1.42 in placebo to 2.90 in the 70-mg condition (see Table 3 for RCI descriptive statistics). In similar fashion, the percentage of positive responders (i.e., participants with RCI ≥ 1.96) ranged from 39.1% in placebo to 63.6% in 30-mg and 70-mg conditions (see Figure 4). Furthermore, 86.4% of participants exhibited a positive response to at least one LDX dosage condition.
Reliable Change Indices for Self-Report Ratings of ADHD and Executive Function
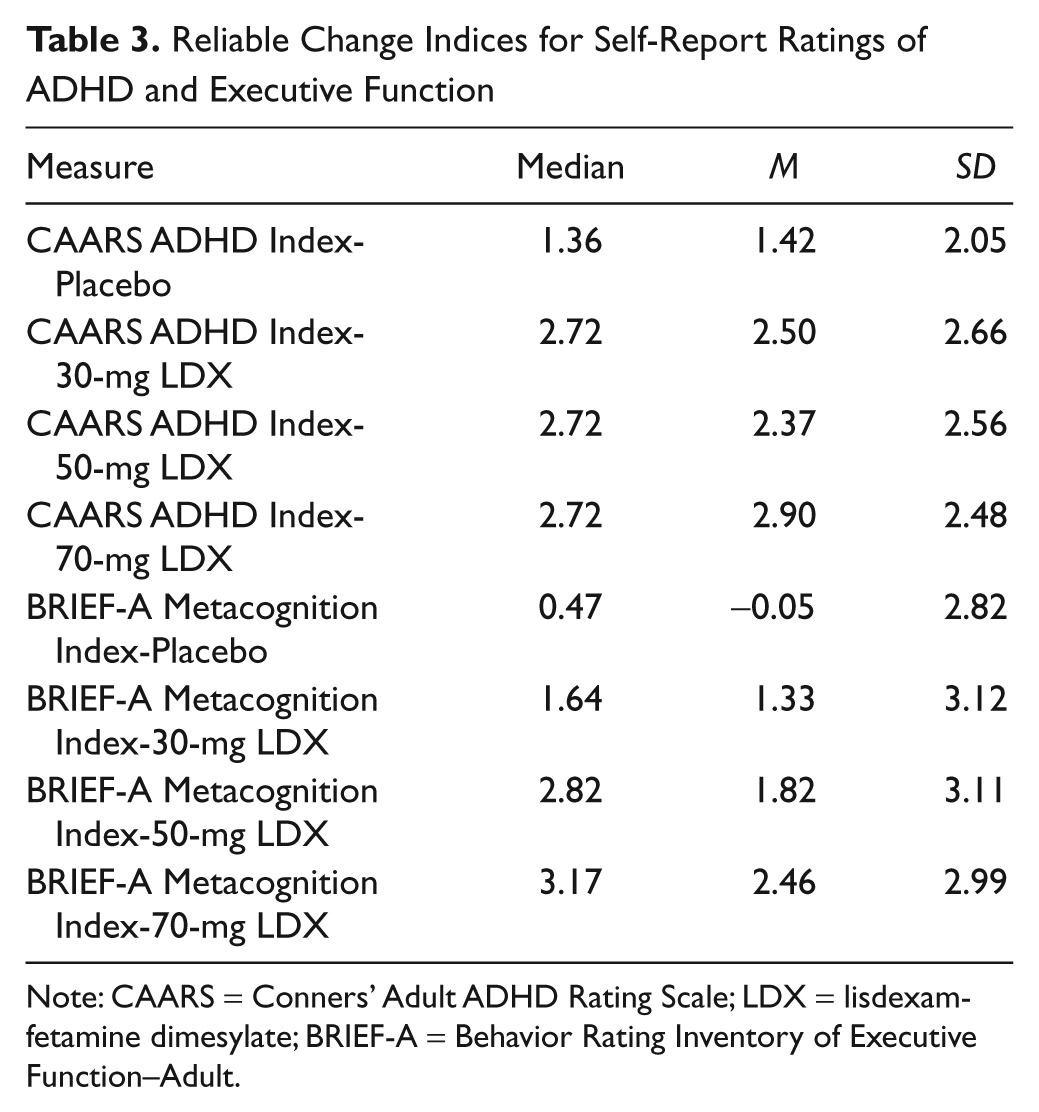
Note: CAARS = Conners’ Adult ADHD Rating Scale; LDX = lisdexamfetamine dimesylate; BRIEF-A = Behavior Rating Inventory of Executive Function–Adult.
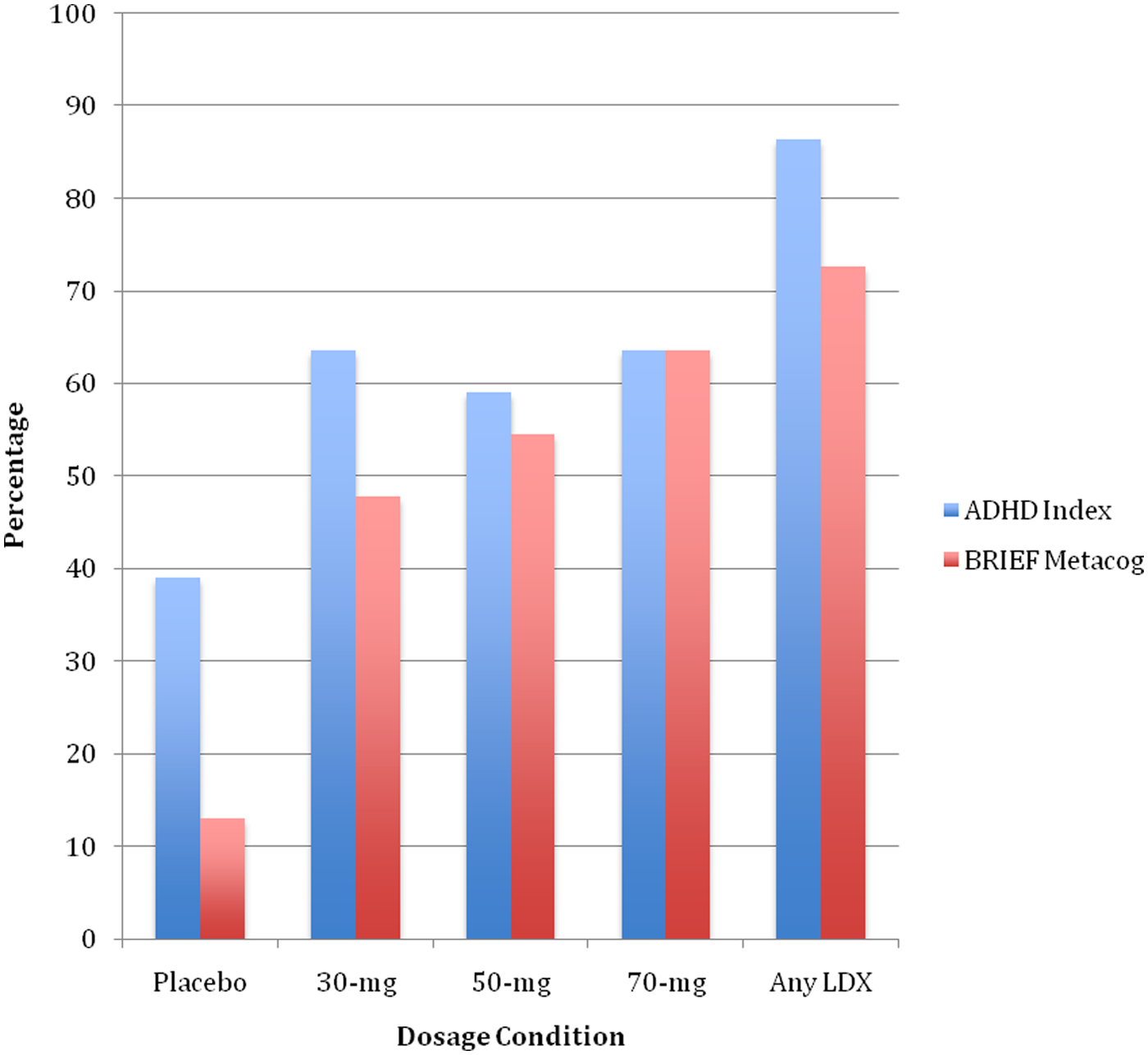
Percentage of positive responders (RCI ≥ 1.96) across dosage conditions
Mean RCIs for BRIEF Metacognition Index ranged from -0.05 in placebo to 2.46 in the 70-mg condition (see Table 3). The percentage of positive responders ranged from 13% in placebo to 63.6% in the 70-mg condition (see Figure 4). Finally, 72.7% of participants exhibited a positive response to at least one LDX dosage condition.
Comparison With Non-ADHD Controls
A series of independent sample t tests was used to compare ratings on the two primary outcome measures (CAARS ADHD Index and BRIEF Metacognition Index) for non-ADHD controls (n = 26) during no-medication baseline relative to participants with ADHD during placebo, 30-mg, 50-mg, and 70-mg LDX conditions. Non-ADHD control ratings were also compared with ratings from participants with ADHD during the lowest effective dosage condition determined by individual response (i.e., lowest dosage associated with RCI ≥ 1.96). In all cases, non-ADHD control ratings were significantly lower for CAARS ADHD Index (M = 36.19; SD = 4.76; all ps < .01) and BRIEF Metacognition Index (M = 44.31; SD = 7.62; all ps < .05). In addition, effect sizes were calculated to estimate the magnitude of ADHD versus non-ADHD control during each medication phase using Glass’s procedure: ADHD rating—non-ADHD control rating divided by non-ADHD control standard deviation (Kline, 2004). All effect sizes were in the large range; however, these were systematically smaller as LDX dosage increased (see Figure 5).
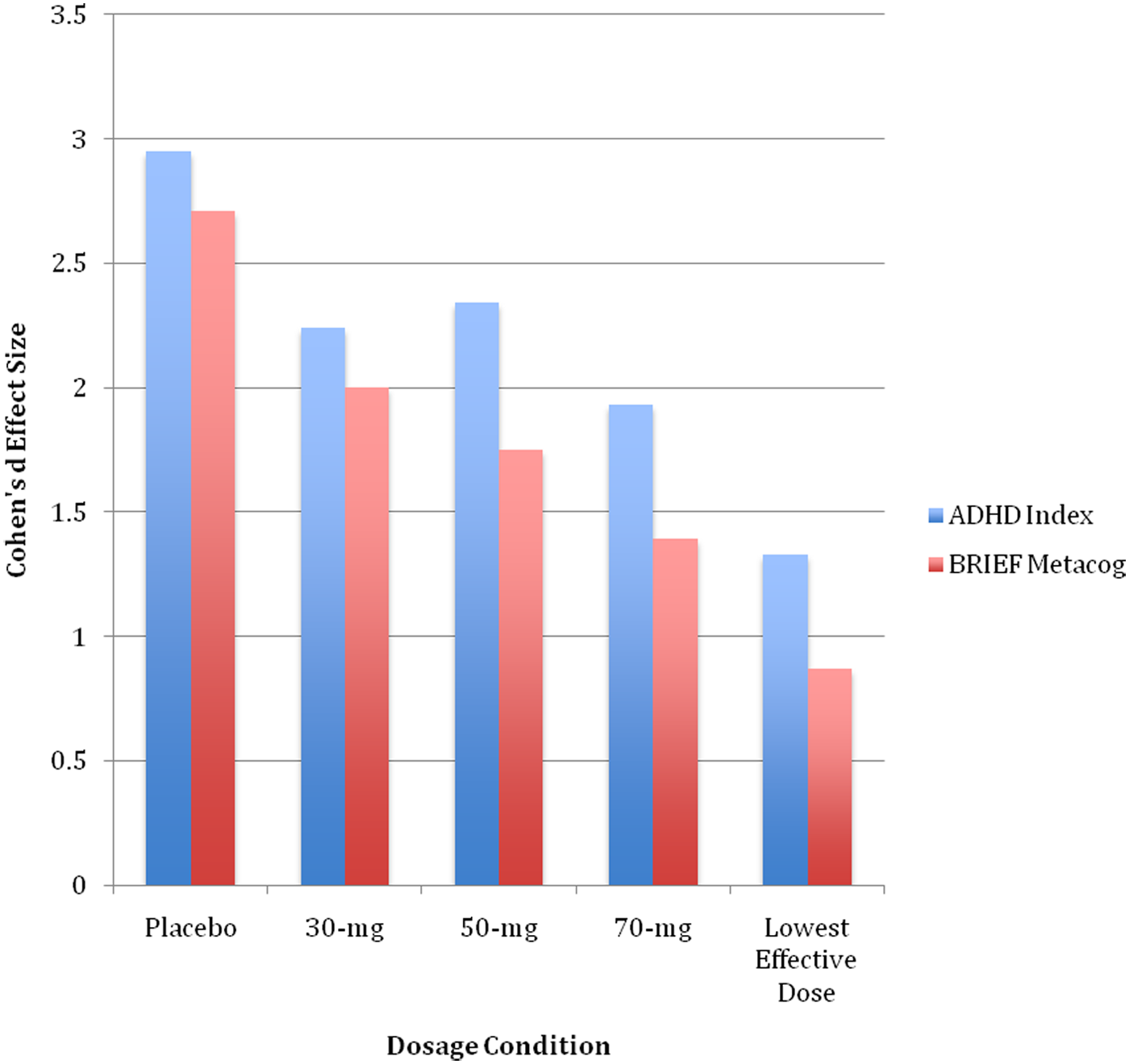
Magnitude of differences between ratings of participants with ADHD during medication conditions and non-ADHD controls
Discussion
As hypothesized, all LDX dosages were associated with statistically significant and large reductions in ADHD symptoms relative to nonmedication baseline and placebo. LDX-associated reductions were particularly evident for inattention, variability of attention over time, and hyperactivity/restlessness. Effects were smaller and less consistent for problems with impulse control, presumably because CAARS and CPT-II scores in this dimension were well within the normal range at baseline. LDX dose-response effects on ADHD symptoms were primarily linear indicating symptom decrease associated with increase in dosage. These findings are consistent with prior studies of LDX with adult samples (e.g., Adler et al., 2008) and support the efficacy of this medication for symptom relief in college students with ADHD.
Equally strong and linear LDX effects were found for specific aspects of executive functioning related to task management, planning, organization, study skills, and working memory. These results are not surprising given the strong relationship between attention and executive function (Scope, Empson, & McHale, 2010). The large magnitude of these effects is particularly compelling given the critical importance of organization, planning, and study skills for academic success (Hale et al., 2011; Peterson et al., 2003). In contrast, there were weaker and less consistent LDX effects on self-report of behavioral regulation and direct assessment of verbal learning/memory. As was the case for impulse control, behavioral regulation and verbal learning/memory scores at baseline were within normal limits, thereby minimizing the potential impact of pharmacotherapy.
Using the RCI (Jacobson & Truax, 1991) as a metric for clinically significant individual treatment response, more than 85% of the sample evidenced statistically significant ADHD symptom reduction in response to at least one of the three LDX dosages. There were fewer positive responders on the executive functioning measure; however, a substantial majority of participants met criteria for positive treatment response in this critical area. A substantial percentage (39.1%) of participants showed a positive placebo response for reduction of ADHD symptoms; however, very few positive placebo responders were found related to improvements in executive functioning (13%). When considering individual responses based on ADHD symptoms, the obtained response rates for placebo and individual dosages are similar to those found previously for adolescents (Findling et al., 2011) and adults with ADHD (Adler et al., 2008), and the overall rate of response to any LDX dosage is very similar to that found for children with ADHD (Findling, Ginsberg, Jain, & Gao, 2009).
Despite the large and clinically significant LDX effects on ADHD symptoms and executive functioning, participants with ADHD still showed large deficits when compared with a sample of typical, nondisordered college students. Effect size differences between groups decreased with increasing dosage but even at the 70-mg dosage condition, this difference was in what is typically considered the large range (Cohen, 1988). Thus, although mean standard scores for ADHD symptoms and executive functioning were in the normal range relative to the standardization sample for each measure, college students with ADHD remained at significant disadvantage relative to their peers. Given the relative brevity of this trial, it may be unrealistic to expect college students with ADHD to improve to the point of “normalization.” This finding, however, highlights the need to develop effective psychosocial treatment for the college ADHD population as an adjunct to pharmacotherapy.
LDX Effects on Psychological and Social Functioning
Although self-report of psychopathological disorder symptoms was reduced by LDX relative to nonmedication baseline, the apparent impact of medication in this area of functioning was relatively small. In fact, only one significant LDX versus placebo difference was obtained, with 70 mg resulting in lower depression scores relative to placebo. Commensurate functioning in this area is a notable finding, however, as it indicates that LDX did not increase symptoms of psychopathological disorders, including anxiety and depression. In similar fashion, LDX did not increase flat affect or emotional lability nor did it diminish positive affect. Furthermore, there were no significant effects of LDX on social functioning. Thus, although LDX was not associated with improved social functioning, it is noteworthy that this medication did not appear to negatively impact social functioning.
Adverse Side Effects
There was very little evidence of significant adverse side effects for LDX in this trial. Only two participants (8.3%) dropped out of the trial; this is a substantially lower drop-out rate relative to prior LDX investigations with adults (e.g., Adler et al., 2008). Admittedly, the current study was briefer in duration than prior investigations; however, stimulant side effects are most likely to appear early rather than late in treatment (D. F. Connor, 2006). Furthermore, LDX was not associated with an increase in self-reported alcohol or substance use. In fact, participants reported diminished overall use of substances, especially hallucinogens, relative to baseline. Similarly, there was no significant change in self-report of possible adverse side effects, although the percentage of these appears to increase from placebo to 50 mg if the data are viewed descriptively. Consistent with the stimulant medication literature (D. F. Connor, 2006), insomnia and reduction of appetite were the most common adverse events, and these were uniformly reported to be mild in severity. Finally, there were no significant changes in systolic blood pressure or pulse rate associated with LDX; however, there was a mild increase in mean diastolic blood pressure. This increase was not clinically significant and was only statistically significant for 30 mg relative to baseline.
Limitations
Conclusions based on this investigation are limited by several factors. First, this study included a small sample relative to prior trials of LDX in the adult ADHD population. Additional investigations with larger samples are necessary to support the efficacy of LDX for treatment of ADHD in college students. A second limitation of the present study is that individuals with cardiovascular conditions and some psychiatric comorbidities (e.g., bipolar disorder) were excluded due to safety concerns thereby limiting the generalizability of these findings to the ADHD college student population as a whole. Third, the relatively short duration of the trial (i.e., only 1 week per dosage condition) limited the opportunity to assess possible longer term impact of LDX, particularly for psychological and social functioning. In addition, direct measures of academic/educational functioning were not included. We attempted to obtain professor and self-report ratings of academic performance; however, complete data on these measures were available for very few participants, and the duration of the study was too brief to adequately assess overall academic functioning.
Clinical Implications and Conclusions
Although untreated college students with ADHD may be only mildly impaired relative to the typical young adult population, they are at a significant disadvantage in multiple areas of functioning relative to their classmates. LDX is associated with statistically and clinically significant improvement in the two areas that college students with ADHD are most deficient relative to their nondisordered peers: ADHD symptoms and executive functioning. Therefore, LDX should be considered a primary treatment for ADHD in the college population, and response to treatment should be assessed not only in terms of ADHD symptom reduction but also with respect to executive functions most critical for educational success (i.e., planning, organization, and task management). Less-pronounced LDX effects were found for psychological and social functioning; however, there was no evidence that LDX worsens performance in these areas nor were significant adverse side effects experienced by most participants. It is unclear at this point whether the continued relative deficit in executive functioning despite salutary effects of LDX is associated with continued educational/academic deficits. There is a critical need, therefore, to examine the impact of LDX and similar medications on the academic functioning of college students with ADHD as well as the development and evaluation of psychosocial/educational interventions to supplement pharmacotherapy.
Footnotes
Acknowledgements
The conduct of this study was ably assisted by Cheryl Ashcroft and Pamela Rohland who facilitated recruitment of participants with ADHD on each campus as well as Sharon DeLuca, Susan Kitei, and Thomas Novak who conducted physical examinations and monitored adverse side effects throughout the trial. In addition, Derek DeBellis, Matthew Gormley, Christine Perndorfer, and Hana Reissner assisted with data collection, scoring, and data entry.
The authors independently made decisions regarding all aspects of this study, including design, data collection, analysis, and interpretation.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an Investigator Sponsored Trial by Shire Pharmaceuticals, Wayne, PA.