
Abstract
Individuals with ADHD—children, adolescents, and young adults—smoke at rates that are significantly higher than those of the general population or of healthy controls (Lambert & Hartsough, 1998; Milberger, Biederman, Faraone, Chen, & Jones, 1997a, 1997b; Molina & Pelham, 2003; O. F. Pomerleau, Downey, Stelson, & Pomerleau, 1995; Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008). The association between ADHD symptoms and tobacco smoking, which has been confirmed in large population-based studies in nonclinical samples (Kollins, McClernon, & Fuemmeler, 2005; Tercyak, Lerman, & Audrain, 2002), is due to a multifactorial model of etiology (McClernon & Kollins, 2008).
Biological Vulnerability
The ADHD-smoking comorbidity is in part assumed to be the result of a “genetic linkage” because variants of genes involved in the dopaminergic and serotonergic neurotransmission and metabolism are involved in the pathogenesis of both disorders (Faraone et al., 2005; Gerra et al., 2005; Hutchison, LaChance, Niaura, Bryan, & Smolen, 2002; Lerman et al., 1998; Luciano et al., 2004; Skowronek, Laucht, Hohm, Becker, & Schmidt, 2006; Timberlake et al., 2006). Moreover, smoking seems to be more rewarding in ADHD individuals than in healthy controls due to an amplified dopamine response stimulated by nicotine (Brody et al., 2004; Volkow et al., 2007).
Psychological Vulnerability
Apart from the biological vulnerability, ADHD individuals do also exhibit psychological and social vulnerabilities that might be of influence by increasing the risk for initial tobacco use. People suffering from ADHD are more impulsive, have more difficult peer interactions, and, due to their novelty-seeking traits, are predisposed to experiment early with tobacco (Milberger et al., 1997a). The transition to regular smoking is more likely in ADHD individuals because of a mechanism of negative reinforcement (Levin et al., 1996). Therefore, this transition occurs earlier (Lambert & Hartsough, 1998). The mechanism of negative reinforcement works because typical ADHD symptoms are reduced or improved by consuming nicotine (Levin et al., 1996; Potter & Newhouse, 2008). Executive function deficits, especially inattention, seem to significantly predict smoking in adolescents and young adults, not only in ADHD-diagnosed children but also in children without a diagnosis of the disorder (Aytaclar, Tarter, Kirisci, & Lu, 1999; Burke, Loeber, & Lahey, 2001; Molina & Pelham, 2003). The number of ADHD symptoms reported independent of an ADHD diagnosis significantly predicted the number of cigarettes smoked per day in a population-based study published by Kollins et al. (2005). These findings support the “self-medication” hypothesis of smoking among individuals with ADHD. Because of this negative and positive reinforcement loop, ADHD is also a predictor for progression from initiation of smoking to daily use (Rohde, Kahler, Lewinsohn, & Brown, 2004). These processes explain, in part, an altered sensitivity of ADHD individuals to smoking abstinence (McClernon et al., 2008), the perceived increased withdrawal severity in ADHD patients (C. S. Pomerleau et al., 2003), the more severe physical dependence on nicotine (Wilens, Vitulano, Upadhyaya, Adamson, Parcell, et al., 2008; Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008), and the greater difficulty quitting (Humfleet et al., 2005; O. F. Pomerleau et al., 1995) in these patients.
Symptom Domains
The relative contribution of the different symptom domains in ADHD (inattentive vs. hyperactive-impulsive ADHD symptoms) on smoking behavior remains controversial to date and has to be judged carefully under a developmental perspective. Burke (Burke et al., 2001; Burke, Loeber, White, Stouthamer-Loeber, & Pardini, 2007) reported inattention to be an important risk factor for tobacco use in early adolescence. In his first sample consisting of 199 clinic-referred boys, a sample composed primarily of children who qualified for diagnoses of disruptive behavior disorders, he described adolescent inattention as associated with a 2.2 times greater risk for tobacco use at the age of 15, even after controlling for conduct disorder (CD). The second study found inattention predicting tobacco use in adolescence in a community sample followed into young adulthood. In contrast, in a nonclinical population of young adults, symptoms of hyperactivity have been reported to be more strongly associated with the lifetime risk of smoking than inattentive symptoms (Kollins et al., 2005). A recent population-based longitudinal study in (n = 13,494) young adults evaluating the relative contributions of different symptom domains on smoking progression found the following results: Individuals reporting high levels of hyperactive-impulsive ADHD symptoms were more likely to progress from no smoking at mean age of 15.7 years to regular smoking at the age of 23 years, whereas high levels of inattentive ADHD symptoms did not predict smoking progression. High levels of self-reported inattentive symptoms were significantly associated with a high level of nicotine dependence as measured with the Fagerström Test for Nicotine Dependence (FTND; Fuemmeler, Kollins, & McClernon, 2007).
Gender Differences
Little is known with respect to gender differences in smoking habits of individuals with ADHD. Most research has been undertaken in hyperactive boys. Only Biederman reported a fourfold increased risk for smoking in ADHD girls as compared with control girls (Biederman et al., 1999).
Gender differences in smoking habits in ADHD individuals have been reported recently as a trend in Wilens’ study (Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008) in a sample of 80 young ADHD patients (between 15 and 25 years) as compared with 86 control probands. Given that there were higher percentages of females relative to males (43% male patients, 38% male controls) and the control sample was not gender matched, the significance of the finding seems to be limited, but there was a trend toward more severe nicotine dependence in female smokers with ADHD than in male smokers with ADHD as measured with the Fagerström Tolerance Questionnaire (FTQ), the original instrument to measure cigarette use and precursor of the FTND.
Galera investigated the link between childhood hyperactivity-inattention symptoms and smoking in adolescence in a large population-based sample, a cohort representative of the general population, of 421 boys and 495 girls aged 7 to 18. In females, the hyperactivity-inattention symptoms contributed independently to subsequent daily smoking. In contrast, in males hyperactivity-inattention symptoms alone did not increase the risk for smoking but CD symptoms did (Galera, Fombonne, Chastang, & Bouvard, 2005). In a large population-based study, girls with ADHD seemed to be at a slightly higher risk for nicotine dependence than did boys with ADHD independently of the effects of CD mediating the risk for substance use and abuse in both genders (Disney, Elkins, McGue, & Iacono, 1999).
Therefore, as far as gender differences are concerned, current knowledge is scarce. But girls with ADHD seem to be at a higher risk for smoking than boys suffering from ADHD independently of CD.
In this study, we wanted to investigate smoking behavior in an adult sample of ADHD patients in comparison with a control group carefully matched for age, gender, and educational level. We hypothesized first to find a higher cigarette use in the ADHD population as compared with the control group and second, to find a higher degree of dependence in the ADHD group. Furthermore, we wanted to investigate if gender differences found in adolescent samples would be replicated in an adult sample of ADHD patients.
Method
A total of 60 participants with adult ADHD referred for diagnostics were consecutively recruited at the outpatient clinic of the Department of Psychiatry and Psychotherapy of the University Medical Centre Freiburg, which has long-standing experience in offering diagnostic and therapeutic services to adults with ADHD. The study was approved by the local ethics committee. Written informed consent was obtained from the patients after full explanation of the study. In all, 60 healthy control participants were recruited through newspaper advertisements. Patients and control participants were matched pairwise for gender, age, and educational level.
In both groups, Axis I disorders were carefully assessed with the Mini-International Neuropsychiatric Interview (MINI; Ackenheil, Stotz, & Dietz-Bauer, 1998; Sheehan et al., 1998). Patients suffering from severe, acute Axis I disorders requiring inpatient treatment such as major depression, severe anxiety disorders, and psychotic states were excluded from the study (Hirschfeld, 1999). Severity of depressive symptoms was assessed with the Beck Depression Inventory (BDI-II; Beck, Steer, Ball, & Ranieri, 1996) German version (Hautzinger, Keller, & Kühner, 2006), with a sum score between 0 and 63. General level of psychopathology was measured with the Symptom Check List–90–Revised (SCL-90-R; Derogatis & Cleary, 1977), German version (Franke, 1995; Schmitz et al., 2000).
Assessment of ADHD symptoms
As recommended by the German guidelines for adult ADHD (Ebert, Krause, & Roth-Sackenheim, 2003), the ADHD diagnosis was assessed following a detailed psychiatric interview that integrates common psychiatric and somatic differential diagnoses and the patients’ medical history. An experienced psychiatrist was in charge of the diagnostic procedure. Only patients who met the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for ADHD were included in the study (onset of ADHD symptoms before age 7, impairment present in two or more settings). Six of nine DSM-IV criteria for inattention as well as six of nine criteria for hyperactivity/impulsivity were required for the diagnosis of the combined subtype.
ADHD symptoms in childhood were self-rated retrospectively with the validated short-version of the Wender Utah Rating Scale–German (German: WURS-k; Retz-Junginger et al., 2002; Ward, Wender, & Reimherr, 1993), including 25 items on a 5-point Likert-type scale (not at all to severe, cutoff score = 30). Severity of ADHD symptoms in adulthood was also self-rated on a 4-point Likert-type scale corresponding to the diagnostic criteria of DSM-IV adapted for adults (ADHD–Self-report [German: ADHD-SB], 18 items, scale ranging from 0 to 3, not at all to severe; Rosler et al., 2004).
Differential assessment of the current ADHD symptoms was done with the Conners’ Adult ADHD Rating Scales (CAARS; Conners et al., 1999), German version (Christiansen et al., 2011). The self-rating instrument, long version (CAARS-S:L), was used in this study consisting of 66 items (rated on a 4-point Likert-type scale from not at all/never to very often). The CAARS provides eight empirically derived scales that help assess a broad range of disorder-specific problem behaviors: inattention/memory problems (Scale A), hyperactivity/restlessness (Scale B), impulsivity/emotional lability (Scale C), and problems with self-concept (Scale D). The CAARS also provides separated symptom scores for inattention (Scale E) and hyperactivity/impulsivity (Scale F) and a total ADHD symptom score (Scale G). The subscores are sums of the corresponding items divided by the number of items.
Assessment of Smoking Habits
Assessment of smoking habits was done with the FTND, a valid and widely used self-report instrument for assessing cigarette use (Heatherton, Kozlowski, Frecker, & Fagerstrom, 1991). The FTND is a revision of the FTQ (Fagerstrom & Schneider, 1989). The score of this instrument has been found to be correlated with cotinine concentration, a biomarker of nicotine dependence (C. S. Pomerleau, Carton, Lutzke, Flessland, & Pomerleau, 1994). The FTND consists of six questions (see Figure 1). A higher FTND score indicates a greater degree of nicotine dependence or use (range = 0-10).

Items and scoring for FTND.
A screening question divided participants into current smokers and nonsmokers. Participants then completed additional items, including questions relating to past smoking, such as age when he or she started smoking and attempts to quit.
To assess the degree of inclination toward smoking from our data, we calculated two scores: a score measuring early onset of smoking (Nicotine onset score (NIC) onset score = 30 − age of onset of smoking) and a Fagerström total score (FAG) total score, which represents the severity of nicotine addiction depending on different factors—having never smoked, having smoked but being abstinent weighted by the period of abstinence, age of onset of smoking, and being a current smoker. Current smokers have the highest FAG total score identical to the FTND score. In participants who quit smoking, the FAG total score was calculated as follows using x = years of abstinence: FAG total score = 5 × (1 − x / 20). Thus, the longer the abstinence period, the smaller the FAG total score. In ex-smokers without known abstinence period, the abstinence period was assumed to be 10 years, resulting in FAG total score = 2.5. Finally, participants who never smoked were represented with a FAG total score of −5. This was chosen to distinguish participants who never smoked from current smokers because the minimum FTND score in current smokers is zero. In this way, both scores are constructed to be available for all included participants.
Statistical Analysis
Group comparison
We compared ADHD patients with control participants using two-sided t test for parametric data and chi-square test for nonparametric data.
To test a possible relationship between ADHD symptoms and nicotine dependence in the whole sample, we calculated a one-way, between-group MANOVA with group (ADHD vs. controls) as main factor and two dependent variables: FAG total score and NIC onset score. Another MANOVA was performed to investigate gender differences in the mentioned variables for the two groups (ADHD vs. controls). All data were analyzed using SPSS for Windows (Release 15.0). A p value of .05 was chosen as the criterion of significance.
Results
Study Group Structure
We assessed a total number of 120 participants. Data were obtained from 60 ADHD patients and 60 control participants. Mean age of all participants was 35.27 years (SD = 10.62, range = 18-58). There were no significant differences with respect to age, educational level, or gender distribution, χ2(1, N = 120) = .000, p = .574, (40% males in ADHD group as well as controls) between the two groups. Educational level was coded low after 8 years of school education, middle after 10 years of education, and high after 13 years of education. A total of 18% of our sample had a low educational level, 32.8% a middle educational level, and 47.5% a high educational level. As expected, the load of psychopathological symptoms measured with SCL-90R, symptoms of depression measured with the BDI, and ADHD symptoms in child and adulthood (actual ADHD symptoms: ADHD-SB-score and CAARS-G, childhood ADHD symptomatology: WURS-score) was significantly higher in the ADHD group (see also Table 1).
Demographic Characteristics of the Sample.
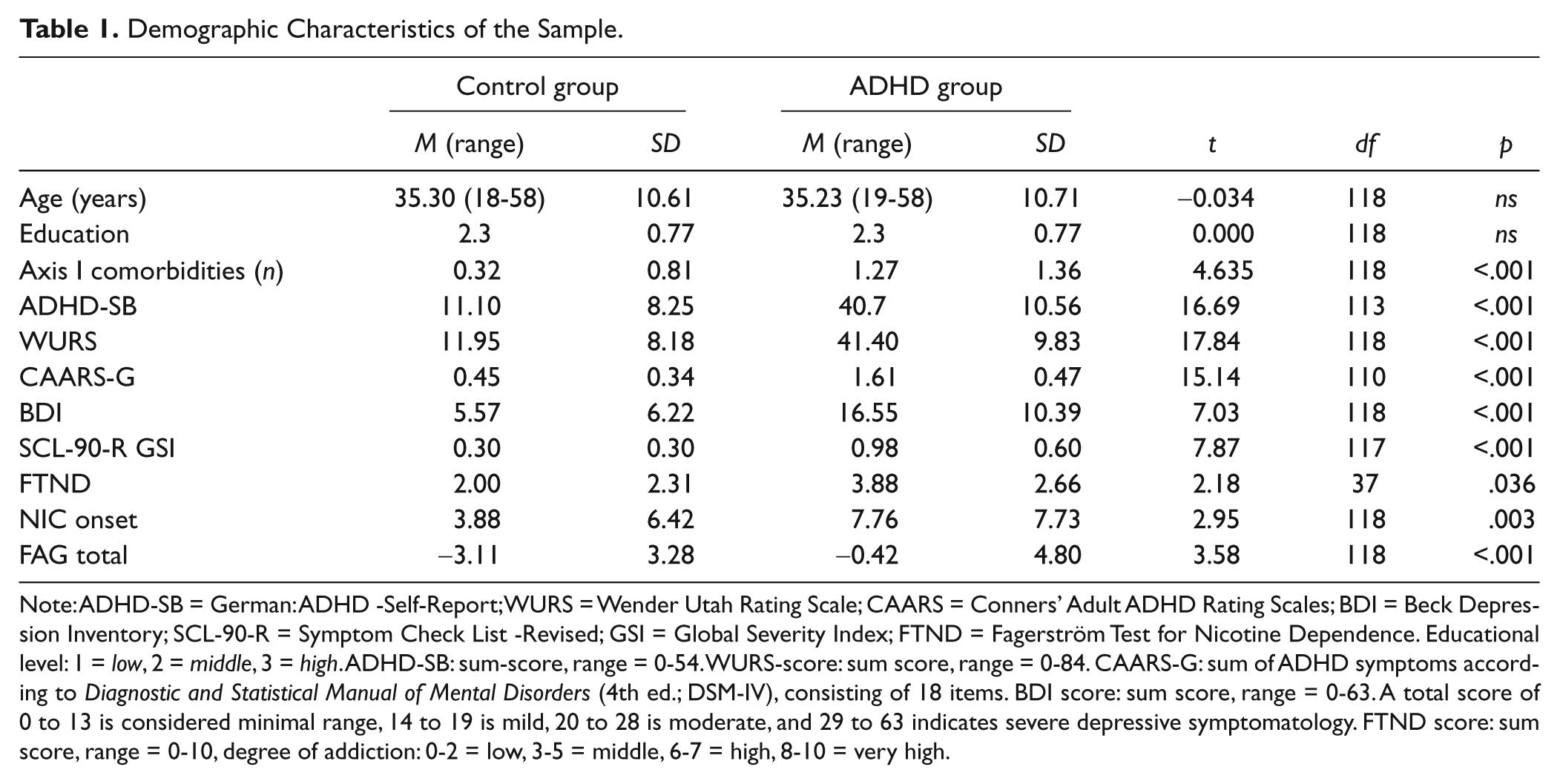
Note: ADHD-SB = German: ADHD -Self-Report; WURS = Wender Utah Rating Scale; CAARS = Conners’ Adult ADHD Rating Scales; BDI = Beck Depression Inventory; SCL-90-R = Symptom Check List -Revised; GSI = Global Severity Index; FTND = Fagerström Test for Nicotine Dependence. Educational level: 1 = low, 2 = middle, 3 = high. ADHD-SB: sum-score, range = 0-54. WURS-score: sum score, range = 0-84. CAARS-G: sum of ADHD symptoms according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV), consisting of 18 items. BDI score: sum score, range = 0-63. A total score of 0 to 13 is considered minimal range, 14 to 19 is mild, 20 to 28 is moderate, and 29 to 63 indicates severe depressive symptomatology. FTND score: sum score, range = 0-10, degree of addiction: 0-2 = low, 3-5 = middle, 6-7 = high, 8-10 = very high.
ADHD patients had significantly more comorbidities. ADHD patients had at least one lifetime Axis I comorbidity in 66.6% of cases compared with 16.7% of cases with at least one psychiatric diagnosis in the control group. Thus, 40 participants of the ADHD group suffered from lifetime psychiatric comorbidities. These were as follows: unipolar depression (n = 35), bipolar disorder (n = 3), anxiety and obsessive compulsive disorders (n = 12), and alcohol abuse or dependence (n = 3). Control probands had the following psychiatric diagnoses according to the MINI: unipolar depression (n = 9), anxiety and obsessive compulsive disorders (n = 4), and alcohol abuse or dependence (n = 3).
A total of 16 ADHD patients (26.7%) were diagnosed according to DSM-IV as having an inattentive subtype of ADHD. All other ADHD patients had a combined type diagnosis.
At the time of assessments, patients did not receive any ADHD-specific medication at least 6 months before assessments. Most participants had not received ADHD-specific medication during childhood and adolescence (n = 58). In all, 18 patients had been medicated with methylphenidate or atomoxetine in adulthood.
Smoking Prevalence and Smoking Habits
Based on the additional screening question of the FTND, we calculated the rate of current smokers in the two study groups. In all, 31.6% of the whole sample (n = 38 participants, 13 men [27% of all males] and 25 women [34.7% of all women]) were current smokers.
Current smoking was significantly more frequent in the ADHD group: 25 (41.7%) of the ADHD patients were current smokers, whereas only 13 (21.7%) of the controls reported current smoking, χ2(1, N = 120) = 5.55, p = .015.
There was a trend for the participants with ADHD to smoke sooner after waking as compared with the control probands (cutoff score = 2), χ2(1, N = 39) = 3.337, p = .067. ADHD participants smoked significantly more often while sick, χ2(1, N = 39) = 11.607, p = .001, and had a significantly higher FTND score (t = 2.16, df = 37, p = .036). The two groups did not differ significantly with regard to age of onset of regular smoking (t = −1.77, df = 46, p = .083) and other variables given in Tables 2 and 3.
Group Comparison Concerning Smoking Variables.
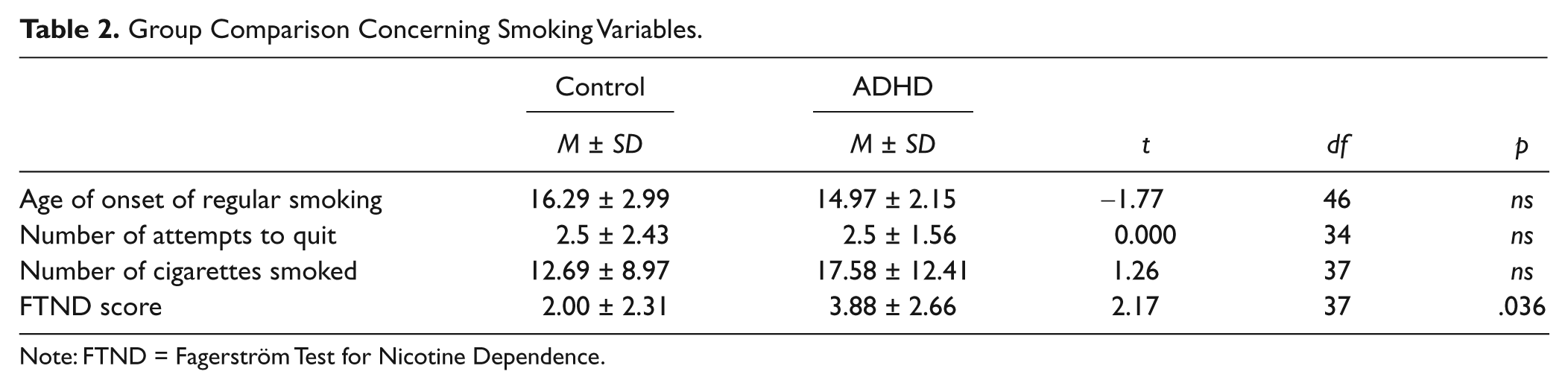
Note: FTND = Fagerström Test for Nicotine Dependence.
Group Comparison Concerning Smoking Variables.
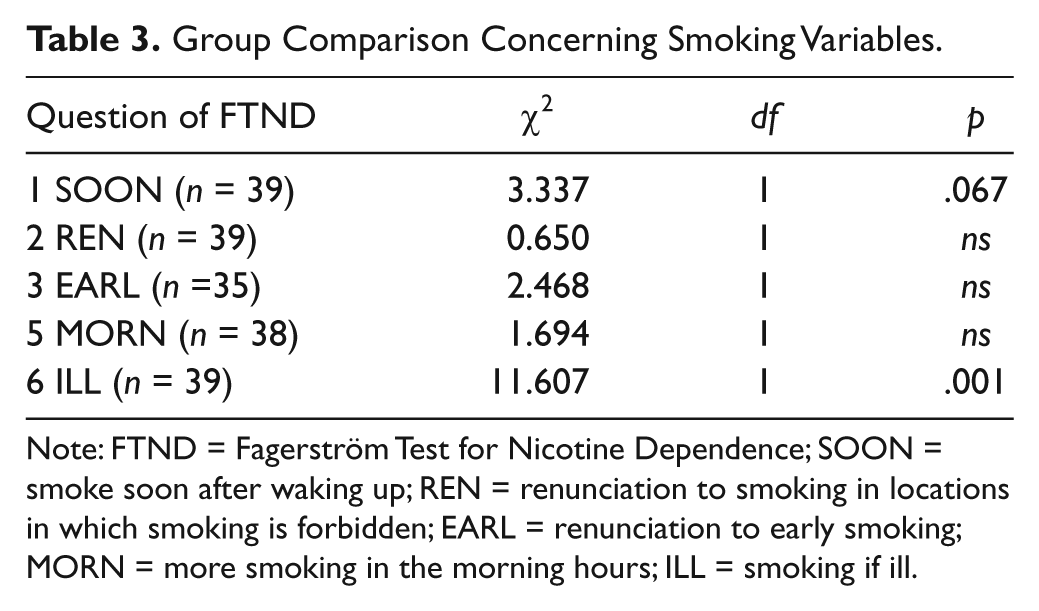
Note: FTND = Fagerström Test for Nicotine Dependence; SOON = smoke soon after waking up; REN = renunciation to smoking in locations in which smoking is forbidden; EARL = renunciation to early smoking; MORN = more smoking in the morning hours; ILL = smoking if ill.
Correlations Between ADHD Symptoms and Nicotine Dependence
There were only low correlations between ADHD symptoms and the FAG total score as well as the NIC onset score in the whole sample. Among them the highest and highly significant correlations were found between the hyperactivity/restlessness (Scale B) of the CAARS and the NIC onset score (Pearson’s r = .392, n = 114, p ≤ .001) as well as the FAG total score (Pearson’s r = .399, n = 114, p ≤ .001). There was also a significant correlation between the CAARS hyperactivity/impulsivity scale (Scale F) and the FAG total score (Pearson’s r = .394, n = 114, p ≤ .001). The correlation between childhood ADHD symptoms measured with the WURS and FAG total score was also found highly significant (Pearson’s r = .394, n = 114, p ≤ .001).
Relationship Between ADHD and Nicotine Dependency
To test a possible relationship between ADHD symptoms and nicotine dependence as well as early smoking initiation in the whole sample, we calculated a one-way between-groups MANOVA with group (ADHD vs. controls) as main factor and two dependent variables: FAG total score and NIC onset score. There was a statistically significant difference between ADHD patients and controls on the combined dependent variables, F(2, 117) = 6.55, p = .002, Wilks’s λ = .89; partial η2 = .101. When the results for the dependent variables were considered separately, the difference between the groups reached statistical significance for both scores using a Bonferroni-adjusted alpha level of .025: for the FAG total score, F(1, 118) = 12.84, p ≤ .001; partial η2 = .098, and for the NIC onset score, F(1, 118) = 8.96, p = .003; partial η2 = .071. An inspection of the mean scores indicated that the ADHD group had a higher NIC onset score (M = 7.76, SD = 7.76) than did the controls (M = 3.88, SD = 6.42), representing early onset of smoking, and presented also a higher FAG score (M = −.42, SD = 4.7) than did the controls (M = −3.11, SD = 3.2), representative for a higher weighted inclination to smoke.
The influence of the factor group (ADHD vs. controls) on the dependent variable FAG score remained significant after inclusion of the covariate BDI score in the MANOVA, F(1, 118) = 4.093, p = .045, whereas the influence on NIC onset score was not longer significant after inclusion of the BDI score, F(1, 118) = 2.745, p = .100.
Gender Differences
As far as gender differences are concerned, we calculated a one-way between-groups MANOVA with group (ADHD vs. controls) as a main factor, layered by sex (male or female), and FAG total score and NIC onset score as dependent variables and found significant influence of gender on the dependent variables.
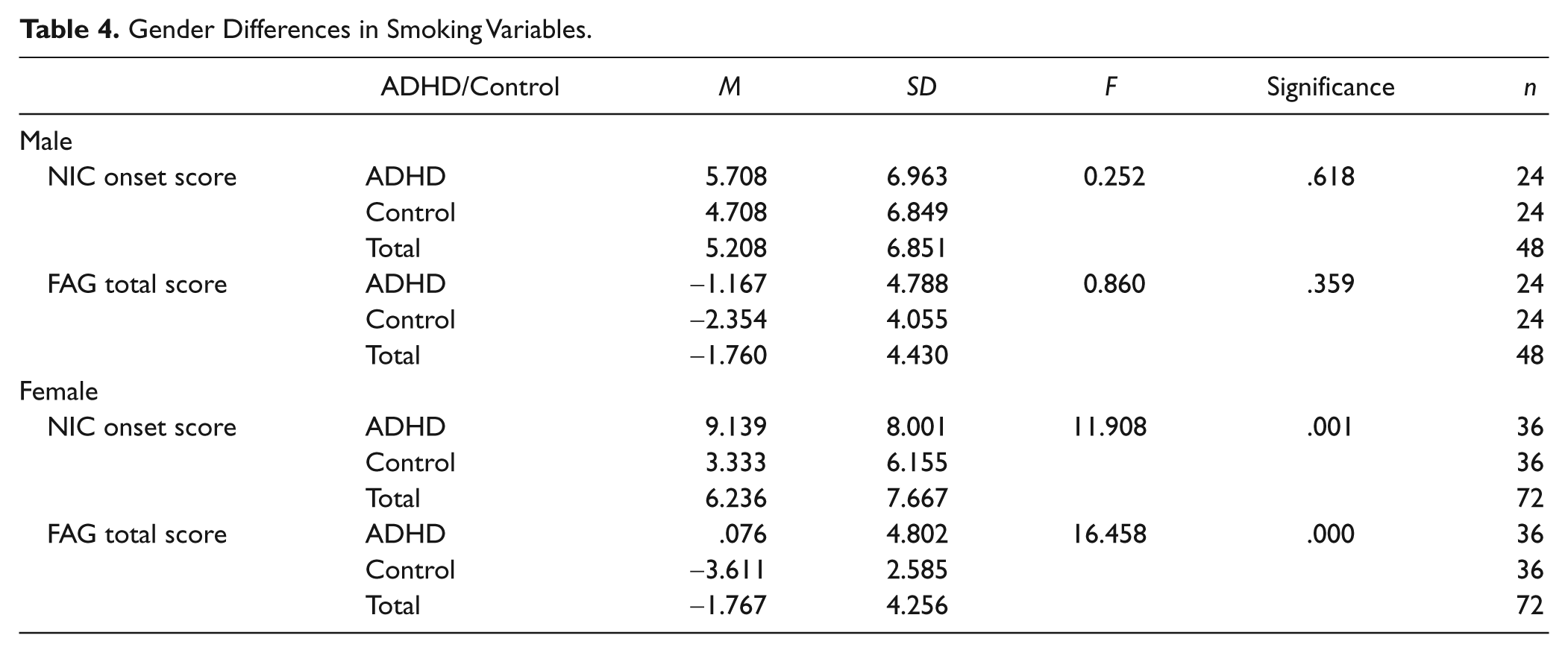
There was a statistically significant difference between ADHD patients and controls on the combined dependent variables only for women, F(2, 69) = 8.15, p = .001; Wilks’s λ = .81; partial η2 = .191. When the results for the dependent variables were considered separately for women only, the difference between the groups reached statistical significance for both scores using a Bonferroni-adjusted alpha level of .025: for the FAG total score, F(1, 72) = 16.46, p = .000, partial η2 = .19, and for the NIC onset score, F(1, 72) = 11.91, p = .001, partial η2 = .145. The mean scores (see Table 4) indicated that the women with ADHD had a much higher NIC onset than did the controls, representing early onset of smoking. Women also presented a higher FAG score representative for a higher weighted inclination to smoke.
Gender Differences in Smoking Variables.
Discussion
According to our expectations, we found a high rate of smokers in adult patients with ADHD (41.7%) as compared with an age- and gender-matched control group (21.7%). This observation is in line with previous studies in this field (Fischer, Barkley, Smallish, & Fletcher, 2002; Lambert & Hartsough, 1998; Milberger et al., 1997a, 1997b; Molina & Pelham, 2003; O. F. Pomerleau et al., 1995; Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008). The results of our study confirm more severe nicotine dependency as reflected in the FTND score in ADHD patients. Moreover, we were able to show earlier onset of smoking initiation and a much higher inclination to smoke in the adult ADHD sample when compared with the control participants. Women with ADHD seem to be a high-risk population, given their high inclination to smoke and the early onset of smoking in this group.
Prevalence of Smoking in Adult ADHD
In the general population, the prevalence of regular smoking according to the German Mikrozensus data from 2005 in the age group of 30 to 35 years was 36.1% for men and 24.2% for women (www.destatis.de). According to the telephonic health survey in 2003, 36.8% of the German male population and 29.9% of the female population of the relevant age group were current smokers (Lampert & Burger, 2005). Thus, in our whole sample, we had a higher smoking rate in females with 34.7% and a lower smoking rate of 27% in males than in the general population probably due to the higher smoking prevalence in the female ADHD patients.
The percentage of smoking in ADHD patients was significantly higher than the percentage of smoking in the control sample (41.7% vs. 21.7%). This finding is in line with previous study results. For example, Lambert reported results from a longitudinal study: 42% of the grown up hyperactive patients were smokers, whereas only 26% of the healthy control probands reported current smoking (Lambert & Hartsough, 1998). Similar results were reported also by Wilens in a study population aged 19.2 years in which 41% in the ADHD group versus 21% in the controls were smoking (Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008). In a prospective study investigating an adolescent population aged 6 to 17 years, Milberger found current smoking in 19% of the ADHD patients versus 10% in the control group (Milberger et al., 1997a).
In the ADHD subgroup, only 25% of the male patients (vs. 29% of the male controls) smoked, whereas a high percentage of 52.7% of females suffering from ADHD (vs. 16.6% of the female controls) smoked. This finding is unexpected because of the generally higher smoking prevalence in males in the general population. O. F. Pomerleau et al. (1995) reported data from an adult ADHD patient sample of 71 patients with a mean age of 33.9 years. A total of 42% of males and 38% of the women with ADHD smoked (O. F. Pomerleau et al., 1995). In part, this finding might be attributable to the higher percentage of females in the whole sample. The higher percentage of women might be due to a selection bias: We are investigating a treatment-seeking population, and therefore, we see generally more women in our specialized outpatient department.
More Severe Nicotine Dependency in ADHD Patients
We were able to confirm the results of previous studies concerning the degree of physical dependence. In our sample, ADHD patients had a significantly higher FTND score as compared with the control probands. ADHD patients had a mean FTND score of 3.88, indicating a medium-ranged degree of addiction, whereas controls had a mean FTND score of 2.00, indicating a low degree of addiction. O. F. Pomerleau found a mean FTQ score of 6.7, characterizing the ADHD patients in his sample as moderately dependent (O. F. Pomerleau et al., 1995). Wilens found a mean FTQ score of 4 in the ADHD patients compared with a mean FTQ score of 2.1 in the controls (Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008). Therefore, the results of the present study fit well in this line of studies. Wilens reported that ADHD patients smoked more often while sick, a finding that could be reproduced in our sample. This item of the FTND together with the item measuring the tendency to smoke sooner after waking up in the morning for which a trend was found in the present study are indicators of the difficulty refraining from smoking and therefore behavioral indicators of dependency.
Influence of Depression on Smoking in Adult ADHD
Depression is known to be strongly correlated with severe nicotine dependence (Khaled, Bulloch, Williams, Lavorato, & Patten, 2011). According to the literature, in our sample more than half of ADHD patients suffered from comorbid unipolar affective disorders. One could speculate that the finding of significantly more severe nicotine dependence (measured with FAG score) in adult ADHD is simply the result of more pronounced depressive symptoms in the adult ADHD group compared with controls. However, our finding remained significant after including the severity of current depressive symptoms measured with the BDI in our analyses.
Sex Differences in Smoking
Wilens found a trend toward more severe nicotine dependence in female smokers with ADHD than in male smokers with ADHD (Wilens, Vitulano, Upadhyaya, Adamson, Sawtelle, et al., 2008). In the present study, women in the ADHD group began earlier to smoke regularly than the males with ADHD (14.3 vs. 16.3 years) and had a significantly higher inclination to smoke as measured with the FAG score. Although, this finding should be interpreted cautiously given the selection bias in our study, our findings could have important implications with regard to the risks of maternal nicotine consumption for the fetus (e.g., growth retardation) and the findings of generally strong cessation problems in adult ADHD (Covey, Manubay, Jiang, Nortick, & Palumbo, 2008). Women with ADHD seem to experience even greater withdrawal severity during early abstinence as men (McClernon et al., 2011). As early initiation of smoking decreases the likelihood of cessation (Breslau & Peterson, 1996), women with ADHD might be a population with a heightened barrier to quit smoking. Studies investigating the association between maternal smoking during pregnancy and the risk of hyperactivity and inattention in the child have yielded inconsistent results, although recent studies seem to find no or only small causal relationships (Ball et al., 2010; Obel et al., 2011).
ADHD Symptoms and Smoking
We found higher rates of ADHD symptoms from the hyperactivity/restlessness and impulsive domains associated with earlier smoking initiation and higher inclination to smoke in the whole sample. A finding relating well to the population-based findings of Kollins’s study (Kollins et al., 2005). Interestingly, the degree of dependence as measured with the FAG score correlated with the severity of childhood ADHD symptomatology.
Limitations
The limitations of the present study are obvious. Our sample was well matched for gender, age, and educational status, but women were overrepresented. Furthermore, a selection bias due to the patient characteristics (treatment seeking) of a university outpatient department cannot be excluded.
Summary and Conclusion
In spite of those shortcomings, our data highlight the high rate of smokers among adult ADHD patients. The special relevance of this study is that it highlights the role of gender for nicotine dependency in adult ADHD patients.
Contrary to general expectations, we found a higher percentage of women smoking in the ADHD group. Our data indicate an earlier onset of regular smoking in female ADHD patients. The significant association between the degree of addiction and the severity of childhood ADHD symptoms as well as the degree of hyperactive and impulsive symptoms points to a developmental relationship between these symptoms and the severity of nicotine dependence.
From a clinical perspective, our data illustrate a clinically important link between adult ADHD and smoking and point to the importance of measures to prevent smoking initiation in these vulnerable patients as well as therapeutic options for patients with adult ADHD who want to quit smoking. As stimulant medication is known to alleviate withdrawal and cessation in smokers with ADHD and as there is some evidence for the preventive effect of stimulant medication in children and adolescents (Gehricke, Hong, Wigal, Chan, & Doan, 2011; Monuteaux, Spencer, Faraone, Wilson, & Biederman, 2007), their prescription in girls might be considered a preventive measure for the treated individual and probably also for his or her future children.
Footnotes
Authors’ Note
Dr. Philipsen served as an advisory role for Janssen-Cilag, Lilly, Novartis, and Shire. She received conference attendance support or speakers fees by Janssen-Cilag, Lilly, and Medice. She has been involved in clinical trials conducted by Janssen-Cilag, Medice, Lilly, and Novartis. The present work is unrelated to the stated grants. Dr. Matthies received speakers fees by Janssen-Cilag and has been involved in clinical trials conducted by Janssen-Cilag and Lilly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported in part by a grant from the German Federal Ministry of Education and Research (BMBF, 01GV0606, Comparison of Methylphenidate and Psychotherapy in Adult ADHD Study, COMPAS).